high risk of cardiac events in hypertrophic cardiomyopathy
TRANSCRIPT

High risk of cardiac events in hypertrophic cardiomyopathy patients with double/compound heterozygosity
Serio A, Pasotti M, Gambarin F, Pilotto A, Serafini E, Diegoli M, Grasso M, Tagliani M, Disabella E, Arbustini E
Centre for Inherited Cardiovascular Diseases
IRCCS Fondazione Policlinico San Matteo, Pavia
Italy
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
Background
• Hypertrophic Cardiomyopathy (HCM) is caused by mutations of genes coding:– sarcomeric proteins (sarcomeric HCM)
– non sarcomeric proteins (non-sarcomeric HCM)
with considerable genetic heterogeneity and variability in phenotypic
expression.
• Major complications are sudden cardiac death (SCD) and evolution through left ventricular dilatation and dysfunction.
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
Marian AJ et al. J Mol Cell Cardiol 2001Seidman CE et al. Basic Res Cardiol 1998
Maron BJ. JAMA 2002
Background
• Most HCM are autosomal dominant, associated with a single heterozygous mutation of one disease gene. A minority is associated with double or combined heterozygosity.
• When all known disease genes are systematically screened in consecutive patients, a minority of cases show double/triple or compound heterozygosity.
• The prevalence of these latter cases is still provisional.• Phenocopies (drug toxicity such as chloroquine) may clinically
mimic HCM.
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
Kwon JB et al. J Clin Reumatol 2010Keating RJ et al. J Am Soc Echocardiogr 2005
Arbustini E et al. Heart 1998Girolami F et al. J Am Coll Cardiol 2010

Background Compound or double heterozygosity
• First implication: genetic screening should systematicallyinclude at least major disease genes
• Second implication: in the families reported by Richard et al.the age of onset, the degree of hypertrophy or the prognosisare related to the number of mutations.
• Compound or double heterozygosity (5%, 4/80 pts) wasassociated with more severe clinical phenotype (more severehypertrophy, more frequent sudden death)
→ CMGCV: genetic diagnosis in families without co-segregationby age is provided as non-conclusive
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
Richard et al. Eurogene Heart Failure Project. Circulation 2003
Ingles et al, Seidman, J Med Genet 2005

Purpose
• We aimed at determining the prevalence of double or compound heterozygosity in a consecutive series of genotyped families with HCM and analyzing their outcome during a mean follow-up of 87±65 months
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia

Methods
• Population: 495 mutated patients
– 188 unrelated probands
– 307 relatives
(December 2009)
• HCM diagnosis:
– done according to the WHO criteria
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
Methods
Clinical and instrumental evaluation: • physical examination• ECG• Echocardiography• Holter ECG monitoring• biochemical testing: sCPK, lactic acid, Troponin• neuromyological examination• coronary angiography• electrophysiology study, right catheterization• endomyocardial biopsy (when clinically indicated)
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
for probands and relatives
Methods
Genetic testing:– genetic testing was performed after counselling and
written informed consent.
– MYH7, MYBPC3, TNNT2, TNNI3, tCAP, MYL2, TPM1, MYH6, MYL3, MYO6, and MYOZ1 were routinely screened, while LAMP2, PRKAG2 and mtDNA were screened in the presence of specific clinical markers
• Patients with Anderson-Fabry disease were excluded.
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia

Results
• Out of the 495 mutated individuals:
– 361 affected (73%)
– 134 healthy carriers (27%)
• The mean age of affected members was significantly higher compared to those of the healthy carriers
34.3 ± 15.2 versus 26.9 ± 15.3 years (p=0.003)
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
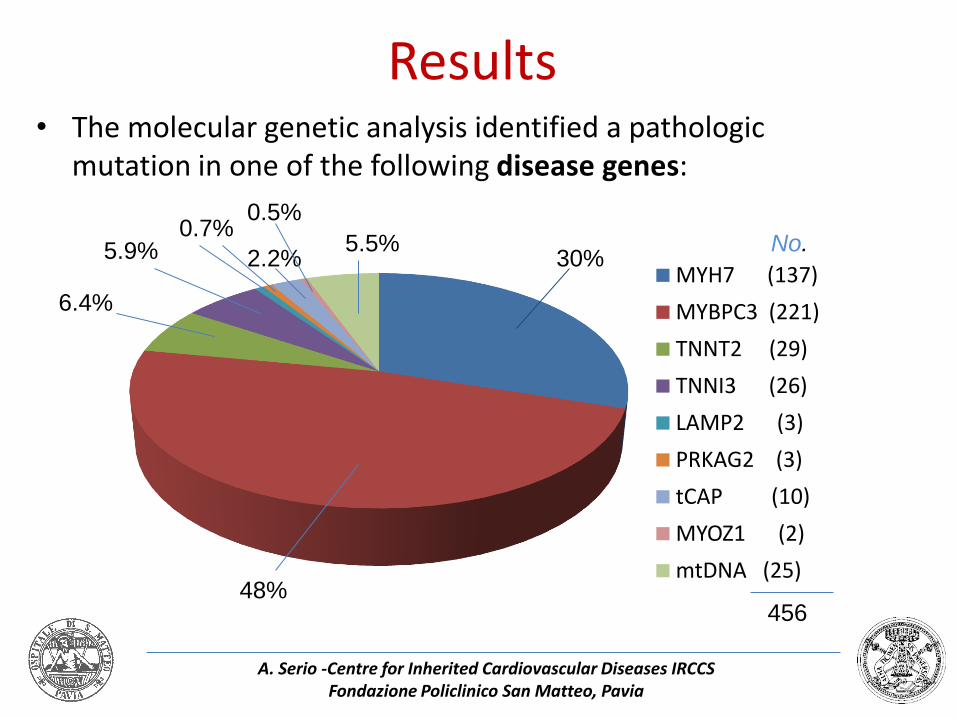
Results• The molecular genetic analysis identified a pathologic
mutation in one of the following disease genes:
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
MYH7 (137)
MYBPC3 (221)
TNNT2 (29)
TNNI3 (26)
LAMP2 (3)
PRKAG2 (3)
tCAP (10)
MYOZ1 (2)
mtDNA (25)48%
30%
6.4%
5.9% 5.5%2.2%
No.
456
0.7%0.5%
Results
• 39 patients (7%) were found to carry a compound or double heterozygosity.
• Among the patients with double or compound heterozygosity:
– 37 were affected (95%)
– 2 were young healthy carriers (13 and 15 y.o.)
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia

EVENTS IN THE OVERALL GENOTYPED HCM PATIENTSAfter 87±65 months:
79 of 361 (22%) phenotypically affected HCM patients had one of the following events:
12 20 4 43
Results
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
No.
%
Results
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
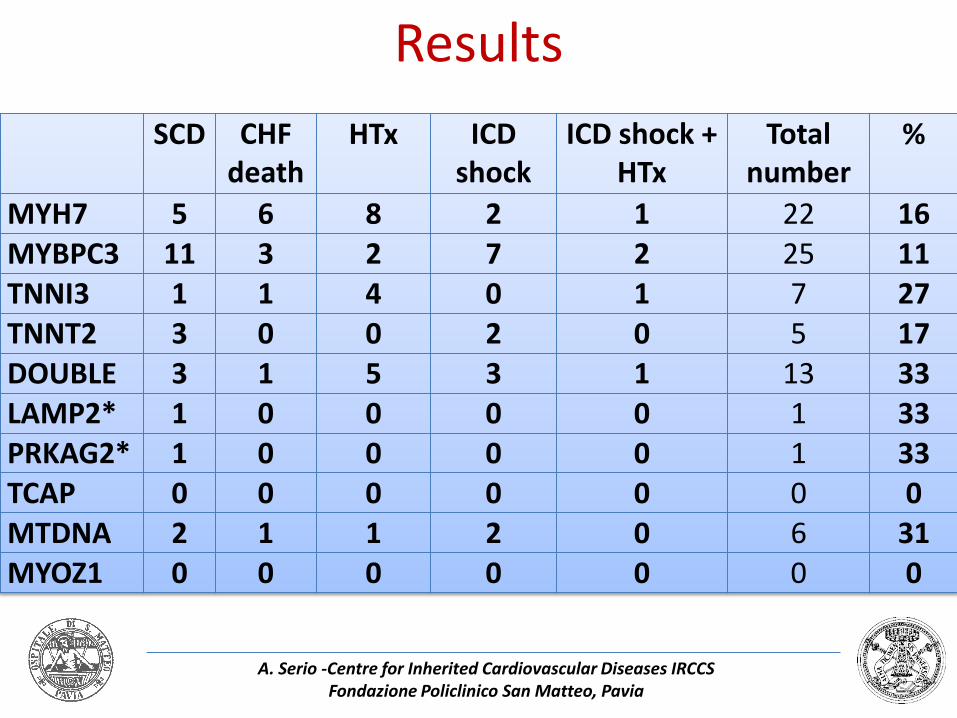
SCD CHF death
HTx ICD shock
ICD shock + HTx
Total number
%
MYH7 5 6 8 2 1 22 16
MYBPC3 11 3 2 7 2 25 11TNNI3 1 1 4 0 1 7 27TNNT2 3 0 0 2 0 5 17
DOUBLE 3 1 5 3 1 13 33LAMP2* 1 0 0 0 0 1 33PRKAG2* 1 0 0 0 0 1 33TCAP 0 0 0 0 0 0 0
MTDNA 2 1 1 2 0 6 31MYOZ1 0 0 0 0 0 0 0

Genes No. %
Double MYBPC3 16 41.1
MYH7+ MYBPC3 11 28.2
MYH7+ mtDNA 6 15.4
MYH7 + double MYBPC3 4 10.2
tCAP + mtDNA 2 5.1
39 patients (7%)
with double or compound heterozygosity
39
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
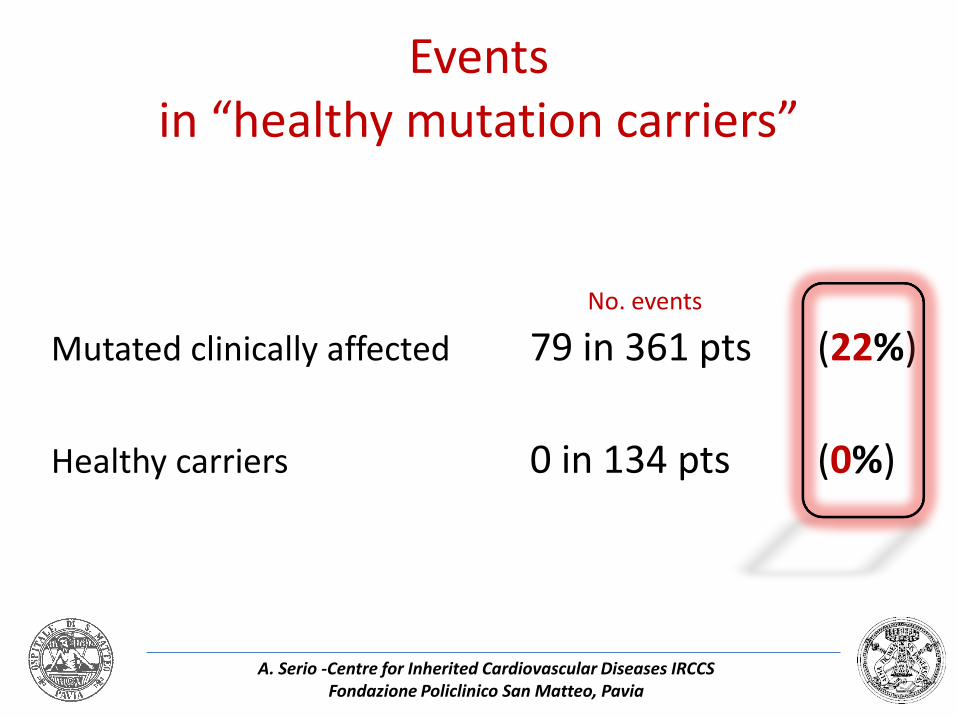
Eventsin “healthy mutation carriers”
No. events
Mutated clinically affected 79 in 361 pts (22%)
Healthy carriers 0 in 134 pts (0%)
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia
Conclusions
• The prevalence of double/compound heterozygosity in our series was 7%.
• The rate of complications and malignant evolution was higher in HCM associated with double/compound mutation (higher rate of adverse events in a shorter period of time).
A. Serio -Centre for Inherited Cardiovascular Diseases IRCCS Fondazione Policlinico San Matteo, Pavia

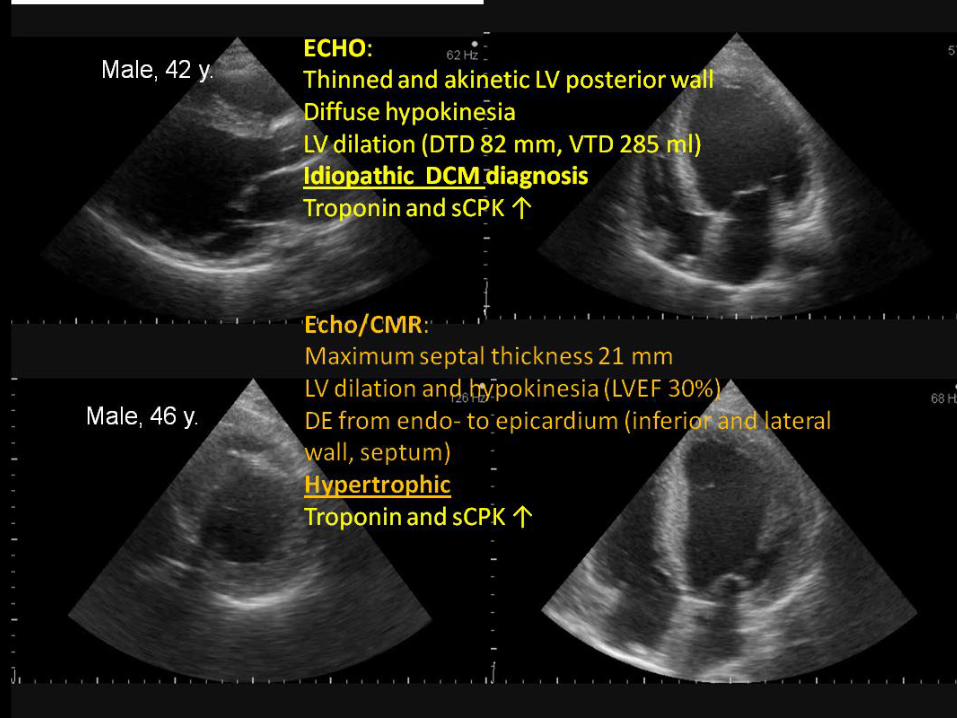
In the clinical practice…
• Male, 42 y.
• Idiopathic DCM (coro -)
• acute heart failure episodes
• ICD implantation
FIRST EXAMPLE: same family, two brothers…
Similar ecg…but different diagnosis
• Male, 46 y.
• HCM

Molecular diagnosisAnalysis of sarcomeric genes for HCM:
MYBPC3 mutation found: Asp228Asn 1Both in the proband and in the younger brother
1 Andersen, Eur J Hum Genet 2004
Family screening:
+ -
- + +
-
An additional known mutation wasfound in mtDNA in the mother and in the three sons
+/- -/+
-/+ +/+ +/+
-/-mtDNA DEFECTS
a. as unique cause of cardiomyopathy
b. as modifier or co-causative of the phenotype
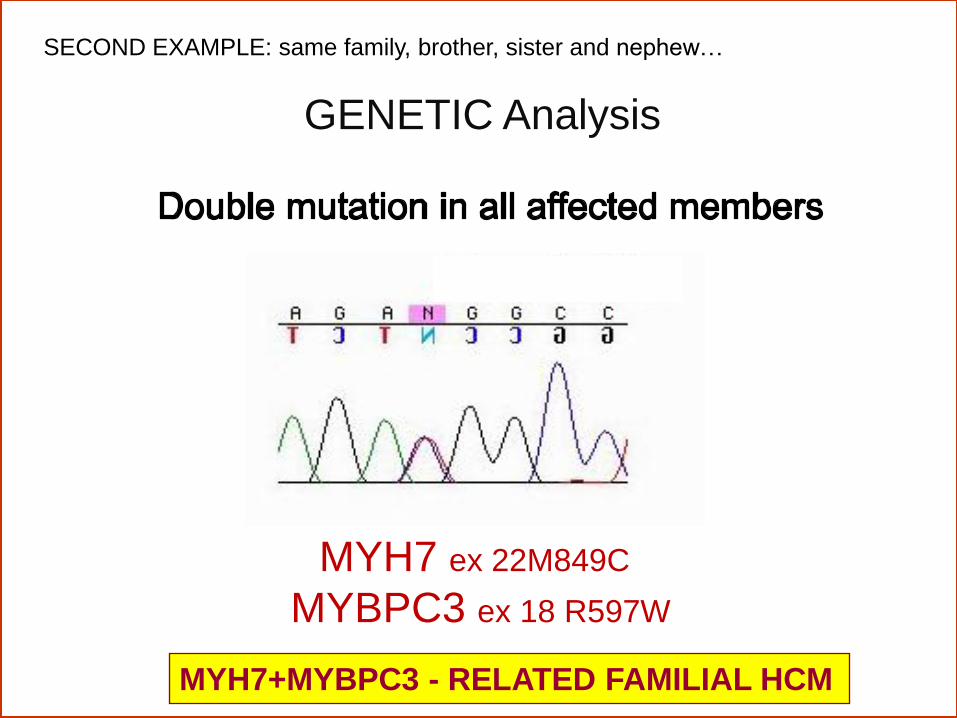
MYH7 ex 22M849C
MYBPC3 ex 18 R597W
GENETIC Analysis
MYH7+MYBPC3 - RELATED FAMILIAL HCM
SECOND EXAMPLE: same family, brother, sister and nephew…

• proband with HCM evoluted in dilated form with LV
dysfunction and CHF, heart transplanted (52 y.)
• mother “with cardiac problems” (HCM?)
• sister with HCM, initial LV dysfunction
• nephew with HCM
FAMILY HISTORY
?

proband
nephew
sister

LV enlargement
LV progressive dysfunction (EF 25%)
Loss of hypertrophy (12 mm)
progressive atrial enlargement
Nephew
EF 50%
Septum 21 mm
Sister
EF 40%
Septum 14 mm

Thank you