helen whiteside mrpharms ip medicines optimisation pharmacist pharmacy lead for older people, care...
TRANSCRIPT
Helen Whiteside MRPharmS IP
Medicines Optimisation PharmacistPharmacy lead for older people,
care homes and dementia
PreviouslyClinical Care Home Pharmacist
Medicines Optimisation
in Care Homes
Learning and Practice
Development
Learning ObjectivesThis session will
1. Summarise the key elements of national guidance and standards
2. Summarise the guidance on optimising medicines use in older people with multimorbidities and polypharmacy
3. Describe the key aspects of the NHS Leeds West CHAMOIS model which optimises medicines for care home residents through a cost effective medication review service linked to the CCG strategic priority health goals in areas including cardiovascular, respiratory, diabetes, mental health and dementia
4. Describe some of the challenges with medicines safety in care homes for the elderly –a very vulnerable group of people.
5. Use case examples and data to illustrate how the service incorporates best available evidence to tackle some of these challenges and has been a driver of change in the local commissioning arrangements for care home residents
6. Share the learning and resources from the service to support similar initiatives
Paracelsus(1493-1541)
• “All substances are poisons;
there is none which is not a poison.
• The right dose differentiates a poison from a remedy.”
This is what medication guidance
in older people is all about…
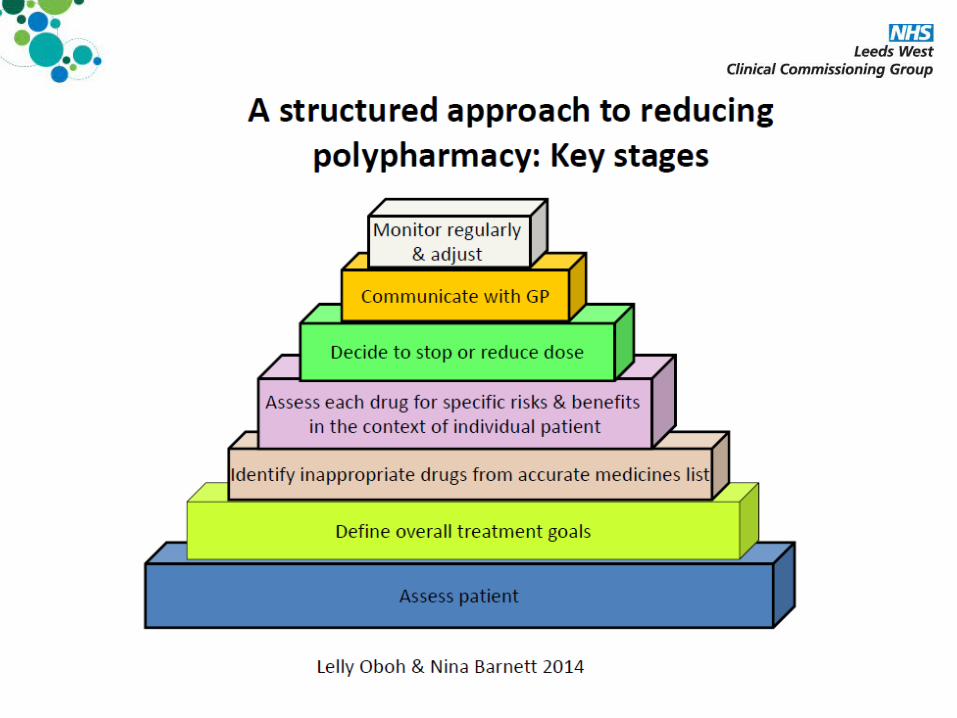
Polypharmacy in a nutshell
Polypharmacy –Is it appropriate or problematic?
• Appropriate Polypharmacy– Prescribing for an individual for
complex conditions or for multiple conditions in circumstances where medicines use has been optimised and where the medicines are prescribed according to best evidence.
• Problematic Polypharmacy– Prescribing of multiple medications
inappropriately, or where the intended benefit of the medication is not realised

Deprescribing Tools
Background
• August 2013• 2.4 WTE 8a pharmacists • Employed to carry out
medication reviews in older persons care homes
• By July 2014 – just 1.8
• By December 2014 – just 0.8
Our MO interventions focussed on…• Personalised and holistic reviews
• CCG priority disease areas
• Specific high risk medicines
• Deprescribing of less beneficial medicines
• Appropriate monitoring

How we started
• CCG aim – invest to provide savings for medicines budget
• 3 pharmacists with 3 different backgrounds – rounded team
• List of care homes (>1 yr out of date!)• SOP and standard letters written• Checklist for care homes / practices• Introduction leaflet for practices/care
homes• Patient leaflet• No standard review template - PREVENT• Data collection tool created• Smartcards and ICE forms
Leeds West CCGStandard Operating Procedurefor Care Home Pharmacistsproviding a medication review serviceto care home residents
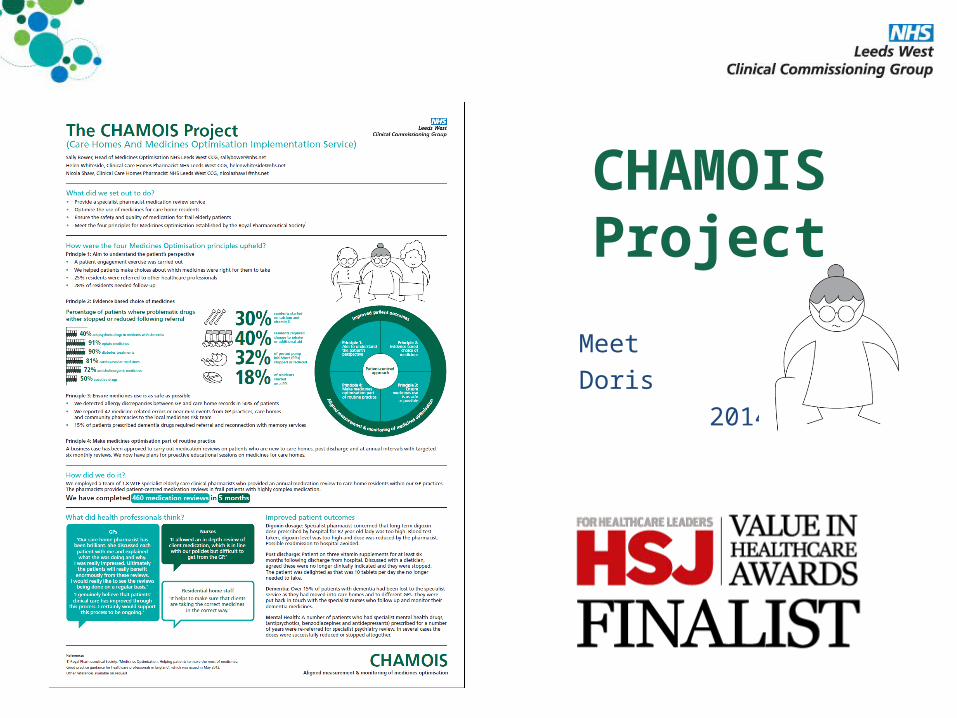
CHAMOIS Project
MeetDoris
2014

Show Doris video
10 mins
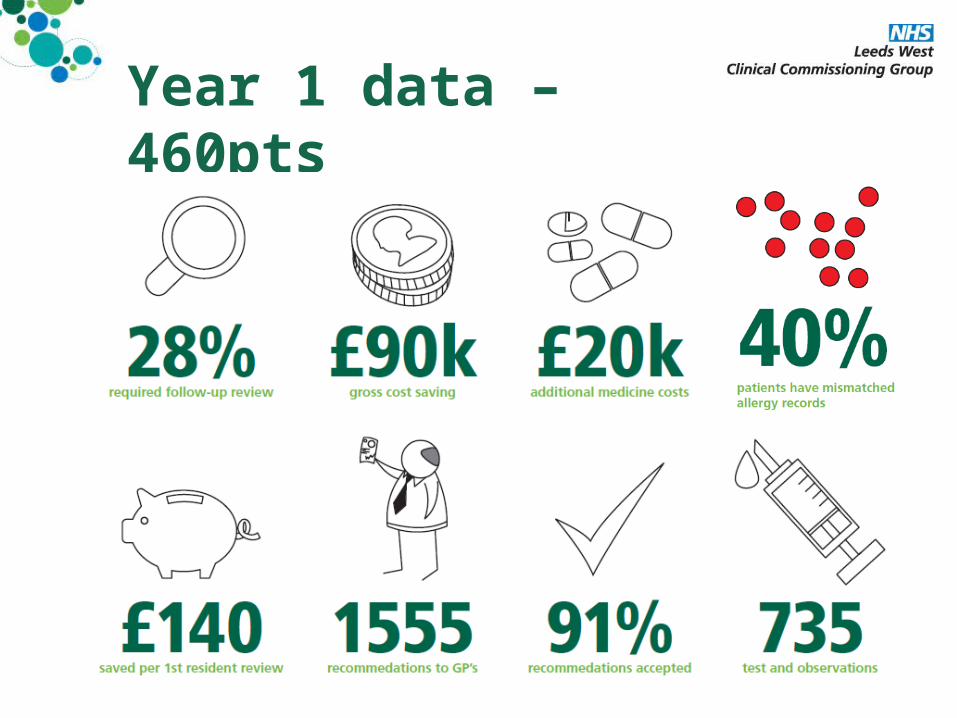
Year 1 data – 460pts
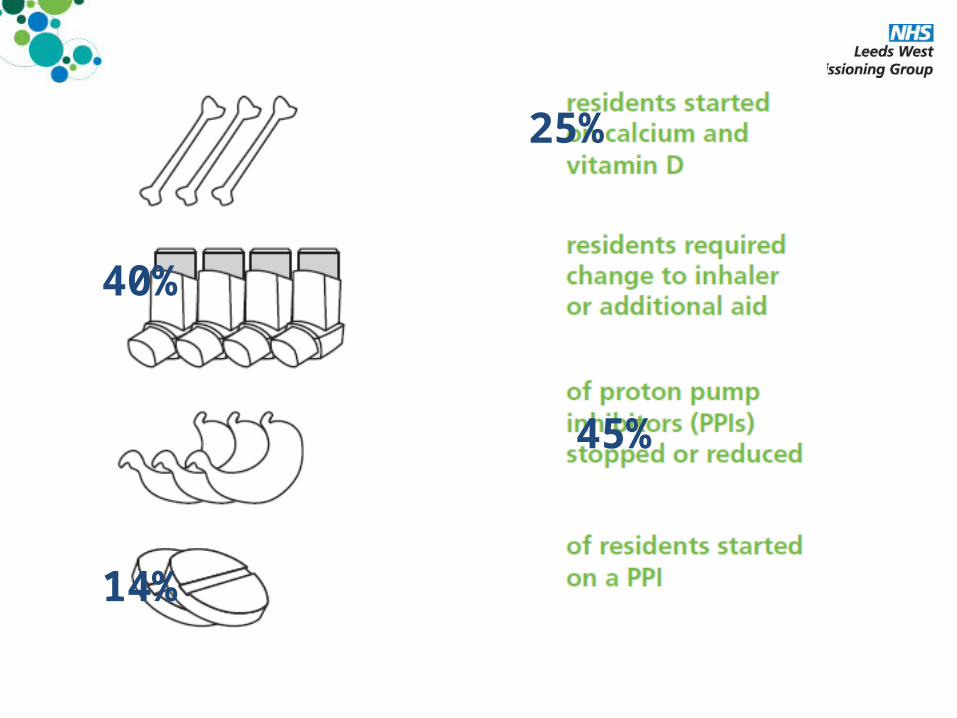
25%
40%
45%
14%

End of 2 year projectNo. of patients reviewed 680
No. of follow up reviews 435
Net cost saving £ 124,804
Saving per patient £ 184
No of medicine changes 3.75 per patient (2562)
No of tests required >2 per patient (1440)
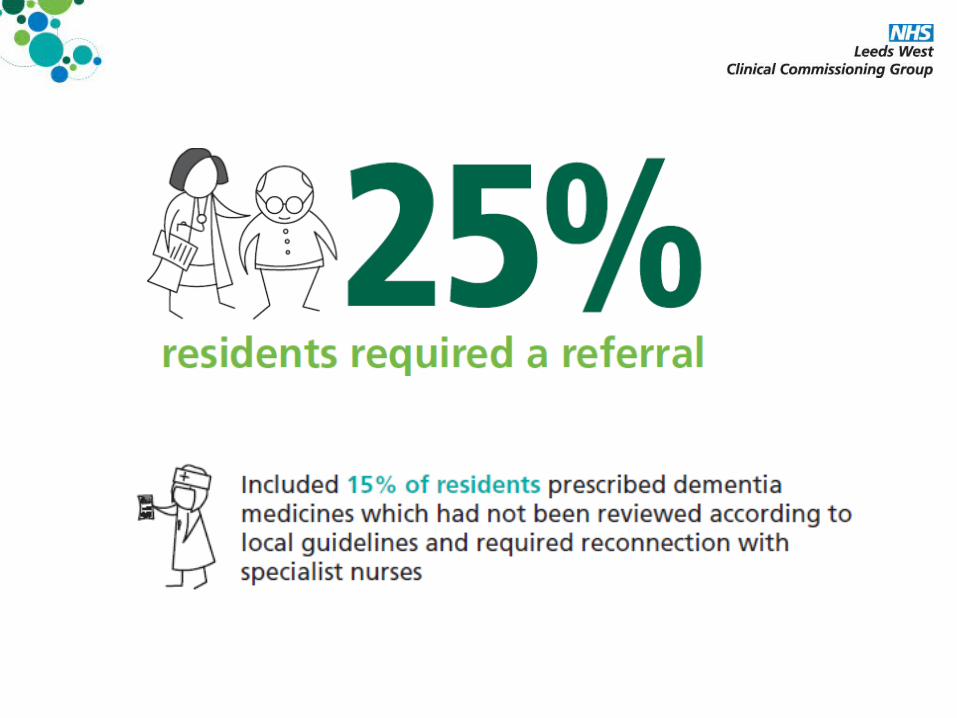
Referrals needed in 1 in 4 patients 27% (183)
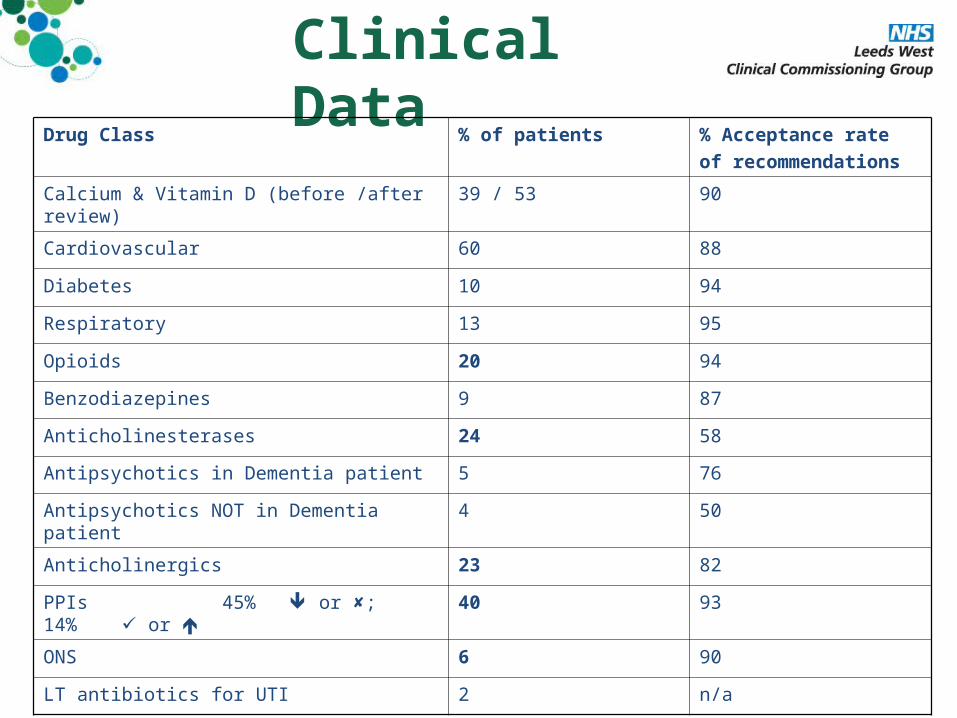
Clinical Data
Drug Class % of patients % Acceptance rate of recommendations
Calcium & Vitamin D (before /after review)
39 / 53 90
Cardiovascular 60 88
Diabetes 10 94
Respiratory 13 95
Opioids 20 94
Benzodiazepines 9 87
Anticholinesterases 24 58
Antipsychotics in Dementia patient 5 76
Antipsychotics NOT in Dementia patient 4 50
Anticholinergics 23 82
PPIs 45% or ; 14% or 40 93
ONS 6 90
LT antibiotics for UTI 2 n/a
What makes our day…
Thanks, you've been a great help to us!
I’ve enjoyed working with you and hope to be able to continue in the future
Just dropping you a line about my mum.
Since you came 3 months ago she has had no falls. This is the longest in two
years she has gone without a fall. Thank you
Now that you have stopped
Margaret's’ medicines she is
more alert, socialising in the lounge with other residents and has put on weight as her appetite has
improved.Thank you
The End Result…
Four permanent Band 8a Medicines Optimisation Pharmacists
Medication Reviews Polypharmacy/Care Homes
MOP Medication Reviews
New residents & post discharge LWCCG Integrated Care Home Scheme
Scenarios
• 15 mins then feedback
Scenarios Feedback
• 15 mins
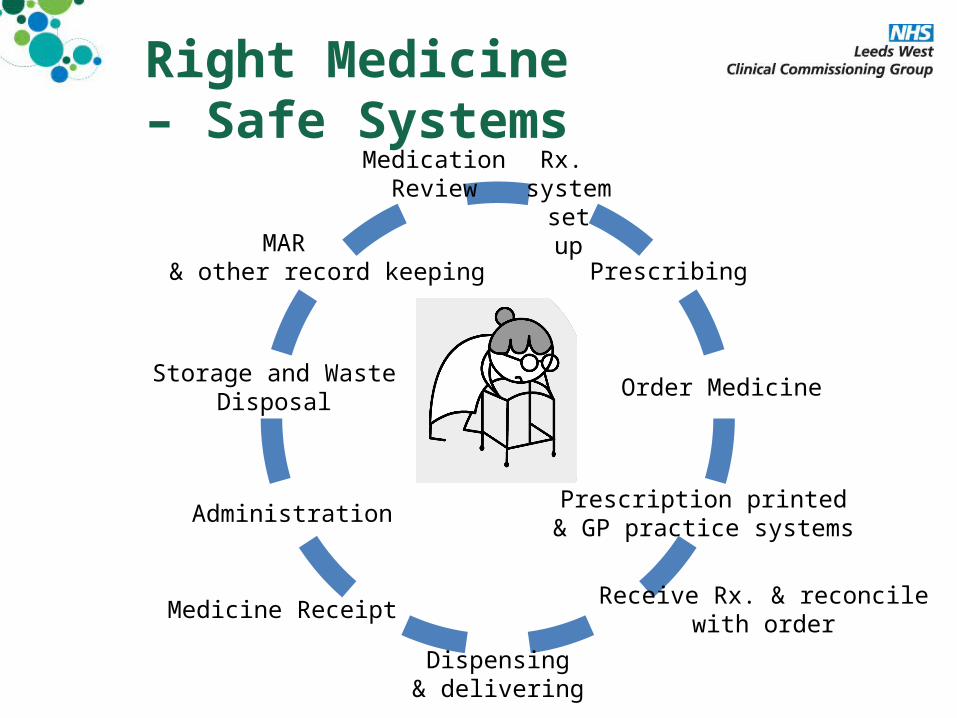
Right Medicine – Safe Systems
Rx. system
set up
Prescription printed& GP practice systems
MAR & other record keeping
Receive Rx. & reconcile with order
Dispensing& delivering
Administration
Storage and WasteDisposal
Medicine Receipt
MedicationReview
Order Medicine
Prescribing
NICE guidance and quality standards• Managing medicines in care
homes– Guidance– Quality Standard– Support for commissioning
• Local government briefing: Older people in care homes
Improved standards for LCC inspections
Implement
• ALL guidance/ standards • or• 1 at a TIME?
Commissioning- what should be in your contract?• Medicines listed on day of transfer
• Discharge summaries sent WITH person
• 1st Self administration
• Prescribing - – Safe repeat prescribing systems– Comprehensive instructions for ALL medicines
• Medication Reviews as part of MDT– At least annually
• Covert medicines– NOT until FORMAL best interests meeting has
been held with CH staff, Rxer and family/advocate
– Consider training
Standard- review checklist- review template or - data input?
or not?
Learning – 1

Learning 2 – know your baseline Rx data
• LWCCG = £180 per patient / year
• In long term annual reviews drops to
£100
• Long term business case
• NH vs. residential homes – impact on £
• Other influences to these residents care– Eating and drinking team– Admission avoidance scheme– Winter planning schemes– Care coordinators– Antipsychotic reviews / audits & care pathways
Learning 3Solving the problems –Connecting and working together
• Feedback to teams– Prescribing and GP practice issues– Issues with communications/ medicines supplies
from mental health teams, community and acute provider pharmacy departments
– DATIX incidents and medicines safety team /LCC
• Connecting to other clinical leads / commissioners– CCG Diabetes /Long term conditions– CCG Quality managers/ LA Contract managers– CCG QI leads– CCG Primary care team – practice intelligence
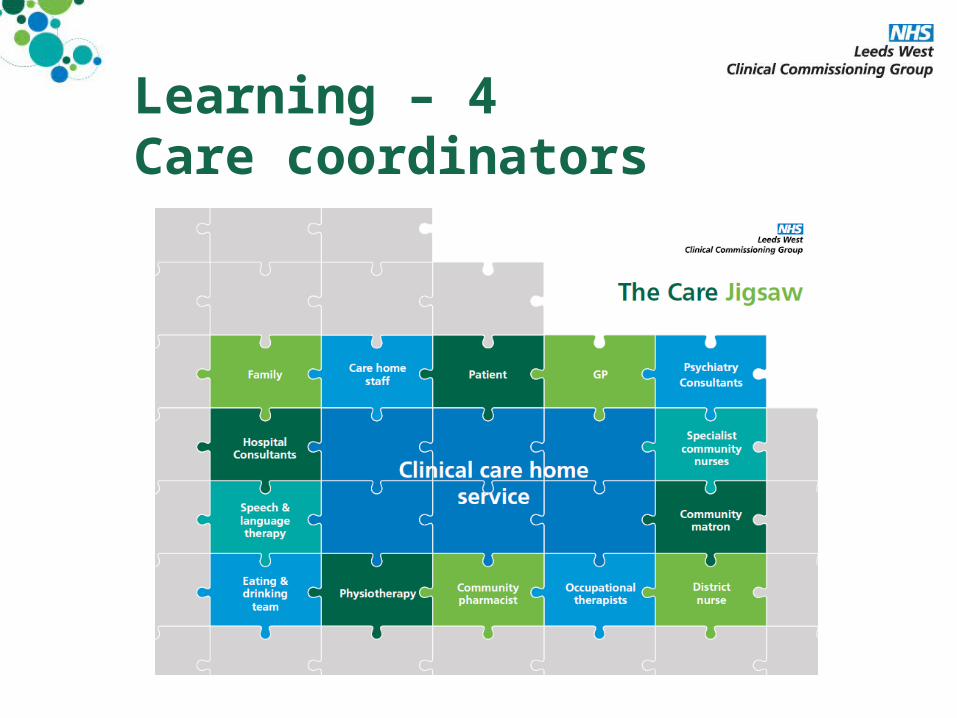
Learning – 4Care coordinators
Learning 5 –Medicines Safety
• 200 incident reports completed
• Medicines Safety – Knowledge and skills– Decision making– Practices, processes and systems
• At different levels– National guidance– Inspections– Commissioners– HCPs– Health and Social Care Providers
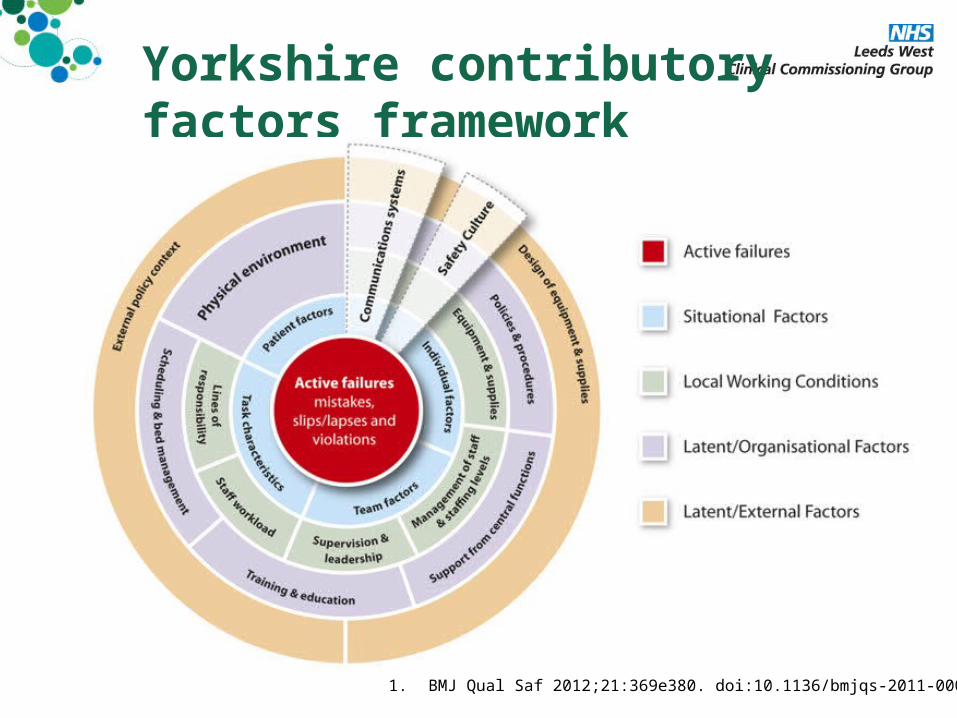
Yorkshire contributory factors framework
1. BMJ Qual Saf 2012;21:369e380. doi:10.1136/bmjqs-2011-000443
Learning 6-Quality Improvement for Patients
• Ensuring appropriate care and monitoring
• Reduced problematic polypharmacy
• Ensuring accurate diagnosis
• Identifying personal medicine preferences, non adherence and agreed and actioned solutions
• Feeding back issues with transfer of care to ward based teams / lead pharmacists to lead improvement in Trust
Learning 7 –Education, Training and Peer Review• Clinical pharmacy in the community Pharmacists
and Technicians meet • 2-3 a year in London and North (Leeds/Manchester/
N’castle)
• In the South• next date is 4th Dec and you can contact
the administrator Sam at [email protected]
• Now in the North!– Lead by Heather Smith Consultant Pharmacist- Care of
Older People and Interfaces of Care at Leeds Teaching Hospital NHS Trust for more information
– email [email protected] – Next meeting : – Monday 12th October 2015 1pm-4pm – Venue: Martin OE meeting room (Neurology Seminar
room), Level E, Martin Wing, Leeds General Infirmary
Key areas 1 – Improve Knowledge and Skills•Prescribers/ Nurses
– Up-skill Primary Care Professionals in frail elderly medicine, pathophysiology and effect on medicines, prescribing choices and processes and monitoring
•All heath care providers– Safe medicines administration and record keeping
•Initiate proactive care / admission avoidance plans INC. medicines / monitoring section
•End of Life - Use of GSF and EPaCCS records
•Commissioners
Key areas 2 –Practices, processes and systems•My role is to facilitate teams to work together
– Care Home– GP practice– Pharmacy
•Medicines safety team role is to provide and ensure– Good practice guidelines / effective policies and safe
processes in the system
•Commissioners– To be aware of current patient groups needs– Set standards and put safety measure in place and monitor
Key areas 3 – Medicines Safety• Medication Errors- record record record – learn learn learn
• New Residents / New care episode / New meds from other team
• Repeat Prescribing
• Repeat person, disease and drug monitoring
• Medicines Plans
• Deprescribing
• Safely record
• Contracts
• Human Factors
• End of Life- key meds, anticipatory prescribing

GRW 80 yr old female in a care home
• Aspirin 75 OD• Bisoprolol 1.25mg
OD• Furosemide 80 OD • Ramipril OD• Digoxin 125 OD• Pravastatin OD• Clopidogrel 75 OD
• Tramadol 100 QDS• Pregabalin TDS• Metformin 850 BD• Gliclazide 80 BD• Citalopram 40 OD• Trazadone 100 ON• Salbutamol MDI
Falls, Sleepy, Constipated, lethargic, dry skin,
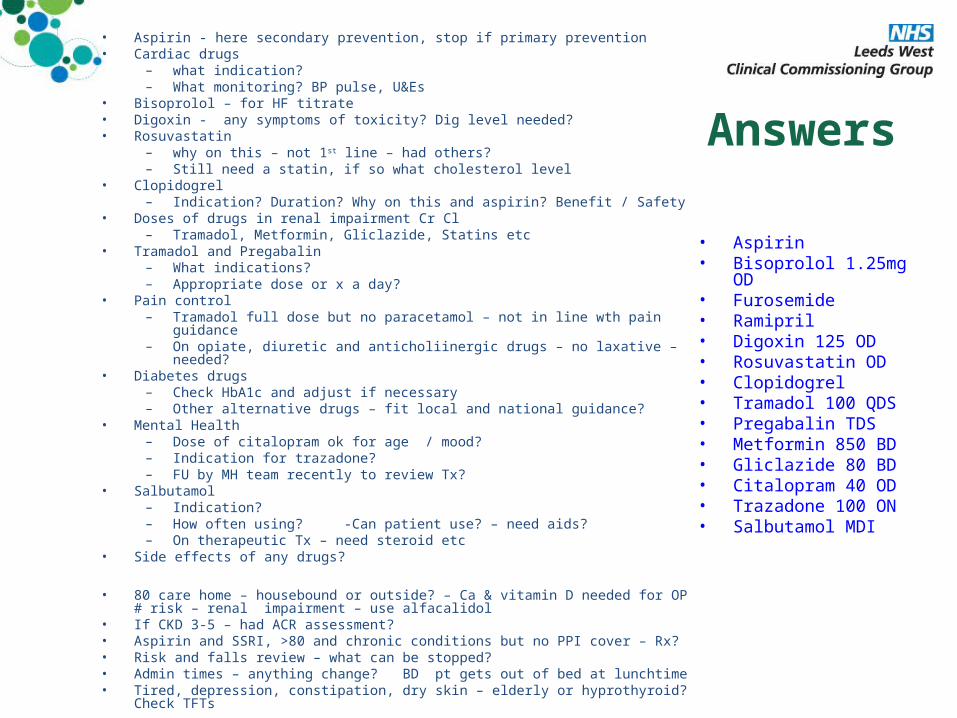
Answers
• Aspirin• Bisoprolol 1.25mg
OD• Furosemide • Ramipril • Digoxin 125 OD• Rosuvastatin OD• Clopidogrel• Tramadol 100 QDS• Pregabalin TDS• Metformin 850 BD• Gliclazide 80 BD• Citalopram 40 OD• Trazadone 100 ON• Salbutamol MDI
• Aspirin - here secondary prevention, stop if primary prevention• Cardiac drugs
– what indication?– What monitoring? BP pulse, U&Es
• Bisoprolol – for HF titrate• Digoxin - any symptoms of toxicity? Dig level needed?• Rosuvastatin
– why on this – not 1st line – had others?– Still need a statin, if so what cholesterol level
• Clopidogrel– Indication? Duration? Why on this and aspirin? Benefit / Safety
• Doses of drugs in renal impairment Cr Cl – Tramadol, Metformin, Gliclazide, Statins etc
• Tramadol and Pregabalin– What indications?– Appropriate dose or x a day?
• Pain control– Tramadol full dose but no paracetamol – not in line wth pain guidance– On opiate, diuretic and anticholiinergic drugs – no laxative – needed?
• Diabetes drugs– Check HbA1c and adjust if necessary– Other alternative drugs – fit local and national guidance?
• Mental Health– Dose of citalopram ok for age / mood?– Indication for trazadone?– FU by MH team recently to review Tx?
• Salbutamol– Indication?– How often using? -Can patient use? – need aids?– On therapeutic Tx – need steroid etc
• Side effects of any drugs?
• 80 care home – housebound or outside? – Ca & vitamin D needed for OP # risk – renal impairment – use alfacalidol
• If CKD 3-5 – had ACR assessment?• Aspirin and SSRI, >80 and chronic conditions but no PPI cover – Rx?• Risk and falls review – what can be stopped?• Admin times – anything change? BD pt gets out of bed at lunchtime• Tired, depression, constipation, dry skin – elderly or hyprothyroid? Check
TFTs
Patient Story- Monitoring for safety and effectiveness
– PEG fed patient not had bloods done for >18 months– FU of care from specialist – case management from dietetics every
year– Sodium 161 Digoxin >1.3 (0.5-1.0 microgram/L) Urea and Creatinine
high– Dehydrated – insufficient fluid in PEG regimen – AKI– Even stable CrCl too low for Rx medicines (DO NOT USE eGFR for
drugs doses)– Poor wound healing – related to high HbA1c– HbA1c excess – insulin and oral meds– Contraindications- stricture but prescribed alendronic acid– Memory drug FU missing
• Need standard PRESET annual (6/12) monitoring systems

Change Agent• Start with myself
• Work out what might help others to change
• Build alliances
• Don't be a martyr
“if you want to go fast, go alone. If you want
to go far, go together”
African proverb quoted by Al Gore

Medicines systems- care homes and EPS• Any top tips for successful
implementation?
For more information go to…..• http://www.leedswestccg.nhs.uk/ne
ws/leeds-care-home-patients-benefit-medication-review-service/
• 0113 84 35528 or 0113 84 35470• [email protected]• @NHSLeedsWestCCG

Thank you for listening
Any Questions?
References 1• Managing medicines in care homes (2013). NICE. London
– NICE Good Practice Guidance. http://www.nice.org.uk/guidance/sc/SC1.jsp – Quality Standards https://www.nice.org.uk/guidance/qs85– Commissioning support http://guidance.nice.org.uk/sfcqs85– Local authority guidance http://publications.nice.org.uk/lgb25
• NHS Scotland. Polypharmacy Guidance. March 2015 • http://www.sehd.scot.nhs.uk/publications/DC20150415polypharmacy.pdf (accessed 11th September 2015)
• Welsh Deprescribing Guidance• http://www.awmsg.org/docs/awmsg/medman/Polypharmacy%20-%20Guidance%20for%20Prescribing%20in%20Fr
ail%20Adults.pdf
• Kings Fund Deprescribing• http://www.kingsfund.org.uk/sites/files/kf/field/field_publication_file/polypharmacy-and-medicines-optimisation-kin
gsfund-nov13.pdf
• East and South East England Specialist Pharmacy Service.• A patient-centred polypharmacy (incorporating 7 steps to deprescribing). Version 12 Updated July
2015• http://www.medicinesresources.nhs.uk/en/Communities/NHS/SPS-E-and-SE-England/Meds-use-and-safety/Service-
deliv-and-devel/Older-people-care-homes/Polypharmacy-oligopharmacy--deprescribing-resources-to-support-local-delivery/. (accessed 11th September 2015)
• New approaches to Polypharmacy, oligopharmacy and deprescribing. London: 2014. http://www.medicinesresources.nhs.uk/upload/documents/Communities/SPS_E_SE_England/Presn_OPNet_19Nov13_New_approaches_Polypharm_Oligopharm_and_deprescribing_NB_LO.pdf (accessed 11th September 2015).
• All others accessed 26 04 2015

References 2• Care Quality Commission. Managing patients’ medicines after
discharge from hospital. October 2009• Polypharmacy and Medicines Optimisation – Making it safe and
sound (2013). The Kings Fund. London. Authors M Duerden, T Avery and R Payne. Accessed 7 4 14
• http://www.kingsfund.org.uk/sites/files/kf/field/field_publication_file/polypharmacy-and-medicines-optimisation-kingsfund-nov13.pdf
• Making our health and care systems fit for an aging population (2014). The Kings Fund. London. Authors D Oliver, C Foot, R Humphries.
• http://www.kingsfund.org.uk/sites/files/kf/field/field_publication_file/making-health-care-systems-fit-ageing-population-oliver-foot-humphries-mar14.pdf Accessed 7 4 14
• Quest for Quality (2011). BGS Joint Working Party Inquiry into the Quality of Healthcare Support for Older People in Care Homes: A Call for Leadership, Partnership and Quality Improvement
• http://www.bgs.org.uk/campaigns/carehomes/quest_quality_care_homes.pdf Accessed 19 12 13
• British Geriatric Society (BGS) Commissioning Guidance. High quality healthcare for older care home residents (2013)
• http://www.bgs.org.uk/campaigns/2013commissioning/Commissioning_2013.pdf Accessed 19 12 13
• Fit for Frailty. British Geriatrics Society • http://www.bgs.org.uk/index.php/fit-for-frailty accessed 26 04 2015
References 3• Care Home’ use of medicines study (CHUMS): Prevalence, causes & potential
harm of medication errors in care homes for older people• http://www.birmingham.ac.uk/Documents/college-mds/haps/projects/cfhep/psrp/
finalreports/PS025CHUMS-FinalReportwithappendices.pdf Accessed 19 12 13 and also published as
• Barber ND, Alldred DP, Dickenson R et al. Care homes’ use of medicines (CHUMS) study: prevalence, causes and potential harm of medication errors in care homes for older people. Quality and Safety in Healthcare 2009;18:341–346
• Safety of Medicines in Care Homes. National Care Forum (2013)• http://patientsafety.health.org.uk/sites/default/files/resources/
safety_of_medicines_in_the_care_home_0.pdf Accessed 19 12 13• Clinical Medication Review. A Practical Guide. NHS Cumbria 2013 Accessed 4 4
14• http://www.cumbria.nhs.uk/ProfessionalZone/MedicinesManagement/
Guidelines/MedicationReview-PracticeGuide2011.pdf• Task Force on Medicines Partnership and the National Collaborative Medicines
Management Services Programme. Room for Review. A guide to medication review: the agenda for patients, practitioners and managers. 2002
• Report and Action Plan of the Steering Group on Improving the Use of Medicines (for better outcomes and reduced waste). Improving the use of medicines for better outcomes and reduced waste: An action Plan. October 2012
• Royal Pharmaceutical Society of Great Britain. Moving Patient, Moving Medicines, Moving Safely – Discharge and Transfer Planning. March 2008