heart failure-updates and practical ... at the completion of this presentation, participants will be...
TRANSCRIPT
HEART FAILURE-UPDATES AND PRACTICAL APPROACHES TO PATIENT CARE
DR DEAN T. GOROSKI, BCPS, CAPT, USPHS
2018 MPA WINTER CE AND SKI MEETING
BIG SKY, MT JANUARY 6, 2018
DISCLOSURE
➢Dr. Goroski has no actual, perceived, probable, suggested,
potential, imaginary, conceptualized, likely, hopeful, aggravated,
insinuated, or otherwise conflict of interest in relation to this
program/presentation.
OBJECTIVES
➢At the completion of this presentation, participants
will be able to :
➢Describe and differentiate the main diagnoses of heart failure
➢Describe the pharmacologic goals of heart failure treatment
and identify opportunities to optimize treatment
➢ Identify lifestyle changes to promote positive patient
outcomes in heart failure management
OBJECTIVES
➢Describe and differentiate the main diagnoses of heart failure
➢Describe the pharmacologic goals of heart failure treatment
and identify opportunities to optimize treatment
➢ Identify lifestyle changes to promote positive patient
outcomes in heart failure management
CHRONIC HEART FAILURE (CHF)
➢HF is a complex clinical syndrome that results from any
structural or functional impairment of ventricular
filling(diastole) or ejection(systole) of blood.
➢The cardinal manifestations of HF are dyspnea and fatigue-
which may limit exercise tolerance, and fluid retention-which
may lead to pulmonary and/or splanchnic congestion and/or
peripheral edema.
Clyde W. Yancy et al. Circulation. 2013;128:e240-e327
HF DEFINITION IN BASIC TERMS
➢Previously defined as Congestive Heart Failure
➢Heart is unable to pump blood a sufficient volume of blood
(cardiac output) to meet metabolic demands of the body
➢Cardiac Output (CO) = Heart Rate (HR) x Stroke Volume
(SV)
MORE DEFINITIONS
➢Afterload--tension developed
in the LV wall as systole
occurs. Mainly determined by
arterial blood pressure
➢Preload--combination of
pressure and volume in the
left ventricle at the end of
diastole (completely filled
ventricle)
AND MORE DEFINITIONS…
➢Ejection Fraction (EF)
➢The percentage of left ventricular blood volume ejected
during systole(contraction)
➢Normal is generally defined as 60-70%
➢Right-sided and Left-sided HF
➢Anatomical definitions only
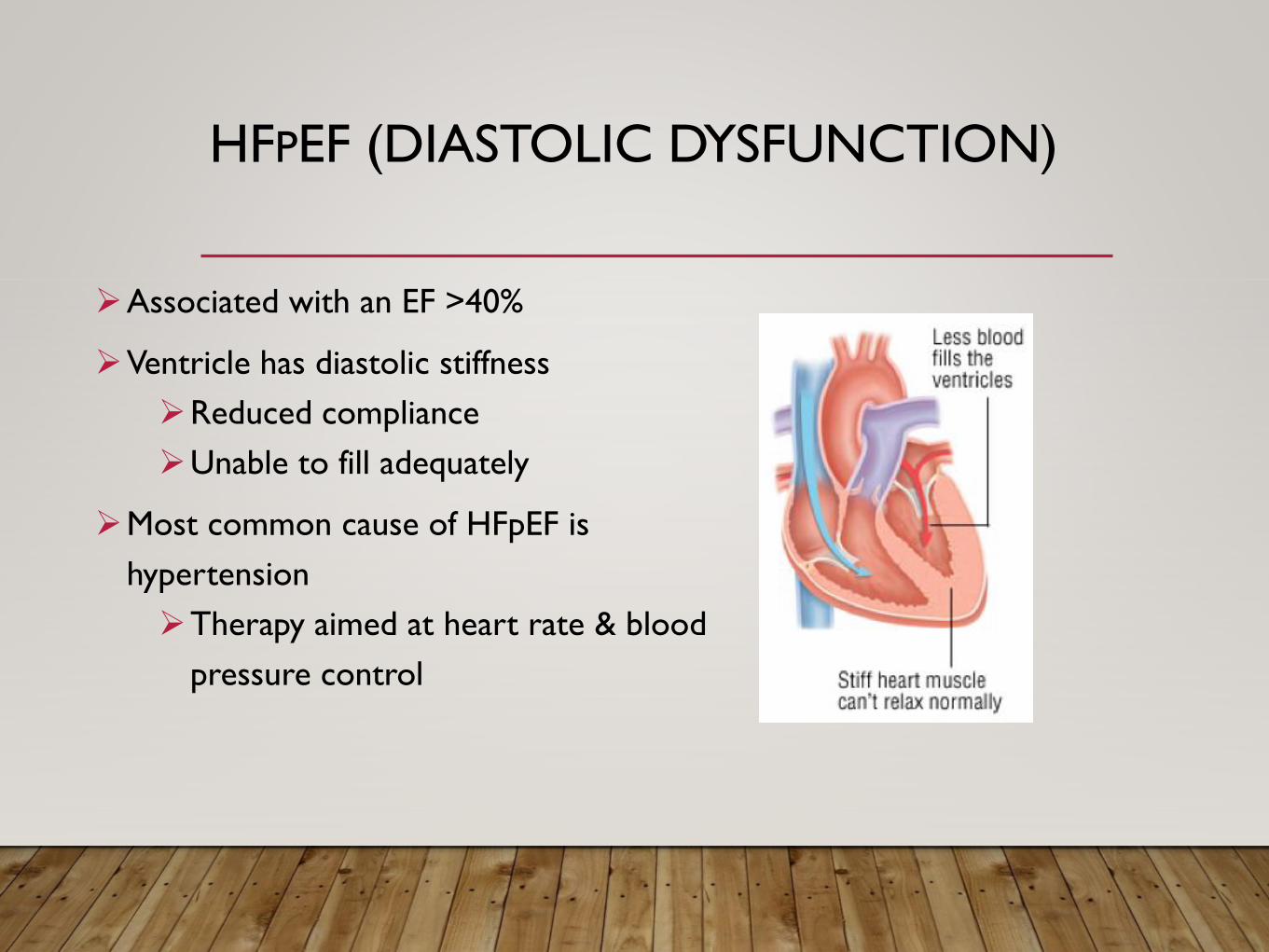
HFPEF (DIASTOLIC DYSFUNCTION)
➢Associated with an EF >40%
➢Ventricle has diastolic stiffness
➢Reduced compliance
➢Unable to fill adequately
➢Most common cause of HFpEF is
hypertension
➢Therapy aimed at heart rate & blood
pressure control
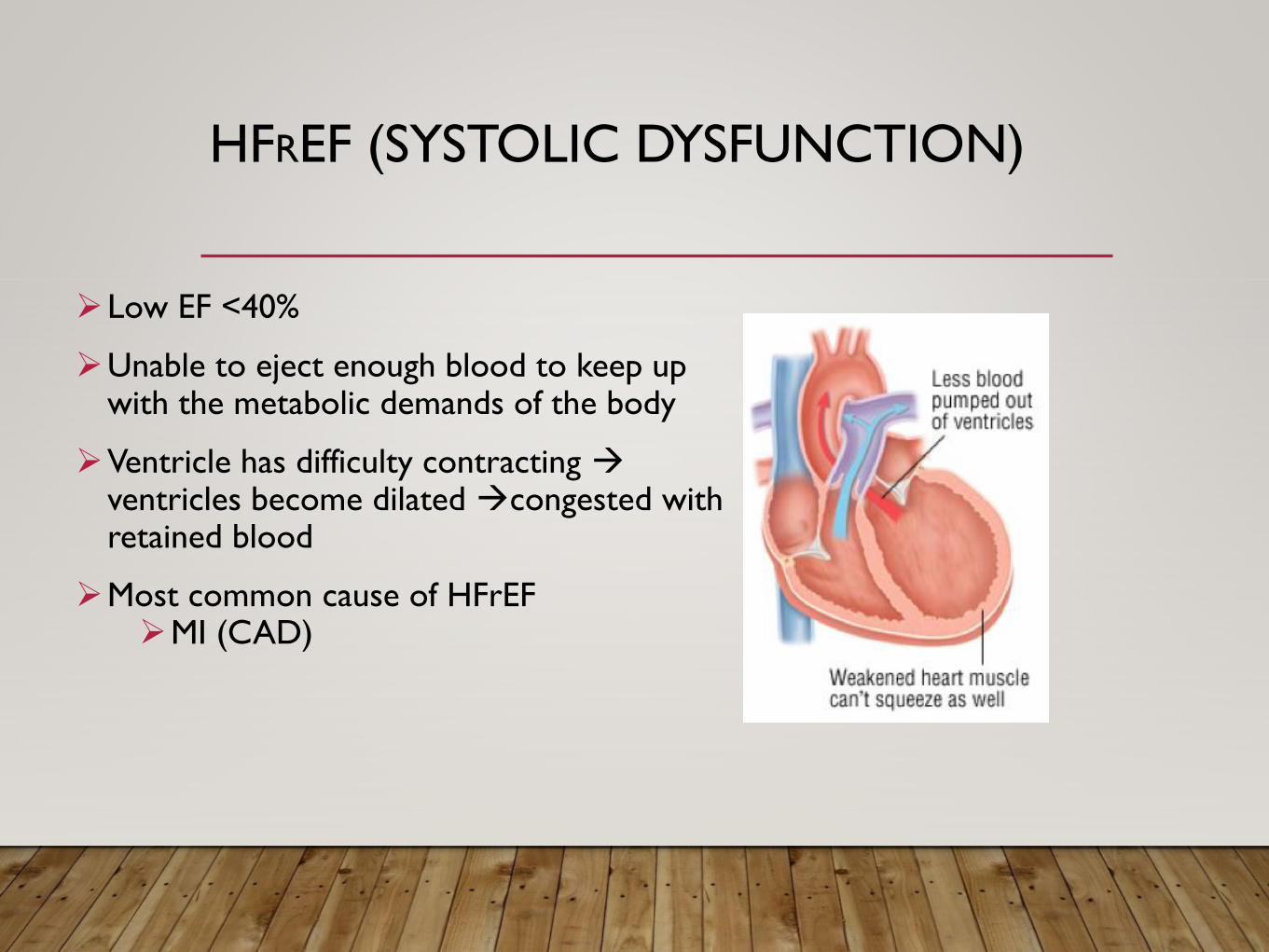
HFREF (SYSTOLIC DYSFUNCTION)
➢Low EF <40%
➢Unable to eject enough blood to keep up with the metabolic demands of the body
➢Ventricle has difficulty contracting ventricles become dilated congested with retained blood
➢Most common cause of HFrEF➢MI (CAD)
PRESENTATION
SIGNS
➢Pulmonary rales
➢Lower leg edema
➢ Jugular venous distention
➢ Increase BNP
SYMPTOMS
➢Dyspnea (on exertion)
➢Orthopnea
➢Paroxysmal nocturnal dyspnea
➢Edema
➢Fatigue
➢Exercise intolerance
ASSOCIATED COMPLICATIONS IN HF MANAGEMENT
➢Cardiac-AF, heart block, valvular abnormalities, CAD, anti-
clotting therapies
➢Organ systems-renal failure, hepatic failure, respiratory
disease
➢Endocrine-DM, hypo/hyperthyroidism, endocrine tumors
➢Other-obesity, nutrition, tobacco, toxins, emotional,
economic, social, educational, financial, geographic, physical,
transplant considerations, gout, etc…..
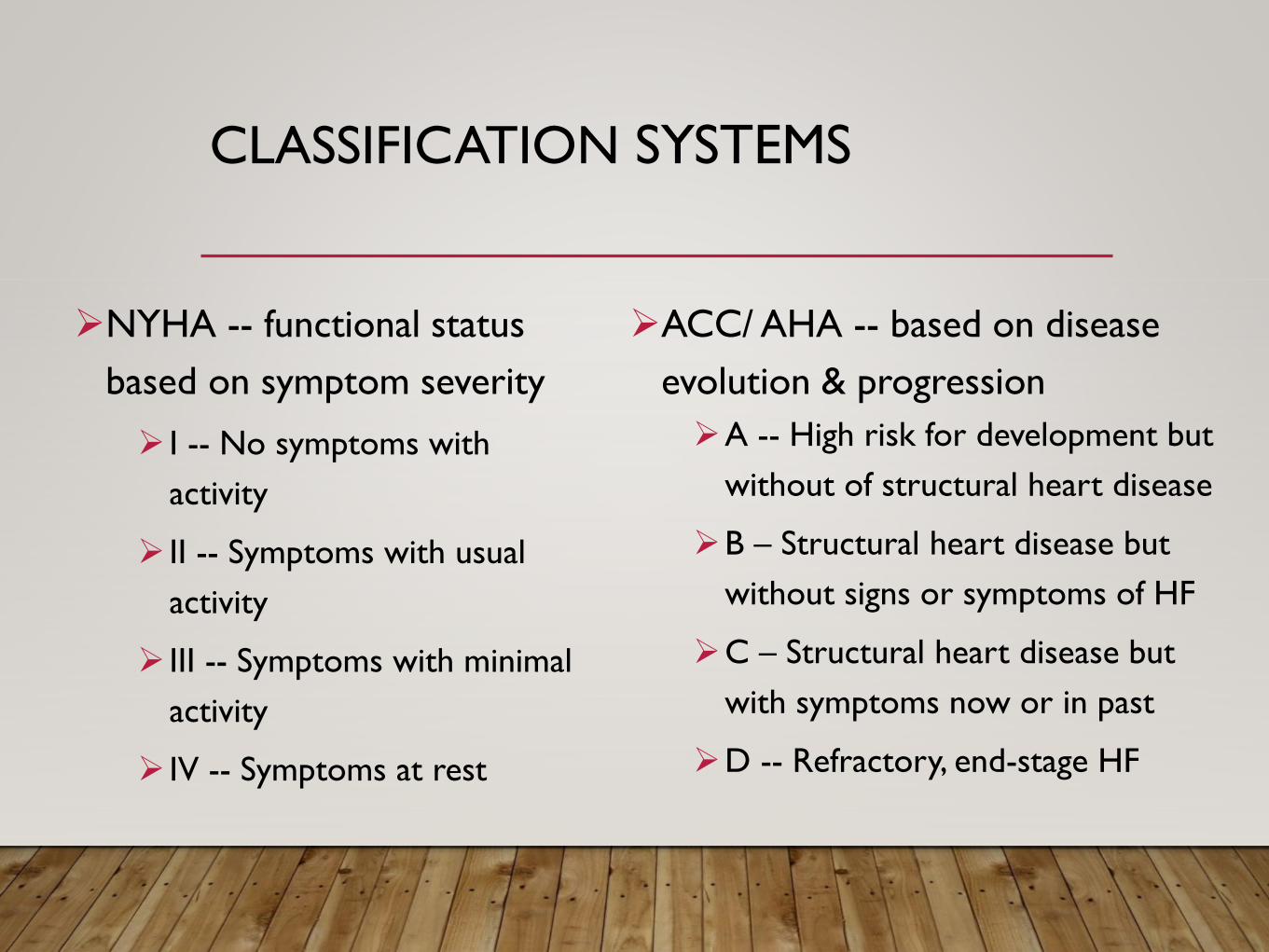
CLASSIFICATION SYSTEMS
➢ACC/ AHA -- based on disease
evolution & progression
➢A -- High risk for development but
without of structural heart disease
➢B – Structural heart disease but
without signs or symptoms of HF
➢C – Structural heart disease but
with symptoms now or in past
➢D -- Refractory, end-stage HF
➢NYHA -- functional status
based on symptom severity
➢ I -- No symptoms with
activity
➢ II -- Symptoms with usual
activity
➢ III -- Symptoms with minimal
activity
➢ IV -- Symptoms at rest
GOALS OF HF MANAGEMENT
➢Reduce morbidity/mortality rates
➢ Increase health-related quality of life measures and functional
status
➢Decrease health care associated costs
OBJECTIVES
➢Describe and differentiate the main diagnoses of heart failure
➢Describe the pharmacologic goals of heart failure treatment and
identify opportunities to optimize treatment
➢ Identify lifestyle changes to promote positive patient
outcomes in heart failure management
PATHOPHYSIOLOGY
➢Damage heart is unable to meet demands
➢Compensatory Mechanisms
➢The body’s response to decreased CO
➢ Intended to be short term response, detrimental in long term
➢Maintain circulatory homeostasis after acute reductions in blood
pressure or renal perfusion
➢Neurohormonal Model
➢Sympathetic nervous system (SNS)
➢Renin-Angiotensin-Aldosterone System (RAAS)
SNS
➢Causes tachycardia
➢Tries to increase CO by increasing HR
➢Causes increase in oxygen demand
➢Eventually decreases filling time actually decreases SV
➢ Increases contractility
➢Tries to increase CO by increasing SV
➢Causes increase in oxygen demand
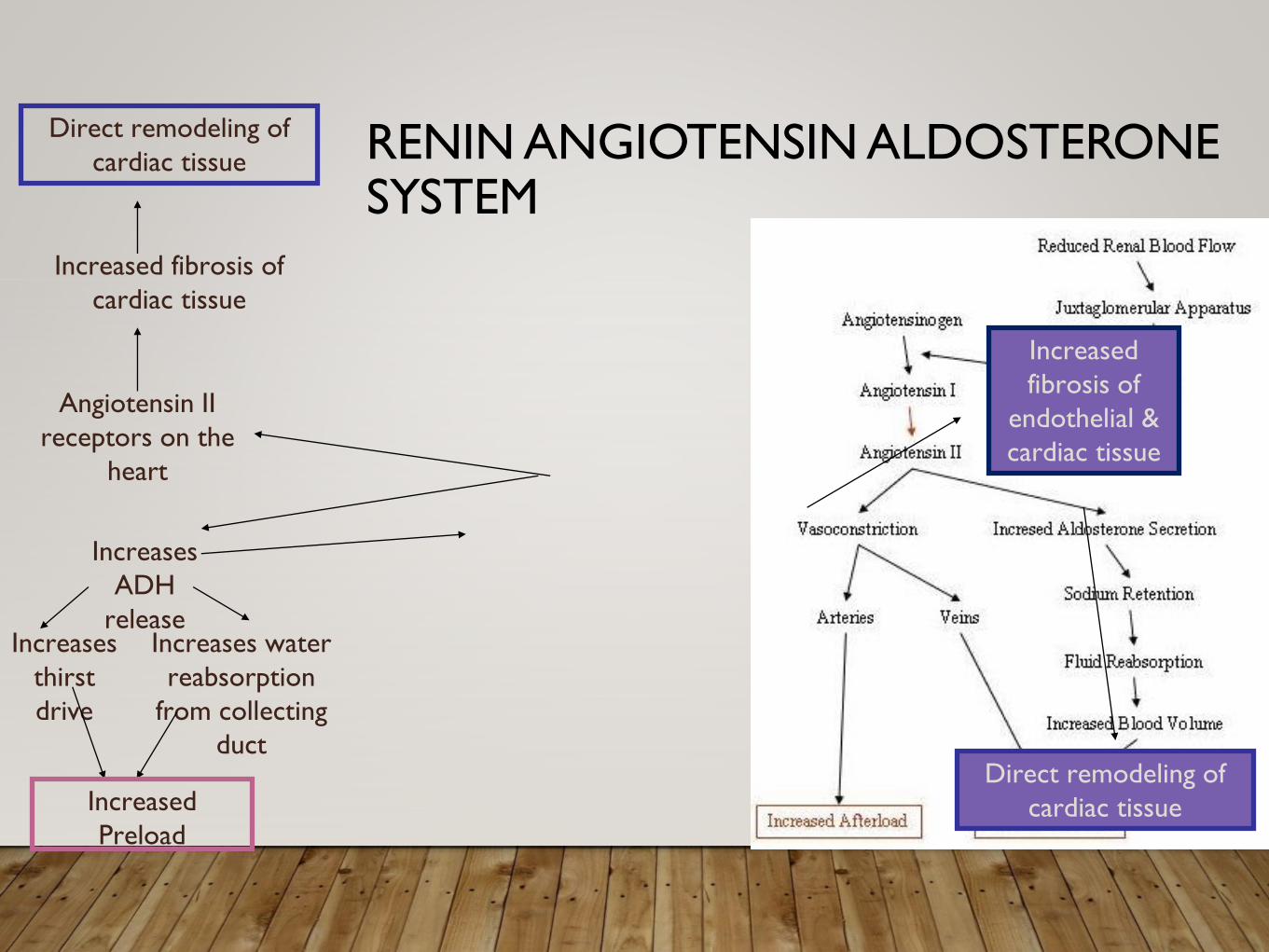
RENIN ANGIOTENSIN ALDOSTERONE SYSTEM
Angiotensin II
receptors on the
heart
Increased fibrosis of
cardiac tissue
Direct remodeling of
cardiac tissue
Increases water
reabsorption
from collecting
duct
Increases
ADH
releaseIncreases
thirst
drive
Increased
Preload
Increased
fibrosis of
endothelial &
cardiac tissue
Direct remodeling of
cardiac tissue
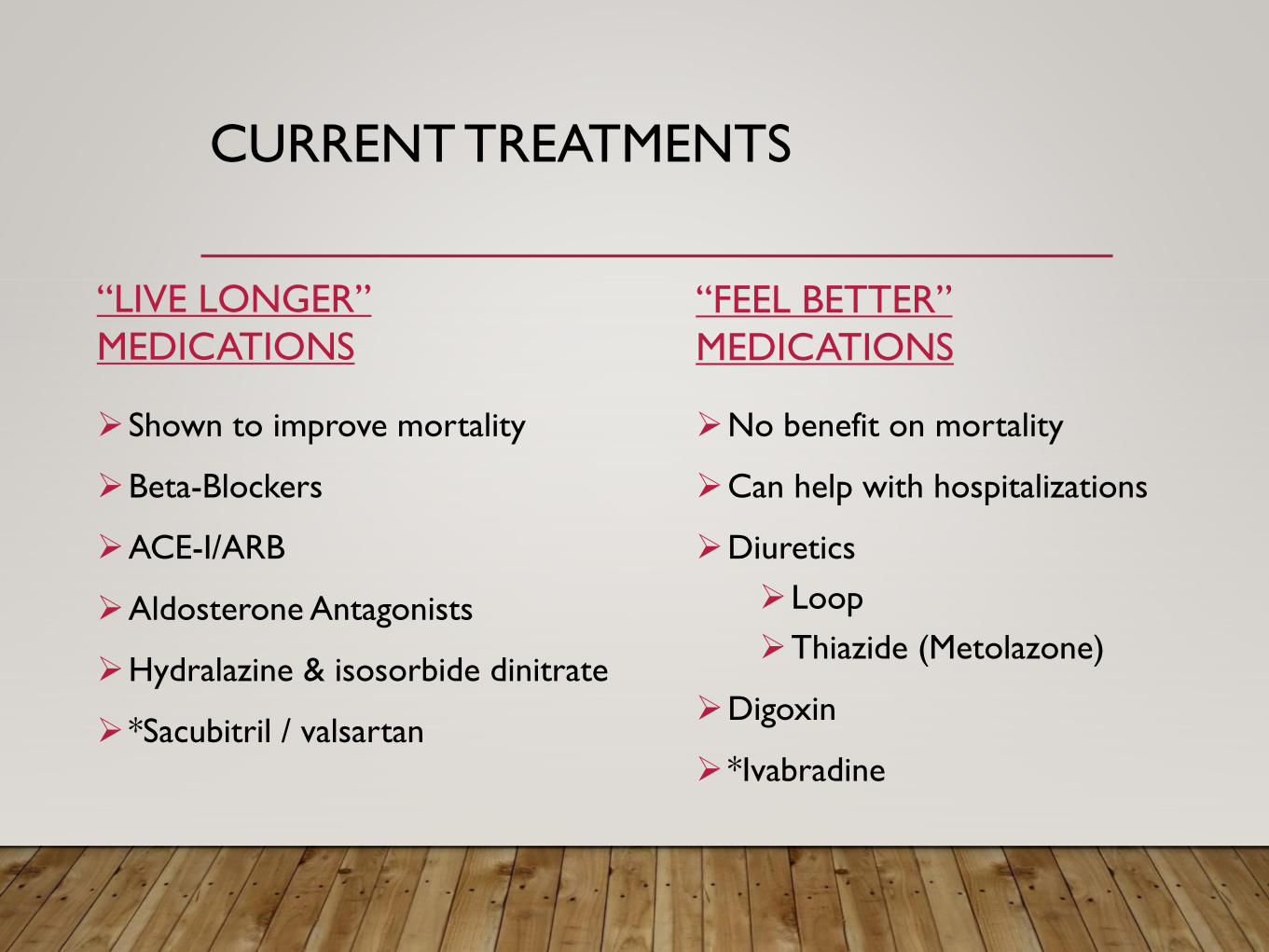
CURRENT TREATMENTS
“LIVE LONGER”
MEDICATIONS
➢Shown to improve mortality
➢Beta-Blockers
➢ACE-I/ARB
➢Aldosterone Antagonists
➢Hydralazine & isosorbide dinitrate
➢*Sacubitril / valsartan
“FEEL BETTER”
MEDICATIONS
➢No benefit on mortality
➢Can help with hospitalizations
➢Diuretics
➢Loop
➢Thiazide (Metolazone)
➢Digoxin
➢*Ivabradine
BETA BLOCKERS
➢Recommended in stage B HFrEF and beyond, even if
asymptomatic
➢ Can increase EF, especially if due to ischemic causes
➢ if compelling need for HR control (reduction of
symptoms)
➢Carvedilol, metoprolol SUCCINATE, bisoprolol only
➢ not a “class effect” for all beta blockers
BETA BLOCKERS
➢ Initiate therapy at low dose and advance, generally by
doubling Q2-4 weeks, to predefined target doses
➢Monitor closely for changes in vitals and symptoms (HF
worsening, fatigue, bradycardia, hypotension)
➢PEARL—metoprolol succ. for hypotensive pts and/or
concomitant respiratory disease
➢PEARL—carvedilol for hypertensive and/or DM
ACE INHIBITORS/ARBS
➢Recommended in all stages and diagnoses of HF, unless
contraindicated (angioedema, bilateral RAS, hyperkalemia)
➢ACEIs generally considered over ARBs, unless
➢ development of kinin related cough (approx 10-20%)
➢ already on ARB therapy
➢Data suggest class effect for ACEI, possible class effect for
ARB
ACE INHIBITORS/ARBS
➢Check renal function and electrolytes in 1-2 weeks after
initiation, periodically thereafter
➢ Initiate therapy at low dose and advance, generally by
doubling, to predefined target doses
➢ If target doses not tolerated, intermediate dosing acceptable
➢PEARL—losartan is the only antihypertensive capable of
reducing uric acid levels (0.5-1.0mg/dl), so………
ALDOSTERONE ANTAGONISTS
➢Recommend in NYHA II-IV or AHA Stage C (stage B?)
➢EF<35%
➢After β blockers, and ACE-I titrated to max dose
➢Of note, class II pts need CV hospitalization or high BNP
➢After acute MI with EF<40%
➢Useful in pts needing additional antihypertensive agents
ALDOSTERONE ANTAGONISTS
➢Spironolactone initial dose 12.5-25mg daily, target 25mg daily
➢Eplerenone initial dose 25mg daily, target 50mg daily
➢More selective, better tolerated
➢Do not start if SCr > 2.5 in men, >2.0 in women, or GFR <
30, or if potassium is greater than 5.0 mEq/L
➢Recheck potassium and renal function 2-3 days after start,
again at 7 days, and again with dose changes (including ACEI
or ARB)
HYDRALAZINE/ISDN
➢Recommended for pts of African descent with symptomatic
HFrEF (NYHA III-IV or AHA Stage C)
➢ADD ON therapy for patients already on optimal
ACEI/ARB and B blocker
➢Recommended in pts of any race with current or prior
symptomatic HFrEF that cannot be given ACEI or ARB
therapy
➢DO NOT substitute hydralazine/ISDN for ACEI or ARB
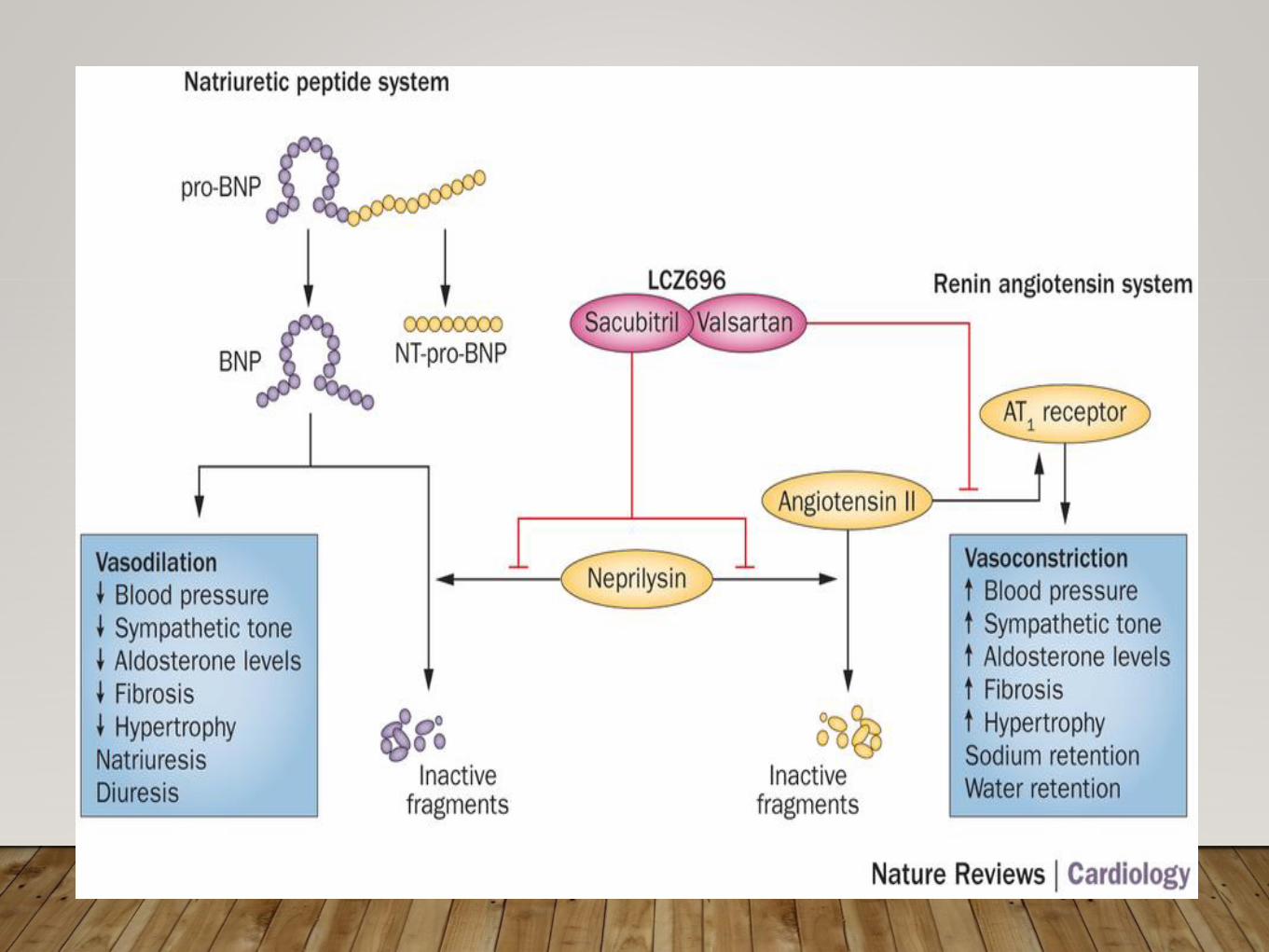
SACUBITRIL / VALSARTAN (ENTRESTO)
➢Newest Class of Medications for HF treatment
➢Angiotensin Receptor-Neprilysin Inhibitor (ARNI) combination
➢Approved for treatment of HFrEF, currently being studied in HFpEF
➢*2016 and 2017 Update: “In patients with chronic symptomatic HFrEF
NYHA class II or III who tolerate an ACE-I or ARB, replacement with an
ARNI is recommended to further reduce morbidity and mortality.” (Used in
place of ACEI or ARB)
➢Target Dose is 97mg/103mg BID
➢ Initial 24mg/26mg BID in ACEI/ARB naïve
➢49mg/51mg BID previously on ACEI/ARB
ADDITIONAL INFO
➢Precautions/
Contraindications
➢Angioedema
➢Contraindicated
with those with
history
➢Hypotension
➢Drugs that increase
potassium
➢Adverse Effects
➢Hypotension
➢Hyperkalemia
➢Cough
➢Dizziness
➢Renal failure
➢Angioedema

LOOP DIURETICS
➢Furosemide, bumetanide and torsemide
➢Bumetanide and torsemide better availability and BP effects
➢Reduce symptoms and hospitalizations, but not mortality
➢Recognized as a “threshold” medication (think of QD vs BID)
➢Risks-hypotension, fluid depletion, azotemia, hypokalemia,
hypomagnesemia, arrhythmia
LOOP DIURETICS
➢Hypotensive effects predominant during threshold phase, less
afterwards
➢Can be used even with GFR < 15ml/min
➢Can potentiate gout through serum concentration effects
➢Long-term use can potentiate diuretic resistance with need
to increase dose or add thiazide
THIAZIDE-LIKE DIURETIC
➢Metolazone acts distal tubule in addition to mild effects in
proximal tubule
➢VERY potent diuresis in combination with loop
➢Retains benefits even with GFR < 30ml/min
➢CAUTION—C-SO2-NH2
➢PEARL—delayed onset, delayed persistence
THIAZIDE DIURETICS
➢Hydrochlorothiazide and Chlorthalidone
➢Effects in the distal tubule (after loop)
➢Greater blood pressure effects and longer persistence than
loop diuretics
➢Remove more sodium from system than loops
➢Beneficial in hypertensive patients with mild fluid retention
➢Can potentiate gout by blocking uric acid excretion
DIURETIC SUMMARY
➢Factors to consider for diuretic therapy
➢ Blood pressure
➢ Volume status-degree of challenge, fluid overload vs fluid
depletion
➢ Electrolyte balance-chem panel 3-5 days after starting or
changing therapy
➢ Response and compliance to therapy
➢ Gout, allergies, lifestyle, adherence, morbidity/mortality
DIGITALIS
➢May be added to HFrEF patients with persistent symptoms
despite optimized GDMT
➢Digoxin + B blocker = better control of ventricular response,
esp during exercise
➢Goal serum levels of 0.5-0.9ng/ml
➢Multiple drug interaction and toxicity concerns
➢ If (Funny) Channel Inhibitor in SA node
➢Consider in those who have a high HR despite optimal treatment
➢ Reduce the risk of hospitalization in chronic HF with the following
characteristics:
➢ Stable, symptomatic heart failure
➢ LVEF <35%
➢ Sinus rhythm with resting HR >70 bpm
➢On maximum tolerated doses of BB or contraindication to BB
therapy
➢ Initial dosing 5mg BID, target dose 10mg BID
IVABRADINE (CORLANOR)
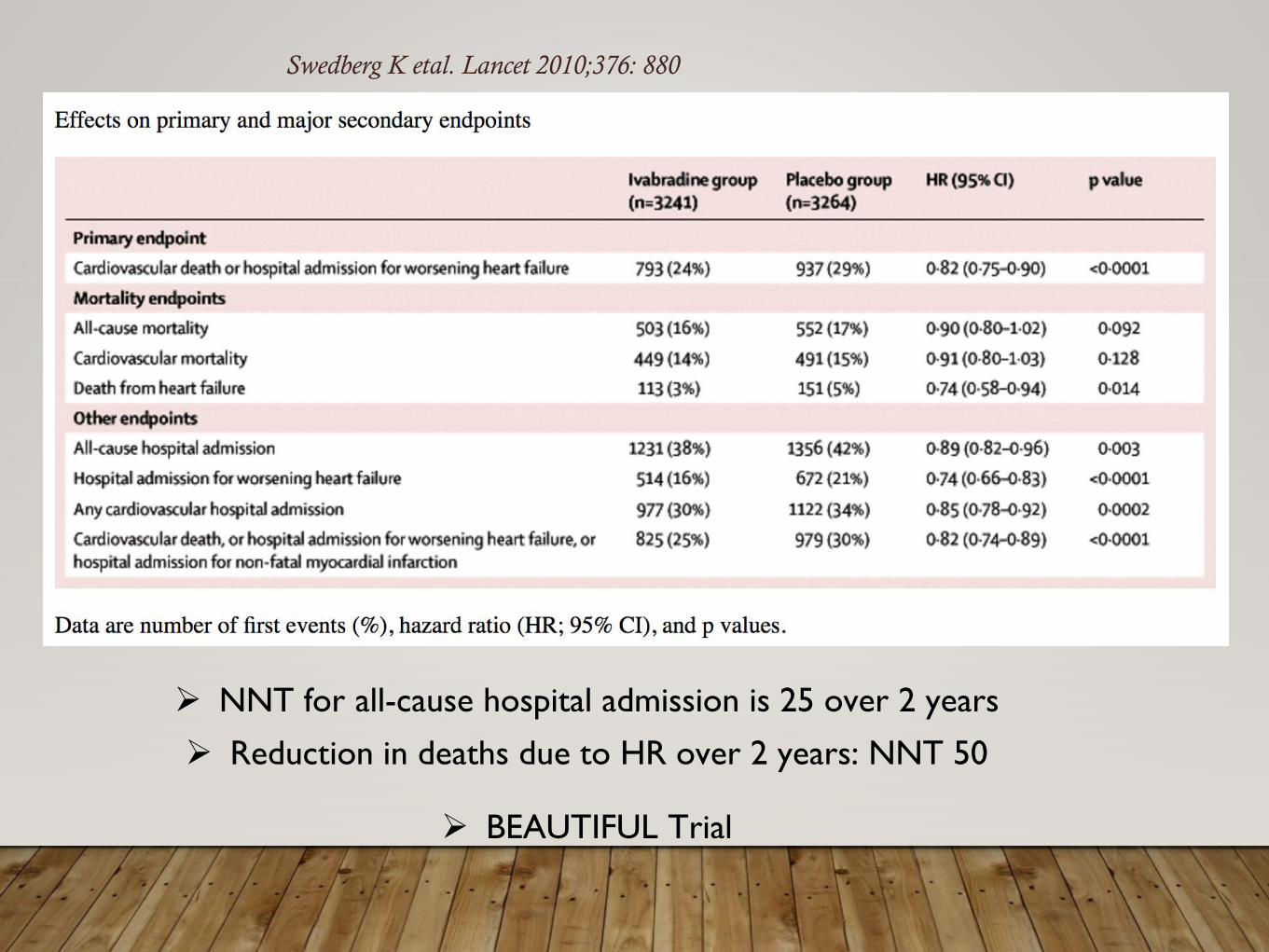
➢ NNT for all-cause hospital admission is 25 over 2 years
➢ Reduction in deaths due to HR over 2 years: NNT 50
➢ BEAUTIFUL Trial
Swedberg K etal. Lancet 2010;376: 880
➢Adverse Effects
➢Bradycardia
➢Atrial fibrillation (d/c in this instance)
➢Phosphenes (visual brightness)
➢Monitoring
➢BP, HR and rhythm
➢Dizziness/fatigue
➢Cost—approx. $375/month
ADDITIONAL INFO
OBJECTIVES
➢Describe and differentiate the main diagnoses of heart failure
➢Describe the pharmacologic goals of heart failure treatment
and identify opportunities to optimize treatment
➢ Identify lifestyle changes to promote positive patient outcomes in
heart failure management
MEDICATIONS TO AVOID
➢Antiarrythmics (except amiodarone and dofetilide)
➢Calcium channel blockers (except amlodipine)
➢NSAIDS
➢Thiazolidinediones
➢Nutritional supplements (except Omega 3s) and hormonal
supplements unless to replace true deficiency
LIFESTYLE MODIFICATIONS
➢Dietary sodium considerations
➢Self-assessment and management
➢Obesity management
➢Exercise
➢End of life considerations
DIETARY SODIUM RECOMMENDATIONS
➢Stage A and B HF—take salt shaker off the table, avoid adding
extra to cooking
➢Stage C and D HF—excessively low and high sodium intake
associated with worse outcomes, restrict <3gm sodium daily
➢Sodium intake generally > 4gm/day in general population
➢Salt substitutes may contain potassium!!
DAILY SELF-ASSESSMENT AND SELF-MANAGEMENT
➢Monitoring of blood pressure at home
➢ direct comparison of personal and clinic readings
➢Daily weight assessment and planning
➢ morning weight and charting
➢ finding “dry” or goal weight
➢ pre-determined strategies for out-of-range
OBESITY MANAGEMENT ??
➢Obesity considered BMI > 30
➢HF-lowest mortality and hospitalization rates seen in BMI 30
- 35
➢Highest mortality— cardiac cachexia > morbidly obese >
normal > overweight > obese —lowest
➢Consider appropriate weight loss if indicated
EXERCISE
➢Exercise training (or regular physical activity) is
recommended as safe and effective for HF patients able to
participate
➢ Regular walking is considered gold standard
➢Cardiac rehabilitation
➢ can increase HRQOL, functional capacity, exercise
duration and morbidity
END OF LIFE PLANNING
➢My take—medical treatments and guidelines focus on battling
mortality to the end, but fail to address acceptance of
mortality and finding peace in dying with dignity.
➢Have “the talk” with patients and family
➢Plan for advanced directives, DNR/DNI, final resting place,
estate planning, etc.
➢Five Wishes Document (excellent resource!!)
QUESTION 1
HF with Reduced Ejection Fraction (HFrEF)is now used to
describe what type of HF?
A. Systolic Heart Failure
B. Diastolic Heart Failure
C. Right-sided Heart Failure
D. Broken-heart syndrome (Tatsukobu’s)
E. No idea………
QUESTION 1
HF with Reduced Ejection Fraction (HFrEF)is now used to
describe what type of HF?
A. Systolic Heart Failure
B. Diastolic Heart Failure
C. Right-sided Heart Failure
D. Broken-heart syndrome (Tatsukobu’s)
E. No idea………
QUESTION 2
Which of the following medications has NOT been shown to
decrease mortality in HFrEF?
A. Carvedilol
B. Spironolactone
C. Furosemide
D. Lisinopril
QUESTION 2
Which of the following medications has NOT been shown to
decrease mortality in HFrEF?
A. Carvedilol
B. Spironolactone
C. Furosemide
D. Lisinopril
QUESTION 3
What home-monitoring technique is best to determine the
efficacy of a diuretic regimen?
A. Skin pinch technique
B. Seeing how your pants fit
C. Asking a friend if you look “puffy”
D. Daily home weights
QUESTION 3
What home-monitoring technique is best to determine the
efficacy of a diuretic regimen?
A. Skin pinch technique
B. Seeing how your pants fit
C. Asking a friend if you look “puffy”
D. Daily home weights
RECOGNITION OF PEERS
➢Dr. Tracy K. Pettinger, Clinical Associate Professor, Idaho State
University
➢Thank you for allowing me to use content from your
2017 presentation at Northwest Pharmacy Conference!!
➢Dr Timothy Murray, CAPT USPHS, BCPS-AQ Cardiology
➢Thank you for years of mentorship and collaboration on
our patients in the Indian Health Service!!
REFERENCES
➢ 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for
the Management of Heart Failure. Available at:
http://circ.ahajournals.org/content/early/2017/04/26/CIR.0000000000000509
➢ 2016 ACC/AHA/HFSA Focused Update on Pharmacological Therapy for Heart
Failure: An Update of the 2013 ACCF/AHA 2013 Guidelines for the
Management of Heart Failure. Available at
http://circ.ahajournals.org/content/circulationaha/early/2016/05/18/CIR.0000000
000000435.full.pdf
➢ACC/AHA Guidelines for the evaluation and management of heart failure. A
report of the American College of Cardiology Foundation/American Heart
Association Task Force on Practice Guidelines. Am J Cardiol. 2013 May 19.
Available at: http://circ.ahajournals.org/content/128/16/e240
REFERENCES CONTINUED
➢ McMurray JJ, et al. Angiotension-neprilysin inhibitor versus enalapril in
heart failure. N Engl J Med 2014; 371:993-1004.
➢ Swedberg K, et al. Ivabradine and outcomes in chronic heart failure
(SHIFT): a randomised placebo-controlled study. Lancet 2010; 376: 875-
85.
➢ Fox, K et al. Ivabradine for patients with stable coronary artery diesase
and left-ventricular systolic dysfunction (BEAUTIFUL): a randomised,
double-blind, placebo-controlled trial. Lancet 2008; 372: 807-16
➢ Klein L, O’Connor CM, Gattis WA, et al. Pharmacologic therapy for
patients with chronic heart failure and reduced systolic function:
Review of trials and practical considerations. Am J Cardiol 2003; 91:18F-
40F.
QUESTIONS??
CAPT Dean T. Goroski
Pharmacy Supervisor
Crow/N. Cheyenne Hospital
Crow Agency, MT
406-638-3578