hiv transmission thru breastfeeding
TRANSCRIPT

ISBN 978 92 4 159659 6
For further information, please contact:
World Health Organization
Department of Child and Adolescent Health and Development ([email protected]) or
Department of HIV/AIDS ([email protected]) or
Department of Nutrition for Health and Development ([email protected])
20 Avenue Appia, 1211 Geneva 27, Switzerland
website: http://www.who.int
UNICEF
Nutrition Section – Programme Division
3 United Nations Plaza
New York, New York 10017, United States of America
Tel +1 212 326 7000
A REVIEW OF AVAILABLE EVIDENCE
HIV Transmission ThroughBreastfeeding
2007 Update
This publication is an update of the review of current knowledge on HIV transmission throughbreastfeeding, with a focus on information made available between 2001 and 2007. It re-views scientific evidence on the risk of HIV transmission through breastfeeding, the impactof different feeding options on child health outcomes, and conceivable strategies to reduceHIV transmission through breastfeeding with an emphasis on the developing world.

HIV TransmissionThrough Breastfeeding
A Review of Available Evidence
2007 Update

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
ii
WHO Library Cataloguing-in-Publication Data
HIV transmission through breastfeeding : a review of available evidence : 2007 update.
1.HIV infections - transmission. 2.Acquired immunodeficiency syndrome - Transmission. 3.Breastfeeding - adverse effects. 4.Disease transmission, Vertical - prevention and control 5.Review litera-ture. I.World Health Organization.
ISBN 978 92 4 159659 6 (NLM classification: WC 503.3)
© World Health Organization 2008
All rights reserved. Publications of the World Health Organization can be obtained from WHO Press,World Health Organization, 20 Avenue Appia, 1211 Geneva 27, Switzerland (tel.: +41 22 7913264; fax: +41 22 791 4857; e-mail: [email protected]). Requests for permission to reproduce ortranslate WHO publications - whether for sale or for noncommercial distribution - should be ad-dressed to WHO Press, at the above address (fax: +41 22 791 4806; e-mail: [email protected]).
The designations employed and the presentation of the material in this publication do not imply theexpression of any opinion whatsoever on the part of the World Health Organization or of the UnitedNations Children's Fund concerning the legal status of any country, territory, city or area or of itsauthorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps repre-sent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers' products does not imply that they areendorsed or recommended by the World Health Organization or the United Nations Children's Fundin preference to others of a similar nature that are not mentioned. Errors and omissions excepted, thenames of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization and the United Na-tions Children's Fund to verify the information contained in this publication. However, the publishedmaterial is being distributed without warranty of any kind, either expressed or implied. The respon-sibility for the interpretation and use of the material lies with the reader. In no event shall the WorldHealth Organization or the United Nations Children's Fund be liable for damages arising from itsuse.
Printed in France.
iii
Table of contents
Preface v
Acknowledgements vii
Acronyms viii
Glossary ix
Executive summary 1
Introduction 3
Mother-to-child transmission of HIV 5
HIV infection in women 5
Rates of, and risk factors for, overall mother-to-child transmission 5
Prevention of mother-to-child transmission of HIV 6
HIV transmission through breastfeeding 9
Pathogenesis and mechanisms of breastfeeding transmission 9
Risk of postnatal transmission through breastfeeding 10
Timing of postnatal transmission through breastfeeding 10
Early postnatal transmission through breastfeeding 10
Late postnatal transmission through breastfeeding 11
Factors associated with risk of transmission through breastfeeding 12
Maternal factors 12
Infant factors 16
Benefits of breastfeeding 19
Health benefits of breastfeeding in the general population 19
Maternal health benefits 19
Child health benefits 19
Health benefits of breastfeeding in children born to HIV-infected mothers 21
HIV-exposed children, regardless of HIV status 21
HIV-infected children 21
Global breastfeeding practices 22
Strategies to reduce HIV transmission through breastfeeding 23
Primary prevention of HIV in women of childbearing age 23
Framework to assess interventions to prevent postnatal transmission 24

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
iv
Modifying infant feeding options for HIV-infected women: replacement feeding 24
Adverse outcomes of alternatives to breastfeeding practices 25
Social acceptability of feeding practices 25
HIV-infection 32
HIV-free survival 32
Discussion 32
Strategies for HIV-infected women who breastfed 33
Exclusive breastfeeding 33
Early cessation of breastfeeding 35
Heat treatment or pasteurization of expressed breast milk. 36
Microbicide treatment of expressed breast milk 36
Antiretroviral therapy during breastfeeding 37
Immunization of breastfed newborns 39
From research to public health recommendations on infant feeding:consequences for practice 39
Ongoing or planned research addressing the breastfeeding period 41
Conclusion 43
References 44

v
Preface
This Review was originally prepared as a background paper for the Technical Consulta-
tion on HIV and Infant Feeding that took placein Geneva in October 2006. It was updated dur-ing 2007 to include relevant new information.
As the Review was going to print at the begin-ning of 2008, several trials were underway toassess use of extended maternal or infantantiretrovirals to reduce transmission amongHIV-exposed breastfed infants. Relevant find-ings were presented at the 15th Conference onRetroviruses and Opportunistic Infections(CROI) held from 3 to 5 February 2008 and aresummarized here.1
Postnatal HIV transmission, infantoutcomes and infant feeding practicesIn a pooled analysis of individual data froma South African and a West African cohortstudy (abstract #46), the overall risk of post-natal HIV infection was 3.9% among childrenbreastfed for <6 months and 8.7% among chil-dren breastfed for >6 months (adjusted hazardratio: 1.8). Breastfeeding duration, as well asmaternal immune status, appear to be majordeterminants of HIV transmission. The risk didnot differ between exclusively and predominantlybreastfed children. Exposure to breastfeedingmixed with solids during the first 2 months in-creased the postnatal risk of acquisition of HIV(adjusted hazard ratio: 2.9).
In the Vertical Transmission Study in SouthAfrica (abstract #636), 18-month HIV-free sur-vival of children of HIV-infected women showsthat breastfeeding of HIV-uninfected infantsbeyond 6 months of age increases the risk of HIV
acquisition without gains for survival. It remainsimportant to identify means of making breastfee-ding safer for HIV-infected women who have nochoice other than to continue breastfeeding.
In a study on mastitis in Zambia (abstract#650), breast milk samples were collected from38 women who had clinical symptoms of masti-tis. The study found that during mastitis, eleva-tions of breast milk viral load are restricted tothe mastitic breast and eventually return to base-line levels, supporting current recommendationsfor women with mastitis to breastfeed from theunaffected breast.
Maternal outcomes and infant feedingpracticesIn the Ditrame-Plus cohort study in Abidjan(abstract #73), the risk of pregnancy before 12months post-partum was comparable in replace-ment feeding and breastfeeding groups: 4%. Be-tween 12 and 24 months post-partum, the riskof pregnancy was significantly lower among re-placement feeders than breastfeeders. Replace-ment feeding was not responsible for a greaterincidence of pregnancies in this West Africanurban context, probably due to the systematicoffer and the frequent use of contraceptive serv-ices.
Antiretrovirals in breastfeeding womenThe Kisumu Breastfeeding Study in Kenya(abstract #45LB) was an observational prospec-tive cohort of children of lactating women tak-ing antiretroviral treatment (ART) to preventmother-to-child transmission (MTCT). Overalltransmission rates were 3.9% at 6 weeks, 5% at6 months, 5.9% at 12 months and 6.7% at 18
1 CROI abstracts are available at http:/www.retroconference. org, accessed February 15, 2008.

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
vi
months. There was no difference in HIV trans-mission by baseline maternal CD4 count. Forthose infants who became infected during thefirst 6 weeks of life, resistance was initially notdetected (abstract #84LB), but emerged duringthe breastfeeding period.
In the MASHI trial in Botswana (abstract#637), the MTCT rate at one month was 1.2%among breastfeeders and 1.1% among formulafeeders. The authors concluded thatbreastfeeding was not a risk for MTCT withinthe first month of life for children exposed tomaternal ART and receiving infant antiretroviralprophylaxis.
The preliminary results of the non-randomized part of the Kesho-Bora studybeing conducted in five African sites (ab-stract #638) showed that the HIV transmis-sion rate at 12 months was 7.6% in women with<200 CD4 with no significant difference accord-ing to infant feeding pattern; the rate was 5.8%among women with >500 CD4 count, respec-tively 7.5% and 0% in ever and never breastfedinfants.
In the Dream cohort in Mozambique (ab-stract #369), 341 mother-infant pairs were fol-lowed from pregnancy until 12 months postpartum; mothers breastfed while receiving ARTuntil 6 months post delivery. ART continuedbeyond 6 months in women who initiated it fortheir own health. The HIV MTCT rates were:1.2% (4) at birth, 1.9% (6) at 6 months, and2.8% (8) at 12 months. Four late post-natal HIV-1 infections (>1 month of age) were observed inthis cohort; 15% were lost to follow-up.
The Breastfeeding, Antiretroviral and Nutri-tion (BAN) Study in Malawi (abstract #648)reports on antiretroviral concentrations. Infants'plasma concentrations for all antiretrovirals were
well below levels required for treatment, suggest-ing minimal risk for drug toxicity. Lamivudine(3TC) and nelfinavir exposure in infants wouldsuggest minimal risk for resistance in HIV-in-fected children; however, low-level nevirapine(NVP) exposure via breast milk may predisposeHIV-infected infants to resistance.
Antiretrovirals in breastfed childrenThe PEPI-Malawi Study (abstract #42LB)evaluated in a randomized controlled trial if 14weeks of extended daily infant antiretroviralprophylaxis with NVP (group 2) or NVP+ZDV(group 3) with breastfeeding cessation from age4-6 months would reduce postnatal transmissionof HIV compared to controls receiving single dose(sd) NVP and one week ZDV (group 1). At age9 months, the risk of HIV infection was 10.6%in group 1, 5.2% in group 2 and 6.4% in group3. However, at 18 months, the HIV rate reach13.9% in group 1, 10.1% in group 2 and 10.2%in group 3. Postnatal transmission occurred af-ter NVP cessation among breastfed children.Post-exposure prophylaxis in breastfed childrencould reduce postnatal transmission but shouldbe maintained over the entire breastfeeding du-ration.
In the SWEN randomized controlled Trialconducted in Ethiopia, India and Uganda(abstract #43), an extended infant post-expo-sure prophylaxis with daily NVP for 6 weeks inbreastfed infants of HIV-infected mothers wasassessed. The 6-week HIV transmission rate inthe extended-NVP arm was 2.5% versus 5.3%in the sd NVP arm (p=0.009), but the 6-monthHIV rate was 6.9% in the extended-NVP armversus 9.0% in the sd NVP arm (p=0.16). Theextended-NVP arm was safe, but postnatal trans-mission occurred after stopping NVP in breastfedchildren with a reduction of long term efficacy.Occurrence of resistance to NVP in infected chil-dren was very high (11/12).

vii
Acknowledgements
This review was updated by Valériane Leroy(INSERM U593, Institut de Santé
Publique, Epidémiologie et Développement,Université Victor Segalen, Bordeaux, France). Itis based on an original review on HIV transmis-sion through breastfeeding prepared by Marie-Louise Newell (Institute of Child Health,London) for WHO in 2003. The 2003 reviewwas updated in 2005 by the WHO Departmentof Nutrition for Health and Development as abackground paper for a consultation on Nutri-tion and HIV.
We are very grateful to Marie-Louise Newellfor helping in structuring the early draft of thisreview and to Lynne Mofenson for providing
useful information on synthesis of the technicalconsultation. We would like to especially thankRajiv Bahl, Renaud Becquet, André Briend,Anirban Chatterjee, Anna Coutsoudis, FrançoisDabis, Mary Glenn Fowler, Peggy Henderson,Lida Lhotska, Jose Martines, Ellen Piwoz, Felic-ity Savage, Constanza Vallenas and Isabelle deVincenzi for reviewing the report and giving help-ful comments. Finally, we would like to acknowl-edge the contributions of Coralie Thore,Christian Weller and Evelyne Mouillet from theISPED library in Bordeaux for their help in re-searching papers.
Kai Lashley performed the final copy-edit ofthe text.

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
viii
Acronyms
3TC lamivudineAIDS acquired immunodeficiency syndromeANRS Agence Nationale de Recherches sur le SIDA (France)ARV antiretroviralART antiretroviral therapyAZT azidothymidineBF breastfeedingCI confidence intervalD4T stavudineddI didanosineDNA deoxyribonucleic acidEBF exclusive breastfeedingFF formula feedingHIVIGLOB HIV hyperimmune globulinHIV human immunodeficiency virusHR hazard ratioMF mixed feedingMTCT mother-to-child transmission of HIVNVP nevirapineOR odds ratioPCR polymerase chain reactionPMTCT prevention of mother-to-child transmission of HIVRF replacement feedingRNA ribonucleic acidSLPI secretory leukocyte protease inhibitorSDS sodium dodecyl sulfateUN United NationsUNAIDS Joint United Nations Programme on HIV/AIDSUNGASS/AIDS United Nations General Assembly Special Session on HIV/AIDSUNICEF United Nations Children’s FundWHO World Health OrganizationZDV zidovudine

ix
Glossary
ART, an abbreviation for antiretroviral therapy,is a combination of three or more differentantiretroviral drugs used in the treatment ofthose infected with HIV to reduce viral load.
Breast-milk substitute refers to any food be-ing marketed or otherwise represented as apartial or total replacement for breast milk,whether or not suitable for that purpose.
CD4 cells (also known as T4 or helper T cells)are lymphocytes (a type of white blood cell),which are key in both humoral and cell-medi-ated immune responses. These are the maintarget cells for HIV. Their numbers decreaseduring HIV infection, and their level is usedas a marker of progression of the infection.CD8 cells are a subtype of T lymphocytes,which also play an important role in fightinginfections. Their numbers may be increasedduring HIV infection.
Cell-associated virus refers to HIV which livesinside the cell, measured as HIV-DNA.
Cell-free virus refers to parts of the virus (viri-ons) not associated with a cell, measured asHIV-RNA.
Cessation of breastfeeding means completelystopping breastfeeding, which includes nomore suckling at the breast.
Colostrum is the thick yellow milk secreted bythe breasts during the first few days after de-livery, which gradually evolves into maturemilk at 3–14 days postpartum. It containsmore antibodies and white blood cells thanmature breast milk.
Commercial infant formula means a breast-milk substitute formulated industrially in ac-cordance with applicable Codex Alimentariusstandards to satisfy the nutritional require-ments of infants during the first months oflife.
Complementary food means any food, wheth-er manufactured or locally prepared, used as acomplement to breast milk or to a breast-milksubstitute, when either becomes insufficientto satisfy the nutritional requirements of theinfant.
DNA, an abbreviation for deoxyribonucleic acid,is the carrier of genetic information found incell nuclei.
Exclusive breastfeeding means an infant re-ceives no other food or drink, not even water,other than breast milk (which can include ex-pressed breast milk), with the exception ofdrops or syrups consisting of vitamins, miner-al supplements or medicines.
Formula feeding involves the use of commer-cial infant formula that is formulated indus-trially in accordance with applicable CodexAlimentarius standards to satisfy the nutri-tional requirements of infants during the firstmonths of life up to the introduction of com-plementary foods.
Human immunodeficiency virus (HIV) refersto HIV-1 in this review. Cases of mother-to-child transmission of HIV-2 are rare.
Immunoglobulins are any of the five distinctantibodies present in the serum and externalsecretions of the body (IgA, IgD, IgE, IgG andIgM).
Incidence density means the incidence rate ofan event, i.e. HIV infection or death per per-son-time (months or years).
Infant refers to a child from birth to 12 monthsof age.
Intrapartum means the period during labourand delivery.

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
x
Lamivudine, or 3TC, is an antiretroviral drugoften used in combination with zidovudine,ZDV, also known as azidothymidine, AZT.
Late postnatal HIV transmission means trans-mission that takes place after about six weeksof life, the earliest time at which it is possibleto determine that transmission did not takeplace during delivery.
Lipid means any one of a widely varying groupof fats and fat-like organic substances.
Macrophage is a large ‘wandering’ phagocyticwhite blood cell that ingests foreign matter,and plays an important role in resisting infec-tion.
Mature breast milk is milk produced from about14 days postpartum until the cessation ofbreastfeeding.
Mixed feeding refers to breastfeeding with theaddition of fluids, solid foods and/or non-hu-man milks such as formula.
Mother-to-child transmission (MTCT) indi-cates instances of transmission of HIV to achild from an HIV-infected woman duringpregnancy, delivery or breastfeeding. The termis used in this document because the immedi-ate source of the child’s HIV infection is themother. Use of the term mother-to-child trans-mission implies no blame, whether or not awoman is aware of her own infection status.
Neonatal describes the period immediately fol-lowing birth through the first 28 days of life.
Nevirapine, or NVP, is an antiretroviral drugcommonly used as a treatment regimen, ei-ther alone or in combination with other drugs,to prevent MTCT.
Partial breastfeeding means giving a baby somebreastfeeds and some artificial feeds, eithermilk or cereal, or other food.
PCR means polymerase chain reaction, a labo-ratory method in which the genetic material(DNA or RNA) of the virus is detected andamplified. It can be both qualitative and quan-titative.
Peripartum transmission is mother-to-childtransmission of HIV occurring around the timeof delivery (i.e. late in pregnancy, during orimmediately after delivery).
Postnatal transmission is mother-to-childtransmission of HIV after delivery, during thebreastfeeding period.
Predominant breastfeeding means breastfeed-ing is the main source of nourishment, but aninfant is also given small amounts of non-nu-tritious drinks, such as tea, water and water-based drinks.
Replacement feeding means the process of feed-ing a child who is not receiving any breast milkwith a diet that provides all the nutrients thechild needs until the child is fully fed on fam-ily foods.
RNA, an abbreviation for ribonucleic acid, is asubstance found in the nucleus of all livingcells and in many viruses. An intermediate ofDNA, it is the medium by which genetic in-structions from the nucleus are transmittedto the rest of the cell. RNA viral load, ex-pressed as copies of RNA per ml of plasma orother body fluid, reflects the amount of ac-tively replicating virus in the body. High viralRNA levels occur (temporarily) immediatelyafter acquisition of infection and later withprogression of disease, and are associated withhigher rates of transmission.
Virion refers to those parts of the virus that areable to replicate HIV.
Wet-nurse refers to the breastfeeding of an infantby someone other than the infant’s mother.
Zidovudine, or ZDV, is an antiretroviral drugwhich inhibits HIV replication. It was the firstdrug licensed to treat HIV infection. Today itis frequently used in combination with otherantiretroviral drugs and, alone or in combina-tion, it is used in the prevention of mother-to-child transmission of HIV. (It is also knownas retrovir or azidothymidine, AZT.)

1
Breastfeeding is best for infants, andis an effective method of reducing the risk
of common childhood morbidity, particularlygastrointestinal and respiratory infections, andof promoting child survival and maternal healththrough child spacing. In 2001, the World HealthAssembly endorsed the recommendation thatinfants should be exclusively breastfed for thefirst six months of life to achieve optimal growth,development and health. Thereafter, infantsshould receive nutritionally adequate and safecomplementary foods while breastfeeding con-tinues to 24 months or beyond.
While breastfeeding carries significant healthbenefits to infants and young children, HIV canbe transmitted during breastfeeding from anHIV-infected mother to her infant. Reducing thistransmission while ensuring improved HIV-freesurvival1 is one of the most pressing public healthdilemmas confronting researchers, health-careprofessionals, health policy-makers and HIV-in-fected women in many areas of the world, espe-cially in developing countries.
In 2007, 2.5 million children aged less than15 years worldwide were living with HIV and anestimated 420 000 children aged less than 15years were newly infected with HIV in 2007alone, nearly always through mother-to-childtransmission (MTCT). HIV/AIDS is an increas-ingly important cause of mortality in those agedless than five years in Africa. Before theantiretroviral therapy (ART) era, child mortal-ity due to HIV was estimated to be 35.2% byage one year and 52.5% by two years of age.
Mother-to-child transmission of HIV can oc-cur during pregnancy, labour or delivery, orthrough breastfeeding. Without specific interven-tions, HIV-infected women will pass the virus to
their infants during pregnancy or delivery inabout 15-25% of cases; and an additional 5-20%of infants may become infected postnatally dur-ing breastfeeding, for an overall risk of 30-45%.Breastfeeding may thus be responsible for onethird to one half of HIV infections in infantswhen interventions are not available.
HIV has been detected in breast milk in cell-free and cell-associated compartments and thereis now evidence that both compartments are in-volved in transmission of HIV through breastmilk. Following ingestion of HIV infected breastmilk, infant gut mucosal surfaces are the mostlikely site at which transmission occurs.
The rate of late postnatal transmission (thatis, after six weeks of age) can be better quanti-fied in 2007 than previously. Data from a meta-analysis show that the cumulative probability oflate postnatal transmission at 18 months is 9.3%(95% confidence interval, CI, 3.8-14.8%). Latepostnatal transmission, therefore, could contrib-ute as much as 42% to the overall rate of MTCT.Analysis indicates that late postnatal transmis-sion risk is around 1% per month of breastfeedingand is constant over time from between four andsix weeks to 18 months. Transmission can takeplace at any point during breastfeeding, and thelonger the duration of breastfeeding, the greaterthe cumulative risk.
The risk of postnatal transmission throughbreastfeeding is associated with clinical, immu-nological and virological maternal factors andinfant feeding patterns. Maternal seroconversionduring breastfeeding, low maternal CD4 cellcount, increased maternal RNA viral load inplasma and breast milk and a lack of persistenceof HIV-specific IgM in breast-milk at 18 monthsare strongly associated with increased risk of
Executive summary
1 HIV-free survival refers to young children who are both alive and HIV-uninfected at a given point in time, usually 18months.

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
2
transmission through breastfeeding. Breastpathologies such as clinical and subclinical mas-titis, nipple bleeding, and abscesses, fissures orlesions are also associated with a higher risk oftransmission through breastfeeding. Exclusivebreastfeeding for up to six months, however, isassociated with a three to fourfold decreased riskof transmission of HIV compared to non-exclu-sive breastfeeding; mixed feeding, therefore, ap-pears to be a clear risk factor for postnataltransmission. One study found that about 4%of exclusively breastfed infants became infectedthrough exclusive breastfeeding from six weeksto six months.
The incidence of HIV infection among womenduring the postpartum period is high in Africa.The overall risk of MTCT is increased in recently-infected lactating women and estimated to be29% (95% Cl, 16–42%), illustrating the impor-tance of prevention of primary infection through-out the breastfeeding period.
The most appropriate infant feeding optionfor an HIV-infected mother depends on her in-dividual circumstances, including her health sta-tus and the local situation. The health servicesavailable and the counselling and support she islikely to receive should be considered. The WorldHealth Organization (WHO) recommends HIV-infected women breastfeed their infants exclu-sively for the first six months of life, unlessreplacement feeding is acceptable, feasible, af-fordable, sustainable and safe for them and theirinfants before that time. When those conditionsare met, WHO recommends avoidance of allbreastfeeding by HIV-infected women.
To help HIV-positive mothers make the bestchoice, they should receive appropriate counsel-ling that includes information about the risksand benefits of various infant feeding optionsbased on local assessments, and guidance in se-lecting the most suitable option for their ownsituation. Counselling, information provision andsupport during the antenatal period is key forwomen to make informed choices. Postnatal fol-
low-up with repeated growth measurements isalso crucial to this support, as is nutritional coun-selling, particularly around the period ofbreastfeeding cessation.
Early cessation of breastfeeding could alsoprevent a sizable proportion of postnatal HIVinfections but several studies in Africa have re-ported that it was associated with an increasedrisk of infant morbidity (especially diarrhoea)and mortality in HIV-exposed children. Recentdata from Zambia and Botswana show that pro-longed breastfeeding of children already infectedwith HIV is associated with improved survivalcompared to early cessation of breastfeeding.
It is also important to identify approaches totreating expressed breast milk to eliminate therisk of transmission while preserving the milk'snutritional content and protective qualities. Withthis aim, expressed heat-treated breast milk andmicrobicides to treat HIV-infected breast milkmay have a role to play in shortening the dura-tion of breastfeeding and allowing for a safe tran-sition period to other types of foods.
More research is required to provide practicaltools that can be used routinely – especiallyaround the time of early breastfeeding cessation– to contribute to the assessment of the nutri-tional adequacy of complementary feeding andguide efficiently the nutritional counselling ofchildren exposed to HIV.
Other possibilities for preventing HIV frombeing transmitted through breast milk are emerg-ing. These include giving ART to women duringbreastfeeding (whether or not necessary for themother's health) and post-exposure prophylaxisto the infant. Recent studies have sought to de-termine the effects of the former, and severalstudies on the latter are ongoing; both are dis-cussed in this review. Finally, passive and activeimmunization strategies of breastfed newbornsare increasingly being studied. Further researchon their potential role in reducing MTCT of HIVis needed and ongoing.

3
Introduction
Despite substantial progress in reducing childmorbidity and mortality and promoting
family health in recent decades, there are stillunacceptable disparities in maternal and childhealth worldwide (Black et al. 2003; WHO2005). While child mortality has declined in thepast decades in many regions, progress on keyindicators has begun to slow down. In parts ofsub-Saharan Africa, child mortality is on the rise(Black et al. 2003). About 9.7 million childrenunder five die each year (WHO mortality databank, access on request), mainly from prevent-able causes and almost all in poor countries. Inthe period between 2000 and 2003, four causesaccounted for over 80% of the then estimated10.6 million yearly deaths in children aged lessthan five years: pneumonia (19%), diarrhoea(17%), malaria (8%), and neonatal conditions(37%). Among neonatal deaths, 36% were dueto infections including sepsis, pneumonia, teta-nus and diarrhoea, 28% were due to being pre-term and 23% were due to asphyxia (Bryce etal. 2005). Undernutrition is an underlying causeof more than half of all deaths in children agedless than five years, and is associated with infec-tious diseases (Bryce et al. 2005). It is also theleading underlying cause of disability and illnessworldwide, particularly so in countries with highinfant mortality, where suboptimal feeding prac-tices are a major cause of underweight (Bryce etal. 2005). Promotion of breastfeeding has playedan important role in protecting infants and youngchildren, since breastfeeding provides optimal nu-trition, protects against common childhood in-fections, reduces mortality significantly, and haschild-spacing effects (Nicoll et al. 2000a; WHOCollaborative Study Team 2000). Exclusivebreastfeeding is therefore recommended until sixmonths of age (WHO 2001).
In 2007, 2.5 million children aged less than15 years worldwide were living with HIV. An es-
timated 420 000 children aged less than 15 yearswere newly infected in 2007 (UNAIDS 2006).There were also an estimated 380 000 deathsdue to AIDS among children. Africa has the high-est prevalence: 90% of both new infections andAIDS-related deaths among children occur there,particularly in southern Africa (UNAIDS 2007).
MTCT is the most significant source of HIVinfection in young children. The virus may be trans-mitted during pregnancy, labour or delivery, orthrough breastfeeding (De Cock et al. 2000). With-out specific interventions, HIV-infected women willpass the virus to their infants during pregnancy ordelivery in about 15–25% of cases; and an addi-tional 5–20% of infants may become infected post-natally during breastfeeding (De Cock et al. 2000;Nduati et al. 2000). About two thirds of infantsborn to HIV-infected mothers will not be infected.Breastfeeding may thus be responsible for one thirdto one half of HIV infections in infants and youngchildren in African settings (De Cock et al. 2000).HIV/AIDS is an increasingly important cause ofmortality in children aged less than five years inAfrica (Dabis & Ekpini 2002; Walker et al. 2002).Before the antiretroviral therapy (ART) era, childmortality due to HIV was estimated to be 35.2%by age one year and 52.5% by two years of ageamong HIV-infected children in a meta-analysis,which pooled information from the African clini-cal trials that aimed to assess the efficacy of inter-ventions to reduce MTCT. Mortality varied bygeographical region, and was associated with ma-ternal death, maternal CD4 cell counts <200μl,and infant HIV infection and its timing. In HIV-infected children, mortality was significantly lowerfor those with late infection than those with earlyinfection (Newell et al. 2004). These findings high-light the need for effective prevention of MTCT,early paediatric HIV diagnosis and antiretroviralcare and support for HIV-infected children and allmembers of affected families.

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
4
Prevention of MTCT of HIV using availableantiretroviral interventions can be achieved, evenin breastfeeding populations. Considerable effortis ongoing to scale-up these interventions toreach a wider population (WHO 2006). How-ever, in settings where breastfeeding beyond oneyear is the norm, postnatal transmission throughbreastfeeding reduces the impact of perinatalantiretroviral interventions (Leroy et al. 2002).While breastfeeding carries the risk of HIV trans-mission, not breastfeeding carries other signifi-cant health risks to infants and young children,such as an increased risk of diarrhoea and pneu-monia morbidity and mortality (Nicoll et al.2000a; WHO Collaborative Study Team 2000;Thior et al. 2006).
The prevention of HIV transmission shouldbe balanced against the risk of other morbidityand mortality risks, including malnutrition. Thereduction of HIV transmission through thebreastfeeding period is one of the most pressingpublic health dilemmas confronting researchers,health-care professionals, health policy-makersand HIV-infected women in many areas of theworld, especially in developing countries. Preven-tion of HIV transmission during breastfeedingshould be considered in a broad context thattakes into account the need to promotebreastfeeding of infants and young childrenwithin the general population. Countries needto develop (or revise) comprehensive nationalfeeding policies of infants and young children toconsider the risks of HIV transmission duringinfant feeding, while continuing to protect, pro-mote and support breastfeeding for infants ofHIV-negative women and women whose HIVinfection status is unknown.
The Declaration of Commitment endorsed atthe United Nations General Assembly SpecialSession on HIV (UNGASS) in 2001 set the goalof reducing the proportion of infants infectedwith HIV by 20% by 2005 and 50% by 2010(Harwood & Planetwire.org 2001; UN 2001).A further goal was ensuring that 80% of preg-nant women who receive antenatal care haveaccess to HIV prevention services. However, theJoint United Nations Programme on HIV/AIDS(UNAIDS) reports that less than 10% of HIV-infected pregnant women have access to appro-
priate care and highlights missed sexual and re-productive health opportunities (UNAIDS2006). To meet international goals for reductionsin child mortality, efforts must continue to focuson preventing MTCT, but must also prevent un-dernutrition and strengthen health systems andprogrammes that can deliver available interven-tions for the other major diseases killing chil-dren in the developing world (Bryce et al. 2006a).The fourth Millennium Development Goal(MDG) calls for a two thirds reduction between1990 and 2015 in deaths of children aged lessthan five years (http://www.un.org/millenniumgoals).Achieving this goal will require widespread useof effective interventions for preventing deaths,and is also linked to MDG5 on maternal mor-tality, as infant health and survival is closelylinked to maternal health (Bryce & Victora2005; Costello & Osrin 2005; Mason 2005;Bryce et al. 2006b).
This report is an update of the review of currentknowledge on HIV transmission throughbreastfeeding (WHO/UNICEF/UNFPA/UNAIDS2004) with a focus on information made availablebetween 2001 and 2007. It reviews recent scien-tific evidence on the risk of HIV transmissionthrough breastfeeding, the impact of different feed-ing options on child health outcomes, and con-ceivable strategies to reduce HIV transmissionthrough breastfeeding with a specific emphasis onthe developing world. This review further informsguidance on HIV prevention and infant feedingstrategies (WHO 2006).
To update this review, published and unpub-lished literature contributing to recent evidenceabout children affected and infected by HIV/AIDS and infant feeding patterns since 2001 wasconsulted. Medline, one of the main biblio-graphic scientific databases, was used, facilitat-ing a wide variety of studies to be selected,ranging from randomized clinical trials to epide-miological cohort studies (investigating HIV/AIDS-related morbidity and mortality amongchildren, MTCT and infant feeding patterns),to demographic and national surveillance surveys(infant feeding indicators). The most relevantreferences have been included in this review, in-cluding other systematic reviews.

5
Mother-to-child transmission of HIV
HIV infection in women
Sexual contact continues to be the major modeof HIV transmission, leading to high preva-
lence of HIV infection in women making accessto sexual and reproductive health services essen-tial (Schmid et al. 2004).
The prevalence of HIV infection varies con-siderably from region to region. Children in sub-Saharan Africa are disproportionately affected,with nearly nine in every 10 newly-infected chil-dren worldwide living in this region (UNAIDS2007). In West and Central Africa, HIV preva-lence in pregnant women currently reaches upto about 7% in some urban areas, with generallylower rates in rural areas. Prevalence in East Af-rica is up to about 9% in urban areas, while inSouthern Africa antenatal seroprevalences ofabout 16-39% have been reported. In the Carib-bean, Central America and South America, ratesamong pregnant women are generally below 1%.In Asia, seroprevalence rates in some cities orprovinces of Cambodia, India, Indonesia andThailand range from less than 1% up to about5%. In Eastern Europe, where there has been anexceptionally rapid increase in the number ofHIV-infections, the estimated antenatal preva-lence is still less than 1% (UNAIDS 2007).
The incidence of HIV among women duringthe postpartum period is also high in Africa. TheHIV incidence rate was 3.5/100 women-years(95% confidence interval, CI, 1.9–5.0) in early1990 in Rwanda (Leroy et al. 1994). In Zimba-bwe in late 1990, among the 9562 women whowere HIV-negative at the time of giving birth,3.4% (95% CI 3.0–3.8) and 6.5% (95% CI 5.7–7.4) acquired HIV infection over 12 and 24months postpartum, respectively (Humphrey etal. 2006). As 85% of women still breastfeed at15 months and 30% at 21 months in this popu-lation, new postpartum infections subsequentlyincrease the number of children exposed to HIV.
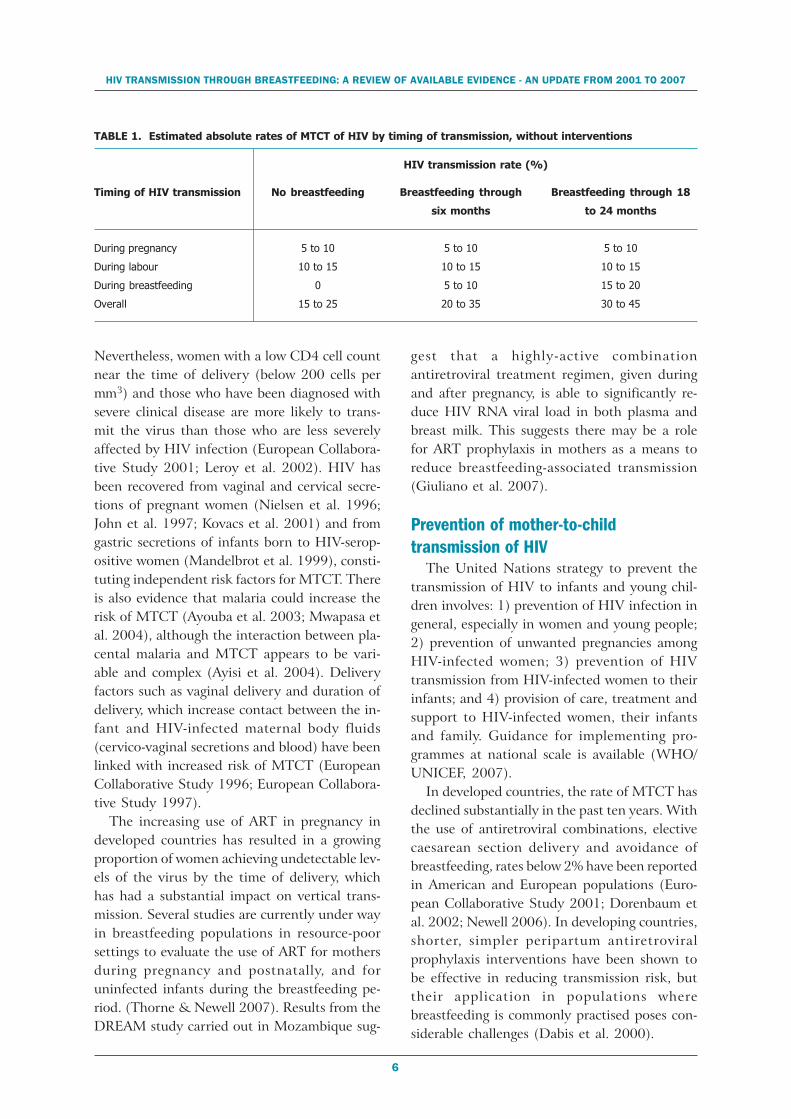
Rates of, and risk factors for overallmother-to-child transmission of HIVIn HIV-infected pregnant women, MTCT canoccur before, during or after delivery, but trans-mission in early pregnancy is rare (Rouzioux etal. 1993). Without specific interventions aimedat reducing the risk of transmission, estimatedrates of MTCT range from 15% to 25% in Eu-rope and the United States of America and from25% to 45% in developing countries (The Work-ing Group on Mother-to-Child Transmission ofHIV 1995). The additional risk posed bybreastfeeding as commonly practised in devel-oping countries ranges from 5% to 20%, withan attributable risk of 40% (Table 1) (De Cocket al. 2000). These breastfeeding practices ac-count for a large part of the estimated differencesin the risks of MTCT between developing anddeveloped countries (where breastfeeding is lesscommon). The overall risk of MTCT is increasedimmediately after HIV is acquired, due to theinitially high levels of maternal viral load. There-fore, when a woman contracts HIV during preg-nancy or the breastfeeding period, the risk ofvirus transmission is increased. There is someevidence of an increased risk of acquisition ofHIV during pregnancy (Gray et al. 2005).
The overall risk of MTCT is associated withfactors related to the virus, the mother and theinfant (Newell 2001). Maternal RNA viral loadin plasma has been strongly associated with therisk of MTCT (European Collaborative Study1996; European Collaborative Study 1997;Mayaux et al. 1997; Simonds et al. 1998; Shafferet al. 1999b; Leroy et al. 2001). However, al-though the risk of transmission increases sub-stantially with increasing viral load, transmissionof the virus to the fetus or infant can occur, al-beit rarely, even with very low, or undetectable,viral load levels. Similarly, at very high levels ofHIV RNA, transmission does not always occur.
HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
6
Nevertheless, women with a low CD4 cell countnear the time of delivery (below 200 cells permm3) and those who have been diagnosed withsevere clinical disease are more likely to trans-mit the virus than those who are less severelyaffected by HIV infection (European Collabora-tive Study 2001; Leroy et al. 2002). HIV hasbeen recovered from vaginal and cervical secre-tions of pregnant women (Nielsen et al. 1996;John et al. 1997; Kovacs et al. 2001) and fromgastric secretions of infants born to HIV-serop-ositive women (Mandelbrot et al. 1999), consti-tuting independent risk factors for MTCT. Thereis also evidence that malaria could increase therisk of MTCT (Ayouba et al. 2003; Mwapasa etal. 2004), although the interaction between pla-cental malaria and MTCT appears to be vari-able and complex (Ayisi et al. 2004). Deliveryfactors such as vaginal delivery and duration ofdelivery, which increase contact between the in-fant and HIV-infected maternal body fluids(cervico-vaginal secretions and blood) have beenlinked with increased risk of MTCT (EuropeanCollaborative Study 1996; European Collabora-tive Study 1997).
The increasing use of ART in pregnancy indeveloped countries has resulted in a growingproportion of women achieving undetectable lev-els of the virus by the time of delivery, whichhas had a substantial impact on vertical trans-mission. Several studies are currently under wayin breastfeeding populations in resource-poorsettings to evaluate the use of ART for mothersduring pregnancy and postnatally, and foruninfected infants during the breastfeeding pe-riod. (Thorne & Newell 2007). Results from theDREAM study carried out in Mozambique sug-
gest that a highly-active combinationantiretroviral treatment regimen, given duringand after pregnancy, is able to significantly re-duce HIV RNA viral load in both plasma andbreast milk. This suggests there may be a rolefor ART prophylaxis in mothers as a means toreduce breastfeeding-associated transmission(Giuliano et al. 2007).
Prevention of mother-to-childtransmission of HIV
The United Nations strategy to prevent thetransmission of HIV to infants and young chil-dren involves: 1) prevention of HIV infection ingeneral, especially in women and young people;2) prevention of unwanted pregnancies amongHIV-infected women; 3) prevention of HIVtransmission from HIV-infected women to theirinfants; and 4) provision of care, treatment andsupport to HIV-infected women, their infantsand family. Guidance for implementing pro-grammes at national scale is available (WHO/UNICEF, 2007).
In developed countries, the rate of MTCT hasdeclined substantially in the past ten years. Withthe use of antiretroviral combinations, electivecaesarean section delivery and avoidance ofbreastfeeding, rates below 2% have been reportedin American and European populations (Euro-pean Collaborative Study 2001; Dorenbaum etal. 2002; Newell 2006). In developing countries,shorter, simpler peripartum antiretroviralprophylaxis interventions have been shown tobe effective in reducing transmission risk, buttheir application in populations wherebreastfeeding is commonly practised poses con-siderable challenges (Dabis et al. 2000).
TABLE 1. Estimated absolute rates of MTCT of HIV by timing of transmission, without interventions
Timing of HIV transmission
During pregnancy
During labour
During breastfeeding
Overall
No breastfeeding
5 to 10
10 to 15
0
15 to 25
Breastfeeding through
six months
5 to 10
10 to 15
5 to 10
20 to 35
Breastfeeding through 18
to 24 months
5 to 10
10 to 15
15 to 20
30 to 45
HIV transmission rate (%)

7
Early randomized clinical trials from 1998 inAfrica and Thailand demonstrated the short-term efficacy of several antiretroviral regimensadministered around the time of delivery(peripartum) to prevent transmission (Dabis etal. 1999; Guay et al. 1999; Saba 1999; Shafferet al. 1999a; Wiktor 1999). This short-term ef-ficacy was measured by comparing infant HIVinfection status at six and eight weeks of agebetween groups receiving different antiretroviralinterventions or a placebo. These regimens in-volved three different ARV drugs, used alone orin combination: zidovudine (ZDV), lamivudine(3TC) and nevirapine (NVP).
The NVP prophylactic regimen is particularlyeasy to use with one single dose given to thewoman at the onset of labour, and one dose ofsyrup administered to the baby within 72 hoursof delivery, reducing transmission by around40%, from a rate of 20% to 12% at six to eightweeks postpartum (Guay et al. 1999). Transmis-sion rates at six to eight weeks of 15% have beenreported when ZDV is given to the mother fromweek 36 of gestation (Dabis et al. 1999; Wiktor1999). Peripartum ZDV efficacy has been re-ported as greater in women with higher CD4 cellcounts, even at six weeks postpartum (Leroy etal. 2002). In another regimen, ZDV given incombination with 3TC to the mother from weeks28–36 of gestation until one week postpartum,while the newborn receives ZDV prophylaxisduring one week, reduced transmission to be-tween 6% and 9% (Saba et al. 2002).
The respective efficacy of these differentantiretroviral regimens was compared in a recentpooled analysis using a standardized definitionof peripartum HIV infection (Leroy et al. 2005).This study included 4125 singleton live birthsfrom six African trials, which adjusted MTCTrates at six to eight weeks for other maternaland child determinants. In comparison with pla-cebo, the adjusted relative reduction in MTCTreached 77% for the combination of ZDV and3TC administered antepartum, intrapartum andseven days postpartum; 51% for the combina-tion of ZDV and 3TC during the intrapartumand postpartum periods only; 45% for ZDV only,administered antepartum, intrapartum and post-partum; and 40% for single-dose NVP. Thus, at
six to eight weeks, in comparison with NVP, onlythe longest combination of ZDV and 3TC is sig-nificantly more effective, leading to a 61% ad-justed reduction (p=<0.0005). These resultssuggest that there exists an equivalence of choicebetween single-dose NVP and short-course ZDV.They confirm that a combination of ZDV and3TC from 36 weeks of gestation has a greaterefficacy in reducing early transmission than thesame combination starting during labour anddelivery or than any single antiretroviral prophy-laxis (short-course ZDV or single-dose NVP).
There is no doubt that even lower peripartumtransmission rates, comparable to those obtainedin developed countries, could be achievedthrough enhanced short-course antiretroviralregimens. In the ANRS 1201/1202 Ditrame Pluscohort in Abidjan, Côte d’Ivoire, transmissionrates at six to eight weeks postpartum were 6.5%(95% CI 3.9–9.1%) with ZDV plus single-doseNVP, a relative 72% reduction compared withZDV alone (95% CI 52–88%, p=0.0002 ad-justed on maternal CD4 cell count, clinical stageof infection and breastfeeding status) (Dabis etal. 2005). The overall rate was 4.7% (95% CI2.4–7.0%) when mothers were given both ZDVand 3TC from week 32 of gestation, continuedfor one week postpartum (for both mother andchild), in addition to single-dose NVP to motherand infant. Despite these considerable advances,several problems remain to be addressed, whichare detailed elsewhere (WHO 2006).
Single-dose NVP given to women and infantsreduces mother-to-child HIV transmission andis easy to use, but NVP resistance develops in alarge percentage of women, raising concerns forfuture maternal treatment (Eshleman et al.2004a; Eshleman et al. 2004b; Jourdain et al.2004; Eshleman et al. 2005). Alternatives toNVP are being considered, but this problem canbe avoided to a considerable extent by a post-partum three-day to one week regimen of AZTand 3TC.
Residual MTCT rates remain high in motherswho have advanced HIV disease (Leroy et al.2002). Antiretroviral therapy is now recom-mended for these women (WHO 2006). Morerecent cohort studies in Côte d’Ivoire and Mo-zambique indicate that when three-drug combi-
MOTHER-TO-CHILD TRANSMISSION OF HIV

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
8
nation antiretroviral therapy (i.e. ART) is givento HIV-infected pregnant women either univer-sally – irrespective of CD4 cell count (Giulianoet al. 2007) – or only to those who require it fortheir own health (Tonwe-Gold 2007), MTCTrates below 5% can be achieved at four weekspostpartum.
Women presenting late for delivery withoutknowing their HIV status, which frequently hap-pens in resource-constrained settings, do not re-ceive the ante and intrapartum components ofthese regimens. In this context, the efficacy of asimple neonatal-only antiretroviral post-exposureprophylactic regimen has been demonstrated inMalawi. The overall MTCT rate at six to eightweeks was 15.3% in 484 babies who receivedNVP and ZDV and 20.9% in 468 babies whoreceived NVP only in the NVAZ trial conductedin Malawi (p=0.03) (Taha et al. 2003). In SouthAfrica, single-dose NVP given to newborns ex-posed to HIV tended to reduce MTCT. The rateat 12 weeks was 14.3% in 518 babies who re-ceived NVP, and 18.1% in 533 babies who re-ceived ZDV during six weeks postnatally(p=0.4). Among newborns who were not in-fected at birth, the 12-week MTCT rate was7.9% in the NVP arm and 13.1% in the ZDVarm (p=0.06) (Gray et al. 2005).
All these short-course peripartum antiretro-viral regimens have lower field efficacy when tak-ing into account the subsequent risk of postnataltransmission of HIV in African populations
where prolonged breastfeeding is the norm (Leroyet al. 2003). In the West African trials, the 24-month efficacy of short-course ZDV to motherswas still significant, giving a 26% reduction, witha residual MTCT rate of 22.5% in the ZDV armcompared to 30.2% in the placebo arm (Leroyet al. 2002). In the NVP trial, the 18-monthefficacy was sustained with a residual MTCT rateof 15.7% in the NVP arm, a 41% significant re-duction (Jackson et al. 2003). In the PETRA trial,although the six-week efficacy of the combinedZDV+3TC long-course (ante, intra and postpar-tum/postnatal) regimen and the ZDV+3TCmedium-course (intra- and postpartum/postna-tal) regimen was significantly effective, the 18-month long-term efficacy was lost mainlybecause of postnatal transmission (Saba et al.2002). However, this trial lacked statistical powerto address differences at 18 months.
Given the considerable advances that havebeen made in the past ten years, peripartum HIVtransmission rates below 5% can be achieved,even in African breastfeeding populations, withrelatively inexpensive, easy-to-use and feasibleshort-term antiretroviral combinations (WHO2006). The introduction of short-courseantiretroviral regimens to prevent MTCT in less-developed countries should be accompanied byinterventions to minimize the risk of subsequenttransmission through breastfeeding (Leroy et al.2003). Postnatal transmission will be detailedin the next section.

9
HIV transmission throughbreastfeeding
Transmission of HIV through breastfeedinghas been well documented since 1985. The
first reports indicating the possibility of HIVtransmission through breast milk were inbreastfed infants of women who had acquiredinfection postnatally through blood transfusionsor through heterosexual exposure (Ziegler et al.1985; Hira et al. 1990; Van de Perre et al. 1991;Palasanthiran et al. 1993). There were also re-ports of infants – with no other known exposureto HIV – who were infected through being wet-nursed and through pooled breast milk (Nduatiet al. 1994). There is a theoretical risk of oraltransmission from infant to wet-nurse, with caseshaving been reported (Visco-Comandini et al.2005).
Pathogenesis and mechanisms ofbreastfeeding transmissionHIV has been detected in breast milk in cell-freeand cell-associated compartments. To date moststudies have used DNA or RNA polymerasechain reaction assays to evaluate breast milk forHIV. In an early study from Kenya, breast milkHIV RNA was detected in 39% of 75 specimens(Lewis et al. 1998). In this study viral levels inbreast milk were about one log lower than inplasma. However, there were some cases thatsuggested compartmentalization of virus tobreast milk with higher levels in breast milk thanplasma. Viral variants in blood and breast milkwere found to be distinct, with some major vari-ants in breast milk not detected in blood. Thisfinding would suggest that some virus in breastmilk replicates independently, in the mammarycompartment. The observation of a compart-mentalization of HIV between peripheral bloodand breast milk highlights that postnatal trans-mission of HIV can occur with variants that may
not be predicted from the analysis of circulatingviral populations (Becquart et al. 2002).
The origin of HIV in breast milk is still notwell understood. There is now evidence that bothcell-free and cell-associated HIV in breast milkare responsible for breast-milk transmission(Koulinska et al. 2006). Studies have demon-strated the presence of cell-free virus and latent(non-productive) infected cells, but not produc-tive HIV infective cells. Cells, includingmacrophages and lymphocytes, and cell-free vi-rus may migrate from the systemic compartmentto breast milk. Recently, it has been reported thatinfected CD4 cells demonstrate a greater capac-ity to enter into a viral replication cycle in thebreast-milk compartment compared with blood(Petitjean et al. 2006).
Following ingestion of HIV infected breastmilk, infant gut mucosal surfaces are the mostlikely site at which transmission occurs. Cell-freeor cellular HIV may penetrate to the submucosathrough mucosal breaches or lesions, viatranscytosis through M cells or enterocytes ex-pressing galactosyl ceramide (Gal Cer) or Fcreceptors. In vitro models suggest that secretoryIgA or IgM may inhibit transcytosis of HIVacross enterocytes (Bomsel 1997; Bomsel et al.1998). Breast-milk HIV immunoglobins mayplay a role in protection from transmission bycoating infant mucosal surfaces: in a cohort oflactating women infected with HIV in Rwanda,anti-HIV antibodies of the IgG isotype were morefrequently detected in breast milk followed bysecretory IgM (Van de Perre et al. 1993). Tonsilsmay also be a portal of entry for HIV in breast-milk transmission. Tonsils include M cells in closeproximity to lymphocytes and dendritic cells, andtonsillar M cells are capable of HIV replication(Frankel et al. 1997).

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
10
Risk of postnatal transmission throughbreastfeedingThe risk attributable to transmission of HIVthrough breastfeeding has been difficult to meas-ure because of the difficulty in distinguishingintrapartum transmission from early transmis-sion through breastfeeding.
Based on an assessment of the limited dataavailable in the early 1990s, the additional riskof transmission from breast milk – above thatoccurring during pregnancy and delivery – amongwomen with established HIV infection was esti-mated to be approximately 15% whenbreastfeeding continued for two years or more.When the mother acquires HIV postnatally, theestimated risk of transmission is estimated to be29% (95% Cl: 16–42%) (Dunn et al. 1992).
Subsequent data, including the results of arandomized clinical trial, confirm these initialfindings in HIV-infected pregnant women. In theclinical trial in Nairobi, HIV-infected pregnantwomen were randomly allocated to either breast(n=212) or formula (n=213) feeding groups inthe absence of any preventive antiretroviral in-tervention (Nduati et al. 2000). Compliance withassigned feeding modality was 96% in thebreastfeeding arm and 70% in the formula arm.Median duration of breastfeeding was 17months. The cumulative probability of HIV in-fection at 24 months of age was 36.7% in thebreastfeeding arm and 20.5% in the formula-feeding arm, with 44% of HIV infection in thebreastfeeding arm attributable to breastfeeding.Most breastfeeding transmission occurred early,although transmission continued throughout theduration of exposure (Nduati et al. 2000). Al-though exclusive breastfeeding was recom-mended in this trial it was likely not alwaysexclusive in this population. Furthermore, infor-mation on the mode of breastfeeding was notcollected.
Other estimations of the rate of transmissionthrough breastfeeding can be inferred from theresults of trials in which a peripartum interven-tion to reduce MTCT risk was evaluated both inthe short-term (four to six weeks) and in the long-term, after the end of breastfeeding exposure at18–24 months. Additional postnatal transmis-
sion beyond four to six weeks ranging from 4%to 12% was reported from these trials (Ekpini etal. 1997; Saba et al. 2002; Jackson et al. 2003;Leroy et al. 2003). Differences need to be inter-preted according to the risk factors for postnataltransmission. However, there is strong evidenceof a continued increase in cumulative transmis-sion risk as long as the child is breastfed (Leroyet al. 1998; Miotti et al. 1999; Leroy et al. 2003;The Breastfeeding and HIV International Trans-mission Study Group (BHITS) 2004; Iliff et al.2005).
Timing of postnatal transmissionthrough breastfeedingTransmission of HIV through breastfeeding cantake place at any time during lactation. There isinsufficient information available to estimate theexact association between duration of breast-feeding and the timing of transmission. How-ever, there is some evidence that there is anincreased early postnatal risk within the first sixto eight weeks. This still remains uncertain, how-ever; a late postnatal risk beyond six to eightweeks has been better characterized recently(The Breastfeeding and HIV International Trans-mission Study Group (BHITS) 2004).
Early postnatal transmission throughbreastfeedingData suggest that the first six to eight weeks ofbreastfeeding could be a high risk period fortransmission of HIV. However, it is difficult toinvestigate for technical reasons, and thus diffi-cult to draw any conclusions about the relativerisk of transmission through colostrum and ma-ture breast milk (Van de Perre et al. 1993; Ruffet al. 1994; Lewis et al. 1998). First, colostrumand mature breast milk contain different typesof cells and varying levels of immune-modulat-ing components (e.g. vitamin A, immunoglobu-lins and lactoferrin). Second, the total volumeof colostrum ingested by the infant is muchsmaller than that of mature breast milk. Third,the infant’s immune system is less well-devel-oped during the first few days of lactation thanin later lactation, while younger infants have anincreased blood concentration of maternal anti-

11
bodies. There is no evidence to suggest thatavoidance of colostrum would reduce the risk ofbreastfeeding transmission to the infant.
Based on statistical modelling using data fromstudies with a limited duration of breastfeeding,it appears that the highest risk period for trans-mission is within the first four to eight weeks oflife, and that infectivity may vary in populationsat different stages of the disease (Dunn 1998).Evidence remains weak to detail the percentageof transmission occurring early. In the rando-mized clinical trial of breast milk versus formulacarried out in Nairobi, Kenya, 10% of the total16% cumulative difference in infection rates be-tween infants in the breastfed and formula-fedarms apparently occurred by week six of age. Thecumulative rate of HIV infection in the formula-feeding arm was approximately half that of thebreastfeeding arm at birth (3.1% versus 7.0%,p=0.35). Although not statistically significant,this differential between arms raised concernabout the true comparability of the two arms atbirth, with women in the breastfeeding arm hav-ing more advanced disease than in the formula-feeding arm (Bulterys 2000).
Additionally, the breastfeeding women werelikely more ill as evidenced by the much higherthan expected mortality in this group comparedto the women giving formula to their children(Nduati et al. 2001). In the Kenya trial, the pro-portion of new HIV infections between birth andsix to eight weeks was 6.3% (from 3.1% to 9.7%in formula-fed versus 7.0% vs19.9% in breastfedbabies, p=0.005) (Nduati et al. 2000). Seventy-five per cent of the risk difference between thetwo arms occurred by six months of age, althoughtransmission continued throughout the durationof exposure (Nduati et al. 2000). In a subsequentanalysis of this data, 75% of the risk differencebetween the two arms occurred by six months ofage, although transmission continued through-out the duration of exposure (Nduati et al. 2000).In a subsequent analysis of this trial data, theprobability of transmission through breastfeedingwas estimated to be 0.00064 per litre of breastmilk ingested and 0.00028 per day ofbreastfeeding (Richardson et al. 2003). Breast-milk infectivity was significantly higher for moth-ers with low CD4 cell counts and high RNA viral
load in plasma. Of note, the probability of infec-tion through breastfeeding per day of exposurewas not significantly different for children agedless than four months versus those older thanthis (0.00015 versus 0.00031, p=0.4).
In the SAINT trial in South Africa, althoughnot randomized on infant feeding modalities, theproportion of new infections having occurredbetween birth and six to eight weeks increasedto 5.6% when comparing breastfed infants toformula-fed infants (Moodley et al. 2003).
Late postnatal transmission throughbreastfeedingLate postnatal risk of HIV transmissionthrough breastfeeding can be reliably estimatedamong children born to infected mothers whotested negative at four to six weeks postpar-tum. These children are followed until afterthey cease breastfeeding to determine their rateof acquisition of HIV infection throughbreastfeeding. The time at which the exposurestarts is determined by the age at which in-fants are tested. This is now usually aroundfour to six weeks of age, but in earlier studieswas between three and six months of age. Thesedifferent ‘starting points’ may explain differ-ent estimates of rates of late postnatal trans-mission between studies (Table 2).
The best evidence on the risk of late postna-tal transmission comes from a meta-analysis ofa large number of data relating to breastfeedingand postnatal transmission of HIV fromrandomized controlled trials of peripartum in-terventions conducted in sub-Saharan Africa.Early transmission was defined as a positive HIVtest before four weeks, and late postnatal trans-mission as a negative diagnostic test at or afterfour weeks of age, followed by a subsequent posi-tive test result (The Breastfeeding and HIV In-ternational Transmission Study Group (BHITS)2004). Of 4085 children (breastfed singletonsfor whom HIV testing was performed) from nineeligible trials, 993 (24%) were definitively in-fected (placebo arms, 25.9%; treatment arms,23.4%, p=0.08). The time of infection was un-known for 454 children. Of 539 children wherethe time of infection was known, 225 (42%) wereinfected during the late postnatal period. Late
HIV TRANSMISSION THROUGH BREASTFEEDING

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
12
postnatal transmission occurred throughoutbreastfeeding. The cumulative probability of latepostnatal transmission at 18 months was 9.3%(95% CI 3.8-14.8%). The overall risk of latepostnatal transmission was 8.9 transmissions per100 child-years of breastfeeding (95% CI 7.8-10.2 per 100 child-years) follow-up (Table 2).Late postnatal transmission could contribute asmuch as 42% to the overall rate of MTCT (TheBreastfeeding and HIV International Transmis-
sion Study Group (BHITS) 2004). Analysis ofhow transmission rates vary with time from birthindicated that late postnatal transmission risk isaround 1% per month of breastfeeding and isconstant over time from four to six weeks and18 months, i.e. between 0.8 and 1.2 per 100child-months of breastfeeding. The longer theduration of breastfeeding, the higher the cumu-lative risk of postnatal transmission of HIV.
TABLE 2. Estimated rates of late postnatal transmission of HIV in African cohorts
Study location
(citation)
Malawi (Miotti et al. 1999)
Africa (Leroy et al. 1998)
West Africa(Leroy et al.
2003)
Africa BHITS (The
Breastfeeding and HIV
International Transmission
Study Group (BHITS)
2004)
Zvitambo, Zimbabwe (Iliff
et al. 2005)
South Africa, the Vertical
Transmission Study
(Coovadia et al. 2007)
Côte d’Ivoire, the ANRS
1201/1202 Ditrame Plus
study (Leroy et al. 2004)
Age at nega-
tive test
(determining
denominator)
1 month
3 months
4 weeks
4 weeks
6 weeks
4-8 weeks
4 weeks
Median
duration of
breastfeeding
>12 months
16 months
12 months
10 months
>18 months
6 months
5 months
Infection inci-
dence per 100
child-years of
breastfeeding
(%)
6.9
3
8.6
8.9
9.2
10.7 (EBF only)
3.8
EBF: 5.9
PBF: 11.3
MF: 31.6
Cumulative
percentage of
infants in-
fected by 12
months
8.9
2.5
9.5
7
7.7
EBF: 3.42
PBF: 7.29
MF: 8.41
NA
NA
Cumulative
percentage of
infants in-
fected at last
follow-up
10.3 (18 months)
9.2 (36 months)
13.1 (18
months); 13.1
(24 months)
9.3 (18 months)
12.1 (18 months)
EBF: 6.94
PBF: 8.56
MF: 13.92
EBF: 4.04 (6
months)
NA
NA, not available; EBF, exclusive breastfeeding; PBF, predominant breastfeeding; MF, mixed feeding (breast milk and other
fluids, foods and/or formula).

13
HIV TRANSMISSION THROUGH BREASTFEEDING
In conclusion, the rate of late postnatal trans-mission is now better characterized than previ-ously and is estimated to be around 1% permonth of breastfeeding and constant over time.When breastfeeding is prolonged to 18-24months or beyond, the additional cumulativepostnatal risk of transmission throughbreastfeeding varies from 4% to 16% accordingto the study (Miotti et al. 1999; Nduati et al.2000; Jackson et al. 2003; Leroy et al. 2003).
Factors associated with risk oftransmission of HIV throughbreastfeedingThere is reliable quantification of the effect ofrisk factors associated with an increased or de-creased likelihood of transmission of the virusthrough breastfeeding. Clinical, immunologicaland virological factors in mothers, as well as in-fant feeding patterns, affect postnatal transmis-sion (Table 3).
Maternal factorsMaternal seroconversion during breastfeedingHIV maternal seroconversion during breastfee-ding constitutes a high risk factor for postnatalHIV transmission; it is higher than amongwomen who have been infected previous tobreastfeeding (Van de Perre et al. 1991; Dunn etal. 1992). High levels of virus in plasma, andprobably also in breast milk, are seen in primary
HIV infection, when the rate of postnatal trans-mission has been estimated to be nearly 30%(Dunn et al. 1992). In a study in Kenya, therelative risk of MTCT was increased about six-fold during primary infection of the mother(Embree et al. 2000).
HIV-related immune statusMore data are now available on the associationbetween maternal immune status (CD4 cellcounts) and MTCT through breastfeeding. Ma-ternal immunosuppression defined by low CD4cell count, although strongly correlated withplasma RNA viral load, is an independent riskfactor for breastfeeding transmission in all stud-ies with available information. In an analysis ofpooled data from two West African ZDV trials(Leroy et al. 2002; Leroy et al. 2003), maternalCD4 cell counts below 500 cells per mm3 inplasma close to time of delivery was associatedwith a threefold increase in risk of late postnataltransmission compared to women with CD4 cellcounts equal to or greater than 500 per mm3(Leroy et al. 2003). In the BHITS meta-analysisof data from nine intervention trials in sub-Sa-haran Africa, the risk of late postnatal acquisi-tion of infection after four weeks of age wasstrongly associated with maternal CD4 cellcount. Transmission increased eightfold whenCD4 cell counts were below 200 per ml, and 3.7-fold where CD4 cell counts were between 200and 500 per ml, compared to the reference group
Table 3. Factors associated with transmission of HIV through breastfeeding
InfantFactors associated with the immune system
Pattern of infant feeding (exclusive breastfeeding versus
mixed)
Morbidity leading to less vigorous suckling, milk stasis and
increased leakage of virus across milk ducts (oral thrush)
MaternalYounger maternal age, lower parity
Maternal seroconversion during lactation
Clinical and/or immunological (CD4 cell count) disease
progression
RNA viral load in plasma
RNA viral load in breast milk
Local immune factors in breast milk
Breast health (subclinical or clinical mastitis, abscess,
cracked nipples) (indirect factor)
Maternal nutritional status
Duration of breastfeeding
Source: Adapted from John-Stewart et al. (2004).

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
14
of CD4 cell count above 500 per ml (TheBreastfeeding and HIV International Transmis-sion Study Group (BHITS) 2004). In the Verti-cal Transmission Study in South Africa, infantsborn to mothers with CD4 cell counts less than200 cells per mm3 were almost four times morelikely to acquire HIV or die than were those bornto mothers with CD4 cell counts greater than500 cells per mm3; and those born to motherswith CD4 cell counts between 200 and 500 cellsper mm3 were 2.2 times more likely to acquireHIV or die (Coovadia et al. 2007).
RNA viral load in plasma and breast milkIncreased maternal RNA viral load in plasma andbreast milk are both strongly associated withincreased risk of transmission throughbreastfeeding. In West Africa, the rate of latepostnatal transmission increased 2.6-fold forevery one log10 increase in plasma RNA viralload (measured in late pregnancy) (Leroy et al.2001; Leroy et al. 2003). Breast-milk HIV RNAlevels correlate with systemic viral load(Willumsen 2003), and are likely to be associ-ated with risk of breast-milk HIV transmission(Semba et al. 1999a; Willumsen 2003). In Ma-lawi, the risk of transmission increased fivefoldwhen RNA virus had been detected in breast-milk samples taken at six weeks postpartum(Semba et al. 1999a). In Nairobi, breast-milkRNA levels were assessed in serial samples up totwo years after delivery (John et al. 2001). Inanalyses comparing 92 infected infants with 187infants who were uninfected at two years, ma-ternal plasma RNA, mastitis and breast abscesswere associated with late transmission (occur-ring after two months postpartum). Median RNAload in colostrum and early milk was higher thanin mature milk collected more than 14 days af-ter delivery. Breast-milk RNA load was signifi-cantly associated with transmission throughbreastfeeding. In a study conducted in Durban,South African women with detectable RNA vi-ral load in breast milk at any time during thefirst six months postpartum were more likely totransmit than those with undetectable RNA vi-ral load (Pillay et al. 2000).
The evolution of HIV RNA in breast milk af-ter peripartum antiretrovirals needs to be better
understood. In particular, viral load rebound (i.e.increased levels of the virus after cessation ofantiretrovirals) in breast milk after discontinua-tion of peripartum antiretrovirals is of concern(Van de Perre et al. 1997). An increase in thelevels of HIV RNA in breast milk from day eightto day 45 after delivery was associated withmaternal short-course ZDV prophylaxis com-pared to the placebo group in the Ditrame PlusANRS 049a trial (Manigart et al. 2004). In thisWest African trial, breast-milk HIV-RNA from28 women who transmitted HIV postnatally andfrom 130 women who did not transmit HIV wascompared. Levels of HIV RNA in breast milk atday eight after delivery and its increase from dayeight to days 45-90 postpartum were both inde-pendently associated with postnatal transmission(Manigart et al. 2004). Although HIV transmis-sion continues after cessation of peripartumantiretroviral therapy, there is no clinical evidenceto suggest that stopping antiretroviral therapyin this early period is associated with an increasedrate of breastfeeding transmission due to viralrebound after cessation of antiretrovirals. Indeed,in the pooled analysis of the West African trialsusing short-course perinatal ZDV prophylaxis,the cumulative postnatal transmission risks weresimilar in the ZDV (9.8%, n=254) and placebogroups (9.1%, n=225) at age 24 months (Leroyet al. 2003). The long-term overall efficacy ofthis peripartum ZDV regimen was reduced inboth groups. Global recommendations onantiretrovirals during pregnancy are available(WHO, 2006).
Anti-infective properties of breast milk in HIV-infected womenBreast milk contains maternal antibodies, withall basic forms of immunoglobulins IgG, IgM,IgA, IgD, and IgE present. The most abundantis usually secretory IgA (Lawrence & Lawrence2004). The role of breast-milk HIV-specific an-tibodies in inhibiting HIV transmission throughbreastfeeding has been investigated ( Van de Perreet al. 1993, Kuhn et al. 2006). The breast milkof women with established HIV infection hasbeen found to have HIV-specific IgG, with itswide spectrum of activity against HIV proteins,comparable to HIV-specific IgG in serum. The

15
HIV TRANSMISSION THROUGH BREASTFEEDING
spectrum of activity of serum IgA against HIVhas been found to be similar to that of serumIgG, but the spectrum of activity of HIV-spe-cific secretory IgA (sIgA) in breast milk is di-rected against only a limited number of viralproteins (envelope protein, glycoprotein 160,core proteins). In Zambia, HIV-specific sIgA wasdetected more often in breast milk of transmit-ting mothers (76.9%) than in breast milk of non-transmitting mothers (46.9%, p=.009). Theauthors concluded that HIV-specific sIgA inbreast milk did not appear to be a protective fac-tor against HIV transmission among breastfedinfants (Kuhn et al. 2006).
In another study in Zambia, the concentra-tion of alpha-defensins in breast milk was sig-nificantly associated with reduced transmissionthrough breastfeeding (Kuhn et al. 2005). Thisis consistent with earlier work in Rwanda (Vande Perre et al. 1993), where the most frequentlyidentified HIV-specific antibody in breast milkwas IgG (in >95% of samples), the next was IgM(in 41-78% of samples) and the least frequentwas IgA (in 23-41% of samples). Low levels ofHIV-specific IgM in breast milk collected at 18months were associated with a high risk of trans-mission of HIV.
Other components of breast milk are protec-tive against viral infections. Human lactoferrinhas been shown in vitro to have an inhibitoryactivity against HIV (Van de Perre 1999), andlipid-dependent antiviral activity, specifically di-rected at HIV. Data suggest the presence of HIV-specific major HIV CD8(+) cytotoxic Tlymphocytes in breast milk of HIV-infectedwomen could play a role in limiting transmis-sion and provide a rationale for vaccine strate-gies to enhance these responses (Sabbaj et al.2002).
Breast healthBreast health has also been associated with therisk of transmission through breastfeeding, withbreast pathologies such as clinical and subclini-cal mastitis, nipple bleeding, abscess or fissuresrelatively common in HIV-infected populations.In Kenya, clinical mastitis was detected in 7-11%of HIV infected mothers (John et al. 2001), whilethe estimated prevalence of subclinical mastitis
elsewhere, defined as having elevated levels ofsodium and/or potassium in breast milk, in stud-ies of HIV-infected mothers six to 14 weeks af-ter delivery ranged from 11 to 16% (Semba etal. 1999b; Willumsen 2001; Willumsen 2003).Nipple lesions have been detected in 10-13% ofHIV-infected mothers in several cohort studies(Embree et al. 2000; John et al. 2001; Ekpini etal. 2002). Breast abscess on clinical exam wasdetected at least once in 12% of breastfeedingmothers over a two-year follow-up period in onestudy and in 3% of mothers in another studywith a shorter follow-up period. Mastitis, abscess,and nipple lesions have all been associated witha relative increase in the risk of transmissionthrough breastfeeding (Semba et al. 1999a;Embree et al. 2000; Willumsen 2000; John etal. 2001; Willumsen 2003).
Nutritional statusMaternal nutritional status may influence riskof transmission overall, as well as breastfeedingtransmission. In a randomized trial investigat-ing the effect of multivitamins and vitamin A onthe risk of transmission, multivitamins (exclud-ing A) given to the mother had no effect on theoverall risk of transmission. However, vitamin Aalone was associated with a slight increase inMTCT, and an increased risk of transmissionduring breastfeeding (Fawzi et al. 2002b).Multivitamins were associated with a non-sig-nificant reduction in breastfeeding transmissionand mortality of the infant in the first two yearsof life. In a further analysis of these data, chil-dren of women who were randomized to receivemultivitamins during pregnancy and lactationhad a significantly lower risk of diarrhoea(p=0.03) and a substantially higher mean CD4cell count (p=0.006) than those in the arm withno multivitamins. The benefit for HIV-infectedchildren was similar to that for uninfected chil-dren.
Vitamin A supplementation given to mothersreduced the risk of respiratory infections in thechild (p=0.03) but was not associated with areduction in diarrhoea. It has been speculatedthat antioxidant micronutrient (e.g. vitamin E,selenium, vitamin A and B-carotene) deficien-cies may increase the risk of mastitis and there-

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
16
fore the risk of MTCT (Semba et al. 1994; Semba& Neville 1999). Finally, in Zimbabwe, theZvitambo trial did not report a significant roleof vitamin A supplementation on the risk of post-natal transmission (Iliff et al. 2005). However,the investigators reported that severe anaemia(<70g/l) and low maternal arm circumferencerelated to nutritional maternal health, were in-dependent risk factors for HIV transmission post-natally (Iliff et al. 2005). These findings highlightthe importance of nutritional support for HIV-infected breastfeeding women, but more clarityis needed about which interventions would bestdecrease postnatal transmission of HIV.
Infant factorsIntegrity of mucous membranesFactors resulting in disruption of the integrity ofinfants' mucous membranes, such as oral thrush,may be associated with an increased risk of trans-mission through breastfeeding. However, the di-rection of any causality is difficult to establishsince early HIV infection may also be associatedwith thrush (Ekpini et al. 1997; Embree et al.2000). Infant oral thrush can also lead to ma-ternal nipple thrush and fissures. Feeding withcow's milk, allergic reactions to complementaryfoods and infectious illness can all result in in-testinal damage, which could also be a risk fac-tor for transmission. It has also beenhypothesized that the intestinal permeability ofthe young infant may be affected by mode offeeding, with infants who receive only breast milkhaving a less permeable and therefore healthierlining of the gut than those who also receive otherfoods. However, in the one study carried out toinvestigate this further, feeding mode was notassociated with infant intestinal permeability(measured with lactulose-mannitol ratios, i.e.dual sugars), although infants who had been di-agnosed with HIV infection at 14 weeks hadhigher permeability at six and 14 weeks thandid uninfected children (Rollins et al. 2001).
Immune factorsA well-characterized innate factor that has beenconsidered for protection against mucosal trans-mission of HIV, including by breast milk, is se-
cretory leukocyte protease inhibitor (SLPI). In-fant salivary SLPI has been associated with de-creased risk of late breast-milk HIV transmission(Farquhar & John-Stewart 2003). However, in astudy of 43 unselected HIV-infected breastfeed-ing mothers in Bangui, with breast-milk samplesobtained at one week, four weeks and six monthsafter delivery, the mean levels of SLPI in breastmilk of mothers who transmitted HIV did notsignificantly differ from those of mothers whodid not transmit HIV (Becquart et al. 1999).Further controlled studies are needed to confirmthe role of maternal and infant SLPI in trans-mission, either alone or in combination withother innate and specific immune factors. Inaddition, HIV-specific cellular immune responsesto HIV envelope peptides detected in HIV-ex-posed infants are associated with reduced trans-mission through breastfeeding (Kuhn et al.2001).
Patterns of infant feeding: mode and durationOf greater importance than other factors, themode of infant feeding is now clearly associatedwith HIV transmission through breast milk. Inmost populations worldwide, breastfeeding isusually initiated, but supplemented with water,other drinks or foods at an early age (Nicoll etal. 2000a). Exclusive breastfeeding for the rec-ommended six months is uncommon, althoughglobally rates are increasing (UNICEF 2005).There is observational evidence from three largestudies that exclusive breastfeeding is associatedwith a lower risk of postnatal transmission ofHIV compared to non-exclusive breastfeeding,that is, breastfeeding with formula, other fluids(water, fruit juice) or solids (Table 2). In a studyin Durban, South Africa, 551 HIV-infectedwomen self-selected to breastfeed or formula feedafter being counselled (Coutsoudis et al. 2001).Breastfeeding women were encouraged to prac-tise exclusive breastfeeding for three to sixmonths. A total of 157 women formula-fed theirinfants from birth and never breastfed, 118 ex-clusively breastfed for three months or more and276 women mixed fed. The three feeding groupsdid not differ in any of the significant risk fac-tors for transmission, and at birth the rate of

17
infection in their infants was similar at about7%. Children who received both breast milk andother foods before three months were signifi-cantly more likely to be infected by 15 monthsof age (36%) than those who were exclusivelybreastfed until at least three months (25%) orthose who had been formula-fed (19%). Exclu-sive breastfeeding was associated with a signifi-cantly lower risk of HIV infection than mixedbreastfeeding (hazard ratio, HR, 0.56, 95% CI0.32-0.98) and had a similar risk to children whowere never breastfed (HR 1.19, 95% CI 0.63-2.22).
In the Vertical Transmission Study in SouthAfrica, 1132 of 1372 (83%) infants born to HIV-infected mothers initiated exclusive breastfeedingfrom birth. Of 1276 infants with complete feed-ing data, median duration of cumulative exclu-sive breastfeeding was 159 days (first quartile tothird quartile, 122-174 days). Further, 14.1%(95% CI 12.0-16.4) of exclusively breastfed in-fants were infected with HIV by age six weeksand 19.5% (95% CI 17.0-22.4) by six months;risk was significantly associated with maternalCD4 cell counts below 200 per mm3 (adjustedHR 3.79, 95% CI 2.35-6.12), and birth weightless than 2500 g (adjusted HR 1.81, 95% CI1.07-3.06). Kaplan-Meier estimated risk of ac-quisition of infection at age six months was4.04% (95% CI 2.29-5.76) (Coovadia et al.2007). Breastfed infants who also received sol-ids were significantly more likely to acquire in-fection than were exclusively breastfed children(HR 10.87, 95% CI 1.51-78.00, p=0.018), aswere infants who at 12 weeks received bothbreast milk and formula milk (HR 1.82, 95%CI 0.98-3.36, p=0.057). Cumulative three-month mortality in exclusively breastfed infantswas 6.1% (95% CI 4.74-7.92) versus 15.1%(95% CI 7.63-28.73) in infants given replace-ment foods (HR 2.06, 95% CI 1.00-4.27,p=0.051) (Coovadia et al. 2007).
In Zimbabwe, children who received bothbreast milk and other foods or were predomi-nantly breastfed during the first three monthsof life were significantly more likely to be infectedby 18 months of age (13.9% and 8.6% respec-tively) than those who were exclusively breastfed
(6.9%) (Iliff et al. 2005). In Côte d'Ivoire, mixedbreastfed children tended to have a higher post-natal transmission risk than exclusively breastfedchildren, although the difference was not signifi-cant (Leroy et al. 2004). These data support thehypothesis that exclusive breastfeeding carries alower risk than mixed feeding. This phenomenoncould be explained by the effect of enteric infec-tion caused by the early introduction of foodson the integrity of the infant intestinal gut (Gotoet al. 1999). It has been hypothesized that in-creased risk of transmission with mixed feedingearly in life could be associated with increasedgut permeability or levels of local inflammation.Another potential mechanism is that mixed feed-ing may be associated with suboptimalbreastfeeding practices and with subclinical mas-titis, or it could be due to confounding betweenmixed feeding and susceptibility to infection.
Duration of breastfeeding is confirmed to beone of the main risk factors for HIV transmis-sion through breastfeeding. In Zimbabwe, amongthe 2060 children exposed to breastfeeding, therisk of postnatal transmission was 12%; 68% oftransmission events occurred after six months(Iliff et al. 2005). This is consistent with studiesin West Africa (Leroy et al. 2003), South Africa(Coutsoudis et al. 2001) and the United Repub-lic of Tanzania (Fawzi et al. 2002a). The authorsin Zimbabwe concluded that early cessation ofbreastfeeding could prevent a sizable proportionof postnatal HIV infections, but that this canonly be done when women are socially supportedto do so, and when safe, nutritionally adequatealternatives are available.
SexIn the international meta-analysis of late post-natal transmission (The Breastfeeding and HIVInternational Transmission Study Group(BHITS) 2004), covariates potentially affectingthe relationship between breastfeeding and latepostnatal transmission of HIV were evaluated,including both maternal variables (age, parity,CD4 cell count) and child variables (birth weight,sex). Neither maternal age, parity nor birthweight were significantly associated with latepostnatal transmission, but maternal CD4 cell
HIV TRANSMISSION THROUGH BREASTFEEDING

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
18
count and child's sex were, with girls being 40%less likely to become infected after four weeks ofage during breastfeeding than boys (HR 0.6, 95%CI 0.4-0.9, p=0.014). The risk of late postnataltransmission was highest for boys breastfed bymothers with CD4 cell counts below 200 permm3, followed by boys breastfed by mothers withCD4 cell counts between 200 and 499 per mm3
and then girls breastfed by mothers with CD4cell counts below 200 per mm3. It was previouslyreported in the European Collaborative Study,which studied the effect of sex among newbornsdelivered by elective caesarean section, that girlswere more at risk of antepartum and peripartum
infection than boys were (Thorne & Newell2004). Duration of breastfeeding was similaramong boys and girls, but no information wasavailable on the age at which, and what type ofother foods were introduced. This difference maybe due to boys receiving complementary foodsat an earlier age, which thus put them at higherrisk of becoming infected. Further research isongoing to confirm this finding, although a re-cent study did not confirm these differences intransmission rates between boys and girls dur-ing exclusive breastfeeding (Coovadia et al.2007).

19
Benefits of breastfeeding
Health benefits of breastfeeding in thegeneral population
Maternal health benefits
Exclusive breastfeeding helps a mother spaceher pregnancies. Healthy birth spacing is as-
sociated with improved birth outcomes and ma-ternal recovery following birth. A woman whoexclusively, or almost exclusively, breastfeeds herinfant during the first six months of life, and hasnot resumed menstruation, has a less than 2%risk of becoming pregnant during that time(WHO et al. 1995).
Child health benefitsCurrent evidence that breastfeeding is beneficialfor infant health is mainly based on observationalstudies. Potential sources of bias in such studieshave led to doubts about the magnitude of thesehealth benefits in developed countries. However,several randomized clinical trials show thatbreastfeeding is the best nutrition during the firstmonths of life (Nicoll & Williams 2002).
One of the most important benefits of breastmilk is its ability to protect against commonchildhood infections such as diarrhoea, pneumo-nia, neonatal sepsis and acute otitis media. In arecent outbreak of diarrhoea in Botswana, notbeing breastfed was the most significant risk fac-tor for diarrhoea and death among children(Creek 2006). Following a period of unusuallyheavy rainfall cases of diarrhoea quadrupled,from about 8500 in 2004 to more than 35 000,while deaths increased more than 20-fold, from24 to about 530. An epidemiological investiga-tion of the outbreak revealed that a large pro-portion of the infants who experienced diarrhoeawere not breastfed. In a multivariate analysis,lack of breastfeeding was the strongest predictorof infant diarrhoea, increasing the risk 50-fold.In one village, one third of formula-fed babies
died of diarrhoea, while none that were breastfeddid. Details are provided in section 5.3.5.
In a substudy of the Botswana outbreak, 93%of 153 babies with diarrhoea were not breastfed(about 75% were fed infant formula and the re-mainder were fed cow’s milk). Sixty-five per centof their mothers were HIV-positive, and amongthe infants, 18% were HIV-infected at the timeof the study. Kwashiorkor was the only signifi-cant predictor of death, not maternal or infantHIV status. In the United States of America, anationally representative cross-sectional homesurvey conducted from 1988 to 1994 docu-mented an increased risk of respiratory tract in-fections, including pneumonia and recurrentotitis media, in children who were fully breastfedfor four versus six months (Chantry et al. 2006).There are earlier studies showing the benefits ofbreastfeeding (Habicht et al. 1986; Victora etal. 1987; Victora et al. 2000; WHO Collabora-tive Study Team 2000). In a study in Brazil, therisk of hospital admissions for pneumonia wasincreased 17-fold in infants who were not beingbreastfed (odds ratio, OR, 16.7, 95% CI 7.7–36.0) compared to those being breastfed (Cesaret al. 1999).
Results from a pooled analysis of six case–con-trol studies carried out from 1983 to 1991 con-firm that breastfed infants have a reducedmortality risk compared to non-breastfed chil-dren (WHO Collaborative Study Team 2000).In the three studies in non-African settings whereoutcomes for breastfed infants could be comparedto that of non-breastfed infants, mortality rateswere significantly higher for non-breastfed in-fants through the first eight months of life. Thisfinding was particularly striking in the first fewmonths of life with a pooled odds ratio of 5.8(95% CI 3.4–9.8) for infants less than twomonths of age, indicating a nearly sixfold in-creased risk of mortality for these young non-

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
20
breastfed infants. The protective effect ofbreastfeeding is most marked in the first sixmonths of life and gradually diminishes as theinfant grows older.
More recently, the Promotion of BreastfeedingIntervention Trial (PROBIT), a cluster-randomized trial, has produced convincing evi-dence of benefit for term infants (Kramer et al.2001). Maternity hospitals were randomly allo-cated to receive an evidence-based interventiondesigned to increase the uptake and duration ofbreastfeeding according to the principles of theBaby-friendly Hospital Initiative sponsored bythe World Health Organization (WHO) and theUnited Nations Children’s Fund (UNICEF).Among the 16 491 mother-baby pairs followedfor 12 months, those born in intervention hos-pitals were significantly more likely to be exclu-sively breastfed at three and six months of age.Moreover these children had approximately halfthe risk of experiencing gastrointestinal infection(OR 0.60, 95% CI 0.40–0.91) and atopic eczema(OR 0.54, 95% CI 0.31–0.95).
The optimum duration of exclusivebreastfeeding in terms of health benefit has longbeen a subject of debate. In the PROBIT trial,the effects on infant growth and health compar-ing 2862 infants exclusively breastfed for threemonths with 621 infants who were exclusivelybreastfed at least six months were reported(Kramer et al. 2003). Weight and length gainwere slightly greater in the three-month groupbut the six-month group had a faster length gainfrom nine to 12 months and a larger head cir-cumference at 12 months. A significant reduc-tion in the incidence of gastrointestinal infectionswas observed during the period from three to sixmonths in the six-month group (adjusted inci-dence density ratio: 0.35 [0.13, 0.96]), but therewere no significant differences in risk of respira-tory infectious outcomes or atopic eczema. Ex-clusive breastfeeding for six months wasassociated with a lower risk of gastrointestinalinfection and no demonstrable adverse healtheffects in the first year of life in a general popu-lation with low HIV prevalence (Kramer et al.2003). This trial shows both that exclusivebreastfeeding prevalence can be increased by ahospital intervention promoting breastfeeding,
and that this is accompanied by significant healthgains during an infant’s first year of life. It alsodemonstrates that implementing exclusivebreastfeeding on a population basis is feasiblewith adequate support and training of health-care professionals (Kramer et al. 2001).
In a secondary analysis of a large randomizedclinical trial on immunization and Vitamin A,infant feeding patterns (exclusive breastfeeding,predominant breastfeeding, partial breastfeedingand no breastfeeding) were studied in relationto mortality and hospital admissions over sixmonths. Altogether, 9424 infants and theirmothers in Ghana, India and Peru were enrolledwhen infants were in the neonatal period. Themain outcome measures were all-cause mortal-ity, diarrhoea-specific mortality, mortality causedby acute lower respiratory infections and hospi-tal admissions. There was no significant differ-ence in the risk of death between children whowere exclusively breastfed and those who werepredominantly breastfed (adjusted HR 1.46,95% CI 0.75–2.86). Non-breastfed infants hada higher risk of dying when compared with thosewho had been predominantly breastfed (adjustedHR 10.5, 95% CI 5.0–22.0, p<0.001) as didpartially breastfed infants (adjusted HR 2.46,95% CI 1.44–4.18, p=0.001). These findingshighlight that the risks of death are high in non-breastfed children, but are significatly lower andsimilar for infants who are predominantlybreastfed and those who are exclusively breastfed.The authors suggested that in settings whererates of predominant breastfeeding are alreadyhigh, promotion efforts should focus on sustain-ing these high rates rather than on attemptingto achieve a shift from predominant breastfeedingto exclusive breastfeeding (Bahl et al. 2005).
In 2001, the World Health Assembly endorsedthe recommendation that infants should be ex-clusively breastfed for the first six months of lifeto achieve optimal growth, development andhealth. Thereafter, infants should receive nutri-tionally adequate and safe complementary foodswhile breastfeeding continues to 24 months orbeyond (WHO 2001). This recommendation hasconsidered the benefits of breastfeeding, as wellas the adverse effects associated with formulafeeding at an early age in the general population

21
with low HIV-prevalence (Kramer & Kakuma2004).
Health benefits of breastfeeding inchildren born to HIV-infected mothersThere is little information regarding whether thebreast milk from HIV-infected women confersimmune properties for both their uninfected andinfected children. HIV-infected women may haveimmune dysfunction and produce lower levelsof protective antibody and cell-associated immu-nity against diarrhoeal and respiratory infections;hence their milk would have lower levels of pro-tective antibodies, than women without HIVinfection. The findings from these two studiesindicate that breastfeeding does confer protec-tive benefits on HIV-exposed infants.
HIV-exposed children, regardless of HIV statusOnly two trials randomized on infant feedingpractices have been conducted among HIV-in-fected pregnant women and these have providedinformation on the health benefits of breastfee-ding among HIV-exposed children.
In a secondary analysis from a randomizedtrial aimed at evaluating mode of infant feedingon the risk of MTCT of HIV in Nairobi, Kenya(Nduati et al. 2000), the two-year mortality rateamong infants in the formula-feeding group was20%, not significantly different from the 24%figure in the breastfeeding group (HR 0.8, 95%CI 0.5–1.3), even after adjusting for HIV infec-tion status (HR 1.1, 95% CI: 0.7–1.7). The in-cidence of diarrhoea during the first two years oflife was also similar in both groups: 155 and 149per 100 child-years of follow-up in the formulaand breastfeeding groups respectively, while theincidence of pneumonia was identical at 62 per100 child-years of follow-up (Mbori-Ngacha etal. 2001). Infants in the breastfeeding armtended to have better nutritional status thanthose in the formula arm (p=0.06 overall), sig-nificantly so during the first six months of life(p=0.003). After adjusting for HIV infectionstatus, infants in the breastfeeding arm had sig-nificantly better nutritional status than those inthe formula arm over the two-year period(p=0.04). In this trial, there was substantial
movement between arms, and many in the for-mula arm left the study before follow-up.
On the other hand, in the Mashi trial in Bot-swana, results were slightly different from theKenya trial (Thior et al. 2006). The Mashi trialevaluated the efficacy and safety of breastfeedingand ZDV prophylaxis in infants for six monthscompared to formula feeding from birth and onemonth of ZDV prophylaxis of the infant for re-ducing postnatal transmission of HIV. There weresignificantly higher rates of mortality (mainlyrelated to diarrhoeal disease and pneumonia) informula-fed than in breastfed children in the firstsix months of life. The cumulative incidence ofinfant death was significantly higher in the for-mula-fed group than in the breastfed plus ZDVgroup at age seven months (9.3% versus 4.9%,p=0.003); however, this difference diminishedbeyond seven months, such that the mortalitythrough 18 months of age was not significantlydifferent (10.7% in the formula-fed arm versus8.5% in the breastfed arm, p=0.21).
HIV-infected childrenThere is more reliable information relating to thebenefits of breastfeeding for HIV-infected chil-dren issued from observational cohort studies(with available data from highly selective sam-ples). In a small study from Durban, South Af-rica, HIV-infected infants who were neverbreastfed had a poorer outcome than breastfedHIV-infected children: 60% of 15 never-breastfedinfected infants had three or more morbidityepisodes in the first 18 months of life comparedto 32% of 47 breastfed HIV-infected infants(Coutsoudis et al. 2003). During the first twomonths of life, never-breastfed infants, regard-less of their HIV status, were nearly twice aslikely to have had an illness episode as comparedto breastfed infants (OR 1.91, p=0.006). Twoearlier studies from South Africa compared 90 par-tially breastfed and exclusively formula-fed HIV-infected infants (Bobat et al. 1997); both groupshad similar frequencies of failure to thrive, episodesof diarrhoea and pneumonia, as did 43 uninfectedinfants born to HIV-positive mothers.
More recently, preliminary data presentedfrom Zambia in the ZEBS trial (Thea et al.
BENEFITS OF BREASTFEEDING

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
22
2004), showed that breastfeeding of HIV-in-fected infants beyond four months was associ-ated with improved survival compared tostopping breastfeeding at four months (Kuhn etal. 2007). These studies indicate that HIV-in-fected infants fare better when breastfed ratherthan formula fed.
Global breastfeeding practicesNearly all infants in developing countries areinitially breastfed from the first week of life(WHO Global Databank on Breastfeeding andComplementary Feeding 2006), and most chil-dren continue to be breastfed until at least sixmonths of age, frequently into the second yearof life (Nicoll et al. 2000a; WHO CollaborativeStudy Team 2000). Continued breastfeeding(beyond 12 months) is common in sub-SaharanAfrica and Asia, but less so elsewhere (Nicoll &Williams 2002). In 2005, it was estimated that
94% of infants in the world were breastfed forsome time, 79% of infants continuedbreastfeeding at age one year and 52% at twoyears of age (WHO Global Databank onBreastfeeding and Complementary Feeding2006).
Non-exclusive breastfeeding is common, andgiving fluids and foods in addition to breast milkis frequent (Becquet et al. 2005a). The practiceof exclusive breastfeeding at age one month var-ies according to geographic region and is mainlyobserved in East Africa and Nepal, while it re-mains low (less than 30%) in other regions (Fig-ure 1) (Nicoll et al. 2000b). Between 1990 and2000, the data suggest that exclusive breastfeed-ing levels in the developing world increased 15%overall among infants aged less than four months(from 46% to 53%) and aged less than sixmonths (from 34% to 39%) (Labbok et al. 2006;UNICEF Global Breastfeeding Databank 2005).
FIGURE 1. Prevalence of exclusive breastfeeding at four weeks of age in African and Asian children
Source: Adapted from Nicoll et al. (2000b)
100
90
80
70
60
50
40
30
20
10
0
Mal
awi 1
992
Nig
er 1
992
Burk
ina
Faso
199
3
Nig
eria
199
0
Cote
d’Iv
oire
199
4
Cent
ral A
fric
an R
epub
lic 1
994-
5
Gha
na 1
993
Sene
gal 1
992-
3
Cam
eroo
n 19
91
Zam
bia
1992
Mal
i 199
5
Zim
babw
e 19
94
Keny
a 19
93
Nam
ibia
199
2
Uni
ted
Repu
blic
of
Tanz
ania
199
1-2
Mad
agas
car
1992
Uga
nda
1995
Rwan
da 1
992
Paki
stan
199
0-1
Phili
ppin
es 1
993
Indo
nesi
a 19
94
Indi
a 19
92-3
Bang
lade
sh 1
993-
4
Nep
al 1
996
AFRICA ASIA

23
Strategies to reduce HIV transmissionthrough breastfeeding
Because guidance on prevention of HIV trans-mission in the peripartum period is relatively
non-controversial, research on the prevention ofmother-to-child transmission of HIV now con-centrates mostly on the breastfeeding period,including the primary prevention of HIV in lac-tating women, antiretroviral prophylaxis tomothers or their infants and other interventionsrelating to infant feeding practices (Dabis et al.2004; Kourtis et al. 2006). These interventionsneed to be tailored according to different con-texts.
Primary prevention of HIV in women ofchildbearing ageThe best approach to preventing HIV infectionin infants and young children, including trans-mission through breast milk, is to prevent HIVinfection of young girls and women of childbear-ing age (De Cock et al. 2002). In sub-SaharanAfrica, Asia and the Caribbean, the main modeof HIV transmission is heterosexual contact(Buve et al. 2002). In developed countries, al-though most women with HIV have a history ofinjecting drug use, or sexual partners with a his-tory of injecting drug use or bi-sexuality, hetero-sexual transmission has become an increasinglyimportant route of infection (European Collabo-rative Study 2001). The risk of HIV infection inwomen is increased by such factors as immatu-rity of the genital tract, cervical ectopy, sexuallytransmitted infections and poor nutritional sta-tus (Mostad et al. 1999). Cultural, social andeconomic factors also contribute to HIV trans-mission by increasing the vulnerability of girlsand women (Buve et al. 2002; De Cock et al.2002).
Strategies to prevent all MTCT should belinked to primary prevention programmes that
provide education about safer sex, condoms, anddiagnosis and treatment of sexually transmittedinfections, and that ensure the safety of medicalprocedures. HIV prevention should be empha-sized for women who test seronegative in preg-nancy (a considerable percentage of whom mayacquire infection in the two years after deliverywhile still breastfeeding) because of the particu-larly high risk of MTCT if mothers are infectedwith HIV during breastfeeding. In poorer set-tings, some of the benefits of breastfeeding re-sult from its physiological contraceptive effect,which helps to maintain an advantageous birthinterval; lactational amenorrhoea is 98% effec-tive as a contraceptive method (Vekemans 1997).Additionally, in some cultures there is a reduc-tion in coitus associated with breastfeeding,which may enhance this effect. Hence, the issueof contraception should be addressed, given thatinterventions for the prevention of MTCT in-clude replacement feeding and may include modi-fications to breastfeeding, such as early cessationas an option. Antenatal testing and counselling(including infant feeding options) for HIV-in-fected pregnant women are part of the strategyto reduce HIV transmission during breastfeeding.Such strategies must include high rates of ante-natal testing and use of interventions to reduceHIV transmission; ensuring continued contactbetween health-care professionals and mothersand infants from 18 to 24 months postpartumis also vital (Temmerman et al. 2003).
HIV prevention interventions directed at preg-nant and lactating women could contribute toreducing MTCT in several settings, but this cur-rently does not attract much research or program-matic effort (Rollins et al. 2007).

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
24
Framework to assess interventions toprevent postnatal transmissionThere are several conceivable interventions toprevent mother-to-child transmission of HIVthat are applicable to different settings. Theseinterventions need to be assessed as complexpublic health interventions using several evalu-ation criteria. The basic principle is to providedecision-makers (including women) with all rel-evant information needed to make interventionsavailable to solve this public health issue in theirspecific context. Safety is a key issue which ad-dresses negative adverse effects of interventionsaimed at preventing postnatal transmission. Itcould be assessed in various groups using differ-ent criteria: for the infant (morbidity, mortality,growth), for the woman (mortality, fertility), forthe general population (the spillover effect).1
Acceptability is a key issue in assessing inter-ventions aimed at reducing postnatal transmis-sion of HIV. It should be assessed at threedifferent population levels: the target population(in terms of social acceptability), the health sys-tem and decision-makers. Alternatives to pro-longed breastfeeding are often considered asunusual infant feeding practices in some partsof the world. It is therefore essential to evaluatemothers’ acceptance and use of these interven-tions, and their compliance with them in the longterm.
Effectiveness is the level to which the inter-vention meets its objectives when used in real-life conditions after the evidence of its efficacyis assessed in ideal conditions. Documentationof effectiveness in preventing postnatal transmis-sion could be assessed using both the residualoverall MTCT rate after the complete cessationof breastfeeding and the postnatal rate of trans-mission in conditions close to those of the con-text where implementation of the interventionis considered.
The full assessment of strategies aimed at pre-venting postnatal transmission of HIV throughbreastfeeding should balance benefits and risksof each infant feeding option in its specific con-text. An intervention should be recommendedonly if its positive effects outweigh its negativeeffects after balancing benefit and risk. The nega-tive effects of the intervention, therefore, mustalways be judged on whether risks can be mini-mized to an acceptable level, given the effective-ness. With this aim, HIV-free survival2 is a usefulindex with which to assess both effectiveness andsafety; indeed, it is now the most reliable andeasy measurement to assess the long-term effectof postnatal interventions (Alioum et al. 2001).
Modifying infant feeding options for HIV-infected women: replacement feedingModifying infant feeding practices could play animportant role in preventing postnatal risk andneeds to be assessed according to the local con-text. The first alternative to prolonged breastfee-ding consists of the complete avoidance ofbreastfeeding, which is then usually replaced bycommercial infant formula. Support for adequatereplacement feeding is needed throughout theperiod for which breast milk is normally recom-mended and during which the child is at great-est risk of malnutrition; that is, the first two yearsof life.
Table 4 presents data on replacement feedingoptions from various recent studies. The studiesinclude the Kenya trial conducted in an urbansite and published in early 2000 (Nduati et al.2000; Mbori-Ngacha et al. 2001); the MASHIrandomized clinical trial conducted in a semi-rural setting in Botswana (Thior et al. 2006);and the ANRS 1201/1202 Ditrame Plus cohortstudy conducted in an urban setting in Abidjan,Côte d’Ivoire (Becquet et al. 2007; Leroy et al.2007).
1 Spillover is a term used to designate the feeding behaviour of new mothers who either know that they are HIV-negativeor are unaware of their HIV status – they do not breastfeed, or they breastfeed for a short time only, or they mix-feed,because of unfounded fears about HIV or of misinformation or of the ready availability of breast-milk substitutes.
2 HIV-free survival refers to young children who are both alive and HIV-uninfected at a given point in time, usually 18months.

25
Adverse outcomes of alternatives tobreastfeeding practicesCompared to unrestricted breastfeeding, replace-ment feeding was shown to be safe in the clini-cal trial in Kenya, which allocated infant feedingpractices at random: morbidity and mortalityrates were similar over two years in breastfed andformula-fed children (Mbori-Ngacha et al.2001). The incidence of diarrhoea and pneumo-nia during the two years of follow-up was simi-lar in the formula and breastfeeding arms, andthere were no significant differences in incidenceof other recorded illnesses. Infants in thebreastfeeding arm tended to have better nutri-tional status, significantly so during the first sixmonths of life. However, the population studiedin this trial was urban with access to a relativelygood water supply, and it is crucial to determinewhether formula feeding could be a safe inter-vention in a more resource-poor population (Ta-ble 4).
In the Mashi trial in Botswana, all of themothers received ZDV from week 34 of gesta-tion and during labour. Mothers and infants werefirst randomized to receive single-dose NVP or aplacebo. Infants were then randomized to groupsprovided with six months of breastfeeding andprophylactic ZDV (breastfed plus ZDV), or sixmonths of formula feeding and one month ofZDV prophylaxis (Shapiro et al. 2005b; Thioret al. 2006). The median duration ofbreastfeeding was six months, and self-reportedcompliance with formula feeding high (93%).However, compliance with exclusive breastfeed-ing was poor. The cumulative incidence of in-fant death by month seven was significantlyhigher in the formula-fed group than in thebreastfed plus ZDV group (9.3% versus 4.9%,p=0.003), but this difference diminished beyondmonth seven, such that the time-to-mortalitydistributions through 18 months of age were notsignificantly different (10.7% versus 8.5%,p=0.21). Formula feeding was more commonlyassociated with severe diarrhoea and pneumo-nia (17.6%), which were also the leading causesof death in this group, compared to breastfedchildren (13.1%, p=.03). These results highlight
the relatively high morbidity and mortality ratesassociated with the feeding of formula, and theneed to carefully assess the local management ofchildhood illnesses before the implementationof a formula-feeding strategy in a given context.
In the ANRS 1201/1202 Ditrame Plus studyconducted in Côte d’Ivoire, the two-year occur-rence of adverse health events defined as hospi-talization or death was similar amongearly-weaned breastfed and formula-fed children(15% and 14%, respectively) (Becquet et al.2007). To assess whether these two modifiedinfant-feeding practices were safe as opposed toa longer breastfeeding period, the 18-monthmortality among these children was comparedwith the mortality observed in long-termbreastfed children within an historical cohortfollowed in the same population. No differencesin mortality were observed in the children givenalternative foods over the same period as thosebreastfed, when taking into account HIV status:an overall 18-month probability of survival of96% was observed among HIV-uninfected earlyweaned infants and formula-fed children, whichwas similar to the 95% probability observed inthe long-term breastfed children. Given appro-priate nutritional counselling and care, access toclean water and a supply of breast-milk substi-tutes, replacement feeding could be a safe inter-vention to prevent MTCT of HIV in urbanAfrican settings.
Social acceptability of feeding practicesAs the infant feeding option was allocated atrandom in the Kenyan and the Botswana trials,the social acceptability of the intervention can-not be fully studied. In the Kenya trial, compli-ance for women in the formula-feeding group wasestimated to be 70%, compared to 96% in thebreastfeeding group (Nduati et al. 2000). InMashi, full adherence to formula feeding was self-reported as 93% (Thior et al. 2006). However,three infants of 245 in the formula-fed groupwere infected between four weeks and sevenmonths, presumably because they were exposedto breast milk.
STRATEGIES TO REDUCE HIV TRANSMISSION THROUGH BREASTFEEDING

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
26
The ANRS 1201/1202 Ditrame Plus cohortstudy of women attending community-run healthfacilities was conducted in poor areas in Abidjan,Côte d’Ivoire (Becquet et al. 2005c; Leroy et al.2007). Two nutritional interventions were sys-tematically proposed to the women during ante-natal visits, and the staff was trained to supportindividual women’s choices (Table 4). The firstoption consisted of the complete avoidance ofbreastfeeding: replacement feeding from birth tonine months of age with free provision of infantformula, facilitated by the use of a single oraldose of cabergoline for inhibiting lactation. Thesecond option consisted of practising exclusivebreastfeeding for the first few months with theaim of stopping after a short period (not exceed-ing two weeks) and obtaining complete cessa-tion of breastfeeding by four months of age.Replacement feeding from cessation ofbreastfeeding until nine months of age as well asthe materials needed were provided free of charge,while cup feeding was encouraged from threemonths of age. Overall, 53% of women initiatedformula feeding. Of those, only 15% were non-compliant to this intervention at age one year(i.e. they had breastfed their child at least once),of whom 41% mixed-breastfed temporarily atday two, mainly because of the pressure of theirenvironment or because of low birth-weight(Leroy et al. 2007).
Among the breastfeeding mothers, the prob-ability of practising exclusive breastfeeding frombirth was extremely low: only 10% at threemonths of age (Becquet et al. 2005c). The dura-tion of breastfeeding was considerably reducedin this population: breastfeeding cessation oc-curred at approximately four months of age, af-ter a short (median: nine days) transition periodof mixed feeding when breast milk and infantformula were given simultaneously to the infant.Provided with the necessary support, women’sacceptance of, and compliance with, formulafeeding and early cessation of breastfeeding werehigh. Exclusive breastfeeding was not practiseddespite regular nutritional counselling given dur-ing antenatal and postnatal counselling to pro-mote it. In this setting, formula feeding was more
socially acceptable than breastfeeding. This so-cial acceptability must be balanced with long-term health outcomes of the mother and childin order to guide safe recommendations on in-fant feeding among HIV-infected women in ur-ban African settings.
In contrast, Bland and colleagues (2007)found that exclusive breastfeeding was more so-cially acceptable than replacement feeding in astudy near Durban, South Africa. The purposeof the study was to examine the intentions ofHIV-infected and uninfected women with regardto feeding their infants. This involved assessingthe appropriateness of their choices according totheir local resources, as well as determining themothers’ adherence to those choices during thefirst week postpartum. The intentions of preg-nant women were studied within the context offour resources that facilitate replacement feed-ing: clean water, adequate fuel, access to a re-frigerator and regular maternal income.First-week feeding practices were documented.The antenatal feeding intentions of 1253 HIV-infected women were: exclusive breastfeeding73%; replacement feeding 9%; undecided 18%.Significantly more HIV-infected women intend-ing to exclusively breastfeed adhered to their in-tention in week one (exclusive breastfeeding78%; replacement feeding 42%; p<0.001). Of1238 HIV-negative women, 82% intended toexclusively breastfeed; 2% to replacement feed;and 16% were undecided. Seventy-five per centwho intended to exclusively breastfeed adheredto this intention postnatally, and only 11 infants(<1%) received no breast milk. The number ofantenatal home visits during the study signifi-cantly influenced adherence to feeding intention.The authors concluded that adherence to inten-tion among HIV-infected women was higher inthose who chose to exclusively breastfeed thanto replacement feed, and that with appropriatecounselling and support, spillover of suboptimalfeeding practices to HIV-negative women wasminimal.
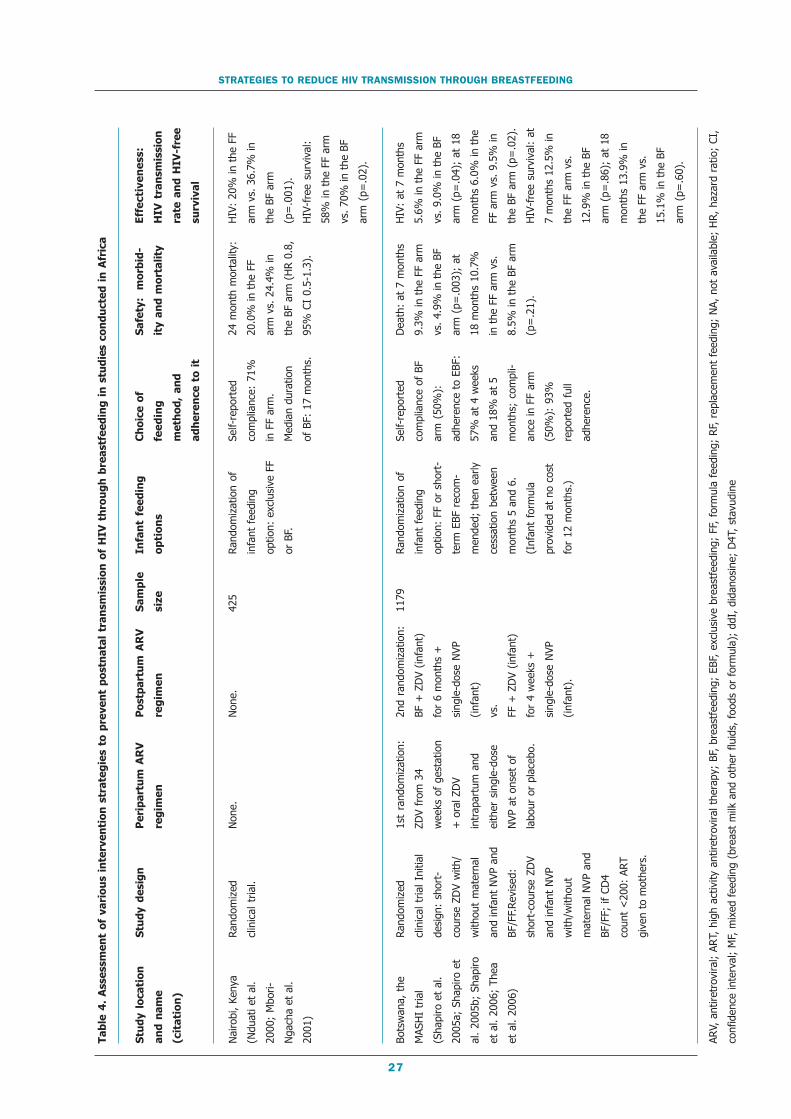
27
STRATEGIES TO REDUCE HIV TRANSMISSION THROUGH BREASTFEEDING
Tab
le 4
. A
sses
smen
t o
f va
rio
us
inte
rven
tio
n s
trat
egie
s to
pre
ven
t p
ost
nat
al t
ran
smis
sio
n o
f H
IV t
hro
ug
h b
reas
tfee
din
g i
n s
tud
ies
con
du
cted
in
Afr
ica
Stu
dy
loca
tio
n
and
nam
e
(cit
ati
on
)
Nai
robi
, Ke
nya
(Ndu
ati e
t al
.
2000
; M
bori-
Nga
cha
et a
l.
2001
)
Bots
wan
a, t
he
MAS
HI
tria
l
(Sha
piro
et
al.
2005
a; S
hapi
ro e
t
al.
2005
b; S
hapi
ro
et a
l. 20
06;
Thea
et a
l. 20
06)
Stu
dy
des
ign
Rand
omiz
ed
clin
ical
tria
l.
Rand
omiz
ed
clin
ical
tria
l Ini
tial
desi
gn:
shor
t-
cour
se Z
DV
with
/
with
out
mat
erna
l
and
infa
nt N
VP a
nd
BF/F
F.Rev
ised
:
shor
t-co
urse
ZD
V
and
infa
nt N
VP
with
/with
out
mat
erna
l NVP
and
BF/F
F; if
CD
4
coun
t <
200:
ART
give
n to
mot
hers
.
Per
ipar
tum
AR
V
reg
imen
Non
e.
1st
rand
omiz
atio
n:
ZDV
from
34
wee
ks o
f ge
stat
ion
+ o
ral Z
DV
intr
apar
tum
and
eith
er s
ingl
e-do
se
NVP
at
onse
t of
labo
ur o
r pl
aceb
o.
Po
stp
artu
m A
RV
reg
imen
Non
e.
2nd
rand
omiz
atio
n:
BF +
ZD
V (in
fant
)
for
6 m
onth
s +
sing
le-d
ose
NVP
(inf
ant)
vs.
FF +
ZD
V (in
fant
)
for
4 w
eeks
+
sing
le-d
ose
NVP
(inf
ant)
.
Sa
mp
le
size
425
1179
Infa
nt
feed
ing
op
tio
ns
Rand
omiz
atio
n of
infa
nt f
eedi
ng
optio
n: e
xclu
sive
FF
or B
F.
Rand
omiz
atio
n of
infa
nt f
eedi
ng
optio
n: F
F or
sho
rt-
term
EBF
rec
om-
men
ded;
the
n ea
rly
cess
atio
n be
twee
n
mon
ths
5 an
d 6.
(Inf
ant
form
ula
prov
ided
at
no c
ost
for
12 m
onth
s.)
Ch
oic
e o
f
fee
din
g
met
ho
d,
and
adh
eren
ce t
o i
t
Self-
repo
rted
com
plia
nce:
71%
in F
F ar
m.
Med
ian
dura
tion
of B
F: 1
7 m
onth
s.
Self-
repo
rted
com
plia
nce
of B
F
arm
(50
%):
adhe
renc
e to
EBF
:
57%
at
4 w
eeks
and
18%
at
5
mon
ths;
com
pli-
ance
in F
F ar
m
(50%
): 9
3%
repo
rted
ful
l
adhe
renc
e.
Saf
ety:
m
orb
id-
ity
and
mo
rtal
ity
24 m
onth
mor
talit
y:
20.0
% in
the
FF
arm
vs.
24.
4% in
the
BF a
rm (
HR
0.8,
95%
CI
0.5-
1.3)
.
Dea
th:
at 7
mon
ths
9.3%
in t
he F
F ar
m
vs. 4
.9%
in t
he B
F
arm
(p=
.003
); a
t
18 m
onth
s 10
.7%
in t
he F
F ar
m v
s.
8.5%
in t
he B
F ar
m
(p=
.21)
.
Eff
ecti
ven
ess:
HIV
tra
nsm
issi
on
rate
an
d H
IV-f
ree
surv
ival
HIV
: 20
% in
the
FF
arm
vs.
36.
7% in
the
BF a
rm
(p=
.001
).
HIV
-fre
e su
rviv
al:
58%
in t
he F
F ar
m
vs. 7
0% in
the
BF
arm
(p=
.02)
.
HIV
: at
7 m
onth
s
5.6%
in t
he F
F ar
m
vs. 9
.0%
in t
he B
F
arm
(p=
.04)
; at
18
mon
ths
6.0%
in t
he
FF a
rm v
s. 9
.5%
in
the
BF a
rm (
p=.0
2).
HIV
-fre
e su
rviv
al:
at
7 m
onth
s 12
.5%
in
the
FF a
rm v
s.
12.9
% in
the
BF
arm
(p=
.86)
; at
18
mon
ths
13.9
% in
the
FF a
rm v
s.
15.1
% in
the
BF
arm
(p=
.60)
.
ARV,
ant
iretr
ovira
l; AR
T, h
igh
activ
ity a
ntire
trov
iral t
hera
py;
BF,
brea
stfe
edin
g; E
BF,
excl
usiv
e br
east
feed
ing;
FF,
for
mul
a fe
edin
g; R
F, r
epla
cem
ent
feed
ing;
NA,
not
ava
ilabl
e; H
R, h
azar
d ra
tio;
CI,
conf
iden
ce in
terv
al;
MF,
mix
ed f
eedi
ng (
brea
st m
ilk a
nd o
ther
flu
ids,
foo
ds o
r fo
rmul
a);
ddI,
did
anos
ine;
D4T
, st
avud
ine

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
28
Stu
dy
loca
tio
n
and
nam
e
(cit
ati
on
)
Abid
jan,
Côt
e
d’Iv
oire
,AN
RS
1201
/120
2
Ditr
ame
Plus
stud
y, (
Becq
uet
et
al.
2005
c; D
abis
et
al.
2005
; Be
cque
t
et a
l. 20
06;
Lero
y
et a
l. 20
08;
Becq
uet
et a
l.
2007
; Le
roy
et a
l.
2007
)
Abid
jan,
Côt
e
d’Iv
oire
, AN
RS
1201
/120
2
Ditr
ame
Plus
stu
dy
(Bec
quet
et
al.
2005
c; D
abis
et
al.
2005
; Be
cque
t et
al.
2006
; Le
roy
et
al.
2008
; Be
cque
t
et a
l. 20
07;
Lero
y
et a
l. 20
07)
Stu
dy
des
ign
Ope
n la
bel c
ohor
t:
ZDV
+ s
ingl
e-do
se
NVP
.
Ope
n la
bel c
ohor
t:
ZDV
+ 3
TC +
sing
le-d
ose
NVP
.
Per
ipar
tum
AR
V
reg
imen
ZDV
from
36
wee
ks o
f ge
sta-
tion;
int
rapa
rtum
oral
ZD
V +
sin
gle-
dose
NVP
at
onse
t
of la
bour
.
ZDV
+ 3
TC f
rom
32 w
eeks
of
gest
atio
n;
intr
apar
tum
ora
l
ZDV
+ 3
TC +
sing
le-d
ose
NVP
at
onse
t of
labo
ur.
Po
stp
artu
m A
RV
reg
imen
Mot
her:
non
e;
infa
nt:
sing
le-d
ose
NVP
, an
d ZD
V fo
r
seve
n da
ys.
Mot
her:
ZD
V +
3TC
for
3 da
ys;
infa
nt:
sing
le-d
ose
NVP
,
and
ZDV
for
seve
n
days
.
Sa
mp
le
size
373
420
Infa
nt
feed
ing
op
tio
ns
Ante
nata
l
choi
ce:
RF o
r
shor
t-te
rm E
BF
then
ces
satio
n
betw
een
mon
ths
4 an
d 5.
(In
fant
form
ula
prov
ided
at
no
cost
for
9
mon
ths.
)
Ante
nata
l
choi
ce:
RF o
r
shor
t-te
rm E
BF
(4 m
onth
s).
Eff
ecti
ven
ess:
HIV
tra
nsm
issi
on
rat
e
and
HIV
-fre
e su
rviv
al
At 6
wee
ks:
6.5%
; at
18
mon
ths:
FF:
9%
; sh
ort-
term
BF:
16%
.
His
toric
al c
ontr
ol g
roup
give
n sh
ort-
cour
se Z
DV
only
, an
d w
ere
brea
stfe
d:
6 w
eeks
: 12
.8%
; 18
mon
ths:
22%
.
18 m
onth
HIV
-fre
e
surv
ival
:
FF :
15.
8%
shor
t-te
rm B
F: 1
8.4%
long
-ter
m B
F: 2
4.5%
At 6
wee
ks:
4.7%
; at
18
mon
ths:
FF:
6%
; sh
ort-
term
BF:
7%
.
His
toric
al c
ontr
ol g
roup
expo
sed
to s
hort
-cou
rse
ZDV
only
, an
d w
ere
brea
stfe
d: 6
wee
ks:
12.8
%;
18 m
onth
s: 2
2%.
18 m
onth
HIV
-fre
e
surv
ival
:
FF :
12.
3%
shor
t-te
rm B
F: 1
0.4%
long
-ter
m B
F: 2
4.5%
Ch
oic
e o
f
fee
din
g
met
ho
d,
and
adh
eren
ce t
o i
t
53%
of
mot
hers
chos
e FF
, of
who
m 1
5%
brea
stfe
d at
leas
t
once
; 47
% c
hose
shor
t-te
rm E
BF.
EBF
at 3
mon
ths:
10%
; m
edia
n
dura
tion:
4
mon
ths.
Com
plet
e
cess
atio
n of
any
BF:
in 4
5% a
nd
63%
of
BF
wom
en]
by 4
and
6 m
onth
s,
resp
ectiv
ely.
Saf
ety:
m
orb
id-
ity
and
mo
rtal
ity
Prob
abili
ty o
f a
seve
re e
vent
(mor
bidi
ty)
in 2
year
s: F
F in
fant
s:
14%
; sh
ort-
term
BF
child
ren:
15%
(adj
uste
d H
R 1.
19,
95%
CI
0.75
-1.9
1,
p=0.
44).
18-m
onth
pro
babi
l-
ity o
f su
rviv
al o
f
96%
for
bot
h FF
and
shor
t-te
rm B
F
infa
nts.
(Si
mila
r to
the
95%
pro
babi
lity
obse
rved
in t
he
long
-ter
m B
F
child
ren
of t
he
hist
oric
al A
NRS
Ditr
ame
tria
l.)

29
STRATEGIES TO REDUCE HIV TRANSMISSION THROUGH BREASTFEEDING
Stu
dy
loca
tio
n
and
nam
e
(cit
ati
on
)
Sout
h Af
rica,
the
Vert
ical
Tra
nsm
is-
sion
Stu
dy
(Coo
vadi
a et
al.
2007
)
Zvita
mbo
, Zi
mba
-
bwe
(Piw
oz e
t al
.
2004
; Ili
ff e
t al
.
2005
; Pi
woz
et
al.
2005
)
Rwan
da a
nd
Uga
nda,
the
SIM
BA
tria
ls
(Vya
nkan
dond
era
et a
l. 20
03)
Stu
dy
des
ign
Ope
n la
bel c
ohor
t.
Ope
n la
bel c
ohor
t.
Rand
omiz
ed c
linic
al
tria
l: N
VP v
s. 3
TC
post
nata
lly in
brea
stfe
edin
g
infa
nts
born
to
wom
en w
ho
rece
ived
ZD
V +
ddI
ante
nata
lly a
nd 7
days
pos
tpar
tum
.
Per
ipar
tum
AR
V
reg
imen
Sing
le-d
ose
NVP
.
Non
e.
ZDV
+ d
dI f
rom
36
wee
ks o
f ge
sta-
tion;
int
rapa
rtum
oral
ZD
V +
ddI
.
Po
stp
artu
m A
RV
reg
imen
Non
e.
Non
e.
ZDV
+ d
dI f
or 7
days
(m
othe
r);
NVP
once
dai
ly f
or 1
4
days
the
n tw
ice
daily
vs.
3TC
tw
ice
daily
whi
le
brea
stfe
edin
g
(inf
ant)
.
Sa
mp
le
size
1372
14 1
10
358
Infa
nt
feed
ing
op
tio
ns
Prom
otio
n of
EBF.
Prom
otio
n of
EBF.
Shor
t-te
rm E
BF.
Eff
ecti
ven
ess:
HIV
tra
nsm
issi
on
rat
e
and
HIV
-fre
e su
rviv
al
Ove
rall
cont
ract
ion
of
HIV
: at
4-8
wee
ks:
15%
;
at 6
mon
ths:
21.
6%.
HIV
-fre
e su
rviv
al:
at 6
mon
ths:
75%
; am
ong
infa
nts
EBF:
at
4-8
wee
ks:
15%
; at
6
mon
ths:
16%
.
(Ear
ly m
ixed
fee
ding
was
a ris
k fa
ctor
.)
Ove
rall
post
nata
l HIV
tran
smis
sion
: at
18
mon
ths:
12.
1%,
68%
occu
rrin
g af
ter
6 m
onth
s.
(Ear
ly m
ixed
fee
ding
was
a ris
k fa
ctor
.)
HIV
-fre
e su
rviv
al:
NA
HIV
infe
ctio
n at
4 w
eeks
:
6.9%
; 7.
8% a
t 6
mon
ths
(diff
eren
ce n
ot s
tatis
ti-
cally
sig
nific
ant)
;
tran
smis
sion
rat
e 2.
4%
betw
een
day
3 an
d 6
mon
ths.
HIV
-fre
e su
rviv
al:
NA
Ch
oic
e o
f
fee
din
g
met
ho
d,
and
adh
eren
ce t
o i
t
82.5
% o
f m
othe
rs
initi
ated
EBF
;
med
ian
dura
tion
of E
BF:
159
days
;
40%
of w
omen
cont
inue
d BF
to 6
mon
ths.
Mot
hers
with
CD
4 co
unt
<20
0 w
ere
mor
e
likel
y to
use
RF.
100%
of
mot
hers
initi
ated
EBF
.
EBF
at 3
mon
ths:
7.6%
.
Med
ian
dura
tion
of B
F: 3
.5 m
onth
s
(inte
rqua
rtile
rang
e 2.
9-5.
1
mon
ths)
.
Saf
ety:
m
orb
id-
ity
and
mo
rtal
ity
RF w
as a
ssoc
iate
d
with
an
incr
ease
d
mor
talit
y co
mpa
red
with
EBF
(15
.12%
vs.
6.13
% a
t 3
mon
ths)
.
NA
NA
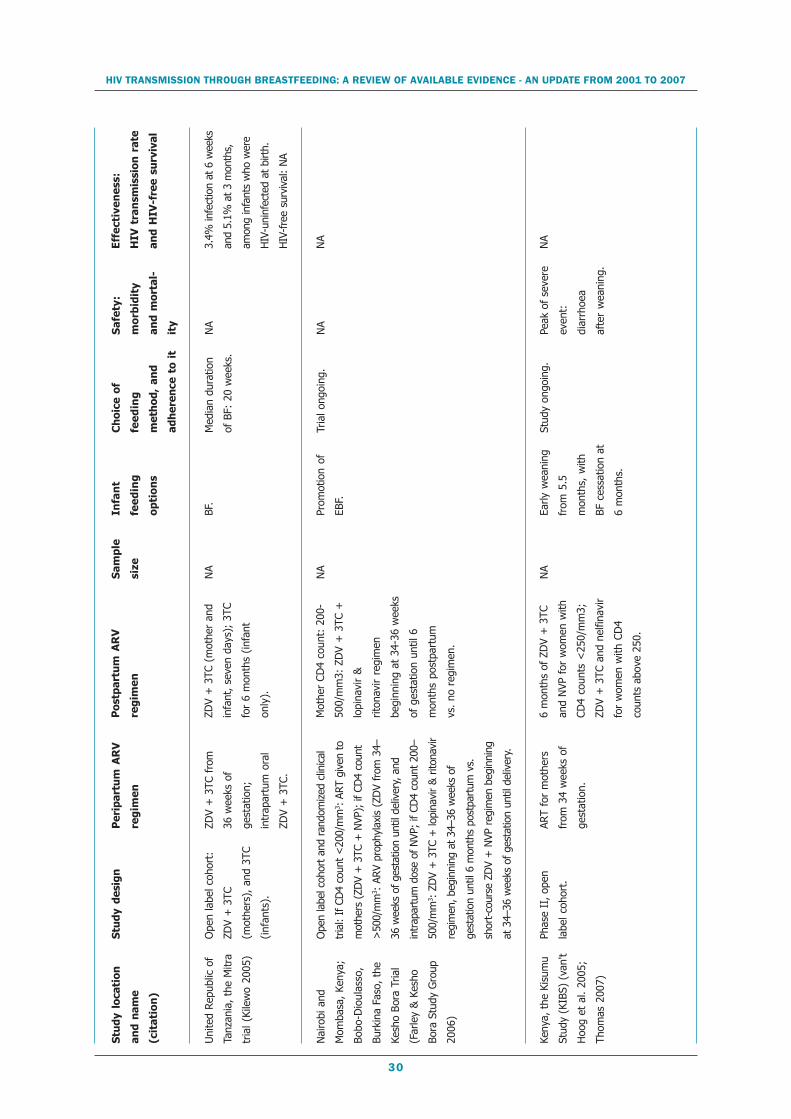
HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
30
Stu
dy
loca
tio
n
and
nam
e
(cit
ati
on
)
Uni
ted
Repu
blic
of
Tanz
ania
, th
e M
itra
tria
l (Ki
lew
o 20
05)
Nai
robi
and
Mom
basa
, Ke
nya;
Bobo
-Dio
ulas
so,
Burk
ina
Faso
, th
e
Kesh
o Bo
ra T
rial
(Far
ley
& K
esho
Bora
Stu
dy G
roup
2006
)
Keny
a, t
he K
isum
u
Stud
y (K
IBS)
(va
n't
Hoo
g et
al.
2005
;
Thom
as 2
007)
Stu
dy
des
ign
Ope
n la
bel c
ohor
t:
ZDV
+ 3
TC
(mot
hers
), a
nd 3
TC
(inf
ants
).
Phas
e II
, ope
n
labe
l coh
ort.
Per
ipar
tum
AR
V
reg
imen
ZDV
+ 3
TC f
rom
36 w
eeks
of
gest
atio
n;
intr
apar
tum
ora
l
ZDV
+ 3
TC.
ART
for
mot
hers
from
34
wee
ks o
f
gest
atio
n.
Po
stp
artu
m A
RV
reg
imen
ZDV
+ 3
TC (
mot
her
and
infa
nt,
seve
n da
ys);
3TC
for
6 m
onth
s (in
fant
only
).
Mot
her
CD4
coun
t: 2
00-
500/
mm
3: Z
DV
+ 3
TC +
lopi
navi
r &
riton
avir
regi
men
begi
nnin
g at
34-
36 w
eeks
of g
esta
tion
until
6
mon
ths
post
part
um
vs.
no r
egim
en.
6 m
onth
s of
ZD
V +
3TC
and
NVP
for
wom
en w
ith
CD4
coun
ts <
250/
mm
3;
ZDV
+ 3
TC a
nd n
elfin
avir
for
wom
en w
ith C
D4
coun
ts a
bove
250
.
Sa
mp
le
size
NA
NA
NA
Infa
nt
fee
din
g
op
tio
ns
BF.
Prom
otio
n of
EBF.
Early
wea
ning
from
5.5
mon
ths,
with
BF c
essa
tion
at
6 m
onth
s.
Eff
ecti
ven
ess:
HIV
tra
nsm
issi
on
rat
e
and
HIV
-fre
e su
rviv
al
3.4%
infe
ctio
n at
6 w
eeks
and
5.1%
at 3
mon
ths,
amon
g in
fant
s w
ho w
ere
HIV
-uni
nfec
ted
at b
irth.
HIV
-fre
e su
rviv
al:
NA
NA
NA
Ch
oic
e o
f
fee
din
g
met
ho
d,
and
adh
eren
ce t
o i
t
Med
ian
dura
tion
of B
F: 2
0 w
eeks
.
Tria
l ong
oing
.
Stud
y on
goin
g.
Sa
fety
:
mo
rbid
ity
and
mo
rtal
-
ity
NA
NA
Peak
of
seve
re
even
t:
diar
rhoe
a
afte
r w
eani
ng.
Ope
n la
bel c
ohor
t an
d ra
ndom
ized
clin
ical
tria
l: If
CD
4 co
unt
<20
0/m
m3 :
ART
giv
en t
o
mot
hers
(ZD
V +
3TC
+ N
VP);
if C
D4
coun
t
>50
0/m
m3 :
ARV
pro
phyl
axis
(ZD
V fr
om 3
4–
36 w
eeks
of g
esta
tion
until
del
iver
y, a
nd
intr
apar
tum
dos
e of
NVP
; if
CD4
coun
t 20
0–
500/
mm
3 : Z
DV
+ 3
TC +
lopi
navi
r &
rito
navi
r
regi
men
, beg
inni
ng a
t 34
–36
wee
ks o
f
gest
atio
n un
til 6
mon
ths
post
part
um v
s.
shor
t-co
urse
ZD
V +
NVP
reg
imen
beg
inni
ng
at 3
4–36
wee
ks o
f ges
tatio
n un
til d
eliv
ery.
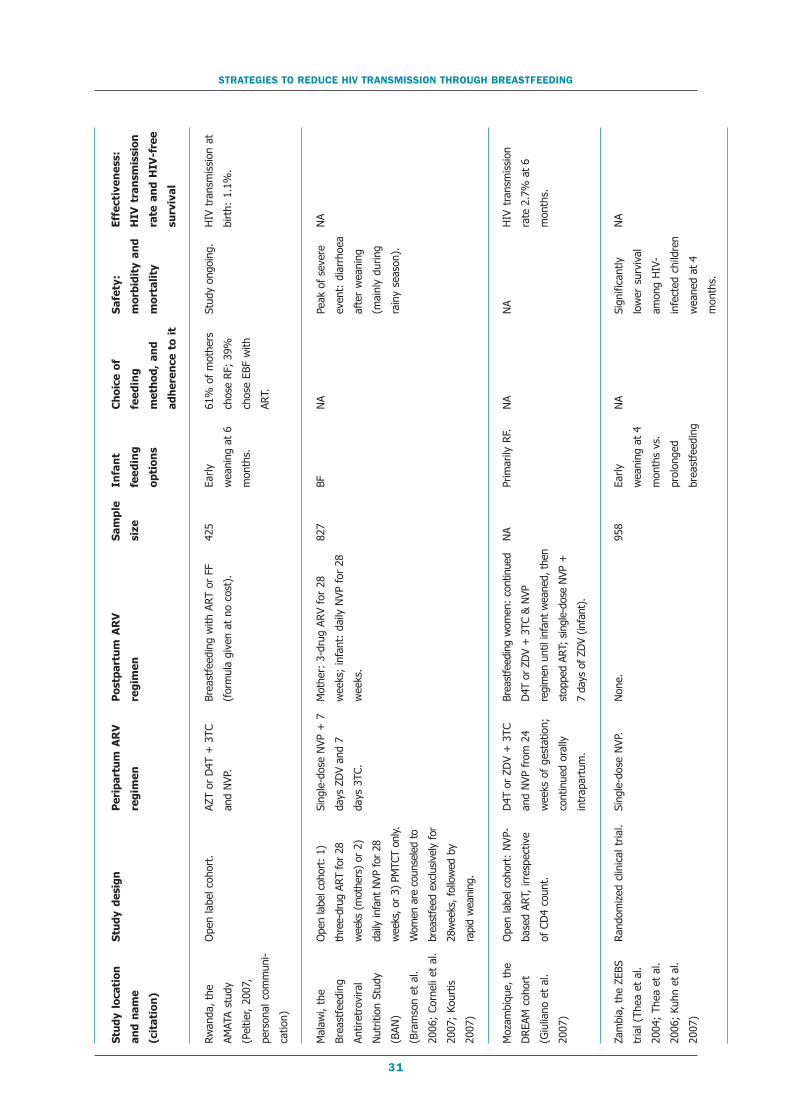
31
STRATEGIES TO REDUCE HIV TRANSMISSION THROUGH BREASTFEEDING
Stu
dy
loca
tio
n
and
nam
e
(cit
ati
on
)
Rwan
da, th
e
AMAT
A st
udy
(Pel
tier,
2007
,
pers
onal
com
mun
i-
catio
n)
Mal
awi,
the
Brea
stfe
edin
g
Antir
etro
vira
l
Nut
ritio
n St
udy
(BAN
)
(Bra
mso
n et
al.
2006
; Co
rnel
i et
al.
2007
; Ko
urtis
2007
)
Moz
ambi
que,
the
DRE
AM c
ohor
t
(Giu
liano
et
al.
2007
)
Zam
bia,
the
ZEB
S
tria
l (Th
ea e
t al
.
2004
; Th
ea e
t al
.
2006
; Ku
hn e
t al
.
2007
)
Stu
dy
des
ign
Ope
n la
bel c
ohor
t.
Ope
n la
bel c
ohor
t: 1
)
thre
e-dr
ug A
RT fo
r 28
wee
ks (
mot
hers
) or
2)
daily
infa
nt N
VP fo
r 28
wee
ks, o
r 3)
PM
TCT
only.
Wom
en a
re c
ouns
eled
to
brea
stfe
ed e
xclu
sive
ly f
or
28w
eeks
, fo
llow
ed b
y
rapi
d w
eani
ng.
Ope
n la
bel c
ohor
t: N
VP-
base
d AR
T, ir
resp
ectiv
e
of C
D4
coun
t.
Rand
omiz
ed c
linic
al t
rial.
Per
ipar
tum
AR
V
reg
imen
AZT
or D
4T +
3TC
and
NVP
.
Sing
le-d
ose
NVP
+ 7
days
ZD
V an
d 7
days
3TC
.
D4T
or
ZDV
+ 3
TC
and
NVP
fro
m 2
4
wee
ks o
f ge
stat
ion;
cont
inue
d or
ally
intr
apar
tum
.
Sing
le-d
ose
NVP
.
Po
stp
artu
m A
RV
reg
imen
Brea
stfe
edin
g w
ith A
RT o
r FF
(for
mul
a gi
ven
at n
o co
st).
Mot
her:
3-d
rug
ARV
for
28
wee
ks;
infa
nt:
daily
NVP
for
28
wee
ks.
Brea
stfe
edin
g w
omen
: co
ntin
ued
D4T
or
ZDV
+ 3
TC &
NVP
regi
men
unt
il in
fant
wea
ned,
the
n
stop
ped
ART;
sin
gle-
dose
NVP
+
7 da
ys o
f ZD
V (in
fant
).
Non
e.
Sa
mp
le
size
425
827
NA
958
Infa
nt
fee
din
g
op
tio
ns
Early
wea
ning
at
6
mon
ths.
BF Prim
arily
RF.
Early
wea
ning
at
4
mon
ths
vs.
prol
onge
d
brea
stfe
edin
g
Eff
ecti
ven
ess:
HIV
tra
nsm
issi
on
rate
an
d H
IV-f
ree
surv
ival
HIV
tra
nsm
issi
on a
t
birt
h: 1
.1%
.
NA
HIV
tra
nsm
issi
on
rate
2.7
% a
t 6
mon
ths.
NA
Ch
oic
e o
f
fee
din
g
met
ho
d,
and
adh
eren
ce t
o i
t
61%
of
mot
hers
chos
e RF
; 39
%
chos
e EB
F w
ith
ART.
NA
NA
NA
Sa
fety
:
mo
rbid
ity
and
mo
rtal
ity
Stud
y on
goin
g.
Peak
of
seve
re
even
t: d
iarr
hoea
afte
r w
eani
ng
(mai
nly
durin
g
rain
y se
ason
).
NA
Sign
ifica
ntly
low
er s
urvi
val
amon
g H
IV-
infe
cted
chi
ldre
n
wea
ned
at 4
mon
ths.

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
32
HIV-infectionThe clinical trial randomized on infant feedingpractices in Kenya showed that the cumulativeprobability of HIV infection at age two years was37% in breastfed children and 21% among theformula-fed arm (p=0.001) (Nduati et al. 2000).In the Mashi trial, HIV infection at age 18months was higher in breastfed children than informula-fed children despite six months of ZDVprophylaxis, 9.5% and 6.0%, respectively(p=0.02) (Thior et al. 2006).
In the ANRS 1201/1202 Ditrame Plus studyin Côte d’Ivoire, the provision of peripartumantiretroviral prophylaxis combined with thepromotion of alternatives to prolongedbreastfeeding considerably reduced MTCT rateswith a long-term benefit sustained until age 18months (Becquet et al. 2007). HIV transmissionrates as low as 6.8% and 5.6% at 18 monthswere found in short-term breastfed and formula-fed children, respectively, whose mothers hadreceived a peripartum short-course regimen ofZDV, in addition to a single-dose of NVP.
In Kampala, Uganda, 306 children were en-rolled in a programme to prevent MTCT provid-ing short-course ZDV prophylaxis andreplacement feeding to mothers (Magoni et al.2005). Transmission rates were 12.0% at monthsix (3.7% in the exclusively formula-fed group,16.0% in the exclusively breastfed group, and20.4% in the mixed-fed group). No significantrisk difference was observed between the exclu-sive breastfed and the mixed-fed groups. How-ever, there are no follow-up data to furthermeasure the long-term outcome of this interven-tion within this context, and there have beensome methodological concerns.
HIV-free survivalHIV-free survival at two years was significantlyhigher in the formula arm compared to thebreastfeeding arm in the Kenya trial and in theANRS 1201/1202 Ditrame Plus study comparedto the ANRS Ditrame historical cohort(Valériane Leroy, personal communication, 25October 2006). In the Mashi trial, transmissionrates were significantly lower among formula-fedchildren, but infant mortality was also higher inthis group compared to breastfed children, re-
sulting in similar HIV-free survival in these twogroups by age 18 months (Thior et al. 2006).
DiscussionAvailable findings in 2006 on replacement feed-ing options show that formula feeding is highlyeffective in reducing postnatal transmission, butits safety depends greatly on the local context inwhich it is implemented. In the Kenya trial andthe ANRS 1201/1202 Ditrame Plus study, re-duction of postnatal transmission outweighed therisks of adverse events. In Mashi, benefits andrisks are balanced between infant feeding optionswith a comparable HIV-free survival at 18months.
In these studies, infant formula was providedat no cost for up to 12 months with demonstra-tion of its safe preparation. The differences be-tween the findings of the Kenya and theBotswana trials have been explained by the factthat the Kenyan women were urban and hadbetter access to clean municipal water and prob-ably a higher socioeconomic status. Other dif-ferences in these contexts could explain thesediscrepancies and need to be further explored:access to, and the content and quality of postna-tal follow-up, including nutritional counselling;and the characteristics of formula delivery. Fi-nally, the fact that in both these trials, the in-fant feeding choice was allocated byrandomization is informative in terms of causal-ity analysis, but this methodological choice raisesother problems that could interfere with infanthealth if women’s choices are not assessed basedon acceptability, feasibility, affordability,sustainability and safety.
An outbreak of diarrhoeal disease in Botswanashowed that replacement feeding is of concernin such instances: a recent study of infant feed-ing practices showed that early weaning was fre-quent even in HIV-negative women and thispractice predisposed children to greater morbid-ity in this outbreak (Creek 2006). Governmentpolicy in Botswana is to provide free formula forthe infants of all HIV-infected women whochoose that option, and about 63% of thesewomen formula feed. During the outbreak, thenumber of reported cases of diarrhoea in chil-dren aged less than five years increased fourfold

33
from between 2004 and 2005 to 2006; anddeaths from diarrhoeal illnesses of those aged lessthan five years increased from 24 and 21 reportedin 2004 and 2005, respectively, to at least 532in 2006. These deaths were associated with di-arrhoea and malnutrition and followed unusu-ally heavy rains, in which 25% of patients’families had overflowing latrines. Among chil-dren hospitalized for diarrhoea, 96% were agedless than two years and 93% were notbreastfeeding. When reviewing the records of 20infants who died after being fed with formula, itwas found that their mothers reported receivingonly 51% of the formula they should have re-ceived before their infant’s illness. In such con-ditions, formula feeding may not save lives.
This highlights the need to ensure that mini-mal conditions are in place for safe replacementfeeding practices: inter alia, access to clean wa-ter; counselling and information on whichwomen can base sound choices during the ante-natal period; regular postnatal follow-up (withrepeated growth measurements) and nutritionalcounselling; an uninterrupted supply of formula(whether formula is given at no cost or subsi-dized) as well as the materials to dispense it.Thus, programmes that provide infant formulaon a large scale need to review management dif-ficulties. Further, health staff should be taughtthat formula-fed infants are at high risk of mor-bidity. They should be shown the clinical signsof diseases and how to intervene in such cases toaid the child. Formula feeding should be proposedonly alongside regular postnatal follow-up toadapt the formula to the nutritional requirementsof the growing child. In settings where infantformula is used widely by HIV-negative women,the promotion of breastfeeding needs strength-ening in the general population.
These restrictive and selective conditions serveto remind that formula feeding could be an op-tion to replace breastfeeding but is far from be-ing applicable in all settings; thus, the need formore studies on alternative strategies forbreastfeeding (e.g. antiretroviral prophylaxis).
Strategies for HIV-infected women whobreastfeedSeveral options could be considered to reducepostnatal transmission in breastfeedingpopulations. A potential intervention would bethe promotion of exclusive breastfeeding duringthe first six months of life. Another alternativeto prolonged breastfeeding consists of shorten-ing the duration of breastfeeding. These two in-terventions can be combined and constitute analternative to prolonged breastfeeding: exclusivebreastfeeding with early cessation, which is ex-pected to reduce the cumulative risk of postna-tal transmission of HIV while retaining thebenefits of exclusive breastfeeding during the firstmonths of life.
Exclusive breastfeedingImproving breastfeeding practices by promotingexclusive breastfeeding and breastfeeding cessa-tion as soon as it is acceptable, feasible, afford-able, sustainable and safe, in conjunction withlactation management to reduce (sub)clinicalmastitis could be effective in reducing postnataltransmission of HIV (Piwoz et al. 2005).
Several studies are completed or currentlyongoing in Africa (Côte d’Ivoire, South Africa,Zambia and Zimbabwe) to evaluate the feasibil-ity and acceptability of exclusive breastfeedingfor up to six months in HIV-infected women,and its efficacy to decrease postnatal transmis-sion of HIV though breastfeeding. There is con-sistent evidence from four different studiesshowing a lower postnatal risk in exclusively-breastfed children and those predominantlybreastfed, compared to those who were mixedfed (Tables 2 and 4).
In Zimbabwe, the Zvitambo trial assessed theeffect of postpartum vitamin A supplementation,and provided education and counselling aboutinfant feeding practices and HIV (Iliff et al.2005). Information on infant feeding practicesand associated infant infections and deaths wereprospectively collected. A total of 14 110mother-newborn pairs were enrolled, randomlyassigned to a vitamin A-treatment group afterdelivery, and followed for two years. At baseline,six weeks and three months, mothers were asked
STRATEGIES TO REDUCE HIV TRANSMISSION THROUGH BREASTFEEDING

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
34
whether they were still breastfeeding, andwhether any of 22 liquids or foods offered in thestudy had been given to the infant. Breastfedinfants were classified as exclusively or predomi-nantly breastfed, or mixed fed. However, onelapse in the exclusivity of breastfeeding at oneof the three time points was allowed if the non-breast-milk item consumed was not a milk-basedliquid (e.g. fruit juice). One lapse in predomi-nant breastfeeding was allowed only if themother reported exclusive breastfeeding for thetime period. A total of 4495 mothers tested HIV-positive at baseline, and 2060 HIV-exposed in-fants tested negative through polymerase chainreaction (PCR) at age six weeks. All infants ini-tiated breastfeeding: 156 were exclusivelybreastfed, 490 predominantly breastfed and1414 received mixed feeding. Overall postnataltransmission (defined by a positive HIV test af-ter a negative test at six weeks) was 12.1%, with68.2% of these transmissions occurring after sixmonths of age. Compared with exclusivebreastfeeding, early mixed feeding was associatedwith a 4.03 (95% CI 0.98–16.61), 3.79 (95%CI 1.40–10.29) and 2.60 (95% CI 1.21–5.55)greater risk of postnatal transmission at six, 12and 18 months, respectively. Predominantbreastfeeding was associated with a 2.63 (95%CI 0.59–11.67), 2.69 (95% CI 0.95–7.63) and1.61 (95% CI 0.72–3.64) trend towards greaterpostnatal transmission risk at six, 12, and 18months, respectively, compared with exclusivebreastfeeding.
In the Vertical Transmission Study, high ratesof exclusive breastfeeding were obtained in ruralSouth Africa (Bland et al. 2006). Women will-ing to practise exclusive breastfeeding were sup-ported at home by people trained in breastfeedingcounselling, but with no previous health back-ground. In this context, the median duration ofexclusive breastfeeding from birth was fivemonths, which is elevated in the African con-text, and adherence to exclusive breastfeedingwas higher than for formula feeding (Bland etal. 2007). Replacement feeding was practised by8% of the Vertical Transmission Study cohortand was associated with increased mortality com-pared with exclusive breastfeeding (15.12% ver-sus 6.13% at three months). The risk of postnatal
transmission by age six months in exclusivelybreastfed infants who were HIV-negative at fourto eight weeks of age was about 4% (Coovadiaet al. 2007). This risk was about 11 times higherwith the introduction of solids and two timeshigher with mixed feeding. Similarly, in theANRS 1201/1202 Ditrame Plus cohort, a trendfor a higher postnatal risk in mixed-fed childrencompared to exclusively breastfed infants wasreported (Leroy et al. 2004).
These data support the recommendation,originally based on other considerations, thatmixed feeding should be avoided to decrease therisk of HIV transmission. They also show thatexclusive breastfeeding is possible and acceptableamong both HIV-infected and uninfectedwomen. However, frequent, good-quality coun-selling and support is necessary to achieve highrates of exclusive breastfeeding. Among womenwho decide to breastfeed, exclusive breastfeedingshould be promoted until six months of age.
Early cessation of breastfeedingFollowing the period of exclusive breastfeeding,it has been suggested that HIV-infected womenshould cease breastfeeding completely. Early ces-sation could substantially prevent breastfeeding-associated HIV transmission, while still providingthe many benefits of breastfeeding in terms ofmorbidity and mortality prevention during theearly months of an infant’s life. However, thereis little experience on how this early cessationcan be achieved with a minimum of adverse ef-fects for the infant. There is also no evidence yetto inform the timing of this cessation. Never-theless it would be appropriate for many womento do this as soon as replacement feeding be-comes acceptable, feasible, affordable, sustain-able and safe, or at six months of age, whenexclusive breastfeeding is no longer adequate tomeet an infant’s nutritional needs. As statedabove, continued support is needed beyond thefirst six months to ensure adequate nutrition forthe young child throughout the first years of life.
A clinical trial was conducted in Zambia totest the safety and efficacy of exclusivebreastfeeding to four months of age to reduceHIV transmission and child mortality (the ZEBStrial): half of the women were randomly selected

35
to cease breastfeeding at age four months (Theaet al. 2004), although many women found it dif-ficult to stop and continued for longer. This studywas expected to assess the magnitude of reduc-tion of postnatal transmission associated withearly cessation at four months compared to pro-longed breastfeeding. Early results showed thatbreast-milk viral load increased after early wean-ing in this trial. Breast milk was obtained at 22weeks from 222 women who had either stoppedor continued to breastfeed past four months.Breast-milk viral load was measured at 20 and22 weeks in 71 randomly selected women fromboth groups: breast-milk viral load was detect-able in 68% of those who stopped breastfeedingat four months vs. 42% of those who continuedbeyond, p=0.03); median breast-milk viral load(448 copies versus <50 copies HIV-RNA/ml,p=0.005) was significantly higher among thosewho had stopped in comparison with those whowere still breastfeeding and was significantlyhigher in the same women after stopping com-pared with two weeks earlier (p=0.001). It isunclear whether this increase was temporary.Breast-milk viral load is substantially higher af-ter rapid cessation, and this may pose an in-creased risk of HIV transmission if childrenresume breastfeeding after a period of cessation.Increases in breast-milk viral load with differingdegrees of mixed feeding needs to be assessed(Thea et al. 2006), together with the long-termefficacy of such an intervention.
To be assessed fully, the benefits of early ces-sation in terms of reduction of postnatal HIVtransmission have to be balanced with their po-tential risks for infant health. Complementaryfeeding practices are often inadequate in devel-oping countries, resulting in a significant nutri-tional decline between six and 18 months of age(Bhandari et al. 2004). One of the potential ad-verse effects is that if complementary foods wereto displace breast milk it would not be nutri-tionally appropriate. International guidelinesstress that from six months breastfeeding shouldbe coupled with the introduction of nutrition-ally adequate and safe complementary foods(WHO 1998; WHO 2001). Early cessation ofbreastfeeding may induce undernutrition if an-other milk source is not available, which in turn
could enhance morbidity compared to those chil-dren who are breastfed for a longer period.
Indeed, early cessation of breastfeeding beforesix months was associated with an increased riskof infant morbidity (especially diarrhoea) andmortality in HIV-exposed children in preliminaryresults from three studies in Kenya, Malawi andUganda. These studies included the phase IIIinfant prophylaxis Post-Exposure Prophylaxis forInfant (PEPI) trial in Blantyre, Malawi(Kafulafula 2007); the Kisumu Kenya KIBSstudy (van’t Hoog et al. 2005) in which mothersreceived ART in the last month of pregnancy andfor six months postpartum; and the HIVIGLOBtrial in Kampala, Uganda, a phase II/III study,which compared either an infusion of HIVhyperimmune globulin (HIVIGLOB) to themother and newborn or six weeks of NVP dailyto the infant compared to the HIVNET 012 sin-gle-dose NVP regimen1 (Onyango 2007). In theKenya and Malawi studies there was a signifi-cantly increased risk of diarrhoea-relatedhospitalizations for the infants whose mothersstopped breastfeeding by six months comparedto historical data where mothers breastfed intothe second year of life (Kafulafula 2007; Tho-mas 2007). In addition, in the Malawi PEPIstudy there was a significantly increased risk ofboth overall and diarrhoea-related mortality com-pared to historical data. In the HIVIGLOB study,among 579 uninfected infants there was a dou-bling of gastroenteritis hospitalizations in thethree months following cessation of breastfeedingwhen compared to the three months beforebreastfeeding stopped; and of the 15 infantdeaths that occurred among uninfected infants,all occurred after cessation of breastfeeding(Onyango 2007). Early breastfeeding cessationat four months was associated with reduced HIVtransmission but also with increased child mor-tality from four to 24 months in preliminary datapresented from the randomized ZEBS trial inZambia. Consequently, in this trial, early cessa-tion of breastfeeding did not improve HIV-freesurvival (Kuhn et al. 2007).
STRATEGIES TO REDUCE HIV TRANSMISSION THROUGH BREASTFEEDING
1 One dose of NVP given to the mother at the onset oflabour and one dose of NVP given to the neonate <72hours postpartum.

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
36
The nutritional adequacy of complementaryfeeding was recently assessed in Côte d’Ivoireamong breastfed children exposed tobreastfeeding for a median of four months(Becquet et al. 2006). After early cessation,breastfeeding was replaced by food which metnutritional requirements in terms of source ofmilk (e.g. infant formula, baby food), but thediversity of diet was not appropriate for the nu-tritional needs of babies aged six months (e.g.lacking sufficient protein). Inadequate comple-mentary feeding at age six months was associ-ated with impaired growth during at least thenext 12 months. However, in this cohort study,where regular nutritional counselling was pro-vided, the nutritional adequacy of complemen-tary feeding was then improved to cover thenutritional needs of most of the children at agesnine and 12 months. As a result, two-year mor-bidity was not different in short-term breastfedinfants compared to long-term breastfed children(Becquet et al. 2007).
More research is needed in this area to pro-vide practical tools that can be used routinely,especially around the period of cessation, to con-tribute to the assessment of the nutritional ad-equacy of complementary feeding. Such toolscould help detect children who are at risk formalnutrition and whose mothers need to receiveappropriate and reinforced nutritional counsel-ling.
In Burkina Faso, an ongoing study is assess-ing a locally-produced fortified flour formulationdesigned to meet nutrient and energy needs ofinfants among women practising earlybreastfeeding cessation in the Kesho Bora study(Cames et al. 2006). It is provided free of cost,while mothers have to pay for cow milk. Thefirst results suggest high acceptability amongmothers who choose either breastfeeding withearly cessation or replacement feeding. The studyon mothers’ perceptions of the product, and theinfants’ food consumption, growth and morbid-ity is ongoing.
In addition, a randomized clinical trial in In-dia showed that improving complementary feed-ing practices through an educational programmeis feasible, but the effect on physical growth islimited (Bhandari et al. 2004). Factors that limit
physical growth must be better understood toplan more effective nutrition programmes.
Heat treatment or pasteurization of expressedbreast milkHeat-treated expressed breast milk is a methodendorsed by WHO to reduce postnatal transmis-sion of HIV. Initial results show that methodssuch as Pretoria Pasteurization or Flash HeatTreatment can effectively inactivate the virus inbreast milk from HIV-infected mothers (Jeffery& Mercer 2000; Israel-Ballard et al. 2006b; Is-rael-Ballard et al. 2007). These methods can alsoeliminate potential contaminants and adequatelyinhibit bacterial growth while retaining nutrientscontained in breast milk (Jeffery et al. 2003; Is-rael-Ballard et al. 2006a). It was recently re-ported that heat-treated human milk may be afeasible infant-feeding option for HIV-positivemothers in Zimbabwe. Yet, its field feasibilitynow needs to be assessed among HIV-infectedwomen (Israel-Ballard et al. 2006b). It could beuseful after a period of exclusive breastfeedingin children older than six months. Expressedheat-treated breast milk may also have a valu-able role as an alternative to breastfeeding dur-ing periods of increased risk, such as mastitis andcracked or bleeding nipples. Pasteurization ofbreast milk seems difficult to implement on alarge scale, however, and shares some of the sameobstacles as replacement feeding – it requiresmothers have access to a developed infrastruc-ture and safe practices (such as sterilization ofmaterials used in the process), which can be dif-ficult to achieve in resource-poor settings.
Microbicide treatment of expressed breast milkMicrobicides to treat HIV-infected breast milkcould present an alternative to reduce transmis-sion of HIV through breast milk (Urdaneta etal. 2005). It has been reported that alkyl sulfates(i.e. sodium dodecyl sulfate, SDS) are microbi-cidal against HIV at low concentrations, are bio-degradable, have little or no toxicity and areinexpensive. Therefore, they may be used fortreatment of HIV-infected breast milk. Humanmilk was infected artificially by adding HIV (cell-free or cell-associated); it was then treated withan SDS dilution d”1% at 37 degrees Celsius or

37
room temperature for 10 minutes. SDS was viru-cidal against cell-free and cell-associated HIV inbreast milk. Viral load in artificially-infected milkwas reduced to undetectable levels after treat-ment with 0.1% SDS. SDS could be removedfrom breast milk if necessary, and milk was notinfectious after SDS removal. The proposed treat-ment concentrations are within reported safe lim-its for ingestion of SDS by children of 1 g perkg/day. This treatment could be helpful to pro-tect infants from postnatal transmission after sixmonths, where heat treatment is not feasible.The feasibility, acceptability and safety of SDShave not yet been studied.
Antiretroviral therapy during breastfeedingIn addition to replacement feeding, possibilitiesfor preventing HIV from being transmittedthrough breast milk include ART duringbreastfeeding (whether or not necessary for themother’s health) and post-exposure prophylaxisto the infant. Antiretroviral regimens were re-cently designed to provide either maternal treat-ment, reducing the maternal viral load, orpost-exposure prophylaxis to the infant duringthe period of breastfeeding, thus maximally re-ducing the risk of MTCT in settings wherebreastfeeding is common (Gaillard et al. 2004).
Maternal antiretroviral prophylaxisPreliminary data are available from a trial con-ducted in Rwanda and Uganda evaluating post-exposure antiretroviral prophylaxis in childrenduring the breastfeeding period, combined withthe promotion of early cessation of breastfeeding(Vyankandondera et al. 2003). The trialrandomized newborns in Rwanda and Ugandato receive either 3TC or NVP from birth untilone month after their mothers stoppedbreastfeeding. The duration of breastfeeding wasaround three months and the overall six-monthtransmission rate was estimated to be 7.8% anddid not differ between these two groups. Long-term outcome estimates are still awaited to fullyunderstand the effect of this intervention.
In the Mashi trial in Botswana, it was reportedthat antiretrovirals given to breastfeeding moth-ers (NVP, 3TC and ZDV) were measured inbreast milk in concentrations inhibiting HIV.
With regard to NVP this exposed infants to thepotential for beneficial and adverse effects (e.g.hepatotoxicity) of the drug (Shapiro et al.2005a). These antiretrovirals suppressed cell-freeHIV RNA in breast milk but had no apparenteffect on cell-associated HIV DNA loads in breastmilk (Shapiro et al. 2005b). These facts high-light the need for further research on this issueto fully assess the public health effectiveness andsafety of antiretroviral treatment.
Maternal antiretroviral treatment duringbreastfeedingART for pregnant or lactating women is of indis-putable benefit when the mother has a CD4 cellcount £200/mm3 or HIV-related symptoms.HIV-infected women who require antiretroviraltherapy for their own health and arebreastfeeding should continue to receive it, asthe benefit to the health of the woman outweighspotential risks to the infant, with a beneficialexpected outcome for infant health (Newell etal. 2004; WHO 2006).
ART to lactating women is expected to sub-stantially reduce the overall risk of transmissionto infants by lowering viral load in plasma andbreast milk. Whether it will prevent all, most orpart of postnatal transmission whenbreastfeeding exposure cannot be avoided mustbe established: will breast-milk HIV viral loadbe lowered as it is lowered in the blood compart-ment? Not only is it crucial to assess the effectof these highly-active antiretroviral regimens onbreast-milk HIV viral load, but also on antiviraldrug diffusion and pharmacokinetics in bothbreast milk and in breastfed infants, as well ason transmission of resistant mutations of thevirus. Additional evidence is needed on the safetyof antiretroviral prophylaxis given to women orthe infant for preventing HIV transmission dur-ing breastfeeding.
The optimal duration of antiretroviral prophy-laxis is unknown, and there are concerns thatviral rebound following cessation of prophylaxismay lead to a high risk of MTCT among infantswho continue to breastfeed after prophylaxis hasstopped; it may also be detrimental to themother. There are limited data about the levelof penetration of antiretroviral therapies into
STRATEGIES TO REDUCE HIV TRANSMISSION THROUGH BREASTFEEDING

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
38
breast milk; some drugs may have high levels ofpenetration while others may have low orundetectable levels in breast milk. Therefore thedetrimental effects on mother and child cannotbe established, and the link between drug pen-etration into breast milk and risk of HIV trans-mission through breastfeeding has not yet beenestablished. Data from a study in Botswana in-dicated that levels of NVP in breast milk ofwomen receiving NVP-based antiretroviraltherapy were lower than their plasma, while lev-els of 3TC and AZT in breast milk were aboutthreefold higher (Shapiro et al. 2005a). Moreresearch is needed, and is indeed ongoing to ad-dress these important issues and to guide thedefinition of comprehensive strategies for boththe care of women and prevention of MTCT,which are safe and adapted to different contexts.
When a pregnant and/or lactating woman isnot eligible for ART, the benefit in terms ofprophylaxis for postnatal transmission has stillto be demonstrated and balanced against the riskof maternal intolerance and/or emergence ofantiretroviral drug resistance and safety for thebaby. It is hypothesized that antiretroviral drugsgiven to breastfeeding women will reduce the riskof postnatal transmission of HIV. Several ongo-ing studies are evaluating the effect of single orcombination antiretroviral regimens given tobreastfeeding women and/or the infant to pre-vent early and/or late postnatal transmissionduring breastfeeding. The WHO-coordinatedKesho Bora study randomized control trial com-pared women with CD4 cell counts between200–500/mm3 given a short-course ZDV/NVPregimen beginning at 34–36 weeks versus ART(regimen of ZDV and 3TC + lopinavir/ritonavirbeginning at 34–36 weeks) during six months ofbreastfeeding (Farley & Kesho Bora Study Group2006).
The Breastfeeding Antiretroviral Nutrition(BAN) study is a prospective randomized con-trolled clinical trial of antiretroviral and nutri-tional interventions conducted in the postpartumperiod in Malawi (Bramson et al. 2006). At birth,mother-infant pairs with mothers whose CD4cell counts were greater than 200 per ml receivedsingle-dose NVP and seven days ZDV and 3TCto prevent perinatal PMTCT. Further, study par-
ticipants received either: 1) three-drugantiretroviral therapy for 28 weeks (mothers),or daily NVP for 28 weeks (infants), or 3) noth-ing more than the initial drugs to prevent peri-natal PMTCT. Women were counseled tobreastfeed exclusively for 28 weeks, followed byrapid weaning.
In the ongoing Kisumu Kenya KIBS phase IIstudy, mothers are receiving ART in the lastmonth of pregnancy and for six months postpar-tum. The DREAM study in Mozambique is alsoconsidering this.
Infant prophylaxis during breastfeedingPost-exposure prophylaxis (PEP) to the infant isan attractive intervention in breastfeedingwomen which deserves attention. It has beenshown to prevent HIV infection after occupa-tional exposure of health-care workers (Panlilioet al. 2005). The use of NVP perinatally, amount-ing to ‘peri-exposure’ prophylaxis, approachespost-exposure prophylaxis. Post-exposureprophylaxis can offer protection against HIVinfection to babies of women who missed oppor-tunities to be tested and counselled before orduring pregnancy. Recent studies in Malawi (Tahaet al. 2003) showed that neonatal prophylaxiswith short-course NVP and/or ZDV reduced peri-natal transmission of HIV even when mothersreached the health centre after delivery. TheSIMBA trial (Vyankandondera et al. 2003)tested two peri-exposure prophylaxis regimens(with no control arm) associated with a short-ened duration of breastfeeding (three months).Several studies are planned or ongoing in Brazil,Ethiopia, India, South Africa and Uganda aimedat comparing single-dose NVP versus six weeksNVP as peri-exposure prophylaxis. Extendingthis perinatal PEP for the entire duration ofbreastfeeding thus seems to be an attractive op-tion but its efficacy needs to be assessed. PEPhas several advantages over ART. First,antiretroviral drug prophylaxis in an uninfectedchild carries no risk that the virus will developresistance to antiretroviral drugs (although itwould if the infant became infected); second, itspares the mother from treatment when she doesnot need it for herself, avoiding the frequent side-effects such treatment entails; third, it may be

39
applicable in a great deal more settings; and fi-nally, it is cheaper.Immunization of breastfed newbornsAn infant vaccine regimen, begun at birth, wouldbe an attractive strategy and might also providethe basis for lifetime protection. Unique featuresof MTCT and HIV-positive children could behelpful in understanding correlates of immuneprotection and could facilitate rapid assessmentof vaccine efficacy (Luzuriaga et al. 2006). Astudy on acceptability of paediatric vaccine wasperformed in Kenya, which reported that con-cerns about side-effects of such interventions arepresent in the population (Farquhar et al. 2006).Research on this issue is ongoing and urgentlyneeded. The HIVIGLOB trial in Kampala,Uganda is a phase II/III study comparing eitheran infusion of HIVIGLOB to the mother andnewborn or six weeks of NVP daily to the infantcompared to the HIVNET 012 single-dose NVPregimen.
Translating research to public healthrecommendations on infant feedingA key issue concerns the translation of researchfindings into practical recommendations: thesedepend on several criteria (acceptable, feasible,affordable, sustainable and safe) that need to becarefully defined according to the context beforeconsidering interventions to prevent postnataltransmission. The consideration of these crite-ria needs to be adapted to each individual con-text. Bland and colleagues (2007) explored therelationship of some of these criteria in provi-sion of feeding options, and adherence by moth-ers to that choice.
To help HIV-positive mothers make the bestchoice, they should receive appropriate counsel-ling that includes information about both therisks and benefits of various infant feeding op-tions based on local assessments, and guidancein selecting the most suitable option for theirown situation. Individual women’s choice aboutinfant feeding options is highly influenced bysociodemographic factors, including both part-ner or family environment and access to cleanwater (Becquet et al. 2005c; Leroy et al. 2007).Counselling and information during the antena-
tal period are important determinants in mater-nal choices, and mothers’ adherence to thosechoices; further, improved education will helpthem avoid risky practices of mixed feeding dueto social pressure. There is a need to train health-care professionals on how to conduct timelycounselling without any coercion (Becquet et al.2005b), and how to include antenatal home vis-its (Bland et al. 2007).
Mother and child pairs should also have ac-cess to follow-up care and support, including fam-ily planning and nutritional support WHO2006). The longer-term health needs of bothHIV-infected and uninfected children and theirmothers, the mortality of children living in fami-lies with HIV, and the plight of increasing num-bers of orphans should not be underestimated.These issues deserve further research and imple-mentation of effective interventions, includingmonitoring and evaluation for better understand-ing the impact of those interventions (UNAIDS2006).
National health services should make specialefforts to support primary prevention for HIVseronegative women in the antenatal andbreastfeeding periods. In situations where moth-ers are being screened and identified as HIV-in-fected, provision will need to be made for theirsubsequent care and for that of their infectedand uninfected children. Counselling on infantfeeding for women known to be HIV-infectedneeds to be appropriate to their situations. Policy-makers should also consider the effect such coun-selling will have on uninfected women and thoseof unknown HIV status in the same setting; allthese women should continue to be advised andsupported to exclusively breastfeed for the firstsix months (WHO 2001; WHO 2006).
Early cessation of breastfeeding among HIV-negative women in some settings seems common,and in these settings breastfeeding promotionneeds strengthening. The Vertical TransmissionStudy conducted in South Africa recently showedit is possible for lay counsellors, with no healthbackground, to help both HIV-infected anduninfected women make appropriate infant feed-ing choices based on their socioeconomic condi-tions (Bland et al. 2006). The counsellingapproach used was based on the set of tools de-
STRATEGIES TO REDUCE HIV TRANSMISSION THROUGH BREASTFEEDING

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
40
veloped by WHO and was effective, in mostcases, in matching the intention of HIV-infectedwomen with their resources: access to water, re-frigerator, fuel and regular income. Another is-sue concerns the effect of providing formula atno cost to HIV-infected women in areas of highHIV prevalence. This South African studyshowed that the ‘spillover’ of suboptimal feed-ing practices to HIV-negative women is minimalif investment is made in provision of high-qual-
ity counselling. In clinics offering HIV testingand counselling to pregnant women (and whereformula was furnished to HIV-infected women)most HIV-negative women opted for breastfee-ding and <1% of infants born to HIV-uninfectedwomen received no breast milk at all in their firstweek of life. It is therefore possible to put in prac-tice international guidelines on infant feeding ifinvestment is made in the training of lay coun-sellors involved in infant feeding counselling.

41
Ongoing or planned researchaddressing the breastfeeding period
In 2007 there were new key research prioritieson HIV and infant feeding. They are listed
below.
Factors affecting HIV transmission throughbreast milkThese include: protective and risk factors, in boththe absence and presence of antiretroviral drugs;factors affecting early and late transmission; vi-ral factors affecting transmission includingsubtypes; proportion of transmission occurringvia cell-free versus cell-associated virus; evalua-tion of immunologic quality of breast milk ofinfected women at different disease stages andCD4 cell counts, such as antibody contentagainst common pathogens; quantification of riskof MTCT during the transition period frombreastfeeding to replacement feeding; evaluationof the risk of postnatal MTCT in women whoseroconvert during lactation.
Early cessation of breastfeedingResearch is ongoing to: determine the conse-quences of cessation of breastfeeding the infantbefore six months of age in terms of morbidityand mortality; define the optimal time and du-ration of the transition period from breast milkto replacement formula, as well as the optimallength of breastfeeding; and determine effectiveinterventions to optimize nutrition followingbreastfeeding cessation.
Transition from exclusive breastfeeding tomixed feedingThese issues include: assessing the risks ofbreastfeeding cessation after six months includ-ing postnatal MTCT of HIV, and infant morbid-ity/mortality during the transition from exclusivebreastfeeding to breastfeeding with complemen-tary foods; determining the optimal time to ceasebreastfeeding for HIV-exposed uninfected in-fants; and the feasibility and effectiveness of dif-
ferent interventions to optimize nutrition, de-velopment and survival among older infants.
Antiretroviral therapiesResearch includes: determining the effects of dif-ferent antiretroviral treatments on timing of HIVtransmission among breastfeeding women; iden-tifying the ways in which antiretroviral drugsaffect the risk factors for HIV transmissionthrough breast milk; determining levels ofantiretroviral drugs in breast milk and in thebreastfeeding infant; ensuring infant safetythrough the course of their exposure toantiretroviral drugs in breast milk; determiningthe efficacy of antiretroviral therapies in reduc-ing postnatal MTCT, and the effects they haveon cell-free and cell-associated viral load; identi-fying the mechanisms through which HIV de-velops resistance to antiretroviral treatments inbreast-milk; and finally, determining howantiretroviral resistance develops amongbreastfeeding infants who become infected post-natally.
Efficacy and safety for mothers and infantsResearch is ongoing to: ascertain the efficacy andsafety of antiretroviral prophylaxis for mothersand infants during breastfeeding (currently be-ing evaluated in clinical trials); define the effi-cacy and optimal regimen and duration ofantiretroviral prophylaxis for mothers and infantsduring the postnatal period; and to determinethe safety of ceasing antiretroviral treatments forthe mother, when they are being used solely forprophylaxis.
Role of passive and active immunizationstrategiesThis includes: researching the potential role ofpassive and active immunization strategies forHIV prevention; assessing the safety andimmunogenicity of HIV vaccine candidates (in-

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
42
fants exposed to HIV, both those that remainuninfected and those who become infected de-spite prophylaxis); and determining the efficacyand safety of passive, active or passive/activeimmunization for prevention of postnatal MTCT.
Alternatives to replacement feedingAlternatives to replacement feeding include strat-egies to reduce infectivity of breast milk by useof heat treatment, microbicides, etc. Further ef-forts are required to: study the effects of suchinterventions on cell-free and cell-associated vi-rus and milk components; determine the safety,feasibility, and effectiveness of such interventionswhen used for prevention of postnatal MTCT,
or when used temporarily during the transitionperiod to mixed feeding or during periods ofbreast pathology, such as mastitis.
Social factorsMore research is required on: counselling, pro-gramme implementation and monitoring of in-fant feeding practices; the social factorsinfluencing maternal decision-making with re-gard to infant feeding practices, including part-ner involvement; the optimal level of counselling,training, and the assessment of the quality ofthat counselling; the efficacy of community-based interventions.

43
Conclusion
The most appropriate infant feeding optionfor an HIV-infected mother depends on her
individual circumstances, including her healthstatus and the local situation, and should alsoconsider the health services available and thecounselling and support she is likely to receive.Exclusive breastfeeding is recommended for HIV-infected women for the first six months of lifeunless replacement feeding meets five criteria -that it is acceptable, feasible, affordable, sustain-able and safe - before that time. When theseconditions are met avoidance of all breastfeedingby HIV-infected women is recommended (WHO2006).
In considering replacement feeding, the fol-lowing conditions are critical: sustainable accessto clean water; regular postnatal follow-up (withrepeated growth monitoring); nutritional coun-selling; and drugs and supplies at no cost or at asubsidized price, and with a controlled distribu-
tion. The family environment in which themother lives plays a key role in her choice of feed-ing option.
Early cessation of breastfeeding by HIV-in-fected women remains a challenge that needs tobe addressed. The five criteria (acceptable, fea-sible, affordable, sustainable and safe) need tobe reassessed at the time of early HIV diagnosisin infants and at other times when feeding prac-tices may be changing. Evidence now clearlyshows that infants who are known to be HIV-infected should continue breastfeeding.
It is anticipated that new data will be avail-able in 2008 to help clarify the issue of infantfeeding in the context of HIV. Current recom-mendations as contained in the Report from the2006 technical consultation (WHO et al. 2007)provide the best guidance for preventing post-natal HIV infection and improving HIV-free sur-vival while awaiting the new data.

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
44
References
Alioum A et al. (2001). Estimating the efficacyof interventions to prevent mother-to-childtransmission of HIV in breast-feeding popu-lations: development of a consensus method-ology. Statistical Medecine, 20(23):3539–3556.
Ayisi JG et al. (2004). Maternal malaria andperinatal HIV transmission, Western Kenya.Emerging infectious diseases [serial online]April [date cited]. Available at: http://www.cdc.gov/ncidod/EID/vol10no4/03-0303.htm, accessed 6 December 2007.
Ayouba A et al. (2003). Mother-to-child trans-mission of human immunodeficiency virustype 1 in relation to the season in Yaounde,Cameroon. American Journal of Tropical Medi-cine and Hygiene, 69(4):447–9.
Bahl R et al. (2005). Infant feeding patterns andrisks of death and hospitalization in the firsthalf of infancy: multicentre cohort study. Bul-letin of the World Health Organization,83(6):418–426.
Becquart P et al. (1999). Secretory leukocyteprotease inhibitor in colostrum and breast milkis not a major determinant of the protectionof early postnatal transmission of HIV. AIDS,13(18):2599–2602.
Becquart P et al. (2002). Compartmentalizationof HIV between breast milk and blood of HIV-infected mothers. Virology, 300(1):109–117.
Becquet R et al. (2005a). Infant feeding practic-es before implementing alternatives to pro-longed breastfeeding to reduce HIVtransmission through breastmilk in Abidjan,Cote d’Ivoire. Journal of Tropical Pediatrics,51(6):351–355.
Becquet R et al. (2005b). Knowledge, attitudes,and beliefs of health care workers regardingalternatives to prolonged breast-feeding(ANRS 1201/1202, Ditrame Plus, Abidjan,Cote d’Ivoire). Journal of Acquired Immune De-ficiency Syndrome, 40(1):102–105.
Becquet R et al. (2005c). Acceptability of exclu-sive breast-feeding with early cessation to pre-vent HIV transmission through breast milk(ANRS 1201/1202 Ditrame Plus, Abidjan,Cote d’Ivoire). Journal of Acquired Immune De-ficiency Syndrome, 40(5):600–608.
Becquet R et al. (2006). Complementary feed-ing adequacy in relation to nutritional statusamong early weaned breastfed children whoare born to HIV-infected mothers: ANRS1201/1202 Ditrame Plus, Abidjan, Coted’Ivoire. Pediatrics, 117(4):e701–710.
Becquet R et al. (2007). Two-year morbidity-mortality and alternatives to prolonged breast-feeding among children born to HIV-infectedmothers in Cote d’Ivoire. Public Library of Sci-ence Medicine, 4(1):e17.
Bhandari N et al. (2004). An educational inter-vention to promote appropriate complemen-tary feeding practices and physical growth ininfants and young children in rural Haryana,India. Journal of Nutrition, 134(9):2342–2348.
Black RE, Morris SS, Bryce J (2003). Where andwhy are 10 million children dying every year?Lancet, 361(9376):2226–2234.
Bland RM et al. (2006). WHO and UNICEFinfant feeding policy for HIV-positive women - howfeasible is it? 16th International Conference onAIDS, August 13-18 2006, Toronto, Canada(Abstract: TUPE0342.). Available online:h t t p : / / w w w . a i d s 2 0 0 6 . o r g /abstract.aspx?elementId=2193736 , accessedAugust 31, 2007.

45
Bland RM et al. (2007). Infant feeding counsel-ling for HIV-infected and uninfected women:appropriateness of choice and practice. Bulle-tin of the World Health Organization, 85(4):289–296.
Bobat R et al. (1997). Breastfeeding by HIV-infected women and outcome in their infants:a cohort study from Durban, South Africa.AIDS, 11:1627–1633.
Bomsel M (1997). Transcytosis of infectioushuman immunodeficiency virus across a tighthuman epithelial cell line barrier. Nature Med-icine, 3(1):42–47.
Bomsel M et al. (1998). Intracellular neutrali-zation of HIV transcytosis across tight epi-thelial barriers by anti-HIV envelope proteindIgA or IgM. Immunity, 9(2):277–287.
Bramson C et al. (2006). Toxicity of nevirapine inHIV-infected women with high CD4 counts inMalawi: the BAN study. 16th InternationalConference on AIDS, August 13-18 2006,Toronto, Canada. Poster WEPE0082. Availa-ble online at: http://www.iasociety.org/Default.aspx?pageId=11&abstractId=2199496,accessed August 31, 2007.
Bryce J & Victora CG (2005). Child survival:countdown to 2015. Lancet, 365(9478):2153–2154.
Bryce J et al. (2005). WHO estimates of thecauses of death in children. Lancet365(9465):1147–1152.
Bryce J et al. (2006a). Getting it right for chil-dren: a review of UNICEF joint health andnutrition strategy for 2006-15. Lancet368(9538):817–819.
Bryce J et al. (2006b). Countdown to2015:tracking intervention coverage for childsurvival. Lancet 368(9541):1067–1076.
Bulterys M (2000). Breastfeeding in women withHIV. Journal of the American Medical Association,284(8):956; author reply 956–7.
Buve A, Bishikwabo-Nsarhaza K, MutangaduraG (2002). The spread and effect of HIV in-fection in sub-Saharan Africa. Lancet,359(9322):2011–2017.
Cames C et al. (2006). A sustainable baby foodsupport for HIV-infected mothers. The Kesho Borastudy initiative in Bobo Dioulasso, Burkina Faso.16th International Conference on AIDS, Au-gust 13-18 2006, Toronto, Canada. PosterTUPE0356. Available online at: http://www.iasociety.org/Default.aspx?pageId=11&abstractId=2192216, accessed August31, 2007.
Cesar JA et al. (1999). Impact of breast feedingon admission for pneumonia during postneo-natal period in Brazil: nested case-controlstudy. British Medical Journal, 318(7194):1316–1320.
Chantry CJ, Howard CR, Auinger P (2006). Fullbreastfeeding duration and associated decreasein respiratory tract infection in US children.Pediatrics, 117(2):425–432.
Coovadia HM et al. (2007). Mother-to-childtransmission of HIV infection during exclu-sive breastfeeding in the first 6 months of life:an intervention cohort study. Lancet,369(9567):1107–1116.
Corneli AL et al. (2007). Involving communi-ties in the design of clinical trial protocols: theBAN Study in Lilongwe, Malawi. Contempo-rary Clinical Trials, 28(1):59–67.
Costello A & Osrin D (2005). The case for anew Global Fund for maternal, neonatal, andchild survival. Lancet, 366(9485):603–605.
Coutsoudis A et al. (2001). Method of feedingand transmission of HIV from mothers to chil-dren by 15 months of age: prospective cohortstudy from Durban, South Africa. AIDS,15(3):379–387.
Coutsoudis A et al. (2003). Morbidity in chil-dren born to women infected with humanimmunodeficiency virus in South Africa: doesmode of feeding matter? Acta Paediatrica,92(8):890–895.
Creek T (2006). Role of infant feeding and HIV ina severe outbreak of diarrhea and malnutritionamong young children - Botswana, 2006. PEP-FAR Implementers Meeting, Durban. (Ab-stract #LB1).
REFERENCES

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
46
Dabis F & Ekpini ER (2002). HIV/AIDS andmaternal and child health in Africa. Lancet,359(9323):2097–2104.
Dabis F et al. (1999). Six months efficacy, toler-ance and acceptability of a short regimen oforal zidovudine in reducing vertical transmis-sion of HIV in breast-fed children. A doubleblind placebo controlled multicentre trial,ANRS049a, Côte d’Ivoire and Burkina Faso.Lancet, 353:786–792.
Dabis F et al. (2000). Preventing mother-to-childtransmission of HIV in Africa in the year2000. AIDS, 14:1017–1026.
Dabis F et al. (2004). Prevention of HIV trans-mission through breast-feeding: strengtheningthe research agenda. [Report]. Journal of Ac-quired Immune Deficiency Syndrome, 35(2):167–168.
Dabis F et al. (2005). Field efficacy of zidovu-dine, lamivudine and single-dose nevirapineto prevent peripartum HIV transmission.AIDS, 19(3):309–318.
De Cock KM et al. (2000). Prevention of moth-er-to-child HIV transmission in resource-poorcountries: translating research into policy andpractice. Journal of the American Medical Associ-ation, 283:1175–1182.
De Cock KM, Mbori-Ngacha D, Marum E(2002). Shadow on the continent: publichealth and HIV/AIDS in Africa in the 21stcentury. Lancet, 360(9326):67–72.
Dorenbaum A et al. (2002). Two-dose intrapar-tum/newborn nevirapine and standard antiret-roviral therapy to reduce perinatal HIVtransmission: a randomized trial. Journal of theAmerican Medical Association, 288(2):189–198.
Dunn DT (1998). A review of statistical meth-ods for estimating the risk of vertical humanimmunodeficiency virus transmission. Interna-tional Journal of Epidemiology, 27:1064–1070.
Dunn DT et al. (1992). Risk of human immun-odeficiency virus type 1 transmission throughbreastfeeding. Lancet, 340(8819):585–588.
Ekpini E et al. (1997). Late post-natal mother-to-child transmission of HIV -1 in Abidjan,Côte d’Ivoire. Lancet, 349:1054–1059.
Ekpini R et al. (2002). Changes in plasma HIVRNA viral load and CD4 count and lack ofzidovudine resistance among HIV-infectedpregnant women receiving short-course zido-vudine. AIDS, 16:625–630.
Embree JE et al. (2000). Risk factors for post-natal mother-child transmission of HIV. AIDS,14(16):2535–2541.
Eshleman SH et al. (2004a). Characterizationof nevirapine resistance mutations in womenwith subtype A vs. D HIV 6-8 weeks after sin-gle-dose nevirapine (HIVNET 012). Journal ofAcquired Immune Deficiency Syndrome,35(2):126–130.
Eshleman SH et al. (2004b). Comparison ofnevirapine (NVP) resistance in Ugandan wom-en 7 days vs. 6-8 weeks after single-dose NVPprophylaxis: HIVNET 012. AIDS Research andHuman Retroviruses 20(6):595–599.
Eshleman SH et al. (2005). Nevirapine (NVP)resistance in women with HIV subtype C,compared with subtypes A and D, after theadministration of single-dose NVP. Journal ofInfectious Diseases, 192(1):30–36.
European Collaborative Study (1996). Verticaltransmission of HIV: maternal immune sta-tus and obstetric factors. AIDS, 10:1675–81.
European Collaborative Study (1997). Maternalviral load and vertical transmission of HIV:an important factor but not the only one.AIDS, 13:1377–1385.
European Collaborative Study (2001). HIV-in-fected pregnant women and vertical transmis-sion in Europe since 1986. Europeancollaborative study. AIDS, 15(6):761–770.
Farley T & Kesho Bora Study Group (2006).Antiretroviral prophylaxis/treatment and in-fant feeding modality among HIV-infectedwomen in sub-Saharan Africa: the Kesho Borastudy. 16th International Conference onAIDS, August 13-18 2006, Toronto, Canada.(Abstract: CDB0402). Available online at:http://www.iasociety.org/Default.aspx?pageId=11&abstractId=2196917, accessedAugust 31, 2007.

47
Farquhar C & John-Stewart G (2003). The roleof infant immune responses and genetic fac-tors in preventing HIV acquisition and dis-ease progression. Clinical and ExperimentalImmunology 134(3):367–377.
Farquhar C et al. (2006). Pediatric HIV type 1vaccine trial acceptability among mothers inKenya. AIDS Research and Human Retroviruses22(6):491–495.
Fawzi WW et al. (2002a). Transmission of HIVthrough breastfeeding among women in Dares Salaam, Tanzania. Journal of Acquired ImmuneDeficiency Syndromes 31(3):331–338.
Fawzi WW et al. (2002b). Randomized trial ofvitamin supplements in relation to transmis-sion of HIV through breastfeeding and earlychild mortality. AIDS, 16(14):1935–1944.
Frankel SS et al. (1997). Active replication of HIVat the lymphoepithelial surface of the tonsil.American Journal of Pathology, 151(1):89–96.
Gaillard P et al. (2004). Use of antiretroviraldrugs to prevent HIV transmission throughbreast-feeding: from animal studies to rand-omized clinical trials. Journal of Acquired Im-mune Deficiency Syndrome, 35(2):178–187.
Giuliano M et al. (2007). Triple antiretroviralprophylaxis administered during pregnancyand after delivery significantly reduces breastmilk viral load: a study within the Drug Re-source Enhancement Against AIDS and Mal-nutrition Program. Journal of Acquired ImmuneDeficiency Syndrome, 44(3):286–291.
Goto K et al. (1999). Epidemiology of alteredintestinal permeability to lactulose and man-nitol in Guatemalan infants. Journal of Pediat-ric Gastroenterology and Nutrition, 28:282–290.
Gray GE et al. (2005). A randomized trial oftwo post exposure prophylaxis regimens toreduce mother-to-child HIV transmission ininfants of untreated mothers. AIDS,19(12):1289–1297.
Guay LA et al. (1999). Intrapartum and neona-tal single-dose nevirapine compared with zi-dovudine for prevention of mother-to-childtransmission of HIV in Kampala, Uganda:HIVNET 012 randomized trial. Lancet,354:795–802.
Habicht J, DaVanzo J, Butz W (1986). Doesbreastfeeding really save lives, or are apparentbenefits due to biases? American Journal of Ep-idemiology, 123:279–290.
Harwood D & PLANetWIRE.org (2001). Sum-mary of UNGASS and the Declaration ofCommitment. Available online at: http://www.PLANetWIRE.org.
Hira S et al. (1990). Apparent vertical transmis-sion of Human Immunodeficiency Virus type1 by breast-feeding in Zambia. Journal of Pedi-atrics, 117:421–424.
Humphrey JH et al. (2006). HIV incidenceamong postpartum women in Zimbabwe: riskfactors and the effect of vitamin A supplemen-tation. AIDS, 20(10):1437–1446.
Iliff PJ et al. (2005). Early exclusive breastfeed-ing reduces the risk of postnatal HIV trans-mission and increases HIV-free survival. AIDS,19(7):699–708.
Israel-Ballard K et al. (2006a). Bacterial safetyof flash-heated and unheated expressed breast-milk during storage. Journal of Tropical Pediat-rics, 52(6):399–405.
Israel-Ballard K et al. (2006b). Acceptability ofheat treating breast milk to prevent mother-to-child transmission of human immunodefi-ciency virus in Zimbabwe: a qualitative study.Journal of Human Lactation 22(1):48–60.
Israel-Ballard K et al. (2007). Viral safety offlash-heated breast milk: a method to reducemother-to-child transmission of HIV in re-source-poor countries. Journal of Acquired Im-mune Deficiency Syndrome (in press).
Jackson JB et al. (2003). Intrapartum and neo-natal single-dose nevirapine compared withzidovudine for prevention of mother-to-childtransmission of HIV in Kampala, Uganda: 18-month follow-up of the HIVNET 012 rand-omized trial. Lancet, 362(9387):859–868.
Jeffery BS & Mercer KG (2000). Pretoria pas-teurisation: a potential method for the reduc-tion of postnatal mother to child transmissionof the human immunodeficiency virus. Jour-nal of Tropical Pediatrics 46(4):219–223.
REFERENCES

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
48
Jeffery BS et al. (2003). The effect of Pretoriapasteurization on bacterial contamination ofhand-expressed human breastmilk. Journal ofTropical Pediatrics, 49(4):240–244.
John G et al. (1997). Genital shedding of hu-man immunodeficiency virus type 1 DNAduring pregnancy: association with immuno-depression, abnormal cervical vaginal dis-charge and severe vitamin A deficiency. Journal ofInfectious Diseases, 175:57–62.
John GC et al. (2001). Correlates of mother-to-child human immunodeficiency virus type 1(HIV) transmission: association with mater-nal plasma HIV RNA load, genital HIV DNAshedding, and breast infections. Journal of In-fectious Diseases, 183(2):206–212.
John-Stewart G et al. (2004). Breast-feeding andtransmission of HIV. Journal of Acquired ImmuneDeficiency Syndrome, 35(2):196–202.
Jourdain G et al. (2004). Intrapartum exposureto nevirapine and subsequent maternal re-sponses to nevirapine-based antiretroviral ther-apy. New England Journal of Medicine,351(3):229–240.
Kafulafula G (2007). Post-weaning gastroenteritisand mortality in HIV-uninfected African infantsreceiving antiretroviral prophylaxis to preventMTCT of HIV. Fourteenth Conference on Ret-roviruses and Opportunistic Infections, Feb-ruary 25-28 2007, Los Angeles, USA(Abstract 773). Available online at: http://www.retroconference.org/2007/Abstracts/28294.htm, accessed August 31, 2007.
Kilewo C (2005). Prevention of mother to child trans-mission of HIV through breastfeeding by treatinginfants prophylactically with lamivudine in Dar esSalaam, Tanzania. 3rd IAS Conference on HIVPathogenesis and Treatment, Rio de Janeiro,Brazil (Abstract TuPe5.3P01). Available on-line at: http://www.aegis.org/conferences/IASHIVPT/2005/TuPe5-3P01.html, accessedAugust 31, 2007.
Koulinska IN et al. (2006). Transmission of cell-free and cell-associated HIV through breast-feeding. Journal of Acquired Immune DeficiencySyndrome, 41(1):93–99.
Kourtis AP (2007). Diarrhea in uninfected infantsof HIV-infected mothers who stop breastfeeding at6 months: the BAN study experience. FourteenthConference on Retroviruses and Opportunis-tic Infections, February 25-28 2007, Los An-geles, USA (Abstract 772). Available onlineat: http://www.retroconference.org/2007/Ab-stracts/29630.htm, accessed August 31, 2007.
Kourtis AP et al. (2006). Mother-to-child trans-mission of HIV: timing and implications forprevention. Lancet Infectious Diseases,6(11):726–732.
Kovacs A et al. (2001). Determinants of HIVshedding in the genital tract of women. Lan-cet, 358(9293):1593–1601.
Kramer MS & Kakuma R (2004). The optimalduration of exclusive breastfeeding: a system-atic review. Advances in experimental medicine andbiology, 554:63–77.
Kramer MS et al. (2001). Promotion of Breast-feeding Intervention Trial (PROBIT): a rand-omized trial in the Republic of Belarus. Journal ofthe American Medical Association, 285(4):413–420.
Kramer MS et al. (2003). Infant growth andhealth outcomes associated with 3 comparedwith 6 months of exclusive breastfeeding.American Journal of Clinical Nutrition,78(2):291–295.
Kuhn L et al. (2001). T-helper cell responses toHIV envelope peptides in cord blood: protec-tion against intrapartum and breast-feedingtransmission. AIDS, 15(1):1–9.
Kuhn L et al. (2005). Alpha-defensins in theprevention of HIV transmission among breast-fed infants. Journal of Acquired Immune DeficiencySyndrome, 39(2):138–142.
Kuhn L et al. (2006). HIV-specific secretory IgAin breast milk of HIV-positive mothers is notassociated with protection against HIV trans-mission among breast-fed infants. Journal ofPediatrics 149(5):611–616.
Kuhn, L. et al. (2007) High Uptake of ExclusiveBreastfeeding and Reduced Early Post-NatalHIV Transmission. Public Library of SciencesONE. 2 (12): e1363.

49
Labbok MH et al. (1994). The lactational amen-orrhea method (LAM): a postpartum intro-ductory family planning method with policyand program implications. Advances in contra-ception 10(2):93–109.
Lawrence RM & Lawrence RA (2004). Breastmilk and infection. Clinics in perinatology31(3):501–528.
Leroy V et al. (1994). Seroincidence of HIV in-fection in African women of reproductive age:a prospective cohort study in Kigali, Rwanda,1988-1992. AIDS, 8(7):983-986.
Leroy V et al. (1998). International multicentrepooled analysis of late postnatal mother-to-child transmission of HIV infection. Lancet,352:597–600.
Leroy V et al. (2001). Maternal plasma viral load,zidovudine and mother-to-child transmissionof HIV in Africa: DITRAME ANRS 049a tri-al. AIDS, 15(4):517–522.
Leroy V et al. (2002). Twenty-four month effi-cacy of a maternal short-course zidovudineregimen to prevent mother-to-child transmis-sion of HIV in West Africa. AIDS, 16(4):631–641.
Leroy V et al. (2003). Postnatal transmission ofHIV after a maternal short-course zidovudineperipartum regimen in West Africa. AIDS,17(10):1493–1501.
Leroy V et al. (2004). Postnatal transmission riskaccording to feeding modalities in children born toHIV-infected mothers in a PMTCT project in Abid-jan, Côte d’Ivoire. The Ditrame Plus ANRS1201/1202 study. Presented at the XV Inter-national AIDS conference, Bangkok, Thai-land. Available online at: http://gateway.nlm.nih.gov/MeetingAbstracts/102280584.html, accessed August 31, 2007.
Leroy V et al. (2005). Is there a difference in theefficacy of peripartum antiretroviral regimensin reducing mother-to-child transmission ofHIV in Africa? AIDS, 19(16):1865–1875.
Leroy, V. et al. (2008) 18-Month Effectivenessof Short-Course Antiretroviral Regimens Com-bined with Alternatives to Breastfeeding toPrevent HIV Mother-to-Child Transmission.Public Library of Sciences ONE. 3 (2): e1645.
Leroy V et al. (2007). Acceptability of formula-feeding to prevent HIV postnatal transmis-sion, Abidjan, Cote d’Ivoire: the ANRS 1201/1202 Ditrame Plus Study. Journal of AcquiredImmune Deficiency Syndrome, 44(1):77–86.
Lewis P et al. (1998). Cell-free human immuno-deficiency virus type 1 in breast milk. Journalof Infectious Diseases, 177(1):34–39.
Luzuriaga K et al. (2006). Vaccines to preventtransmission of HIV via breastmilk: scientificand logistical priorities. Lancet, 368(9534):511–521.
Magoni M et al. (2005). Mode of infant feedingand HIV infection in children in a programfor prevention of mother-to-child transmissionin Uganda. AIDS, 19(4):433–437.
Mandelbrot L et al. (1999). Frequent detectionof HIV in the gastric aspirates of neonatesborn to HIV-infected mothers. AIDS, 13(15):2143–2149.
Manigart O et al. (2004). Effect of perinatal zi-dovudine prophylaxis on the evolution of cell-free HIV RNA in breast milk and on postnataltransmission. Journal of Infectious Diseases,190(8):1422–1428.
Mason E (2005). Child survival: time to matchcommitments with action. Lancet, 365(9467):1286–1288.
Mayaux M et al. (1997). Maternal virus loadduring pregnancy and mother-to-child trans-mission of human immunodeficiency virustype 1: the French perinatal cohort study. Jour-nal of Infectious Diseases, 175:172–175.
Mbori-Ngacha D et al. (2001). Morbidity andmortality in breastfed and formula-fed infantsof HIV-infected women: a randomized clini-cal trial. Journal of the American Medical Associ-ation, 286(19):2413–2420.
Miotti PG et al. (1999). HIV transmissionthrough breastfeeding - a study in Malawi.Journal of the American Medical Association,282:744–749.
REFERENCES

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
50
Moodley D et al. (2003). A multicenter rand-omized controlled trial of nevirapine versus acombination of zidovudine and lamivudine toreduce intrapartum and early postpartummother-to-child transmission of human immu-nodeficiency virus type 1. Journal of InfectiousDiseases, 187(5):725–735.
Mostad SB et al. (1999). Cervical shedding ofcytomegalovirus in human immunodeficien-cy virus type 1-infected women. Journal ofMedical Virology, 59(4):469–473.
Mwapasa V et al. (2004). The effect of plasmo-dium falciparum malaria on peripheral andplacental HIV RNA concentrations in preg-nant Malawian women. AIDS, 18(7):1051–1059.
Nduati R, John G, Kreiss J (1994). Postnataltransmission of HIV through pooled breastmilk. Lancet, 344:1432.
Nduati R et al. (2000). Effect of breastfeedingand formula feeding on transmission of HIV.A randomized clinical trial. Journal of the Amer-ican Medical Association, 283:1167–1174.
Nduati R et al. (2001). Effect of breastfeedingon mortality among HIV infected women: arandomized trial. Lancet, 357(9269):1651–1655.
Newell ML (2001). Prevention of mother-to-child transmission of HIV: challenges for thecurrent decade. Bulletin of the World HealthOrganization, 79(12):1138–1144.
Newell ML (2006). Current issues in the pre-vention of mother-to-child transmission ofHIV infection. Transactions of the Royal Societyof Tropical Medicine and Hygiene, 100(1):1–5.
Newell ML et al. (2004). Mortality of infectedand uninfected infants born to HIV-infectedmothers in Africa: a pooled analysis. Lancet,364(9441):1236–1243.
Nicoll A et al. (2000a). Infant feeding and HIVinfection. AIDS, 14(Suppl 3):S57–S74.
Nicoll A, Newell ML, Peckham CS (2000b).Breast feeding is a major factor in HIV trans-mission. British Medical Journal, 321(7266):963.
Nicoll A & Williams A (2002). Breast feeding.Archives of Disease in Childhood, 87(2):91-92.
Nielsen K et al. (1996). Presence of human im-munodeficiency virus (HIV) type 1 and HIV-specific antibodies in cervicovaginal secretionsof infected mothers and in the gastric aspi-rates of their infants. Journal of Infectious Dis-eases, 173:1001–1004.
Onyango C (2007). Early breastfeeding cessationamong HIV-exposed negative infants and risk ofserious gastroenteritis: findings from a perinatalprevention trial in Kampala, Uganda. FourteenthConference on Retroviruses and Opportunis-tic Infections, February 25-28 2007, Los An-geles, USA (Abstract 775). Available onlineat: http://www.retroconference.org/2007/Ab-stracts/29008.htm, accessed August 31, 2007.
Palasanthiran P et al. (1993). Breastfeeding dur-ing primary maternal HIV infection and riskof transmission from mother to child. Journalof Infectious Diseases, 167:441–444.
Panlilio AL et al. (2005). Updated U.S. PublicHealth Service guidelines for the managementof occupational exposures to HIV and recom-mendations for postexposure prophylaxis.Morbidity and Mortality Weekly Report (US Cent-ers for Disease Control), 54(RR-9):1–17.
Petitjean G et al. (2006). Compartment-specificHIV resting T-cell reservoirs. AIDS, 20(9):1338–1340.
Pillay K et al. (2000). Cell-free virus in breastmilk of HIV-seropositive women. Journal ofAcquired Immune Deficiency Syndrome,24(4):330–336.
Piwoz EG et al. (2005). An education and coun-seling program for preventing breast-feeding-associated HIV transmission in Zimbabwe:design and impact on maternal knowledge andbehavior. Journal of Nutrition, 135(4):950–955.
Piwoz EG, Ross J, Humphrey J (2004). Humanimmunodeficiency virus transmission duringbreastfeeding: knowledge, gaps, and challengesfor the future. Advances in experimental medicineand biology, 554:195–210.

51
Richardson BA et al. (2003). Breast-milk infec-tivity in human immunodeficiency virus type1-infected mothers. Journal of Infectious Diseas-es, 187(5):736–740.
Rollins NC et al. (2001). Feeding mode, intesti-nal permeability, and neopterin excretion: alongitudinal study in infants of HIV-infectedsouth African women. Journal of Acquired Im-mune Deficiency Syndrome, 28(2):132–139.
Rollins NC et al. (2007). Surveillance of moth-er-to-child transmission prevention pro-grammes at immunization clinics: the case foruniversal screening. AIDS, 21(10):1341–1347.
Rouzioux C et al. (1993). Timing of mother-to-child transmission depends on maternal sta-tus. The HIV Infection on Newborns FrenchCollaborative Study Group. AIDS, 7(Suppl2):S49–S52.
Ruff A et al. (1994). Prevalence of HIV and p24antigen in breast milk and correlation withmaternal factors. Journal of Acquired ImmuneDeficiency Syndrome, 7:68–73.
Saba J (1999). The results of the PETRA interven-tion trial to prevent perinatal transmission in sub-Saharan Africa. 6th Conference on Retrovirusesand Opportunistic Infections, Chicago, USA(Abstract S6).
Saba J et al. (2002). Efficacy of three short-courseregimens of zidovudine and lamivudine in pre-venting early and late transmission of HIVfrom mother to child in Tanzania, South Afri-ca, and Uganda (Petra study): a randomized,double-blind, placebo-controlled trial. Lancet,359(9313):1178–1186.
Sabbaj S et al. (2002). Human immunodeficien-cy virus-specific CD8(+) T cells in humanbreast milk. Journal of Virology, 76(15):7365–7373.
Schmid GP et al. (2004). Transmission of HIVinfection in sub-Saharan Africa and effect ofelimination of unsafe injections. Lancet,363(9407):482–488.
Semba RD & Neville MC (1999). Breast-feed-ing, mastitis, and HIV transmission: nutrition-al implications. Nutrition Reviews, 57:146–153.
Semba R et al. (1994). Maternal vitamin A defi-ciency and mother-to-child transmission ofHIV. Lancet, 343:1593–1597.
Semba RD et al. (1999a). Human immunodefi-ciency virus load in breast milk, mastitis, andmother-to-child transmission of human immu-nodeficiency virus type 1. Journal of InfectiousDiseases, 180:93–98.
Semba RD et al. (1999b). Mastitis and immu-nological factors in breast milk of lactatingwomen in Malawi. Clinical and Diagnostic Lab-oratory Immunology, 6:671–674.
Shaffer N et al. (1999a). Short-course zidovu-dine for perinatal HIV transmission in Bang-kok, Thailand: a randomized controlled trial.Lancet, 353:773–780.
Shaffer N et al. (1999b). Maternal viral load andperinatal HIV subtype E transmission, Thai-land. Journal of Infectious Diseases, 179:590–599.
Shapiro RL et al. (2005a). Antiretroviral con-centrations in breast-feeding infants of wom-en in Botswana receiving antiretroviraltreatment. Journal of Infectious Diseases,192(5):720–727.
Shapiro RL et al. (2005b). Highly active antiret-roviral therapy started during pregnancy orpostpartum suppresses HIV RNA, but notDNA, in breast milk. Journal of Infectious Dis-eases, 192(5):713–719.
Shapiro RL et al. (2006). Maternal single-dosenevirapine versus placebo as part of anantiretroviral strategy to prevent mother-to-child HIV transmission in Botswana. AIDS,20(9):1281–1288.
Simonds R et al. (1998). Impact of zidovudineuse on risk and risk factors for perinatal trans-mission of human immunodeficiency virus.AIDS, 12:301–308.
Taha TE et al. (2003). Short postexposure proph-ylaxis in newborn babies to reduce mother-to-child transmission of HIV: NVAZrandomized clinical trial. Lancet, 362(9391):1171–1177.
REFERENCES

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
52
Temmerman M et al. (2003). Mother-to-childHIV transmission in resource poor settings:how to improve coverage? AIDS, 17(8):1239–1242.
The Breastfeeding and HIV International Trans-mission Study Group (BHITS) (2004). Latepostnatal transmission of HIV in breast-fedchildren: an individual patient data meta-anal-ysis. Journal of Infectious Diseases, 189(12):2154–2166.
The Working Group on Mother-to-Child Trans-mission of HIV (1995). Rates of mother-to-child transmission of HIV in Africa, Americaand Europe: results from 13 perinatal studies.Journal of acquired immune deficiency syndromesand human retrovirology, 8:506–510.
Thea DM et al. (2004). Issues in the design of aclinical trial with a behavioral intervention -the Zambia Exclusive Breast-Feeding Study.Controlled Clinical Trials, 25(4):353–365.
Thea DM et al. (2006). Post-weaning breast milkHIV viral load, blood prolactin levels andbreast milk volume. AIDS, 20(11):1539–1547.
Thior I et al. (2006). Breastfeeding plus infantzidovudine prophylaxis for 6 months vs for-mula feeding plus infant zidovudine for 1month to reduce mother-to-child HIV trans-mission in Botswana: a randomized trial: theMashi Study. Journal of the American MedicalAssociation, 296(7):794–805.
Thomas T (2007). Rates of diarrhea associated withearly weaning among infants in Kisumu, Kenya.Fourteenth Conference on Retroviruses andOpportunistic Infections, February 25-282007, Los Angeles, USA (Abstract 774).
Thorne C and Newell ML (2004). Are girls moreat risk of intrauterine-acquired HIV infectionthan boys? AIDS, 18(2):344–347.
Thorne C. and Newell, M. L. (2007). Safety ofagents used to prevent mother-to-child trans-mission of HIV: is there any cause for con-cern? Drug Safety, 30(3):203–213.
Tonwe-Gold, B. et al. (2007) Antiretroviral treat-ment and prevention of peripartum and post-natal HIV transmission in West Africa:evaluation of a two-tiered approach. PublicLibrary of Sciences Med. 4 (8): e257
UNAIDS (2006). AIDS epidemic update. Availa-ble online at: http://www.unaids.org/en/HIV_data/2006GlobalReport/default.asp, ac-cessed 1 September 2007.
UNAIDS and WHO (2007). AIDS Epidemic Up-date. UNAIDS and World Health Organiza-tion, Geneva.
UNICEF (2005). Celebrating the Innocenti decla-ration on the protection, promotion and support ofbreastfeeding: past achievements, present challeng-es and the way forward for infant and young childfeeding. Florence, Innocenti Research Centre.
UN (2001). Declaration of Commitment on HIV/AIDS. United Nations General Assembly Spe-cial Session on HIV/AIDS, No. 54. New York,United Nations.
Urdaneta S et al. (2005). Inactivation of HIV inbreast milk by treatment with the alkyl sul-fate microbicide sodium dodecyl sulfate (SDS).Retrovirology, 2(1):28.
Van de Perre P (1999). Transmission of humanimmunodeficiency virus type 1 through breast-feeding: how can it be prevented? Journal ofInfectious Diseases, 179(Suppl 3):S405–S407.
Van de Perre P, Manigart O, Meda N (2001).Long-term reduction of HIV transmissionfrom mother to breastfed child by antiretrovi-ral agents: are more drugs better than less?AIDS, 15(5):658–659.
Van de Perre P et al. (1991). Postnatal transmis-sion of human immunodeficiency virus type-1 from mother to infant. A prospective cohortstudy in Kigali, Rwanda. New England Journalof Medicine, 325:593–598.
Van de Perre P et al. (1993). Infective and anti-infective properties of breastmilk from HIV-infected women. Lancet, 341(8850):914–918.
Van de Perre P et al. (1997). Zidovudine and breast-feeding. AIDS Patient Care STDs, 11:4–5.

53
Van’t Hoog et al. (2005). Preventing mother-to-child transmission of HIV in Western Kenya:operational issues. Journal of Acquired ImmuneDeficiency Syndrome, 40(3):344–349.
Vekemans M (1997). Postpartum contraception:the lactational amenorrhea method. EuropeanJournal of Contraception and Reproductive HealthCare, 2(2):105–111.
Victora CG et al. (1987). Evidence for protec-tion by breast-feeding against infant deathsfrom infectious diseases in Brazil. Lancet,ii:319–322.
Visco-Comandini U et al. (2005). Possible child-to-mother transmission of HIV by breastfeed-ing. Journal of the American Medical Association,294(18):2301–2302.
Vyankandondera J et al. (2003). Reducing risk ofHIV transmission from mother to infant throughbreastfeeding using antiretroviral prophylaxis ininfants (SIMBA study). 2nd IAS Conferenceon HIV Pathogenisis and Treatment. July2003, Paris, France (Abstract No. LB7).
Walker N, Schwartlander B, Bryce J (2002).Meeting international goals in child survivaland HIV/AIDS. Lancet, 360(9329):284–289.
Wiktor S et al. (1999). Short-course oral zido-vudine for prevention of mother-to-child trans-mission of HIV in Abidjan, Côte d’Ivoire: arandomized trial. Lancet, 353:781–785.
Willumsen JF et al. (2000). Subclinical mastitisas a risk factor for mother-infant HIV trans-mission. Advances in experimental medicine andbiology, 478:211–223.
Willumsen JF et al. (2001). Variation in breast-milk HIV viral load in left and right breastsduring the first 3 months of lactation. AIDS,15(14):1896–1898.
Willumsen JF et al. (2003). Breastmilk RNA vi-ral load in HIV-infected South African wom-en: effects of subclinical mastitis and infantfeeding. AIDS, 17(3):407–414.
WHO (1998). Complementary feeding of young chil-dren in developing countries: a review of current sci-entific knowledge. Geneva, World HealthOrganization.
WHO (2001). The optimal duration of exclusivebreasfeeding. Report of an expert consultation.Geneva, Switzerland, 28-30 March 2001.Available online at: http://www.who.int/child-adolescent-health/New_Publications/NUTRI-TION/WHO_CAH_01_24.pdf, accessed 1September 2007.
WHO (2005). World health report 2005: make everymother and child count. Geneva, World HealthOrganization.
WHO (2006). WHO HIV prevention and treat-ment guidelines. Antiretroviral drugs for treat-ing pregnant women and preventing HIV infectionin infants, towards universal access: recommenda-tions for a public health approach. Geneva, WorldHealth Organization.
WHO Collaborative Study Team (2000). Effectof breastfeeding on infant and child mortalitydue to infectious diseases in less developedcountries: a pooled analysis. WHO Collabo-rative Study Team on the Role of Breastfeed-ing on the Prevention of Infant Mortality.Lancet, 355(9202):451–455.
WHO and UNICEF (2007). Guidance on globalscale-up of the prevention of mother-to-child trans-mission of HIV: towards universal access for wom-en, infants and young children and eliminating HIVand AIDS among children. World Health Or-ganization, Geneva.
WHO, UNICEF, UNFPA and UNAIDS (2007).HIV and infant feeding: new evidence and pro-grammatic experience: report of a technical consul-tation. World Health Organization, Geneva.
WHO, UNICEF, UNFPA and UNAIDS (2004).HIV transmission through breastfeeding: a reviewof available evidence. Geneva, World HealthOrganization.
WHO et al. (1995). Consensus Statement: Lacta-tional Amenorrhea Method for Family Planning.Bellagio, Italy.
Ziegler J et al. (1985). Postnatal transmission ofAIDS-associated retrovirus from mother-to-infant. Lancet, i:896–898.
REFERENCES

HIV TRANSMISSION THROUGH BREASTFEEDING: A REVIEW OF AVAILABLE EVIDENCE - AN UPDATE FROM 2001 TO 2007
54

ISBN 978 92 4 159659 6
For further information, please contact:
World Health Organization
Department of Child and Adolescent Health and Development ([email protected]) or
Department of HIV/AIDS ([email protected]) or
Department of Nutrition for Health and Development ([email protected])
20 Avenue Appia, 1211 Geneva 27, Switzerland
website: http://www.who.int
UNICEF
Nutrition Section – Programme Division
3 United Nations Plaza
New York, New York 10017, United States of America
Tel +1 212 326 7000
A REVIEW OF AVAILABLE EVIDENCE
HIV Transmission ThroughBreastfeeding
2007 Update
This publication is an update of the review of current knowledge on HIV transmission throughbreastfeeding, with a focus on information made available between 2001 and 2007. It re-views scientific evidence on the risk of HIV transmission through breastfeeding, the impactof different feeding options on child health outcomes, and conceivable strategies to reduceHIV transmission through breastfeeding with an emphasis on the developing world.