hemiplegic shoulder pain & complex regional pain syndrome · patients with right hemiplegia...
TRANSCRIPT
11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 1 of 42 www.ebrsr.com
EBRSR [Evidence-Based Review of Stroke Rehabilitation]
11 Hemiplegic Shoulder Pain &
Complex Regional Pain Syndrome Evidence Tables
Joshua Wiener BHSc, Andreea Cotoi MSc, Ricardo Viana MD, John Chae MD, Richard Wilson MD, Tom
Miller MD, Norine Foley MSc, Robert Teasell MD
Last Updated: March 2018
Dr. Robert Teasell Parkwood Institute, 550 Wellington Road, London, Ontario, Canada, N6C 0A7
Phone: 519.685.4000 ● Web: www.ebrsr.com ● Email: [email protected]

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 2 of 42 www.ebrsr.com
Table of Contents
Table of Contents ...............................................................................................................................2 11.2 Shoulder Subluxation and Hemiplegic Shoulder Pain .................................................................3
11.2.2 Scapular Rotation .......................................................................................................................... 3 11.2.3 Pain in Shoulder Subluxation ........................................................................................................ 4
11.3 Spasticity, Contractures, and Hemiplegic Shoulder Pain .............................................................7 11.3.2 Spastic Muscle Imbalance ............................................................................................................. 7 11.3.3 Contracted/Frozen Shoulder ........................................................................................................ 7
11.6 Functional Impact of Hemiplegic Shoulder Pain .........................................................................9 11.7 Management of Hemiplegic Shoulder Pain .............................................................................. 10
11.7.1 Positioning of the Hemiplegic Shoulder ..................................................................................... 10 11.7.2 Slinging the Hemiplegic Shoulder ............................................................................................... 12 11.7.3 Strapping/Taping the Hemiplegic Shoulder ................................................................................ 13 11.7.4 Active Therapies for the Hemiplegic Shoulder ........................................................................... 15 11.7.5 Electrical Stimulation of the Hemiplegic Shoulder ..................................................................... 17 11.7.6 Botulinum Toxin Injections for the Hemiplegic Shoulder ........................................................... 22 11.7.7 Steroid Injections for the Hemiplegic Shoulder .......................................................................... 24 11.7.8 Hyaluronic Acid Injections for the Hemiplegic Shoulder ............................................................ 26 11.7.9 Suprascapular Nerve Block for the Hemiplegic Shoulder ........................................................... 27 11.7.10 Segmental Neuromyotherapy for the Hemiplegic Shoulder .................................................... 27 11.7.11 Surgery of the Hemiplegic Shoulder ......................................................................................... 28 11.7.12 Complementary & Alternative Therapies for the Hemiplegic Shoulder ................................... 28
11.8 Complex Regional Pain Syndrome (CRPS) ................................................................................ 30 11.8.6 Pharmacological Interventions for CRPS .................................................................................... 30 11.8.7 Mirror Imagery Therapy for CRPS ............................................................................................... 32 11.8.8 Exercise for the Prevention and Treatment of CRPS .................................................................. 33 11.8.10 Calcitonin for the Prevention of CRPS ...................................................................................... 34
References ....................................................................................................................................... 35

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 3 of 42 www.ebrsr.com
11.2 Shoulder Subluxation and Hemiplegic Shoulder Pain
11.2.2 Scapular Rotation Table 11.2.2 Scapular Rotation in the Hemiplegic Shoulder
Author, Year Country
Study Design PEDro Score
Time Post Stroke Sample Size
Methods Outcomes
Prévost et al. (1987) Canada Observational No Score TPS=NA N=50
Intervention: Patients with right hemiplegia were measured for inferior subluxation using a tridimensional x-ray technique, giving true vertical distance separating the apex of the humeral head and the inferior margin of the glenoid cavity. Both shoulders were evaluated and the difference used as a measure of subluxation. The measure was then compared to the orientation of the scapula relative to the vertical and the abduction of the arm. Outcomes: Subluxation.
1. The angle of abduction of the arm of the affected side was significantly greater than on the non-affected side (p<0.05), but the relative abduction of the arm was on the same order of magnitude for both sides. There was no significant relationship between the orientation of the scapula and the severity of the subluxation.
2. The abduction of the humerus was weakly (r=0.24) related to the subluxation, which partly explained the weak association found between the relative abduction of the arm and the subluxation.
Culham et al. (1995) Canada Case Control No Score TPS=NA N=34
Intervention: Patients with hemiplegia were divided into high-tone and low-tone groups according to Ashworth scoring of muscle tone. Low tone patients scored less than 4 and high tone patients had a score of 4 or greater on the MAS. Outcomes: Subluxation.
1. Scapula was significantly further from the midline and lower on the thorax on the affected side in the low-tone group.
2. Glenohumeral subluxation was significantly greater in the low-tone group.
3. Scapular abduction angle was significantly greater on the non-affected side in the low-tone group. In the high-tone group, no differences were found between the affected and the non-affected side in either the angular or linear measures.
Price et al. (2001) UK Observational No Score TPS=Chronic N=30
Intervention: Patients received a standardized clinical assessment, whereby manual palpitation of the subacrimonial space was performed to identify those with subluxation. Outcomes: Upper Limb Motricity Score (ULMS); Scapular downward tilt; Dynamic scapular lateral rotation.
1. 24 patients had no shoulder subluxation, 6 patients suffered from shoulder subluxation.
2. Among all patients, the average degree of scapular downward tilt was 10.04 for the unaffected side and 10.46 for the affected side (p>0.05).
3. There was no difference in the scapular downward tilt of the affected shoulder of subjects with and without subluxation.
Niessen et al. (2008) Netherlands Observational No Score TPS=NA N=27
Intervention: Patients were compared to matched controls in terms of shoulder kinematics. Outcomes: Pain.
1. In patients with shoulder pain, scapular lateral rotation was increased at rest, abduction, and flexion when compared to those without pain and controls.
2. In patients with shoulder pain, glenohumeral elevation was decreased

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 4 of 42 www.ebrsr.com
during passive abduction compared to those without pain and controls.
11.2.3 Pain in Shoulder Subluxation Table 11.2.3.1 Studies Supporting an Association Between Pain and Hemiplegic Shoulder Subluxation
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Shai et al. (1984) Israel Observational No Score TPS=Subacute-Chronic N=33
Intervention: Patients received at least a single radiograph early in their hospitalization. Outcomes: Subluxation; Pain.
1. There was a significant correlation between abnormal radiologic findings early in the course of stroke and the development of pain. 19/33 patients had evidence of subluxation on radiograph and 17/33 had shoulder pain.
2. Of those with shoulder pain 14/17 (82%) had subluxed shoulders.
Lo et al. (2003) Taiwan Observational No Score TPS=NA N=32
Intervention: Patients with shoulder pain were assessed for shoulder subluxation, which was diagnosed by a gap of more than one finger breadth between the acromion and the head of the humeral bone on palpation. Outcomes: Subluxation; Pain.
1. 14 (44%) of patients with pain had clinically diagnosed shoulder subluxation.
Aras et al. (2004) Turkey Observational No Score TPS=NA N=85
Intervention: Patients admitted to rehabilitation were studied to identify the incidence of shoulder pain and the factors associated with it. Outcomes: Subluxation; Pain.
1. 27 patients had glenohumeral joint subluxation and reported shoulder pain, compared to 5 patients with the same finding, but without pain.
Paci et al. (2007) Italy Observational No Score TPS=Acute N=107
Intervention: Patients were categorized according to those presence (N=52) or lack (N=55) of glenohumeral subluxation. Outcomes: Pain; Fugl-Meyer Assessmet (FMA).
1. Subluxation was significantly correlated with shoulder pain at admission, discharge, and 30d follow-up (p<0.001).
2. Subluxation at admission accounted for nearly 50% of shoulder pain at follow-up (R2=0.458, p<0.001).
3. Subluxation at admission was associated with FMA upper limb score at follow-up (R2=0.766, p<0.001).
Suethanapornkul et al. (2008) Observational Thailand No Score TPS=NA N=327
Intervention: Patients from rehabilitation centres were assessed weekly during inpatient rehabilitation for the presence of pain and subluxation. (Neither the criteria used to measure subluxation, nor the scale used to assess pain is described). Outcomes: Subluxation; Pain.
1. 62 patients (19%) were found to have shoulder pain and 122 (37%) patients had shoulder subluxation.
2. Shoulder pain was significantly more frequent in subjects with shoulder subluxation (odds ratio (OR) 2.48, and at 2-6 months after stroke onset (OR 4.0).
3. Shoulder subluxation was significantly associated with hemorrhagic stroke, loss of proprioceptive sensation and was negatively associated with Brunnstrom's

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 5 of 42 www.ebrsr.com
stage of arm recovery.
Table 11.2.3.2 Studies Not Supporting an Association Between Pain and Hemiplegic Shoulder Subluxation
Author, Year Country
Study Design PEDro Score
Time Post Stroke Sample Size
Methods Outcomes
Bohannon (1988) USA Observational No Score TPS=Acute N=30
Intervention: Patients admitted for inpatient rehabilitation as average of 31 days following stroke. A variety of tests were performed at admission and discharge to assess their correlation with shoulder pain. Outcomes: Subluxation.
1. 24 patients had shoulder pain on initial assessment and 27 on final assessment. 30% of shoulders were subluxed on initial assessment and 47% at final assessment.
2. There was no statistical significant relationship between pain and subluxation.
Van Langenberghe &
Hogan (1988)
UK Observational No Score TPS=NA N=48
Intervention: Patients were assessed using goniometry and radiography. Outcomes: Pain; Subluxation.
1. There was no significant difference in degree of pain between patients with and without subluxation.
2. There was no significant correlation between grade of subluxation and degree of pain.
Bohannon & Andrews (1990) USA Observational No Score TPS=NA N=28
Intervention: Patients undergoing rehabilitation for their first stroke who could follow instructions, and were aware of the position of their paretic limb in space were included. Paretic shoulder subluxation and paretic shoulder pain were measured. Shoulder subluxation was measured while the patients sat on the edge of a mat table with their paretic upper extremity dependent and the examiner used his thumb to palpate the separation between the acromion and the head of the humerus. He then graded subluxation as none (0), minimal (1) or substantial (2). Shoulder pain was measured during slow lateral rotation of the joint while the patients were supine. All patients’ shoulders were abducted about 450 and their elbows were held at 900 with their forearms pronated with measurements beginning from neutral shoulder rotation. Outcomes: Ritchie Articular Index (RAI); Shoulder Range of Motion Pain (SROMP).
1. 70.8% of patients demonstrated enough shoulder pain on RAI to at least cause them to wince when their shoulders were rotated laterally 900; the SROMP of the paretic side was measured as 64.50+28.80 and 64.60+28.90.
2. A significant correlation (-77s, p<0.001) was observed between the RAI and SROMP, indicating that patients with higher scores on the RAI had fewer degrees of ROM before pain was experienced.
Joynt (1992) USA Observational No Score TPS=Acute-Chronic N=97
Intervention: Patients with upper extremity pain were examined. The interval from stroke onset to examination ranged from several days to a few years. Outcomes: Subluxation.
1. 49 patients with specific shoulder pain were compared to 18 patients with pain, not localized to the shoulder.
2. Patients complaining of shoulder pain did not exhibit subluxation more frequently than patients with general pain in the affected extremity.
Wanklyn et al. (1996) UK
Intervention: Patients were assessed clinically, 3 times over a 6-month period following stroke.
1. Subluxation was detected clinically in 31 (29%) patients at hospital discharge and 27

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 6 of 42 www.ebrsr.com
Observational No Score TPS=NA N=108
Subluxation was assessed clinically and graded in finer-breadths palpable below the acrimonion process. Outcomes: Subluxation.
(26%) at 26 weeks. 2. Shoulder pain was not associated with
subluxation at 2/3 assessment points. The authors do not provide details of the data.
Zorowitz et al. (1996) Observational USA No Score TPS=Acute N=20
Intervention: Patients with shoulder pain admitted to a rehabilitation hospital within 6 weeks of their first stroke were studied. Outcomes: Subluxation.
1. Shoulder pain after stroke was not correlated with age, vertical, horizontal, or total asymmetry, shoulder flexion or abduction, or Fugl-Meyer scores.
2. However, shoulder pain was strongly correlated with degree of shoulder external rotation.
Ikai et al. (1998) Japan Observational No Score TPS=NA N=75
Intervention: Patients with shoulder subluxation were assessed for pain using a visual analogue scale at rest and during passive range of motion. The degree of pain was expressed as nonexistent (0), mild (1-3), moderate (4-7), or severe (8-10) during passive movement. Outcomes: Pain.
1. At rest, 10 patients reported pain. During passive range of motion, 5 patients reported no pain, 25 reported mild pain, 36 reported moderate pain and 9 reported severe pain.
2. Shoulder pain was not related to the degree of shoulder subluxation.
Barlak et al. (2009) Turkey Observational No Score TPS=NA N=187
Intervention: Patients admitted for inpatient rehabilitation were evaluated for the presence of pain. Each patient was evaluated by clinical, radiographic, and ultrasonographic examination. Patients were divided into two groups, one comprising patients with shoulder pain and the other comprising patients without shoulder pain. They were then compared with respect to clinical characteristics, radiologic findings, and FIM scores. Outcomes: Functional Independence Measure (FIM); Pain.
1. Shoulder pain was present in 114 (61%) patients. Of the 114 patients with pain, 71 patients showed various grades of glenohumeral joint subluxation.
2. There was no association between pain and degree of subluxation.
3. The group without HSP showed significantly more improvement than the group with HSP in functional outcomes (P=0.01) and the hospitalization period was significantly shorter (P=0.03).
4. The mean discharge FIM score was higher among patients without HSP (93 vs. 82, p<0.001)
Mohamed et al. (2014) Egypt Observational No Score TPS=NA NStart=80 NEnd=80
Population: Mean age=62.29±8.93yr. Gender: Males=56.25%, Females=43.75%. Intervention: Patients were examined for structural abnormalities of both the painful hemiplegic shoulder and contralateral unaffected shoulder by ultrasound (U/S). Outcomes: Brunnstrom Staging; Brief Pain Inventory (BPI); Range of Motion (ROM).
1. For the painful hemiplegic shoulder, U/S grades were positively correlated with age and shoulder pain duration, though these correlations were not significant.
2. For the unaffected shoulder, U/S grades were significantly correlated with BPI score and shoulder pain duration (p<0.05).
3. There was no significant relationship between U/S grades of the affected painful hemiplegic shoulder and the Brunnstrom motor recovery stages.
Lin et al. (2014) Taiwan Observational No Score TPS=NA NStart=145 NEnd=145
Population: Mean age=62.1±13.2yr; Gender: Males=89, Females=56. Intervention: Patients were divided into three groups according to time post stroke (≤3mo, 3mo-1yr, and >1 yr).Three muscle tender points (MTePs) were assessed. Outcomes: Numerical Rating Scale (VRS); Pressure Pain Threshold (PPT).
1. Spontaneous pain (VRS) was more severe in the hemiparetic side than in the healthy side, but there was no obvious difference between the sides in the PPT of the muscle or the periosteum.

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 7 of 42 www.ebrsr.com
11.3 Spasticity, Contractures, and Hemiplegic Shoulder Pain
11.3.2 Spastic Muscle Imbalance Table 11.3.2 Spastic Muscle Imbalance
Author, Year Country
Study Design PEDro Score
Time Post Stroke Sample Size
Methods Outcomes
Bohannon et al. (1986) USA Observational No Score TPS=NA N=50
Intervention: Patients with hemiplegia was secondary to cerebrovascular accident, whose unaffected shoulders demonstrated normal and pain-free range of hemiplegia shoulder external rotation (ROSER, 900); able to adequately follow instructions to allow testing of all variables pertinent to the study. Information was retrieved from patients’ records concerning their initial physical therapy evaluation. Outcomes: Pain; Spasticity.
1. Of the 50 patients reviewed, 72% had shoulder pain. 20 had some pain while 16 had severe pain. Three zero-order correlations were significant: ROSER and shoulder pain (r=-0.061, p<0.001), time since onset of hemiplegia and shoulder pain (r=0.45, p<0.01), and time since onset of hemiplegia and ROSER (r=0.37, p<0.01).
2. One-way ANOVA demonstrated that time since onset of hemiplegia (F=8.28, p<0.001) and the ROSER (F=18.44, p<0.001) were significantly different in patients with no pain, some pain, and pronounced/severe pain.
van Ouwenaller et al. (1986) Switzerland Observational No Score TPS=Chronic N=219
Intervention: Patients with hemiplegia were followed for 1 year after their stroke. Radiographic examinations were done for each patient. Outcomes: Pain; Spasticity.
1. 72% of patients had shoulder pain at least once during their recovery occurring most often in patients having spasticity (85%) than in patients which flaccidity (18%).
2. Appearance of spasticity was evident in 80% of patients while 20% remained hypotonic.
Joynt (1992) USA Observational No Score TPS=Chronic N=97
Intervention: Patients were examined between 6-9 months post stroke for evidence of shoulder dysfunction and pain, based on clinical examination. Outcomes: Pain; Spasticity.
1. 67 patients were diagnosed with a shoulder problem. 49% of patients reported shoulder pain.
2. Shoulder pain was unrelated to spasticity, assessed by resistance to rapid stretch.
Aras et al. (2004) Turkey Observational No Score TPS=NA N=85
Intervention: Patients were grouped by the presence or absence of shoulder pain. The association between spasticity measured by the Ashworth scale and shoulder pain was assessed. Outcomes: Pain; Spasticity.
1. 54 patients had shoulder pain and 31 did not.
2. There was no association between spasticity and shoulder pain.
11.3.3 Contracted/Frozen Shoulder Table 11.3.2 Contracted/Frozen Shoulder
Author, Year Methods Outcomes

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 8 of 42 www.ebrsr.com
Country Study Design PEDro Score
Time Post Stroke Sample Size
Hakuno et al. (1984) Japan Observational No Score TPS=NA N=77
Intervention: Patients were randomly selected from all hemiplegic patients treated at rehab centre. Paralysis affected the right side in 35 patients and the left side in 42 patients. In 35 cases the affected arm was dominant whereas 42 cases had paralysis in non-dominant arm. Positive contrast arthography was performed on both shoulders of all patients. An anterior approach for injection of the joint with contrast material was employed. The needle was inserted directly into the glenohumeral joint space under fluoroscopic control. Anteroposterior radiographs were made in internal and external rotation. Outcomes: Contractures; Capsular structure.
1. Contractures/adhesions were found in paralyzed shoulders at a statistically significant higher rate (54.6%) than in the non-paralysed side (32.5%).
2. The occurrence rate of contrast leakage from a capsule tear on the subscapular bursa and the bicipital tendon sleeve was higher on the non-paralysed side than on the paralysed side.
3. It was suggested that capsular contracture due to hemiplegia reduces capsular tearing during arthrographic manoeuvres.
Grossens-Sills & Schenkman (1985) USA Observational No Score TPS=NA N=21
Intervention: Patients received standard physical therapy treatment and were assessed at admission, three weeks, and discharge. Outcomes: Pain; Subluxation; Range of Motion (ROM).
1. 67% of the patients entered the rehab centre with signs of shoulder pain.
2. An additional 10% developed initial signs of shoulder pain by 3 weeks post-admission and another 5% developed signs of pain at time of discharge.
3. Positive correlation noted between loss shoulder ROM and increase in pain and between subluxation and pain was found however, these findings may not necessarily be indicative of frozen shoulder.
4. There was no correlation between subluxation and ROM.
5. Suggestion that pain began in the acute care facility and worsened while in rehabilitation.
Rizk et al. (1984) USA Observational No Score TPS=NA N=30
Intervention: Patients with painful ipsilateral shoulders meeting the following criteria: maximum passive range of motion (ROM) of 600 abduction, 900 forward flexion, 150 external rotation, 450
extension; any stress at the limit of motion produced severe shoulder, with no improvement during the previous 2 weeks, no history of recent trauma to the affected shoulder during the previous 2 weeks, no history of seizures or anticonvulsant medications; no clinical signs suggesting shoulder-hand syndrome, no bone disease or polyarthritis or previous shoulder pain before stroke onset. All patients had shoulder arthrograms performed. Outcomes: Electromyographic studies on the deltoid, triceps, and biceps brachii muscles.
1. 23 patients had capsular constriction typical of frozen shoulder (adhesive capsulitis). 7 patients had normal arthrograms.
2. None showed rotator cuff of capsular tears. 3. Electromyography revealed electrical
silence in the shoulder musculature at rest.
Lo et al. (2003) Intervention: Consecutive patients with shoulder 1. 16 (54%) of patients had rotator cuff tears
11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 9 of 42 www.ebrsr.com
Taiwan Observational No Score TPS=NA N=32
pain following stroke were assessed for shoulder subluxation, which was diagnosed by a gap of more than one finger breadth between the acromion and the head of the humeral bone on palpation. Outcomes: Rotator cuff tears.
diagnosed by arthrography.
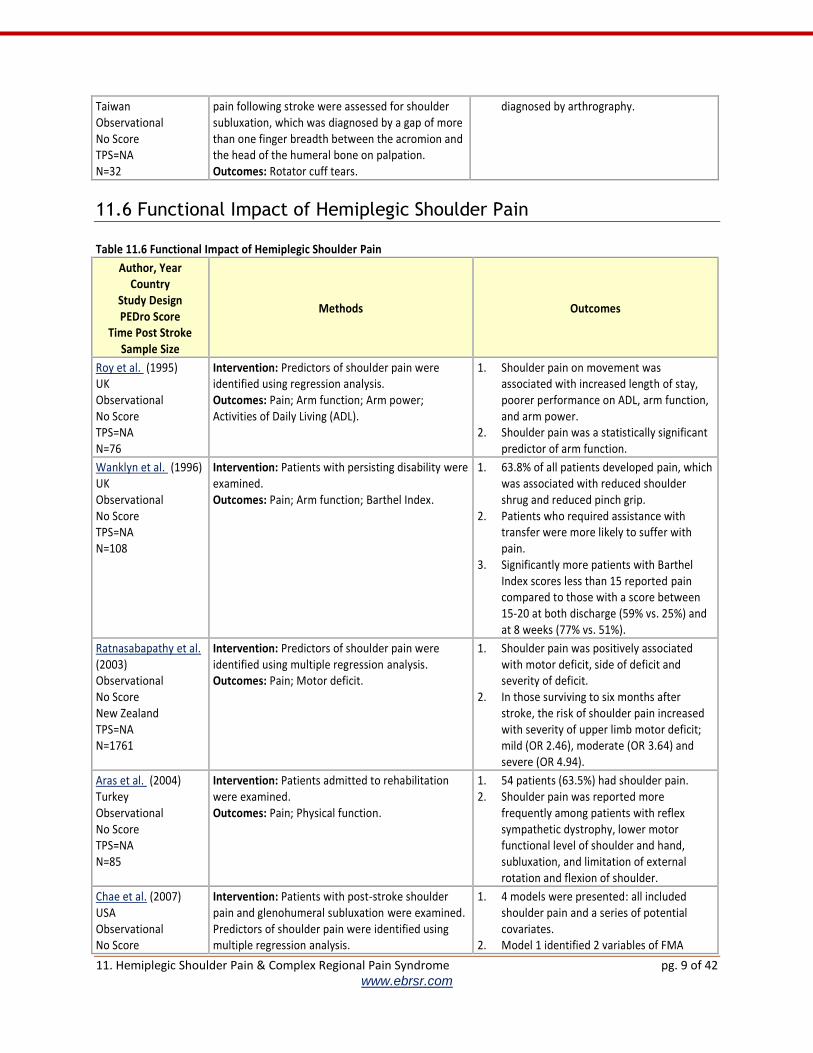
11.6 Functional Impact of Hemiplegic Shoulder Pain Table 11.6 Functional Impact of Hemiplegic Shoulder Pain
Author, Year Country
Study Design PEDro Score
Time Post Stroke Sample Size
Methods Outcomes
Roy et al. (1995) UK Observational No Score TPS=NA N=76
Intervention: Predictors of shoulder pain were identified using regression analysis. Outcomes: Pain; Arm function; Arm power; Activities of Daily Living (ADL).
1. Shoulder pain on movement was associated with increased length of stay, poorer performance on ADL, arm function, and arm power.
2. Shoulder pain was a statistically significant predictor of arm function.
Wanklyn et al. (1996) UK Observational No Score TPS=NA N=108
Intervention: Patients with persisting disability were examined. Outcomes: Pain; Arm function; Barthel Index.
1. 63.8% of all patients developed pain, which was associated with reduced shoulder shrug and reduced pinch grip.
2. Patients who required assistance with transfer were more likely to suffer with pain.
3. Significantly more patients with Barthel Index scores less than 15 reported pain compared to those with a score between 15-20 at both discharge (59% vs. 25%) and at 8 weeks (77% vs. 51%).
Ratnasabapathy et al. (2003) Observational No Score New Zealand TPS=NA N=1761
Intervention: Predictors of shoulder pain were identified using multiple regression analysis. Outcomes: Pain; Motor deficit.
1. Shoulder pain was positively associated with motor deficit, side of deficit and severity of deficit.
2. In those surviving to six months after stroke, the risk of shoulder pain increased with severity of upper limb motor deficit; mild (OR 2.46), moderate (OR 3.64) and severe (OR 4.94).
Aras et al. (2004) Turkey Observational No Score TPS=NA N=85
Intervention: Patients admitted to rehabilitation were examined. Outcomes: Pain; Physical function.
1. 54 patients (63.5%) had shoulder pain. 2. Shoulder pain was reported more
frequently among patients with reflex sympathetic dystrophy, lower motor functional level of shoulder and hand, subluxation, and limitation of external rotation and flexion of shoulder.
Chae et al. (2007) USA Observational No Score
Intervention: Patients with post-stroke shoulder pain and glenohumeral subluxation were examined. Predictors of shoulder pain were identified using multiple regression analysis.
1. 4 models were presented: all included shoulder pain and a series of potential covariates.
2. Model 1 identified 2 variables of FMA

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 10 of 42 www.ebrsr.com
TPSRange>12wk N=61
Outcomes: Brief Pain Inventory 12 (BPI-12); Numeric Rating Scale (NRS); Fugl-Meyer Assessment (FMA); Arm Motor Ability Test (AMAT); Functional Independence Measure (FIM); Quality of Life (QOL).
scores: subluxation and external rotation ROM.
3. Model 2 found there were no predictors of FIM self-care.
4. Model 3 found FMA and stroke type were predictors of AMAT function.
5. Model 4 found pain was a predictor of QoL. 6. Pain was not a predictor of function in any
of the other 3 models.
Lindgren et al. (2014) Sweden Observational No Score TPSMean=15±8mo N=49
Population: Mean age=64±9yr; Gender: Males=35, Females=14. Intervention: Patients with shoulder pain (N=24) were compared to those without it (N=25). Outcomes: Range of Motion (ROM); Modified Motor Assessment Scale (MMAS); Fugl-Meyer Assessment (FMA); Modified Ashworth Scale (MAS); Stroke Impact Scale (SIS); Life Satisfaction (LS).
1. Patients with shoulder pain had significantly lower median ROM for passive abduction than those without (90° vs 130°, p=0.001), but there was no significant difference in ROM for external rotation (40° vs 50°, p=0.12).
2. Patients with shoulder pain had significantly poorer MMAS scores than those without (p=0.03).
3. There were no significant differences between groups on FMA, MAS, SIS, or LS.
Caglar et al. (2016) Turkey Case Series TPSMedian=11.1mo NStart=156 NEnd=156
Population: Mean age=64.3±12.5yr; Gender: Males=75, Females=81. Intervention: Patients with shoulder pain (N=46) were compared to those without it (N=110). Outcomes: Functional Independence Measure (FIM); Functional Ambulation Scale (FAS); Brunnstrom Recovery Stages (BRS).
1. Both groups showed significant improvements after rehabilitation on both the FAS and FIM, as well as BRS for hand and lower limb (p<0.001)
2. There were no significance differences between groups (p>0.05).
11.7 Management of Hemiplegic Shoulder Pain
11.7.1 Positioning of the Hemiplegic Shoulder Table 11.7.1 Positioning of the Hemiplegic Shoulder in Stroke Patients
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Dean et al. (2000) Australia RCT PEDro=7 TPSE=32.1d TPSC=35.3d N=23
Intervention: Patients were randomized to receive an experimental therapy or to a control group. Subjects in both groups participated in a multidisciplinary rehabilitation program and participated in active training of reaching and manipulation tasks. The experimental group received prolonged positioning to the affected shoulder each day, five days a week for six days (positioning). Outcomes: Range of Motion (ROM); Pain.
1. Changes in active and passive ROM were not significant between the groups with the level of pain remaining unchanged.
Ada et al. (2005) Australia RCT
Intervention: Patients were randomized to an intervention or a control condition. Patients in the experimental group received two, 30-minute
1. Positioning the shoulder in maximal external rotation (position 1) significantly reduced the development of contractures,

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 11 of 42 www.ebrsr.com
PEDro=8 TPSMean=14d N=36
sessions of sustained shoulder positioning. Patients in both groups received 10 minutes of shoulder exercises and routine upper limb care. The treatment was provided for 4 weeks and assessments were taken at weeks 2 and 6. Outcomes: Contracture; Pain; Range of Motion (ROM).
compared to the control group. 2. In position 2 (where patients sat with the
affected arm resting on a table with the shoulder at 900, for 30 minutes daily), did not prevent the development of contractures.
3. There were fewer subjects with pain on maximum passive shoulder external rotation in the experimental group (33%) than in the control group (50%) by post-test but this difference was not significant (p=0.55).
Turton & Britton (2005) UK RCT PEDro=6 TPSMean=4wk N=25
Intervention: Patients were randomized to receive usual care alone or with a static muscle stretch regime. The regime consisted of two 30min stretches for wrist and finger flexors and two 30min stretches for shoulder adductors and internal rotators. Patients performed rehabilitation, and the regime, daily for 12wk. Outcomes: Range of Motion (ROM); Contracture.
1. There was no significant difference between groups on any outcome measure at 4wk, 8wk, or 12wk.
2. Time had a significant effect on ROM for shoulder (F=14.1, p<0.001) and wrist (F=10.9, p<0.001).
3. There was a significant loss of shoulder ROM between 8-12wk (t=3.1, p<0.01)
4. Time had a significant effect on contracture for shoulder (F=16.2, p<0.001) and wrist (F=12.5, p<0.001).
5. There was a significant increase in contracture between 4-8wk for shoulder (t=3.2, p<0.01) and wrist (t=3.5, p<0.01).
Gustafsson & McKenna (2006) Australia RCT PEDro=6 TPSE=16.5d TPSC=19.7d N=34
Intervention: Patients with upper extremity hemiparesis admitted within 100 days of stroke were randomized to a participated in a programme of two static positional stretches, each held for 20 minutes, once daily or to a control condition where the affected arm was supported when seated in bed. Outcomes were assessed at hospital admission and discharge. Outcomes: Ritchie Articular Index (RAI); Pain-Free Passive Range of Motion (PFP ROM); Motor Assessment Scale (MAS); Modified Barthel Index (mBI).
1. There were no significant between group differences reported for any of the outcomes.
2. Subjects in both groups demonstrated a reduction in mean PFP ROM into external rotation.
3. All participants reported increases on MAS and mBI.
4. There was a non-significant increase in RAI with movement among subjects in the treatment group and a decrease among subjects in the control group.
5. There was a non-significant decrease in RAI at rest among subjects in both the treatment and control groups.
de Jong et al. (2006) Netherlands RCT PEDro=7 TPSRange<12wk N=19
Intervention: Patients with stroke onset no greater than 12 weeks post stroke with severe arm paresis were randomized to receive routine inpatient rehabilitation (n=10) or rehabilitation + a prescribed positioning procedure for 5 weeks, twice daily for a ½ hour (n=9). The arm was positioned with as much shoulder abduction, shoulder external rotation, elbow extension and supination of the forearm as the patient could endure. Outcomes were assessed at baseline, 5 and 10 weeks following treatment Outcomes: Pain; Passive Range of Motion (PFP
1. There were no significant differences between the groups on any of the other outcomes.
2. No statistical tests were carried out at week 10 due to dropouts.
11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 12 of 42 www.ebrsr.com
ROM); Ashworth Scale (AS); Fugl-Meyer Assessment (FMA); Modified Barthel Index (mBI).
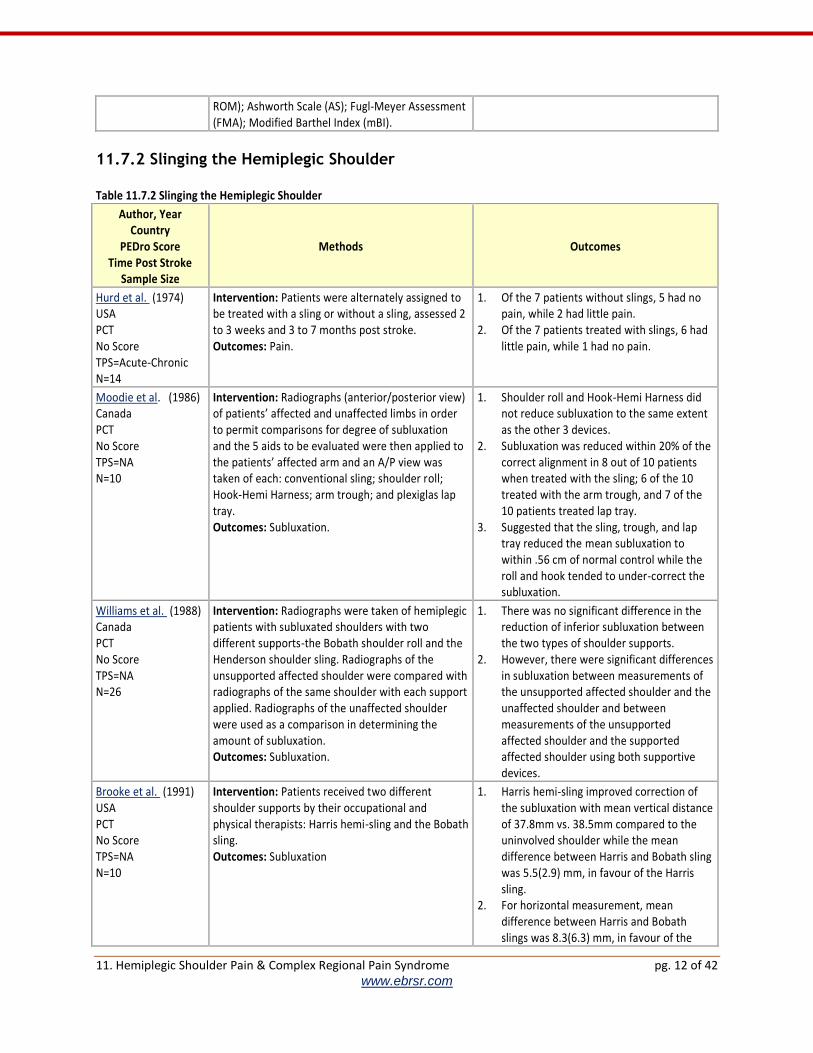
11.7.2 Slinging the Hemiplegic Shoulder Table 11.7.2 Slinging the Hemiplegic Shoulder
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Hurd et al. (1974) USA PCT No Score TPS=Acute-Chronic N=14
Intervention: Patients were alternately assigned to be treated with a sling or without a sling, assessed 2 to 3 weeks and 3 to 7 months post stroke. Outcomes: Pain.
1. Of the 7 patients without slings, 5 had no pain, while 2 had little pain.
2. Of the 7 patients treated with slings, 6 had little pain, while 1 had no pain.
Moodie et al. (1986) Canada PCT No Score TPS=NA N=10
Intervention: Radiographs (anterior/posterior view) of patients’ affected and unaffected limbs in order to permit comparisons for degree of subluxation and the 5 aids to be evaluated were then applied to the patients’ affected arm and an A/P view was taken of each: conventional sling; shoulder roll; Hook-Hemi Harness; arm trough; and plexiglas lap tray. Outcomes: Subluxation.
1. Shoulder roll and Hook-Hemi Harness did not reduce subluxation to the same extent as the other 3 devices.
2. Subluxation was reduced within 20% of the correct alignment in 8 out of 10 patients when treated with the sling; 6 of the 10 treated with the arm trough, and 7 of the 10 patients treated lap tray.
3. Suggested that the sling, trough, and lap tray reduced the mean subluxation to within .56 cm of normal control while the roll and hook tended to under-correct the subluxation.
Williams et al. (1988) Canada PCT No Score TPS=NA N=26
Intervention: Radiographs were taken of hemiplegic patients with subluxated shoulders with two different supports-the Bobath shoulder roll and the Henderson shoulder sling. Radiographs of the unsupported affected shoulder were compared with radiographs of the same shoulder with each support applied. Radiographs of the unaffected shoulder were used as a comparison in determining the amount of subluxation. Outcomes: Subluxation.
1. There was no significant difference in the reduction of inferior subluxation between the two types of shoulder supports.
2. However, there were significant differences in subluxation between measurements of the unsupported affected shoulder and the unaffected shoulder and between measurements of the unsupported affected shoulder and the supported affected shoulder using both supportive devices.
Brooke et al. (1991) USA PCT No Score TPS=NA N=10
Intervention: Patients received two different shoulder supports by their occupational and physical therapists: Harris hemi-sling and the Bobath sling. Outcomes: Subluxation
1. Harris hemi-sling improved correction of the subluxation with mean vertical distance of 37.8mm vs. 38.5mm compared to the uninvolved shoulder while the mean difference between Harris and Bobath sling was 5.5(2.9) mm, in favour of the Harris sling.
2. For horizontal measurement, mean difference between Harris and Bobath slings was 8.3(6.3) mm, in favour of the

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 13 of 42 www.ebrsr.com
Harris sling.
Zorowitz et al. (1995) USA PCT No Score TPS=NA N=20
Intervention: Patients received shoulder support by an occupational therapist in the following order: (1) single-strap hemisling; (2) Rolyan humeral cuff sling; (3) Bobath roll; and (4) Cavalier support. Outcomes: Subluxation.
1. The single-strap hemisling corrected vertical displacement, while the Roylan and Bobath roll significantly reduced vertical displacement.
2. The Bobath roll and the Cavalier support produced a significant lateral displacement of the humeral head of the affected shoulder compared with the unaffected shoulder.
3. The Roylan humeral cuff sling significantly decreased the total subluxation asymmetry.
Hartwig et al. (2012) Germany RCT PEDro=7 TPS=NA N=41
Intervention: Patients admitted for inpatient stroke rehabilitation with caudal subluxation of the glenohumeral joint and hemiparesis of the upper extremity after ischemic injury were randomized to 2 groups. Patients in the intervention group received usual care and wore a functional orthosis (Neuro-Lux) for 10 hours each day designed to reduce subluxation. Patients in the control group received usual care only. Outcomes were assessed on days 14, 21 and 28. Outcomes: Shoulder-Hand Syndrome Score (SHSS); Discomfort; Compliance.
1. After adjusting for baseline differences, the mean SHSS was significantly lower by 3.1 points in the intervention compared to the control subjects.
2. Marginal or no discomfort from treatment with the orthosis was reported in 15 patients (75%), and only a single patient (5%) felt severe discomfort during the entire treatment.
3. Compliance with the use of the orthosis during the prescribed time was 89%.
11.7.3 Strapping/Taping the Hemiplegic Shoulder
Table 11.7.3 Strapping/Taping the Hemiplegic Shoulder
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Ancliffe (1992) Australia Pre-Post No Score TPS=Acute N=8
Intervention: Patients were assigned to receive strapping of the shoulder applied by one physiotherapist and changed every 3 to 4 days as needed to the hemiplegic side or to receive no strapping. Treatment began within 48 hours of admission to hospital. Outcomes: Pain-Free Period (PFP).
1. Patients in the strapping group experienced a significantly longer PFP than the patients who were not strapped (21 vs. 5.5 days).
2. However, all patients in the strapping group eventually did experience pain. The longest PFP was 25 days.
Hanger et al. (2000) New Zealand RCT PEDro=7 TPS=Acute N=98
Intervention: Patients were randomized to have their affected shoulder strapped for 6 weeks in addition to standard physiotherapy or to receive standard physiotherapy only 15 days following stroke. Outcomes: Visual Analogue Scale (VAS); Range of Motion (ROM); Functional Independence Measure (FIM); Motor Assessment Scale (MAS); Rankin Disability Index (RDI).
1. No significant differences were found between groups on any outcome measure.
2. There was a trend toward lower VAS score at 6 weeks and improved upper limb FIM score for the strapping group.
Griffin & Bernhardt Intervention: Patients at risk of developing 1. One person in the TS group developed
11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 14 of 42 www.ebrsr.com
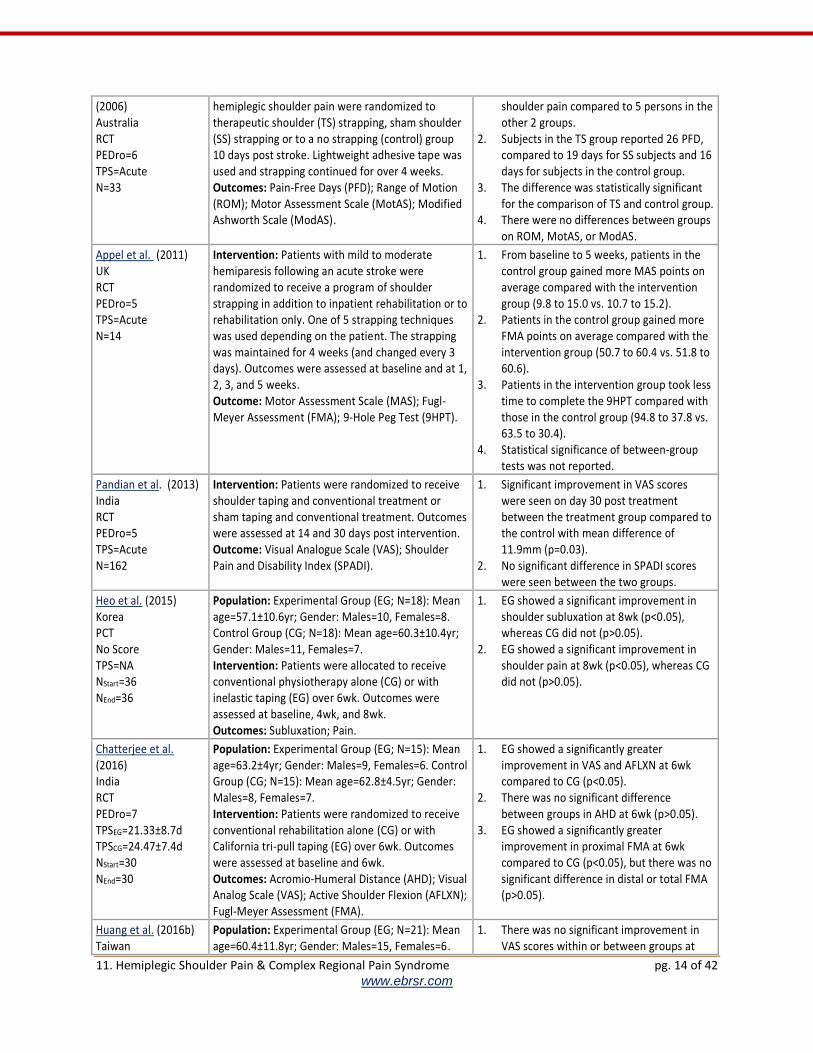
(2006) Australia RCT PEDro=6 TPS=Acute N=33
hemiplegic shoulder pain were randomized to therapeutic shoulder (TS) strapping, sham shoulder (SS) strapping or to a no strapping (control) group 10 days post stroke. Lightweight adhesive tape was used and strapping continued for over 4 weeks. Outcomes: Pain-Free Days (PFD); Range of Motion (ROM); Motor Assessment Scale (MotAS); Modified Ashworth Scale (ModAS).
shoulder pain compared to 5 persons in the other 2 groups.
2. Subjects in the TS group reported 26 PFD, compared to 19 days for SS subjects and 16 days for subjects in the control group.
3. The difference was statistically significant for the comparison of TS and control group.
4. There were no differences between groups on ROM, MotAS, or ModAS.
Appel et al. (2011) UK RCT PEDro=5 TPS=Acute N=14
Intervention: Patients with mild to moderate hemiparesis following an acute stroke were randomized to receive a program of shoulder strapping in addition to inpatient rehabilitation or to rehabilitation only. One of 5 strapping techniques was used depending on the patient. The strapping was maintained for 4 weeks (and changed every 3 days). Outcomes were assessed at baseline and at 1, 2, 3, and 5 weeks. Outcome: Motor Assessment Scale (MAS); Fugl-Meyer Assessment (FMA); 9-Hole Peg Test (9HPT).
1. From baseline to 5 weeks, patients in the control group gained more MAS points on average compared with the intervention group (9.8 to 15.0 vs. 10.7 to 15.2).
2. Patients in the control group gained more FMA points on average compared with the intervention group (50.7 to 60.4 vs. 51.8 to 60.6).
3. Patients in the intervention group took less time to complete the 9HPT compared with those in the control group (94.8 to 37.8 vs. 63.5 to 30.4).
4. Statistical significance of between-group tests was not reported.
Pandian et al. (2013) India RCT PEDro=5 TPS=Acute N=162
Intervention: Patients were randomized to receive shoulder taping and conventional treatment or sham taping and conventional treatment. Outcomes were assessed at 14 and 30 days post intervention. Outcome: Visual Analogue Scale (VAS); Shoulder Pain and Disability Index (SPADI).
1. Significant improvement in VAS scores were seen on day 30 post treatment between the treatment group compared to the control with mean difference of 11.9mm (p=0.03).
2. No significant difference in SPADI scores were seen between the two groups.
Heo et al. (2015) Korea PCT No Score TPS=NA NStart=36 NEnd=36
Population: Experimental Group (EG; N=18): Mean age=57.1±10.6yr; Gender: Males=10, Females=8. Control Group (CG; N=18): Mean age=60.3±10.4yr; Gender: Males=11, Females=7. Intervention: Patients were allocated to receive conventional physiotherapy alone (CG) or with inelastic taping (EG) over 6wk. Outcomes were assessed at baseline, 4wk, and 8wk. Outcomes: Subluxation; Pain.
1. EG showed a significant improvement in shoulder subluxation at 8wk (p<0.05), whereas CG did not (p>0.05).
2. EG showed a significant improvement in shoulder pain at 8wk (p<0.05), whereas CG did not (p>0.05).
Chatterjee et al. (2016) India RCT PEDro=7 TPSEG=21.33±8.7d TPSCG=24.47±7.4d NStart=30 NEnd=30
Population: Experimental Group (EG; N=15): Mean age=63.2±4yr; Gender: Males=9, Females=6. Control Group (CG; N=15): Mean age=62.8±4.5yr; Gender: Males=8, Females=7. Intervention: Patients were randomized to receive conventional rehabilitation alone (CG) or with California tri-pull taping (EG) over 6wk. Outcomes were assessed at baseline and 6wk. Outcomes: Acromio-Humeral Distance (AHD); Visual Analog Scale (VAS); Active Shoulder Flexion (AFLXN); Fugl-Meyer Assessment (FMA).
1. EG showed a significantly greater improvement in VAS and AFLXN at 6wk compared to CG (p<0.05).
2. There was no significant difference between groups in AHD at 6wk (p>0.05).
3. EG showed a significantly greater improvement in proximal FMA at 6wk compared to CG (p<0.05), but there was no significant difference in distal or total FMA (p>0.05).
Huang et al. (2016b) Taiwan
Population: Experimental Group (EG; N=21): Mean age=60.4±11.8yr; Gender: Males=15, Females=6.
1. There was no significant improvement in VAS scores within or between groups at

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 15 of 42 www.ebrsr.com
RCT PEDro=7 TPSEG=28.0±2.7d TPSCG=28.5±1.8d NStart=49 NEnd=44
Control Group (CG; N=23): Mean age=62.2±9.6yr; Gender: Males=15, Females=8. Intervention: Patients with were randomized to receive kinesiology taping (EG) or sham taping (CG). Both groups received conventional therapy 5d/wk over 3wk. Outcomes were assessed at baseline and 3wk. Outcomes: Visual Analog Scale (VAS); Fugl-Meyer Assessment-Upper Extremity (FMA-UE); Modified Barthel Index (mBI); Stroke-Specific Quality of Life (SSQOL); Modified Ashworth Scale (MAS); Range of Motion (ROM).
3wk (p≥0.17). 2. There was no significant difference
between groups at 3wk in MAS scores or shoulder ROM.
3. There was a significant improvement in both groups at 3wk in FMA-UE, mBI, and SSQOL (p<0.01), but there were no significant differences between groups (p≥0.56).
Kalichman et al. (2016) Israel Pre-Post No Score TPS=NA NStart=11 NEnd=11
Population: Mean age=60.6±8.9yr; Gender: Males=7, Females=4. Intervention: Patients received kinesiology taping and continued their usual rehabilitation protocol. Outcomes were assessed before and 24hr after taping. Outcomes: Visual Analogue Scale (VAS); Range of Motion (ROM); Fugl-Meyer Assessment (FMA); Box & Blocks Test (BBT); Subluxation.
1. After taping, there were no significant improvements in passive VAS (t=-1.103, p=0.299), active VAS (t=1.360, p=0.207), passive ROM (t=-1.827, p=0.101), active ROM (t=0.804, p=0.442), or subluxation (Z=0.000, p=1.000).
2. After taping, there were no significant improvements on FMA (z=-1.265, p=0.206) or BBT (z=-0.850, p=1.395).
Pillastrini et al. (2016) Italy RCT PEDro=8 TPSEG=3.1±2.2yr TPSCG=2.9±2.3yr NStart=32 NEnd=31
Population: Experimental Group (EG; N=16): Mean age=66±8yr; Gender: Males=13, Females=3. Control Group (CG; N=15): Mean age=66±11yr; Gender: Males=9, Females=6. Intervention: Patients were randomized to receive a standard rehabilitation program alone (CG) or with neuromuscular taping (EG). The program was comprised of 4 sessions of 45min over 4wk. Outcomes were assessed at 0wk, 4wk, and 8wk. Outcomes: Visual Analogue Scale (VAS); Modified Ashworth Scale (MAS); Range of Motion (ROM).
1. VAS scores significantly improved in the EG at 4wk and 8wk (p<0.05), while the CG showed no significant improvements. The EG had significantly greater improvement than the CG at 4wk and 8wk (p<0.05).
2. MAS scores significantly improved in the EG at 4wk and 8wk (p<0.05), while the CG showed no significant improvements. There was no significant difference between groups at either time (p>0.05).
3. ROM significantly improved in both the EG and CG at 4wk and 8wk (p<0.05). There was no significant difference between groups at either time (p>0.05).
11.7.4 Active Therapies for the Hemiplegic Shoulder Table 11.7.4 Active Therapies for the Hemiplegic Shoulder
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Inaba & Piorkowski (1972) USA RCT PEDro=7 TPS=NA N=33
Intervention: Patients with hemiplegia who experienced shoulder pain in the range of 0-90 degrees of flexion or abduction of the arm after stroke were treated. Patients were randomly assigned to 1 of 3 groups: Range of motion (ROM) exercises and positioning group; ROM exercises and ultrasound; or ROM exercises and mock ultrasound.
1. No significant differences between the groups were observed in measures of ROM.

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 16 of 42 www.ebrsr.com
All patients received ROM exercises for 4 weeks and given a minimum of 15 treatments. Outcomes: Range of Motion (ROM).
Kumar et al. (1990) USA RCT PEDro=5 TPS=NA N=28
Intervention: Patients were assigned to receive a rehabilitation program of range of motion by therapist (ROMT) once a day, 5 days a week; or a rehabilitation program with use of skate board once a day, 5 days a week; or a rehabilitation program with use of overhead pulley once a day, 5 days a week while an inpatient on a stroke rehabilitation unit. Outcomes: Pain; Subluxation.
1. Significant difference in the incidence of pain reported between the groups.
2. Shoulder pain was more common in the overhead pulley (63%) group than in the ROMT group (8%).
3. ROM was significantly reduced in those patients who developed shoulder pain when compared to those who did not develop shoulder pain motion abduction, forward flexion, internal rotation and external rotation.
4. Shoulder subluxation was found in 46% of all patients with no significant difference between treatment groups.
Partridge et al. (1990) UK RCT PEDro=5 TPS=NA N=65
Intervention: Patients were randomized to receive cryotherapy or Bobath therapy daily for five days and then after at the therapist’s discretion for a total of four additional weeks and assessed by a blinded investigator. Outcomes: Pain.
1. A greater proportion of patients treated by the Bobath method reported no pain or only occasional pain on exit of the study compared to those treated by the cryotherapy method.
Poduri et al. (1993) USA PCT No Score TPS=NA N=28
Intervention: Patients with stroke experiencing shoulder pain after completing outpatient therapy were studied. One group of patients received either a nonsteroidal anti-inflammatory drugs (Ibuprofen 400-800g tid, and Sulindac, 150 mg bid.) taken 30 to 60 minutes prior to occupational therapy. A second group of patients received only occupational therapy consisting of range of motion, active assistive and strengthening exercises and activities of daily living training. Outcomes: Pain; Flexion; Abduction; Functional recovery.
1. A significantly greater proportion of patients receiving the treatment drug prior to therapy experienced pain relief.
2. Flexion, abduction and functional recovery were significantly greater in those patients who were taking the non-steriodal anti-inflammatory drug before therapy.
Lynch et al. (2005) USA RCT PEDro=6 TPS=NA N=35
Intervention: Patients with significant upper motor impairment were randomized to a control group (n=16), which received self-range of motion exercises under the supervision of a physiotherapist or to the experimental group (n=19) of continuous passive motion treatments with the use of a device (25 min sessions, 5 days/week until discharge). All patients received rehabilitation therapies for 3.5 hours per day. Outcomes: Modified Ashworth Scale (MAS); Fugl-Meyer Assessment (FMA); Joint stability.
1. There were no between group differences in changed scores between groups on any of the outcome measures.
Hafsteinsdottir et al. (2007) Netherlands PCT TPS=NA NStart=326
Population: Experimental Group (EG; N=223): Mean age=68±13yr; Gender: Males=122, Females=101. Control Group (N=101): Mean age=72±11yr; Gender: Males=51, Females=50. Intervention: Patients received either Bobath therapy (EG) or standard therapy (CG) in hospital.
1. There was no significant differences between groups in VAS score at discharge, 6mo, or 12mo.

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 17 of 42 www.ebrsr.com
NEnd=286 Patients receiving Bobath therapy continued receiving it after discharge. Outcomes were assessed at baseline (N=326), discharge (N=316), 6mo (N=299), and 12mo (N=286). Outcomes: Visual Analogue Scale (VAS).
You et al. (2014) Korea PCT No Score TPS=NA NStart=45 NEnd=41
Population: Normal development therapy (Group 1; N=14): Mean age=58±74yr; Gender: unspecified. Stretching exercise therapy (Group 2; N=13): Mean age=57.8 ±8.1yr; Gender: unspecified. Stretching and joint stabilization exercise therapy (Group 3; N=14) Mean age=58.7±6.6 yr; Gender: unspecified. Intervention: 8 weeks of exercise therapy; Patients were allocated to one of three groups. All groups received normal development therapy for 1.5hr 3x/wk and occupational therapy for 1hr 5x/wk, in addition to 30min of their specific exercise therapy program. Outcomes were assessed at baseline, 4wk, and 8wk. Outcomes: Motor Assessment Scale (MAS).
1. In all three groups, there was a statistically significant improvement indicated by repeated measures over time (p<0.05).
2. There was no statistically significant between-group difference for groups 1 and 2 on MAS.
3. There were statistically significant differences between groups 1 and 3 on MAS; group 3 demonstrated a greater improvement (p<0.05).
Jeon et al. (2016) Korea RCT PEDro=5 TPSEG=15.8±8.9mo TPSCG=14.9±7.6mo NStart=12 NEnd=12
Population: Experimental Group (EG; N=6): Mean age=58.0±13.6; Gender: Males=3, Females=3. Control Group (CG; N=6): Mean age=50.5±8.9yr; Gender: Males=4, Females=2. Intervention: Patients were randomized to receive therapy with (EG) or without (CG) the ‘monkey chair and band’ system. Therapy was delivered in 30min sessions 3x/wk over 12wk. Outcomes were at baseline, 4wk, 8wk, and 12wk. Outcomes: Visual Analogue Score (VAS); Range of Motion (ROM); Modified Motor Assessment Scale (MMAS).
1. VAS score significantly decreased in EG by 12wk (p<0.05). There was no significant VAS reduction in CG.
2. ROM significantly increased in EG by 12wk for flexion, abduction, and adduction (p<0.05), but not extension. There was no significant ROM improvement in CG.
4. MMAS score significantly increased in EG by 12wk for upper arm (p<0.01), hand movement (p<0.01), and walking (p<0.05). There was no significant MMAS improvement in CG.
11.7.5 Electrical Stimulation of the Hemiplegic Shoulder Table 11.7.5.1 Surface Electrical Stimulation of the Hemiplegic Shoulder
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Baker & Parker (1986) USA RCT PEDro=4 TPS=Chronic N=63
Intervention: Patients with a minimum of 5mm of shoulder subluxation in their involved upper extremity were randomized to a treatment or control group. Patients in the treatment group received neuromuscular electrical stimulation (NMES) for 5 weeks, while patients in the control group used conventional hemi-slings or wheelchair arm supports. Outcomes: Subluxation; Pain.
1. At six weeks, the mean subluxation of the study group was significantly less compared to the control (8.6 vs. 13.3).
2. Three-month radiographs demonstrated that patients in the treatment group had lost an average of 1-2 mm, which had been achieved during the study period.
3. The authors did not demonstrate a causal relationship between subluxation and shoulder pain.
Leandri et al. (1990) Intervention: Patients with chronic hemiplegic 1. Significant improvements in PROM were

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 18 of 42 www.ebrsr.com
Italy RCT PEDro=5 TPS=Chronic N=60
shoulder pain were randomized to one of three groups. Group 1 received high intensity TENS plus basic physical treatment. Group 2 received low intensity TENS plus basic physical treatment. Group 3 received sham intensity TENS plus basic physical treatment. Outcomes: Passive Range of Motion (PROM).
recorded for group 1 but not for the other groups.
2. No between-group comparisons were made.
Faghri et al. (1994) USA RCT PEDro=4 TPS=NA N=26
Intervention: Patients were randomized to receive either functional electrical stimulation (FES) in addition to conventional therapy or conventional therapy alone. FES targeted two flaccid/paralyzed shoulder muscles (supraspinatus and posterior deltoid), which were induced to contract repetitively up to 6 hours daily for 6 days. Outcomes: Arm function; Arm tone; EMG activity.
1. After treatment, the FES group showed a significant increase in arm function, tone and EMG activity compared to control patients.
Chantraine et al. (1999) Switzerland PCT No Score TPS=Acute N=115
Intervention: Patients were assigned to receive functional electrical stimulation (FES) in addition to traditional Bobath treatment for 5 weeks or traditional Bobath treatment alone for 5 weeks. Outcomes: Motor recovery; Pain; Subluxation.
1. Significant motor recovery was noted in favour of FES treatment at 3 months and was maintained at 24 months.
2. Significant reduction in pain in favour of FES treatment at 3 months and was maintained at 24 months.
3. Significant reduction in shoulder subluxation in favour of FES treatment was noted at 3 months and maintained at 24 months.
Kobayashi et al. (1999) Japan RCT PEDro=5 TPS=Chronic N=17
Intervention: Patients with chronic shoulder subluxation were randomized to receive therapeutic electrical stimulation (TES) for 15 minutes twice a day to either the supraspinatus muscle (group 1) or middle deltoid muscle (group 2) in conjunction with conventional therapy, or to receive conventional therapy only (group 3). Outcomes: Subluxation; Abduction force.
1. Difference in subluxation in group 1 and group 2 was significantly greater than that of group 3 under the stress test.
2. Mean abduction force tended to increase in group 1 and was significantly greater in group 2.
Linn et al. (1999) Scotland RCT PEDro=6 TPS=Acute N=40
Intervention: Patients were randomly assigned to a control or treatment group for 4wk. Patients in the treatment group received electrical stimulation (ES) 4 times daily for 30-60 minutes. Both groups received daily occupational and physical therapy. Assessments were carried out at 4 and 12 weeks after stroke. Outcomes: Pain; Subluxation.
1. The treatment group had significantly less subluxation and pain after the treatment period.
2. At the end of the follow-up period, there were no significant differences between the two groups.
Wang et al. (2000) Taiwan RCT PEDro=5 TPS=NA N=32
Intervention: Patients with hemiplegia were assigned to one of two groups based on the duration of hemiplegia: short or long. Each group was randomly assigned to either a control subgroup or an experimental subgroup. The experimental subgroups were treated in a type A-B-A study design, which consisted of an FES training (A), routine therapy or regular daily activity without FES training (B), and another FES training (A). Each period lasted for 6 wk. FES training consisted of five sessions per week.
1. The experimental subgroup of short duration showed significant improvements in reducing subluxation as indicated by x-ray compared with the control subgroup of short duration after the first FES treatment.
2. The same effect was not shown for the experimental subgroup of long duration. The second FES treatment program only resulted in an insignificant change of shoulder subluxation for both the short- and long-duration subgroups.
11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 19 of 42 www.ebrsr.com
Outcomes: Subluxation.
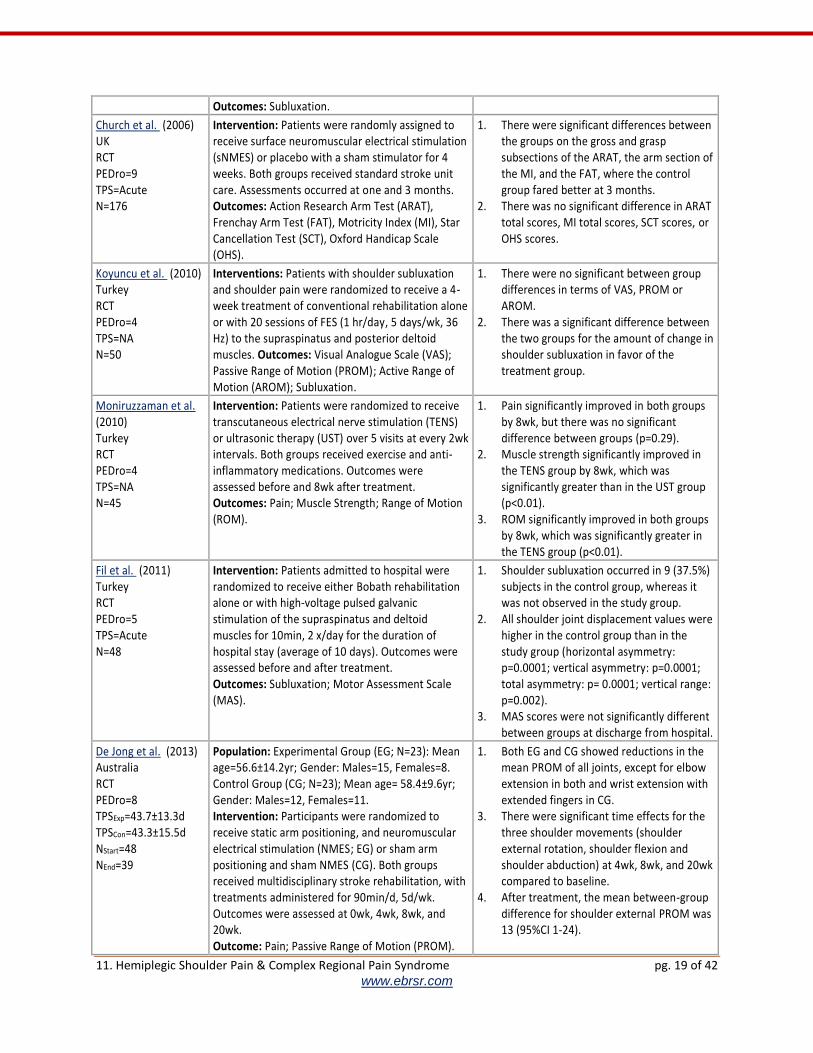
Church et al. (2006) UK RCT PEDro=9 TPS=Acute N=176
Intervention: Patients were randomly assigned to receive surface neuromuscular electrical stimulation (sNMES) or placebo with a sham stimulator for 4 weeks. Both groups received standard stroke unit care. Assessments occurred at one and 3 months. Outcomes: Action Research Arm Test (ARAT), Frenchay Arm Test (FAT), Motricity Index (MI), Star Cancellation Test (SCT), Oxford Handicap Scale (OHS).
1. There were significant differences between the groups on the gross and grasp subsections of the ARAT, the arm section of the MI, and the FAT, where the control group fared better at 3 months.
2. There was no significant difference in ARAT total scores, MI total scores, SCT scores, or OHS scores.
Koyuncu et al. (2010) Turkey RCT PEDro=4 TPS=NA N=50
Interventions: Patients with shoulder subluxation and shoulder pain were randomized to receive a 4-week treatment of conventional rehabilitation alone or with 20 sessions of FES (1 hr/day, 5 days/wk, 36 Hz) to the supraspinatus and posterior deltoid muscles. Outcomes: Visual Analogue Scale (VAS); Passive Range of Motion (PROM); Active Range of Motion (AROM); Subluxation.
1. There were no significant between group differences in terms of VAS, PROM or AROM.
2. There was a significant difference between the two groups for the amount of change in shoulder subluxation in favor of the treatment group.
Moniruzzaman et al. (2010) Turkey RCT PEDro=4 TPS=NA N=45
Intervention: Patients were randomized to receive transcutaneous electrical nerve stimulation (TENS) or ultrasonic therapy (UST) over 5 visits at every 2wk intervals. Both groups received exercise and anti-inflammatory medications. Outcomes were assessed before and 8wk after treatment. Outcomes: Pain; Muscle Strength; Range of Motion (ROM).
1. Pain significantly improved in both groups by 8wk, but there was no significant difference between groups (p=0.29).
2. Muscle strength significantly improved in the TENS group by 8wk, which was significantly greater than in the UST group (p<0.01).
3. ROM significantly improved in both groups by 8wk, which was significantly greater in the TENS group (p<0.01).
Fil et al. (2011) Turkey RCT PEDro=5 TPS=Acute N=48
Intervention: Patients admitted to hospital were randomized to receive either Bobath rehabilitation alone or with high-voltage pulsed galvanic stimulation of the supraspinatus and deltoid muscles for 10min, 2 x/day for the duration of hospital stay (average of 10 days). Outcomes were assessed before and after treatment. Outcomes: Subluxation; Motor Assessment Scale (MAS).
1. Shoulder subluxation occurred in 9 (37.5%) subjects in the control group, whereas it was not observed in the study group.
2. All shoulder joint displacement values were higher in the control group than in the study group (horizontal asymmetry: p=0.0001; vertical asymmetry: p=0.0001; total asymmetry: p= 0.0001; vertical range: p=0.002).
3. MAS scores were not significantly different between groups at discharge from hospital.
De Jong et al. (2013) Australia RCT PEDro=8 TPSExp=43.7±13.3d TPSCon=43.3±15.5d NStart=48 NEnd=39
Population: Experimental Group (EG; N=23): Mean age=56.6±14.2yr; Gender: Males=15, Females=8. Control Group (CG; N=23); Mean age= 58.4±9.6yr; Gender: Males=12, Females=11. Intervention: Participants were randomized to receive static arm positioning, and neuromuscular electrical stimulation (NMES; EG) or sham arm positioning and sham NMES (CG). Both groups received multidisciplinary stroke rehabilitation, with treatments administered for 90min/d, 5d/wk. Outcomes were assessed at 0wk, 4wk, 8wk, and 20wk. Outcome: Pain; Passive Range of Motion (PROM).
1. Both EG and CG showed reductions in the mean PROM of all joints, except for elbow extension in both and wrist extension with extended fingers in CG.
3. There were significant time effects for the three shoulder movements (shoulder external rotation, shoulder flexion and shoulder abduction) at 4wk, 8wk, and 20wk compared to baseline.
4. After treatment, the mean between-group difference for shoulder external PROM was 13 (95%CI 1-24).

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 20 of 42 www.ebrsr.com
Kim et al. (2013) Korea Pre-Post No Score TPS=24.6±11.7mo N=57
Population: Mean age=55.4±13.2yr; Gender: Males=33, Females=24. Intervention: Patients received radial extracorporeal shockwave therapy (8Hz) in 5 sessions of 15min over 2wk. Outcomes were assessed after each session and weekly for 6wk after treatment. Outcomes: Visual Analogue Scale (VAS); Modified Ashworth Scale (MAS); Range of Motion (ROM).
1. Patients showed significant improvements from baseline for VAS, MAS, and ROM at every time point following the second session (p<0.0001).
2. Improvements were most significant after the 4wk follow-up for VAS (B=1.34, p<0.0001), MAS (B=0.414, p<0.0001), and ROM (B=-11.523, p<0.0001).
Manigandan et al. (2014) PCT No Score TPS=NA N=24
Population: Experimental Group 1 (EG1; N=12): Mean age=51.8±7.6yr; Gender: Males=8, Females=4. Experimental Group 2 (EG2; N=12): Mean age=50.2±8.6yr; Gender: Males=8, Females=4. Intervention: Patients were allocated to receive surface electrical stimulation to the deltoid and supraspinatus only (EG1) or the bicep as well (EG2). Both groups received stimulation (300ms, 30Hz) in 30-60min sessions 2x/wk over 5wk, along with standard rehabilitation. Outcomes were assessed before and after treatment. Outcomes: Pain-Free Range of Motion (PFROM); Subluxation.
1. Both groups showed significant improvements over time in PFROM (p=0.001) and subluxation (p<0.001).
2. EG2 showed significantly greater improvement in PFROM (p=0.001) and subluxation (p<0.001) than EG1.
Suriya-Amarit et al. (2014) Thailand RCT PEDro=6 TPS=NA NStart=30 NEnd=30
Population: Experimental Group (EG; N=15): Mean age=65.87±9.35yr; Gender: Males=6, Females=9. Control Group (CG; N=15): Mean age=67.13±10.84yr; Gender: Males=6, Females=9. Intervention: Patients were randomized to receive interferential current stimulation (EG) or sham stimulation (CG). Outcomes: Pain; Passive Range of Motion (PROM).
3. For pain during the most painful movement, participants reported a greater reduction in pain intensity in EG than CG (p<0.05).
4. After treatment, EG had greater mean change in pain-free PROM for flexion (p<0.01), abduction (p<0.05), internal rotation (p<0.05) and external rotation (p<0.05) compared to CG.
Kim et al. (2016) Korea RCT PEDro=6 TPSEG=28.8±33mo TPSCG=22.2±18mo NStart=40 NEnd=34
Population: Experimental Group (EG; N=17): Mean age=65.88±8.27yr; Gender: Males=7, Females=10. Control Group (CG; N=17): Mean Age=66.11±15.79yr; Gender: Males=10, Females=7. Intervention: Patients were randomized to receive radial extracorporeal shock wave therapy (EG) or control (CG). Treatment was administered 4x/wk over 2wk. Outcomes were assessed at baseline, 2wk, 4wk, and 6wk. Outcomes: Visual Analog Scale (VAS); Constant-Murley Scale (CS).
1. EG had a significantly greater improvement in VAS compare to CG at 2wk (p=0.036), 4wk (p=0.009), and 6wk (p=0.016).
2. There was no significant difference in CS score between groups at any time points (p≥0.231).
Table 11.7.5.2 Intramuscular Electrical Stimulation
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 21 of 42 www.ebrsr.com
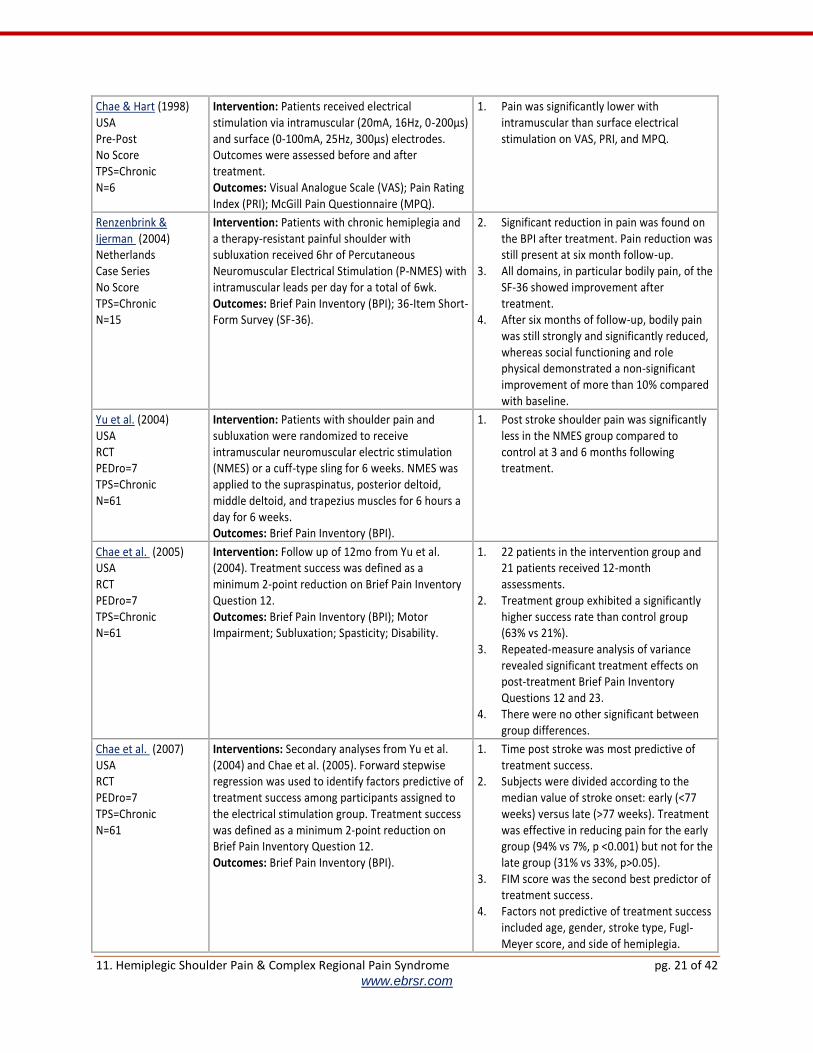
Chae & Hart (1998) USA Pre-Post No Score TPS=Chronic N=6
Intervention: Patients received electrical stimulation via intramuscular (20mA, 16Hz, 0-200µs) and surface (0-100mA, 25Hz, 300µs) electrodes. Outcomes were assessed before and after treatment. Outcomes: Visual Analogue Scale (VAS); Pain Rating Index (PRI); McGill Pain Questionnaire (MPQ).
1. Pain was significantly lower with intramuscular than surface electrical stimulation on VAS, PRI, and MPQ.
Renzenbrink & Ijerman (2004) Netherlands Case Series No Score TPS=Chronic N=15
Intervention: Patients with chronic hemiplegia and a therapy-resistant painful shoulder with subluxation received 6hr of Percutaneous Neuromuscular Electrical Stimulation (P-NMES) with intramuscular leads per day for a total of 6wk. Outcomes: Brief Pain Inventory (BPI); 36-Item Short-Form Survey (SF-36).
2. Significant reduction in pain was found on the BPI after treatment. Pain reduction was still present at six month follow-up.
3. All domains, in particular bodily pain, of the SF-36 showed improvement after treatment.
4. After six months of follow-up, bodily pain was still strongly and significantly reduced, whereas social functioning and role physical demonstrated a non-significant improvement of more than 10% compared with baseline.
Yu et al. (2004) USA RCT PEDro=7 TPS=Chronic N=61
Intervention: Patients with shoulder pain and subluxation were randomized to receive intramuscular neuromuscular electric stimulation (NMES) or a cuff-type sling for 6 weeks. NMES was applied to the supraspinatus, posterior deltoid, middle deltoid, and trapezius muscles for 6 hours a day for 6 weeks. Outcomes: Brief Pain Inventory (BPI).
1. Post stroke shoulder pain was significantly less in the NMES group compared to control at 3 and 6 months following treatment.
Chae et al. (2005) USA RCT PEDro=7 TPS=Chronic N=61
Intervention: Follow up of 12mo from Yu et al. (2004). Treatment success was defined as a minimum 2-point reduction on Brief Pain Inventory Question 12. Outcomes: Brief Pain Inventory (BPI); Motor Impairment; Subluxation; Spasticity; Disability.
1. 22 patients in the intervention group and 21 patients received 12-month assessments.
2. Treatment group exhibited a significantly higher success rate than control group (63% vs 21%).
3. Repeated-measure analysis of variance revealed significant treatment effects on post-treatment Brief Pain Inventory Questions 12 and 23.
4. There were no other significant between group differences.
Chae et al. (2007) USA RCT PEDro=7 TPS=Chronic N=61
Interventions: Secondary analyses from Yu et al. (2004) and Chae et al. (2005). Forward stepwise regression was used to identify factors predictive of treatment success among participants assigned to the electrical stimulation group. Treatment success was defined as a minimum 2-point reduction on Brief Pain Inventory Question 12. Outcomes: Brief Pain Inventory (BPI).
1. Time post stroke was most predictive of treatment success.
2. Subjects were divided according to the median value of stroke onset: early (<77 weeks) versus late (>77 weeks). Treatment was effective in reducing pain for the early group (94% vs 7%, p <0.001) but not for the late group (31% vs 33%, p>0.05).
3. FIM score was the second best predictor of treatment success.
4. Factors not predictive of treatment success included age, gender, stroke type, Fugl-Meyer score, and side of hemiplegia.

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 22 of 42 www.ebrsr.com
Chae et al. (2013) USA Case Series No Score TPS=NA N=8
Intervention: Patients had a single electrode placed between the motor points of the middle and posterior deltoid muscles. Two monopolar needles were used to guide placement. The Rehabilicare NT2000 external stimulator was used to provide biphase waveform with current amplitude of 20mA at 12 Hz on the middle and posterior deltoids. Participants received therapy for 6hr/d over 3wk. Outcomes were measured at 4 and 12 weeks after treatment. Outcomes: Pain.
1. At 4wk, all participants reported a 2-point pain reduction.
2. At 12wk, 6 out of 8 participants maintained pain reduction.
Wilson et al. (2014) USA RCT PEDro=9 TPSPNS=2.6d TPSUC=2.3d NStart=25
NEnd=21
Population: Experimental Group (EG; N=13): Mean age=54yr; Gender: Males=53.8%, Females=46.2%. Control Group (CG; N=12): Mean age=55yr; Gender: Males=41.7%, Females=58.3%. Intervention: Participants were randomized to receive peripheral nerve stimulation (EG) or usual care (CG). PNS involved 6 hours of stimulation daily for 3 weeks, in either single or divided doses, for a total of 126 hours over 4 weeks. UC involved 8 hours of outpatient physiotherapy over 4 weeks from a licensed therapist along with prescribed daily home exercises. Outcome assessments were performed before and after treatment, and at 6- and 12-week follow-ups. Outcomes: Brief Pain inventory (BPI).
1. There was a significantly greater reduction in pain intensity on BPI for the EG compared to the CG over time (2.9 at 10 weeks and 3.1 at 16 weeks).
2. There were significant reductions in pain interference on BPI over time for both groups, but these changes were not significant between groups over time.
11.7.6 Botulinum Toxin Injections for the Hemiplegic Shoulder Table 11.7.6 Botulinum Toxin for Hemiplegic Shoulder
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Hecht (1995) USA Pre-Post No Score TPS=NA N=20
Intervention: Patients received botulinum toxin block to the subscapular and pectoralis major musculature. Outcomes: Clinical benefit; Range of Motion (ROM).
1. 85% benefited from subscapularis block, 55% benefited from pectoralis major block, and 45% showed improved active ROM.
Bhakta et al. (1996) UK Pre-Post No Score TPS=NA N=17
Intervention: Patients received a single course of intramuscular botulinum toxin to biceps brachii, flexor digitorum profundus, flexor digitorum superficialis, and flexor carpi ulnaris. Outcomes: Pain.
1. Shoulder pain improved in 6 of 9 patients with shoulder pain.
Yelnik et al. (2007) France RCT PEDro=7
Intervention: Patients with hemiplegia and upper limb spasticity were randomly assigned to receive either one injection of 500U botulinum toxin A (BTA; N=10) or placebo (N=10) in the subcapularis muscle.
1. There was a significant decrease in pain on VAS for BTA over placebo (-6 vs -1.5, p=0.025).
2. There was significant improvement in

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 23 of 42 www.ebrsr.com
TPS=NA N=20
Non-standardized physical therapy was given to both groups on weekdays. Outcomes were assessed at baseline and 4wk. Outcome: Visual Analogue Scale (VAS); Movements.
lateral rotation for BTA over placebo (12.5% vs -2.5%, p=0.018), but not for abduction (70% vs 72.5%, p>0.05).
Kong et al. (2007) Singapore RCT PEDro=8 TPS>3mo N=17
Intervention: Patients recruited from an outpatient clinic with spastic shoulder pain were randomized to receive a single injection of 500U Dysport (N=8) or saline placebo (N=9) injected into the pectoralis major and biceps brachii. Outcomes were assessed at baseline, 4wk, 8wk, and 12wk. Outcome: Visual Analogue Scale (VAS); Ashworth Scale (AS).
1. At week 4, there was no significant difference in the resolution of shoulder pain between the groups.
2. At week 4, the Dysport group showed significantly greater improvements in median shoulder adductor and elbow flexor AS scores than the placebo group, but not at weeks 8 and 12.
Marco et al. (2007) Spain RCT PEDro=8 TPS>3mo N=31
Intervention: Patients with moderate to severe spastic shoulder pain admitted for inpatient rehabilitation were randomized to receive transcutaneous electric stimulation for 6wk with either 500U Dysport (N=16) or placebo (N=15) injected into 4 sites of the pectoralis major muscle of the paretic side under EMG guidance. Outcomes were assessed at baseline, 1wk, 1mo, 3mo, and 6mo. Outcome: Visual Analogue Scale (VAS); Modified Ashworth Scale (MAS); Range of Motion (ROM).
1. Pain on VAS was reduced significantly in the Dysport group than placebo group at 6 months (76.4 to 30.1 vs 70.1 to 48.3, p=0.035).
2. External ROM increased significantly more in the Dysport group than placebo group at 6 months (7.9 to 38.9 vs 6.7 to 19.3, p=0.041).
3. There were no other statistically significant differences between groups.
de Boer et al. (2008) Netherlands RCT PEDro=6 TPS=NA N=22
Intervention: Patients with spastic hemiplegia, substantial shoulder pain, and reduced external rotation of the humerus were randomized to receive a single injection of either botulinum toxin A (100U) or placebo applied to the subscapularis muscle at two locations. Assessments were carried out at baseline, 6 weeks, and 12 weeks. Outcomes: Visual Analogue Scale (VAS); Goniometry.
1. Pain on VAS significantly decreased over time in both groups, but there was no between-group difference.
2. External rotation improved significantly over time in both groups, but there was no between-group difference.
Pedreira et al. (2008) Brazil Pre-Post No Score TPS=NA N=15
Intervention: Patients with spastic hemiparesis received a single injection of 280U botulinum toxin A. Assessments were performed at 1, 2 and 4 months after treatment. Outcomes: Visual Analogue Scale (VAS); Goniometry.
1. Mean VAS was reduced non-significantly over the study period.
2. There was a significant improvement in flexion and rotation.
Ashford & Turner-Stokes (2009) UK Pre-Post No Score TPS=Chronic N=16
Intervention: Patients received an individualized dose of Dysport (100-500U) injection and concurrent therapy for spasticity of the shoulder girdle or proximal upper limb. Outcomes: Goal Attainment Scaling (GAS); Modified Ashworth Scale (MAS); Numerical Rating Scale (NRS); Passive function.
1. At 16 weeks post injection, significant improvements were identified on MAS (p<0.001) and passive function (p=0.002), but not NRS (p=0.052).
2. GAS scores improved in all but one subject, with goals either achieved or overachieved.
Castiglione et al. (2011) Italy Pre-Post No Score
Population: Mean age=63.8±5.1yr; Gender: Males=4, Females=1. Interventions: Patients received an intraarticular injection of 100U botulinum toxin A. Outcomes were assessed at baseline, 2wk, and 8wk..
1. At 2wk and 8wk, VAS scores were significantly improved at rest (p=0.001) and during passive abduction (p<0.001).
2. There were no significant differences in VAS scores between 2wk and 8wk.
11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 24 of 42 www.ebrsr.com
TPS=3.8±0.8mo N=5
Outcomes: Visual Analogue Scale (VAS).
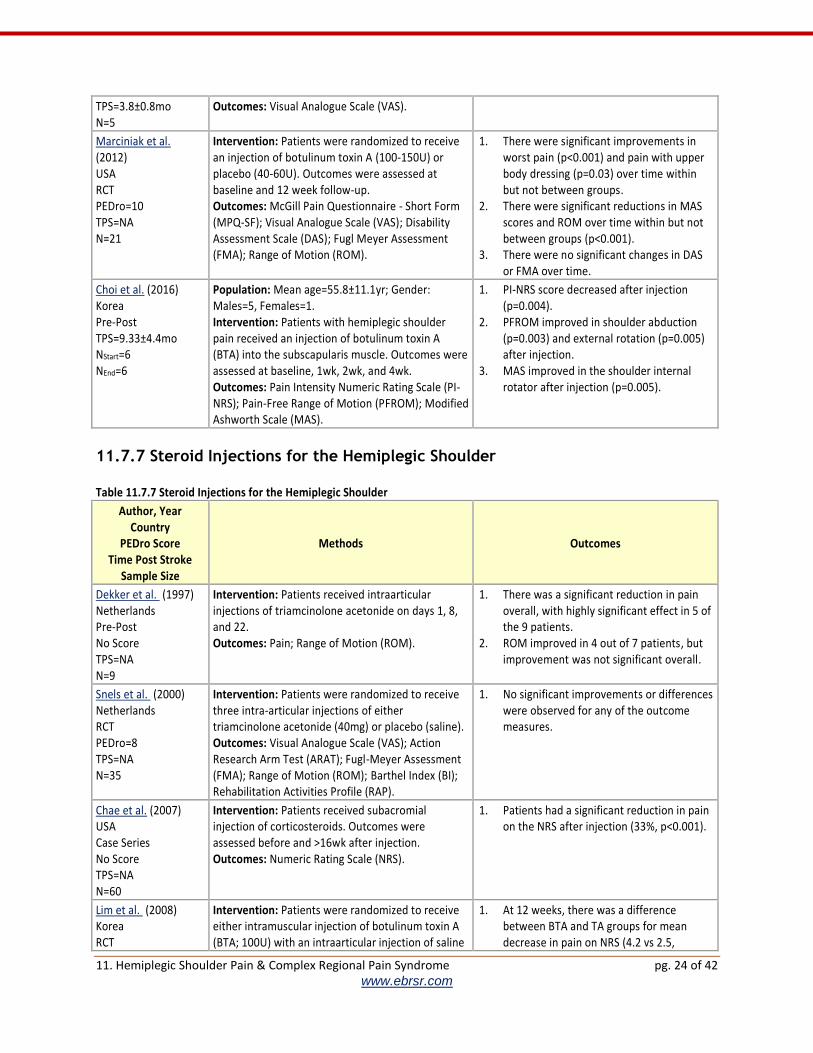
Marciniak et al. (2012) USA RCT PEDro=10 TPS=NA N=21
Intervention: Patients were randomized to receive an injection of botulinum toxin A (100-150U) or placebo (40-60U). Outcomes were assessed at baseline and 12 week follow-up. Outcomes: McGill Pain Questionnaire - Short Form (MPQ-SF); Visual Analogue Scale (VAS); Disability Assessment Scale (DAS); Fugl Meyer Assessment (FMA); Range of Motion (ROM).
1. There were significant improvements in worst pain (p<0.001) and pain with upper body dressing (p=0.03) over time within but not between groups.
2. There were significant reductions in MAS scores and ROM over time within but not between groups (p<0.001).
3. There were no significant changes in DAS or FMA over time.
Choi et al. (2016) Korea Pre-Post TPS=9.33±4.4mo NStart=6 NEnd=6
Population: Mean age=55.8±11.1yr; Gender: Males=5, Females=1. Intervention: Patients with hemiplegic shoulder pain received an injection of botulinum toxin A (BTA) into the subscapularis muscle. Outcomes were assessed at baseline, 1wk, 2wk, and 4wk. Outcomes: Pain Intensity Numeric Rating Scale (PI-NRS); Pain-Free Range of Motion (PFROM); Modified Ashworth Scale (MAS).
1. PI-NRS score decreased after injection (p=0.004).
2. PFROM improved in shoulder abduction (p=0.003) and external rotation (p=0.005) after injection.
3. MAS improved in the shoulder internal rotator after injection (p=0.005).
11.7.7 Steroid Injections for the Hemiplegic Shoulder Table 11.7.7 Steroid Injections for the Hemiplegic Shoulder
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Dekker et al. (1997) Netherlands Pre-Post No Score TPS=NA N=9
Intervention: Patients received intraarticular injections of triamcinolone acetonide on days 1, 8, and 22. Outcomes: Pain; Range of Motion (ROM).
1. There was a significant reduction in pain overall, with highly significant effect in 5 of the 9 patients.
2. ROM improved in 4 out of 7 patients, but improvement was not significant overall.
Snels et al. (2000) Netherlands RCT PEDro=8 TPS=NA N=35
Intervention: Patients were randomized to receive three intra-articular injections of either triamcinolone acetonide (40mg) or placebo (saline). Outcomes: Visual Analogue Scale (VAS); Action Research Arm Test (ARAT); Fugl-Meyer Assessment (FMA); Range of Motion (ROM); Barthel Index (BI); Rehabilitation Activities Profile (RAP).
1. No significant improvements or differences were observed for any of the outcome measures.
Chae et al. (2007) USA Case Series No Score TPS=NA N=60
Intervention: Patients received subacromial injection of corticosteroids. Outcomes were assessed before and >16wk after injection. Outcomes: Numeric Rating Scale (NRS).
1. Patients had a significant reduction in pain on the NRS after injection (33%, p<0.001).
Lim et al. (2008) Korea RCT
Intervention: Patients were randomized to receive either intramuscular injection of botulinum toxin A (BTA; 100U) with an intraarticular injection of saline
1. At 12 weeks, there was a difference between BTA and TA groups for mean decrease in pain on NRS (4.2 vs 2.5,

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 25 of 42 www.ebrsr.com
PEDro=9 TPS=NA N=29
to the painful shoulder joint (N=16), or an intraarticular injection of triamcinolone acetonide (TA; 40mg) and an intramuscular injection of normal saline (N=13). Outcomes were assessed at baseline and 2, 6, and 12 weeks. Outcomes: Numeric Rating Scale (NRS); Global Rating Scale (GRS); Range of Motion (ROM); Fugl-Meyer Assessment (FMA); Modified Ashworth Scale (MAS).
p=0.051) and mean improvement in overall ROM (82.9° vs 51.8°, p=0.059).
2. There were no significant differences between groups on GRS, FMA, or MAS.
Chae & Jedlicka (2009) USA Pre-Post No Score TPS=NA N=10
Intervention: Patients received a single subacromial injection of triamcinolone acetonide (60mg) and lidocaine (2.5mL). Outcomes were assessed at baseline, weekly for the first 4 weeks, and then at 8 and 12 weeks. Outcomes: Brief Pain Inventory (BPI).
1. Mean BP1 Q2 score significantly decreased from baseline to 12 weeks (7.8 to 3.8, p<0.05).
2. Greatest decrease on BPI Q12 was seen at the end of 2 weeks (p<0.05).
Lakse et al. (2009) Turkey RCT PEDro=4 TPS=NA N=38
Intervention: Patients received conventional therapy including 5 sessions of transcutaneous electrical stimulation over 3 weeks. Patients were then randomized to receive no additional treatment or a single injection of triamcinolone acetonide. Outcomes were assessed at baseline, 1 week, and 4 weeks. Outcomes: Verbal Analogue Scale (VAS); Passive Range of Motion (PROM); Modified Ashworth Scale (MAS); Barthel Index (BI); Brunnstrom Scale (BS).
1. Patients who received steroid injection had significantly greater improvement in pain on VAS (at rest, at night, and during activity) and shoulder ROM.
2. There were no significant differences between groups on any of the secondary outcomes (MAS, BI, BS).
Yasar et al. (2011) Turkey RCT PEDro=5 TPS=Chronic N=26
Intervention: Patients were randomized to receive a single injection of intraarticular triamcinolone acetonide (40mg; N=11) or suprascapular nerve block (SSNB; N=15). Outcomes were assessed at baseline, 1 hour, 1 week, and 1 month. Outcomes: Visual Analogue Scale (VAS).
1. Pain on VAS was reduced in both groups over the study period.
2. There were no significant differences in VAS scores between groups.
Rah et al. (2012) Korea RCT PEDro=9 TPS=NA N=58
Intervention: Patients were randomly assigned to receive a single ultrasound-guided subacromial injection with triamcinolone acetonide (40mg; N=29), or lidocaine (N=29). Both groups participated in an exercise program. Outcomes were assessed at 2, 4, and 8 weeks. Outcomes: Visual Analogue Scale (VAS); Modified Barthel Index (mBI); Shoulder Disability Questionnaire (SDQ); Range of Motion (ROM).
1. There was significantly greater improvement favouring the treatment group on VAS scores (day and night), SDQ scores, and ROM (flexion, external rotation, and internal rotation).
Baykal et al. (2013) Turkey RCT PEDro=4 TPS=NA Nstart=30 Nend=30
Population: Experimental Group (EG; N=15): Mean age=62.3±7.5yr; Gender: Males7, Females=8. Control Group (CG; N=15): Mean age=62.0±8.9yr; Gender: Males=6, Female=9. Intervention: Patients were randomized to receive physiotherapy alone (CG) or with subacromial steroid injection (EG). Outcomes were assessed at baseline, 1wk, and 7wk. Outcomes: Range of Motion (ROM); Visual Analog Scale (VAS).
1. In the EG, there were significant improvements in all directions of shoulder ROM between all time periods (p<0.05).
2. In the CG, there were significant improvements all directions of shoulder ROM between all time periods (p<0.05), except for flexion (only 0-1wk).
3. In the EG and CG, there were significant reductions in resting, activity, and night VAS values between all time periods (p<0.05).

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 26 of 42 www.ebrsr.com
4. There were no significant differences between groups (p>0.05).
Dogan et al. (2013) Turkey PCT No Score TPSOverall=NA NStart=60 NEnd=60
Population: Group 1 (G1; N=20): Mean age=65.2±6.8yr; Gender: Males=7, Females=13. Group 2 (G2; N=20): Mean age=62.4±8.2yr; Gender: Males=4, Females=16. Group 3 (G3; N=20): Mean age=62.4±7.1yr; Gender: Males=10, Females=10. Intervention: Patients received either physiotherapy alone (G1), with intraarticular steroid injection (G2), or with injection and hydraulic distension (G3). Outcomes were assessed at baseline, 24hr, and 1mo. Outcomes: Range of Motion (ROM); Visual Analog Scale (VAS).
1. For flexion and abduction, there were significant within-group differences for G2 and G3 24hr after treatments (p<0.001).
2. For internal and external rotations, there were significant within-group differences for G3 24hr after treatment (p<0.05).
3. At 1mo, all groups had significant improvements for ROM in all directions and VAS pain at rest (p<0.05).
Jeon et al. (2014) Korea PCT No Score TPSEG1=16±14wk TPSEG2=20±16wk TPSEG3=20±16wk NStart=33 NEnd=30
Population: Experimental Group 1 (EG1; N=10): Mean age=64.3±16.2yr; Gender: Males=4, Females=6. Experimental Group 2 (EG2; N=10): Mean age=64.0±8.4yr; Gender: Males=5, Females=5. Experimental Group 3 (EG3; N=10): Mean age=61.0±11.3yr; Gender: Males=5, Females=5. Intervention: Patients were allocated to receive intraarticular steroid injection of 40mg triamcinolone acetonide (EG1), supraspacular nerve block of 5ml 1% lidocaine (EG2), or combined (EG3). Outcomes were assessed before and after injection, at 1hr, 1wk, and 1mo. Outcomes: Visual Analogue Scale (VAS); Range of Motion (ROM).
1. All groups showed significant improvements in VAS and ROM after treatment (p<0.001) but there were no significant differences between groups.
2. Pain on VAS was significantly greater at 1mo than 1wk, but significantly lower than before injection.
11.7.8 Hyaluronic Acid Injections for the Hemiplegic Shoulder Table 11.7.8 Hyaluronic Acid Injections for the Hemiplegic Shoulder
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Huang et al. (2016a) Taiwan RCT PEDro=8 TPSEG=28.0±8.0d TPSCC=31.0±32.0d NStart=26 NEnd=26
Population: Experimental Group (EG; N=16): Mean age=61.0±16.0yr; Gender: Males=10, Females=6. Control Group (CG; N=10): Mean age=62.5±19.0yr; Gender: Males=7, Females=3. Intervention: Patients were randomized to receive ultrasound-guided subacromial injection of 2.5ml hyaluronic acid (EG) or intraarticular injection of 0.9% sodium chloride (CG). Both groups received 3 weekly injections and conventional rehabilitation. Outcomes were assessed before and after treatment. Outcomes: Visual Analogue Scale (VAS); Range of Motion (ROM); Fugl-Meyer Assessment (FMA);
1. EG showed significant improvements in VAS score (p=0.03), ROM flexion (p=0.03), ROM abduction (p=0.02), and FMA (p=0.003), but not in ROM extension, MAS score, or subluxation (p>0.05).
2. CG showed significant improvements in VAS score (p=0.007), ROM flexion (p=0.035), and FMA (p=0.042), but not in ROM extension, ROM adduction, MAS score, or subluxation (p>0.05).
3. EG had significantly greater improvement in VAS score than CG (p=0.001), but there were no significant between-group

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 27 of 42 www.ebrsr.com
Modified Ashworth Scale (MAS); Subluxation. differences in MAS, FMA, or ROM (p>0.05).
Jang et al. (2016) Korea RCT PEDro=5 TPSEG=56.76±29.8d TPSCG=52.94±33.1d NStart=39 NEnd=31
Population: Experimental Group (EG; N=21): Mean age=56.6±11.3yr; Gender: Males=13, Females=8. Control Group (CG; N=18): Mean age=60.8±13.7yr; Gender: Males=14, Females=4. Intervention: Patients were randomized to receive intraarticular injections of 2ml hyaluronic acid (EG) or 40mg triamcinolone acetonide (CG). EG received three weekly injections and CG receive a single injection. Outcomes were assessed at baseline, 4wk, and 8wk. Outcomes: Wong-Baker Scale (WBS); Passive Range of Motion (ROM).
1. EG showed significant improvement in WBS night and movement at 4wk and 8wk (p≤0.003), while CG showed significant improvement only for movement at 4wk and 8wk (p≤0.001).
2. EG showed significant improvement in ROM in shoulder flexion and external rotation at 4wk and 8wk (p≤0.006), while CG showed significant improvement only at 8wk (p≤0.014).
3. There were no significant differences between groups for WBS or ROM (p>0.05).
11.7.9 Suprascapular Nerve Block for the Hemiplegic Shoulder Table 11.7.9 Suprascapular Nerve Block for the Hemiplegic Shoulder
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Boonsong et al. (2009) Thailand RCT PEDro=4 TPS=NA N=10
Intervention: Patients were randomized to receive two injections of suprascapular nerve block (SSNB; 10 mL of 1% lidocaine) or ultrasound therapy (UST) 5d/wk for 4wk. Both groups were given the same program of range of motion exercises. Outcomes were assessed at baseline, 2wk, and 4wk. Outcomes: Visual Analogue Scale (VAS); Range of Motion (ROM).
1. At 4wk, VAS scores were significantly reduced in the SSNB group compared to the UST group (20 vs 50, p=0.004).
2. There were no significant differences between groups on ROM measures in either flexion and abduction at any time.
Yasar et al. (2011) Turkey RCT PEDro=5 TPS=Chronic N=26
Intervention: Patients were randomized to receive a single injection of intraarticular triamcinolone acetonide (40mg; N=11) or suprascapular nerve block (SSNB; N=15). Outcomes were assessed at baseline, 1 hour, 1 week, and 1 month. Outcomes: Visual Analogue Scale (VAS).
Pain on VAS was reduced in both groups over the study period. There were no significant differences in VAS scores between groups.
Adey-Wakeling et al. (2013) Australia RCT PEDro=9 TPSExp=13±9wk TPSCon=11±8wk NStart=64 NEnd=57
Population: Experimental Group (EG; N=32): Mean age=NA; Gender: Males=21, Females=11. Control Group (CG; N=32): Mean age=NA; Gender: Males=15, Females=17. Intervention: Patients were randomized to receive either suprascapular nerve block (SSNB; EG) or a subcutaneous saline injection (CG). Outcomes were assessed at baseline, 1wk, 4wk, and 12wk. Outcomes: Visual Analogue Scale (VAS).
1. The SSNB group had a significantly greater mean VAS reduction than the CG at 1wk (p=0.02), 4wk (p=0.01), and 12wk (p=0.02).
11.7.10 Segmental Neuromyotherapy for the Hemiplegic Shoulder Table 11.7.10 Segmental Neuromyotherapy for the Hemiplegic Shoulder
Author, Year Methods Outcomes

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 28 of 42 www.ebrsr.com
Country PEDro Score
Time Post Stroke Sample Size
Ratmansky et al. (2012) Israel RCT PEDro=7 TPS<3mo N=24
Intervention: Patients were randomized to receive standard hospital therapy for shoulder pain (1-2hr/d, 5d/wk, 4wk) with oral medication or with 12 additional treatments of segmental neuromyotherapy (SNMT). SNMT included subcutaneous injections of lidocaine, heat application, transcutaneous electrical nerve stimulation, and passive stretching. Outcomes were assessed at baseline, 2wk, 4wk, and 2mo follow-up. Outcomes: Visual Analogue Scale (VAS); Fugl-Meyer Assessment (FMA); Ashworth Scale (AS).
1. At 4wk and 2mo follow-up, VAS scores improved in both groups; the SNMT group had non-significantly greater improvement.
2. SNMT group had significantly greater improvement in median FMA scores (p=0.02) and NT (p=0.014) at 4wk.
11.7.11 Surgery of the Hemiplegic Shoulder Table 11.7.11 Surgery of the Hemiplegic Shoulder
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Braun et al. (1971) USA Pre-Post No Score TPS=NA N=13
Intervention: Patients received a surgical procedure to release the insertion of the major muscle causing internal rotation and adduction of the shoulder. Gradual increase in range of motion was obtained by completing an intensive post-operative exercise therapy program involving passive range of motion, positioning of the shoulder, and abduction while supine, through the use of reciprocal pulley exercises. Outcomes: Movement; Pain; Discomfort.
1. 10 of the 13 patients regained 90 degrees of passive abduction and 20 degrees of external rotation within 2 months.
2. After 6 months, all of the patients complained of pain and discomfort.
Pinzur & Hopkins (1986) Pre-Post No Score TPS=NA N=6
Intervention: Patients received biceps tenodesis through a short deltopectoral approach. Outcomes: Pain; Subluxation.
1. Pain and subluxation did not recur in 5 patients at long-term follow-up.
2. Patient with recurrence had pain that was thalamic in origin.
11.7.12 Complementary & Alternative Therapies for the Hemiplegic Shoulder Table 11.7.12 Complementary & Alternative Therapies for the Hemiplegic Shoulder
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Mok & Woo (2004) Hong Kong
Intervention: Patients were randomly allocated to a treatment or control group. The treatment group
1. There were significant improvements in all outcomes after treatment for the

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 29 of 42 www.ebrsr.com
RCT PEDro=5 TPS=NA N=102
received 10 minutes of slow-stroke back massage for seven successive evenings. Outcomes: Heart Rate (HR); Blood Pressure (BP); Anxiety; Pain.
treatment group compared to the control group (p<0.05).
Shin & Lee (2007) Korea RCT PEDro=6 TPS<30d N=30
Intervention: Patients were randomized to either dry acupressure (N=15) or acupressure combined with 3 essential oils (N=15). Treatment was provided in 20min sessions 2x/d for 2wk. Outcomes: Visual Analogue Scale (VAS).
1. After treatment, there was significantly greater pain reduction on VAS in the aromatherapy group (p=0.001).
Li et al. (2012) China RCT PEDro=6 TPS=NA N=120
Intervention: Patients were randomly allocated to a 6 week treatment group receiving massage and electric acupuncture or a control group receiving rehabilitation therapy (pose training and Bobath exercise). Outcomes were assessed at baseline, 6wk, and 12wk. Outcomes: Numeric Pain Rating Scale (NPRS); Fugl-Meyer Assessment (FMA); Shoulder Hand Syndrome (SHS) stage.
1. Treatment group had significantly lower NPRS scores than the control group at 6wk and 12wk (p<0.05).
2. Significantly less of the treatment group developed stage II or III SHS compared to the control group at 6wk and 12wk (p<0.05).
3. FMA of upper limb was significantly higher in the treatment group than control group at 6wk (p=0.02); this improvement was not maintained at 12wk.
4. No significant difference in functional hand activity level was seen among groups.
Seo et al. (2013) Korea RCT PEDro=7 TPSEG=57±30d TPSCG=54±27d NStart=29 NEnd=24
Population: Experimental Group (EG; N=13): Mean age=63.8±10.8yr; Gender: Males=6, Females=7. Control Group (CG; N=11): Mean age=67.4±7.8yr; Gender: Males=4, Females=7. Intervention: Patients were randomized to receive acupuncture with herbal (EG) or normal (CG) point injections 3x/wk for 2wk. Outcomes were assessed at baseline, 1wk, 2wk, and 3wk. Outcomes: Numerical Rating Scale (NRS); Passive Range of Motion (PROM); Fugl-Meyer Assessment (FMA).
1. NRS was significantly reduced in EG after treatment and at follow-up (p<0.001), but there was no significant reduction in CG (p=0.267).
2. Reduction in NRS was significantly greater in EG than CG (p<0.05).
3. PROM significantly improved in both groups after treatment (p<0.05), but remained significant at follow-up only in EG (p<0.05).
4. Improvement in PROM was similar between groups (p>0.05).
5. FMA significantly improved in both groups after treatment and at follow-up (p<0.05).
6. Improvement in FMA was significantly greater in EG than CG (p=0.039).
Lin et al. (2015) China Pre-Post No Score TPSRange>1yr NStart=25 NEnd=25
Population: Mean age=56yr; Gender: Males=18, Females=7. Intervention: Patients received infrared C radiation (3-1000µm) and hot compress. Outcomes were assessed before and after treatment. Outcomes: Visual Analogue Scale (VAS).
1. In males, there was a significant decrease in VAS after treatment (p<0.001).
2. In females, there was a decrease in VAS after treatment, but it was not significant.
Zhao et al. (2015) China RCT PEDro=7 TPSEG=120±224d TPSCG=104±159d
Population: Experimental Group (EG; N=62): Mean age=63.73±11.65yr; Gender: Males=44, Females=18. Control Group (CG; N=62): Mean age=65.53±10.67yr; Gender: Males=45, Females=17. Intervention: Patients were randomized to receive warm needling therapy and acupuncture at
3. EG improved significantly in VAS score at 2wk and 3mo (p<0.01), whereas the CG showed no improvement (p>0.05).
4. EG showed a significantly greater improvement in VAS score compared to the CG at 2wk and 3mo (p<0.01).

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 30 of 42 www.ebrsr.com
NStart=124 NEnd=119
meridian-sinew sites (EG) or usual care (CG). Treatment was conducted in 30-40min sessions 5x/wk over 2wk. Outcomes were assessed at baseline, 2wk, and 3mo follow-up. Outcomes: Visual Analog Scale (VAS); Range of Motion (ROM); Barthel Index (BI).
5. EG group showed a significantly greater improvement in ROM compared to CG at 2wk and 3mo (p<0.01).
6. There was no significant difference in BI scores between groups at 2wk (p>0.05), but CG showed a significantly greater improvement than EG at 3mo (p<0.01).
Mendigutia-Gomez et al. (2016) Spain RCT PEDro=9 TPS=NA NStart=25 NEnd=20
Population: Mean age=58±2yr; Gender: Males=11, Females=9. Intervention: Patients were randomized to receive rehabilitation alone (control) or with deep dry needling acupuncture (experimental) 1x/wk for 3wk. After a 2wk washout period, patients crossed over to receive the alternate treatment. Outcomes were assessed 1wk before and 1wk after each treatment period. Outcomes: Pressure Pain Threshold (PPT); Range of Motion (ROM); Modified Ashworth Scale (MAS).
1. PPT showed significantly greater improvement after acupuncture than control at the deltoid (p<0.001), infraspinatus (p=0.02), and zygapophyseal joint (p<0.001).
2. ROM showed significantly greater improvement after acupuncture than control for abduction (p=0.001) and external rotation (p=0.045) but not flexion (p=0.444).
3. MAS was significantly lower after acupuncture than control in the infraspinatus (p=0.01), but not in the trapezius (p=0.630), subscapularis (p=0.686), or pectoralis major (p=0.362).
11.8 Complex Regional Pain Syndrome (CRPS)
11.8.6 Pharmacological Interventions for CRPS Table 11.8.6 Pharmacological Interventions for CRPS
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Davis et al. (1977) USA Case Series No Score TPS=NA N=68
Intervention: Patients received triamcinolone diacetate (16mg/d) for 14-21d. Outcomes: Pain.
1. All patients became pain-free, when subjected to passive stretching of the involved joints, within 3wk.
2. Six patients experienced a relapse of their pain, which resolved during a second course of treatment.
Braus et al. (1994) Germany RCT PEDro=5 TPS=NA N=36
Intervention: Patients were randomized to receive either methylprednisolone (8mg/d) or placebo over 4wk, in addition to daily physical therapy. Outcomes: Complex Regional Pain Syndrome (CRPS).
1. Patients receiving corticosteroid treatment demonstrated significant improvement in CRPS at 4wk that was maintained at 6mo.
2. No significant improvement in SHS was noted in the placebo group after 4wk, at which time all patients switched over to corticosteroids.
3. 31 of the 36 patients became almost symptom free within 10d of corticosteroids.
Kalita et al. (2006) India RCT PEDro=7
Intervention: Patients were randomized to receive prednisolone (40mg/d) or piroxicam (20mg/d). Outcomes: Complex Regional Pain Syndrome (CRPS).
1. 83.3% patients showed significant improvement in the prednisolone group compared to 16.7% in the piroxicam group.
2. Mean change in CRPS score was greater in

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 31 of 42 www.ebrsr.com
TPSMedian=28d N=60
the prednisolone group than the piroxicam group (6.47 vs 0.47).
Rah et al. (2012) Korea Score RCT PEDro=6 TPS=NA N=58
Interventions: Patients were randomized to receive an injection of triamcinolone (40mg) or lidocaine. Outcomes were assessed at 2wk, 4wk, and 8wk. Outcomes: Visual Analogue Scale (VAS); Shoulder Disability Questionnaire (SDQ).
1. Improvements in VAS day and SDQ scores were significantly greater with triamcinolone than lidocaine at 4wk and 8wk (p<0.05)
2. Improvements in VAS night scores were significantly greater with triamcinolone than lidocaine at 2wk, 4wk, and 8wk (p<0.05).
Yoo et al. (2012) Korea RCT PEDro=6 TPSEG=2.8±1.1mo TPSCG=2.3±0.9mo N=42
Population: Experimental Group (EG; N=22): Mean age=61.3±5.6yr; Gender: Males=12, Females10. Control Group (CG; N=10): Mean age=59.1±4.5yr; Gender: Males=11, Females=9. Intervention: Patients were randomized to receive stellate ganglion block with (EG) or without (CG) ultrasonography guiding. Outcomes were assessed before, 2wk after, and 4wk after injection. Outcomes: Visual Analogue Scale (VAS); Complex Regional Pain Syndrome Scale (CRPS); Swelling.
1. EG showed significant decrease in VAS score from baseline at 2wk and 4wk (p<0.05), while CG showed significant decrease at only 4wk (p<0.05).
2. Decrease in VAS score was significantly greater in EG than CG at 2wk and 4wk (p<0.01).
3. There were no significant within- or between-group differences in CRPS score or degree of swelling.
Kim et al. (2016) Korea Pre-Post No Score TPSMean=15±15mo N=100
Population: Mean age=60.27±11.59yr; Males=53, Females=47. Intervention: Patients received 1mL triamcinolone injection at the extensor digitorum communis (EDC). Outcomes: Cross-Sectional Area (CSA) of EDC; Visual Analogue Scale (VAS); Swelling.
1. CSA of the EDC, VAS scores, and swelling were significantly reduced after injection (p<0.05).
Eun Young et al. (2016) Korea RCT PEDro=6 TPSEG1=54.9±33.0d TPSEG2=47.9±18.2d NStart=21 NEnd=21
Population: Experimental Group 1 (EG1; N=10): Mean age=67.50±6.95yr; Males=5, Females=5. Experimental Group 2 (EG2; N=11): Mean age=63.09±10.53yr; Males=5, Females=6. Intervention: Patients were randomized to receive either 180mg pamidronate (EG1) or prednisolone (EG2). EG1 received treatment intravenously in 3 equal doses every other day. EG2 received treatment orally at an initial dose of 1mg/kg of body weight. Outcomes were assessed at baseline, 1wk, 2wk, and 4wk. Outcomes: Visual Analogue Scale (VAS); Circumference of the Middle Finger (CMF); Circumference of the Wrist (CW).
1. VAS scores were significantly reduced from baseline in both groups at 1wk, 2wk, and 4wk (p<0.05).
2. On VAS, EG1 had significantly greater reduction than EG2 at 1wk and 2wk (p<0.05).
3. CMF was significantly reduced in both groups at 1wk and 2wk (p<0.05), but only in EG2 at 4wk (p<0.05).
4. For CMF, there were no significant differences between groups at any time.
5. CW of the affected had was significantly reduced in EG2 at 1wk and 2wk (p<0.05) and both groups at 4wk in EG1 (p<0.05).
6. For CW, EG2 had significantly greater reduction than EG1 at 1wk, 2wk, and 4wk (p<0.05).
Kalita et al. (2016) India RCT PEDro=5 TPS=9.52±5.72wk NStart=52 NEnd=39
Population: Experimental Group (EG; N=26) Mean age=56.6±12.5yr; Males=14, Females=12. Control Group (CG; N=26): Mean age=52.5±8.9yr; Males=15, Females=11. Intervention: Patients received prednisolone 10mg/d for 2mo. Patients were randomized to the continue (EG) or discontinue (CG) prednisolone. Outcomes were assessed at baseline, 1mo, and 2mo. Outcomes: Complex Regional Pain Syndrome
1. At 1mo, EG showed significant improvement compared to CG for CRPS severity (pain, autonomic, and abduction subscales) and VAS score (p<0.05), but not mRS or BI scores.
2. After 1mo, CG experienced dropout due to recurrence of symptoms: 50% remained controls (CGa) and 50% restarted prednisolone treatment (CGb).
3. At 2mo, there were no significant differences between EG and Cga for any outcome
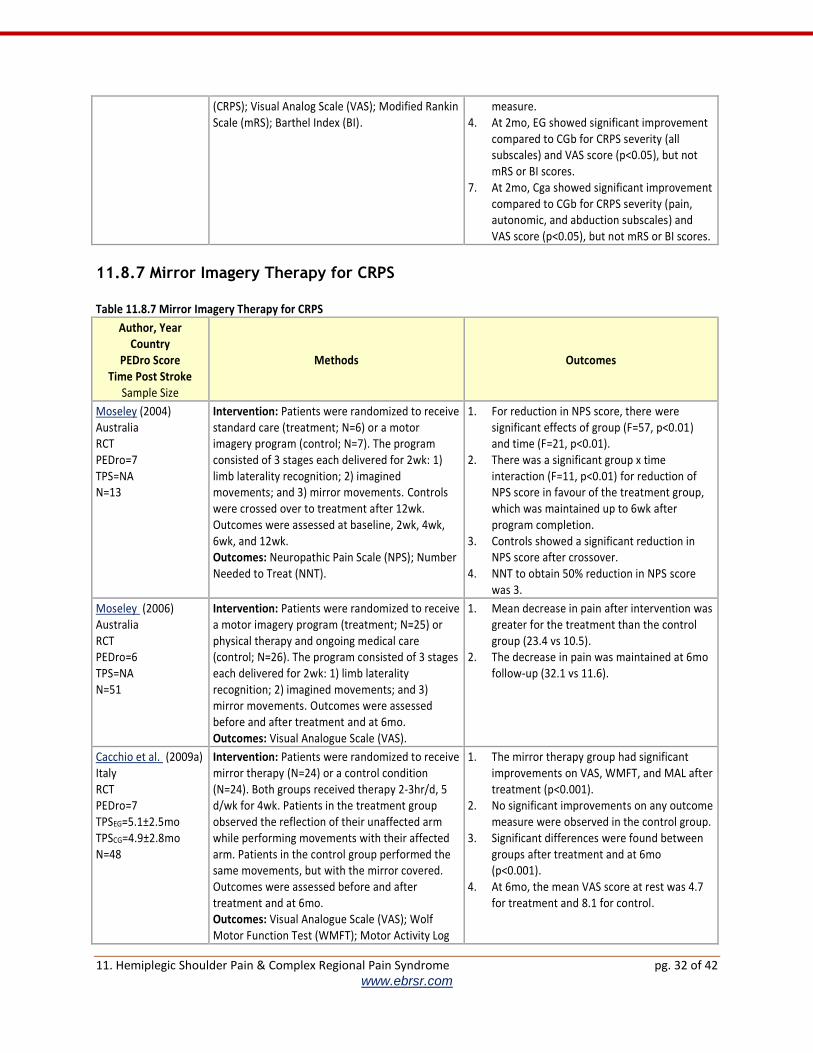
11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 32 of 42 www.ebrsr.com
(CRPS); Visual Analog Scale (VAS); Modified Rankin Scale (mRS); Barthel Index (BI).
measure. 4. At 2mo, EG showed significant improvement
compared to CGb for CRPS severity (all subscales) and VAS score (p<0.05), but not mRS or BI scores.
7. At 2mo, Cga showed significant improvement compared to CGb for CRPS severity (pain, autonomic, and abduction subscales) and VAS score (p<0.05), but not mRS or BI scores.
11.8.7 Mirror Imagery Therapy for CRPS Table 11.8.7 Mirror Imagery Therapy for CRPS
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Moseley (2004) Australia RCT PEDro=7 TPS=NA N=13
Intervention: Patients were randomized to receive standard care (treatment; N=6) or a motor imagery program (control; N=7). The program consisted of 3 stages each delivered for 2wk: 1) limb laterality recognition; 2) imagined movements; and 3) mirror movements. Controls were crossed over to treatment after 12wk. Outcomes were assessed at baseline, 2wk, 4wk, 6wk, and 12wk. Outcomes: Neuropathic Pain Scale (NPS); Number Needed to Treat (NNT).
1. For reduction in NPS score, there were significant effects of group (F=57, p<0.01) and time (F=21, p<0.01).
2. There was a significant group x time interaction (F=11, p<0.01) for reduction of NPS score in favour of the treatment group, which was maintained up to 6wk after program completion.
3. Controls showed a significant reduction in NPS score after crossover.
4. NNT to obtain 50% reduction in NPS score was 3.
Moseley (2006) Australia RCT PEDro=6 TPS=NA N=51
Intervention: Patients were randomized to receive a motor imagery program (treatment; N=25) or physical therapy and ongoing medical care (control; N=26). The program consisted of 3 stages each delivered for 2wk: 1) limb laterality recognition; 2) imagined movements; and 3) mirror movements. Outcomes were assessed before and after treatment and at 6mo. Outcomes: Visual Analogue Scale (VAS).
1. Mean decrease in pain after intervention was greater for the treatment than the control group (23.4 vs 10.5).
2. The decrease in pain was maintained at 6mo follow-up (32.1 vs 11.6).
Cacchio et al. (2009a) Italy RCT PEDro=7 TPSEG=5.1±2.5mo TPSCG=4.9±2.8mo N=48
Intervention: Patients were randomized to receive mirror therapy (N=24) or a control condition (N=24). Both groups received therapy 2-3hr/d, 5 d/wk for 4wk. Patients in the treatment group observed the reflection of their unaffected arm while performing movements with their affected arm. Patients in the control group performed the same movements, but with the mirror covered. Outcomes were assessed before and after treatment and at 6mo. Outcomes: Visual Analogue Scale (VAS); Wolf Motor Function Test (WMFT); Motor Activity Log
1. The mirror therapy group had significant improvements on VAS, WMFT, and MAL after treatment (p<0.001).
2. No significant improvements on any outcome measure were observed in the control group.
3. Significant differences were found between groups after treatment and at 6mo (p<0.001).
4. At 6mo, the mean VAS score at rest was 4.7 for treatment and 8.1 for control.
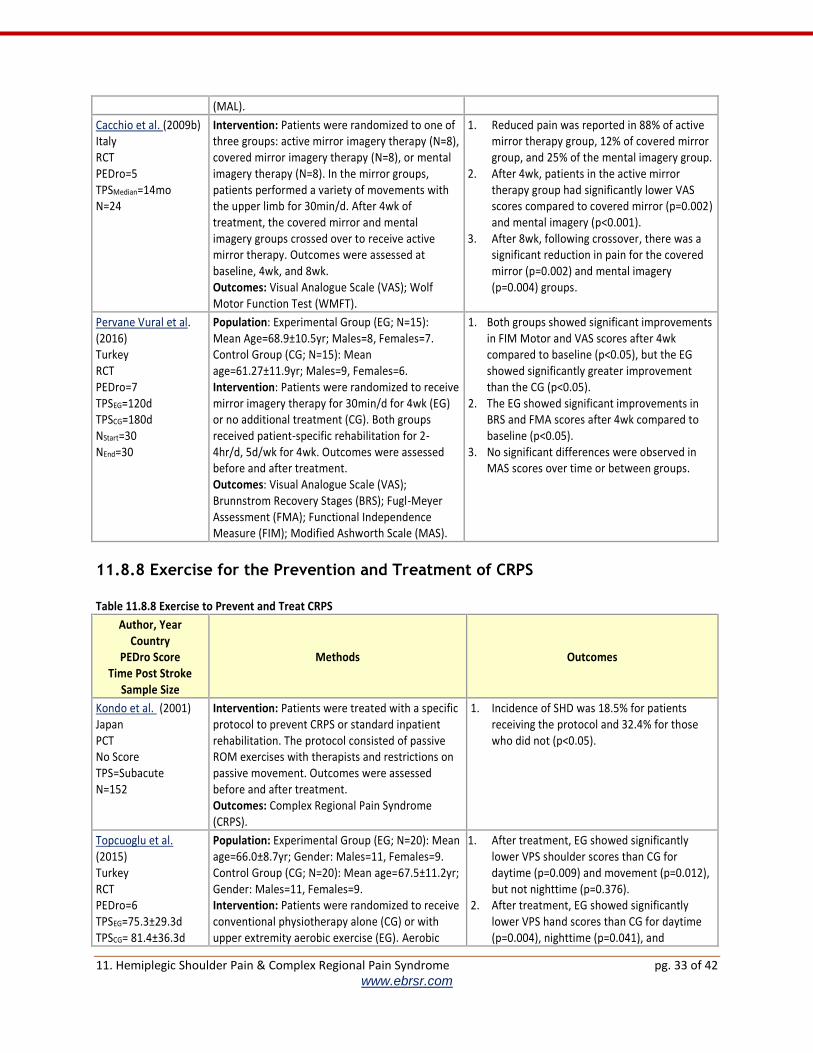
11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 33 of 42 www.ebrsr.com
(MAL).
Cacchio et al. (2009b) Italy RCT
PEDro=5 TPSMedian=14mo N=24
Intervention: Patients were randomized to one of three groups: active mirror imagery therapy (N=8), covered mirror imagery therapy (N=8), or mental imagery therapy (N=8). In the mirror groups, patients performed a variety of movements with the upper limb for 30min/d. After 4wk of treatment, the covered mirror and mental imagery groups crossed over to receive active mirror therapy. Outcomes were assessed at baseline, 4wk, and 8wk. Outcomes: Visual Analogue Scale (VAS); Wolf Motor Function Test (WMFT).
1. Reduced pain was reported in 88% of active mirror therapy group, 12% of covered mirror group, and 25% of the mental imagery group.
2. After 4wk, patients in the active mirror therapy group had significantly lower VAS scores compared to covered mirror (p=0.002) and mental imagery (p<0.001).
3. After 8wk, following crossover, there was a significant reduction in pain for the covered mirror (p=0.002) and mental imagery (p=0.004) groups.
Pervane Vural et al. (2016) Turkey RCT PEDro=7 TPSEG=120d TPSCG=180d NStart=30 NEnd=30
Population: Experimental Group (EG; N=15): Mean Age=68.9±10.5yr; Males=8, Females=7. Control Group (CG; N=15): Mean age=61.27±11.9yr; Males=9, Females=6. Intervention: Patients were randomized to receive mirror imagery therapy for 30min/d for 4wk (EG) or no additional treatment (CG). Both groups received patient-specific rehabilitation for 2-4hr/d, 5d/wk for 4wk. Outcomes were assessed before and after treatment. Outcomes: Visual Analogue Scale (VAS); Brunnstrom Recovery Stages (BRS); Fugl-Meyer Assessment (FMA); Functional Independence Measure (FIM); Modified Ashworth Scale (MAS).
1. Both groups showed significant improvements in FIM Motor and VAS scores after 4wk compared to baseline (p<0.05), but the EG showed significantly greater improvement than the CG (p<0.05).
2. The EG showed significant improvements in BRS and FMA scores after 4wk compared to baseline (p<0.05).
3. No significant differences were observed in MAS scores over time or between groups.
11.8.8 Exercise for the Prevention and Treatment of CRPS Table 11.8.8 Exercise to Prevent and Treat CRPS
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Kondo et al. (2001) Japan PCT No Score TPS=Subacute N=152
Intervention: Patients were treated with a specific protocol to prevent CRPS or standard inpatient rehabilitation. The protocol consisted of passive ROM exercises with therapists and restrictions on passive movement. Outcomes were assessed before and after treatment. Outcomes: Complex Regional Pain Syndrome (CRPS).
1. Incidence of SHD was 18.5% for patients receiving the protocol and 32.4% for those who did not (p<0.05).
Topcuoglu et al. (2015) Turkey RCT PEDro=6 TPSEG=75.3±29.3d TPSCG= 81.4±36.3d
Population: Experimental Group (EG; N=20): Mean age=66.0±8.7yr; Gender: Males=11, Females=9. Control Group (CG; N=20): Mean age=67.5±11.2yr; Gender: Males=11, Females=9. Intervention: Patients were randomized to receive conventional physiotherapy alone (CG) or with upper extremity aerobic exercise (EG). Aerobic
1. After treatment, EG showed significantly lower VPS shoulder scores than CG for daytime (p=0.009) and movement (p=0.012), but not nighttime (p=0.376).
2. After treatment, EG showed significantly lower VPS hand scores than CG for daytime (p=0.004), nighttime (p=0.041), and

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 34 of 42 www.ebrsr.com
NStart=40 NEnd=40
exercise (5W/min) was delivered 30min/d, 5d/wk for 4wk. Outcomes were assessed before and after treatment. Outcomes: Visual Pain Scale (VPS); Functional Independence Measure (FIM); Nottingham Health Profile (NHP); Beck Depression Inventory (BDI).
movement (p=0.001). 3. After treatment, EG showed significantly
greater improvement on NHP and BDI than CG (p<0.05), but not FIM.
11.8.10 Calcitonin for the Prevention of CRPS Table 11.8.10 Calcitonin to Prevent CRPS
Author, Year Country
PEDro Score Time Post Stroke
Sample Size
Methods Outcomes
Matayoshi et al. (2009) Japan PCT No Score TPS=Subacute N=59
Intervention: Patients received conventional therapy with a weekly intramuscular injection of 20U calcitonin (N=24). These patients were compared with a historical control that received rehabilitation therapy only (N=35). All patients were observed during the in-hospital rehabilitation period. Outcomes: Complex Regional Pain Syndrome (CRPS).
1. Incidence of CRPS in all patients during the control period was 8.2%.
2. Among patients with severe stroke who received calcitonin, the incidence of CRPS was significantly lower compared to the control group (12.5% vs. 57.1%, p<0.001).
3. CRPS was completely prevented when calcitonin was started ≤4wk post stroke, but prophylactic effects were weaker when calcitonin was started >6 weeks.

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 35 of 42 www.ebrsr.com
References
Ada, L., Goddard, E., McCully, J., Stavrinos, T., & Bampton, J. (2005). Thirty Minutes Of Positioning Reduces The Development Of Shoulder External Rotation Contracture After Stroke: A Randomized Controlled Trial. Archives of physical medicine and rehabilitation, 86(2), 230-234.
Adey-Wakeling, Z., Crotty, M., & Michael Shanahan, E. (2013). Suprascapular Nerve Block For Shoulder Pain In The First Year After Stroke: A Randomized Controlled Trial. Stroke, 44(11), 3136-3141.
Ancliffe, J. (1992). Strapping The Shoulder In Patients Following A Cerebrovascular Accident (CVA): A Pilot Study. Australian Journal of Physiotherapy, 38(1), 37-41.
Appel, C., Mayston, M., & Perry, L. (2011). Feasibility Study Of A Randomized Controlled Trial Protocol To Examine Clinical Effectiveness Of Shoulder Strapping In Acute Stroke Patients. Clinical rehabilitation, 25(9), 833-843.
Aras, M. D., Gokkaya, N. K. O., Comert, D., Kaya, A., & Cakci, A. (2004). Shoulder Pain In Hemiplegia: Results From A National Rehabilitation Hospital In Turkey. American journal of physical medicine & rehabilitation, 83(9), 713-719.
Ashford, S., & Turner-Stokes, L. (2009). Management of shoulder and proximal upper limb spasticity using botulinum toxin and concurrent therapy interventions: a preliminary analysis of goals and outcomes. Disability & Rehabilitation, 31(3), 220-226.
Baker, L. L., & Parker, K. (1986). Neuromuscular Electrical Stimulation Of The Muscles Surrounding The Shoulder. Physical Therapy, 66(12), 1930-1937.
Barlak, A., Unsal, S., Kaya, K., Sahin-Onat, S., & Ozel, S. (2009). Poststroke Shoulder Pain In Turkish Stroke Patients: Relationship With Clinical Factors And Functional Outcomes. International Journal of Rehabilitation Research, 32(4), 309-315.
Baykal, T., & Senel, K. (2013). The Comparison Of The Effects Of The Combination Of Physical Therapy Modalities And Local Corticosteroid Therapy And Alone Physical Therapy In The Patients With Hemiplegic Shoulder Pain. Turkish Journal of Geriatrics-Turk Geriatri Dergisi, 16(4), 376-382.
Bhakta, B. B., Cozens, J. A., Bamford, J. M., & Chamberlain, M. A. (1996). Use of botulinum toxin in stroke patients with severe upper limb spasticity. Journal of Neurology, Neurosurgery & Psychiatry, 61(1), 30-35.
Bohannon, R. W. (1988). Relationship Between Shoulder Pain And Selected Variables In Patients With Hemiplegia. Clinical rehabilitation, 2(2), 111-117.
Bohannon, R. W., & Andrews, A. W. (1990). Shoulder Subluxation And Pain In Stroke Patients. The American Journal of Occupational Therapy, 44(6), 507-509.
Bohannon, R. W., Larkin, P. A., Smith, M. B., & Horton, M. G. (1986). Shoulder Pain In Hemiplegia: Statistical Relationship With Five Variables. Arch Phys Med Rehabil, 67(8), 514-516.
Boonsong, P., Jaroenarpornwatana, A., & Boonhong, J. (2009). Preliminary Study Of Suprascapular Nerve Block (Ssnb) In Hemiplegic Shoulder Pain. Journal of the Medical Association of Thailand= Chotmaihet thangphaet, 92(12), 1669-1674.
Braun, R., West, F., Mooney, V., Nickel, V., Roper, B., & Caldwell, C. (1971). Surgical Treatment Of The Painful Shoulder Contracture In The Stroke Patient. The Journal of Bone & Joint Surgery, 53(7), 1307-1312.
Braus, D. F., Krauss, J. K., & Strobel, J. (1994). The ShoulderHand Syndrome After Stroke: A Prospective Clinical Trial. Annals of neurology, 36(5), 728-733.
Brooke, M. M., De Lateur, B. J., Diana-Rigby, G. C., & Questad, K. A. (1991). Shoulder Subluxation In Hemiplegia: Effects Of Three Different Supports. Arch Phys Med Rehabil, 72(8), 582-586.
11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 36 of 42 www.ebrsr.com
Cacchio, A., De Blasis, E., De Blasis, V., Santilli, V., & Spacca, G. (2009a). Mirror Therapy In Complex Regional Pain Syndrome Type 1 Of The Upper Limb In Stroke Patients. Neurorehabilitation and neural repair, 23(8), 792-799.
Cacchio, A., De Blasis, E., Necozione, S., Orio, F. d., & Santilli, V. (2009b). Mirror therapy for chronic complex regional pain syndrome type 1 and stroke. New England Journal of Medicine, 361(6), 634-636.
Caglar, N. S., Akin, T., Aytekin, E., Komut, E. A., Ustabasioglu, F., Okur, S., Dogan, Y., Erdem, H. I., Ataoglu, E., & Yalcinkaya, E. (2016). Pain syndromes in hemiplegic patients and their effects on rehabilitation results. J Phys Ther Sci, 28(3), 731-737.
Castiglione, A., Bagnato, S., Boccagni, C., Romano, M. C., & Galardi, G. (2011). Efficacy of intra-articular injection of botulinum toxin type A in refractory hemiplegic shoulder pain. Arch Phys Med Rehabil, 92(7), 1034-1037.
Chae, J., David, T. Y., Walker, M. E., Kirsteins, A., Elovic, E. P., Flanagan, S. R., Harvey, R. L., Zorowitz, R. D., Frost, F. S., & Grill, J. H. (2005). Intramuscular Electrical Stimulation For Hemiplegic Shoulder Pain: A 12-Month Follow-Up Of A Multiple-Center, Randomized Clinical Trial. American journal of physical medicine & rehabilitation, 84(11), 832-842.
Chae, J., & Hart, R. (1998). Comparison of discomfort associated with surface and percutaneous intramuscular electrical stimulation for persons with chronic hemiplegia. Am J Phys Med Rehabil, 77(6), 516-522.
Chae, J., & Jedlicka, L. (2009). Subacromial corticosteroid injection for poststroke shoulder pain: an exploratory prospective case series. Archives of Physical Medicine and Rehabilitation, 90(3), 501-506.
Chae, J., Mascarenhas, D., Yu, D. T., Kirsteins, A., Elovic, E. P., Flanagan, S. R., Harvey, R. L., Zorowitz, R. D., & Fang, Z. P. (2007). Poststroke Shoulder Pain: Its Relationship To Motor Impairment, Activity Limitation, And Quality Of Life. Archives of physical medicine and rehabilitation, 88(3), 298-301.
Chae, J., Wilson, R. D., Bennett, M. E., Lechman, T. E., & Stager, K. W. (2013). Single-lead percutaneous peripheral nerve stimulation for the treatment of hemiplegic shoulder pain: a case series. Pain Pract, 13(1), 59-67.
Chae, J., Wolf-Johnson, T., & Govil, H. (2007). Subacromial corticosteroid injection for poststroke shoulder pain: a retrospective chart review. Arch Phys Med Rehabil, 88(12), 1690-1693.
Chantraine, A., Baribeault, A., Uebelhart, D., & Gremion, G. (1999). Shoulder Pain And Dysfunction In Hemiplegia: Effects Of Functional Electrical Stimulation. Archives of physical medicine and rehabilitation, 80(3), 328-331.
Chatterjee, S., Hayner, K. A., Arumugam, N., Goyal, M., Midha, D., Arora, A., Sharma, S., & Kumar, S. P. (2016). The California Tri-pull Taping Method in the Treatment of Shoulder Subluxation After Stroke: A Randomized Clinical Trial. N Am J Med Sci, 8(4), 175-182.
Choi, J. G., Shin, J. H., & Kim, B. R. (2016). Botulinum Toxin A Injection into the Subscapularis Muscle to Treat Intractable Hemiplegic Shoulder Pain. Ann Rehabil Med, 40(4), 592-599.
Church, C., Price, C., Pandyan, A. D., Huntley, S., Curless, R., & Rodgers, H. (2006). Randomized Controlled Trial To Evaluate The Effect Of Surface Neuromuscular Electrical Stimulation To The Shoulder After Acute Stroke. Stroke, 37(12), 2995-3001.
Culham, E. G., Noce, R. R., & Bagg, S. D. (1995). Shoulder Complex Position And Glenohumeral Subluxation In Hemiplegia. Archives of physical medicine and rehabilitation, 76(9), 857-864.
Davis, S. W., Petrillo, C. R., Eichberg, R. D., & Chu, D. S. (1977). Shoulder-Hand Syndrome In A Hemiplegic Population: A 5-Year Retrospective Study. Archives of physical medicine and rehabilitation, 58(8), 353.
De Boer, K. S., Arwert, H. J., De Groot, J. H., Meskers, C. G. M., Mishre, A. R., & Arendzen, J. H. (2008). Shoulder Pain And External Rotation In Spastic Hemiplegia Do Not Improve By Injection Of

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 37 of 42 www.ebrsr.com
Botulinum Toxin A Into The Subscapular Muscle. Journal of Neurology, Neurosurgery & Psychiatry, 79(5), 581-583.
De Jong, L. D., Dijkstra, P. U., Gerritsen, J., Geurts, A. C., & Postema, K. (2013). Combined Arm Stretch Positioning And Neuromuscular Electrical Stimulation During Rehabilitation Does Not Improve Range Of Motion, Shoulder Pain Or Function In Patients After Stroke: A Randomised Trial. Journal of physiotherapy, 59(4), 245-254.
De Jong, L. D., Nieuwboer, A., & Aufdemkampe, G. (2006). Contracture Preventive Positioning Of The Hemiplegic Arm In Subacute Stroke Patients: A Pilot Randomized Controlled Trial. Clinical rehabilitation, 20(8), 656-667.
Dean, C., Mackey, F., & Katrak, P. (2000). Examination Of Shoulder Positioning After Stroke: A Randomised Controlled Pilot Trial. Australian Journal of Physiotherapy, 46(1), 35-42.
Dekker, J. H., Wagenaar, R. C., Lankhorst, G. J., & de Jong, B. A. (1997). The Painful Hemiplegic Shoulder: Effects of Intra-Articular Triamcinolone Acetonide1. American journal of physical medicine & rehabilitation, 76(1), 43-48.
Dogan, A., Demirtas, R., & Ozgirgin, N. (2013). Intraarticular hydraulic distension with steroids in the management of hemiplegic shoulder. Turkish Journal of Medical Sciences, 43(2), 304-310.
Eun Young, H., Hyeyun, K., & Sang Hee, I. (2016). Pamidronate effect compared with a steroid on complex regional pain syndrome type I: Pilot randomised trial. Neth J Med, 74(1), 30-35.
Faghri, P. D., Rodgers, M. M., Glaser, R. M., Bors, J. G., Ho, C., & Akuthota, P. (1994). The Effects Of Functional Electrical Stimulation On Shoulder Subluxation, Arm Function Recovery, And Shoulder Pain In Hemiplegic Stroke Patients. Archives of physical medicine and rehabilitation, 75(1), 73-79.
Fil, A., Armutlu, K., Atay, A. O., Kerimoglu, U., & Elibol, B. (2011). The Effect Of Electrical Stimulation In Combination With Bobath Techniques In The Prevention Of Shoulder Subluxation In Acute Stroke Patients. Clinical rehabilitation, 25(1), 51-59.
Griffin, A., & Bernhardt, J. (2006). Strapping The Hemiplegic Shoulder Prevents Development Of Pain During Rehabilitation: A Randomized Controlled Trial. Clinical rehabilitation, 20(4), 287-295.
Grossens-Sills, J., & Schenkman, M. (1985). Analysis Of Shoulder Pain, Range Of Motion, And Subluxation In Patients With Hemiplegia. Physical Therapy, 65-73.
Gustafsson, L., & McKenna, K. (2006). A Programme Of Static Positional Stretches Does Not Reduce Hemiplegic Shoulder Pain Or Maintain Shoulder Range Of Motion-A Randomized Controlled Trial. Clinical rehabilitation, 20(4), 277-286.
Hafsteinsdottir, T. B., Kappelle, J., Grypdonck, M. H., & Algra, A. (2007). Effects Of Bobath-Based Therapy On Depression, Shoulder Pain And Health-Related Quality Of Life In Patients After Stroke. J Rehabil Med, 39(8), 627-632.
Hakuno, A., Sashika, H., Ohkawa, T., & Itoh, R. (1984). Arthrographic Findings In Hemiplegic Shoulders. Archives of physical medicine and rehabilitation, 65(11), 706.
Hanger, H. C., Whitewood, P., Brown, G., Ball, M. C., Harper, J., Cox, R., & Sainsbury, R. (2000). A Randomized Controlled Trial Of Strapping To Prevent Post-Stroke Shoulder Pain. Clinical rehabilitation, 14(4), 370-380.
Hartwig, M., Gelbrich, G., & Griewing, B. (2012). Functional Orthosis In Shoulder Joint Subluxation After
Ischaemic Brain Stroke To Avoid Post-Hemiplegic Shoulderçôhand Syndrome: A Randomized Clinical Trial. Clinical rehabilitation, 26(9), 807-816.
Hecht, J. (1995). The Role Of Spasticity In Hemiplegic Shoulder Pain And What To Do About It. . Paper presented at the 57th Annual Assembly Of The American Academy Of Physical Medicine And Rehabilitation, Orlando,Florida.

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 38 of 42 www.ebrsr.com
Heo, M.-Y., Kim, C.-Y., & Nam, C.-W. (2015). Influence Of The Application Of Inelastic Taping On Shoulder Subluxation And Pain Changes In Acute Stroke Patients. Journal of Physical Therapy Science, 27(11), 3393-3395.
Huang, Y. C., Leong, C. P., Wang, L., Chen, M. J., Chuang, C. Y., Liaw, M. Y., & Wang, L. Y. (2016a). The effects of hyaluronic acid on hemiplegic shoulder injury and pain in patients with subacute stroke: A randomized controlled pilot study. Medicine (Baltimore), 95(49), e5547.
Huang, Y. C., Leong, C. P., Wang, L., Wang, L. Y., Yang, Y. C., Chuang, C. Y., & Hsin, Y. J. (2016b). Effect of kinesiology taping on hemiplegic shoulder pain and functional outcomes in subacute stroke patients: a randomized controlled study. Eur J Phys Rehabil Med, 52(6), 774-781.
Hurd, M. M., Farrell, K. H., & Waylonis, G. W. (1974). Shoulder Sling For Hemiplegia: Friend Or Foe? Archives of physical medicine and rehabilitation, 55(11), 519.
Ikai, T., Tei, K., Yoshida, K., Miyano, S., & Yonemoto, K. (1998). Evaluation And Treatment Of Shoulder Subluxation In Hemiplegia: Relationship Between Subluxation And Pain1. American journal of physical medicine & rehabilitation, 77(5), 421-426.
Inaba, M. K., & Piorkowski, M. (1972). Ultrasound In Treatment Of Painful Shoulders In Patients With Hemiplegia. Physical Therapy, 52(7), 737.
Jang, M. H., Lee, C.-H., Shin, Y.-I., Kim, S.-Y., & Huh, S. C. (2016). Effect Of Intra-Articular Hyaluronic Acid Injection On Hemiplegic Shoulder Pain After Stroke. Ann Rehabil Med, 40(5), 835-844.
Jeon, H. J., An, S., Yoo, J., Park, N. H., & Lee, K. H. (2016). The effect of Monkey Chair and Band exercise system on shoulder range of motion and pain in post-stroke patients with hemiplegia. J Phys Ther Sci, 28(8), 2232-2237.
Jeon, W. H., Park, G. W., Jeong, H. J., & Sim, Y. J. (2014). The Comparison Of Effects Of Suprascapular Nerve Block, Intra-Articular Steroid Injection, And A Combination Therapy On Hemiplegic Shoulder Pain: Pilot Study. Ann Rehabil Med, 38(2), 167-173.
Joynt, R. L. (1992). The Source Of Shoulder Pain In Hemiplegia. Arch Phys Med Rehabil, 73(5), 409-413. Kalichman, L., Frenkel-Toledo, S., Vered, E., Sender, I., Galinka, T., Alperovitch-Najenson, D., Ratmansky,
M., & Treger, I. (2016). Effect of kinesio tape application on hemiplegic shoulder pain and motor ability: a pilot study. Int J Rehabil Res, 39(3), 272-276.
Kalita, J., Misra, U., Kumar, A., & Bhoi, S. K. (2016). Long-term Prednisolone in Post-stroke Complex Regional Pain Syndrome. Pain Physician, 19(8), 565-574.
Kalita, J., Vajpayee, A., & Misra, U. K. (2006). Comparison Of Prednisolone With Piroxicam In Complex Regional Pain Syndrome Following Stroke: A Randomized Controlled Trial. Qjm, 99(2), 89-95.
Kim, S. H., Ha, K. W., Kim, Y. H., Seol, P. H., Kwak, H. J., Park, S. W., & Ryu, B. J. (2016). Effect of Radial Extracorporeal Shock Wave Therapy on Hemiplegic Shoulder Pain Syndrome. Ann Rehabil Med, 40(3), 509-519.
Kim, Y. W., Kim, Y., Kim, J. M., Hong, J. S., Lim, H. S., & Kim, H. S. (2016). Is poststroke complex regional pain syndrome the combination of shoulder pain and soft tissue injury of the wrist?: A prospective observational study: STROBE of ultrasonographic findings in complex regional pain syndrome. Medicine (Baltimore), 95(31), e4388.
Kim, Y. W., Shin, J. C., Yoon, J. G., Kim, Y. K., & Lee, S. C. (2013). Usefulness of radial extracorporeal shock wave therapy for the spasticity of the subscapularis in patients with stroke: a pilot study. Chin Med J (Engl), 126(24), 4638-4643.
Kobayashi, H., Onishi, H., Ihashi, K., Yagi, R., & Handa, Y. (1999). Reduction In Subluxation And Improved Muscle Function Of The Hemiplegic Shoulder Joint After Therapeutic Electrical Stimulation. Journal of Electromyography and Kinesiology, 9(5), 327-336.
Kondo, I., Hosokawa, K., Soma, M., Iwata, M., & Maltais, D. (2001). Protocol To Prevent Shoulder-Hand Syndrome After Stroke. Archives of physical medicine and rehabilitation, 82(11), 1619-1623.

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 39 of 42 www.ebrsr.com
Kong, K. H., Neo, J. J., & Chua, K. S. (2007). A Randomized Controlled Study Of Botulinum Toxin A In The Treatment Of Hemiplegic Shoulder Pain Associated With Spasticity. Clinical rehabilitation, 21(1), 28-35.
Koyuncu, E., Nakipoglu-Yuzer, G. F., Dogan, A., & Ozgirgin, N. (2010). The Effectiveness Of Functional Electrical Stimulation For The Treatment Of Shoulder Subluxation And Shoulder Pain In Hemiplegic Patients: A Randomized Controlled Trial. Disability & Rehabilitation, 32(7), 560-566.
Kumar, R., Metter, E. J., Mehta, A. J., & Chew, T. (1990). Shoulder Pain In Hemiplegia: The Role Of Exercise. American journal of physical medicine & rehabilitation, 69(4), 205-208.
Lakse, E., Gunduz, B., Erhan, B., & Celik, E. C. (2009). The Effect Of Local Injections In Hemiplegic Shoulder Pain: A Prospective, Randomized, Controlled Study. American journal of physical medicine & rehabilitation, 88(10), 805-811.
Leandri, M., Parodi, C. I., Corrieri, N., & Rigardo, S. (1990). Comparison Of Tens Treatments In Hemiplegic Shoulder Pain. Scand J Rehabil Med, 22(2), 69-71.
Li, N., Tian, F., Wang, C., Yu, P., Zhou, X., Wen, Q., Qiao, X., & Huang, L. (2012). Therapeutic Effect Of Acupuncture And Massage For Shoulder-Hand Syndrome In Hemiplegia Patients: A Clinical Two-Center Randomized Controlled Trial. Journal of Traditional Chinese Medicine, 32(3), September.
Lim, J. Y., Koh, J. H., & Paik, N. J. (2008). Intramuscular Botulinum Toxin-A Reduces Hemiplegic Shoulder Pain A Randomized, Double-Blind, Comparative Study Versus Intraarticular Triamcinolone Acetonide. Stroke, 39(1), 126-131.
Lin, C. C., Chiang, Y. S., & Lung, C. C. (2015). Effect of infrared-C radiation on skin temperature, electrodermal conductance and pain in hemiparetic stroke patients. Int J Radiat Biol, 91(1), 42-53.
Lin, C. H., Chen, K. H., Chang, C. H., Chen, C. M., Huang, Y. C., Hsu, H. C., & Hong, C. Z. (2014). Muscle Pain Intensity And Pressure Pain Threshold Changes In Different Periods Of Stroke Patients. American journal of physical medicine & rehabilitation, 93(4), 299-309.
Lindgren, I., Ekstrand, E., Lexell, J., Westergren, H., & Brogardh, C. (2014). Somatosensory impairments are common after stroke but have only a small impact on post-stroke shoulder pain. J Rehabil Med, 46(4), 307-313.
Linn, S. L., Granat, M. H., & Lees, K. R. (1999). Prevention Of Shoulder Subluxation After Stroke With Electrical Stimulation. Stroke, 30(5), 963-968.
Lo, S. F., Chen, S. Y., Lin, H. C., Jim, Y. F., Meng, N. H., & Kao, M. J. (2003). Arthrographic And Clinical Findings In Patients With Hemiplegic Shoulder Pain. Archives of physical medicine and rehabilitation, 84(12), 1786-1791.
Lynch, D., Ferraro, M., Krol, J., Trudell, C. M., Christos, P., & Volpe, B. T. (2005). Continuous Passive Motion Improves Shoulder Joint Integrity Following Stroke. Clinical rehabilitation, 19(6), 594-599.
Manigandan, J. B., Ganesh, G. S., Pattnaik, M., & Mohanty, P. (2014). Effect Of Electrical Stimulation To Long Head Of Biceps In Reducing Gleno Humeral Subluxation After Stroke. NeuroRehabilitation, 34(2), 245-252.
Marciniak, C. M., Harvey, R. L., Gagnon, C. M., Duraski, S. A., Denby, F. A., McCarty, S., Bravi, L. A., Polo, K. M., & Fierstein, K. M. (2012). Does Botulinum Toxin Type A Decrease Pain And Lessen Disability In Hemiplegic Survivors Of Stroke With Shoulder Pain And Spasticity?: A Randomized, Double-Blind, Placebo-Controlled Trial. American journal of physical medicine & rehabilitation, 91(12), 1007-1019.
Marco, E., Duarte, E., Vila, J., Tejero, M., Guillen, A., Boza, R., Escalada, F., & Espadaler, J. M. (2007). Is Botulinum Toxin Type A Effective In The Treatment Of Spastic Shoulder Pain In Patients After Stroke? A Double-Blind Randomized Clinical Trial. Journal of Rehabilitation Medicine, 39(6), 440-447.

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 40 of 42 www.ebrsr.com
Matayoshi, S., Shimodozono, M., Hirata, Y., Ueda, T., Horio, S., & Kawahira, K. (2009). Use Of Calcitonin To Prevent Complex Regional Pain Syndrome Type I In Severe Hemiplegic Patients After Stroke. Disability & Rehabilitation, 31(21), 1773-1779.
Mendigutia-Gomez, A., Martin-Hernandez, C., Salom-Moreno, J., & Fernandez-de-Las-Penas, C. (2016). Effect Of Dry Needling On Spasticity, Shoulder Range Of Motion, And Pressure Pain Sensitivity In Patients With Stroke: A Crossover Study. J Manipulative Physiol Ther, 39(5), 348-358.
Mohamed, R. E., Amin, M. A., & Aboelsafa, A. A. (2014). Ultrasonographic and clinical study of post-stroke painful hemiplegic shoulder. Egyptian Journal of Radiology and Nuclear Medicine, 45(4), 1163-1170.
Mok, E., & Woo, C. P. (2004). The Effects Of Slow-Stroke Back Massage On Anxiety And Shoulder Pain In Elderly Stroke Patients. Complementary Therapies in Nursing and Midwifery, 10(4), 209-216.
Moniruzzaman, M., Salek, K. M., Shakoor, M. A., Mia, B. A., & Moyeenuzzaman, M. (2010). Effects Of Therapeutic Modalities On Patients With Post Stroke Shoulder Pain. Mymensingh Med J, 19(1), 48-53.
Moodie, N., Brisbin, J., & Morgan, A. (1986). Subluxation Of The Glenohumeral Joint In Hemiplegia: Evaluation Of Supportive Devices. Physiotherapy Canada, 38(3), 151-157.
Moseley, G. L. (2004). Graded Motor Imagery Is Effective For Long-Standing Complex Regional Pain Syndrome: A Randomised Controlled Trial. Pain, 108(1), 192-198.
Moseley, G. L. (2006). Graded Motor Imagery For Pathologic Pain A Randomized Controlled Trial. Neurology, 67(12), 2129-2134.
Niessen, M., Janssen, T., Meskers, C., Koppe, P., Konijnenbelt, M., & Veeger, D. (2008). Kinematics Of The Contralateral And Ipsilateral Shoulder: A Possible Relationship With Post-Stroke Shoulder Pain. J Rehabil Med, 40(6), 482-486.
Paci, M., Nannetti, L., Taiti, P., Baccini, M., & Rinaldi, L. (2007). Shoulder Subluxation After Stroke: Relationships With Pain And Motor Recovery. Physiother Res Int, 12(2), 95-104.
Pandian, J. D., Kaur, P., Arora, R., Vishwambaran, D. K., Toor, G., Mathangi, S., Vijaya, P., Uppal, A., Kaur, T., & Arima, H. (2013). Shoulder Taping Reduces Injury And Pain In Stroke Patients: Randomized Controlled Trial. Neurology, 80(6), 528-532.
Partridge, C. J., Edwards, S. M., Mee, R., & Van Langenberghe, H. V. K. (1990). Hemiplegic Shoulder Pain: A Study Of Two Methods Of Physiotherapy Treatment. Clinical rehabilitation, 4(1), 43-49.
Pedreira, G., Cardoso, E., & Melo, A. (2008). Botulinum toxin type A for refractory post-stroke shoulder pain. Arquivos de neuro-psiquiatria, 66(2A), 213-215.
Pervane Vural, S., Nakipoglu Yuzer, G. F., Sezgin Ozcan, D., Demir Ozbudak, S., & Ozgirgin, N. (2016). Effects of Mirror Therapy in Stroke Patients With Complex Regional Pain Syndrome Type 1: A Randomized Controlled Study. Arch Phys Med Rehabil, 97(4), 575-581.
Pillastrini, P., Rocchi, G., Deserri, D., Foschi, P., Mardegan, M., Naldi, M. T., Villafane, J. H., & Bertozzi, L. (2016). Effectiveness of neuromuscular taping on painful hemiplegic shoulder: a randomised clinical trial. Disabil Rehabil, 38(16), 1603-1609.
Pinzur, M. S., & Hopkins, G. E. (1986). Biceps tenodesis for painful inferior subluxation of the shoulder in adult acquired hemiplegia. Clin Orthop Relat Res(206), 100-103.
Poduri, K. R. (1993). Shoulder Pain In Stroke Patients And Its Effects On Rehabilitation. Journal of Stroke and Cerebrovascular Diseases, 3(4), 261-266.
Prévost, R., Arsenault, A. B., Dutil, E., & Drouin, G. (1987). Rotation Of The Scapula And Shoulder Subluxation In Hemiplegia. Archives of physical medicine and rehabilitation, 68(11), 786.
Price, C. I., & Pandyan, A. D. (2001). Electrical Stimulation For Preventing And Treating Post-Stroke Shoulder Pain: A Systematic Cochrane Review. Clinical rehabilitation, 15(1), 5-19.
11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 41 of 42 www.ebrsr.com
Rah, U. W., Yoon, S. H., Moon, D. J., Kwack, K. S., Hong, J. Y., Lim, Y. C., & Joen, B. (2012). Subacromial Corticosteroid Injection On Poststroke Hemiplegic Shoulder Pain: A Randomized, Triple-Blind, Placebo-Controlled Trial. Archives of physical medicine and rehabilitation, 93(6), 949-956.
Ratmansky, M., Defrin, R., & Soroker, N. (2012). A Randomized Controlled Study Of Segmental Neuromyotherapy For Post-Stroke Hemiplegic Shoulder Pain. Journal of Rehabilitation Medicine, 44(10), 830-836.
Ratnasabapathy, Y., Broad, J., Baskett, J., Pledger, M., Marshall, J., & Bonita, R. (2003). Shoulder Pain In People With A Stroke: A Population-Based Study. Clinical rehabilitation, 17(3), 304-311.
Renzenbrink, G. J., & IJzerman, M. J. (2004). Percutaneous neuromuscular electrical stimulation (P-NMES) for treating shoulder pain in chronic hemiplegia. Effects on shoulder pain and quality of life. Clinical rehabilitation, 18(4), 359-365.
Rizk, T. E., Christopher, R. P., Pinals, R. S., Salazar, J. E., & Higgins, C. (1984). Arthrographic Studies In Painful Hemiplegic Shoulders. Archives of physical medicine and rehabilitation, 65(5), 254-256.
Roy, C. W., Sands, M. R., Hill, L. D., Harrison, A., & Marshall, S. (1995). The Effect Of Shoulder Pain On Outcome Of Acute Hemiplegia. Clinical rehabilitation, 9(1), 21-27.
Seo, Y. R., Jung, W. S., Park, S. U., Moon, S. K., Park, J. M., & Park, J. Y. (2013). The Effect Of Ouhyul Herbal Acupuncture Point Injections On Shoulder Pain After Stroke. Evid Based Complement Alternat Med, 2013, 504686.
Shai, G., Ring, H., Costeff, H., & Solzi, P. (1984). Glenohumeral Malalignment In The Hemiplegic Shoulder. An Early Radiologic Sign. Scandinavian journal of rehabilitation medicine, 16(3), 133.
Shin, B. C., & Lee, M. S. (2007). Effects Of Aromatherapy Acupressure On Hemiplegic Shoulder Pain And Motor Power In Stroke Patients: A Pilot Study. The Journal of Alternative and Complementary Medicine, 13(2), 247-252.
Snels, I. A., Beckerman, H., Twisk, J. W., Dekker, J. H., De Koning, P., Koppe, P. A., Lankhorst, G. J., & Bouter, L. M. (2000). Effect Of Triamcinolone Acetonide Injections On Hemiplegic Shoulder Pain A Randomized Clinical Trial. Stroke, 31(10), 2396-2401.
Suethanapornkul, S., Kuptniratsaikul, P. S.-a., Kuptniratsaikul, V., Uthensut, P., Dajpratha, P., & Wongwisethkarn, J. (2008). Post Stroke Shoulder Subluxation And Shoulder Pain: A Cohort Multicenter Study. Medical journal of the Medical Association of Thailand, 91(12), 1885.
Suriya-amarit, D., Gaogasigam, C., Siriphorn, A., & Boonyong, S. (2014). Effect Of Interferential Current Stimulation In Management Of Hemiplegic Shoulder Pain. Archives of physical medicine and rehabilitation, 95(8), 1441-1446.
Topcuoglu, A., Gokkaya, N. K., Ucan, H., & Karakus, D. (2015). The effect of upper-extremity aerobic exercise on complex regional pain syndrome type I: a randomized controlled study on subacute stroke. Top Stroke Rehabil, 22(4), 253-261.
Turton, A. J., & Britton, E. (2005). A pilot randomized controlled trial of a daily muscle stretch regime to prevent contractures in the arm after stroke. Clin Rehabil, 19(6), 600-612.
Van Langenberghe, H. V., & Hogan, B. M. (1988). Degree Of Pain And Grade Of Subluxation In The Painful Hemiplegic Shoulder. Scand J Rehabil Med, 20(4), 161-166.
Van Ouwenaller, C., Laplace, P., & Chantraine, A. (1986). Painful Shoulder In Hemiplegia. Arch Phys Med Rehabil, 67(1), 23-26.
Wang, R. Y., Chan, R. C., & Tsai, M. W. (2000). Functional Electrical Stimulation On Chronic And Acute Hemiplegic Shoulder Subluxation. American journal of physical medicine & rehabilitation, 79(4), 385-394.
Wanklyn, P., Forster, A., & Young, J. (1996). Hemiplegic Shoulder Pain (Hsp): Natural History And Investigation Of Associated Features. Disability & Rehabilitation, 18(10), 497-501.
Williams, R., Taffs, L., & Minuk, T. (1988). Evaluation Of Two Support Methods For The Subluxated Shoulder Of Hemiplegic Patients. Physical Therapy, 68(8), 1209-1214.

11. Hemiplegic Shoulder Pain & Complex Regional Pain Syndrome pg. 42 of 42 www.ebrsr.com
Wilson, R. D., Gunzler, D. D., Bennett, M. E., & Chae, J. (2014). Peripheral Nerve Stimulation Compared With Usual Care For Pain Relief Of Hemiplegic Shoulder Pain: A Randomized Controlled Trial. American journal of physical medicine & rehabilitation / Association of Academic Physiatrists, 93(1), 17-28.
Yasar, E., Vural, D., Safaz, I., Balaban, B., Yilmaz, B., Goktepe, A. S., & Alaca, R. (2011). Which Treatment Approach Is Better For Hemiplegic Shoulder Pain In Stroke Patients: Intra-Articular Steroid Or Suprascapular Nerve Block? A Randomized Controlled Trial. Clinical rehabilitation, 25(1), 60-68.
Yelnik, A. P., Colle, F. M., Bonan, I. V., & Vicaut, E. (2007). Treatment Of Shoulder Pain In Spastic Hemiplegia By Reducing Spasticity Of The Subscapular Muscle: A Randomised, Double Blind, Placebo Controlled Study Of Botulinum Toxin A. Journal of Neurology, Neurosurgery & Psychiatry, 78(8), 845-848.
Yoo, S. D., Jung, S. S., Kim, H. S., Yun, D. H., Kim, D. H., Chon, J., & Hong, D. W. (2012). Efficacy Of Ultrasonography Guided Stellate Ganglion Blockade In The Stroke Patients With Complex Regional Pain Syndrome. Ann Rehabil Med, 36(5), 633-639.
You, Y. Y., Her, J. G., Woo, J. H., Ko, T., & Chung, S. H. (2014). The Effects Of Stretching And Stabilization Exercise On The Improvement Of Spastic Shoulder Function In Hemiplegic Patients. Journal of Physical Therapy Science, 26(4), 491-495.
Yu, D. T., Chae, J., Walker, M. E., Kirsteins, A., Elovic, E. P., Flanagan, S. R., Harvey, R. L., Zorowitz, R. D., Frost, F. S., Grill, J. H., Feldstein, M., & Fang, Z.-P. (2004). Intramuscular Neuromuscular Electric Stimulation For Poststroke Shoulder Pain: A Multicenter Randomized Clinical Trial. Archives of physical medicine and rehabilitation, 85(5), 695-704.
Zhao, H., Nie, W., Sun, Y., Li, S., Yang, S., Meng, F., Zhang, L., Wang, F., & Huang, S. (2015). Warm Needling Therapy and Acupuncture at Meridian-Sinew Sites Based on the Meridian-Sinew Theory: Hemiplegic Shoulder Pain. Evid Based Complement Alternat Med, 2015, 694973.
Zorowitz, R. D., Hughes, M. B., Idank, D., Ikai, T., & Johnston, M. V. (1996). Shoulder Pain And Subluxation After Stroke: Correlation Or Coincidence? The American Journal of Occupational Therapy, 50(3), 194-201.
Zorowitz, R. D., Idank, D., Ikai, T., Hughes, M. B., & Johnston, M. V. (1995). Shoulder Subluxation After Stroke: A Comparison Of Four Supports. Archives of physical medicine and rehabilitation, 76(8), 763-771.