high altitude illness richard dionne md emergency medicine – university of ottawa march 2013
TRANSCRIPT
High Altitude Illness
Richard Dionne MDEmergency Medicine – University of Ottawa
March 2013

High Altitude Illness
• Goals & Objectives
• Understand the principles of acclimatization
• Discuss the clinical presentation, prevention and interventions for Acute Mountain Sickness
• Discuss the clinical presentation, prevention and interventions for High Altitude Pulmonary Edema (HAPE)
• Discuss the clinical presentation, prevention and interventions for High Altitude Cerebral Edema (HACE)
Case
You are going on a skiing vacation at Vail, Colorado.
On day 2 you feel tired, lightheaded and a mild headache. You attribute it to accumulated stress and fatigue that is getting back at you.
Could it be all the partying ???

Acute Mountain Sickness« A.M.S.»
Rapid ascension & non-acclimatized Feels like «Hangover» & «viral illness» Close to 25% visitors to Colorado Better in 2 - 7 days Danger : « H.A.P.E. » / « H.A.C.E. » Altitude ...
Moderate > 8000 feet (> 2500 m)High > 10 000 feet (> 3000 m)Extrême > 18 000 feet (> 5500 m)
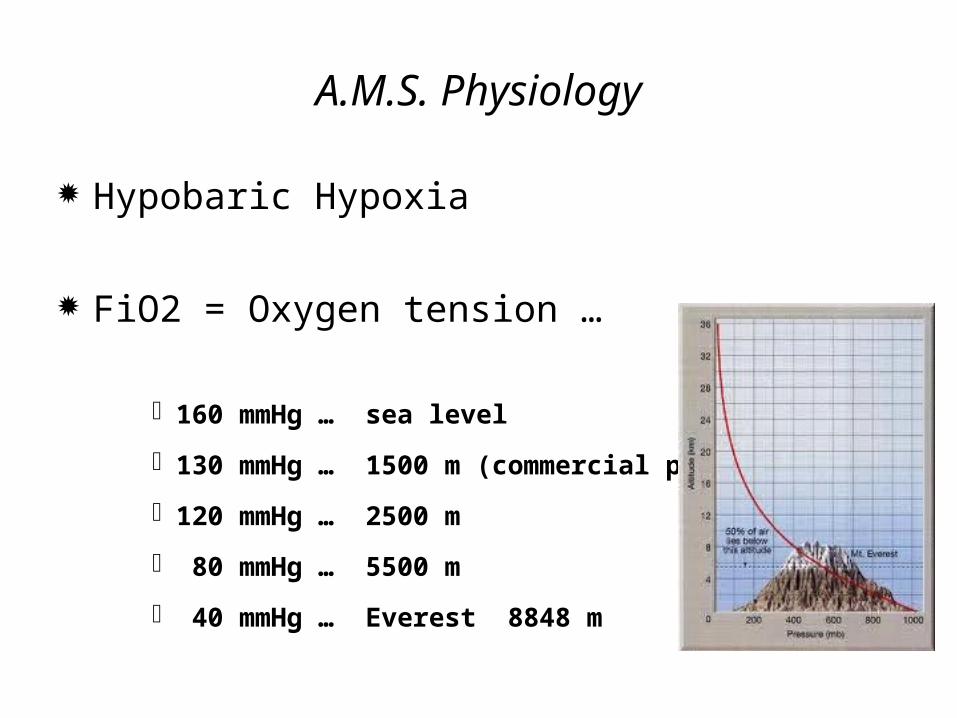
A.M.S. Physiology
Hypobaric Hypoxia
FiO2 = Oxygen tension …
160 mmHg … sea level
130 mmHg … 1500 m (commercial plane)
120 mmHg … 2500 m
80 mmHg … 5500 m
40 mmHg … Everest 8848 m
Video
Prevention of A.M.S.
Staged ascent
No alcohol & tobacco
Normal Hydration
High carbohydrate diet
Diamox prophylaxis
Staged Ascent Recommended > 8000 feet (2500 m)
Above 3000 m …
Do not sleep higher than 1000 feet (300 m) from previous night …
Suggest one day ( 2 nights ) extra of acclimatisation at every 3000 feet (1000 m) … thereafter
Diamox
Anhydrase carbonate inhibitor
Induces HCO3 diuresis causing a metabolic acidosis
Reflex Ventilation & Oxygenation … simulates : HVR
« Hypoxic Ventilatory Response »
Case
You and 3 of your friends decide to ascend Mont Aconcagua in Argentina. Your altitude is now 14000 feet, (4200 m) on your 6th day.
For the last 2 days you ’ve started a dry cough, that is getting worse as the day progresses.
High Altitude Pulmonary Edema« H.A.P.E. »
1-2% when > 12 000 feet
Diagnosis …
cough / dyspnea / bronchospasm / performance / pulmonary edema …
usually day 2 …
Non-cardiogenic pulmonary edema: pulmonary artery pressure ( P.A.P.) but normal wedge & L.V.E.F.
«H.A.P.E.»
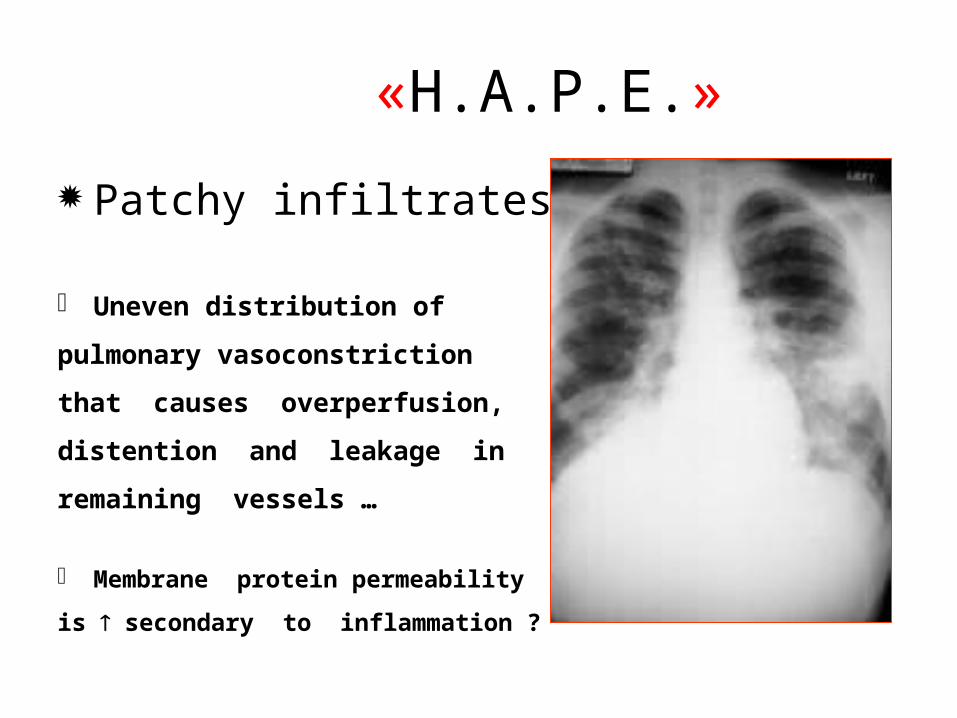
Patchy infiltrates ?
Uneven distribution of
pulmonary vasoconstriction
that causes overperfusion,
distention and leakage in
remaining vessels …
Membrane protein permeability
is secondary to inflammation ?
Treatment
Reheat victim « P.A.P.» Oxygen « SaO2 & P.A.P. » Descent : 1500-3000 feet / Hyperbaric ? C-Pap ? Medication …
Nifedipine (Adalat) 10 mg, then 30 mg SR Bid … « PAP 30-50%»
+/- Diamox Lasix & Morphine ? (non-cardiogenic)
Case
Having decided to go down, you are still in contact with your friends that are now at 16 000 feet, they plan to summit tomorrow am …
One of your teamates as been having an increasing headache and feels unsteady, he may not try to summit but wants to wait for their return ???

High Altitude Cerebral Edema« H.A.C.E »
Usually > 12 000 feet Usually takes 1-3 days Ataxia / headache / N° V° / seizures
Mecanism Vasogenic edema :
« capillary leak syndrome »
Cytotoxic edema : ( Secondary ) « sodium - potassium pump failure »
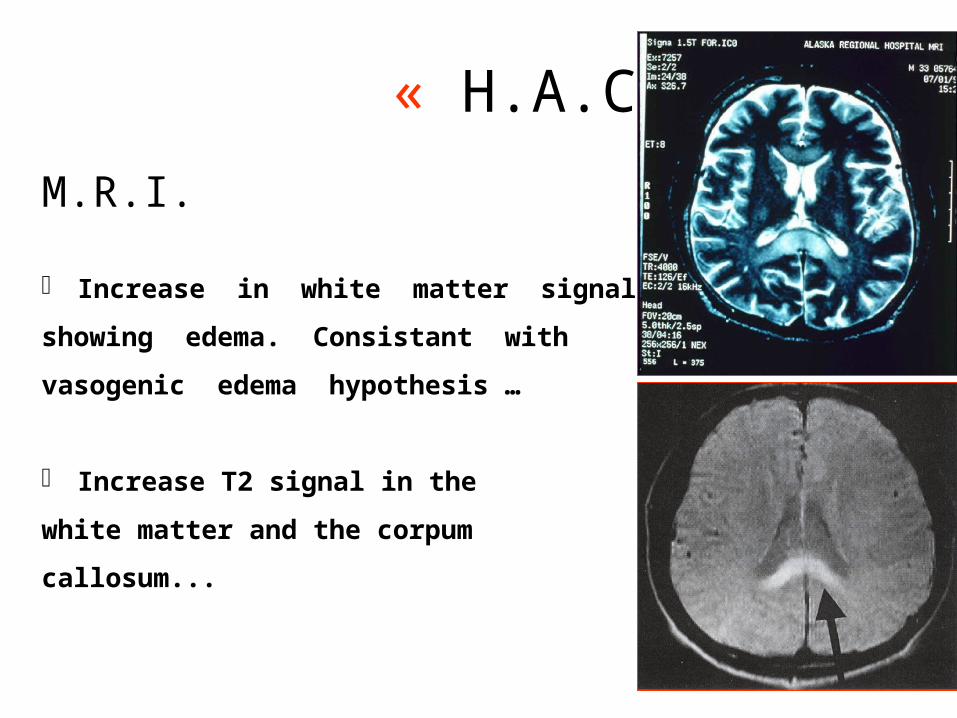
« H.A.C.E »
M.R.I.
Increase in white matter signal
showing edema. Consistant with
vasogenic edema hypothesis …
Increase T2 signal in the
white matter and the corpum
callosum...
« H.A.C.E. »Predisposing factors
1- Rapid ascent : acclimatisation
2- Hypoventilation
3- Gas exchange alterations
4- Fluid retention
5- Individual disposition
1- Acclimatisation
Hypobaric hypoxemia
Alveolar hypoxemia
Arterial hypoxemia
Directly related to speed of ascent...

2- Hypoventilation
Hypoxic Ventilatory Response «H.V.R.»
Initially … Ventilation / Oxygenation & PaO2
Counter balanced … renal excretion of HCO3 in response to hypocapnia & alcalosis
of hyperventilation
H.V.R.= acclimatisation determinant factor
3- Gas exchange alterations Blood adaptation…
erythropoietin / RBC ’s (4-5-days) 2,3-DPG = right shift oxyhemoglobin curve Resp. alkalosis = left shift oxyhemoglobin curve
Interstitial Pulmonary edema... A-a gradient & hypoxemia
In consequence …Vital Capacity … diminishedDiffusion capacity … diminishedV/Q mismatch … elevatedPulm. Artery Press. … elevatedPulm. Vasc. Resistance … elevated
4- Fluid retention
Acclimatised « reset » of osmolar neurocenter …
ADH suppression & Aldosterone … 25% diastolic volume
circulating endogenous norepinephrine
Non-acclimatized antidiuresis with ADH & Aldosterone still elevated
fluid retention and cerebral edema ...
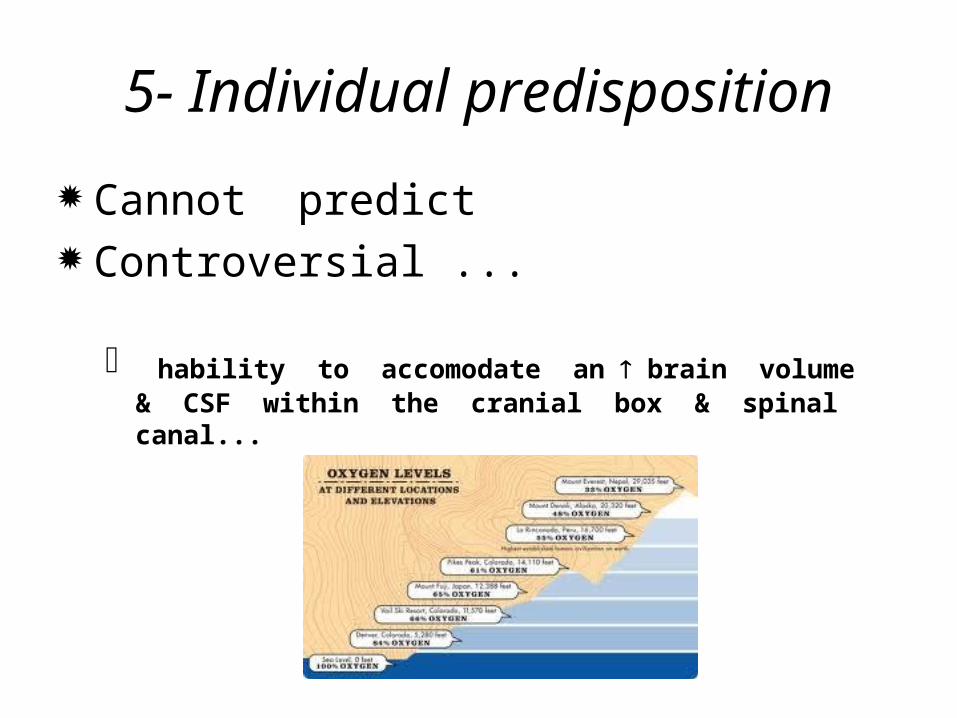
5- Individual predisposition
Cannot predict Controversial ...
hability to accomodate an brain volume & CSF within the cranial box & spinal canal...
Treatment
1- Hypoxemia / Oxygenation
2- Control Acclimatisation
3- Cerebral edema
« capillary leak syndrome »
4- Symptomatic relief
Treatment1- Hypoxemia & Oxygenation
Minimum descent 1500-3000 feet as much as needed
Oxygen 100%
Hyperbaric Chamber portable Gamow / Zertec / P-portable
can generate pressures 200mmHg (7000 feet / 2000 m descent)...
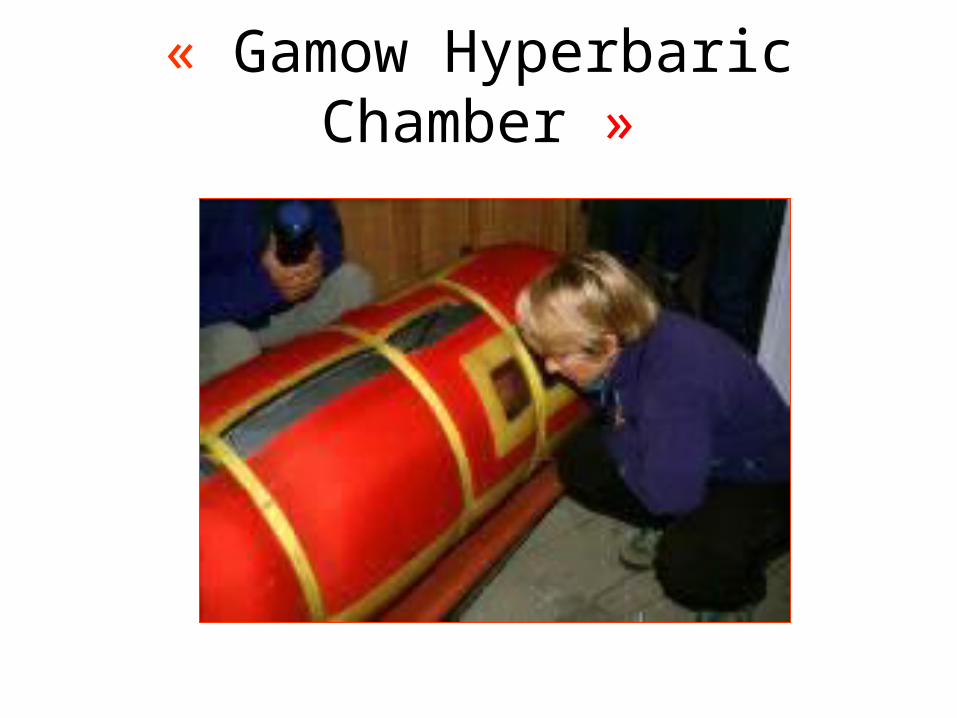
« Gamow Hyperbaric Chamber »
Treatment2- Controlled Acclimatisation
Acetazolamide ( Diamox)
125-250 mg q 12h (2,5mg/Kg) diuresis / CSFstimulated « H.V.R.» ( ventilation )
Start 1-2 days before ascent & continue for 48h …
Gives paresthesias ++ / sulpha allergy
Treatment3- Cerebral Edema
Dexamethasone4-8 mg stat, then 4 mg po / IM / IV q 6hno role in acclimatisation
DiureticsAcetazolamide (Diamox)Furosémide (Lasix)
Mannitol & Hyperventilation exceptionnaly if severe
Treatment4- Symptomatic relief
Analgesic acetaminophen / ASA / codeine ?
Anti-emetics prochlorperazine (Stemetil)
HVR ?
Ginko Biloba as prophylaxis ???
Take Home ...
A.M.S. : can ressemble viral illness...
H.V.R. : determinant factor for acclimatisation ...
H.A.P.E. : non-cardiogenic pulmonary edema / treatment = descent & O2...
H.A.C.E. : subtil cerebellar ataxia … the cerebellum is very sensitive to hypoxia ...