heart failure
TRANSCRIPT
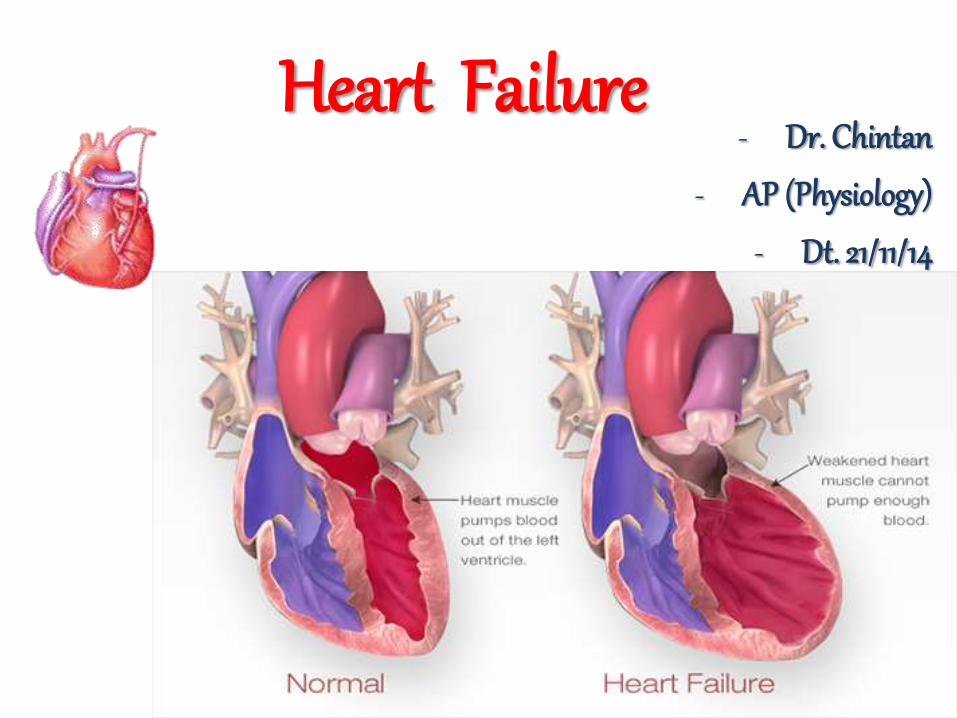
Heart Failure- Dr. Chintan
- AP (Physiology)
- Dt. 21/11/14
Outline• Physiological Anatomy of circulatory system
• Heart as a pump - Cardiac Cycle
• Cardiac Output
• Intro. To heart failure
• Pathophysiology
• Compensated Heart Failure (Acute/Chronic)
• Decompensated Heart Failure
• Types of Heart Failure
• Edema – peripheral, pulmonary
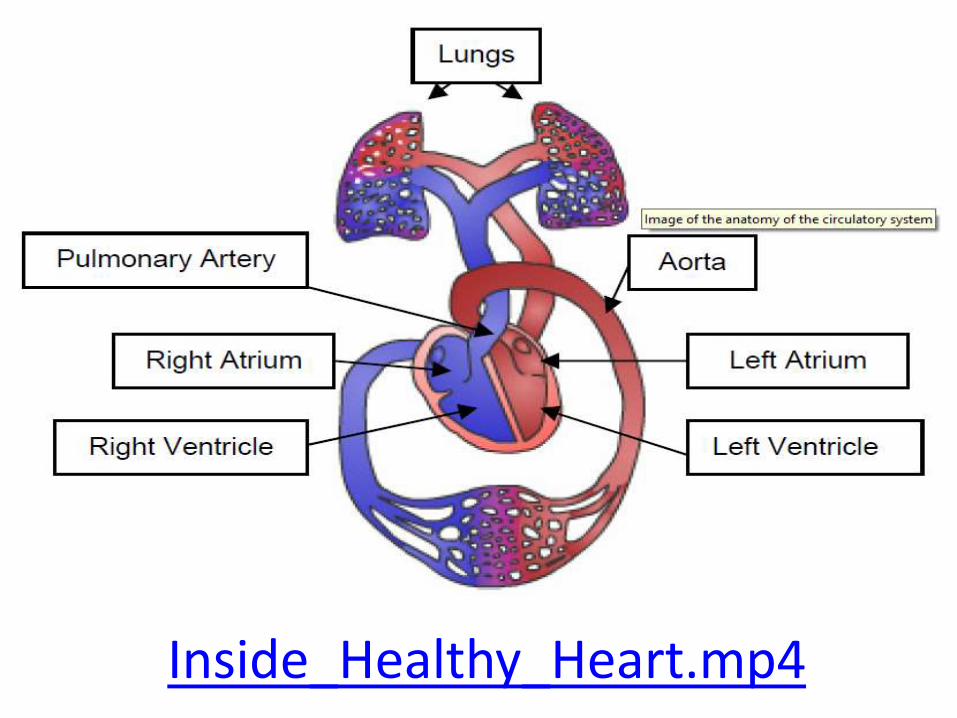
Heart as a pumpRight pump, left pump
Electrical events,mechanical events
The cardiac events that occur from the beginning of oneheartbeat to the beginning of the next are called the cardiaccycle - Each cycle is initiated by spontaneous generation of anaction potential in the sinus node.
AP→ Atria→ A – V bundles→ Ventricles.
AV Delay - .1 sec
Diastole: Period of relaxation – heart fillswith blood.
Systole: Period of contraction – heart pumps the blood.
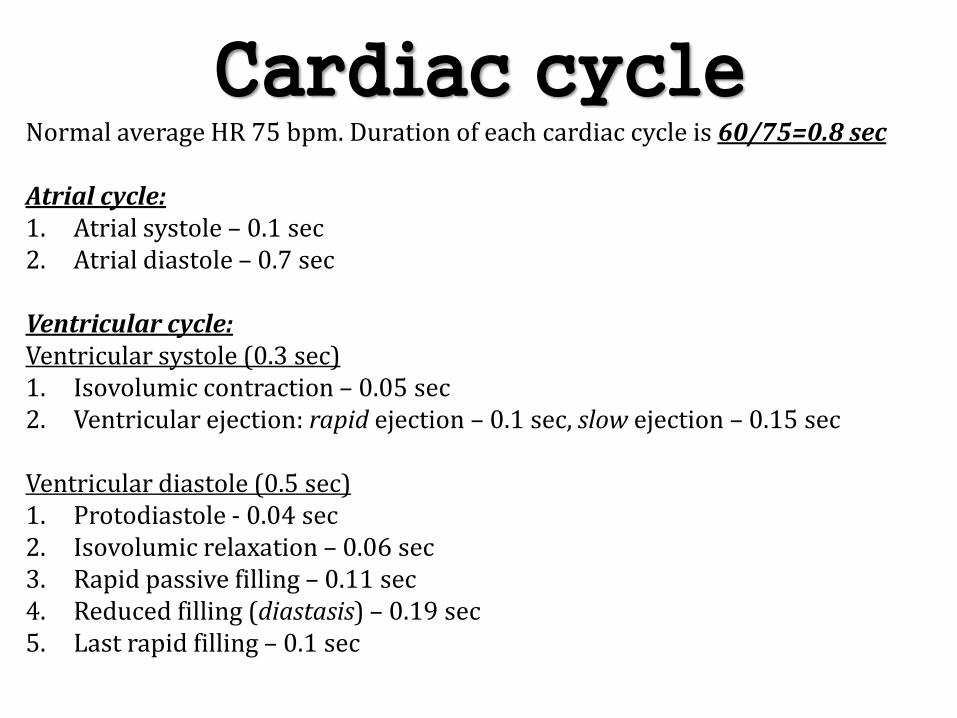
Cardiac cycleNormal average HR 75 bpm. Duration of each cardiac cycle is 60/75=0.8 sec
Atrial cycle:1. Atrial systole – 0.1 sec2. Atrial diastole – 0.7 sec
Ventricular cycle:Ventricular systole (0.3 sec)1. Isovolumic contraction – 0.05 sec2. Ventricular ejection: rapid ejection – 0.1 sec, slow ejection – 0.15 sec
Ventricular diastole (0.5 sec)1. Protodiastole - 0.04 sec2. Isovolumic relaxation – 0.06 sec3. Rapid passive filling – 0.11 sec4. Reduced filling (diastasis) – 0.19 sec5. Last rapid filling – 0.1 sec
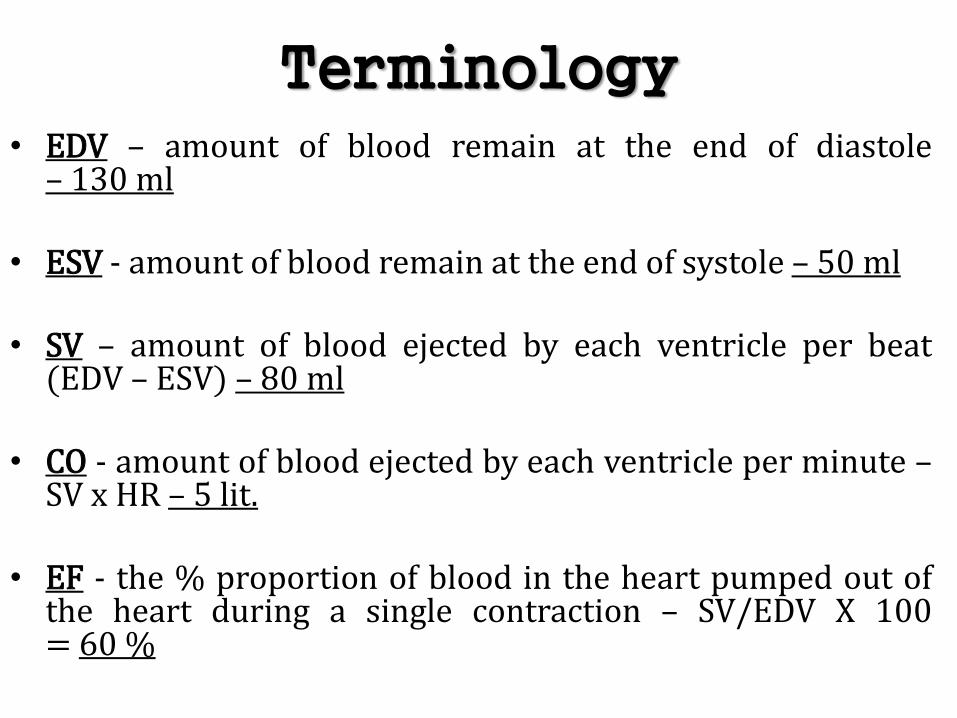
Terminology• EDV – amount of blood remain at the end of diastole
– 130 ml
• ESV - amount of blood remain at the end of systole – 50 ml
• SV – amount of blood ejected by each ventricle per beat(EDV – ESV) – 80 ml
• CO - amount of blood ejected by each ventricle per minute –SV x HR – 5 lit.
• EF - the % proportion of blood in the heart pumped out ofthe heart during a single contraction – SV/EDV X 100= 60 %
Cardiac Output• Cardiac output (CO) = Stroke volume (SV) x Heart Rate
(HR)
• Control of HR
• Autonomic nervous system
• Hormonal (humoral) control
• Control of SV
• Preload (VR, EDV)
• Contractility
• Afterload (PR)
Adaptive mechanisms of the heart to increased load
• Frank - Starling mechanism
• Ventricular hypertrophy
• increased mass of contractile elements → ↑strength of contraction
• Increased sympathetic adrenergic activity
• increased HR, increased contractility
Intro.• Essential functions of the heart
• to cover metabolic needs of body tissue (oxygen,substrates) by adequate blood supply
• to receive all blood coming back from the tissueto the heart
• Essential conditions for fulfilling these functions
• normal structure of the heart
• adequate filling of the heart by blood
Intro.
• Definition - failure of the heart to pump enough blood tosatisfy the needs of the body
• chronic heart failure (CHF), congestive heart failure (CHF),congestive cardiac failure (CCF)
• The cause usually is decreased contractility of themyocardium resulting from diminished coronary blood flow(MI)
• damaged heart valves,• external pressure around the heart,• vitamin B deficiency,• primary cardiac muscle disease (cardiomyopathy)

Heart FailureEtiology
• Primary risk factors– Coronary artery disease (CAD)– Advancing age
• Contributing risk factors – Hypertension– Diabetes– Tobacco use– Obesity– High serum cholesterol– Valvular heart disease– Hypervolemia
Intro.
• Acute – Chronic
• compensated – decompensated
• Forward - backward
• Systolic - diastolic
• Left – right
• Low – high output
• HeartFailureExplained.mp4
Pathophysiology• Reduced force of contraction (↑ preload)
• due to overloading of the ventricle (normal – frank starling low)
• A reduced stroke volume
• Increased ESV is usually caused by reduced contractility.
• Decreased EDV results from impaired ventricular filling – whenthe walls stiffen
• Increased heart rate
• Increased sympathetic activity - increasing coronary perfusionrequirements
• Hypertrophy (↑ afterload)
• increased stiffness and decreased ability to relax during diastole.
Dynamics of the Circulation• Acute Cardiac Failure
• MI
• (1) reduced cardiac output and
• (2) impeding of blood in the veins, resulting inincreased venous pressure
• acute stage usually lasts for only a few seconds,
• because sympathetic nerve reflexes occur immediatelyand compensate for the damaged heart
Compensation for Acute Failure
• circulatory reflexes
• Baroreceptor reflex,
• chemoreceptor reflex,
• CNS ischemic response
• Sympathetic system becomes strongly stimulatedwithin a few seconds – parasympathetic systembecomes reciprocally inhibited
• two major effects on the circulation:
• first on the heart itself,
• second on the peripheral vasculature
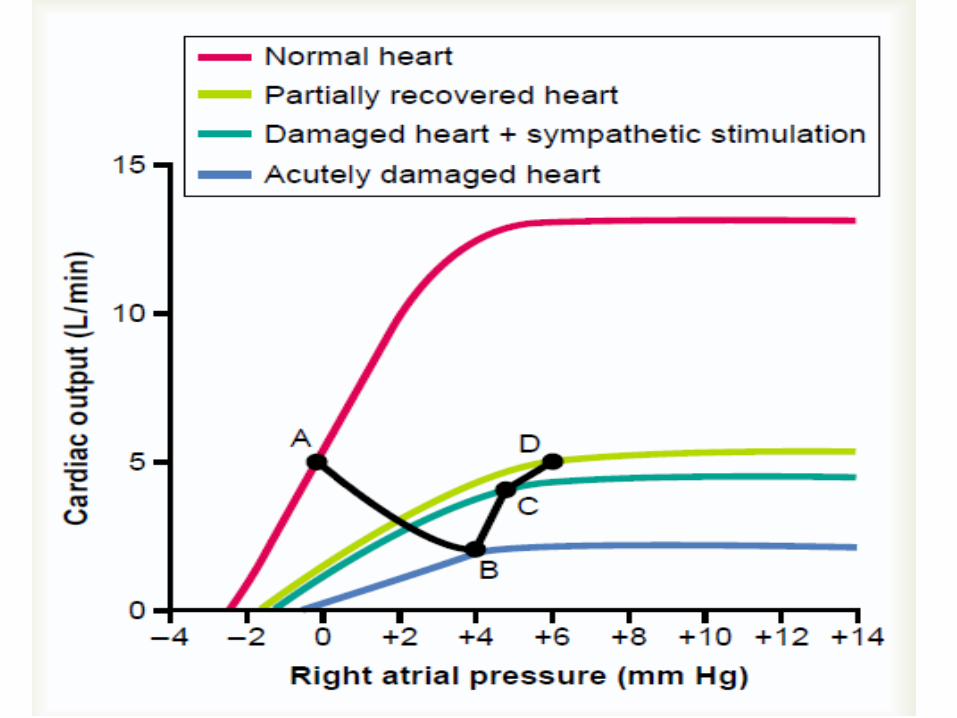
Sympathetic stimulation• Normal muscle is strongly stimulated by sympathetic
stimulation - compensating for the nonfunctional muscle
• Sympathetic stimulation also increases venous returnbecause it increases the tone of most of the blood vessels ofthe circulation, especially the veins
• increased filling pressure greatly increases the tendency forblood to flow from the veins back into the heart.
• the damaged heart becomes primed with more inflowingblood than usual - helps the heart to pump larger quantitiesof blood (Frank Starling Law)
Chronic Stage of Failure• A low cardiac output has a profound effect on renal function
causing anuria - Renal Retention of Fluid
• a moderate increase in body fluid and blood volume is animportant factor in helping to compensate by increasing thevenous return
• Severe fluid retention - severe edema – detrimental - canlead to death
• (1) overstretching of the heart, thus weakening the heartstill more;
• (2) filtration of fluid into the lungs, causing pulmonaryedema
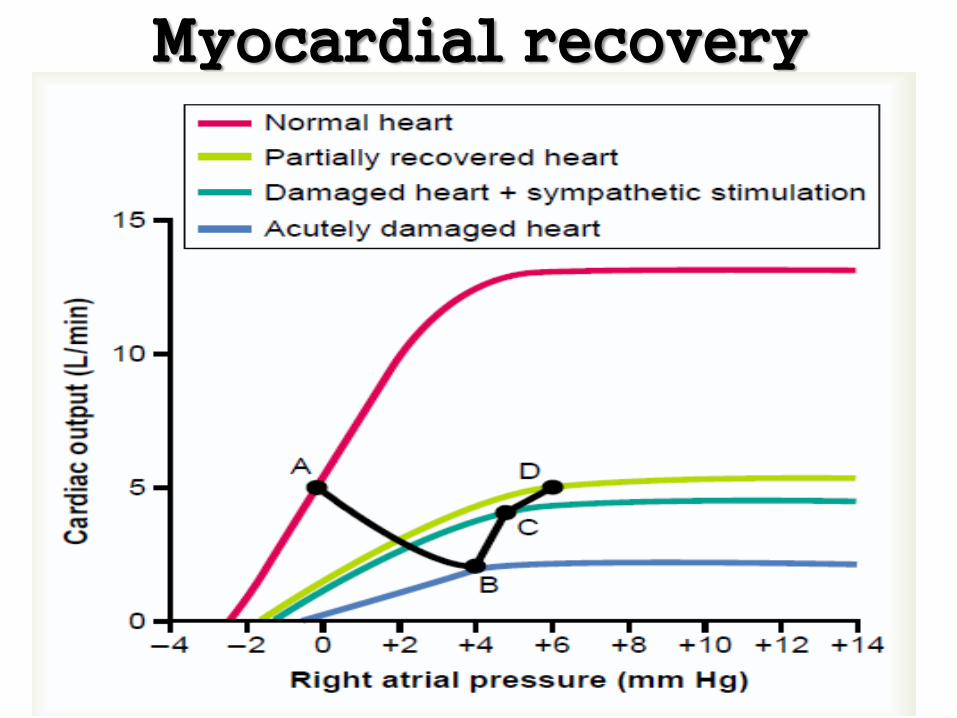
Myocardial recovery
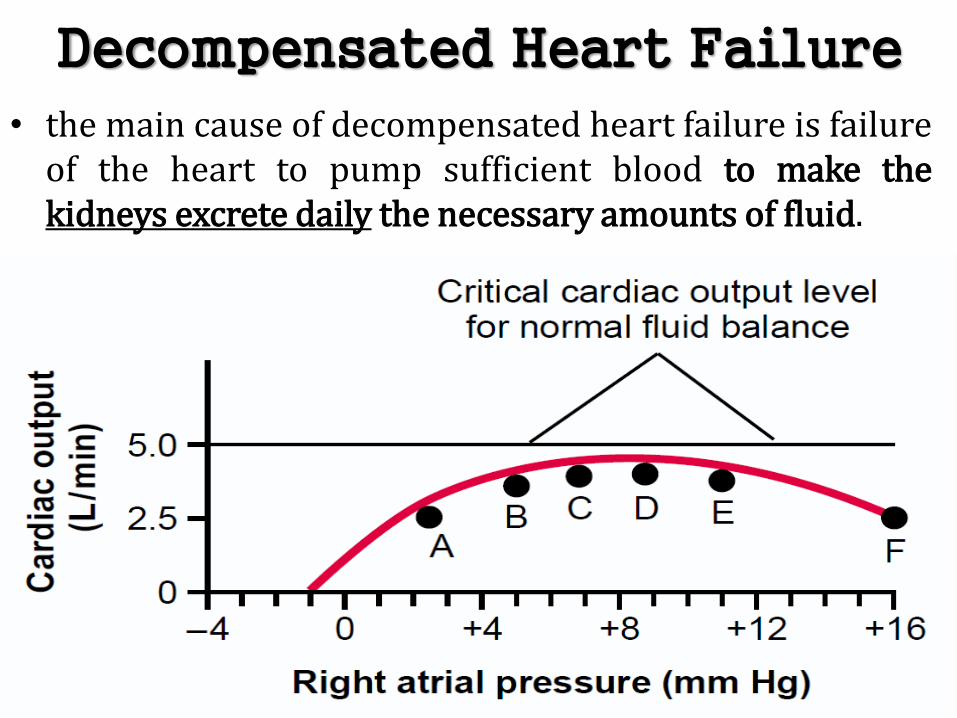
Decompensated Heart Failure
• the main cause of decompensated heart failure is failureof the heart to pump sufficient blood to make thekidneys excrete daily the necessary amounts of fluid.
Forward / backward Heart Failure
• Forward failure – poor ventricular contractility –inadequate perfusion
• Fatigue, Weakness, oliguria, hypotension – CNSischemia, ↑ EDV – cardiomegaly
• Backward failure – poor ventricular filling – venouscongestion – ↑ venous pressure – CCF/CHF
• LVF
• RVF
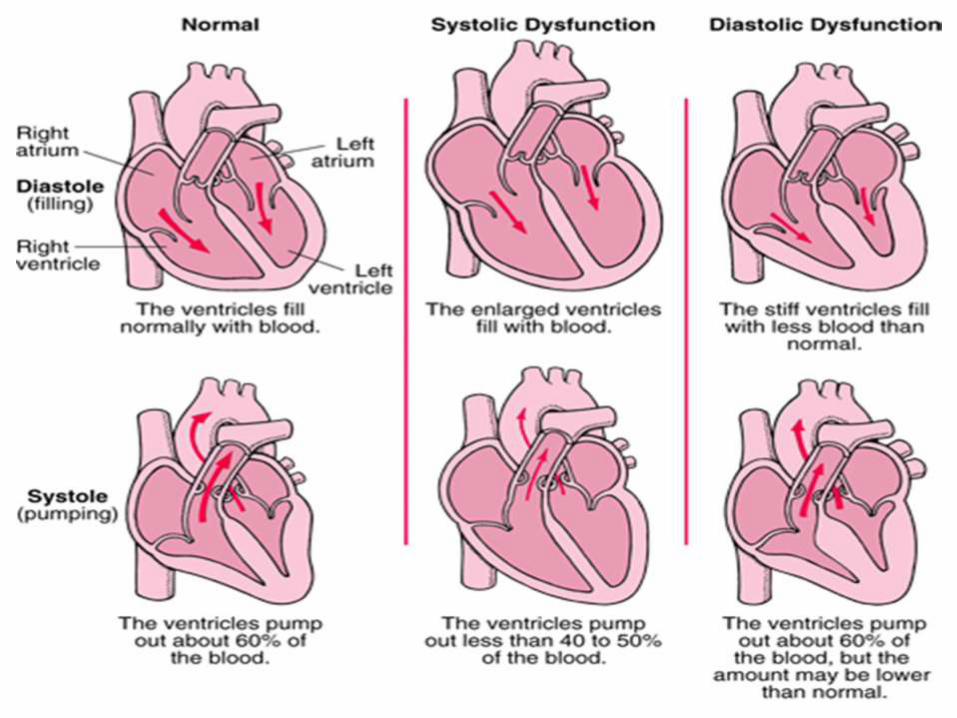
Systolic / Diastolic heart failure• systolic heart failure
• reduced ejection fraction
• left ventricular systolic dysfunction
• poor myocardial contractility
• diastolic heart failure
• preserved ejection fraction
• defective relaxation
• poor ventricular filling
Left Heart Failure• When the left side of the heart fails→ blood continues to be
pumped into the lungs
• it is not pumped adequately out of the lungs by the left heartinto the systemic circulation
• the mean pulmonary filling pressure rises because of shift oflarge volumes of blood from the systemic circulation intothe pulmonary circulation
• pulmonary vascular congestion and pulmonary edema
• Dyspnea, PND, Sputum• LeftSideFailure.mp4
Right Heart Failure• When the right side of the heart fails - ↑ systemic
venous pressure
• Dependent edema – feet, sacral region
• Distended neck veins (↑ JVP)
• Hepato-splenomegaly
• Ascites
• RightSideFailure.mp4
Low Output Cardiac Failure• circulatory shock syndrome caused by inadequate
cardiac pumping is called cardiogenic shock or simplycardiac shock
• the low arterial pressure that occurs during shockreduces the coronary blood supply
• – heart becomes weak
• - arterial pressure fall still more
• - makes the shock still worse
• - eventually becoming a vicious circle
• IHD, HT, valvular-pericardial diseases
High Output Cardiac Failure• Arteriovenous fistula that overloads the heart because
of excessive venous return - pumping capability of theheart is depressed.
• Beriberi, in which the venous return is greatly increasedbecause of diminished systemic vascular resistance -pumping capability of the heart is depressed
• weakening of the heart because of the avitaminosis(mainly lack of thiamine) – peripheral vasodilatation
• Anemia, fever, thyrotoxicosis, A-V malformations
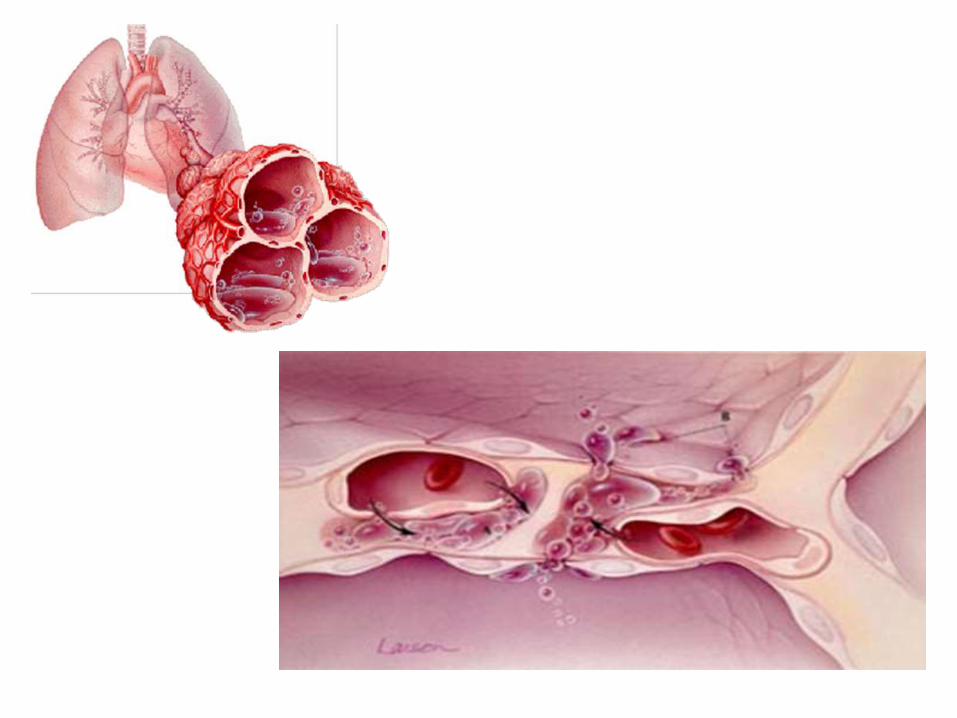
Edema• Acute left heart failure can cause rapid congestion of the
lungs, with development of pulmonary edema and evendeath within minutes to hours.
• Either left or right heart failure is very slow to causeperipheral edema because of fluid retention by the kidneys.
• The retention of fluid increases the mean systemic fillingpressure, resulting in increased tendency for blood to returnto the heart → elevates the right atrial pressure to a stillhigher value and returns the arterial pressure back towardnormal.
• The capillary pressure now also rises markedly, thus causingloss of fluid into the tissues and development of severeedema.
Fluid retention by kidneys• 1. Decreased glomerular filtration.• A decrease in cardiac output has a tendency to reduce the
glomerular pressure in the kidneys because of• (1) reduced arterial pressure• (2) intense sympathetic constriction of the afferent arterioles of
the kidney
• 2. Activation of the renin-angiotensin system• The reduced blood flow to the kidneys causes marked increase in
renin secretion by the kidneys• increased reabsorption of water and salt by the renal tubules
• 3. Increased aldosterone secretion• potassium concentration rises in response to reduced renal
function• ADH secretion – Role of ANP
Acute Pulmonary Edema in Late-Stage
• Pulmonary edema occurs in a person without newcardiac damage - temporary overload of the heart
• heavy exercise, some emotional experience, or severecold
• temporarily increased load on the already weak leftventricle
• → blood begins to dam up in the lungs
• → elevates the pulmonary capillary pressure
• → fluid begins to transude into the lung tissues andalveoli.
Acute Pulmonary Edema in Late-Stage
• increased fluid in the lungs diminishes the degree ofoxygenation of the blood
• → The decreased oxygen in the blood further weakens theheart and also weakens the arterioles everywhere in thebody, thus causing peripheral vasodilation.
• peripheral vasodilation increases venous return of bloodfrom the peripheral circulation still more
• → The increased venous return further increases thedamming of the blood in the lungs,
• → still more transudation of fluid,
• → more arterial oxygen desaturation,
• → more venous return and so forth.