health systems financing and the path to universal coverage new york, october 2010 1 |1 | health...
TRANSCRIPT

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
1 |
Health Systems Financing and the Path to Universal Coverage
by
David B Evans, Director, Health Systems Financing, Health Systems and Services
Carissa Etienne, Assistant Director General, Health Systems and Services
Health Systems Financing and the Path to Universal Coverage
by
David B Evans, Director, Health Systems Financing, Health Systems and Services
Carissa Etienne, Assistant Director General, Health Systems and Services

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
2 |
OUTLINEOUTLINEOUTLINEOUTLINE
1. Universal coverage: the state of the world
2. Health systems financing: determinant and solution
3. The World Health Report 2010 and beyond

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
3 |
Intervention CoverageIntervention CoverageIntervention CoverageIntervention Coverage
1. Coverage with skilled birth attendants as low as 5%. More than 20 countries less than 50%.
2. Coverage with 3 doses of DTP at 1 year: as low as 20% and around 25 countries less than 70%.
3. Great inequalities within most countries – the rich typically have coverage similar to high income countries, and the poor obtain substantially less

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
4 |
Overall coverage and level of inequity differ by types of services
Generally access to delivery by medically trained person more inequitable than vaccination services
05
01
00
1 2 3 4 5
MAR, 2004
SBA DTP
Measles
Pe
rce
nta
ge
quintile
Graphs by code and year
05
01
00
1 2 3 4 5
KHM, 2000
SBA DTP
Measles
Pe
rce
nta
ge
quintile
Graphs by code and year
Patterns of exclusion: delivery by a medically trained person (SBA), DTP3 (DTP) and MCV (MCV)
– from DHS
Patterns of exclusion: delivery by a medically trained person (SBA), DTP3 (DTP) and MCV (MCV)
– from DHS

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
5 |
Financial Risk ProtectionFinancial Risk ProtectionFinancial Risk ProtectionFinancial Risk Protection
Around 150 million people suffer financial catastrophe each year and 100 million pushed into poverty because they use health services, and are forced to pay out of pocket.
Health Systems Financing and the Path to Universal CoverageNew York, October 2010
6 |
A long way from Universal CoverageA long way from Universal CoverageA long way from Universal CoverageA long way from Universal Coverage
World Health Assembly Resolution 58.33, 2005:
Urged countries to develop health financing systems to:
Ensure all people have access to needed services
Without the risk of financial catastrophe linked to paying for care
Defined this as achieving Universal Coverage: coverage with health services; with financial risk protection; for all
Health Systems Financing and the Path to Universal CoverageNew York, October 2010
7 |
What role does health financing play? What role does health financing play?
Three inter-related contributing factors
1. Constant battle to raise sufficient funds for health in all settings, but fundamental insufficiency of resources in many countries. Need to diversify funding sources in others
2. Too much reliance on direct out-of-pocket payments to finance health in many countries – limited financial risk protection. In others, the search for cost–containment means there is pressure to increase cost-sharing.
3. Inefficiency and inequity in use of the available resources in countries, rich and poor

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
8 |
Solutions?Solutions?
Social determinants of health
Socio-economic context
Health systemsoutputs
Health systemsinputs
Health systems &health
outcomes
Supply Demand & Supply Direct effects

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
9 |
Many interacting solutions but health financing is keyWHO Framework for Assessing Health Systems
(World Health Report 2000; Everybody's Business 2006)
Many interacting solutions but health financing is keyWHO Framework for Assessing Health Systems
(World Health Report 2000; Everybody's Business 2006)
INPUTS

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
10 |
Raising Sufficient Funds: Fundamental Insufficiencies Raising Sufficient Funds: Fundamental Insufficiencies
High Level Task Force on Innovative International Financing for Health Systems 2009:
A set of essential services that includes HIV prevention and treatment, and the accompanying health systems development for all interventions – average of $42 per capita (unweighted) in 49 low-income countries in 2009, rising to $65 in 2015
31 of them spent less than $31 per capita per year 2008. Only 8 have any chance of reaching the required funding from domestic sources by 2015.
Health Systems Financing and the Path to Universal CoverageNew York, October 2010
11 |
How to raise more domestically or diversify funding sources in higher-income countriesHow to raise more domestically or diversify funding sources in higher-income countriesIncrease the priority given to health in government budget
allocations– 45 countries currently devote less than 8% of their total
spending to health, and 14 countries devote less than 5%
– Taken as a group, the 49 low-income countries could raise an additional US$ 15 billion per year for health from domestic sources by increasing health’s share of total government spending to 15%.

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
12 |
Raise more domestically or diversify funding sources (cont)
Raise more domestically or diversify funding sources (cont)
Raise revenue for health more efficiently– In Indonesia clear and consistent regulations and a policy of zero-
tolerance for corruption increased tax yield from 9.9% to 11% of non-oil GDP over four years
Find new or diversified sources of funds e.g.– Sales taxes: Ghana funded its national health insurance partly by
increasing the value-added tax (VAT) by 2.5% (p27) – "Sin" taxes, particularly on tobacco and alcohol: a 50% increase in
tobacco tax alone would yield an additional US$1.42 billion just 22 low income countries for which sufficient data exists.
– A currency transaction levy would be feasible in many countries. – Solidarity levies - Gabon raised $30 million for health in 2009 by
imposing a 1.5% levy on companies handling remittances and a 10% tax on mobile phone operators

Proportion of households with catastrophic expenditures vs.share of out-of-pocket payment in total health expenditure
.01
.03
.1.3
13
815
% o
f house
hold
s w
ith c
ata
stro
phic
exp
end
iture
(lo
g)
3 5 8 14 22 37 61 100
out-of-pocket payment in total health expenditure % (logarithm)
OECD others
High Reliance on Direct, Out-of-Pocket Payments (OOPs). Catastrophic expenditures and reliance on OOPs
(OOPs/THE)
No difference is found between social health insurance or tax-based financing systems in terms of protecting households against catastrophic expenditures (Xu et al., Health Affairs 2006).
Health Systems Financing and the Path to Universal CoverageNew York, October 2010
14 |
Threshold?Threshold?
Only when the proportion of direct, out-of-pocket payments in total health expenditures gets to around 20-30% that the incidence of financial catastrophe and impoverishment falls to negligible levels.
Recommendation: move as closely as possible towards this level by strengthening compulsory prepayment (tax, insurance) and pooling

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
15 |
Optimizing prepayment and pooling: learning from country experiences
Optimizing prepayment and pooling: learning from country experiences
– It is possible to make substantial progress towards reducing direct payments, increasing prepayment and covering all people from pooled funds even at lower levels of national income. Chile, Colombia, Mexico, Rwanda, Thailand and Turkey have all made significant progress towards universal access by creating mechanisms that spread the financial risk across the population in the last decade - as have Brazil, China, Costa Rica, Ghana, Kyrgyzstan and the Republic of Moldova.
– Countries choose different mechanisms, mostly involving some mix of tax-based funding with various forms of mandatory insurance, Community insurance and micro-insurance have and can play a valuable role in the transition.
– Where people are allowed to opt-out, it is difficult to ensure that everyone has access to needed services of good quality. The rich and the healthy opt out and the poor and sick are left with poor services.
– Where pools are fragmented, equity goals are much more difficult to achieve – different groups capture better benefits and are reluctant to share

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
16 |
Progressive Realization and Tradeoffs

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
17 |
Inefficiency: Some countries obtain higher levels of Inefficiency: Some countries obtain higher levels of health and coverage for the same expenditure health and coverage for the same expenditure
Inefficiency: Some countries obtain higher levels of Inefficiency: Some countries obtain higher levels of health and coverage for the same expenditure health and coverage for the same expenditure
10
100
1,000
60 62 64 66 68 70 72 74 76 78 80
Life expectancy (years)
To
tal
he
alt
h e
xp
en
dit
ure
pe
r c
ap
ita (
US
$,
20
06)
India
Thailand
China
Uzbekistan
Sri Lanka
Viet Nam
RussiaTurkey
Colombia
Peru
Brazil
Egypt
Bangladesh
Cost RicaCuba
UruguayMexico Chile
Kuwait
Comoros
Palau
Namibia
Hungary
Turkmenistan
Seychelles
Czech RepublicCroatia
Grenada
Latvia
Jordan
Haiti
Nauru
Marshall
Trinidad & Tobago
Kazakhstan
Tuvalu

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
18 |
How much is wasted?How much is wasted?
We estimate that somewhere between 20% and 40% of health resources could be wasted through 10 common causes of inefficiency
Possible areas to search for increased efficiency include
Reducing unnecessary expenditure on medicines and health technologies, using them more appropriately and improving quality control
Reducing leakages and corruption Improving hospital efficiency Choosing the right interventions

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
19 |
Systemic causes of inefficiencySystemic causes of inefficiency
Paying providers:• Fee for service inefficient generally• Payment for performance has been shown to increase
coverage and quality, but needs a good information system and has to be modified frequently
Active purchasing:• Has the potential to improve efficiency, but requires
strong management and no corruption
Fragmentation:• not only makes it difficult to achieve equity goals, but is
inherently inefficient
Health Systems Financing and the Path to Universal CoverageNew York, October 2010
20 |
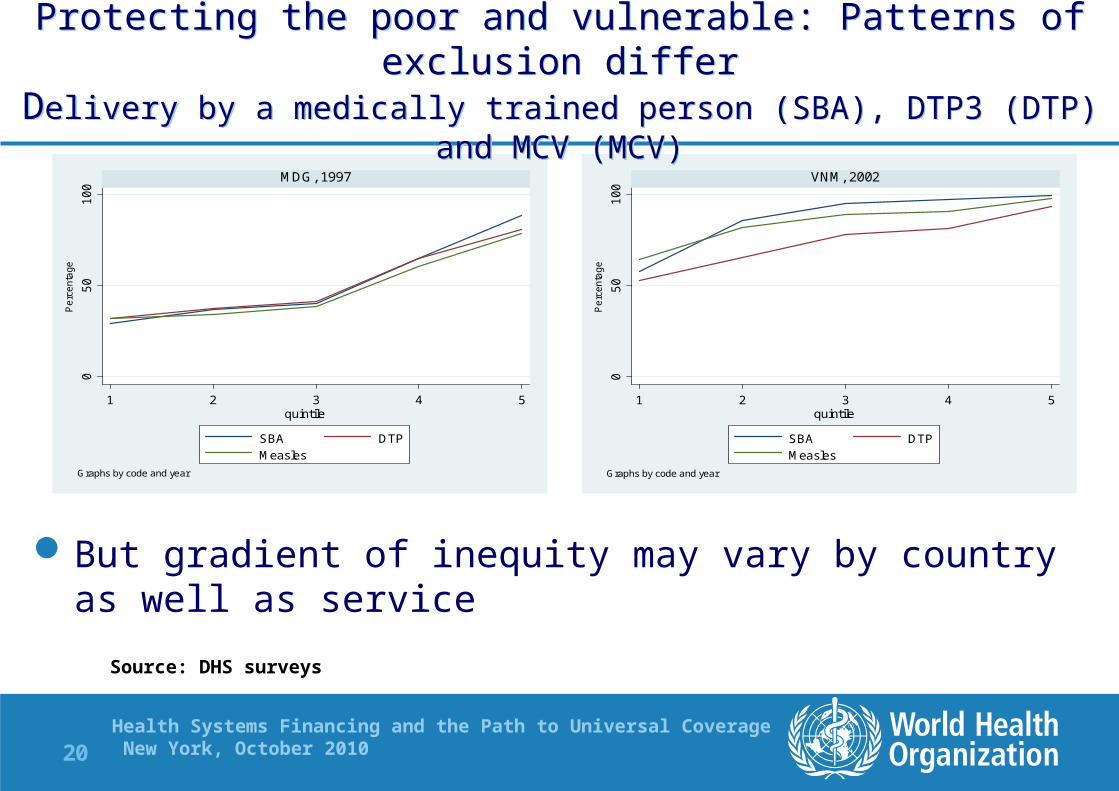
But gradient of inequity may vary by country as well as service
05
01
00
1 2 3 4 5
MDG, 1997
SBA DTP
Measles
Pe
rce
nta
ge
quintile
Graphs by code and year
05
01
00
1 2 3 4 5
VNM, 2002
SBA DTP
Measles
Pe
rce
nta
ge
quintile
Graphs by code and year
Protecting the poor and vulnerable: Patterns of exclusion differDelivery by a medically trained person (SBA), DTP3 (DTP) and MCV (MCV)
Protecting the poor and vulnerable: Patterns of exclusion differDelivery by a medically trained person (SBA), DTP3 (DTP) and MCV (MCV)
Source: DHS surveys

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
21 |
Protecting the poor and vulnerableProtecting the poor and vulnerable
– Free services for groups (exemptions or vouchers) or conditions – exemptions have proved particularly difficult to implement in Africa and ensuring particular services are at zero costs for everyone might be administratively easier
– Charges are not the only financial barrier - see next slide

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
22 |

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
23 |
Protecting the poor and vulnerable (cont)Protecting the poor and vulnerable (cont)
– Cash transfers, conditional or otherwise, offer options for ensuring greater access and providing greater financial risk proteciton. Conditional transfers most appropriate for clearly defined, measureable actions where target group can be easily identified

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
24 |
OUTLINEOUTLINEOUTLINEOUTLINE
1. Universal coverage: the state of the world
2. Health systems financing as a key determinant and solution
3. The World Health Report 2010 and beyond

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
25 |
World Health Report 2010 World Health Report 2010
Health Systems Financing: the Path to Universal CoverageHealth Systems Financing: the Path to Universal Coverage To be launched by WHO on 22 November 2010 followed by a Ministerial
Conference to discuss implications at national and international levels. Hosted by the German Government
Builds on WHO Constitution; Alma Ata and Health for All; World Health Report 2008 on Primary Health Care in which Universal Coverage was
one of the four key areas
Health Systems Financing and the Path to Universal CoverageNew York, October 2010
26 |
World Health Report 2010 World Health Report 2010
1. It builds on country experiences to identify what are options for • Raising more or diversifying funding for health• Minimizing reliance on direct, out-of-pocket payments through
prepayment and pooling• Improving efficiency and equity in resource use
2. It is a message of hope: many examples of countries that have made good progress in at least one of these areas. So every country could do something in at least one of these areas
3. While much of the report is technical, the last chapter recognizes the political realities – there are a lot of necessary steps to ensure that good ideas are implemented in practice

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
27 |
How can the global community better assist countries move more rapidly towards UC
How can the global community better assist countries move more rapidly towards UC
1. Donor and lending institutions agree to mechanisms to ensure predictable, stable, increased flows (for health) – keep promises.
2. Donors and lending institutions fund priority activities included in PRSPs, SWAPs, or strategic plans - or provide budget support to government. Recipient govts should decide priorities rather than donors
2. Channel external funds through existing or nascent institutions for pooling funds rather than bypassing them e.g. Rwanda.

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
28 |
Actions for Global Community - 2Improving Efficiency
Actions for Global Community - 2Improving Efficiency
4. Reduce fragmentation and transaction costs, particularly in the way external funds are channeled and with application and reporting – Estonia for HIV and drug users; Kyrgyzstan for TB funding. Rwanda permanent secretary reported at WHA2010 that Rwanda has to report on 890 different health indicators to the various donors, almost 600 for HIV and TB alone. Vietnam had 400 aid missions to review health projects in 2009.
5. Practice what we preach – get more efficient at global level rather than continually introducing more fragmentation, more secretariats – now more than 140 global health initiatives of various types

Health Systems Financing and the Path to Universal CoverageNew York, October 2010
29 |
Actions for Global Community - 4Actions for Global Community - 4
6. Provide scaled up support to allow countries to develop and implement health financing strategies, and consistent health plans, allowing them to move more quickly towards, or maintain, Universal Coverage
How?