hib disease burden – review of literature
DESCRIPTION
Hib Disease Burden – Review of literature. Dr Raju Shah. Causes of under-five deaths India: WHO 2008. Neonatal 54% (1.003 million). Diarrhea 12.9% (0.237 million). Pneumonia 20.3% (0.371 million). Others 12.8% (0.218 million). 1.829 million under-five deaths (20.8% of world). - PowerPoint PPT PresentationTRANSCRIPT

1
Hib Disease Burden – Review of literature
Dr Raju Shah
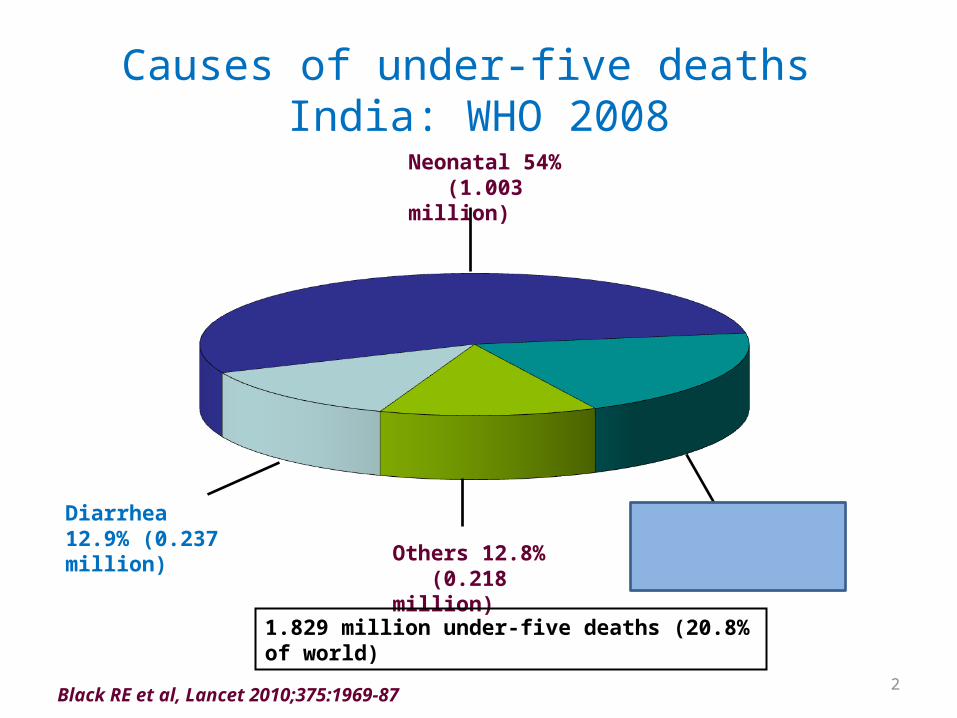
Causes of under-five deaths India: WHO 2008
Pneumonia 20.3% (0.371 million)
Diarrhea 12.9% (0.237 million)
Others 12.8% (0.218 million)
Neonatal 54% (1.003 million)
1.829 million under-five deaths (20.8% of world)
Black RE et al, Lancet 2010;375:1969-87 2

Pneumonia deaths: Top 10 countries
Black RE et al, Lancet 2010;375:1969-87
Number Country Pneumonia deaths (N) (2008)
% of world
01 India 371,605 23.5%
02 Nigeria 177,212 11.2%
03 DR Congo 112,655 7.1%
04 Pakistan 084,210 5.3%
05 Afghanistan 080,694 5.1%
726,376 52.3%
06 China 062,229 3.9%
07 Ethiopia 048,892 3.1%
08 Angola 033,078 2.1%
09 Kenya 030,406 1.9%
10 Indonesia 038,331 2.4%
Total 1,031,392 65.8%
World 1,575,257 100%
3

Clinical Pneumonia burden – Top 15 countriesCountry Predicted no. of
new cases (millions)Estimated incidence(epi/child yr)
India 43.0 0.37
China 21.1 0.22
Pakistan 09.8 0.41
Bangladesh 06.4 0.41
Nigeria 06.1 0.34
Indonesia 06.0 0.28
Ethiopia 03.9 0.35
Democratic Republic of the Congo 03.9 0.39
Viet Nam 02.9 0.35
Philippines 02.7 0.27
Sudan 02.0 0.48
Afghanistan 02.0 0.45
United Republic of Tanzania 01.9 0.33
Myanmar 01.8 0.43
Brazil 01.8 0.11
World 155.84 0.26Rudan I Bull WHO 2008;86:408-16 4

5
• In India, data on Hib particularly on population-based incidence is sparse
• There is marked variability in reported burden of Hib disease in India
• However, a number of hospital-based studies have shown that, as in other parts of the world, Hib is the most common endemic cause of bacterial meningitis in children

6
Challenges in establishing Hib disease burden
• Fastidious organism, difficult to grow• High threshold for cultures• Lack of good microbiology services• Antibiotic treatment before culture• Only severe cases reach the hospitals

7
There is marked variability in reported burden of Hib disease in India
• A study by Panjarathinam R, Shah RK. (Pyogenic meningitis in
Ahmedabad Indian J Pediatr 1993; 60:669–73) - of 135 CSF samples obtained from children with meningitis - cultures yielded no Hib organisms at all
• Study by Venkatesh VC, Steinhoff MC, Moses P, Jadhav M, Pereira SM. (Latex agglutination: an appropriate technology for the diagnosis of bacterial meningitis in developing countries. Ann
Trop Paediatr 1985; 5:33–6) have shown Hib to be a common cause of meningitis in infants and young children

8
Incidence of Hib meningitis in IndiaS. Minz, V. Balraj, M. K. Lalitha*, N. Murali**, T. Cherian**, G. Manoharan†, S. Kadirvan†, A. Joseph & M.C. Steinhoff††Indian J Med Res 128, July 2008, pp 57-64
• Prospective study• 1997 to 99 – for 24 months• Vellore district with 56,153 U5 children• 97 possible meningitis• Annual incidence Rate per 100,000 (AIR)
– (86 for 0-4y while 357 for 0 to 11 m)• 18 ABM (AIR 15.9 for 0-59 months)• 8 Hib (AIR 7.1 for 0-59m - 32 for 0-11m, - 19 for 0-23m )• Vellore study site is well-served and not typical of all of India –
Vellore data would be underestimating for most other regions* *Indian J Med Res 132, October 2010, pp 450-455
9
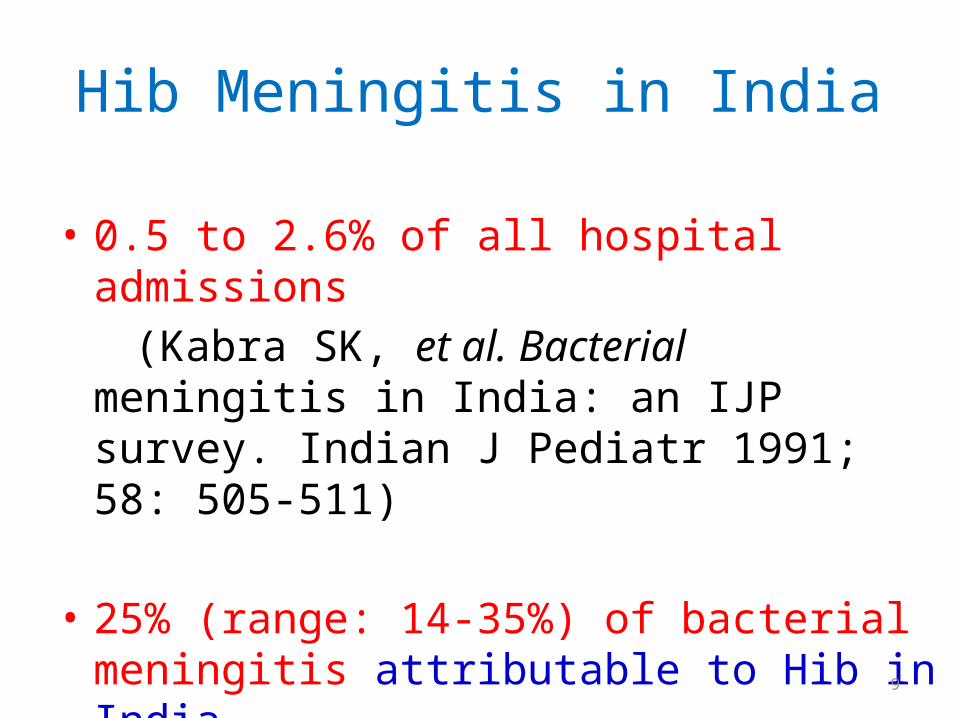
Hib Meningitis in India
• 0.5 to 2.6% of all hospital admissions (Kabra SK, et al. Bacterial meningitis in India: an
IJP survey. Indian J Pediatr 1991; 58: 505-511)
• 25% (range: 14-35%) of bacterial meningitis attributable to Hib in India
10
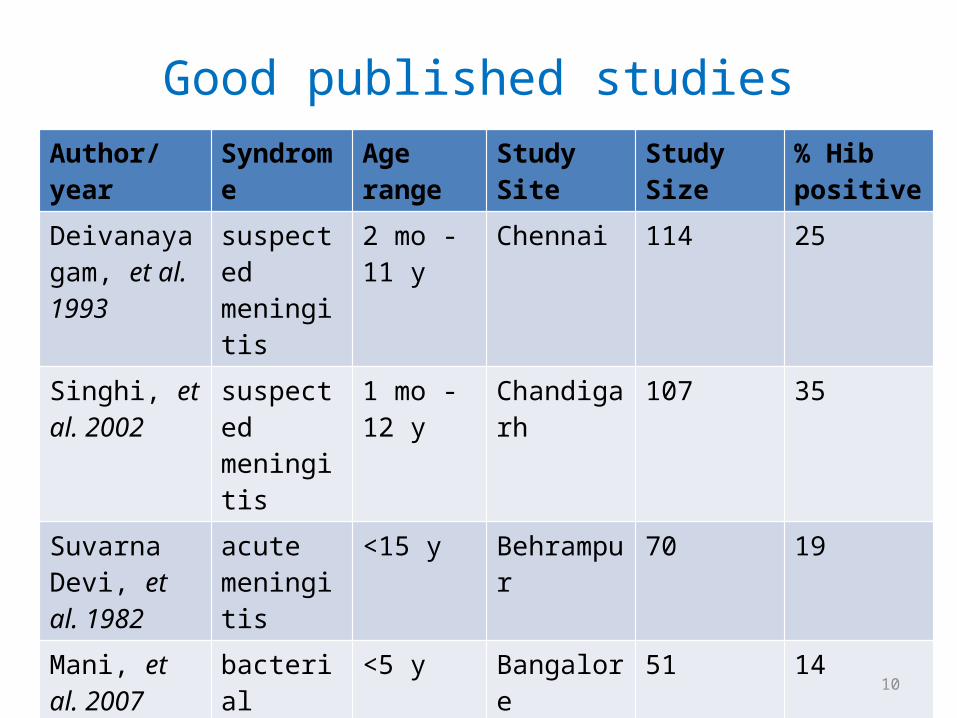
Good published studiesAuthor/year Syndrome Age range Study Site Study Size % Hib
positive
Deivanayagam, et al. 1993
suspected meningitis
2 mo - 11 y
Chennai 114 25
Singhi, et al. 2002
suspected meningitis
1 mo - 12 y
Chandigarh 107 35
Suvarna Devi, et al. 1982
acute meningitis
<15 y Behrampur 70 19
Mani, et al. 2007
bacterial meningitis
<5 y Bangalore 51 14
Chinchankar, et al. 2002
bacterial meningitis
1 mo - 5 y Pune 54 26
11
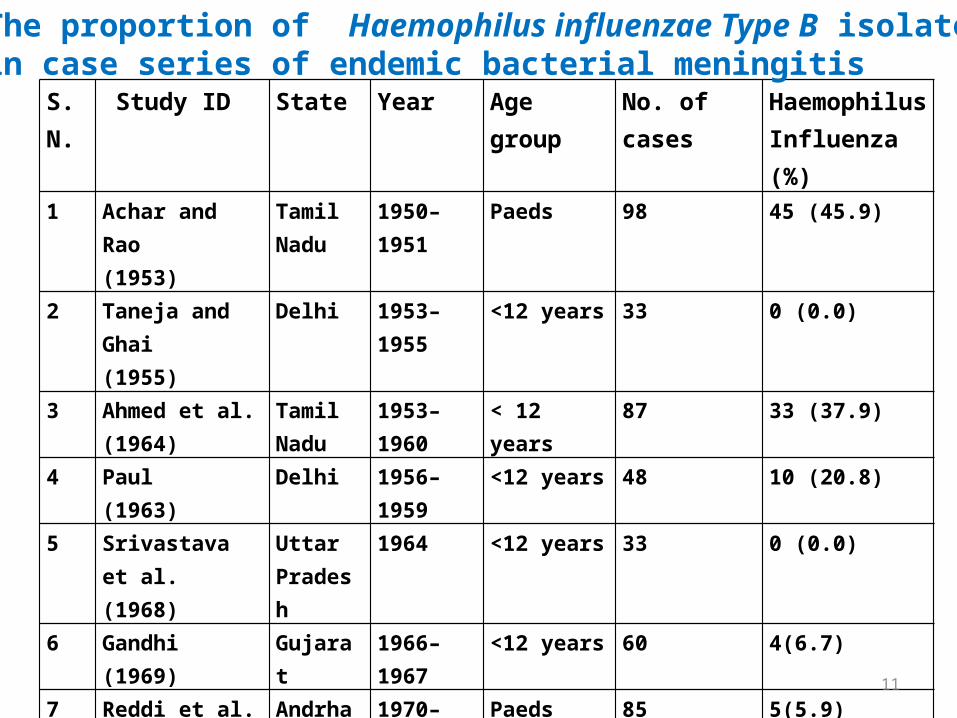
S.N. Study ID State Year Age group No. of cases HaemophilusInfluenza (%)
1 Achar and Rao (1953)
Tamil Nadu
1950–1951 Paeds 98 45 (45.9)
2 Taneja and Ghai (1955)
Delhi 1953–1955 <12 years 33 0 (0.0)
3 Ahmed et al. (1964)
Tamil Nadu
1953–1960 < 12 years 87 33 (37.9)
4 Paul (1963)
Delhi 1956–1959 <12 years 48 10 (20.8)
5 Srivastava et al. (1968)
Uttar Pradesh
1964 <12 years 33 0 (0.0)
6 Gandhi (1969)
Gujarat 1966–1967 <12 years 60 4(6.7)
7 Reddi et al. (1973)
Andrha Pradesh
1970–1971 Paeds 85 5(5.9)
8 Tamaskar andBhandari (1976)
Madhya Pradesh
1971–1972 <12 years 21 3(14.3)
The proportion of Haemophilus influenzae Type B isolates in case series of endemic bacterial meningitis

12
S.N.
Study ID State Year Age group No. of cases HaemophilusInfluenza (%)
9 Kalra and Dayal (1977)
Uttar Pradesh
1966–1969 1 month–12 years
196 0(0.0)
10 Ayyagari et al. (1980)
Chandigarh 1976–1978 Paeds 176 11(6.3)
11 Kumar et al. (1980)
Chandigarh 1977–1979 1 month–12 years
66 17(25.8)
12 Suvarna Devi et al.(1982)
Orissa 1978–1981 <15 years 70 13(18.6)
13 Pal and Sant (1982)
Maharashtra
- - 64 0(0.0)
14 Venkatesh et al.(1985)–
Tamil Nadu 1982 9 day–12 years
44 8(18.2)
15 Bhat (1991)
Pondicherry 1972–1980 Paeds 256 6(2.3)
16 Vincent et al. (1987)
Kerala 1983–1984 1 month–12 years
51 0(0.0)
The proportion of Haemophilus influenzae Type B isolates in case series of endemic bacterial meningitis (cont)
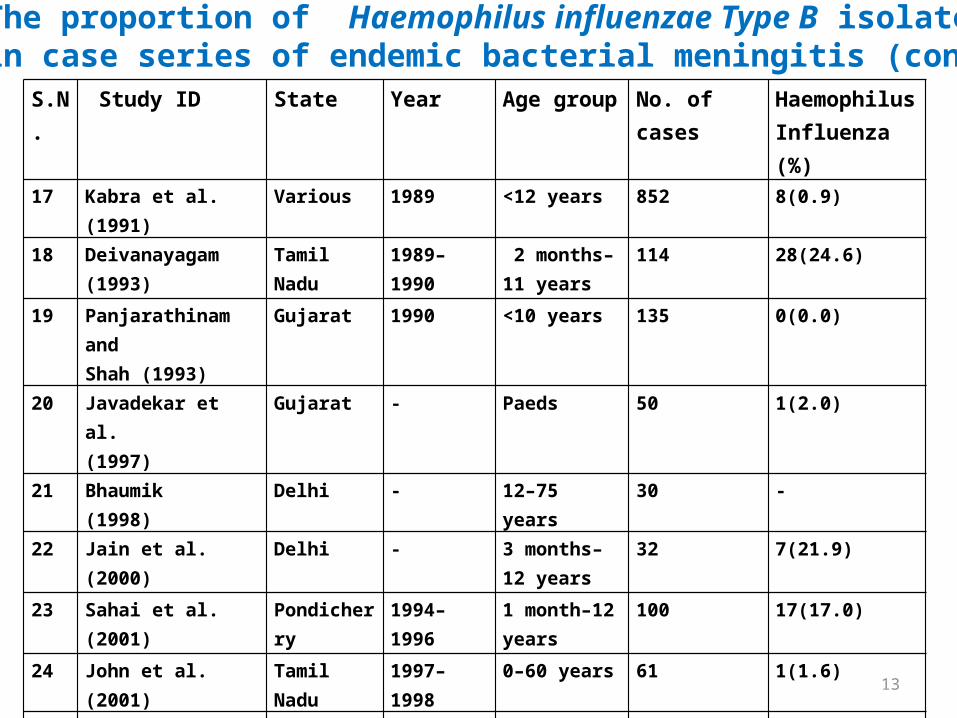
S.N. Study ID State Year Age group No. of cases HaemophilusInfluenza (%)
17 Kabra et al. (1991)
Various 1989 <12 years 852 8(0.9)
18 Deivanayagam (1993)
Tamil Nadu 1989–1990 2 months–11 years
114 28(24.6)
19 Panjarathinam andShah (1993)
Gujarat 1990 <10 years 135 0(0.0)
20 Javadekar et al. (1997)
Gujarat - Paeds 50 1(2.0)
21 Bhaumik (1998)
Delhi - 12–75 years 30 -
22 Jain et al. (2000)
Delhi - 3 months–12 years
32 7(21.9)
23 Sahai et al. (2001)
Pondicherry 1994–1996 1 month–12 years
100 17(17.0)
24 John et al. (2001)
Tamil Nadu 1997–1998 0–60 years 61 1(1.6)
25 Singhi et al. (2002a)
Chandigarh – 1 month–12 years
107 23(21.5)
26 Singhi et al. (2002b)
Chandigarh 1998–1999 3 months–12 years
69 6(8.7)
The proportion of Haemophilus influenzae Type B isolates in case series of endemic bacterial meningitis (cont)
13

S.N Study ID State Year Age group No. of cases HaemophilusInfluenza (%)
26 Singhi et al. (2002b)
Chandigarh 1998–1999 3 months–12 years
69 6(8.7)
27 Chinchankar et al.(2002)
Maharashtra
1997–1999 1 month–5 years
54 14(25.9)
28 Hemalatha et al.(2002)
Andrha Pradesh
1998–2000 1–5 years 120 6(5.0)
29 Shivaprakash et al.(2004)
Karnataka – Paeds 204 3(1.5)
30 Singhi et al. (2004)
Chandigarh 1993–1996 1–12 years 88 9(10.2)
31 Mani et al. (2007)
Karnataka 1996–2005 All ages 385 7(1.8)
32 Shameem et al. (2008)
Karnataka 2003–2007 Paeds 236 61(25.8)
33 Minz et al. (2008)
Tamil Nadu 1997–1999 0–4 years 97 6(6.2)
The proportion of Haemophilus influenzae Type B isolates in case series of endemic bacterial meningitis (cont)
14

15
Case Fatality RatesAuthor/Year Syndrome Site CFR (%)
Kabra 1991 Hib meningitis Jaipur,Jodhpur, Delhi , Kolkata
25
Steinhoff 1998 Hib meningitis Vellore 29
Thomas 2002 Hib meningitis IBIS 20
Chinchankar 2002 Hib meningitis Pune 21
Thomas 2002 Any invasive Hib disease
IBIS/1994-1997 16
CFR in Hib Meningitis – 20-29%Hib invasive disease CFR – 16%
• In ICMR study even the 0.03 per cent death rate in spite of hospital treatment amounts to 1 per cent case fatality; 50 times higher would be 50 per cent case fatality (~15 deaths/1000) – very likely if untreated *• UNICEF projection of 14 deaths due to pneumonia per 1000 under-five children is not at all inconsistent with the ICMR study data – even though they derive through different routes and from different denominators*
*Indian J Med Res 132, October 2010, pp 450-455

16
Bacterial Pneumonia
• A similar pattern is observed in Indian studies of pneumonia also
• A study by Kumar L, Ayyagari A. (The etiology of lobar pneumonia and empyema thoracis in children. Indian Pediatr 1984;
21:133–137) found no blood or pus cultures positive for Hib for 64 children with acute pneumonia or empyema,
- but 2 (8%) of 26 blood and 6 (16%) of 38 pleural fluid specimens were positive for Hib by use of antigen detection methods

17
Hib Pneumonia in India Author/Year Syndrome Location Age Study Size % disease
due to Hib %
isolation rate of any organism
Bahl 1995 Pneumonia Delhi 0-5 years 110* 19 55
Kumar 1984 Pneumonia Chandigarh
< 11 years 64* 13 42
Patwari 1996
Pneumonia Delhi < 12 years 132* 15 88
13% to 19% of pneumonia and LRTI due to Hib
18
Multi-center surveillance for pneumonia & meningitis among children (<2 yr) for Hib vaccine probe trial preparation in India Indian J Med Res 131, May 2010, pp 649-658
• Chandigarh, Vellore, Kolkata• 18 m to 24 m – N 17951• Enrollment from July 05 to Dec 06• Parents explained about s/s of pneuonia and
meningitis• Pneumonia and meningitis admitted to
hospitals also enrolled• CSF culture, PCR, LAT, Bl culture, CXR

19
• Severe clinical pneumonia– 2717 to 7890 per 100,000 child-years
• Suspected meningitis – 1971 to 2433 per 100,000 child-years
• NP carriage – 6 to 7.6 %
• Incidence of clinical pneumonia comparable with other studies from India and a higher incidence of suspected meningitis

20
Drug Resistant Hib
• 1st cases of Drug resistant Hib from Chandigarh (1990)1
• Vellore study (1992) reported – 42.5% of Hib isolate MDR strains2
• Nagpur study (1996) reported – 80% MDR srains3
• IBIS (1999) reported – 56% resistance to Chloramphenicol - 40% resistance to Ampicillin4
1. Singh N et al. Multiple resistant Hib meningitis. Indian Pediatrics 1990;27:502-04. 2. John TJ et al. Hib disease in children in India.Pediatric Infec Dis J. 1998;17(9):5169-71 3. Agarwal v et al. Characterisation of invasive hemophilus Influenza isolated in Nagpur,
Central India. Indian J Med Res. 1996;103:296-98 4. Invasive Hemophillus Influenza disease in India: a preliminary report of prospective
multihospital surveillance IBIS. Pediatr Infect Dis J. 1998; 17:3172-75

21
HIB-Multicentric Study (IBIS)Antimicrobial % of Isolates agents Resistant Intermediate Total Ampicillin 33 7 40 Cefotaxime 0 0 0 Chloramphenicol 43 10 53 Trimetho.-sulfamethox 38 3 41 Erythromycin 5 33 38
Antibiotic Resistance of 57 Haemophilus influenzae isolates from 6 IBIS centres, 1993 to 1995

22
Nasopharyngeal Carriage• Hib nasopharyngeal carriage among infants was
found to be common in India• Study from Chandigarh, researchers found
11.2% of 1000 children below 2 years were carriers of H. influenza - 69% belonged to type b and the rest were non-typable*
• Hib carriage rates increases throughout infancy and into the second year of life, peaking at age 18-21 months at a prevalence of 20.3%*
* Sekhar S, Chakraborti A, Kumar R. Haemophilus influenzae colonization and its risk factors in children aged <2 years in northern India. Epidemiol Infect. 2009; 137:156-60

23
Estimates
• From available studies reviewers estimated that there may be as many as 75 to 100 cases of meningitis caused by this organism per year per 100,000 children <5 years of age1
• Hib vaccine probe - total pneumonia cases caused by Hib would be 2,083,333 or 2 million cases per year. These are crude extrapolations from the multi-centre study2
1. John TJ, Cherian T, Raghupathy P. Haemophilus influenzae disease in children in India: a hospital perspective. Pediatr Infect Dis J 1998; 9: S169–712. Gupta M, Kumar R, Deb AK, Bhattacharya SK, Bose A, John J et al. A multi-centre surveillance for pneumonia and meningitis among children (<2 yr) for Hib vaccine probe trial preparation in India. Indian J Med Res 2010; 131; 649-658.

24
Prospective culture based studies for pneumonia in world
• Pneumococcus: 30-50%• Hib: 10-30%• Others:
– NTHi: • New Papua Guinea (Lung culture)• Pakistan (Blood isolates)
– S. Aureus: • Chile (Lung aspirate)• WHO 42% (Blood aspirate)
– Non-typhoid salmonella: • Africa, Malawi (severe pneumonia)
• Viruses: 30-50% – RSV: 15-40%– Others:
Rudan I Bull WHO 2008;86:408-16

25
Vaccine probe studies
• Pneumococcus and Hib are two important vaccine preventable causes of pneumonia
• Vaccine effectiveness against radiological proven pneumonia studies in developing countries– Hib: 15-30% (Hib conjugate vaccine)
Rudan I Bull WHO 2008;86:408-16

26
3 Hib probe studies• Pilot or Probe introduction of specific vaccine,
with measurement of syndromes pre-and post-vaccination, necessary to quantify the pre-vaccination prevalence/incidence
• Gambia , Chile, Indonesia– 21- 23% of hospitalized pneumonia cases with
radiographic infiltrates were prevented
27
Hib impact studies
• >95% efficacy- Europe, US and Gambia• Also in Chile, Brazil, Columbia, Kenya, Malawi• Lombok
– Measurable impact on clinical pneumonia but no impact on radiological pneumonia
• Bangladesh (SEA)– Meningitis reduced by 90% – Radiological pneumonia reduced by 16-32%
28
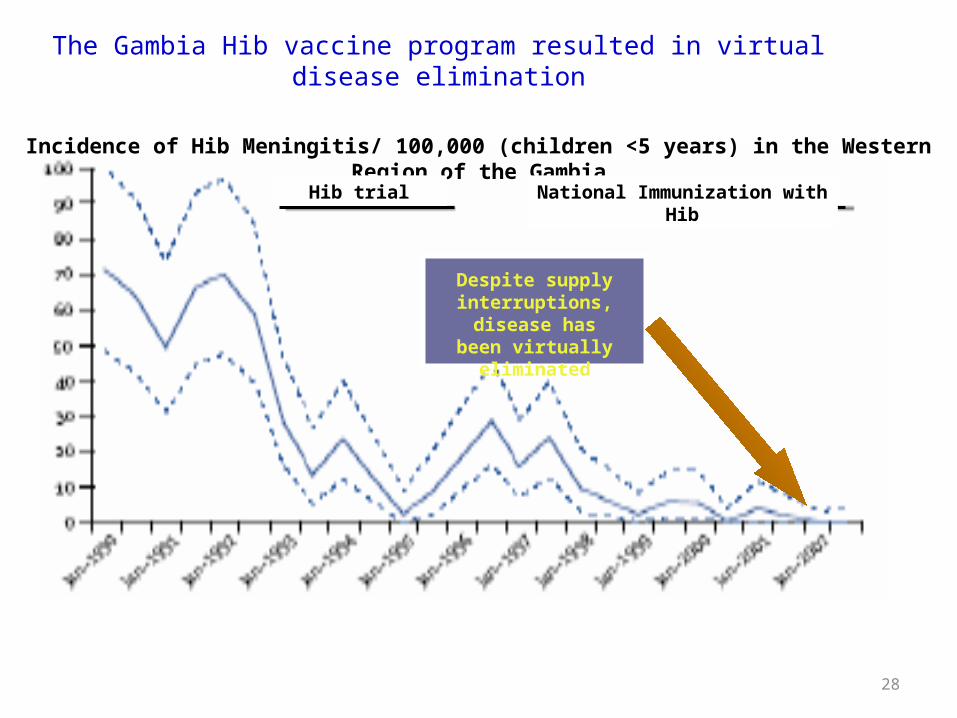
The Gambia Hib vaccine program resulted in virtual disease elimination
Adapted from Adegbola R et al. Lancet, 2005
Incidence of Hib Meningitis/ 100,000 (children <5 years) in the Western Region of the Gambia
Despite supply interruptions, disease
has been virtually eliminated
Hib trial National Immunization with Hib

0
20
40
60
80
100
120
140
160
180
1996 1997 1998 1999 2000
CA
SE
S
0
2
4
6
8
10
12
INC
IDE
NC
E
Cases Incidence/100,000
Hib Cases and IncidenceCHILE, 1996-2000
Children <5 years of age
Source: Notificación Obligatoria, MINSAL. 29

30
WHO statement
The lack of local surveillance data should not delay the introduction of the vaccine especially in countries where regional evidence indicates a high burden of disease

31
THANKS