health education england north west guidance for arcp
TRANSCRIPT
1
Health Education England North West Guidance for ARCP Requirements for ACCS
Trainees in CT1/ST1 and CT2/ST2
Taken from ACCS Core Training Programme Curriculum and Assessment System, April
2012 (https://www.rcoa.ac.uk/system/files/TRG-CU-ACCS2012.pdf)
ACCS is a three year programme consisting of:
Six months Emergency Medicine
Six months Acute Medicine
One year of Anaesthetics and ICM (recommended to be six months in each
specialty)
One further year in chosen parent specialty
Most trainees in HEE NW will complete their year of EM and AM in CT1/ST1 and complete
Anaesthesia and ICM in CT2/ST2.
This document has been prepared to help the trainees and trainers plan for the ARCP at the
end of CT1/ST1 and CT2/ST2.
It is designed to distil much of the key information in the Curriculum into a format that is
easier to navigate. It should be used in conjunction with the HEE NW ACCS ARCP
Checklists which can be found in the Appendix. These checklists have some differences
from the nationally available checklists and reflect the requirements of the local ACCS
scheme.
The checklists must be completed by trainee and supervisor prior to ARCP and they
are mandatory for ARCP Panel A.
If there is any further information required, please consult the Curriculum which has much
more detail about almost all the information in this document.
The evidence of training is divided into sections:
Common Competences: provides generic competences common to all specialities
Major and Acute Presentations: clinical presentations to be covered throughout training
Practical Procedures: to be covered throughout training
Anaesthesia specific curriculum
Intensive Care specific curriculum: in addition to the above competencies
2
Common Competences
These are 25 competences that all doctors should acquire during training. The ways in which
the Curriculum suggests they can be demonstrated are in brackets.
1. History taking (E, Mi, CBD, MSF, ACAT,)
2. Clinical examination (E, Mi, CBD, ACAT)
3. Therapeutics and safe prescribing (E, Mi, CBD, ACAT)
4. Time management and decision making (E, Mi, CBD, M, ACAT)
5. Decision making and clinical reasoning (E, Mi, CBD, ACAT, AA)
6. The patient as central focus of care (E, Mi, CBD, ACAT, PS)
7. Prioritisation of patient safety in clinical practice (E, Mi, CBD, M, ACAT)
8. Team working and patient safety (Mi, CBD, MSF, ACAT)
9. Principles of quality and safety improvement (E, Mi, CBD, MSF, ACAT, AA)
10. Infection control (E, Mi, CBD, ACAT, PS, D,)
11. Managing long term conditions and promoting patient self-care (E, Mi, CBD, MSF,
ACAT, PS)
12. Relationships with patients and communication within a consultation (E, Mi, CBD,
MSF, ACAT, PS)
13. Breaking bad news (E, Mi, CBD, MSF, ACAT, PS, D)
14. Complaints and medical error (CBD, D, MSF)
15. Communication with colleagues and cooperation (Mi, CBD, MSF, ACAT)
16. Health promotion and public health (E, Mi, CBD, MSF, PS)
17. Principles of medical ethics and confidentiality (E, Mi, CBD, MSF, ACAT, PS)
18. Valid consent (E, Mi, CBD, MSF, ACAT, PS)
19. Legal framework for practice (E, Mi, CBD, MSF, ACAT)
20. Ethical research (CBD, Mi, ACAT, AA, D)
21. Evidence and guidelines (E, Mi, CBD, MSF, ACAT)
22. Audit (CBD, AA)
23. Teaching and training (CBD, MSF, TO)
24. Personal behaviour (E, Mi, CBD, MSF, ACAT, PS, D, CBD, Mini-CEX)
25. Management and NHS structure (Mi, CBD, MSF, ACAT, PS, CBD)
At least half of the competences should be at level two or higher by the end of ACCS year
two (i.e. 13/25) with all at level two by the end of year three. Within the NHS ePortfolio, the
common competences level must be completed by your supervisor. For those trainees
without access to the NHS ePortfolio (ACCS-Anaesthesia Trainees), a document that should
be used by you and your supervisor to confirm your level is in the Appendix. The descriptor
definitions of what the four levels represent can be found in the Curriculum.
Guide to assessment methods
AA Audit Assessment
ACAT Acute Care Assessment Tool
CBD Case Based Discussions
D DOPS
E Examination
Mi Mini-CEX
MSF Multisource Feedback
PS Patient Survey
3
Major and Acute Presentations
These competences are focussed on the Core Major Presentations (CMPs) of patients who
need resuscitation and the Core Acute Presentations (CAPs) of patients seen in the ED,
AMU, ICU and in areas where anaesthetics are given
There must be evidence demonstrating competence in all 44 CMPs and CAPs by the end of
CT2/ST2.
At the end of CT2/ST2, trainees will have used Mini-CEX, DOPs, CBD and ACAT for the
assessment of a minimum:
All 6 Core Major Presentations
20 of 38 Core Acute Presentations
The remaining 18 Core Acute Presentations can be completed by Mini-CEX, CBD, ACAT,
eLearning, reflective entries, teaching delivered or audit assessments.
The RCEM have identified a limited number of key CMPs and CAPs that it wishes to be
assessed summatively whilst in the EM placement by an EM Consultant or equivalent. If the
summative assessments are judged unsatisfactory, the assessment can be repeated.
Core Major Presentations (CMPs)
1. Anaphylaxis
2. Cardio-respiratory arrest
3. Major trauma
4. Septic patient
5. Shocked patient
6. Unconscious patient
4
Core Acute Presentations (CAPs)
1. Abdominal pain (including loin pain)
20. Limb pain and swelling (atraumatic)
2. Abdominal swelling/mass/constipation
21. Neck pain
3. Acute back pain
22. Oliguria
4. Aggressive/disturbed behaviour
23. Pain management
5. Blackout/collapse
24. Painful ear
6. Breathlessness
25. Palpitations
7. Chest pain
26. Pelvic pain
8. Confusion (acute)/delirium
27. Poisoning
9. Cough
28. Rash
10. Cyanosis
29. Red eye
11. Diarrhoea
30. Sore throat
12. Dizziness and vertigo
31. Suicidal ideation
13. Falls
32. Syncope and pre-syncope
14. Fever
33. Traumatic limb and joint injuries
15. Fits/seizure
34. Vaginal bleeding
16. Haematemesis and melaena
35. Ventilatory support
17. Headache
36. Vomiting and nausea
18. Head injury
37. Weakness and paralysis
19. Jaundice
38. Wound assessment and management

5
Minimum number of assessments required at each stage of ACCS CT1/ST1 and
CT2/ST2 (and when to do them)
EM
Major Presentations (6) Acute Presentations (38) Practical Procedures (44) 2 of 6 completed summatively (mini-CEX or CBD) by EM Consultant or equivalent:
Major Trauma (if you are not placed in a Trauma Centre/Unit, this could be covered by ATLS/ETC)
Shock
Altered level of consciousness
Sepsis
Anaphylaxis (could be covered by simulation)
Cardiorespiratory arrest (could be covered by ALS or Anaes sign off)
5 of 38 completed summatively (mini-CEX or CBD) by EM consultant or equivalent:
Chest Pain
Abdominal Pain
Breathlessness Mental Health
Head Injury An additional 5 CAPs must be covered using an ACAT, mini-CEX or CBD Further 10 recommended to be completed using combination of:
ACAT
eLearning
Reflective entries
Teaching delivered Audit assessments
5 of 44 completed using DOPs RCEM suggests:
Airway
Primary Survey
Wound Care Fracture/Joint Reduction
At least one other
At the end of the EM placement, seek a summary description of the number and location of
patients seen. This is required for the Structured Training Report.
AM
Major Presentations (6) Acute Presentations (38) Practical Procedures (44)
2 of 6 completed formatively:
Major Trauma Shock
Altered level of consciousness
Sepsis
Anaphylaxis
Cardiorespiratory arrest
10 of 38 using:
Mini-CEX CBD
ACAT 8-10 remaining AP covered using combination of:
ACAT
eLearning Reflective entries
Teaching delivered
Audit assessments
5 of 44 completed using DOPs Please note that some PPs are best suited to completion during AM including:
Lumbar puncture
Pleural tap
Ascitic tap
Abdominal paracentesis
Intensive Care Medicine
Major Presentations (6) Acute Presentations (38) Practical Procedures (44)
2 of 6 completed formatively Complete any of the MPs not covered in EM or AM
Any AP seen in the ICM setting and not completed in EM or AM
13 of 44 using DOPs and other tools

6
Practical Procedures (PPs)
There are 45 practical procedures that trainees are expected to complete during ACCS.
Evidence must be recorded against all 45 PPs by the end of CT2/ST2. Some of these
procedures may not be encountered directly during ACCS training. Whilst it is desirable that
all procedures should be directly observed, evidence may be provided against some of them
using other means (eLearning, simulation or in date ALS or ATLS). The PPs that could be
covered by other forms of evidence are marked by a star below. When not directly observed
during CT/ST1-2, trainees must identify means of becoming competent in each of these
procedures during training.
Procedure AM EM ICM Anaes
1. Arterial cannulation
DOPs
2. Peripheral venous cannulation
DOPs
3. Central venous cannulation
DOPs
4. Arterial blood gas sampling Mini-CEX DOPs
5. Lumbar puncture (expected as DOPs)
6. Pleural tap and drain*
7. Seldinger intercostal drain*
8. Open intercostal drain* (or could be covered by in date ATLS/ETC)
9. Ascitic tap*
10. Abdominal paracentesis*
11. Airway protection
DOPs
12. BLS/ALS DOPs
13. DC cardioversion (could be covered by in date ALS)
14.Knee Aspiration*
15. Temporary pacing (external or wire) (could be covered by in date ALS)
16. Reduction of fracture/dislocation
DOPs
17. Large joint examination (expected as DOPs)
18. Wound management
DOPs
19. Trauma primary survey
DOPs
20. Initial assessment of acutely unwell (expected as DOPS)
21. Secondary assessment of acutely unwell (expected as DOPS)

7
Procedure AM EM ICM Anaes
22. Connection to mechanical ventilator
DOPs
23. Safe use of drugs to facilitate mechanical ventilation
CBD
24. Managing the patient fighting the ventilator
CBD
25. Monitoring respiratory function
CBD
26. Preoperative assessment (IAC)
Mini-CEX
27. Management of spontaneously breathing patient (IAC)
Mini-CEX
28. Administer anaesthesia for laparotomy (IAC)
Mini-CEX
29. Demonstrate RSI (IAC)
Mini-CEX
30. Recover patient from anaesthesia (IAC)
Mini-CEX
31. Demonstrate function of anaesthetic machine (IAC)
DOPs
32. Transfer patient to operating table (IAC)
DOPs
33. Technique of scrubbing up and donning gown and gloves (IAC)
DOPs
34. Basic competences for pain management (IAC)
DOPs
35. Patient identification (IAC)
CBD
36. Post-op N&V (IAC)
CBD
37. Airway Assessment (IAC)
CBD
38. Choice of muscle relaxants and induction agents (IAC)
CBD
39. Post-op analgesia (IAC)
CBD
40. Post-op oxygen therapy (IAC)
CBD
41. Emergency surgery (IAC)
CBD
42. Safe use of vasoactive drugs and electrolytes
Mini-CEX CBD
43. Delivers a fluid challenge safely to an acutely unwell patient
Mini-CEX CBD
44. Describes action required for accidental displacement of tracheal tube or tracheostomy
CBD
45. Demonstrate CPR resuscitation on a manikin
DOPs
Numbers 26 – 41 are required as part of the Anaesthetic Initial Assessment of Competence
8
Anaesthetics within ACCS
The duration of time spent doing anaesthesia has varied between 3 and 9 months nationally
but all trainees are now expected to complete a minimum of six months anaesthesia in
CT1/ST1 or CT2/ST2.
Trainees must complete the Initial Assessment of Anaesthetic Competence and must also
provide evidence at ARCP demonstrating progress towards completion (at least one WPBA
in each module) of the following modules:
1. Preoperative assessment
2. Premedication
3. Induction of general anaesthesia
4. Intra-operative care
5. Post-operative and recovery room care
6. Management of respiratory and cardiac arrest
7. Control of infection
8. Introduction to anaesthesia for emergency surgery
In the ACCS Curriculum and in the NHS ePortfolio these eight modules are called the Basis
of Anaesthetic Practice. In the RCoA Curriculum and ePortfolio, they are called the
Introduction to Anaesthesia.
The further following modules are of interest to the ACCS trainee and it is suggested that the
learning outcomes may also be addressed once all the other modules are completed:
1. Airway management
2. Sedation
3. Transfer medicine
4. Critical incidents
We are aware that there is some discrepancy in some of the national ACCS guidance
regarding the fourth of these optional modules (Regional anaesthesia appears instead of
Critical incidents). We have put Critical incidents in the checklist because it is what appears
in the 2012 Curriculum. As these modules are purely optional, they will not affect Outcome at
ARCP.
Intensive Care Medicine
Time in ICM used to sample the major and acute presentations not covered during EM or
ICM. The minimum number of assessments during ICM part of training is:
3 x Mini-CEX
6 x DOPs
4 x CBD
ICM competences to be completed
1. Demonstrates aseptic peripheral venous cannulation
2. Demonstrates aseptic arterial cannulation (+ local anaesthetic)
3. Obtains arterial blood gas sample and interprets result correctly
4. Demonstrates aseptic placement of central venous catheter
5. Connects mechanical ventilator and selects initial settings
6. Describes safe use of drugs to facilitate mechanical ventilation
7. Describes principles of monitoring respiratory function

9
8. Describes assessment of patient with poor compliance during ventilator support
(fighting the ventilator)
9. Prescribes safe use of vasoactive drugs and electrolytes
10. Delivers a fluid challenge safely to an acutely unwell patient
11. Describe actions required for accidental displacement of tracheal tube or
tracheostomy
Educational Supervision
ACCS trainees will have a different Educational Supervisor in each of their four posts. Their
supervisors will need to complete a Structured Training Report (STR) at the end of each of
post. The STR is called an Educational Supervisors Structured Report (ESSR) in the RCoA
ePortfolio. For ACCS-Anaes trainees in CT1 whose supervisors do not have access to the
RCoA ePortfolio, there is a blank copy of an STR in the Appendix of this document.
Most Trusts have identified a Trust ACCS Training Lead (TATL). This is a consultant who
has overall responsibility for the ACCS trainees in their Trust. They may act as a local point
of contact for any training issues that cannot be resolved by the Educational Supervisor.
Further Requirements
MSF
These must have a minimum of twelve responses and we expect them to include a range of
professions and seniority (including consultants).
There are three MSFs required over the two years:
1. One performed whilst in AM and EM (for most people this is CT1/ST1)
2. One performed whilst in ICM
3. One performed whilst in Anaesthesia
Audit
Evidence of participation in an audit or Quality Improvement Project undertaken each year
Safeguarding Children Level 2
This can be completed locally or via eLearning. A suitable eLearning module can be found
via the e-LfH platform (http://www.e-lfh.org.uk/programmes/safeguarding-children/).
Curriculum Checklists
Please complete the curriculum checklists for your posts and year of training. They
summarise all the evidence that we need to see at ARCP. They are now mandatory for
ARCP.
Form R
Required for revalidation
GMC Survey
Evidence of GMC survey completion should be provided each year
Note for ACCS Anaesthesia Trainees
The RCoA ePortfolio does not include the forms needed to demonstrate competences of the
AM and EM elements of ACCS. The forms required can be found in Appendix A of the 2012

10
ACCS Curriculum. Please use the forms for your current specialty (not parent specialty).
These forms can be uploaded to your ePortfolio but please retain the paper copies which
may be required at ARCP.
Dr Thomas Wiles
Training Programme Director ACCS (Mersey), HEE NW
March 2018
11
Appendices
Contents
Page 11: CT1/ST1 Checklist (Emergency Medicine and Acute Medicine Placements)
Page 15: CT2/ST2 Checklist (Anaesthesia and Intensive Care Medicine Placements)
Page 18: ACCS-Anaes STR for completion in EM and AM Placements
Page 22: ACCS-Anaes Common Competences Record

12
HEE NW ACCS ARCP Checklist ST1/CT1
Trainee: DRN/NTN:
Emergency Medicine
Summative assessments by EM Consultant (or equivalent) in at least 2 Major Presentations (CBD/Mini-CEX)
Date of assessment
Assessor’s name
CMP1 Anaphylaxis
CMP2 Cardio-respiratory arrest (or current ALS) CMP3 Major trauma
CMP4 Septic patient CMP5 Shocked patient
CMP6 Unconscious patient
Summative assessments by EM Consultant (or equivalent) in each of these 5 Acute Presentations (CBD/Mini-CEX)
Date of assessment
Assessor’s name
CAP1 Abdominal pain CAP6 Breathlessness
CAP7 Chest pain CAP18 Head injury
CAP30 Mental health
Non-summative assessment in at least 5 further Acute Presentations using ACAT(EM), CBD or mini-CEX (please insert name & number of each CAP covered)
Date of assessment
Assessor’s name
CAP CAP
CAP CAP
CAP
10 further Acute Presentations completed using teaching delivered/Audit/elearning/Reflective practice/WPBAs (please insert name & number of each CAP covered)
Date of assessment
Assessors name if applicable
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)

13
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
Minimum of 5 Practical Procedures (PPs) as DOPS in 4 following domains and at least one other
Date of assessment
Assessor’s name
Airway maintenance Primary survey
Wound care
Fracture/joint manipulation PP:
PP: PP:
PP: PP:
PP: PP:
14
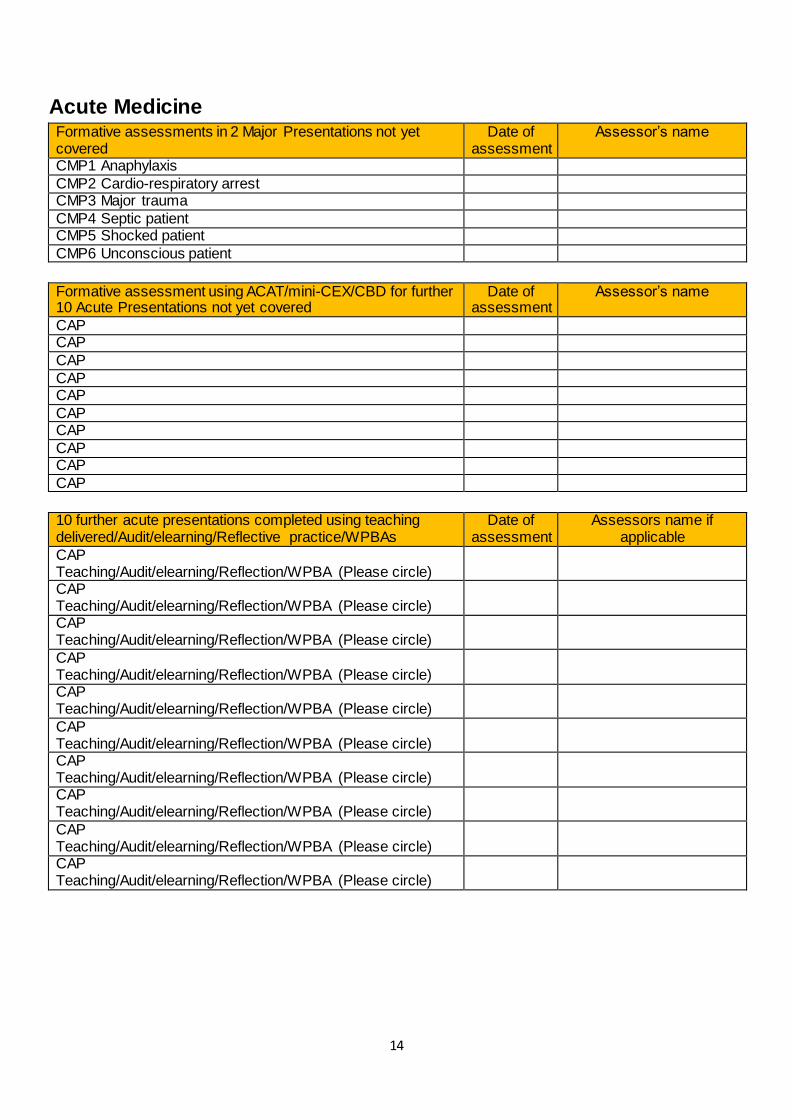
Acute Medicine Formative assessments in 2 Major Presentations not yet covered
Date of assessment
Assessor’s name
CMP1 Anaphylaxis
CMP2 Cardio-respiratory arrest CMP3 Major trauma
CMP4 Septic patient CMP5 Shocked patient
CMP6 Unconscious patient
Formative assessment using ACAT/mini-CEX/CBD for further 10 Acute Presentations not yet covered
Date of assessment
Assessor’s name
CAP CAP
CAP
CAP CAP
CAP CAP
CAP CAP
CAP
10 further acute presentations completed using teaching delivered/Audit/elearning/Reflective practice/WPBAs
Date of assessment
Assessors name if applicable
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)
CAP Teaching/Audit/elearning/Reflection/WPBA (Please circle)

15
Minimum of 5 different practical procedures as DOPS Date of assessment
Assessor’s name
PP:
PP: PP:
PP: PP:
PP: PP:
PP: PP:
PP:
Overview by the end of CT1/ST1
Structured Training Report for each placement
Yes/No
MSF (minimum of 12 responses, reflecting composition of MDT and including consultants)
Yes/No
Evidence of audit or quality improvement project
Yes/No
Resuscitation courses completed:
Safeguarding Children Level 2
Yes/No
Satisfactory progress towards achieving level two in common competences confirmed by supervisor and trainee
Yes/No
Multi Consultant Review x 4 (ACCS-AM trainees only)
Yes/No
Exams taken/planned:
To be completed by trainee and countersigned by Educational Supervisor
Trainee Signature
Date:
ES Signature
Date:
Educational Supervisor name (please print)
16
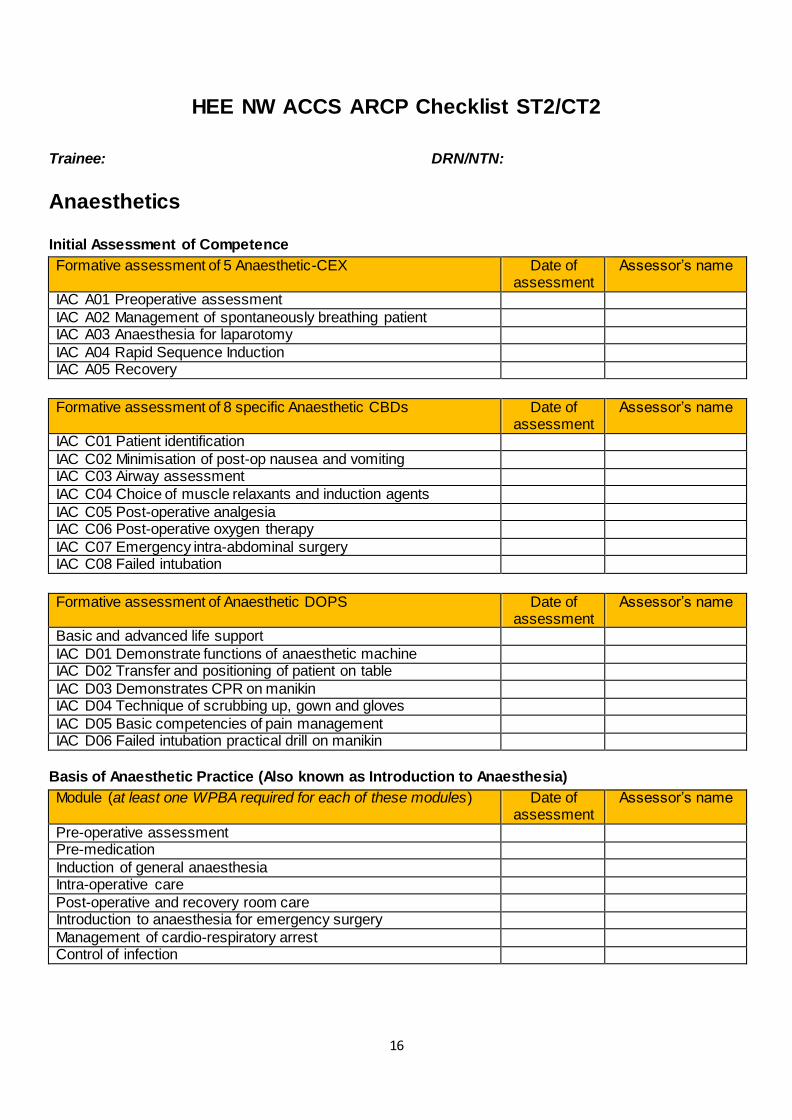
HEE NW ACCS ARCP Checklist ST2/CT2
Trainee: DRN/NTN:
Anaesthetics
Initial Assessment of Competence
Formative assessment of 5 Anaesthetic-CEX Date of assessment
Assessor’s name
IAC A01 Preoperative assessment
IAC A02 Management of spontaneously breathing patient IAC A03 Anaesthesia for laparotomy
IAC A04 Rapid Sequence Induction IAC A05 Recovery
Formative assessment of 8 specific Anaesthetic CBDs Date of assessment
Assessor’s name
IAC C01 Patient identification
IAC C02 Minimisation of post-op nausea and vomiting
IAC C03 Airway assessment
IAC C04 Choice of muscle relaxants and induction agents
IAC C05 Post-operative analgesia
IAC C06 Post-operative oxygen therapy
IAC C07 Emergency intra-abdominal surgery
IAC C08 Failed intubation
Formative assessment of Anaesthetic DOPS Date of assessment
Assessor’s name
Basic and advanced life support
IAC D01 Demonstrate functions of anaesthetic machine IAC D02 Transfer and positioning of patient on table
IAC D03 Demonstrates CPR on manikin IAC D04 Technique of scrubbing up, gown and gloves
IAC D05 Basic competencies of pain management IAC D06 Failed intubation practical drill on manikin
Basis of Anaesthetic Practice (Also known as Introduction to Anaesthesia)
Module (at least one WPBA required for each of these modules) Date of assessment
Assessor’s name
Pre-operative assessment Pre-medication
Induction of general anaesthesia Intra-operative care
Post-operative and recovery room care Introduction to anaesthesia for emergency surgery
Management of cardio-respiratory arrest Control of infection
17
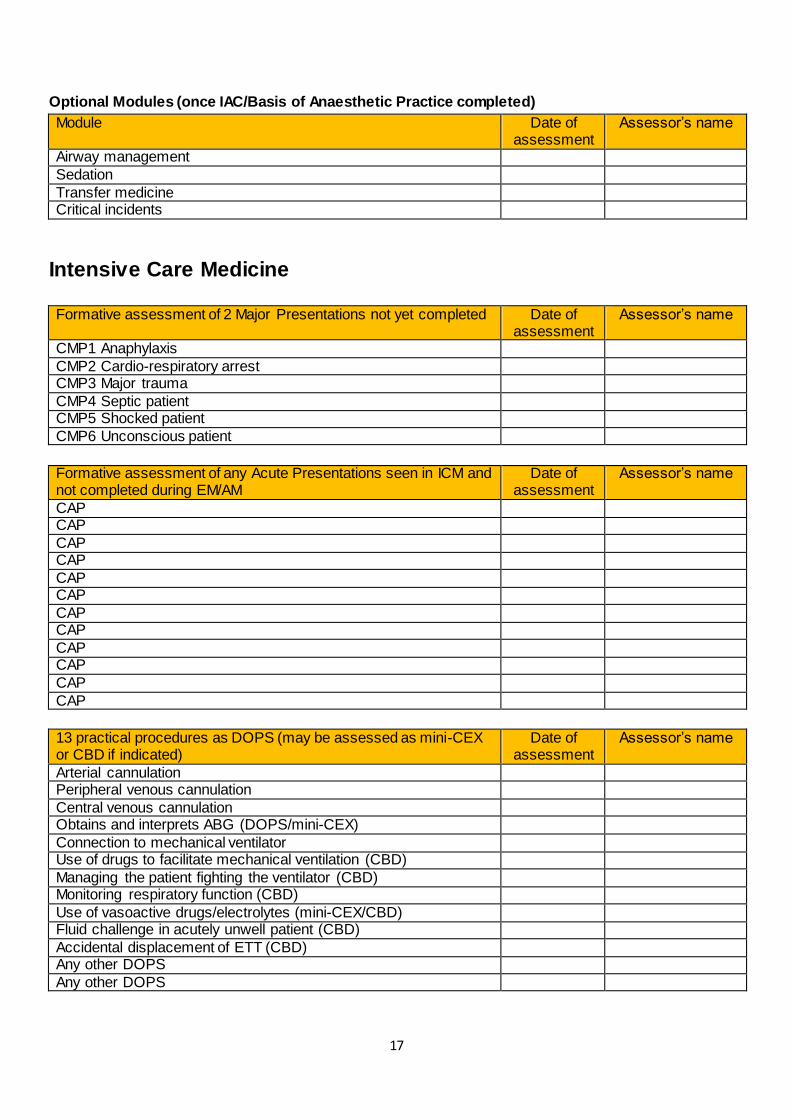
Optional Modules (once IAC/Basis of Anaesthetic Practice completed)
Module Date of assessment
Assessor’s name
Airway management
Sedation
Transfer medicine Critical incidents
Intensive Care Medicine
Formative assessment of 2 Major Presentations not yet completed Date of assessment
Assessor’s name
CMP1 Anaphylaxis
CMP2 Cardio-respiratory arrest CMP3 Major trauma
CMP4 Septic patient CMP5 Shocked patient
CMP6 Unconscious patient
Formative assessment of any Acute Presentations seen in ICM and not completed during EM/AM
Date of assessment
Assessor’s name
CAP CAP
CAP CAP
CAP CAP
CAP CAP
CAP CAP
CAP
CAP
13 practical procedures as DOPS (may be assessed as mini-CEX or CBD if indicated)
Date of assessment
Assessor’s name
Arterial cannulation Peripheral venous cannulation
Central venous cannulation Obtains and interprets ABG (DOPS/mini-CEX)
Connection to mechanical ventilator Use of drugs to facilitate mechanical ventilation (CBD)
Managing the patient fighting the ventilator (CBD) Monitoring respiratory function (CBD)
Use of vasoactive drugs/electrolytes (mini-CEX/CBD) Fluid challenge in acutely unwell patient (CBD)
Accidental displacement of ETT (CBD) Any other DOPS
Any other DOPS
18
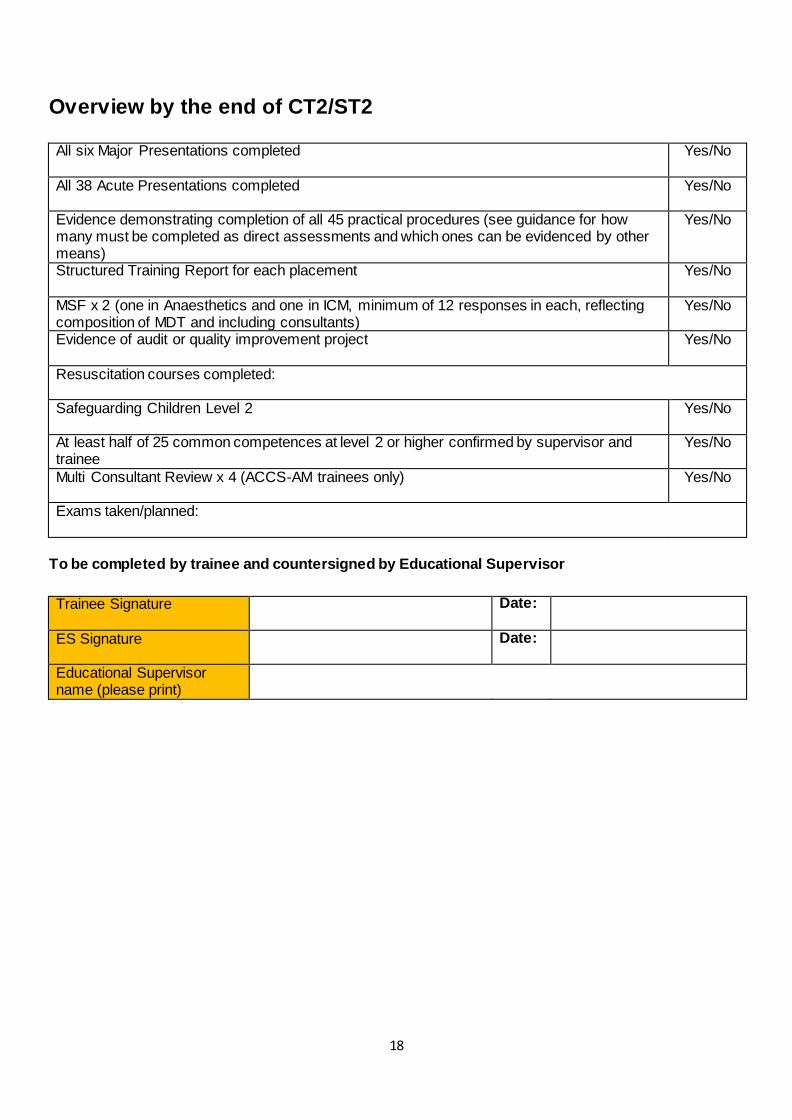
Overview by the end of CT2/ST2
All six Major Presentations completed
Yes/No
All 38 Acute Presentations completed
Yes/No
Evidence demonstrating completion of all 45 practical procedures (see guidance for how many must be completed as direct assessments and which ones can be evidenced by other means)
Yes/No
Structured Training Report for each placement
Yes/No
MSF x 2 (one in Anaesthetics and one in ICM, minimum of 12 responses in each, reflecting composition of MDT and including consultants)
Yes/No
Evidence of audit or quality improvement project
Yes/No
Resuscitation courses completed:
Safeguarding Children Level 2
Yes/No
At least half of 25 common competences at level 2 or higher confirmed by supervisor and trainee
Yes/No
Multi Consultant Review x 4 (ACCS-AM trainees only)
Yes/No
Exams taken/planned:
To be completed by trainee and countersigned by Educational Supervisor
Trainee Signature
Date:
ES Signature
Date:
Educational Supervisor name (please print)
19
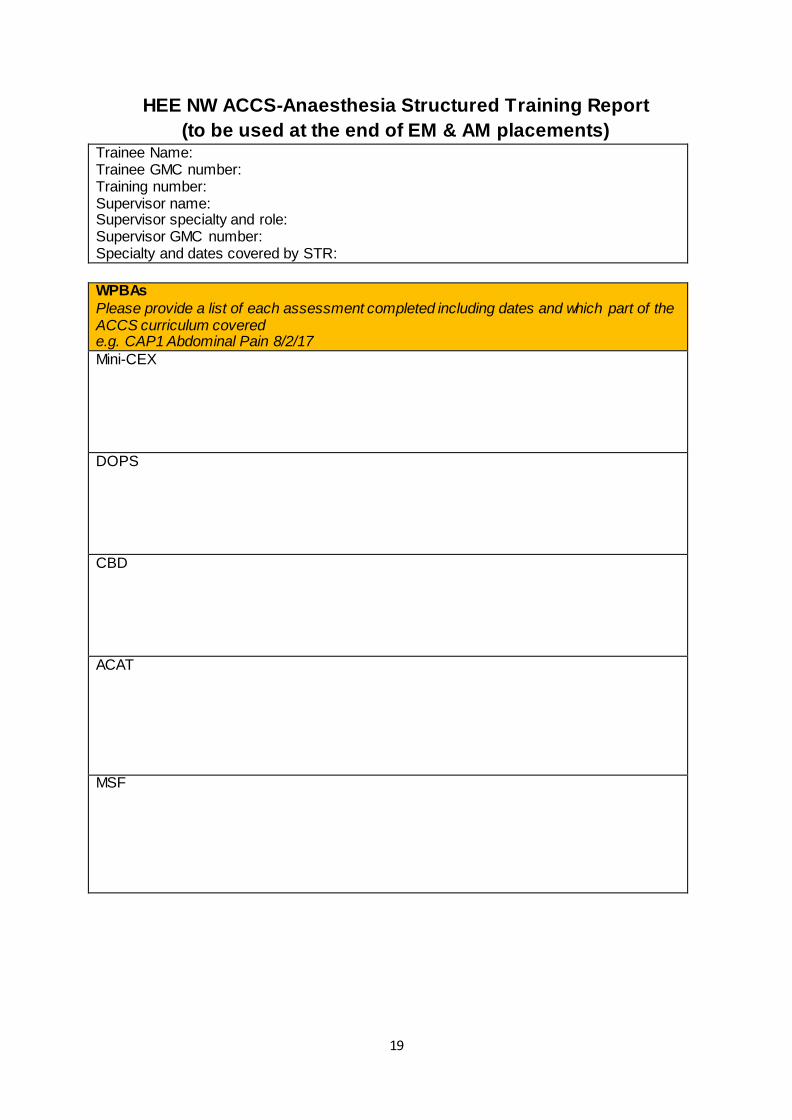
HEE NW ACCS-Anaesthesia Structured Training Report
(to be used at the end of EM & AM placements) Trainee Name: Trainee GMC number: Training number: Supervisor name: Supervisor specialty and role: Supervisor GMC number: Specialty and dates covered by STR:
WPBAs
Please provide a list of each assessment completed including dates and which part of the ACCS curriculum covered e.g. CAP1 Abdominal Pain 8/2/17
Mini-CEX
DOPS
CBD
ACAT MSF

20
Review of other evidence in portfolio
Please review all other evidence (reflection, logs, and eLearning certificates in trainee's portfolio) and provide a brief summary
Reflective practice
Curriculum coverage
Clinical governance/Audit activity
Courses and teaching attended Teaching delivered Management activity Research activity
Mandatory courses
21
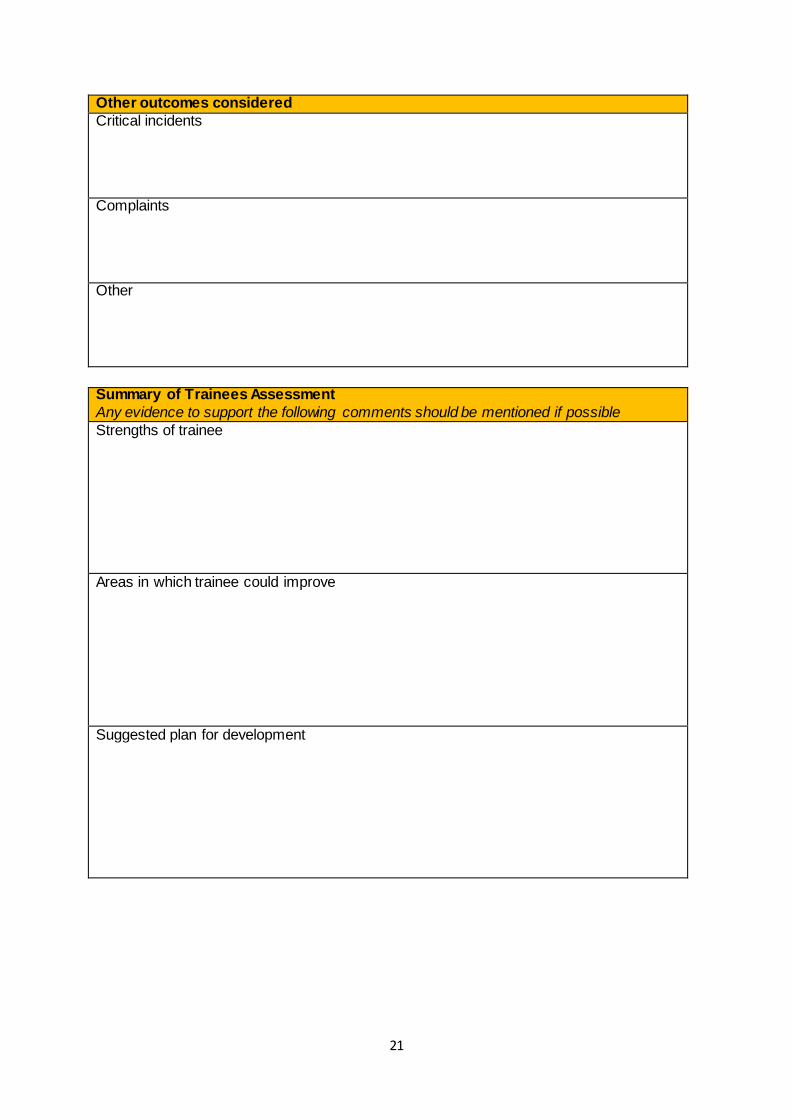
Other outcomes considered
Critical incidents Complaints Other
Summary of Trainees Assessment
Any evidence to support the following comments should be mentioned if possible
Strengths of trainee Areas in which trainee could improve
Suggested plan for development
22
Details of concerns/investigations
Are you aware if this trainee has been involved in any conduct, capability or Serious Untoward Incidents/ Significant Event Investigation or named in any complaint? Yes/No If so are you aware if it has/ these have been resolved satisfactorily with no unresolved concerns about a trainee's fitness to practise or conduct? Yes/No Comments, if any
I confirm that this is an accurate description / summary of this trainee's learning portfolio and WPBA, covering the post specified Supervisor Signature & Date

23
HEE NW ACCS-Anaesthesia Common Competences
Name: DRN/NTN:
Competence Level Achieved (Sign and date)
1 2 3 4
1. 1. History taking 2.
3. 2. Clinical examination 4.
3. Therapeutics & safe prescibing
4. Time & workload
management
5. Decision making & clinical reasoning
6. The patient as central focus
of care
7. Prioritisation of patient safety in clinical practice
8. Team working & patient
safety
9. Principles of quality & safety improvement
10. Infection control
11. Managing long term conditions & promoting patient self-care
12. Relationships with patients and communication within a consultation
13. Breaking bad news
14. Complaints & medical error
15. Communication with
colleagues and cooperation
16. Health promotion and public health
17. Principles of medical ethics
and confidentiality
18. Valid consent
19. Legal framework for
practice
20. Ethical research

24
21. Evidence & guidelines
22. Audit
23. Teaching & training
24. Personal behaviour
25. Management and NHS structure
Please note that the level descriptors can be found in the ACCS Curriculum
Educational Supervisor signature:
Educational Supervisor name (please print):
Trainee signature: