heart failure khalid f alhabib.mbbs.frcpc cardiology consultant king fahad cardiac centre king saud...
TRANSCRIPT

Heart FailureHeart Failure
Khalid F AlHabib.MBBS.FRCPCKhalid F AlHabib.MBBS.FRCPCCardiology ConsultantCardiology Consultant
King Fahad Cardiac CentreKing Fahad Cardiac CentreKing Saud UniversityKing Saud University
Wednesday, April 19, 2023Wednesday, April 19, 2023

Heart Failure: OutlineHeart Failure: Outline
Definition Definition CausesCauses Epidemiology Epidemiology PathophysiologyPathophysiology Clinical AssessmentClinical Assessment ManagementManagement Prognosis Prognosis

Heart FailureHeart Failure: Definition: Definition
Complex syndrome in which abnormal Complex syndrome in which abnormal heart function results in, or increases the heart function results in, or increases the subsequent risk of, clinical symptoms and subsequent risk of, clinical symptoms and signs of low cardiac output &/or pulmonary signs of low cardiac output &/or pulmonary or systemic congestion. or systemic congestion.

CAUSES & FORMSCAUSES & FORMS

Systolic versus Diastolic HF




PREVALENCE & COSTPREVALENCE & COST

The number of CHF patients will almost double between the years 1990-2030, from these 3 million cases of overt CHF to about 6 million.
Heart Failure: a major public health problemHeart Failure: a major public health problem
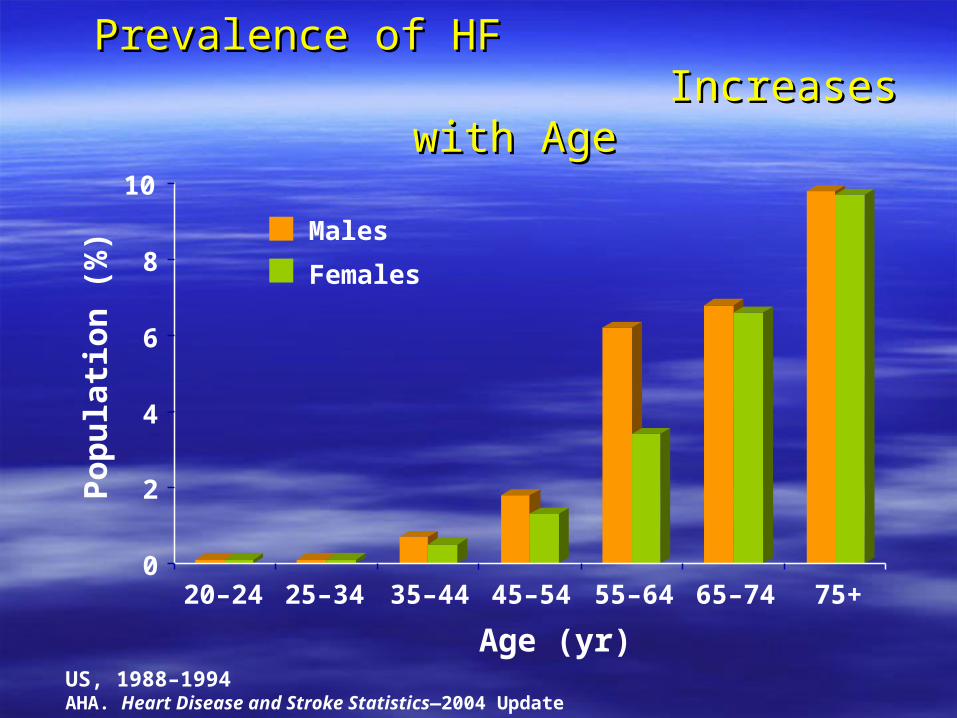
Prevalence of HF Prevalence of HF Increases with AgeIncreases with Age
US, 1988–1994AHA. Heart Disease and Stroke Statistics—2004 Update
0
2
4
6
8
10
20–24 25–34 35–44 45–54 55–64 65–74 75+
Age (yr)
Po
pu
lati
on
(%
)
Males
Females

Estimated Direct and Indirect Costs of HF in USEstimated Direct and Indirect Costs of HF in US
8%
8% 10%
7%
14%
53%
Hospitalization$13.6
Lost Productivity/Mortality*
$2.1
Home Healthcare$2.1
Drugs/Other Medical Durables
$2.7
Physicians/Other Professionals
$1.8
Nursing Home$3.5
*Lost future earnings of persons who will die in 2004, discounted by 3%AHA. Heart Disease and Stroke Statistics—2004 Update
Total Cost$25.8 billion

PATHOPHYSIOLOGYPATHOPHYSIOLOGY







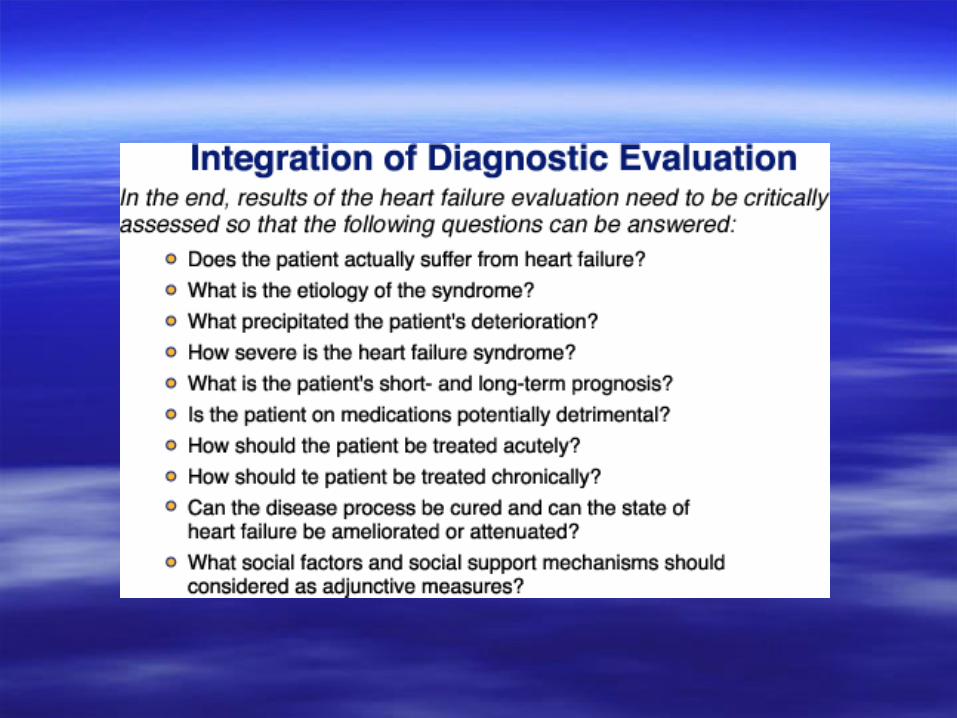
CLINICAL EVALUATIONCLINICAL EVALUATION






ACUTE VS. CHRONIC HEART FAILURE
FEATURE ACUTE HEART FAILURE DECOMPENSATED CHRONIC HEART FAILURE
CHRONIC HEART FAILURE
Symptom severity Marked Marked Mild to moderate
Pulmonary edema Frequent Frequent Rare
Peripheral edema Rare Frequent Frequent
Weight gain None to mild Frequent Frequent
Whole-body fluid volume load No change or mild increase Moderate to marked increase Mild to marked increase
Cardiomegaly Uncommon Usual* Common*
Ventricular systolic function Reduced, normal, or hypercontractile
Reduced* Reduced*
Wall stress Elevated Markedly elevated Elevated
Activation of sympathetic nervous system Marked Marked Mild to marked
Activation of renin-angiotensin-aldosterone system
Often increased Marked Mild to marked
Reparable, reversible causative lesion(s) Common Occasional Occasional
*Patients with diastolic heart failure may have little to no cardiomegaly and normal systolic function.
Clinical and pathophysiological characteristics of the two major categories of unstable heart failure (acute heart failure and decompensated chronic heart failure) are compared with those of chronic heart failure.
Adapted from Leier CV: Unstable heart failure. In Colucci WS (ed): Heart Failure: Cardiac Function and Dysfunction. 2nd ed. In Braunwald E (series ed): Atlas of Heart Diseases, vol 4. Philadelphia, Current Medicine, 1999, pp 9.1–9.17.



A, Pulmonary blood flow redistribution. Enlargement of the upper lobe vessels is seen in a patient with ischemic cardiomyopathy and elevated pulmonary venous pressure. B, Pulmonary interstitial edema. The vessels are indistinct and enlarged, and peribronchial cuffing is present. C, Pulmonary alveolar edema in a patient with congestive cardiomyopathy. The central perihilar distribution of edema, termed “bat wing” edema, is typical of pulmonary alveolar edema caused by cardiovascular or fluid overload (uremic). D, Preferential right upper lobe distribution of pulmonary edema in a 65-year-old man with mitral regurgitation. E, Right pleural effusion and residual right upper and bilateral lower lobe edema in a patient with acute mitral regurgitation.


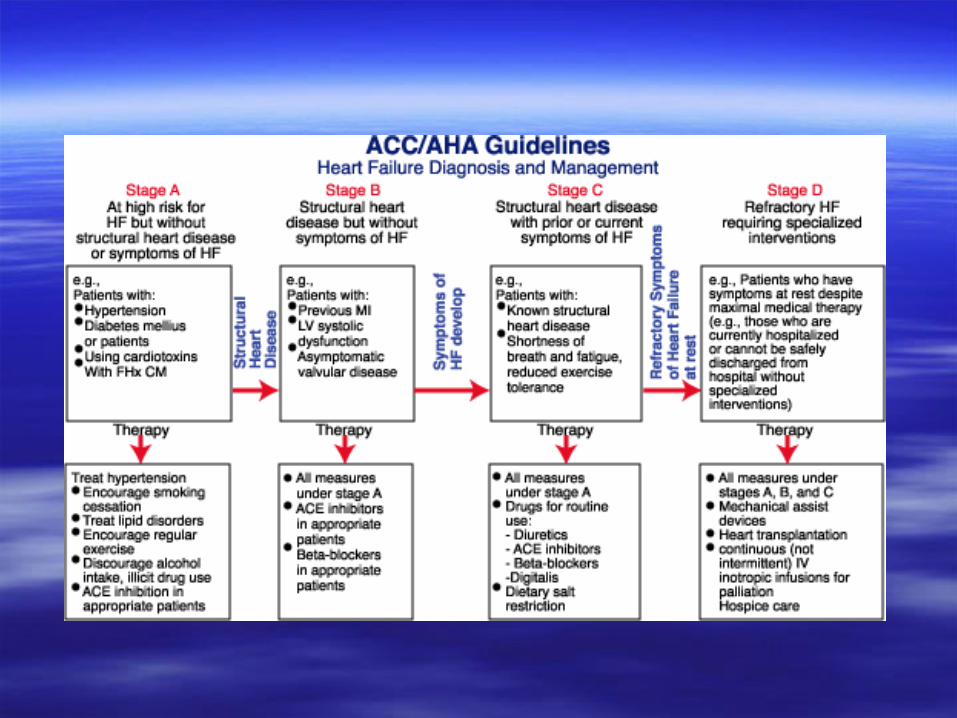
MANAGEMENTMANAGEMENT



PROGNOSISPROGNOSIS


Causes of Hospital Readmission for Causes of Hospital Readmission for Congestive Heart FailureCongestive Heart Failure
17%Other
19%Failure to Seek
Care
16%Inappropriate Rx
Rx Noncompliance 24%
Diet Noncompliance24%
Annals of Internal Medicine 122:415-21, 1995
Over 2/3 of HF Hospitalizations Preventable

Prognosis with Heart Failure: Prognosis with Heart Failure: More “Malignant” Than CancerMore “Malignant” Than Cancer ! !
0102030405060708090
100
0 1 2 3 4 5 6 7 8 9 10
Su
rviv
al %
Women
Men
AHA, 1998 Heart and Statistical UpdateNCHS, National Center for Health Statistics
Survival after the onset of congestive heart failure in Framingham Heart Study subjects
Ho Circulation 1993;88:107-115
Years
Overall5-year mortality 50%

In Summary..In Summary..