heavy menstrual bleeding nice guidelines, aboubakr elnashar
TRANSCRIPT

Heavy menstrual
bleeding
NICE Guidelines
Prof Aboubakr Elnashar Benha university, Egypt
Email: [email protected]

•HMB Excessive MBL which interferes with the woman’s
physical, emotional, social & material quality of life,
and which can occur alone or in combination with
other symptoms.
Any interventions should aim to improve quality of
life.

History 1. Nature of the bleeding
2. Related symptoms that might suggest structural or
histological abnormality
3. Impact on quality of life
4. Other factors that may determine treatment
options (such as presence of comorbidity).

•If the history suggests HMB without structural or
histological abnormality:
pharmaceutical treatment can be started without
carrying out a physical examination or other
investigations, unless the treatment chosen is LNG-IUS. •If the history suggests HMB with structural or
histological abnormality (intermenstrual or
postcoital bleeding, pelvic pain and/or pressure
symptoms):
Physical examination and/or other investigations
(US) should be performed.

•Measuring MBL either directly (alkaline haematin)
or indirectly (Pictorial blood loss assessment chart)
is not routinely recommended.
{Whether MBL is a problem should be determined
not by MBL but by the woman herself}.

Pictorial blood loss chart: (Higham,1990)
Days of the bleeding Score
1 2 3 4 5 6 7 8
Towel
1 ponit
5 ponits
10 points
Clots 1p clot 1 point
5p clot 5 points
Flooding 5 points
Score >100 = Menorrrhagia

Examination •Indications: Before
1. LNG-IUS fittings
2. Investigations for structural abnormalities
3. Investigations for histological abnormalities.

Laboratory tests •A full blood count test should be carried out
•Testing for coagulation disorders (von Willebrand’s
disease) should be considered
1. HMB since menarche
2. Personal or family history suggesting a
coagulation disorder.
•A serum ferritin test should not routinely be carried
out
•Hormone testing should not be carried out
•Thyroid testing should be carried out only when
other S&S of thyroid disease are present.

Structural and histological investigations •Biopsy {exclude endometrial cancer or atypical
hyperplasia}.
Indications:
1. Persistent intermenstrual bleeding
2. Age 45 & over
3. Failure or ineffective treatment.
Advantages:
1. An outpatient procedure
2. No general anesthesia.
3. Complications are rare
An adequate & acceptable screening procedure

Types
Reusable:
Vabra aspirator (95%)
Sharman curette,
Novak curette (90%),
Kevorkian
Randall
Disposable
Pipelle curette (90%)
Accurette
Z-sampler (83%),
Mi-Mark Helix (93%),
Endopap (70%),
Perma curette (73%)
Endorette
Explora (70%)
Karman (95%)
Ti-Utrap
Gynocheck

Pipelle:
Is tolerated better than most other forms
Samples 4.2% of the endometrial surface
Detection rate of endometrial cancer: 90%
Vabra aspiration: Only samples 42% of the endometrial surface Less tolerated than other forms Compared with curretage, complications are less & the detection rate of endometrial abnormalitis are higher (Grimes,1982)

Novak curette
Kevorkian curette

Endocurette Pipelle

•US is the first-line diagnostic tool for identifying
structural abnormalities.
•US should be undertaken when:
1. The uterus is palpable abdominally.
2. Vaginal exam: a pelvic mass of uncertain origin.
3. Pharmaceutical treatment fails.

•Hysteroscopy should be used as a diagnostic tool
only when US results are inconclusive (for example,
to determine the exact location of a fibroid or the
exact nature of the abnormality).
•Saline infusion sonography should not be used as a
first-line diagnostic tool.
•MRI should not be used as a first-line diagnostic
tool.
•Dilatation & curettage alone should not be used as a
diagnostic tool.



Pharmaceutical treatments •Indications:
1. No structural or histological abnormality
2. Fibroids
< 3 cm
no distortion of the uterine cavity.
•Determine she wish to conceive or not

•Treatments should be considered in the following order:
a) LNG-IUS provided long-term (at least 12 ms) use
is anticipated
b) Tranexamic acid (3-6 gm/d for the first 3 days of
the cycle)
or NSAIDs (Mefenamic acid 500 mg tds during
menses).
or COCs
c) Norethisterone (15 mg daily, D5-26 of the cycle)
or injected long-acting progestogens

Mirena
•When HMB coexists with dysmenorrhoea, NSAIDs
should be preferred to tranexamic acid.
•Ongoing use of NSAIDs and/or tranexamic acid is
recommended for as long as it is found to be
beneficial by the woman.
•Use of NSAIDs and/or tranexamic acid should be
stopped if it does not improve symptoms within 3
menstrual cycles.
•When a first pharmaceutical treatment has proved
ineffective, a second pharmaceutical treatment can
be considered rather than immediate referral to
surgery.

•GnRHa: could be considered
1. Prior to surgery or
2. When all other treatment options for fibroids,
including surgery or UAE, are contraindicated.
If this treatment is to be used for >6 ms or if
adverse effects are experienced then HRT‘add-
back’ therapy is recommended.
•Danazol should not be used routinely (200 mg/d)
•Oral progestogens given during the luteal phase
only should not be used.
•Etamsylate should not be used.

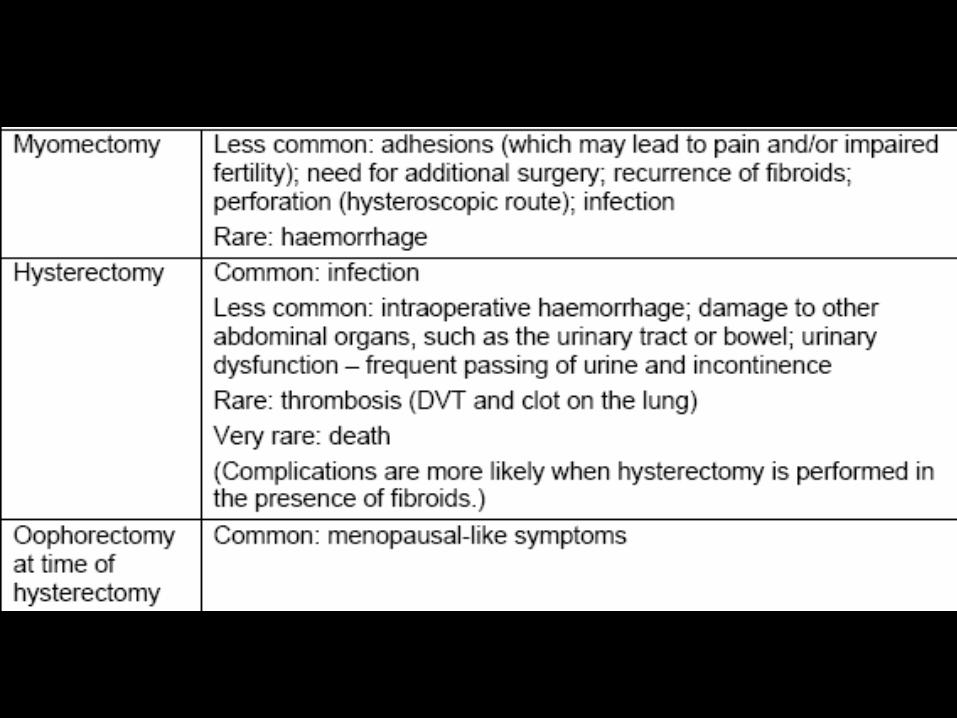
Side effects


Non-hysterectomy surgery Endometrial ablation
Indicated:
Bleeding having a severe impact on a woman’s
quality of life, and she does not want to conceive in
the future.
Types:
Balloon thermal endometrial ablation
Microwave endometrial ablation,
Free fluid endometrial ablation
Impedance-controlled bipolar radiofrequency
ablation
Endometrial cryotherapy is not covered by this
guideline.


•Endometrial ablation
Indications:
1. Initial treatment after full discussion with
the woman of the risks & benefits and of
other treatment options.
2. Small uterine fibroids (<3 cm).
3. Uterus no bigger than a 10-week
pregnancy, endometrial ablation should
be considered preferable to hysterectomy.
Advise after endometrial ablation
Avoid subsequent pregnancy and use
effective contraception, if required

•Second-generation ablation techniques should be
used where no structural or histological abnormality
is present.
•The second-generation techniques:
• Impedance-controlled bipolar radiofrequency
ablation
• Fluid-filled thermal balloon endometrial ablation
(TBEA)
• Microwave endometrial ablation (MEA)
• Free fluid thermal endometrial ablation
•In TBEA, endometrial thinning is not needed.
•In MEA, scheduling of surgery for postmenstrual
phase is an alternative to endometrial thinning.

First-generation ablation techniques
Rollerball endometrial ablation [REA] Transcervical
resection of the endometrium [TCRE])
are appropriate if hysteroscopic myomectomy is to
be included in the procedure.
Dilatation and curettage
should not be used as a therapeutic treatment.

Treatment of large fibroids (>3cm): • With significant symptoms (dysmenorrhoea or
pressure symptoms): surgery or UAE as first-line
treatment.
•UAE, myomectomy or hysterectomy: bleeding
having a severe impact on quality of life.
•Women should be informed that UAE or
myomectomy may potentially allow them to retain
their fertility.
•Myomectomy: Woman wants to retain their uterus.

•UAE: Woman wants to retain their uterus and/or
avoid surgery.
•Prior to scheduling of UAE or myomectomy, the
uterus & fibroid(s) should be assessed by US. If
further information about fibroid position, size,
number and vascularity is required, MRI should be
considered.
•Pretreatment before hysterectomy and
myomectomy with GnRha for 3 to 4 ms should be
considered where uterine fibroids are causing an
enlarged or distorted uterus.
•If a woman is being treated with GnRha & UAE is
then planned, GnRHa should be stopped as soon
as UAE has been scheduled.

Hysterectomy •Should not be used as a first-line treatment solely
for HMB.
Indications:
1. Other treatment options have failed,
contraindicated or declined by the woman
2. There is a wish for amenorrhoea
3. Woman (who has been fully informed) requests it
4. Woman no longer wishes to retain her uterus and
fertility.

•Discussion of the implication of hysterectomy:
1. Sexual feelings, fertility impact, bladder function,
need for further treatment, treatment complications,
the woman’s expectations, alternative surgery and
psychological impact.
2. Increased risk of serious complications (such as
intraoperative haemorrhage or damage to other
abdominal organs)
3. Risk of possible loss of ovarian function and its
consequences, even if their ovaries are retained
during hysterectomy.

•Route of hysterectomy. The following factors need
to be taken into account:
1. Other gynaecological conditions or disease
2. uterine size
3. presence and size of uterine fibroids
4. mobility and descent of the uterus
5. size and shape of the vagina
6. history of previous surgery.
•Taking into account the need for individual
assessment, the route of hysterectomy should be
considered in the following order: first line vaginal;
second line abdominal.

•Morbid obesity or the need for oophorectomy during
vaginal hysterectomy: laparoscopic approach should
be considered, and appropriate expertise sought.
•When abdominal hysterectomy is decided upon then
both the total method and subtotal method should be
discussed with the woman.
•Removal of healthy ovaries at the time of
hysterectomy should not be undertaken
•Removal of ovaries should only be undertaken with
the express wish and consent of the woman.
•Women with a significant family history of breast or
ovarian cancer should be referred for genetic
counselling prior to a decision about oophorectomy.

•In women under 45 considering hysterectomy for
HMB with other symptoms that may be related to
ovarian dysfunction (for example, premenstrual
syndrome), a trial of pharmaceutical ovarian
suppression for at least 3 months should be used as
a guide to the need for oophorectomy.
•If removal of ovaries is being considered, the
impact of this on the woman’s wellbeing and, for
example, the possible need for HRT should be
discussed.
•Women considering bilateral oophorectomy should
be informed about the impact of this treatment on
the risk of ovarian and breast cancer.

Investigate routine use of indirect measurements
of MBL in primary and secondary care
Evidence shows that direct measurement of MBL is
accurate but complex to undertake in clinical
practice, and that subjective assessment of MBL is
inaccurate but easy to undertake in clinical practice.
An alternative is the use of indirect measures of
MBL, such as the ‘Pictorial blood loss assessment
chart’. However, evidence on the use of indirect
measures is contradictory & no data are available to
show whether they could be used in routine practice.
If indirect measures are shown to work then they
could be introduced as a simple technique for
assessing MBL, and from this the management of
HMB could be improved.

What are the long-term recurrence rates of
fibroids after UAE or myomectomy?
Both UAE and myomectomy are undertaken to
reduce symptoms associated with uterine fibroids by
directly removing the fibroid(s) or reducing their size.
Data exist on short- and medium-term recurrence of
fibroids, but no data are available on long-term
recurrence.

What are the effects of hysterectomy and
oophorectomy on the occurrence of cancer?
Epidemiological studies are required to investigate
the impact of hysterectomy and oophorectomy on
cancer. The results of this research will have
fundamental implications on the use of these
treatments.




