histological appearances of the gastric years after ... · lesion stoma lesser curve no. % no. %...
TRANSCRIPT
Journal of Clinical Pathology, 1979, 32, 179-186
Histological appearances of the gastric mucosa15-27 years after partial gastrectomy
ANN SAVAGE AND S. JONES
From the Departments ofPathology and Surgery, Southmead Hospital, Bristol, UK
SUMMARY Sixty-three patients, who had had a partial gastrectomy 15-27 years previously, were
examined by endoscopy and multiple mucosal biopsies. No patient had a completely normal gastricmucosa; they showed varying degrees of gastritis, intestinal metaplasia, and dysplasia; 21 % hadsignificant dysplasia, and these are regarded as an 'at-risk' group requiring frequent follow-upexaminations. One patient had severe dysplasia (carcinoma-in-situ), but no case of infiltratingcarcinoma was found.
Carcinoma of the gastric stump as a late complica-tion of resection for benign disease is a well-recog-nised clinical entity (Saegesser and James, 1972;Morgenstern et al., 1973). There have been a numberof reports of an increased incidence of stumpcarcinoma compared with carcinoma in the normalpopulation (Krause, 1958; Schrumpf et al., 1977),although some authors have drawn the oppositeconclusion (Liavaag, 1962). Opinions also vary overwhether the nature of the original disease or the typeof operation performed is significant (Helsingen andHillestad, 1956; Stalsberg and Taksdal, 1971;Domellof et al., 1976). Some authors (Domellbfet al., 1977b; Schrumpf et al., 1977) have recom-mended endoscopic follow-up on all patients 20years after gastric surgery. We have examined byendoscopy and gastric biopsy a group of patientswho had undergone partial gastrectomy 15-27 yearspreviously. Our aims were to determine the incidenceof carcinoma of the stump, to identify, if possible, ahigh-risk group among the patients, and to study thehistological appearances of the mucosa of thestomach remnant.
Patients and methods
During the years 1951-63 (15-27 years previously) 224patients under the care of one surgeon had had agastric resection for benign ulcer performed atSouthmead Hospital; 115 (51 %) who were still aliveand living in the area were traced and offeredgastroscopy, and 65 (29%) accepted (Table 1).
Received for publication 31 July 1978
Table 1 Clinical data
Original number of patients 224Number traced 115Number submitted to biopsy 63Biops~v patients:Mean age (years) 64
(range 41-85)Original diagnosis: Duodenal ulcer 46
Gastric ulcer 17Type of operation: Billroth I 21
Billroth II 42
None had symptoms sufficiently severe to present totheir doctors and most were asymptomatic. All thepatients were endoscoped by one examiner (SJ) andfour to five biopsy specimens were taken from aroundthe stoma and a further four to five from elsewherein the stomach, usually the lesser curve. Furtherspecimens were taken from any visible lesion. Twopatients reacted adversely to endoscopy and nospecimens were obtained. All the specimens werefixed in formol saline and embedded in paraffin.Five-micron sections at three levels were cut fromeach block and stained with haematoxylin andeosin. An extra section at the second level wasstained with a combined periodic acid-Schiff/alcianblue method. All the histological material wasexamined by one of us (AS) without knowledge ofthe endoscopic appearances, and later reviewedwithout knowledge of the previous report, to arriveat a final diagnosis. The histological appearanceswere classified according to the following criteria:
ACUTE GASTRITISA significant infiltration of neutrophil leucocytes in
179
on 26 June 2019 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.2.179 on 1 F
ebruary 1979. Dow
nloaded from

180
the mucosa was regarded as acute gastritis. A cryptabscess or similar collection of neutrophils wasconsidered significant. Usually the acute inflamma-tion was associated with a considerable chronicinflammatory cell infiltrate.
CHRONIC GASTRITISOur classification is based on that of Lambert (1972).
Chronic superficial gastritis (mild gastritis)The gastric mucosa is of normal depth with noatrophy of specialised cells. There is increasedchronic inflammatory cell infiltration, usually con-fined to the luminal third of the mucosa butoccasionally found more deeply (Fig. 1).
Chronic atrophic gastritis (moderate gastritis)There is infiltration of chronic inflammatory cellsthroughout the lamina propria of varying degree.The mucosa is reduced in depth due to partial atrophyof specialised cells, which are partly replaced byundifferentiated cells. The lesion may be diffuse orfocal (Fig. 2).
Ann Savage and S. Jones
Gastric atrophy (severe gastritis)There is complete atrophy of specialised cells withpartial replacement by undifferentiated cells. Themucosal depth is markedly diminished. Inflammatorycell infiltration is commonly slight, but the lesion isfrequently focal and mixed with atrophic gastritis; inthat case the inflammation is more pronounced(Fig. 3).
INTESTINAL METAPLASIAThe presence of goblet cells containing mucinstaining positively with alcian blue was the patho-gnomonic feature of intestinal metaplasia. Panethcell metaplasia was frequently present in addition.
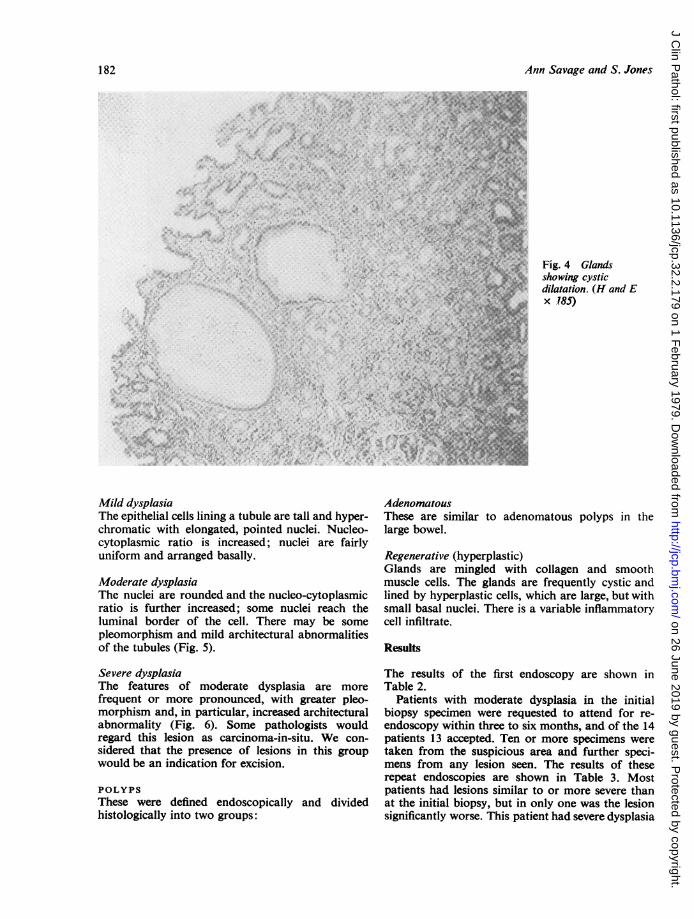
CYSTIC DILATATION OF GLANDSA gland distended to twice or more its normaldiameter was scored as cystic (Fig. 4). There wasrarely any difficulty with borderline lesions.
DYSPLASIADefinition was based on the work of Nagayo (1971).
:.
Fig. 1 Mild gastritis. Chronic inflammatory cell infiltrate is mainly in the luminal third of themucosa. (Haematoxylin and eosin x 170)
on 26 June 2019 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.2.179 on 1 F
ebruary 1979. Dow
nloaded from

Histological appearances of the gastric mucosa 15-27 years after partial gastrectomy
... t .:..:....
.
e. g ^ s
.^. axl l.v' s
:::
Fig. 2 Moderate gastritis. There is inflammation throughout the lamina propria with partialloss of specialised cells. Intestinal metaplasia is present near the bottom of the photograph.(H and E x 500)
Fig. 3 Severe gastritis. There is inflammation with complete atrophy of specialised cells.Many areas show mild dysplasia of epithelial cells. (H and E x 500)
181
on 26 June 2019 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.2.179 on 1 F
ebruary 1979. Dow
nloaded from
Ann Savage and S. Jones
Fig. 4 Glandsshowing cysticdilatation. (H and Ex 185): N ; . e.+ #.
.R S: .. 4ia k* . .. i ' :,", 4: :99 :.... i.:,* .. e.-k-+ w.S.S AB .us e it 1
w ; 82 .@ $
*s C-, LR 19N .esz. ' & 4gUMX
Mild dysplasiaThe epithelial cells lining a tubule are tall and hyper-chromatic with elongated, pointed nuclei. Nucleo-cytoplasmic ratio is increased; nuclei are fairlyuniform and arranged basally.
Moderate dysplasiaThe nuclei are rounded and the nucleo-cytoplasmicratio is further increased; some nuclei reach theluminal border of the cell. There may be somepleomorphism and mild architectural abnormalitiesof the tubules (Fig. 5).
Severe dysplasiaThe features of moderate dysplasia are morefrequent or more pronounced, with greater pleo-morphism and, in particular, increased architecturalabnormality (Fig. 6). Some pathologists wouldregard this lesion as carcinoma-in-situ. We con-sidered that the presence of lesions in this groupwould be an indication for excision.
POLYPSThese were defined endoscopically and dividedhistologically into two groups:
AdenomatousThese are similar to adenomatouslarge bowel.
polyps in the
Regenerative (hyperplastic)Glands are mingled with collagen and smoothmuscle cells. The glands are frequently cystic andlined by hyperplastic cells, which are large, but withsmall basal nuclei. There is a variable inflammatorycell infiltrate.
Results
The results of the first endoscopy are shown inTable 2.
Patients with moderate dysplasia in the initialbiopsy specimen were requested to attend for re-endoscopy within three to six months, and of the 14patients 13 accepted. Ten or more specimens weretaken from the suspicious area and further speci-mens from any lesion seen. The results of theserepeat endoscopies are shown in Table 3. Mostpatients had lesions similar to or more severe thanat the initial biopsy, but in only one was the lesionsignificantly worse. This patient had severe dysplasia
182
on 26 June 2019 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.2.179 on 1 F
ebruary 1979. Dow
nloaded from

H.stological appearances of the gastric mucosa 15-27 years after partial gastrectomy
Fig. 5 Moderate dysplasia, mainly in the glands to the right of the photograph. (H andEx 500)
Fig. 6 Severe dysplasia. The changes are more severe and more extensive than in Fig. 5.(H and E x 500)
183
on 26 June 2019 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.2.179 on 1 F
ebruary 1979. Dow
nloaded from
Ann Savage and S. Jones
Table 2 Results offirst endoscopy (63 patients)
Lesion Stoma Lesser curve
No. % No. %
Normal 0 7 11Acute gastritis 46 73 38 60Chronic gastritis
Mild 7 11 10 15Moderate 34 53 34 53Severe 26 41 11 17
Intestinal metaplasia 22 34 21 33Cystic dilatation of glands 35 55 25 39Dysplasia
Mild 22 34 28 44Moderate* 12 19 3 4Severe 0 0
PolypsAdenomatous 0 0Regenerative 8 12 0
'Lipid island' 0 2 3
*One patient had moderate dysplasia at the stoma and on the lessercurve.
Xe I~~~~1 15 13POLYPS
@ SEVEREDYSPLASIA
Table 3 Results of repeat endoscopy (13 patients)
Lesion Stoma Lesser curse
No. % No.
Acute gastritis 11 85 9 69Chronic gastritis
Mild 1 8 0Moderate 9 69 10 77Severe 4 31 3 23
Intestinal metaplasia 8 62 5 38Cystic dilatation 10 77 6 46Dysplasia
Mild 0 2 15Moderate 11 85 9 69Severe 1 8 0
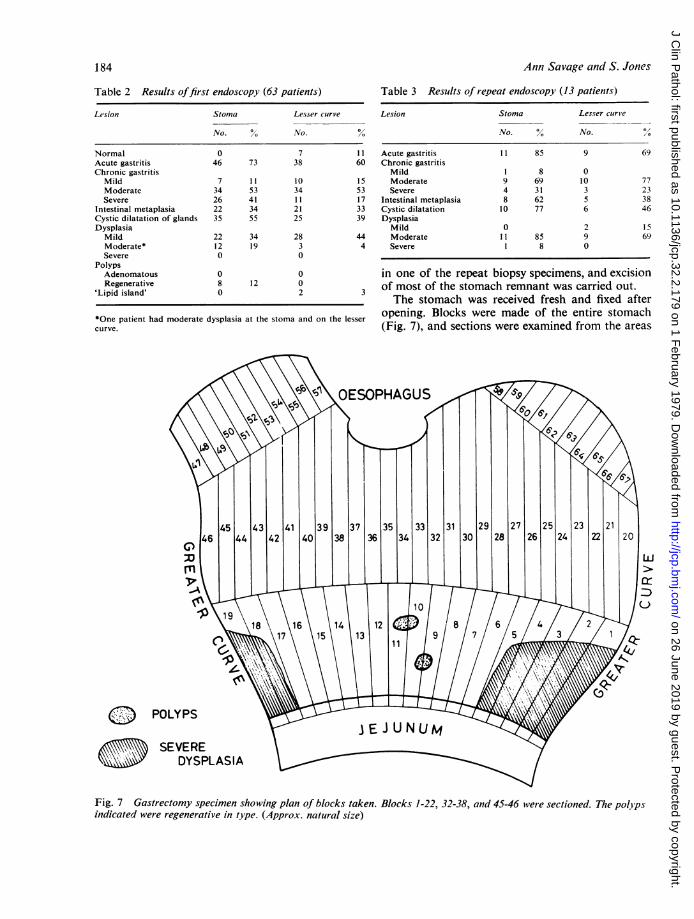
in one of the repeat biopsy specimens, and excisionof most of the stomach remnant was carried out.The stomach was received fresh and fixed after
opening. Blocks were made of the entire stomach(Fig. 7), and sections were examined from the areas
Fig. 7 Gastrectomy specimen showing plan of blocks taken. Blocks 1-22, 32-38, and 45-46 were sectioned. The polyps
indicated were regenerative in type. (Approx. natural size)
184
on 26 June 2019 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.2.179 on 1 F
ebruary 1979. Dow
nloaded from
Histological appearances of the gastric mucosa 15-27 years after partial gastrectomy
indicated. An extensive area of severe dysplasiawas found and, in addition, a wide range of appear-ances, including varying degrees of chronic gastritis,intestinal metaplasia, and dysplasia. No infiltratingcarcinoma was found.
Discussion
Among our 63 mainly asymptomatic patients whoaccepted screening, no case of infiltrating carcinomaand only one of severe dysplasia was found. Thiswas unexpected, as Schrumpf et al. (1977) had foundfour cases of infiltrating carcinoma and three ofsevere dysplasia among their 108 patients who hadhad a previous Billroth II gastrectomy. Domellofet al. (1977b), in their large series of 214 post-gastrectomy patients (Billroth II type), reported thatfour had infiltrating carcinoma, one had 'pre-cancerous' changes, and one had an adenomatouspolyp, if their symptomatic and necropsy cases areexcluded. Of their 74 post-Billroth I patients, fourhad carcinoma and one an adenomatous polyp(Domellof et al., 1976). It is possible that the inci-dence of stump carcinoma is less in British than inScandinavian patients. Although only about halfof our original group of patients were traced, it isunlikely that many had died of carcinoma of thestomach before follow-up. Stalsberg and Taksdal(1971) have shown that the risk of stump carcinomaless than 15 years postoperatively is less than that ofunoperated stomachs, and the risk increases gradu-ally with time thereafter. No firm conclusions canbe drawn about the incidence of stump carcinomafrom our results.The biopsies revealed a wide range of pathological
changes, and no stomach was completely normal,although two had only mild gastritis at the stoma. It isimportant to consider whether the lesions found arepremalignant. Siurala et al. (1974), in a prospectivesurvey of 116 patients with atrophic gastritis, found10 cases of carcinoma that had developed during afollow-up period of 19-23 years, whereas none haddeveloped in similar groups of patients with normalstomachs or with superficial gastritis. In an earliersurvey of a rural population in Finland, Siuralaet al. (1968) found atrophic gastritis in 28% ofthose between 16 and 65 years, and, if those over 50years only are considered, the prevalence was 54%.However, he found that the patient group had moresevere gastritis with an increased frequency of atypiaand metaplasia, compared with his randomlyselected group, and thus he could not conclude thatatrophic gastritis itself was necessarily premalignant.
Intestinal metaplasia was present in 29 (46%) ofour patients in association with either moderate orsevere gastritis. Morson (1955a) has shown that
intestinal metaplasia is more common in stomachswith carcinoma than in those removed for benignlesions and has demonstrated (Morson, 1955b)transitions from metaplastic mucosa to carcinoma.Reynolds et al. (1975) consider intestinal meta-plasia to be premalignant and suggest that allpatients with this lesion should have regular endo-scopic biopsies; they wonder if there is a place forprophylactic surgery in long-standing cases. How-ever, Siurala et al. (1968) found that 24% of theirrandomly selected rural population over 50 yearshad intestinal metaplasia. While one must be cautiousin relating Finnish data to a British population, itseems that intestinal metaplasia is not in itselfsufficient indication for radical measures.No adenomatous polyps were found in our series.
Although polypoid lesions were fairly common thesewere of a regenerative type. Neoplastic transforma-tion is not seen in these polyps (Ming and Goldman,1965), although they are sometimes found in associa-tion with gastric cancer. Cystic dilatation of thegastric glands was a common finding in our series,as in others (Domell6f et al., 1977b), and has beendescribed in the mucosa adjacent to early carcinomas(Nagayo, 1974). There is little evidence, however,that it has any premalignant significance.
'Lipid islands' in the gastric mucosa after gastrec-tomy were described by Domellof et al. (1977a),who found them in 60% of patients 23 years after aBillroth II resection. We found only two in our 42patients who had had a Billroth II gastrectomy (5%)despite a careful search. The reason for this differenceis not clear.
Dysplasia was always associated with acute orchronic inflammation in our cases, and it seemslikely that mild dysplasia is a reactive change whichcan safely be left alone. While it is generally acceptedthat significant dysplasia (moderate or severedysplasia) is premalignant, the degree of risk isunknown. This makes management of individualcases difficult. We decided to follow Japanesepractice (Nagayo, 1971) and to keep all moderatedysplasia lesions under review, probably bi-annually.However, patient cooperation may be a limitingfactor here. Our case with severe dysplasia wassubjected to total gastrectomy, and the lesion foundwas much more extensive than had been suspectedfrom biopsy. However, no infiltrating carcinomawas found. If operation is undertaken nothing lessthan a total gastrectomy can be recommended, sincesignificant dysplasia was found at the gastro-oesophageal junction. At present each of thesepatients must be managed in the light of individualcircumstances.Our results do not confirm the high incidence of
stump carcinoma found by others (Domellof et al.,
185
on 26 June 2019 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.2.179 on 1 F
ebruary 1979. Dow
nloaded from

186 Ann Savage and S. Jones
1976; Domellof et al., 1977b; Schrumpf et al., 1977)but do reveal the presence of an 'at risk' group (21 %of those submitted to biopsy) requiring closefollow-up. A prospective study of this group ofpatients with significant dysplasia may shed furtherlight on the problem.
We thank Mr A. G. McPherson, who kindly allowedus to study patients under his care, and Mrs ElizabethScott and Mr Brian Glover, who provided invaluablehelp in the endoscopy clinic. In addition, we aremost grateful to Mr Vernon Perry and the technicalstaff of the Pathology Department, without whosehelp this study could not have been undertaken. Wealso thank Mr Brian Amer for the photomicro-graphs and Miss Carol Jenkins and Mrs BettyCurtis for secretarial assistance.
References
Domellof, L., Eriksson, S., Helander, H. F., and Janunger,K. G. (1977a). Lipid islands in the gastric mucosaafter resection for benign ulcer disease. Gastroenter-ology, 72, 14-18.
Domellof, L., Eriksson, S., and Janunger, K. G. (1976).Late precancerous changes and carcinoma of thegastric stump after Billroth I resection. AmericanJournal of Surgery, 132, 26-31.
Domellof, L., Eriksson, S., and Janunger, K. G. (1977b).Carcinoma and possible precancerous changes of thegastric stump after Billroth lI resection. Gastro-enterology, 73, 462-468.
Helsingen, N., and Hillestad, L. (1956). Cancer develop-ment in the gastric stump after partial gastrectomy forulcer. Annals oJ Surgery, 143, 173-179.
Krause, U. (1958). Late prognosis after partial gastrec-tomy for ulcer. Acta Chirurgica Scandinavica, 114,341-354.
Lambert, R. (1972). Chronic gastritis. Digestion, 7,83-126.
Liavaag, K. (1962). Cancer development in the gastricstump after partial gastrectomy for peptic ulcer.Annals of Surgery, 155, 103-106.
Ming, S. C., and Goldman, H. (1965). Gastric polyps.Cancer, 18, 721-726.
Morgenstern, L., Yamakawa, T., and Seltzer, D. (1973).Carcinoma of the gastric stump. American Journal ofSurgery, 125, 29-38.
Morson, B. C. (1955a). Intestinal metaplasia of the gastricmucosa. British Journal of Cancer, 9, 365-376.
Morson, B. C. (1955b). Carcinoma arising from areas ofintestinal metaplasia in the gastric mucosa. BritishJournal of Cancer, 9, 377-385.
Nagayo, T. (1971). Histological diagnosis of biopsiedgastric mucosae with special reference to that ofborderline lesions. Gann Monographs on CancerResearch, 11, 245-249.
Nagayo, T. (1974). Histology and histogenesis of earlygastric carcinomas with flat mucosal elevations.Acta Pathologica Japonica, 24, 249-272.
Reynolds, K. W., Johnson, A. G., and Fox, B. (1975).Is intestinal metaplasia of the gastric mucosa a pre-malignant lesion? Clinical Oncology, 1, 101-109.
Saegesser, F., and James, D. (1972). Cancer of the gastricstump after partial gastrectomy (Billroth II principle)for ulcer. Cancer, 29, 1150-1159.
Schrumpf, E., Serck-Hanssen, A. Stadaas, J., Aune, S.,Myren, J., and Osnes, M. (1977). Mucosal changes inthe gastric stump 20-25 years after partial gastrectomy.Lancet, 2, 467-469.
Siurala, M., Isokoski, M., Varis, K., and Kekki, M.(1968). Prevalence of gastritis in a rural population.Scandinavian Journal of Gastroenterology, 3, 211-223.
Siurala, M., Lehtola, J., and Ihamaki, T. (1974). Atrophicgastritis and its sequelae. Scandinavian Journal ofGastroenterology, 9, 441-446.
Stalsberg, H., and Taksdal, S. (1971). Stomach cancerfollowing gastric surgery for benign conditions.Lancet, 2, 1175-1177.
Requests for reprints to: Dr A. Savage, Department ofPathology, Southmead General Hospital, Westbury-on-Trym, Bristol BS10 5NB, UK.
on 26 June 2019 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.32.2.179 on 1 F
ebruary 1979. Dow
nloaded from