hepatitis c treatment in patient- specific populations yemm hepatitis... · ©2016 mfmer | slide-1...
TRANSCRIPT

©2016 MFMER | slide-1
Hepatitis C Treatment in Patient-Specific PopulationsKristyn E. Yemm, PharmDPGY1 Pharmacy ResidentPharmacy Grand RoundsMay 10, 2016

©2016 MFMER | slide-2
Presentation Objectives• Identify a guideline-based approach to select an
appropriate regimen in patients diagnosed with hepatitis C virus
• Discuss treatment options for hepatitis C virus in patients with renal dysfunction
• Review hepatitis C virus treatment strategies in compensated versus decompensated cirrhosis

©2016 MFMER | slide-3
Complications of Acute Hepatitis C Virus (HCV) Infection
AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Accessed April 20, 2016.http://www.cdc.gov/hepatitis/C/cFAQ.htm#statistics. Accessed April 20, 2016.
N Engl J Med 2009; 361: 1279-90.
75-85% 60-70% 5-20% 20-40% 50%
Chronic Infection Chronic Liver Disease Cirrhosis Hepatorenal
Syndrome Mortality
Transplant

©2016 MFMER | slide-4
Which of the following should be considered prior to choosing a HCV therapeutic regimen?1. Genotype2. Degree of liver disease3. Cost/adherence4. Comorbidities5. Potential drug-drug interactions6. All of the above

©2016 MFMER | slide-5
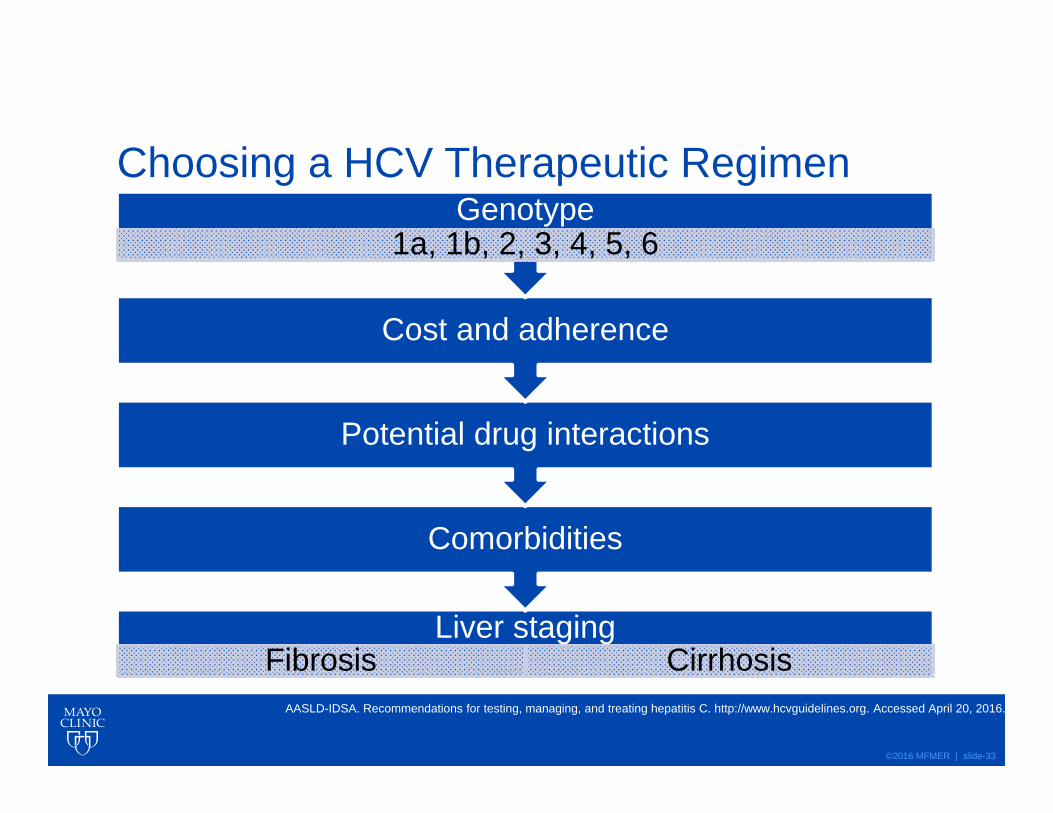
Choosing a HCV Therapeutic Regimen
Liver stagingFibrosis Cirrhosis
Comorbidities
Potential drug interactions
Cost and adherence
Genotype1a, 1b, 2, 3, 4, 5, 6
AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Accessed April 20, 2016.HCV: Hepatitis c virusAASLD-IDSA: American Association for the Study of Liver Disease - Infectious Disease Society of America

©2016 MFMER | slide-6
End Stage Renal Disease (ESRD) and Hemodialysis (HD) Treatment StrategiesPart 1: HCV Specific Populations

©2016 MFMER | slide-7
Accelerates the decline in kidney
dysfunction
Mortality
#1 Cause of post renal
transplant liver disease
J Viral Hepat 2012; 19: 601-07.Am J Transplant. 2005 Oct;5(10):2433-40.
©2016 MFMER | slide-8
Choosing a HCV Therapeutic Regimen for ESRD and HD
Kidney transplant candidacy
Benefits and risks of HCV therapy
Comorbidities
Life expectancy
Kidney Int Suppl. 2008 Apr;(109):S1-99.ESRD: End-stage renal diseaseHD: Hemodialysis

©2016 MFMER | slide-9
Historical Complications to Antiviral Treatment in ESRD/HD• Suboptimal treatment efficacy• Lack of evidence• Toxic accumulation of renal metabolites• Intolerable side effect profile
ESRD: End-stage renal diseaseHD: Hemodialysis
©2016 MFMER | slide-10
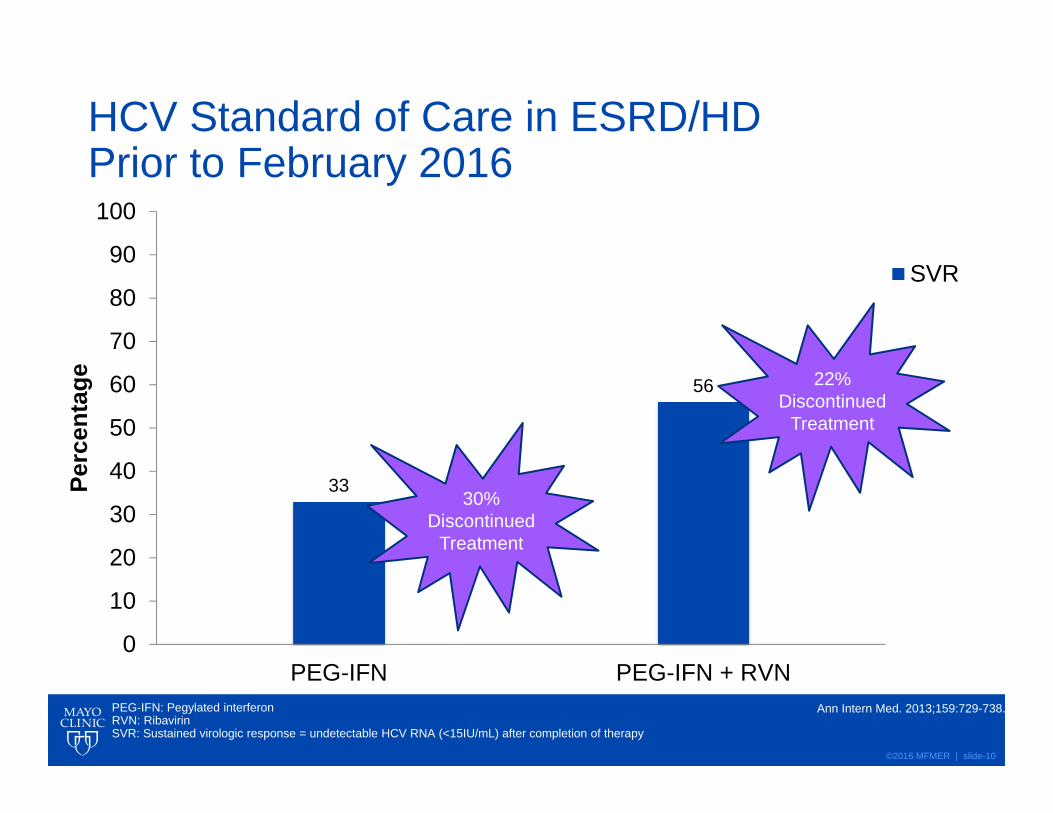
HCV Standard of Care in ESRD/HD Prior to February 2016
33
56
0
10
20
30
40
50
60
70
80
90
100
PEG-IFN PEG-IFN + RVN
Perc
enta
ge
SVR
Ann Intern Med. 2013;159:729-738.
30% Discontinued
Treatment
22% Discontinued
Treatment
PEG-IFN: Pegylated interferon RVN: RibavirinSVR: Sustained virologic response = undetectable HCV RNA (<15IU/mL) after completion of therapy

©2016 MFMER | slide-11
Side Effect Profile PEG-IFN
• Rash
• Flu-like symptoms
• HA/Fatigue
• Arthralgia/myalgia
• Paresthesias
• Dysgeusia
• Mood changes
• Cytopenias (Hgb, ANC, Plt)
RBV
• Rash
• HA/Fatigue
• Anorexia
• Depression
• Anemia
• Hyperuricemia
©2016 MFMER | slide-12
HCV Treatment Limitations in ESRD/HD
Renally Cleared Metabolites
• Sofosbuvir
• Ribavirin
Adverse Reactions
• Poorly tolerated• Pegylated interferon
• Life-threatening• Ribavirin
Ann Intern Med. 2013;159:729-738.

©2016 MFMER | slide-13
Patient Case CK is a 58yoM diagnosed with genotype 1a HCV
PMH: seasonal allergies, ESRD on HD M/W/F secondary to mixed cryoglobulinemia syndrome
SH: alcohol dependence
Medications:
-fluticasone 2 sprays in each nostril QD -vitamin D3 2000un po QD
-ferrous sulfate 325mg po QD -calcium acetate 667mg po TID
What HCV treatment options are available for the patient?

©2016 MFMER | slide-14
Updated Recommendations: ESRD/HDAfter February 2016
Genotype Regimen
1a, 1b, 4 elbasvir 50mg/grazoprevir 100mg(Zepatier®) for 12 weeks
2, 3, 5, 6 PEG-IFN and dose-adjusted RBV at 200mg daily for 48 weeks
*RBV should be discontinued if hemoglobin level declines by more than 2 g/dL despite the use of erythropoietin
ESRD: End-stage renal diseaseHD: HemodialysisPEG-IFN: Pegylated interferon RVN: Ribavirin
Lancet 2015; 386: 1537–45.Ann Intern Med. 2013;159:729-738.
©2016 MFMER | slide-15
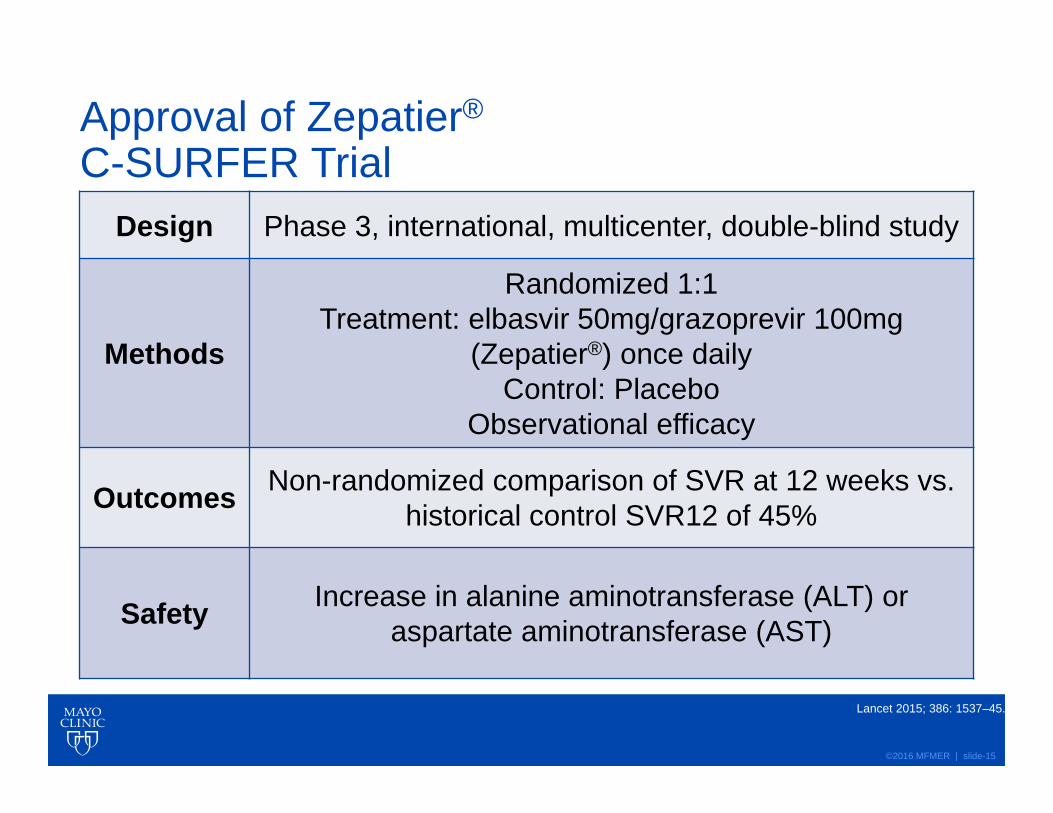
Approval of Zepatier®
C-SURFER TrialDesign Phase 3, international, multicenter, double-blind study
Methods
Randomized 1:1Treatment: elbasvir 50mg/grazoprevir 100mg
(Zepatier®) once dailyControl: Placebo
Observational efficacy
Outcomes Non-randomized comparison of SVR at 12 weeks vs. historical control SVR12 of 45%
Safety Increase in alanine aminotransferase (ALT) or aspartate aminotransferase (AST)
Lancet 2015; 386: 1537–45.

©2016 MFMER | slide-16
C-SURFER Results99.1
94.3
0
10
20
30
40
50
60
70
80
90
100
Modified Full Analysis Full analysis
Perc
enta
ge SVR
Lancet 2015; 386: 1537–45.Modified Full Analysis: Immediate treatment of intensive pharmacokinetic groupFull Analysis: All patients who received at least one dose
0-4.4% Discontinued
Treatment
HeadacheNauseaFatigue
Side EffectsSide Effects

©2016 MFMER | slide-17
C-SURFER Trial Strengths and Limitations
Strengths
• 75% on Hemodialysis
• Historical SVR control
• Treatment naïve and failed treatment
• Potential to increase waitlist for kidney transplant candidacy
Limitations
• Small population
• 6% cirrhosis in population
• Lacking active comparator
• Unclear long term adverse effect profile
Lancet 2015; 386: 1537–45.

©2016 MFMER | slide-18
Zepatier® SVR Comparison to Previous Standard of Care
99
56
33
0
10
20
30
40
50
60
70
80
90
100
Zepatier® PEG-IFN + RBV PEG-IFN
Perc
enta
ge
SVR
Lancet 2015; 386: 1537–45.Modified Full Analysis: Immediate Treatment of Intensive Pharmacokinetic Group
43%
incr
ease
66%
incr
ease

©2016 MFMER | slide-19
Which HCV treatment regimen would be most appropriate for CK?1. Sofosbuvir containing regimen2. PEG-IFN monotherapy for 48 weeks3. PEG-IFN + dose adjusted RBV for 48 weeks4. Zepatier® once daily for 12 weeks
©2016 MFMER | slide-20
Compensated versus Decompensated Cirrhosis Treatment StrategiesPart 2: HCV Specific Populations

©2016 MFMER | slide-21
Progression of Liver Dysfunction
• Progressive hepatic fibrosis
Child Turcotte Pugh Class AChild Turcotte Pugh Class A
CTP: Child Turcotte PughSBP: Spontaneous bacterial peritonitis
Child, CG, III, Turcotte, JG. Surgery and Portal Hypertension. In: The Liver and portal hypertension, Child, CG III (Eds), WB Saunders, Philadelphia 1964. p.50.
• Variceal hemorrhage
• Ascites• SBP• HE• HCC• Hepatorenal
syndrome
Child Turcotte Pugh Class B/CChild Turcotte
Pugh Class B/C
HCC: Hepatocellular carcinomaHE: Hepatic encephalopathy
Decompensated Cirrhosis
©2016 MFMER | slide-22
Patient Case Revisited CK is a 58yoM diagnosed with genotype 1a HCV
PMH: seasonal allergies, ESRD on HD M/W/F secondary to mixed cryoglobulinemia syndrome
SH: alcohol dependence
***CK now has compensated liver disease due to his persistent alcohol consumption***
Medications:
-fluticasone 2 sprays in each nostril QD -vitamin D3 2000un po QD
-ferrous sulfate 325mg po QD -calcium acetate 667mg po TID
What HCV treatment options are available for the patient?

©2016 MFMER | slide-23
0102030405060708090
100
PEG-IFN + RBV PEG-IFN + RBV +PI
IFN Sparing IFN Free
Sustained Virologic Response (%)
All values percentage of sustained virologic responsePI: Protease inhibitorIFN Sparing: Combination with polymerase inhibitor
Lancet 2015; 385: 1124-35.
2001Timeline
40-50
> 90
50-60
80-91
2011 2014 2015

©2016 MFMER | slide-24
Key Viral Replication Targets in Genotype 1• NS3/4A protease inhibitors
• Simeprevir• Paritaprevir• Boceprevir• Telaprevir• Grazoprevir
• NS5A protein inhibitors viral replication/assembly
• Ledipasvir• Ombitasvir• Elbasvir
• NS5B polymerase inhibitors• Sofosbuvir (prodrug)• Dasabuvir• Ribavirin
• Immunomodulators• PEG-IFN• Ribavirin
• Ritonavir is a potent CYP3A inhibitor
• Increases peak and trough plasma drug concentrations of paritaprevir
Lancet 2015; 385: 1124-35.

©2016 MFMER | slide-25
MOA ImmunomodulatorsPEG-IFN• Bind to specific receptors on the
surface of human cells
• Inhibition of virus replication in virus-infected cells
• Suppression of cell proliferation
• Enhancement of the phagocytic activity of macrophages
RBV• Inhibits the initiation and
elongation of RNA fragments resulting in inhibition of viral protein synthesis
©2016 MFMER | slide-26
Historical Complications to Antiviral Treatment Selection in Liver Dysfunction• Suboptimal treatment efficacy • Intolerable side effect profile• Treatment duration• Numerous drug-drug interactions• High pill burden with frequent dosing• PEG-IFN based regimens can worsen
decompensated cirrhosis

©2016 MFMER | slide-27
Compensated Cirrhosis: Treatment Naïve 1st Line Therapies
Genotype 1a
• Zepatier® 50mg/100mg*
• ledipasvir 90mg/sofosbuvir 400mg (Harvoni®)*
Genotype 1b
• Zepatier® 50mg/100mg*
• Harvoni® 90mg/400mg*
• paritaprevir 150mg/ritonavir 100mg/ombitasvir 25mg + BID dasabuvir 250mg (Viekira Pak®)*
*Treatment duration 12 weeksAASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Accessed April 20, 2016.

©2016 MFMER | slide-28
Compensated Cirrhosis: Treatment Naïve 1st Line Therapies SVR12
0
10
20
30
40
50
60
70
80
90
100
Zepatier® Harvoni® Viekira Pak®
SVR
Lancet 385(9973):1087-97.N Engl J Med. 2014a;370(20):1889-1898.
N Engl J Med 2014;370:1973-1982.PHAST Patient Monthly, Dec 2014-Aug 2015, Extracted Oct 2015.
92-99 97-9989-95
HeadacheNauseaFatigue
HeadacheWeakness
Fatigue
HeadacheInsomniaFatigue
Side Effects Side EffectsSide Effects
©2016 MFMER | slide-29
Which of the following would be the best treatment option for CK now that he suffers from compensated liver disease?1. Harvoni® for 12 weeks2. Viekira Pak® for 12 weeks3. Zepatier® for 12 weeks4. None of the above are appropriate treatment
regimens

©2016 MFMER | slide-30
Decompensated CirrhosisGenotype 1 or 4
RBV Eligible
Harvoni® + low dose RBV*
Daclatasvir 60mg +
sofosbuvir 400mg + low dose RBV*
Daclatasvir 60mg +
sofosbuvir 400mg for 24
weeks
Harvoni® for 24 weeks
Failed prior sofosbuvir treatment
Harvoni® + low dose RBV for 24 weeks
Yes No
Gastroenterology 2015;149:649–659.Gastroenterology. 2015b;149(3):649-59.
Lancet Infect Dis. 2015;15(4):397-404.Lawitz E, et al. 50th Annual Meeting of the European Association for the Study of the Liver (EASL). April 22-26, 2015b; Vienna, Austria.
*Treatment duration 12 weeks
Low dose RBV = 600mg starting dose of RBV, increase as tolerated
Yes

©2016 MFMER | slide-31
Decompensated Cirrhosis First and Second Line Therapies SVR
8783
71
0
10
20
30
40
50
60
70
80
90
100
Harvoni® + low doseRBV*
Daclatasvir/sofosbuvir+ low dose RBV*
Harvoni® for 24wks
SVR
Gastroenterology 2015;149:649–659.Gastroenterology. 2015b;149(3):649-59.
Lancet Infect Dis. 2015;15(4):397-404.Lawitz E, et al. 50th Annual Meeting of the European Association for the Study of the Liver (EASL). April 22-26, 2015b; Vienna, Austria.
*Treatment duration 12 weeks

©2016 MFMER | slide-32
Zepatier® and Harvoni® are preferred and first line treatment options in compensated and decompensated liver disease (T/F)• True• False
©2016 MFMER | slide-33
Choosing a HCV Therapeutic Regimen
Liver stagingFibrosis Cirrhosis
Comorbidities
Potential drug interactions
Cost and adherence
Genotype1a, 1b, 2, 3, 4, 5, 6
AASLD-IDSA. Recommendations for testing, managing, and treating hepatitis C. http://www.hcvguidelines.org. Accessed April 20, 2016.

©2016 MFMER | slide-34
HCV Genotype 1: Current Treatment Options of Choice in Special Populations• ESRD/HD
• Zepatier®*
• Compensated liver disease
• Zepatier®* • Harvoni®*
• Decompensated liver disease
• Harvoni® + low dose RBV*
• IFN-free regimens are currently preferred
• Higher SVR• Tolerable side effect
profiles• Significantly reduced
duration of treatment
*Treatment duration 12 weeks


©2016 MFMER | slide-36
Dose Adjustments for PEG-IFN and RBV • For patients with eGFR 15 to 29 mL/min per 1.73 m2:
• PEG-IFN-2a SQ 135 mcg per week• PEG-IFN-alfa2b SQ 1 mcg/kg per week• RBV po 200 mg per day
• For patients with eGFR <15 mL/min per 1.73 m2 or on dialysis:
• PEG-IFN-2a SQ 135 mcg per week• PEG-IFN-alfa2b SQ 1 mcg/kg per week• RBV po 200 mg weekly with an increase as
tolerated to a maximum of every other day

©2016 MFMER | slide-37
HCV-associated vasculitis or glomerulonephritis as primary cause of ESRD• Immunosuppressant doses (delay DAA Tx 1-4 months)
• PEG-IFN• 135mcg weekly• 1-1.5mcg/kg weekly
• Rituximab – vasculitis/skin ulcers/peripheral neuropathy/glomerulonephritis• 375mg/m2
• 1 month prior to antiviral• RBV
• 800-1200mg daily
• Duration up to 72 weeks (if non-responders showing clinical improvement) • Up to 48 weeks for HCV genotypes 2 or 3• 72 weeks for HCV genotypes 1 or 4)
• Apheresis/steroids• GC (1–10 mg/kg) or as pulse therapy, low-dose GC therapy may improve IFN Tx
Ann Intern Med. 2013;159:729-738.Autoimmun Rev. 2011 Jun;10(8):444-54.
Blood. 2010;116(3):326.

©2016 MFMER | slide-38
Indications that Warrant DAA Therapy (Patients who will benefit in the short term)• Advanced fibrosis or cirrhosis• Renal transplant candidates• Mixed cryoglobulinemic vasculitis / HCV-related
glomerulonephritis• Genotypes 1, 4• Timing
• If need urgent immunosuppressant therapy, delay DAA

©2016 MFMER | slide-39
Antiviral Metabolism Studied in severe ESRD/HD?
Sofosbuvir Renal Increased drug exposure, anemia, worsening renal, half-dose +
simeprevir SVR91, minor events
Ombitasvir-paritaprevir-ritonavir plus dasabuvir
(PrOD)
Liver Increased AUC (?clinical relevance)
Simeprevir Liver Safety not studiedLedipasvir Biliary Only fixed dose combo with
sofosbuvir, safety not studied
Daclatasvir Liver, minor renal Only fixed dose combo with sofosbuvir, safety not studied
PEG-IFN Renal Decreased CL, increased t ½, increased AUC
Ribavirin Renal Plasma concentrations correspond with hemolytic anemia SE, not
removed by HD

©2016 MFMER | slide-40
Renal Impairment Dosing Spectrum• eGFR >50 mL/min per 1.73 m2 - Regimen selection is the
same as that for patients without renal impairment
• eGFR 30 to 50 mL/min per 1.73 m2 - Regimen selection is the same as that for patients without renal impairment
• eGFR < 30 mL/min per 1.73 m2 or on dialysis - Zepatier, do not recommend sofosbuvir-containing regimen due to renal metabolism
• Hepatorenal syndrome (I or II) - not candidates for HCV antiviral therapy due to portal hypertension/decompensated liver disease
• Post kidney transplant - IFN is contraindicated• increased risk of acute rejection of the allograft

©2016 MFMER | slide-41
Compensated Cirrhosis: Treatment Naïve 1st Line Therapies
Trial Genotype RegimenPrimary
Outcome (SVR)
Remarks
C-EDGE 1a (50%)1b (41%) ELB 50mg/GRP 100mg* 1a = 92%
1b = 99%
Presence of baseline NS5A RAVs reduced SVR to 58%
ION-1 1LER 90mg/SFB 400mg +/-
RBV12 vs. 24 weeks
12 wk: 97-99%
No difference in SVR:
Length of treatment, +/-
RBV, HCV genotype 1
subtypeELB: elbasvirGRP: grazoprevir LER: ledipasvirSFB: sofosbuvir
RBV: ribavirin*Treatment duration 12 weeks N Engl J Med. 2014a;370(20):1889-1898.

©2016 MFMER | slide-42
Compensated Cirrhosis: Treatment Naïve 1st Line Therapies
Trial Genotype RegimenPrimary
Outcome (SVR)
Remarks
TURQUOISE-II 1aPrOD + RBV
12 vs. 24 weeks
12 wk: 89%24 wk: 95%
Difference between
groups was driven by pts
who failed PEG-
IFN/RBV
ELB: elbasvirGRP: grazoprevir LER: ledipasvirSFB: sofosbuvir
RBV: ribavirinPrOD: paritaprevir/ritonavir /ombitasvir/dasabuvir*Treatment duration 12 weeks
N Engl J Med 2014;370:1973-1982.PHAST Patient Monthly, Dec 2014-Aug 2015, Extracted Oct 2015.
October 2015 WARNINGPrOD and PrO are contraindicated in CTP class B or C

©2016 MFMER | slide-43
Decompensated Cirrhosis: Treatment Naïve 1st Line Therapies Primary Literature
Trial Genotype RegimenPrimary
Outcome (SVR)
Note
ION-1 1LER/SFB +/-
RBV12 vs. 24 weeks
12 wk: 97-99%
No difference in SVR in cirrhosis vs. non-
cirrhosis:Length of treatment,
+/- RBV, HCV genotype 1 subtype
SOLAR-1 14
LER/SFB + RBV
12 vs. 24 weeks
*12 wk: 87%*24 wk: 89%
MELD and CTP scores decreased
from baseline
N Engl J Med. 2014a;370(20):1889-1898.Gastroenterology. 2015b;149(3):649-59.
ELB: elbasvirGRP: grazoprevir LER: ledipasvirSFB: sofosbuvir
RBV: ribavirin*After excluding transplant during the studyMELD: Model For End Stage Liver DiseaseCTP: Child-Turcotte-Pugh

©2016 MFMER | slide-44
Decompensated Cirrhosis: Treatment Experienced 1st Line Therapies Primary Literature
Trial Genotype Regimen Primary Outcome (SVR) Note
SOLAR-2 14
LER/SFB + RBV 12 vs. 24 weeks
*12 wk: 87%*24 wk: 89%
MELD and CTP scores
decreased from baseline
Bourliere et al. 1
LER/SFB + RBV 12 weeks
12 week PBO phase
12 wk: 96%24 wk (+ PBO): 97%
Most common adverse events:
asthenia, headache, pruritus but
frequency was low in both
groups
ELB: elbasvirGRP: grazoprevir LER: ledipasvirSFB: sofosbuvir
RBV: ribavirin*After excluding transplant during the studyMELD: Model For End Stage Liver DiseaseCTP: Child-Turcotte-Pugh
Gastroenterology. 2015b;149(3):649-59.Lancet Infect Dis. 2015;15(4):397-404.

©2016 MFMER | slide-45
Average Wholesale Price (AWP)• Harvoni® $37800.00 for 28 tabs• Zepatier® $21840.00 for 28 tabs• Ribavirin® $496.02 for 50 capsules• Sofosbuvir $33600.00 for 28 tabs• Viekira® $33327.60 for 112 tabs• Daklinza® $25200.00 for 28 tabs• PEG-IFN alfa 2a $4533.65 for 4x135mcg

©2016 MFMER | slide-46
Cost (AWP)• ESRD/HD treatment costs:
• $65,520 for 12 week course of Zepatier®
• PEG-IFN alfa 2a + QOD RBV for 48 weeks • ($54,403.8 + $1666.63 = $56,070.43)
• Compensated cirrhosis treatment costs:• $65,520 for 12 week course of Zepatier®
• $113,400 for 12 week course of Harvoni®• $24,995.7 for a 12 week course of Viekira®
Cost of liver transplant ~$577,100Cost of kidney transplant ~$262,900
http://www.transplantliving.org. (UNOS) Accessed May 2016.

©2016 MFMER | slide-47
Cost (AWP)-Continued• Decompensated cirrhosis
treatment costs:• Harvoni® + daily RBV for
12 week course • ($113,400 + $833.32 =
$114,233.31)• Sofosbuvir + Daklinza® +
daily RBV for 12 week course
• ($100,800 + $75,600 + $833.32 =$177,233.32)
• Failed sofobuvir-Tx:
• Harvoni® + daily RBV for 24 week course
• ($226,800 + $1666.64 =$228,466.64)
• RBV in-eligible:
• $226,800 for 24 week course of Harvoni®
• $352,800 for 24 week course of sofosbuvir + Daklinza®