hjernens plasticitet efter hjerneskade. kliniske aspekter...
TRANSCRIPT

NICK WARD, UCL INSTITUTE OF NEUROLOGY, QUEEN SQUARE
Hjernens plasticitet efter hjerneskade.
Kliniske aspekter for bedring i praksis
@WardLab
@dr_nickward Hjerneskade og armfunktion, Glostrup, 26th January 2017
NICK WARD, UCL INSTITUTE OF NEUROLOGY, QUEEN SQUARE
Brain plasticity after brain injury, clinical
aspects for recovery into practice
@WardLab
@dr_nickward Hjerneskade og armfunktion, Glostrup, 26th January 2017
Overview – summary points
1. Recovery after stroke - reason for optimism
2. Different manifestations of post-stroke plasticity
3. Manipulating plasticity processes to promote recovery
4. Progressing to clinical trials in humans – too early
Promoting Recovery After Stroke
Slides are on my website www.ucl.ac.uk/ion/departments/sobell/Research/NWard
Link will be tweeted from @dr_nickward
STROKE IS A CHRONIC AND PROGRESSIVE DISEASE • 17 million people a year experience first stroke
• Survival is improving but burden still high – 1.5M in UK
• Economic burden is high - £9B a year in UK
• Funding for stroke research lags behind dementia, CHD and cancer
• Turn attention towards treatments to promote recovery
Promoting Recovery After Stroke Stroke – the problem
TIME-LIMITED PERIOD OF INCREASED PLASTICITY 1. How to take advantage of this critical period through
the optimal timing, intensity, amount and even type of behavioural training that makes up neurorehabilitation
2. How to augment the biological mechanisms of post-stroke plasticity to enhance or prolong the effects of behavioural training in human stroke patients
Promoting Recovery After Stroke Stroke – reason for optimism
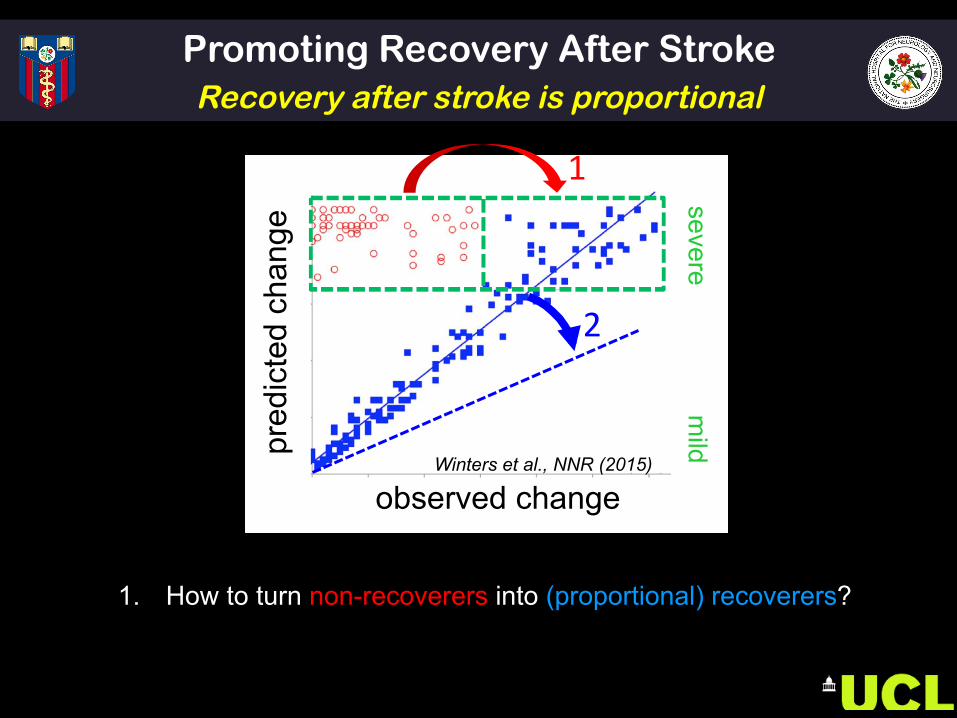
Promoting Recovery After Stroke Recovery after stroke is proportional
1. How to turn non-recoverers into (proportional) recoverers?
2. How to improve on regaining 70% of what is lost?
2
1
pred
icte
d ch
ange
observed change Winters et al., NNR (2015)
mild
severe
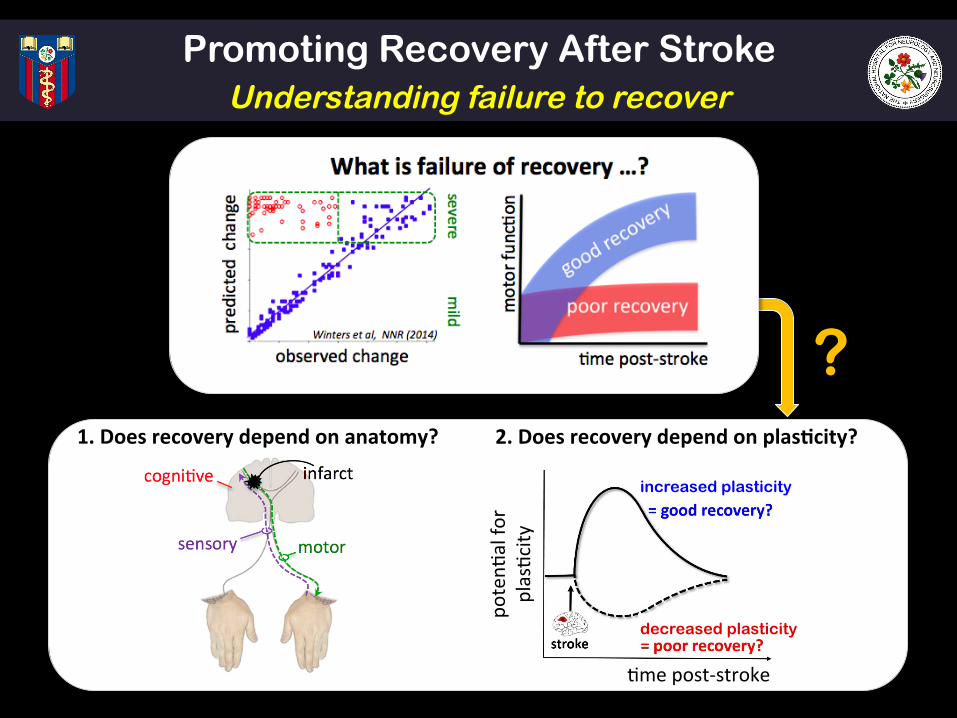
? 1.Doesrecoverydependonanatomy?
r2 = 0
2.Doesrecoverydependonplas5city?
$mepost-stroke
poten$
alfo
rplas$city
increased plasticity
decreased plasticity
Promoting Recovery After Stroke Understanding failure to recover
PART 1 – SUMMARY • Stroke is huge burden
• Early post-stroke plasticity = optimism?
• Need to understand post-stroke plasticity in humans
Promoting Recovery After Stroke Recovery after stroke - reason for optimism
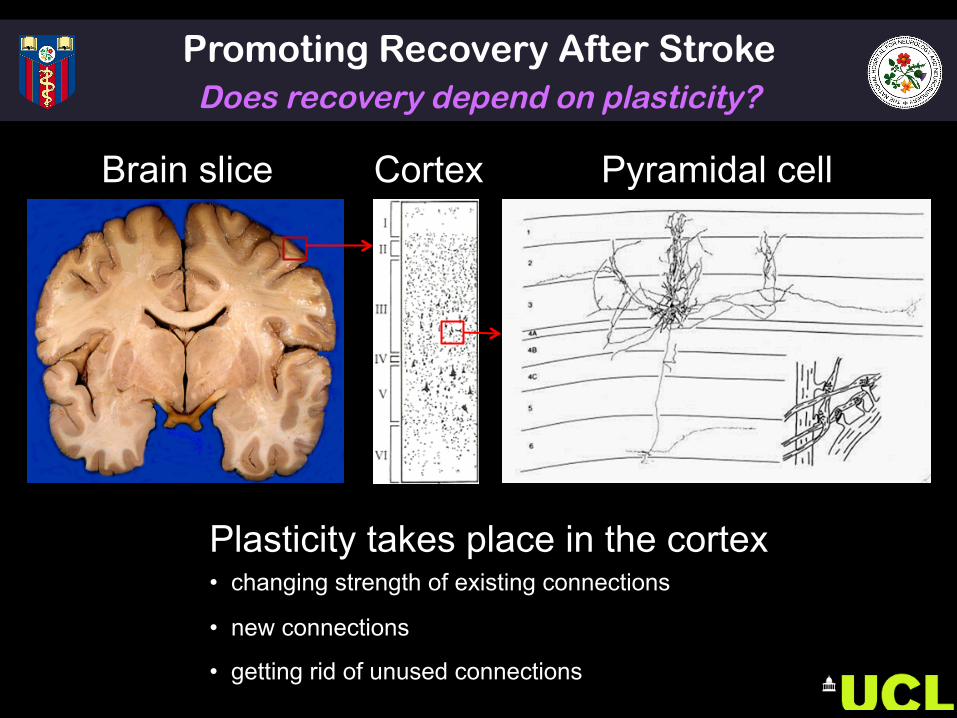
Brain slice
Plasticity takes place in the cortex • changing strength of existing connections • new connections
• getting rid of unused connections
Cortex Pyramidal cell
Promoting Recovery After Stroke Does recovery depend on plasticity?

A
B infarct 3 months
post stroke 17 days
post stroke 24 days
post stroke 31 days
post stroke 10 days
post stroke
affected side
affected side
Promoting Recovery After Stroke Brain system reorganisation after stroke
NS Ward Curr Opin Neurol. 2015; 28: 323-9
Promoting Recovery After Stroke Post-stroke plasticity – window of opportunity
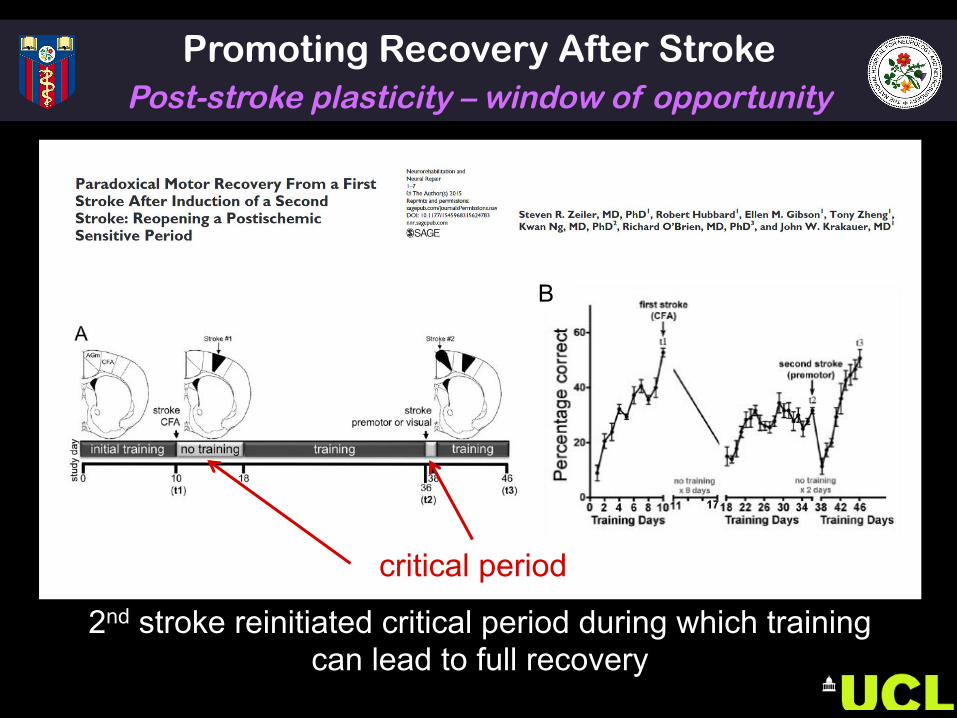
2nd stroke reinitiated critical period during which training can lead to full recovery
B
critical period
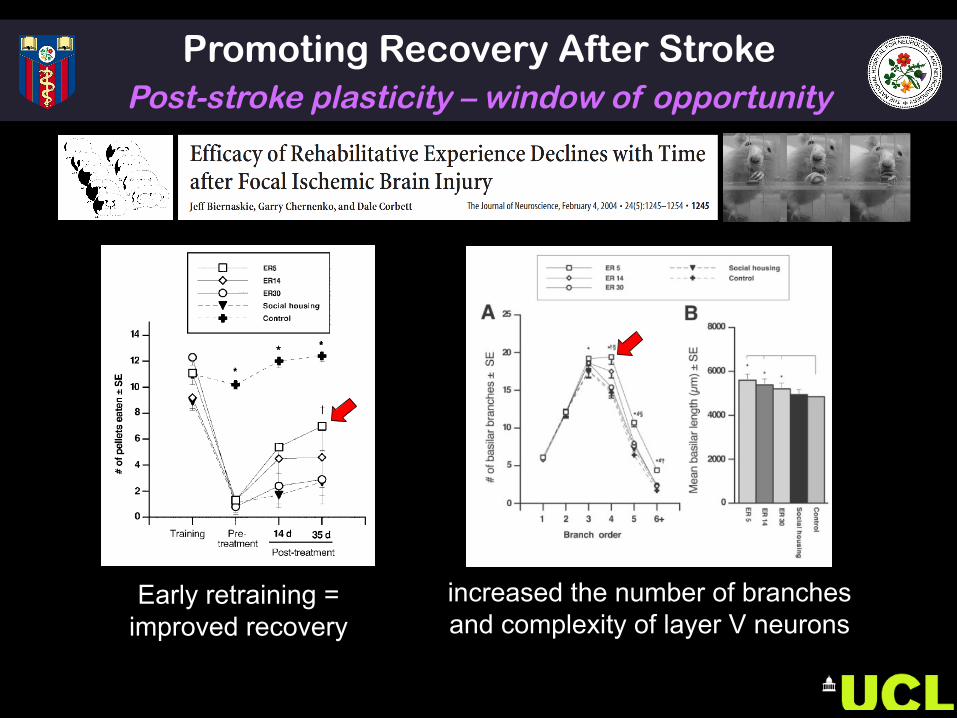
Early retraining = improved recovery
increased the number of branches and complexity of layer V neurons
Promoting Recovery After Stroke Post-stroke plasticity – window of opportunity
‘SPONTANEOUS BIOLOGICAL RECOVERY’ 1. A window of opportunity after focal brain damage within
which behavioural training will have a much greater impact than outside the window
2. A rapid generalised improvement in impairment that is in contrast to modest gains made in the chronic phase
So …… what creates this unique plasticity environment?
Promoting Recovery After Stroke Post-stroke plasticity – window of opportunity
Promoting Recovery After Stroke Early post-stroke changes to support plasticity?
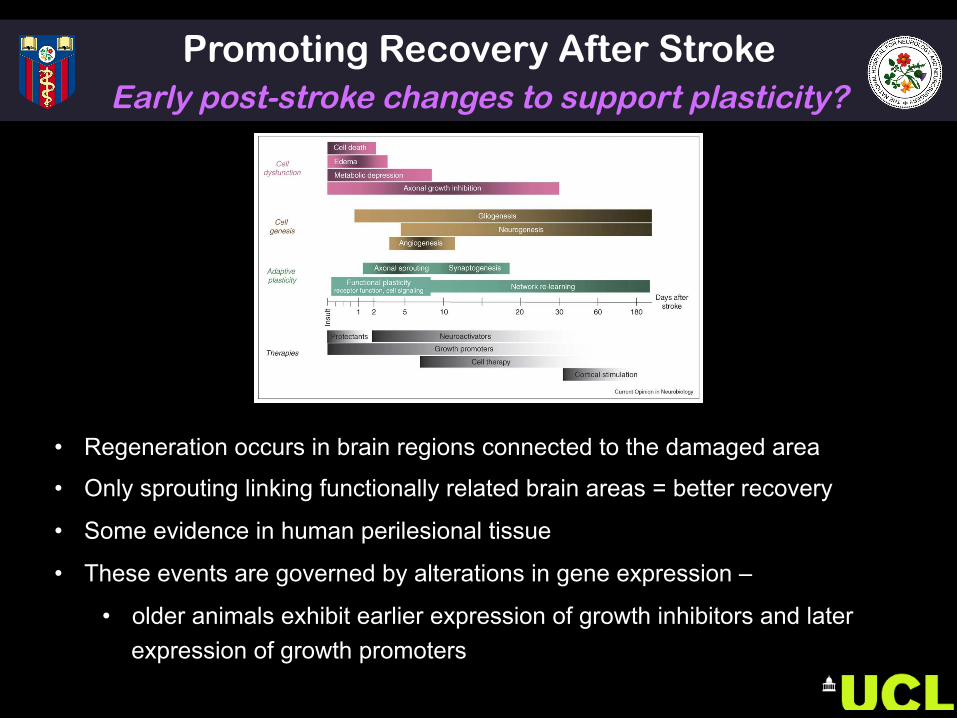
• Regeneration occurs in brain regions connected to the damaged area
• Only sprouting linking functionally related brain areas = better recovery
• Some evidence in human perilesional tissue
• These events are governed by alterations in gene expression –
• older animals exhibit earlier expression of growth inhibitors and later expression of growth promoters
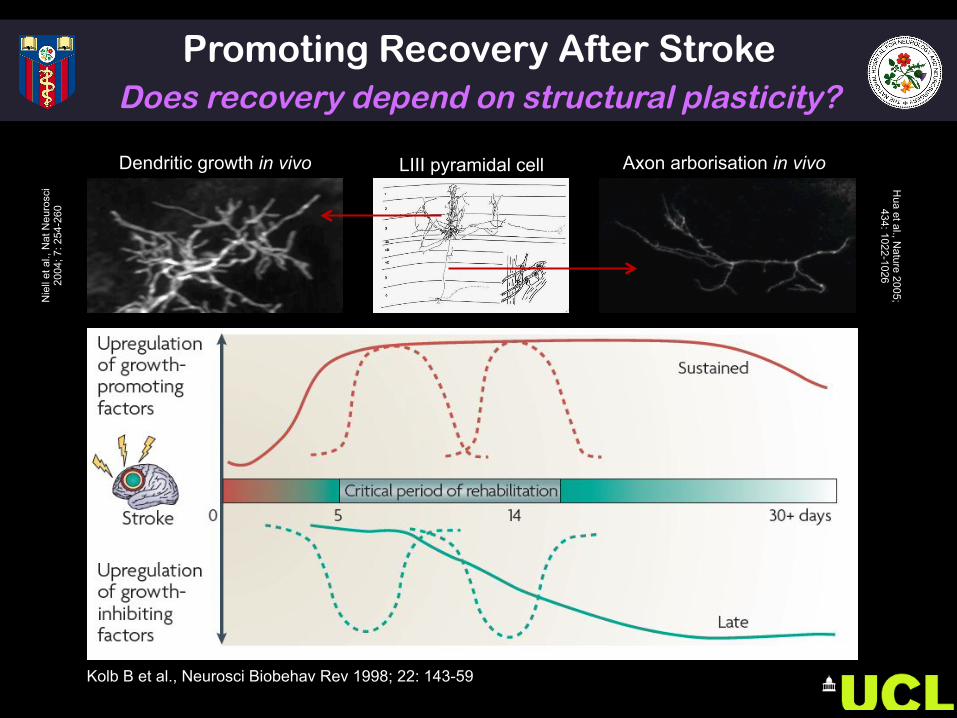
Kolb B et al., Neurosci Biobehav Rev 1998; 22: 143-59
Dendritic growth in vivo
Nie
ll et
al.,
Nat
Neu
rosc
i 20
04; 7
: 254
-260
Axon arborisation in vivo
Hua et al., N
ature 2005; 434: 1022-1026
LIII pyramidal cell
Promoting Recovery After Stroke Does recovery depend on structural plasticity?
Molecules that inhibit neuronal growth • Myelin Associated Proteins (Nogo-A, MAG, OMAP)
o Anti-Nogo A • Extracellular matrix proteins (chondroitin sulphate proteoglycans)
o Chondroitinase • Growth Cone Inhibitors (semaphorins, ephrins)
o Ephrin-A5 blockers
Promoting Neuronal regeneration • Inosine • GDF10
Stem cells, granulocyte-colony stimulating factor (G-CSF) Role of glial cells, inflammatory response?
Promoting Recovery After Stroke Can structural plasticity be manipulated?
Promoting Recovery After Stroke Does recovery depend on structural plasticity?
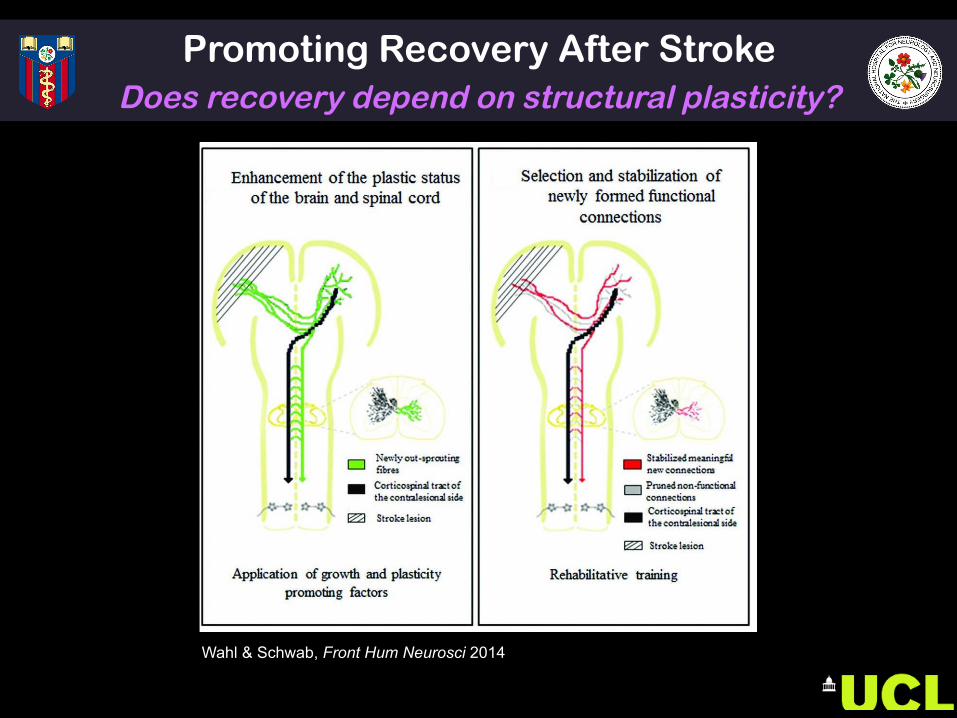
Wahl & Schwab, Front Hum Neurosci 2014
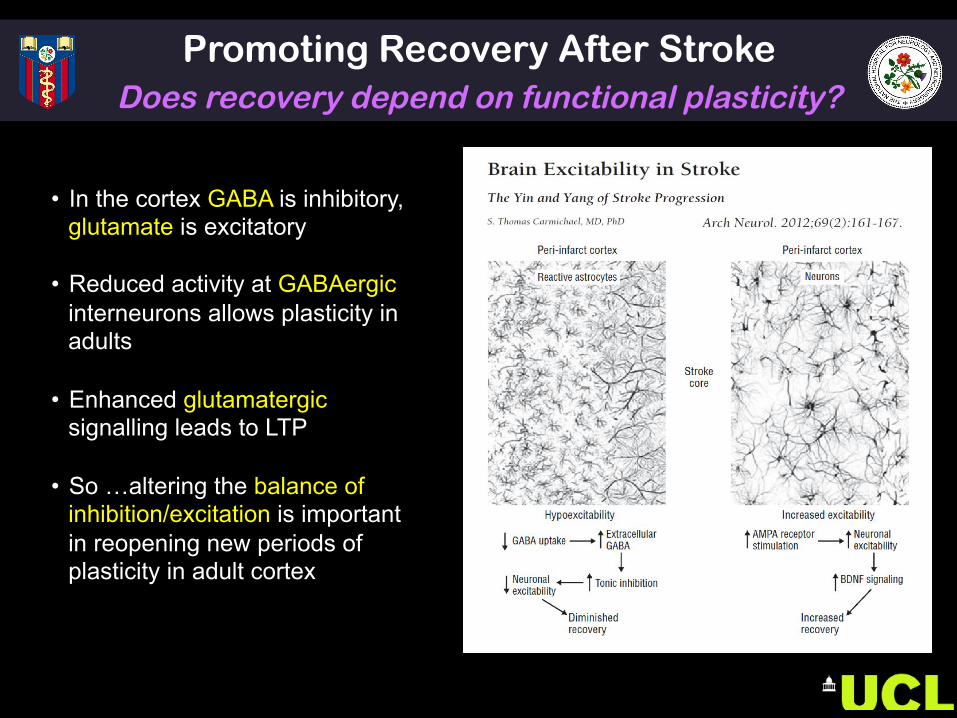
• In the cortex GABA is inhibitory, glutamate is excitatory
• Reduced activity at GABAergic interneurons allows plasticity in adults
• Enhanced glutamatergic signalling leads to LTP
• So …altering the balance of inhibition/excitation is important in reopening new periods of plasticity in adult cortex
Promoting Recovery After Stroke Does recovery depend on functional plasticity?
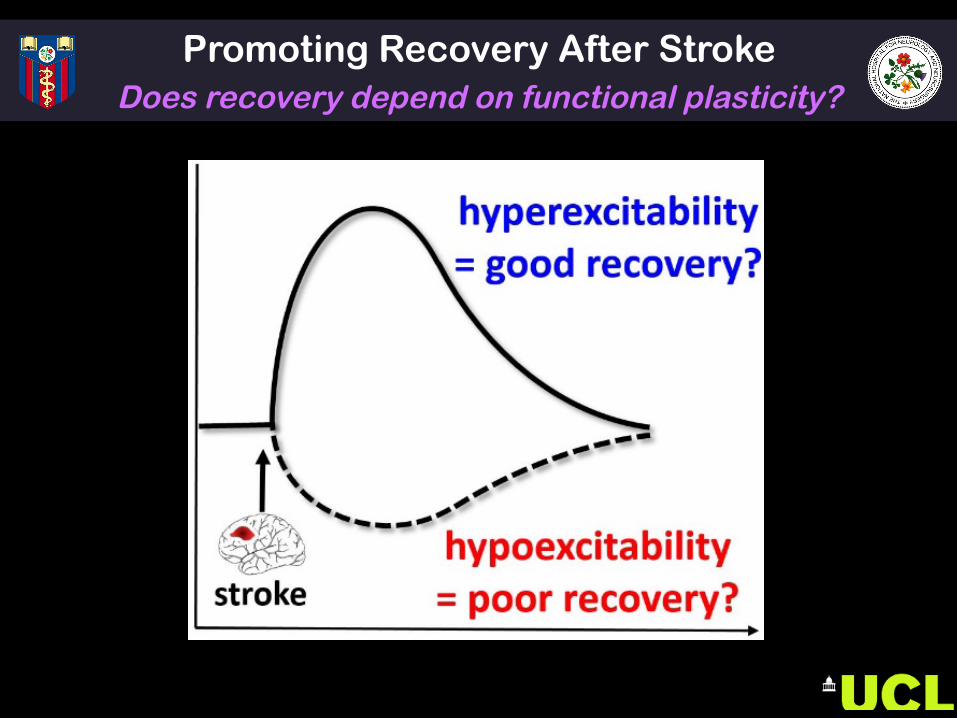
Promoting Recovery After Stroke Does recovery depend on functional plasticity?
$mepost-stroke
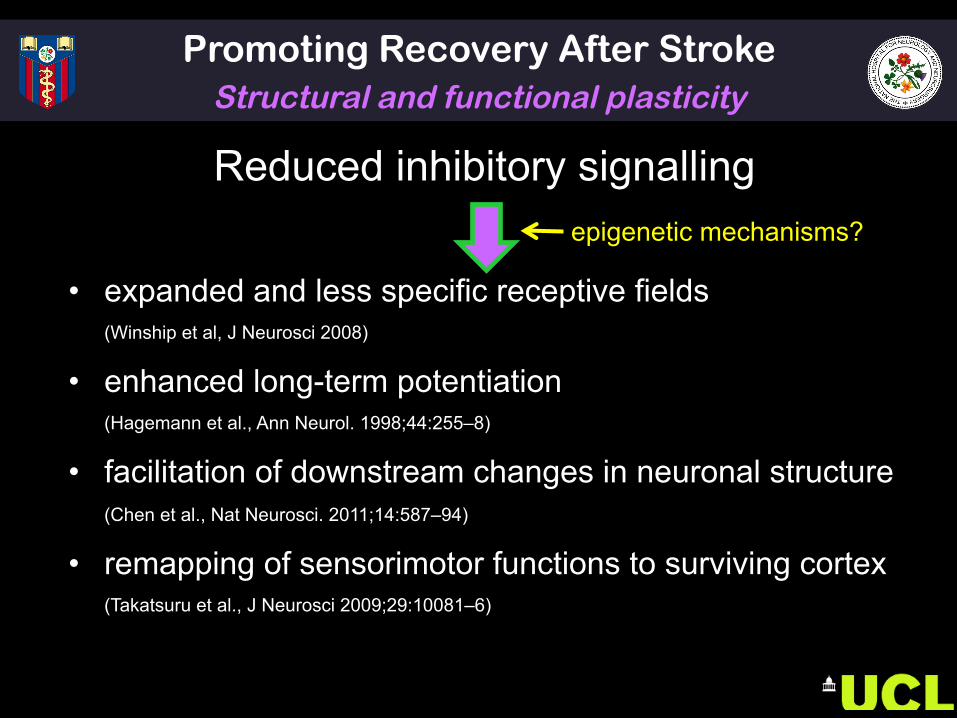
Promoting Recovery After Stroke Structural and functional plasticity
Reduced inhibitory signalling
• expanded and less specific receptive fields (Winship et al, J Neurosci 2008)
• enhanced long-term potentiation (Hagemann et al., Ann Neurol. 1998;44:255–8)
• facilitation of downstream changes in neuronal structure
(Chen et al., Nat Neurosci. 2011;14:587–94)
• remapping of sensorimotor functions to surviving cortex
(Takatsuru et al., J Neurosci 2009;29:10081–6)
epigenetic mechanisms?
PART 2 – SUMMARY • Spontaneous biological recovery is clear
phenomenon in animal models of stroke
• Recovery can be supported by structural and functional plasticity
• Does SBR occur in humans?
Promoting Recovery After Stroke Enhancing use-dependent plasticity
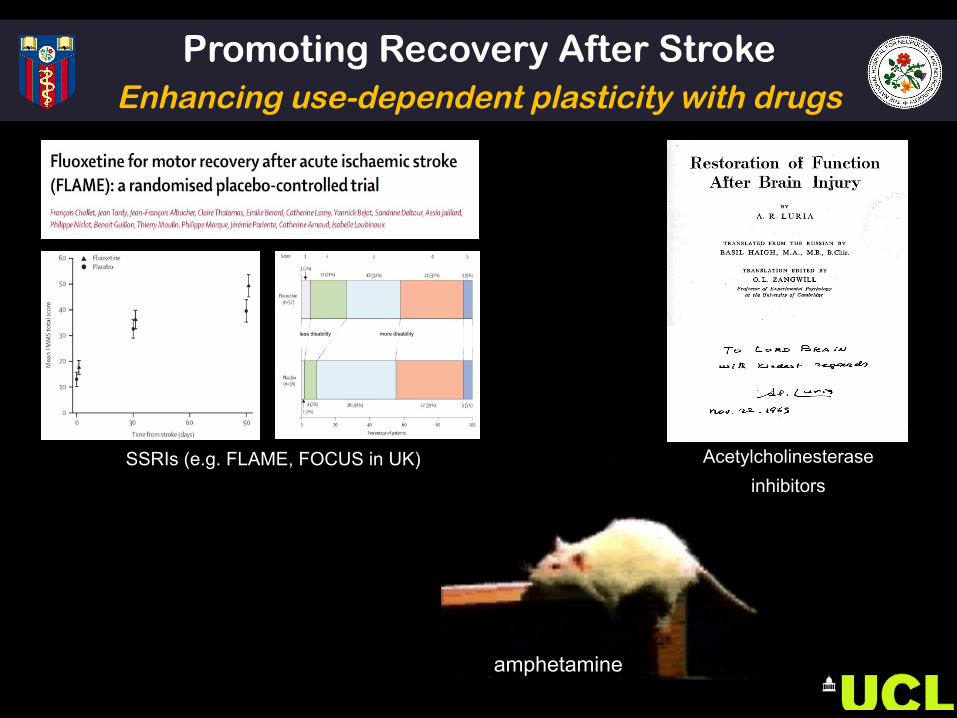
amphetamine
less disability more disability
SSRIs (e.g. FLAME, FOCUS in UK) Acetylcholinesterase inhibitors
Promoting Recovery After Stroke Enhancing use-dependent plasticity with drugs
Promoting Recovery After Stroke Enhancing use-dependent plasticity with drugs
• Functional inhibition of intact neurons after focal damage causes symptoms
• “removal of the diaschisis, restoration of synaptic conduction or to use another term, de-blocking” of intact neurons with anticholinesterases might be helpful.
• Behavioural training promotes ‘de-blocking’, the essence of which is “that by means of various methods the level of excitability in certain functional systems is raised and the corresponding functions are ‘de-inhibited’”
Promoting Recovery After Stroke Enhancing use-dependent plasticity with drugs
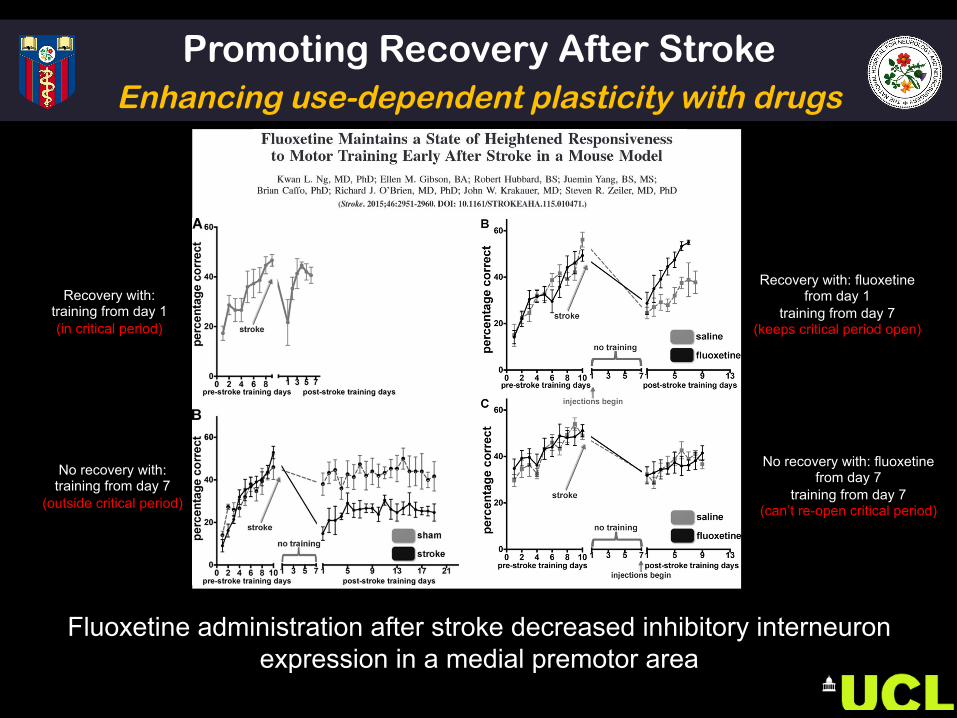
Recovery with: training from day 1 (in critical period)
No recovery with: training from day 7
(outside critical period)
Recovery with: fluoxetine from day 1
training from day 7 (keeps critical period open)
No recovery with: fluoxetine from day 7
training from day 7 (can’t re-open critical period)
Fluoxetine administration after stroke decreased inhibitory interneuron expression in a medial premotor area
Promoting Recovery After Stroke Enhancing use-dependent plasticity with drugs
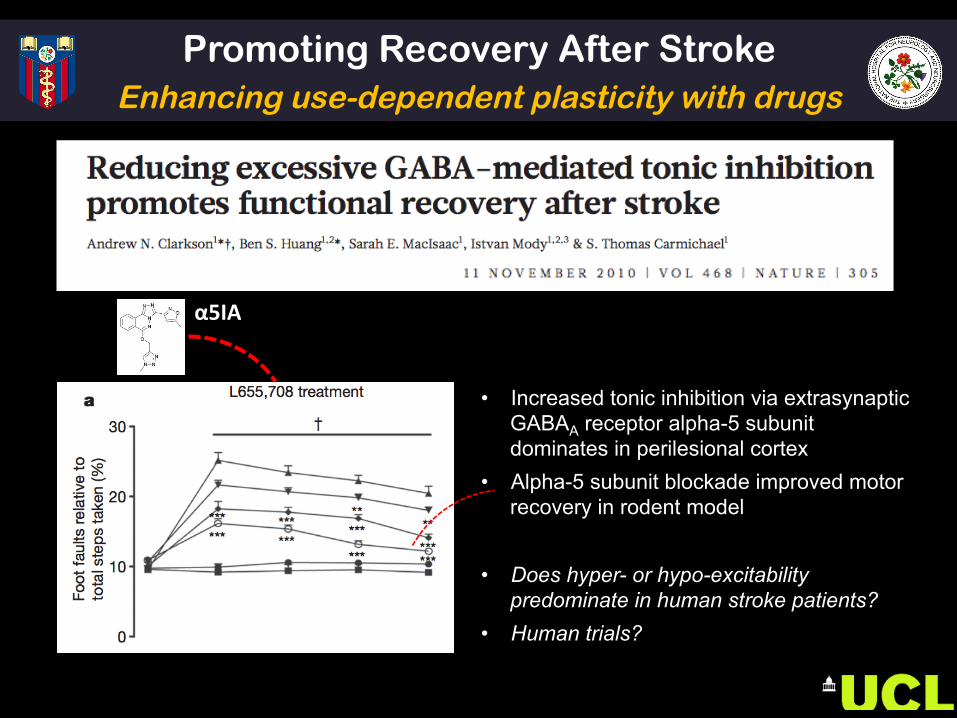
• Increased tonic inhibition via extrasynaptic GABAA receptor alpha-5 subunit dominates in perilesional cortex
• Alpha-5 subunit blockade improved motor recovery in rodent model
• Does hyper- or hypo-excitability
predominate in human stroke patients? • Human trials?
α5IA
Promoting Recovery After Stroke Enhancing use-dependent plasticity with NIBS
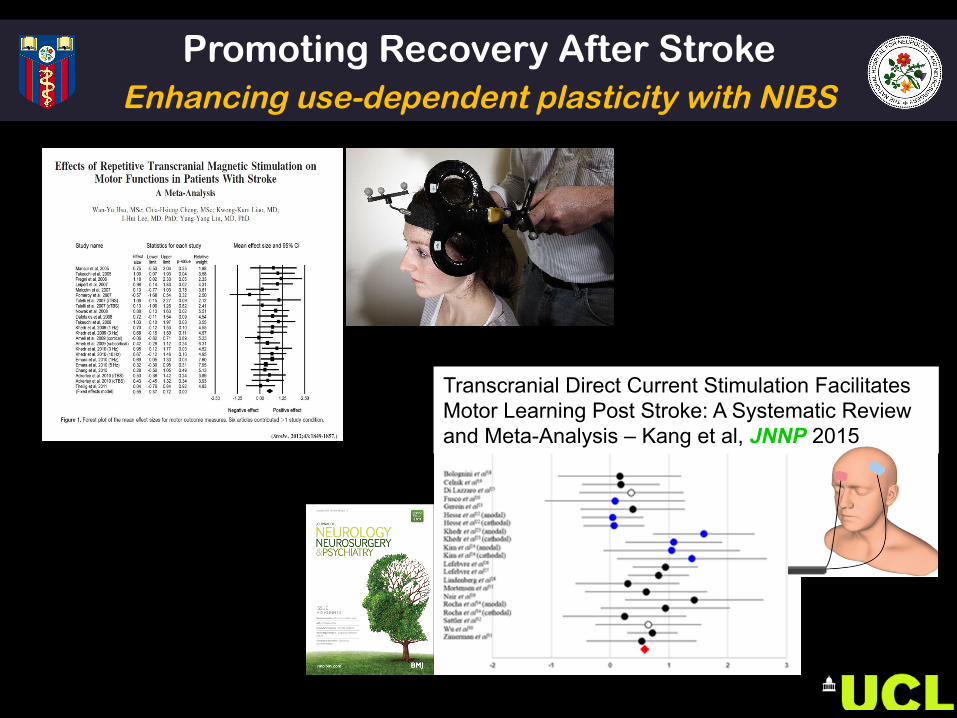
Transcranial Direct Current Stimulation Facilitates Motor Learning Post Stroke: A Systematic Review and Meta-Analysis – Kang et al, JNNP 2015
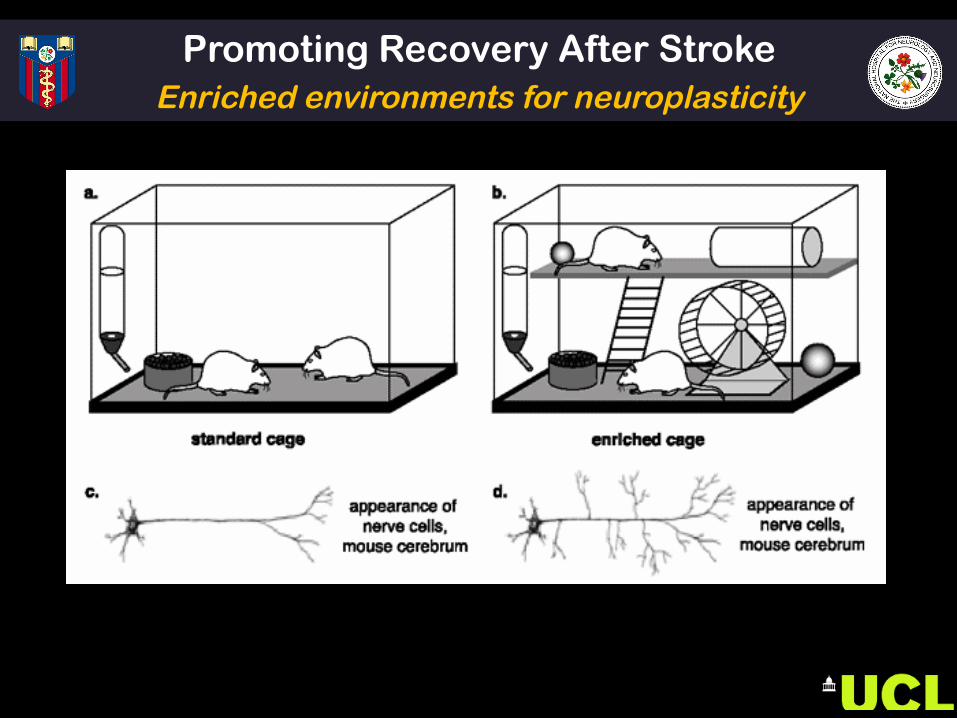
Promoting Recovery After Stroke Enriched environments for neuroplasticity
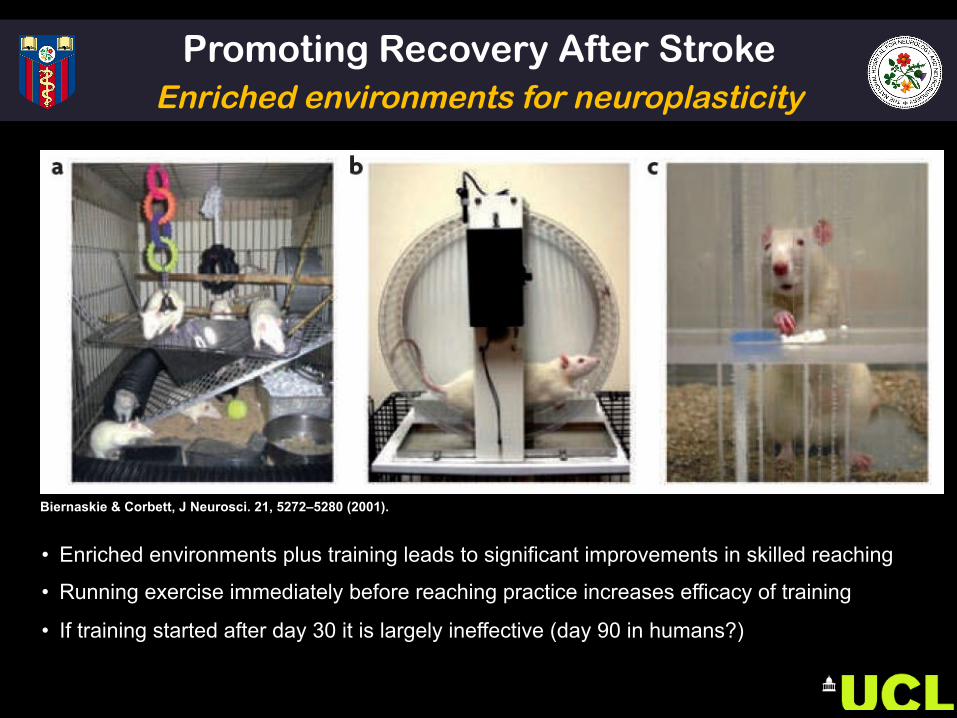
Biernaskie & Corbett, J Neurosci. 21, 5272–5280 (2001).
Promoting Recovery After Stroke Enriched environments for neuroplasticity
• Enriched environments plus training leads to significant improvements in skilled reaching
• Running exercise immediately before reaching practice increases efficacy of training
• If training started after day 30 it is largely ineffective (day 90 in humans?)
Promoting Recovery After Stroke Exercise/priming for neuroplasticity
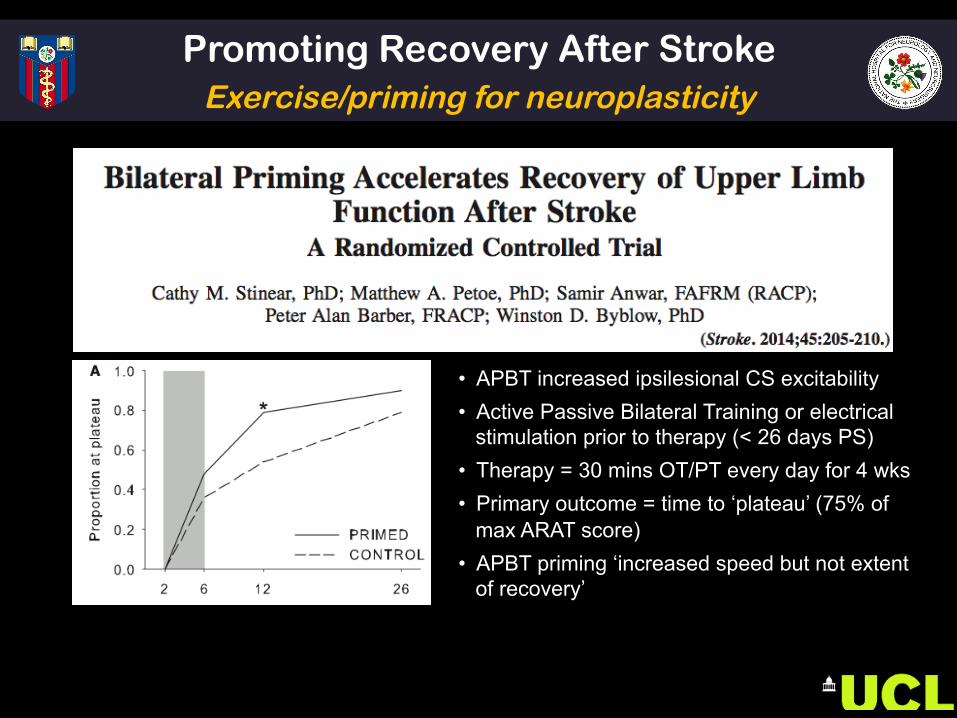
• APBT increased ipsilesional CS excitability • Active Passive Bilateral Training or electrical
stimulation prior to therapy (< 26 days PS) • Therapy = 30 mins OT/PT every day for 4 wks • Primary outcome = time to ‘plateau’ (75% of
max ARAT score) • APBT priming ‘increased speed but not extent
of recovery’
PART 3 – SUMMARY • Priming the brain to be more responsive is an option • Drugs available to manipulate excitation/inhibition in
humans now!
• NIBS could play a role but needs dose control
• Early vs Late? Not clear when to give or who to give them to
Promoting Recovery After Stroke Enhancing use-dependent plasticity
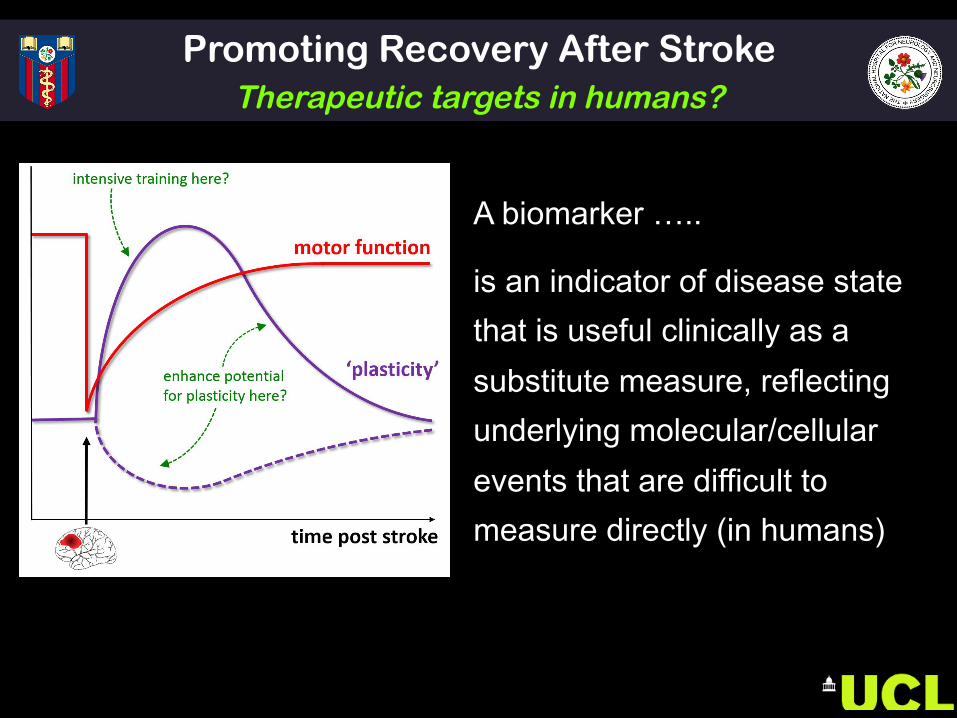
Promoting Recovery After Stroke Therapeutic targets in humans?
A biomarker …..
is an indicator of disease state that is useful clinically as a substitute measure, reflecting underlying molecular/cellular events that are difficult to measure directly (in humans)
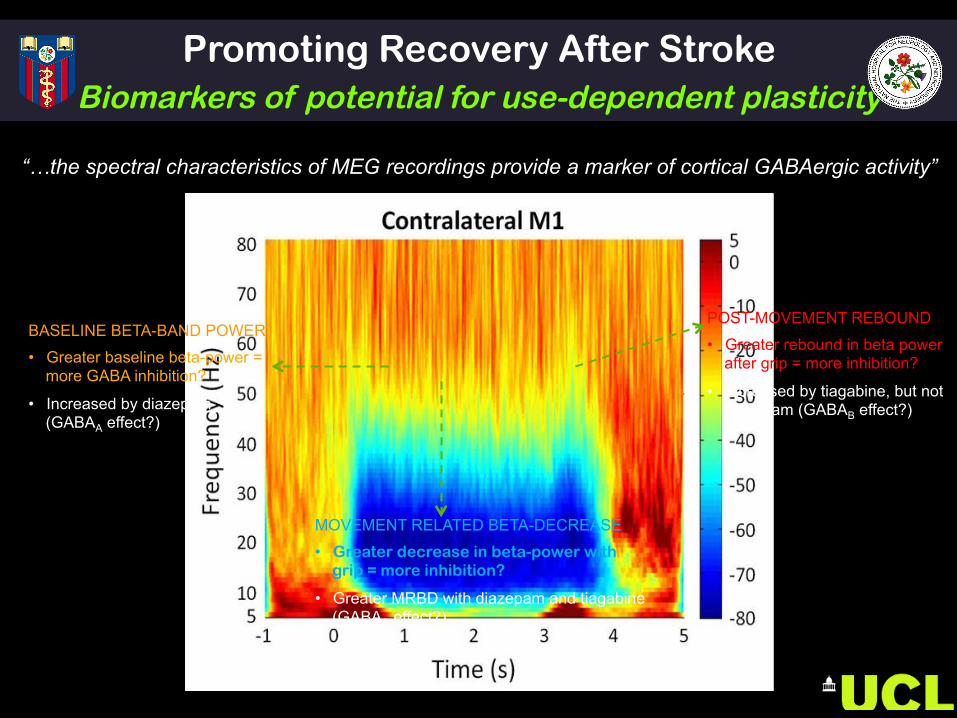
“…the spectral characteristics of MEG recordings provide a marker of cortical GABAergic activity”
Promoting Recovery After Stroke Biomarkers of potential for use-dependent plasticity
BASELINE BETA-BAND POWER
• Greater baseline beta-power = more GABA inhibition?
• Increased by diazepam (GABAA effect?)
POST-MOVEMENT REBOUND
• Greater rebound in beta power after grip = more inhibition?
• Increased by tiagabine, but not diazepam (GABAB effect?)
MOVEMENT RELATED BETA-DECREASE
• Greater decrease in beta-power with grip = more inhibition?
• Greater MRBD with diazepam and tiagabine (GABAA effect?)
Imaging Biomarkers in Neurorehabilitation Biomarkers of potential for plasticity
• Stroke patients with poorer outcomes have increased low-frequency oscillations, (Laaksonen et al. 2013)
• similar to those caused by benzodiazepines (GABAA-agonist - phasic) and tiagabine (GABA re-uptake inhibitor – tonic) suggesting predominant inhibitory mechanisms in peri-lesional cortex?
• Reversing increased peri-lesional beta oscillations ‘paradoxically’ with zolpidem leads to clinical improvement (single stroke patient) (Hall et al. 2010)
• Early post-stroke - less beta-rebound in response to tactile finger stimulation (increased sensorimotor excitability) (Laaksonen et al. 2013) and sensory map size predict good recovery (Roiha et al. 2011)
“…the spectral characteristics of MEG recordings provide a marker of cortical GABAergic activity”
Whatfactorsaccountforrecoverya0erstroke?
Rossiter H, …, Ward NS. J Neurophys (2014)
Ward NS. Brain (2016)
NS Ward Curr Opin Neurol 28: 323-9 (2015)
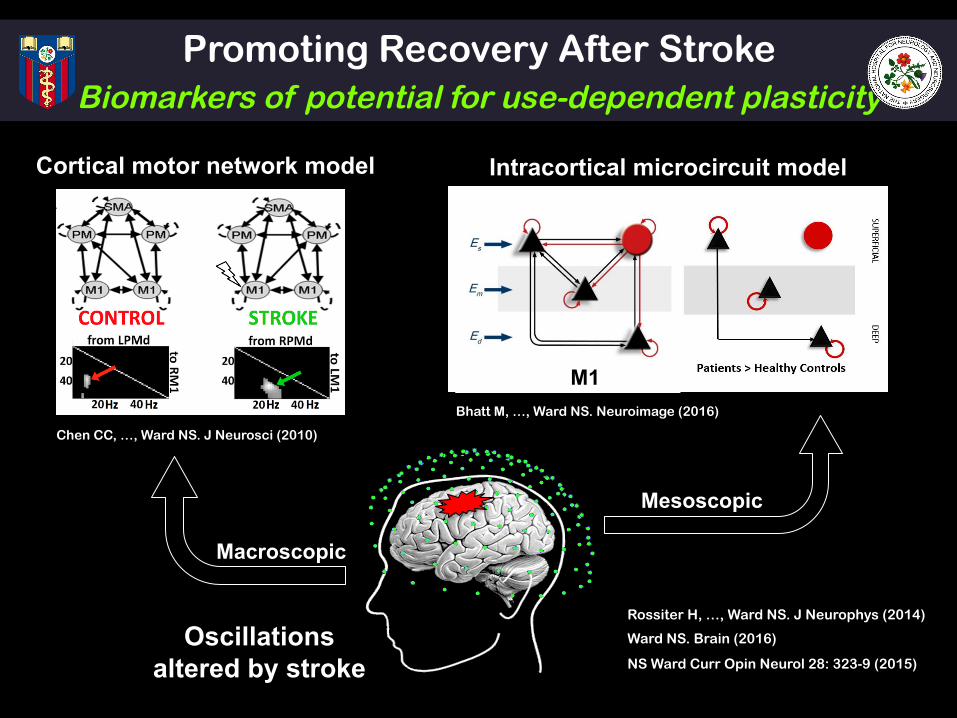
Oscillations altered by stroke
Promoting Recovery After Stroke Biomarkers of potential for use-dependent plasticity
Cortical motor network model
Chen CC, …, Ward NS. J Neurosci (2010)
Intracortical microcircuit model
Bhatt M, …, Ward NS. Neuroimage (2016)
Macroscopic
Mesoscopic
M1
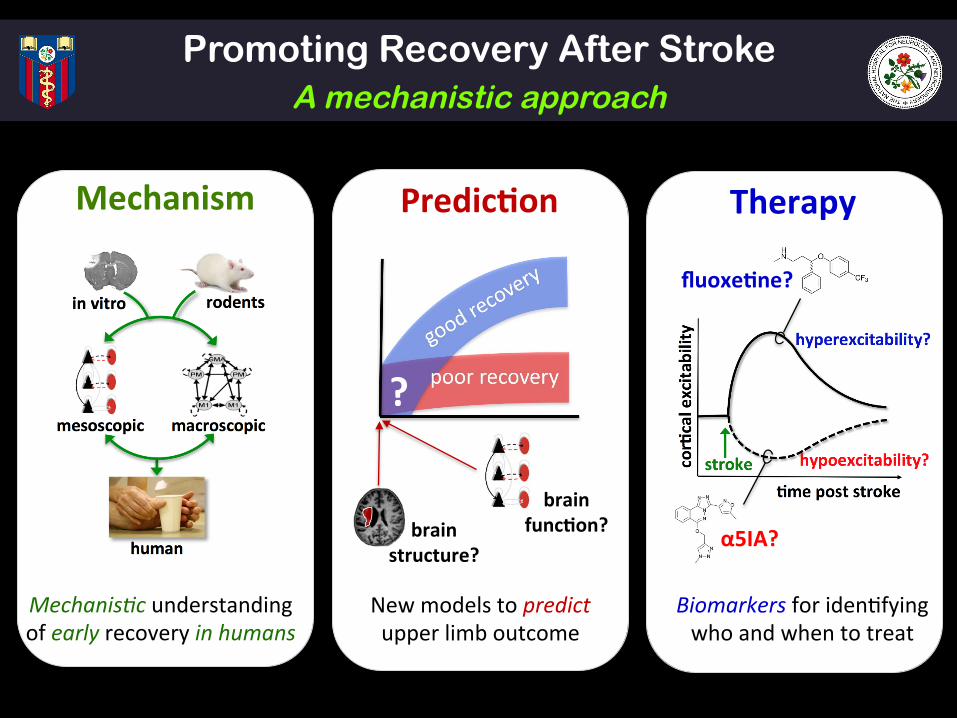
Predic5on TherapyMechanism
Mechanis)cunderstandingofearlyrecoveryinhumans
Biomarkersforiden$fyingwhoandwhentotreat
Newmodelstopredictupperlimboutcome
fluoxe5ne?
α5IA?
Newknowledgetochangeclinicalprac:ce
brainstructure?
brainfunc5on?
?
Promoting Recovery After Stroke A mechanistic approach
1. Spontaneous biological recovery provides cause for optimism
2. Should tell us when to delivery intense impairment based rehabilitation
3. There are clear lesion induced changes in structure that can support recovery – anti NoGo, inosine, GDF10, stem cells
4. Pushing inhibitory/excitatory balance away from inhibition opens door to structural plasticity
5. Need biomarkers of these processes in humans so we know what to target - drugs available now!
6. Too early for phase III trials - Understanding the mechanisms involved first (or at least in parallel) is crucial (funders please note!)
Promoting Recovery After Stroke Summary
FIL:
Karl Friston
Rosalyn Moran
Gareth Barnes
Richard Frackowiak
Will Penny
Jennie Newton
SOBELL DEPARTMENT :
Holly Rossiter
Muddy Bhatt
Stephanie Bowen
Ella Clark
Svenja Espenhahn
Chang-hyun Park
Sven Bestman
John Rothwell
Penny Talelli
Acknowledgements ABIU/NRU:
Fran Brander
Kate Kelly
Diane Playford
Alan Thompson
FUNDING:
Promoting Recovery After Stroke
Slides at www.ucl.ac.uk/ion/departments/sobell/Research/NWard
1. Murphy TH, Corbett D. Plasticity during stroke recovery: from synapse to behaviour. Nat Rev Neurosci 2009;10:861-72.
2. Carmichael ST. Targets for neural repair therapies after stroke. Stroke 2010;41(10 Suppl):S124-6
3. Philips JP, Devier DJ, Feeney DM. Rehabilitation pharmacology: bridging laboratory work to clinical application. J Head Trauma Rehabil 2003 Jul-Aug;18(4):342-56.
4. Stagg CJ, Nitsche MA. Physiological basis of transcranial direct current stimulation. Neuroscientist 2011;17:37-53
5. Stinear CM, Ward NS. How useful is imaging in predicting outcomes in stroke rehabilitation? Int J Stroke. 2013;8(1):33-7.
6. Ward NS. Assessment of cortical reorganisation for hand function after stroke. J Physiol. 2011;589(Pt 23):5625-32.
Promoting Recovery After Stroke Why do only some stroke survivors recover?