hospicesocialwork:linkingpolicy, practice,andresearch · hospice is an increasingly prevalent...
TRANSCRIPT
HOSPICE SOCIAL WORK: LINKING POLICY,PRACTICE, AND RESEARCH
A REPORT FROM THE MARCH 25, 2010SYMPOSIUM
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:32 PM Page 2
©2010 National Association of Social Workers. All Rights Reserved.
About the Symposium ..............................................................
About Hospice ..........................................................................What is Hospice Social Work? ..................................................Current Status of Hospice Social Work Research ......................Federal Rules and Priorities ......................................................
Accreditation and Professional Standards for Practice of Hospic
Conclusions ..............................................................................Social Workers’ Roles in Hospice Care ........................Research and Hospice Social Work ..............................Hospice Social Work/Policy Connections ....................
Recommendations for Action ....................................................To Advance the Role of Hospice Social Work and AddrTo Enhance Diversity in Hospice Services ....................To Promote Interdisciplinary Team Functioning ..........To Promote Research-Practice Linkages ......................To Promote Research on Hospice Social Work ............To Promote Collaborations with Federal Agencies ......
References ................................................................................
Appendix ..................................................................................
Recommended Citation – Social Work Policy Institute (2010). Hospice Social Work: Linking
Policy, Practice and Research, Washington, DC: National Association of Social Workers.
TABLE OF CONTENTS
This report is the product from the Symposium, Hospice Social Work: Linking Policy Practiceand Research, hosted by the Social Work Policy Institute on March 25, 2010. Copies can bedownloaded from the Institute’s website at SocialWorkPolicy.org.
For more information contact:
Joan Levy Zlotnik, PhD, ACSWDirectorSocial Work Policy Institute750 First Street, NE, Suite 700Washington, DC [email protected]
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:32 PM Page 3
Association of Social Workers. All Rights Reserved.
About the Symposium ..........................................................................................................................1
About Hospice ......................................................................................................................................2What is Hospice Social Work? ..............................................................................................................4Current Status of Hospice Social Work Research ..................................................................................6Federal Rules and Priorities ................................................................................................................10
Accreditation and Professional Standards for Practice of Hospice Care ..............................................12
Conclusions ........................................................................................................................................13Social Workers’ Roles in Hospice Care ..................................................................................13Research and Hospice Social Work ........................................................................................15Hospice Social Work/Policy Connections ..............................................................................16
Recommendations for Action ..............................................................................................................18To Advance the Role of Hospice Social Work and Address Practice Issues ............................18To Enhance Diversity in Hospice Services ..............................................................................19To Promote Interdisciplinary Team Functioning ....................................................................20To Promote Research-Practice Linkages ................................................................................21To Promote Research on Hospice Social Work ......................................................................21To Promote Collaborations with Federal Agencies ................................................................22
References ..........................................................................................................................................23
Appendix ............................................................................................................................................24
l Work Policy Institute (2010). Hospice Social Work: Linking
Washington, DC: National Association of Social Workers.
TABLE OF CONTENTS
he Symposium, Hospice Social Work: Linking Policy Practicecial Work Policy Institute on March 25, 2010. Copies can bewebsite at SocialWorkPolicy.org.
W
00
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:32 PM Page 4
Appendix B) included expert presentations (see Appendix C)the presentations, the participants engaged in roundtable delihospice psychosocial research, emerging practices in end-of-lirole on the interdisciplinary team, and strengthening researchDrawing from the presentations and discussions, recommendchallenges identified in regard to research, practice, policy an
The symposium was particularly timely since the Conditionsminimum federal standards for hospice services were compreMedicare and Medicaid Services (CMS) in 2008 and are nowrevised standards could both serve as input to the symposiumrecommendations that emerged from the meeting. In additionactivities, plans were underway for the NASW 2010 AnnualCritical Role in End of Life Care (www.socialworkers.org/nadefault.asp) to be held August 3-4, 2010 in Boston, MA. Theshape the agenda for that conference. In addition, the sympoconnections between the social work community and CMS bsocial work practice and increasing social work’s awareness oits priorities regarding quality improvement.
Planning for the symposium occurred in partnership with theCare Organization (NHPCO), a provider organization with wcollaborative initiatives.
In advance of the symposium, the Social Work Policy Instituthospice legislation, standards and credentials, continuing eduactivities of national organizations involved with hospice, anresearch and researchers. This information helped to inform tincluded in the Appendix of this report.
ABOUT HOSPICEHospice services help patients and their families deal with theinclude palliative care and comfort services as well as follow-bereavement. One of the unique qualities of hospice servicesservices with the patient’s loved ones after the patient’s death
Hospice services may take place in the patient’s own home, inincreasingly as an adjunct to nursing home, hospital and assi
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
ABOUT THE SYMPOSIUMHospice is an increasingly prevalent service to provide end-of-life care that addresses both qualityof care and quality of life and focuses on meeting psychosocial needs for both the patient and theirloved ones. Since the inception of hospice care, social workers have served as key members of thehospice interdisciplinary care team.
In March 2010, to more fully explore the connections between quality hospice social workservices, the mission of hospice, federal requirements, professional standards, and the current stateof hospice research by social workers, a think tank meeting was convened by the Social WorkPolicy Institute (SWPI) of the National Association of Social Workers (NASW) Foundation. Thesymposium, Hospice Social Work: Linking Policy, Practice, and Research brought togetherpractitioners, administrators, regulators, researchers, policy-makers and national leaders. The goalof the symposium was to explore:
• Social work’s contribution and challenges in building comprehensive community-basedend-of-life care,
• Research on hospice social workers’ roles and intervention practices,
• Regulations for hospice and hospice social workers, and
• Promotion of high quality psychosocial care in hospice.
The think tank participants (see Appendix A) included representatives from social work researchand practice and key stakeholders representing hospice programs, federal research and regulatoryagencies, national organizations and foundations. The anticipated outcome was the developmentof a set of action steps to enhance the state of hospice social work. The symposium agenda (see
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 1
HOSPICE SOCIAL WORK: LINKINGPOLICY, PRACTICE AND RESEARCH
Hospice History
The term, “hospice” originates from the Latin word “hospitium” or guesthouse. It described a house provided for sick persons returningfrom pilgrimages. The first modern hospice movement, which used a team approach to professionally administer pain management andcompassionate caregiving to the dying, was founded near London in the 1960s by Cicely Saunders, a British social worker, nurse andphysician. Hospice care arrived in America in 1974, with the first center opening in New Haven, Connecticut (HFA, n.d.; Cicely SaundersFoundation, 2010).
Hospice FactsSource: National Hospice and Palliative Care Organization, 2009
• There are currently more than 4,850 hospice programs in the United States that• It is estimated that about 38.5% of deaths are under hospice care.• Just under half of hospice care organizations are for-profit (46%), half are non-p
U.S. Department of Veterans Affairs).• Nearly all hospice care is paid for through the Medicare or Medicaid Hospice Ben• Social workers have an average caseload of 24.2 patients; nurses have on avera
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:32 PM Page 1

Appendix B) included expert presentations (see Appendix C) and facilitated discussions. Followingthe presentations, the participants engaged in roundtable deliberations on the current status ofhospice psychosocial research, emerging practices in end-of-life care, enhancing the social worker’srole on the interdisciplinary team, and strengthening researcher/practitioner/policy connections.Drawing from the presentations and discussions, recommendations were developed to address thechallenges identified in regard to research, practice, policy and professional development.
The symposium was particularly timely since the Conditions of Participation (CoP) that set theminimum federal standards for hospice services were comprehensively revised by the Centers forMedicare and Medicaid Services (CMS) in 2008 and are now being implemented. Thus, therevised standards could both serve as input to the symposium deliberations and be a catalyst forrecommendations that emerged from the meeting. In addition, among NASW’s hospice-focusedactivities, plans were underway for the NASW 2010 Annual Practice Conference, Social Work’sCritical Role in End of Life Care (www.socialworkers.org/nasw/conferences/boston2010/default.asp) to be held August 3-4, 2010 in Boston, MA. The symposium outcomes could helpshape the agenda for that conference. In addition, the symposium helped to strengthen theconnections between the social work community and CMS by enhancing CMS’s knowledge ofsocial work practice and increasing social work’s awareness of CMS’s rule-making procedures andits priorities regarding quality improvement.
Planning for the symposium occurred in partnership with the National Hospice and PalliativeCare Organization (NHPCO), a provider organization with which NASW has severalcollaborative initiatives.
In advance of the symposium, the Social Work Policy Institute pulled together information onhospice legislation, standards and credentials, continuing education opportunities, the roles andactivities of national organizations involved with hospice, and hospice relevant social workresearch and researchers. This information helped to inform the agenda for the meeting and isincluded in the Appendix of this report.
ABOUT HOSPICEHospice services help patients and their families deal with the complexity of end of life andinclude palliative care and comfort services as well as follow-up support to deal with grief andbereavement. One of the unique qualities of hospice services is that follow-up bereavementservices with the patient’s loved ones after the patient’s death is a core service that is offered.
Hospice services may take place in the patient’s own home, in residential hospice programs, andincreasingly as an adjunct to nursing home, hospital and assisted living services. Hospice services
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 2
Mervice to provide end-of-life care that addresses both qualityon meeting psychosocial needs for both the patient and theirpice care, social workers have served as key members of the
the connections between quality hospice social workal requirements, professional standards, and the current statea think tank meeting was convened by the Social Workl Association of Social Workers (NASW) Foundation. Thenking Policy, Practice, and Research brought togetherrs, researchers, policy-makers and national leaders. The goal
d challenges in building comprehensive community-based
rkers’ roles and intervention practices,
ospice social workers, and
chosocial care in hospice.
ndix A) included representatives from social work researchresenting hospice programs, federal research and regulatoryoundations. The anticipated outcome was the developmentstate of hospice social work. The symposium agenda (see
NKING POLICY, PRACTICE, AND RESEARCH REPORT
1
CIAL WORK: LINKINGCTICE AND RESEARCH
“hospitium” or guesthouse. It described a house provided for sick persons returningent, which used a team approach to professionally administer pain management andd near London in the 1960s by Cicely Saunders, a British social worker, nurse andwith the first center opening in New Haven, Connecticut (HFA, n.d.; Cicely Saunders
Hospice FactsSource: National Hospice and Palliative Care Organization, 2009
• There are currently more than 4,850 hospice programs in the United States that served 1.45 million people in 2008.• It is estimated that about 38.5% of deaths are under hospice care.• Just under half of hospice care organizations are for-profit (46%), half are non-profit (50%), and 4% are operated by the government (e.g.,
U.S. Department of Veterans Affairs).• Nearly all hospice care is paid for through the Medicare or Medicaid Hospice Benefit, which covers about 89% of hospice patients.• Social workers have an average caseload of 24.2 patients; nurses have on average 13.3 patients per caseload.
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 2
WHAT IS HOSPICE SOCIAL WORK?The overall model for hospice services is viewed as a psychosof the interdisciplinary perspective beyond what a physician asocial worker is a member of the interdisciplinary team whospsychosocial support to the patient/family unit, define socialproblems, and provide both counseling and casework to mee
Hospice Social Worker Roles and Responsibilities
Hospice social workers help develop and implement the intergoal of delivering the highest quality social services to patientshould aim to ensure that continuity and comprehensive careworkers’ responsibilities, as members of the interdisciplinary
• Administering a psychosocial assessment and consulta
• Providing patient advocacy (on the team, in the progr
• Educating the family and team on psychosocial issues
• Working toward fostering team collaboration,
• Conducting joint visits with other team members to e
• Arranging group meetings with multiple members of tteam, and
• Participating in medical social worker on-call rotationof patients and families.
In addition, hospice social workers also:
• Maintain appropriate documentation in the hospice p
• Attend weekly team meetings for patient chart review
• Participate in training and in-service education,
• Assist in developing and coordinating relations betwemedical/health care services, and
• Facilitate bereavement group activities.
Social workers provide a critical element to achieving the hosinsight to the patient’s, caregivers’, and/or families’ psychosocto both prevent and cope with crisis and deal with issues as thCode of Ethics and NASW’s Standards for Practice in End-ofto act as an advocate for the patient and family members anddeveloping treatment plans that work to meet the biological,of both the patient and family. Social workers must engage thand at times other outside resources and supports, to help de
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
are provided to persons who are considered to be near the end of life (usually with a lifeexpectancy of six months or less) who are living with cancer, HIV/AIDS, Alzheimer’s disease, heartdisease, chronic respiratory diseases or other serious medical conditions. Hospice services areprovided to individuals in the context of their families, and are provided to both children and adults.
The federal role in hospice care began in 1982 and was made permanent in 1986, by the MedicareHospice Benefit Amendment to the Social Security Act (Title 18, Section 1861, Subsection dd).The law defines hospice care and the extent to which a patient must be terminally ill in order toqualify for services. Further, the law stipulates the minimum requirements for servicesadministered such as core services and the required involvement of a doctor, nurse, pastoral orother counselor, and a social worker on the interdisciplinary care team (see Appendix D forexcerpt from the Social Security Act). Following passage of the law, the Health Care FinancingAdministration (HCFA), which is now called the Centers for Medicare and Medicaid Services(CMS), developed Conditions of Participation (CoP) which set the minimum federal standards bywhich hospice programs must operate.
In addition to the federal minimum standards for hospice care which are monitored through asurvey and certification process, national organizations have also developed hospice standards,accreditation guidelines, credentials and certifications for both programs and hospice professionals.
In 2008 after an extensive review process, CMS issued the revised CoP. This revision resulted in achange to the personnel qualifications for social workers providing hospice care that from theprofession’s perspective somewhat weakened the requirement. Whereas the original CoP requiredeither a bachelor’s or master’s degree in social work, the revised CoP allows a person with a degreein a field other than social work to serve as a hospice social worker under the supervision andclinical guidance of an MSW. During the symposium, representatives from CMS cited that onereason that the end result was a broadened social work personnel qualification in the newlyrevised CoP was the lack of a robust body of research that clearly supported the need forindividuals to hold a specific degree in social work in order to ensure quality patient care andsafety. (See Federal Rules for more discussion of CMS and hospice regulations).
This current requirement is of concern to the social work community, other service providers andadvocates because it can result in someone providing social work services in hospice that mayhave little or no hospice experience or professional training as a social worker. Understanding thesocial work role in hospice and fulfilling those functions is a critical aspect of ensuring qualitypsychosocial care.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 3
Federal Social Work Qualifications for Hospice CareConditions of Participation 418.114 (b) Standard: Personnel qualifications for certain disciplines:
3. Social worker. A person who—(i) (A) Has a Master of Social Work (MSW) degree from a school of social work accredited by the Council on Social Work Education and
one year of social work experience in a healthcare setting; or(B) Has a baccalaureate degree in social work from an institution accredited by the Council on Social Work Education; or a
baccalaureate degree in psychology, sociology, or other field related to social work and is supervised by an MSW as described inparagraph (b)(3)(i)(A) of this section; and
(ii) Has one year of social work experience in a healthcare setting; or(iii) Has a baccalaureate degree from a school of social work accredited by the Council on Social Work Education, is employed by the
hospice before December 2, 2008, and is not required to be supervised by an MSW” (CMS, 2009, p.32218).
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 3
WHAT IS HOSPICE SOCIAL WORK?The overall model for hospice services is viewed as a psychosocial model, valuing the importanceof the interdisciplinary perspective beyond what a physician and nurse might provide. A hospicesocial worker is a member of the interdisciplinary team whose primary function is to providepsychosocial support to the patient/family unit, define social service goals for alleviating identifiedproblems, and provide both counseling and casework to meet the established service goals.
Hospice Social Worker Roles and Responsibilities
Hospice social workers help develop and implement the interdisciplinary plan of care with thegoal of delivering the highest quality social services to patients and families. This plan of careshould aim to ensure that continuity and comprehensive care are provided. Hospice socialworkers’ responsibilities, as members of the interdisciplinary team include:
• Administering a psychosocial assessment and consultation,
• Providing patient advocacy (on the team, in the program, in the community),
• Educating the family and team on psychosocial issues, family and group dynamics,
• Working toward fostering team collaboration,
• Conducting joint visits with other team members to enhance care,
• Arranging group meetings with multiple members of the family, facility, and hospice careteam, and
• Participating in medical social worker on-call rotation/schedule in order to meet the needsof patients and families.
In addition, hospice social workers also:
• Maintain appropriate documentation in the hospice patient chart,
• Attend weekly team meetings for patient chart review,
• Participate in training and in-service education,
• Assist in developing and coordinating relations between the hospice agency and outsidemedical/health care services, and
• Facilitate bereavement group activities.
Social workers provide a critical element to achieving the hospice care mission by providinginsight to the patient’s, caregivers’, and/or families’ psychosocial needs, and are essential in helpingto both prevent and cope with crisis and deal with issues as the illness progresses. The NASWCode of Ethics and NASW’s Standards for Practice in End-of-Life Care call hospice social workersto act as an advocate for the patient and family members and to strive to include them indeveloping treatment plans that work to meet the biological, social, emotional, and spiritual needsof both the patient and family. Social workers must engage the interdisciplinary team, the family,and at times other outside resources and supports, to help develop a comprehensive plan of care
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 4
idered to be near the end of life (usually with a lifeo are living with cancer, HIV/AIDS, Alzheimer’s disease, heartr other serious medical conditions. Hospice services areof their families, and are provided to both children and adults.
in 1982 and was made permanent in 1986, by the Medicareocial Security Act (Title 18, Section 1861, Subsection dd).extent to which a patient must be terminally ill in order totipulates the minimum requirements for servicesd the required involvement of a doctor, nurse, pastoral oron the interdisciplinary care team (see Appendix D forFollowing passage of the law, the Health Care Financing
w called the Centers for Medicare and Medicaid Servicescipation (CoP) which set the minimum federal standards by.
andards for hospice care which are monitored through anal organizations have also developed hospice standards,
nd certifications for both programs and hospice professionals.
cess, CMS issued the revised CoP. This revision resulted in afor social workers providing hospice care that from the
akened the requirement. Whereas the original CoP requiredn social work, the revised CoP allows a person with a degreerve as a hospice social worker under the supervision andthe symposium, representatives from CMS cited that onedened social work personnel qualification in the newlybody of research that clearly supported the need forn social work in order to ensure quality patient care andcussion of CMS and hospice regulations).
n to the social work community, other service providers andeone providing social work services in hospice that mayprofessional training as a social worker. Understanding the
ng those functions is a critical aspect of ensuring quality
NKING POLICY, PRACTICE, AND RESEARCH REPORT
3
ations for Hospice Caredard: Personnel qualifications for certain disciplines:
rom a school of social work accredited by the Council on Social Work Education andthcare setting; orom an institution accredited by the Council on Social Work Education; or agy, or other field related to social work and is supervised by an MSW as described in
healthcare setting; orsocial work accredited by the Council on Social Work Education, is employed by thet required to be supervised by an MSW” (CMS, 2009, p.32218).
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 4
CURRENT STATUS OF HOSPICE SOCIAResearch about hospice by social workers cuts across three mworkers’ roles in hospice care settings; provides the social woand interventions; and identifies issues related to the educatioworkers. Social work research about hospice care brings a cridepth and meaning to our understanding of these services.
Up to now there has been no rigorous systematic review of hare few studies that specifically examine the effectiveness of hfollowing provides an overview of recent research by social wrelevant topics (See Appendix K for full citations).2 It shouldsystematic in its development and therefore may exclude somtopics and/or authors.
Research on the role of social workers in hospice explores:
• Techniques of assessment (Reese, Raymer, Orloff, GerWise-Wright & Huber, 2006).
• The nature of roles of social workers in various end-ohospital palliative care, home hospice, prison hospiceWright, 2006; Lawson, 2007).
• Outcomes of social workers involvement in specific inhospice service delivery, e.g., assessment, treatment, b
• Assessing client and caregiver satisfaction with socialDoherty & Deweaver, 2004).
Research on perspectives about social workers’ roles consider
• Addressing ethical issues of care such as “death withHedlund & Soule, 2006).
• Managing ethical issues: Consider medical condition,terminality (Csikai, 2004).
• Philosophies on palliative and end-of-life care from onsocial workers v. nursing home social workers (Becke
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
that minimizes unmet needs. Furthermore, social workers must also seek to understand thetreatment philosophies and motivations of other disciplines in developing plans of care.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 5
Hospice Social Worker’s Clinical Responsibilities1
• Assessment:◊ Physical◊ Social network, family◊ Psychosocial◊ Cultural and spiritual◊ Financial and legal◊ End of Life “Needs”◊ Home and environment safety◊ Protective issues- abuse and neglect (physical, sexual, fiduciary)
• Interventions◊ Specific symptom relief (interventions for fear, grief, depression, anger, pain. etc.)◊ Patient and family education◊ Community and internal resources and referrals; including governmental benefits◊ Discharge planning◊ Assistance in securing documents◊ Patient and family advocacy◊ Identification of abuse and neglect◊ Bereavement care
• Education and interventions for pediatric patients, siblings and for children of adult patients
• Social workers provide to the team:◊ Psychosocial consultation,◊ Patient advocacy —on the team, in the program, in the community◊ Education re: psychosocial issues/family and group dynamics◊ Care Plan Development—-Team meeting participation◊ Joint visits with other team members to enhance care◊ Group meetings (patient, family, facility, hospice team, etc.).
1 Prepared by Beckwith and Fried for presentation at the Hospice Symposium 2 This review is based on the presentation by Deborah Waldrop at the SWPI Hospic
Dual Pathways of Social Work Research
• PATHWAY ONE relates to the expertise and perspective on clients, systems, ethics,work researcher brings to research questions.
• PATHWAY TWO relates more specifically to research on the development and impused by social workers.
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 5
CURRENT STATUS OF HOSPICE SOCIAL WORK RESEARCHResearch about hospice by social workers cuts across three major areas. It evaluates socialworkers’ roles in hospice care settings; provides the social work perspective on hospice practicesand interventions; and identifies issues related to the education and training of hospice socialworkers. Social work research about hospice care brings a critical perspective that helps to adddepth and meaning to our understanding of these services.
Up to now there has been no rigorous systematic review of hospice social work research and thereare few studies that specifically examine the effectiveness of hospice social work practice. Thefollowing provides an overview of recent research by social workers and about social workrelevant topics (See Appendix K for full citations).2 It should be noted that this analysis is notsystematic in its development and therefore may exclude some related and pertinent researchtopics and/or authors.
Research on the role of social workers in hospice explores:
• Techniques of assessment (Reese, Raymer, Orloff, Gerbino, Valade, Dawson, Butler,Wise-Wright & Huber, 2006).
• The nature of roles of social workers in various end-of-life and palliative care settings, e.g.,hospital palliative care, home hospice, prison hospice, etc. (Bradsen, 2005; Bronstein &Wright, 2006; Lawson, 2007).
• Outcomes of social workers involvement in specific interventions and certain stages ofhospice service delivery, e.g., assessment, treatment, bereavement (Reese & Raymer, 2004).
• Assessing client and caregiver satisfaction with social work (Archer & Boyle, 1999;Doherty & Deweaver, 2004).
Research on perspectives about social workers’ roles considers:
• Addressing ethical issues of care such as “death with dignity” practices in Oregon (Miller,Hedlund & Soule, 2006).
• Managing ethical issues: Consider medical condition, involvement of family, denial ofterminality (Csikai, 2004).
• Philosophies on palliative and end-of-life care from oncology social workers vs. hospicesocial workers v. nursing home social workers (Becker, 2004).
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 6
more, social workers must also seek to understand thens of other disciplines in developing plans of care.
NKING POLICY, PRACTICE, AND RESEARCH REPORT
5
nical Responsibilities1
physical, sexual, fiduciary)
s for fear, grief, depression, anger, pain. etc.)
nd referrals; including governmental benefits
ts, siblings and for children of adult patients
e program, in the communitymily and group dynamicsng participationto enhance carelity, hospice team, etc.).
at the Hospice Symposium 2 This review is based on the presentation by Deborah Waldrop at the SWPI Hospice Symposium.
Dual Pathways of Social Work Research
• PATHWAY ONE relates to the expertise and perspective on clients, systems, ethics, cultural competence, and communities that a socialwork researcher brings to research questions.
• PATHWAY TWO relates more specifically to research on the development and implementation and effectiveness of specific interventionsused by social workers.
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 6
• The ambiguity of dying and the decisions behind dyin(Bern-Klug, 2008).
• “Possible” or “ambiguous dying” among nursing homBern-Klug, 2006).
• How older adult dyads’ negotiate the ambiguity of dylife’s end (Gardner, 2008).
• Short hospice utilization: Can this be enough? (Waldr
• The relationship between terminal restlessness with p& Faul, 2005).
Research on the quality of dying in long-term care facilities a
• Family perspectives on what defines a good death in aexamined include staffing adequacy, training, consisteempathy, hospice contributions (Munn & ZimmermaWilliams, Biola & Zimmerman, 2008),
• The under-utilization of hospice services in long termRachlin, 2007).
• How comfort care should be defined (Waldrop & Kir
Social work research evaluates the experiences of diverse andare facing issues of advanced illness and end -of-life care by:
• Investigating what matters to older African Americantheir decisions to complete or not complete advanced& Bradley. (2005).
• Exploring racial variations in end-of-life decision-mak
• Examining the specific social stressors and facilitatorspopulations who reside there (Francoeur, Payne, Rave
• Examining caregivers experiences with hospice and pa(Sanders, Butcher, Swails, & Power, 2009).
• Identifying factors that contribute to the under-utilizaAmericans (Washington, Bickel-Swenson, & Stephens
With the field of hospice care continually expanding, researchcompetent social workers for careers in hospice. Research onhospice social workers:
• Stresses the need to expand curriculum in MSW progrsocial workers in hospice care through education and& Black, 2006).
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
Research on social workers’ roles as a member of the interdisciplinary team addresses:
• Strengths and challenges social workers face in using collaboration in service delivery(Parker Oliver, Bronstein, & Kurzejeski, 2005; Parker Oliver & Peck, 2006).
• Interfacing with caregivers about pain management (Parker Oliver, Wittenberg-Lyles,Washington, & Sehrawat, 2009).
• Increasing patient and family involvement with interdisciplinary teams (Parker Oliver,Porock, Demiris, & Courtney, 2005).
Research on family and caregiver involvement examines:
• What, if any, unmet needs the families may have (Arnold, Martin, Griffith, Person &Graham, 2006).
• Conflict within the family at life’s end (Kramer, Boelk, & Auer, 2006).
• The roles of family caregivers in decision-making, assistance with daily living activities,and medication management (Hauser & Kramer, 2004).
• Coping with end-of-life transitions in caregiving, including comprehending terminality,near-acute care, executive functioning, and final decision making (Waldrop, Kramer,Skretny, Milch & Finn, 2005).
• Relationships between high levels of caregiver grief and Alzheimer’s Disease (Sanders, Ott,Kelber, & Noonan, 2008).
• Psychosocial stressors in end-of-life caregiving (Waldrop, Milch & Skretny, 2005).
• Consideration of the family’s concerns and values in determining care (Csikai, 2004).
Research that tests and examines interventions includes:
• Study of the FACES Project, a tool to assess caregiver strain (Townsend, Ishier, Vargo,Shapiro, Pitorak & Matthews, 2007.
• Use of formally structured social work visits to accomplish advanced care planning athome (Ratner, Norlander & McSteen, 2001).
• Lessons learned from “model” programs (Kramer & Auer, 2005).
Social work research also seeks to understand a patient’s perspective on the process of dying byassessing:
• How patients seek control over decision-making, independence, mental attitude, dailyliving activities, instrumental daily living activities, and relationships (Schroepfer, Noh &Kavanaugh, 2009).
• The reasons people desire to hasten death, e.g., poor quality of life and concern forsuffering (Arnold, Atkin, Person & Griffith, 2004).
• How conflictual social support systems predict the consideration of hastening death(Schroepfer, 2008).
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 7
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 7
• The ambiguity of dying and the decisions behind dying (is dying allowed v. contested?)(Bern-Klug, 2008).
• “Possible” or “ambiguous dying” among nursing home residents (Bern-Klug, 2005;Bern-Klug, 2006).
• How older adult dyads’ negotiate the ambiguity of dying and the search for meaning atlife’s end (Gardner, 2008).
• Short hospice utilization: Can this be enough? (Waldrop & Rinfrette, 2009).
• The relationship between terminal restlessness with psychosocial & spiritual distress (Head& Faul, 2005).
Research on the quality of dying in long-term care facilities analyzes:
• Family perspectives on what defines a good death in a long term care setting. Factorsexamined include staffing adequacy, training, consistency, facility environment, staffempathy, hospice contributions (Munn & Zimmerman, 2006; Munn, Dobbs, Meier,Williams, Biola & Zimmerman, 2008),
• The under-utilization of hospice services in long term care (Chapin, Gordon, Landry &Rachlin, 2007).
• How comfort care should be defined (Waldrop & Kirkendall, 2009).
Social work research evaluates the experiences of diverse and under-represented populations whoare facing issues of advanced illness and end -of-life care by:
• Investigating what matters to older African Americans at life’s end and what influencestheir decisions to complete or not complete advanced directives (Bullock, McGraw, Blank& Bradley. (2005).
• Exploring racial variations in end-of-life decision-making (Hopp & Duffy, 2000).
• Examining the specific social stressors and facilitators in the inner city and with minoritypopulations who reside there (Francoeur, Payne, Raveis & Shim, 2007).
• Examining caregivers experiences with hospice and patients who have end-stage dementia(Sanders, Butcher, Swails, & Power, 2009).
• Identifying factors that contribute to the under-utilization of hospice services by AfricanAmericans (Washington, Bickel-Swenson, & Stephens, 2008).
With the field of hospice care continually expanding, research also addresses the efforts to preparecompetent social workers for careers in hospice. Research on the education and training ofhospice social workers:
• Stresses the need to expand curriculum in MSW programs and better define the role ofsocial workers in hospice care through education and training (Huff, Weisenfluh, Murphy& Black, 2006).
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 8
member of the interdisciplinary team addresses:
l workers face in using collaboration in service deliveryKurzejeski, 2005; Parker Oliver & Peck, 2006).
out pain management (Parker Oliver, Wittenberg-Lyles,9).
nvolvement with interdisciplinary teams (Parker Oliver,2005).
olvement examines:
families may have (Arnold, Martin, Griffith, Person &
fe’s end (Kramer, Boelk, & Auer, 2006).
in decision-making, assistance with daily living activities,Hauser & Kramer, 2004).
ions in caregiving, including comprehending terminality,ctioning, and final decision making (Waldrop, Kramer,
vels of caregiver grief and Alzheimer’s Disease (Sanders, Ott,
of-life caregiving (Waldrop, Milch & Skretny, 2005).
oncerns and values in determining care (Csikai, 2004).
rventions includes:
tool to assess caregiver strain (Townsend, Ishier, Vargo,2007.
ial work visits to accomplish advanced care planning atMcSteen, 2001).
programs (Kramer & Auer, 2005).
derstand a patient’s perspective on the process of dying by
r decision-making, independence, mental attitude, dailydaily living activities, and relationships (Schroepfer, Noh &
asten death, e.g., poor quality of life and concern foron & Griffith, 2004).
rt systems predict the consideration of hastening death
NKING POLICY, PRACTICE, AND RESEARCH REPORT
7
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 8

FEDERAL RULES AND PRIORITIES3
Revising and Implementing the Conditions of Participatio
The Centers for Medicare and Medicaid Services (CMS) reguStates. Hospice providers and suppliers must be Medicare-cerhospice services that they administer to Medicare beneficiarieSurvey Agency. To be Medicare-certified, hospice agencies muParticipation (CoPs).
It took approximately ten years to fully revise the Hospice Cowithin CMS, the Department of Health and Human ServicesManagement and Budget (OMB) as well as input from the puprescribed public comment period. The final rule was publish2008, and implementation of the new CoPs began in Decemb
A wide variety of comments regarding the need and feasibilitsocial workers was discussed in CMS’s publication of the fina5, 2008. CMS’s response indicated several reasons for a broanoted that because not all states administer equivalent socialrequirements CoP defers to states’ regulations for social worklicensure. All hospice social workers must be licensed in accorequirements of the state(s) in which they practice. Commentpotential need to provide waivers to rural hospice agencies beand qualified social workers if the personnel qualifications wMedicaid Programs, 2008). CMS stated that it encourages hoqualified social workers possible, but expressed that becausehospice industry on this issue,” personnel qualifications couldrewrite of the CoP (Medicare and Medicaid Programs, 2008,
Highlights of the Revised CoP
An important theme of the revised CoPs is the use of a patienreinforce the interdisciplinary team approach and seek to advservice improvement. Highlights of the provisions of the revis(For more detail on the revised CoPs see Appendix E).
• The establishment of patient’s rights CoP in hospice creporting violations of those rights.
• The requirement of an initial assessment of the patienhospice care and a comprehensive assessment within 5hospice care.
• The creation of interdisciplinary groups (IDG) that insocial worker, and a pastoral or other counselor; all othe patient’s and family’s needs during treatment.
• The requirement that the IDG create a comprehensiveregularly reviewed and revised to best meet the patien
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
3 Based on presentations made by CMS staff Mary Rossi-Coajou and Danielle Shea
• Identifies the need for focus on spiritual care; role conflict and ambiguity (Wesley, Tunney& Duncan, 2004).
• Analyzes end-of-life care content in textbooks (Kramer, Pacourek, Hovland & Scafe, 2003)
• Identifies social work competencies in palliative and end-of-life care (Gwyther, Altilio,Blacker, Christ, Csikai, Hooyman, Kramer, Linton, Raymer & Howe, 2005).
• Examines end-of-life content in conferences (Moon & Cagle, 2009).
Agenda Development for Hospice Research: A Look to the Future
Bern-Klug, Kramer, and Linder (2005) and Kramer, Bern-Klug and Francouer (2005) haveproposed a national social work research agenda related to palliative and end-of-life care. Thisagenda highlights areas for research that align with the social work professions’ mission andvalues. The imperative to develop the agenda emerged from the 2002 and 2005 Social WorkSummits on End-of-Life and Palliative Care, organized by the Social Work LeadershipDevelopment Awards Program, sponsored by the Open Society Institute’s Project on Death inAmerica (PDIA), a project of the Soros Foundation. The Leadership Development Programsupported 42 scholars and led to the creation of the Social Work Hospice and Palliative CareNetwork (SWHPN) (www.swhpn.org).
In addition to the social work research agenda, national organizations, such as the NHPCO(2004) and the Hospice and Palliative Nurses Association (HPNA) have released agendas focusingon various elements of care and service administration for palliative and end-of-life care. Theefforts of social work researchers contribute both to the discipline-specific and interdisciplinaryresearch agendas. In the coming year, the effort to increase interdisciplinary research will result inthe release of a collaborative research agenda from the American Academy of Hospice andPalliative Medicine (AAHPM), NHPCO, HPNA, and the Social Work Hospice and Palliative CareNetwork (SWHPN).
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 9
Palliative and End of Life Care Research Agenda
• Continuity, gaps, fragmentation, transitions in care• Diversity and health care disparities• Financing• The policy/practice nexus• Mental health concerns and services• Communication
• Individual and family care needs and experiences• Quality of care• Decision-making• Grief and bereavement• Pain, symptom management• Curriculum
John A. Hartford Foundation’sThe Geriatric Social Work Initiative www.gswi.org
Launched in 1999, the John A. Hartford Foundation’s Geriatric Social Work Initiative has 2 key programs that have helped to support hospiceand end-of-life focused research by social workers. The Hartford Faculty Scholars Program supports early career social work researchersinterested in aging. The Hartford Doctoral Fellows Program provides dissertation support to those social work doctoral students examininggerontology relevant topics. Appendix O provides information on Hartford Scholars and Fellows who have pursued hospice-relevant studies.
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 9
FEDERAL RULES AND PRIORITIES3
Revising and Implementing the Conditions of Participation
The Centers for Medicare and Medicaid Services (CMS) regulates hospice programs in the UnitedStates. Hospice providers and suppliers must be Medicare-certified to be paid by Medicare for thehospice services that they administer to Medicare beneficiaries. This is enforced by the StateSurvey Agency. To be Medicare-certified, hospice agencies must meet the established Conditions ofParticipation (CoPs).
It took approximately ten years to fully revise the Hospice CoP. The process required approvalwithin CMS, the Department of Health and Human Services (DHHS), and the Office ofManagement and Budget (OMB) as well as input from the public that was provided through aprescribed public comment period. The final rule was published in the Federal Register in June2008, and implementation of the new CoPs began in December 2008.
A wide variety of comments regarding the need and feasibility for higher qualifications for hospicesocial workers was discussed in CMS’s publication of the final rule in the Federal Register on June5, 2008. CMS’s response indicated several reasons for a broadened personnel requirement. Itnoted that because not all states administer equivalent social work licensure, the personnelrequirements CoP defers to states’ regulations for social workers to dictate requirements forlicensure. All hospice social workers must be licensed in accordance with the licensurerequirements of the state(s) in which they practice. Commenters also raised concerns about thepotential need to provide waivers to rural hospice agencies because of limited access to supervisionand qualified social workers if the personnel qualifications were increased (Medicare andMedicaid Programs, 2008). CMS stated that it encourages hospice agencies to employ the mostqualified social workers possible, but expressed that because “no standard or consensus in thehospice industry on this issue,” personnel qualifications could not be raised during the presentrewrite of the CoP (Medicare and Medicaid Programs, 2008, p. 32160).
Highlights of the Revised CoP
An important theme of the revised CoPs is the use of a patient-centered focus. The CoPs alsoreinforce the interdisciplinary team approach and seek to advance quality measurement andservice improvement. Highlights of the provisions of the revisions to the CoPs are noted below.(For more detail on the revised CoPs see Appendix E).
• The establishment of patient’s rights CoP in hospice care settings and a method forreporting violations of those rights.
• The requirement of an initial assessment of the patient within 48 hours of the election ofhospice care and a comprehensive assessment within 5 calendar days of the election ofhospice care.
• The creation of interdisciplinary groups (IDG) that include a doctor, a registered nurse, asocial worker, and a pastoral or other counselor; all of which must meet to assess and meetthe patient’s and family’s needs during treatment.
• The requirement that the IDG create a comprehensive plan of care for the patient that isregularly reviewed and revised to best meet the patient’s needs and goals.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 10
3 Based on presentations made by CMS staff Mary Rossi-Coajou and Danielle Shearer at the Symposium
n spiritual care; role conflict and ambiguity (Wesley, Tunney
ent in textbooks (Kramer, Pacourek, Hovland & Scafe, 2003)
ncies in palliative and end-of-life care (Gwyther, Altilio,man, Kramer, Linton, Raymer & Howe, 2005).
n conferences (Moon & Cagle, 2009).
Research: A Look to the Future
) and Kramer, Bern-Klug and Francouer (2005) haverch agenda related to palliative and end-of-life care. Thishat align with the social work professions’ mission andagenda emerged from the 2002 and 2005 Social Worke Care, organized by the Social Work Leadershipored by the Open Society Institute’s Project on Death ins Foundation. The Leadership Development Programcreation of the Social Work Hospice and Palliative Care).
h agenda, national organizations, such as the NHPCONurses Association (HPNA) have released agendas focusinge administration for palliative and end-of-life care. Thetribute both to the discipline-specific and interdisciplinarythe effort to increase interdisciplinary research will result inagenda from the American Academy of Hospice and
CO, HPNA, and the Social Work Hospice and Palliative Care
NKING POLICY, PRACTICE, AND RESEARCH REPORT
9
are Research Agenda
re • Individual and family care needs and experiences• Quality of care• Decision-making• Grief and bereavement• Pain, symptom management• Curriculum
’sitiative www.gswi.org
s Geriatric Social Work Initiative has 2 key programs that have helped to support hospicehe Hartford Faculty Scholars Program supports early career social work researchersrogram provides dissertation support to those social work doctoral students examiningformation on Hartford Scholars and Fellows who have pursued hospice-relevant studies.
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 10
ACCREDITATION AND PROFESSIONAPRACTICE OF HOSPICE CARE
Accreditation of Hospice Programs
CMS has granted deeming authority to the Joint CommisAccreditation Program (CHAP), and the Accreditation Co(See Appendix G for more details of these programs). Eacaccreditation to home care and hospice programs and thestandards established by CMS and the established standa
National Hospice and Palliative Care Organization (NHPwww.nhpco.org/i4a/pages/Index.cfm?pageID=4900
NHPCO provides a framework of standards for both clinhospice organizations to have a means for measuring, evacare. The standards consist of ten components that seek tand families by focusing on patient and family-centered cstriving for clinical excellence, ensuring inclusion and acccomprehensive quality service evaluations (see NHPCO SAppendix H).
National Association of Social Workers Standards for Pawww.socialworkers.org/practice/bereavement/standar
The NASW has established standards for social workand end-of-life care. These standards expand upon tha framework for roles and responsibilities of a hospicethics and values, required knowledge for practice, astreatment planning, attitude and self-awareness, empoquality documentation, interdisciplinary teamwork, ceducation, and supervision, leadership, and training (Appendix I).
National Association of Social Workers Credentials
Advanced Certified Hospice and Palliative Social Wowww.socialworkers.org/credentials/credentials/chpsw
Certified Hospice and Palliative Social Worker (CHPwww.socialworkers.org/credentials/credentials/chpsw
The premier credentials for social workers in hospicea BSW and MSW level credential jointly with the NatOrganization (NHPCO). These credentials were desigand palliative care for social workers who meet natio
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
• The development and implementation of methods for monitoring quality/performance andidentifying opportunities for improvement.
• The definition of personnel qualifications for various members of the IDG, including socialworkers.
Quality Assessment and Performance Improvement (QAPI)
A key focus for CMS is the effort to enhance the quality of care for hospice patients and theirfamilies. This is to be accomplished through provisions for quality assessment and performanceimprovement (QAPI) that are incorporated into the newly implemented Conditions ofParticipation.
QAPI operates at both a patient level and a hospice agency level, requiring data collection at bothlevels to assess quality. For the patient level portion of QAPI a hospice collects data on anindividual patient’s assessment/reassessment, care plan, and clinical notes with the goal ofimproving patient outcomes. The hospice level portion of QAPI looks at the clinically-focusedaggregate data of the patients, as well as data from other sources such as client satisfaction data,administrative data, marketing data, profitability data, and data on fundraising for the entirehospice agency with the goal of improving clinical and non-clinical operations. Data is used toidentify opportunities for improvement, and demonstrate performance improvement in one ormore areas. The goal is to use data in conjunction with clinical and managerial expertise andexperience to drive decision-making at the patient level and hospice agency level. CMS is currentlydeveloping quality measures to comprehensively evaluate hospice services (See Appendix F).
The methods and the quality of record keeping and reporting by hospice social workers and otherclinicians can positively impact a hospice’s ability to measure quality in a consistent andmeaningful manner. Lack of access to electronic clinical records and non-social work-focusedelectronic record formats can, however, diminish the quality of records social workers provide tointerdisciplinary care files.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 11
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 11

ACCREDITATION AND PROFESSIONAL STANDARDS FORPRACTICE OF HOSPICE CARE
Accreditation of Hospice Programs
CMS has granted deeming authority to the Joint Commission, the Community HealthAccreditation Program (CHAP), and the Accreditation Commission for Health Care (ACHC)(See Appendix G for more details of these programs). Each organization administersaccreditation to home care and hospice programs and the deeming is based on the minimumstandards established by CMS and the established standards of the group.
National Hospice and Palliative Care Organization (NHPCO) Standards for Practicewww.nhpco.org/i4a/pages/Index.cfm?pageID=4900
NHPCO provides a framework of standards for both clinical and non-clinical areas of care forhospice organizations to have a means for measuring, evaluating, and improving all areas ofcare. The standards consist of ten components that seek to increase quality of care for patientsand families by focusing on patient and family-centered care, adhering to ethical practice,striving for clinical excellence, ensuring inclusion and access, and regularly conductingcomprehensive quality service evaluations (see NHPCO Standards for Practice Details,Appendix H).
National Association of Social Workers Standards for Palliative and End-of-Life Carewww.socialworkers.org/practice/bereavement/standards/default.asp
The NASW has established standards for social workers practicing in the field of palliativeand end-of-life care. These standards expand upon the NASW Code of Ethics and providea framework for roles and responsibilities of a hospice social worker. Standards discussethics and values, required knowledge for practice, assessment of clients, intervention andtreatment planning, attitude and self-awareness, empowerment and advocacy, proper andquality documentation, interdisciplinary teamwork, cultural competence, continuingeducation, and supervision, leadership, and training (see a summary of NASW Standards,Appendix I).
National Association of Social Workers Credentials
Advanced Certified Hospice and Palliative Social Worker (ACHP-SW)www.socialworkers.org/credentials/credentials/chpsw.asp
Certified Hospice and Palliative Social Worker (CHP-SW)www.socialworkers.org/credentials/credentials/chpsw.asp
The premier credentials for social workers in hospice and palliative care, NASW developeda BSW and MSW level credential jointly with the National Hospice and Palliative CareOrganization (NHPCO). These credentials were designed by social work leaders in hospiceand palliative care for social workers who meet national standards of excellence.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 12
entation of methods for monitoring quality/performance andmprovement.
alifications for various members of the IDG, including social
nce Improvement (QAPI)
nhance the quality of care for hospice patients and theirhrough provisions for quality assessment and performancerated into the newly implemented Conditions of
and a hospice agency level, requiring data collection at bothlevel portion of QAPI a hospice collects data on ansment, care plan, and clinical notes with the goal ofpice level portion of QAPI looks at the clinically-focusedas data from other sources such as client satisfaction data,
profitability data, and data on fundraising for the entireoving clinical and non-clinical operations. Data is used tont, and demonstrate performance improvement in one orconjunction with clinical and managerial expertise andt the patient level and hospice agency level. CMS is currentlyehensively evaluate hospice services (See Appendix F).
d keeping and reporting by hospice social workers and otherpice’s ability to measure quality in a consistent andelectronic clinical records and non-social work-focused
er, diminish the quality of records social workers provide to
NKING POLICY, PRACTICE, AND RESEARCH REPORT
11
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 12
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
• Addressing tensions between different team membersresolving disagreements related to assessing and treati
• Encouraging all team members to provide quality docdeveloping, implementing, and evaluating care plans.
Workload and Organizational Supports May be ChallengingAs in several other fields of social work practice, hospice socicaseloads, low salaries, limited access to training, lack of sociadministrative support. As noted in Assuring the SufficiencyStudy of Licensed Social Workers - Special Report on Social(NASW, 2006), social workers in health care settings have cacomplexity. This is occurring as resources and supports are dsocial workers, the study found that continuing education ishigher than in other healthcare settings and salaries are the lo
DocumentationCMS surveys of hospice programs exposed some challenges tproviding thorough, timely, and quality documentation pertinworkers are often out in the field and may have limited acceselectronic case files do not have space to easily note social wocare. Lastly, some social workers may default to the nurse, thabout the patient’s plan of care. Without this quality documecannot recognize the valuable work that social workers perfo
One step to advocate for the documentation of social workerdocumentation of services provided over the telephone. For snot just with the family or the patient, but may also include ocommunity resources (CR 6440).
Clarity of Roles across Different Service SettingsWith the expansion of eligibility for hospice services to thosegroup care and assisted living settings, the hospice social worsocial workers, nurses, or other professionals in the other settclear roles and functions, and clear communication channelsmembers.
Research and Hospice Social Work
There is a growing body of social work research on hospice ainterdisciplinary hospice research (see Annotated Bibliographagendas have sought to demonstrate the effectiveness of hospreview of the research conclusively demonstrates this effectivecare and/or the interventions used in practice. The PDIA progthe Hartford Faculty Scholars and Doctoral Fellows programvisibility for hospice social work research. The launching of tLife Care & Palliative Care has provided an important venue
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 13
CONCLUSIONS
Social Workers’ Roles in Hospice Care
Social Work Expertise is Essential in End-of-Life CareWorking with individuals and families through transitions during life’s final chapter, includinghospice, requires competent social workers with requisite knowledge, skills and values.Encouraging social workers toward careers in end-of-life care necessitate that social workeducation programs at both the BSW and MSW level offer specialized and infused curriculum aswell as field placements and collaborations with community-based programs. Continuingprofessional development is also critical.
Roles Need On-Going Clarification and AdvocacyAlthough the social worker’s roles in hospice and the importance of having professionally trainedsocial workers deliver such services may be well articulated within the profession, it is not as clearto policy makers, hospice administrators, and other professions involved in hospice care. Thisunclear role definition is compounded by the increasing medicalization of hospice which may limitsocial workers’ opportunities to fully assess and treat the psychosocial needs of the patient andtheir family.
Since a number of agencies may provide both hospice and home health services, such agenciesneed to be clear that hospice and home health regulations differ. For example, in hospice the socialworker might be the first person to engage with a patient and their family; in home health it isrequired that a nurse be at the initial meeting and recommend social work services.
Credentials are a Resource to UseThe recent launch of two credentials for hospice social workers (see NASW credentials), offeredthrough NASW and jointly developed between NASW and NHPCO provide an excellentopportunity to further clarify and quantify the skills and knowledge required for hospice socialwork practice. Encouraging agencies and hospice social workers to pursue the credential andadvocating for hospice agencies to recognize the value of such credentials will be critical.
Interdisciplinary Team ParticipationSocial workers should continually strive to be integral members of the interdisciplinary care teamand remain active and engaged in developing and maintaining a patient’s plan of care. Thecompetencies articulated through NASW standards and credentials as well as the growing researchbase provide a strong framework to use in increasing awareness and understanding of socialwork’s valuable role in hospice.
While role conflicts are not always the case, in some instances role conflicts do occur – sometimesbetween the social worker and the nurse, and in some cases between the social worker andpastoral counselor or other spiritual/religious provider. Efforts to enhance interdisciplinary teamfunctioning includes:
• Holding regular trainings about increasing team functioning and educating each teammember about the responsibilities and perspectives of all the professions in hospice care.
• Stressing the uniqueness and responsibilities of each team member in providing qualityhospice care.
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 13

HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 14
• Addressing tensions between different team members and providing a framework forresolving disagreements related to assessing and treating a patient’s needs.
• Encouraging all team members to provide quality documentation of their efforts indeveloping, implementing, and evaluating care plans.
Workload and Organizational Supports May be ChallengingAs in several other fields of social work practice, hospice social workers often struggle with highcaseloads, low salaries, limited access to training, lack of social work supervision, and a lack ofadministrative support. As noted in Assuring the Sufficiency of a Frontline Workforce: A NationalStudy of Licensed Social Workers - Special Report on Social Work Services In Health Care Settings(NASW, 2006), social workers in health care settings have caseloads that are increasing in size andcomplexity. This is occurring as resources and supports are decreasing. Specifically for hospicesocial workers, the study found that continuing education is often unavailable; vacancy rates arehigher than in other healthcare settings and salaries are the lowest in hospice.
DocumentationCMS surveys of hospice programs exposed some challenges that social workers experience inproviding thorough, timely, and quality documentation pertinent to a patient’s care. Socialworkers are often out in the field and may have limited access to patient clinical records. Manyelectronic case files do not have space to easily note social worker-related items for a patient’scare. Lastly, some social workers may default to the nurse, the case coordinator, to make notesabout the patient’s plan of care. Without this quality documentation, hospices and surveyors alikecannot recognize the valuable work that social workers perform.
One step to advocate for the documentation of social workers’ activities is related todocumentation of services provided over the telephone. For social workers, the contacts are oftennot just with the family or the patient, but may also include other service providers and/orcommunity resources (CR 6440).
Clarity of Roles across Different Service SettingsWith the expansion of eligibility for hospice services to those who are in hospitals, nursing homes,group care and assisted living settings, the hospice social worker may need to coordinate withsocial workers, nurses, or other professionals in the other settings. Efforts must be made to haveclear roles and functions, and clear communication channels with the patient and the familymembers.
Research and Hospice Social Work
There is a growing body of social work research on hospice and social work involvement ininterdisciplinary hospice research (see Annotated Bibliography, Appendix X). Social work researchagendas have sought to demonstrate the effectiveness of hospice social workers, yet no rigorousreview of the research conclusively demonstrates this effectiveness of social workers in hospicecare and/or the interventions used in practice. The PDIA program, participation in SWHPN andthe Hartford Faculty Scholars and Doctoral Fellows programs have provided support andvisibility for hospice social work research. The launching of the Journal of Social Work in End ofLife Care & Palliative Care has provided an important venue for publication of relevant articles.
NKING POLICY, PRACTICE, AND RESEARCH REPORT
13
are
End-of-Life Cares through transitions during life’s final chapter, includingrkers with requisite knowledge, skills and values.areers in end-of-life care necessitate that social workand MSW level offer specialized and infused curriculum astions with community-based programs. Continuingal.
nd Advocacyhospice and the importance of having professionally traineday be well articulated within the profession, it is not as clearors, and other professions involved in hospice care. Thisby the increasing medicalization of hospice which may limit
assess and treat the psychosocial needs of the patient and
de both hospice and home health services, such agenciese health regulations differ. For example, in hospice the socialgage with a patient and their family; in home health it is
meeting and recommend social work services.
or hospice social workers (see NASW credentials), offeredbetween NASW and NHPCO provide an excellentntify the skills and knowledge required for hospice socialand hospice social workers to pursue the credential andognize the value of such credentials will be critical.
ve to be integral members of the interdisciplinary care teameloping and maintaining a patient’s plan of care. TheSW standards and credentials as well as the growing researchse in increasing awareness and understanding of social
e case, in some instances role conflicts do occur – sometimesrse, and in some cases between the social worker andeligious provider. Efforts to enhance interdisciplinary team
ut increasing team functioning and educating each teamties and perspectives of all the professions in hospice care.
esponsibilities of each team member in providing quality
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 14
Interdisciplinary ResearchSince hospice is an interdisciplinary team model, interdisciplishould be used to examine service delivery that can result in ooptimal quality care. Joint research teams that use multiple pa multi-faceted view of interdisciplinary team functioning, anchallenges.
DisseminationDissemination of research to practitioners is a dilemma in masocial workers acquire information used in clinical practice frpublished in peer-reviewed journals and is not necessarily orEnhanced tools for dissemination are needed to get pertinentpractitioners and better use might be made of various on-lineresearch interpreted for practice.
Addressing Disparities in Access to and Use of Hospice CareThere are demographic disparities in both the hospice workfohave access to, and/or receive hospice care. Social workers shdemographic disparities in both the worker and patient popuresearch to develop new methods for reaching these undersermore diverse workforce. As one step to give greater visibilitypreconference that was held in conjunction with the annual Aincluded the session Understanding Diversity: How culturallyand palliative care with presenters Karen Bullock, Karen Kay
Hospice Social Work/Policy Connections
The symposium highlighted the value of building and strengtsocial work and federal agencies in regard to social work’s rofrom CMS were actively engaged in the think tank and valuefamiliar with the social work researchers and practitioners wThere is the potential for forming new exchanges among fedepractitioners, and national organizations with the goal of advdelivery and the role of various members of the interdisciplinregularly engaged with representatives from NHPCO and othwould be extremely beneficial to enhance the involvement oforganizations with CMS and other federal agencies. This wouwell as outcomes from social work research.
CMS’s development of new quality measures is a prime areaand researchers to contribute. Social work ethics and standarCMS goals of providing patient-centered and quality care. Thprovide valuable insight to quality indicators, specifically in eand outcomes of hospice care.
Since the National Institutes of Health (NIH) already has a p(see http://obssr.od.nih.gov/pdf/SWR_Report.pdf) highlightinto build hospice social work research is relevant to multiple iThis would include the National Cancer Institute, the Nation
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
Funding for Hospice Social Work ResearchBeyond the pilot research funding still available through the Hartford Scholars and Fellowsprogram, there is limited research funding available for hospice social work researchers. While thenew health care reform legislation Patient Protection and Affordable Care Act (PPACA (Pub.L.111-148)includes provisions related to hospice services for children, there is little research bysocial workers focused on services to children in hospice.
Only a few social work researchers have been successful in garnering National Institutes of Health(NIH) funding for their scholarship (e.g., Social Work Principal Investigators Otis-Green,Parker-Oliver, Schroepfer, Waldrop, and Zimmerman). In most instances, the successful applicantspreviously had received support as Hartford Faculty Scholars and/or Hartford Doctoral Fellows,and may also have attended summer institutes offered to social work researchers to enhance theirskills and success at applying for NIH funding.
Although NIH hosted a State of the Science Consensus meeting on End of Life Care in 2004(http://consensus.nih.gov/2004/2004EndOfLifeCareSOS024html.htm), social work research wasnot a contributing discipline to this effort. The National Institute on Nursing Research (NINR)has a lead role in the trans-NIH efforts related to end-of-life care. However, there is nostand-alone review group that reviews grant submissions on hospice and end-of-life care nor isthere an NIH effort to particularly develop the research careers of end-of-life and hospiceresearchers. This is a gap identified across multiple disciplines.
Research/Practice DisconnectAnother challenge identified at the symposium included the oft identified problem of thedisconnect between the questions that researchers might seek to ask and the concerns thatpractitioners have in regard to practice and/or patient care. Practitioner involvement in researchdevelopment can help to create study questions that are relevant for practice. Incorporating theexperiences of patients and families within hospice research is also important. However patientinvolvement can be difficult given the deteriorating physical and mental health of the patient.
Creating research that is more relevant and applicable to practice will encourage hospice socialworkers to value research in practice and help to legitimize the field of social work as driven byevidenced-based interventions.
Research Design and MethodsUse of multiple methods of research is important in order to expand and better define ourknowledge on the role and interventions of hospice social work. Qualitative research methods canhelp to give insight about quality indicators and better understand the nuances of hospice.Quantitative research techniques will help to establish the effectiveness of hospice social workersand the interventions used to treat hospice patients and families. Further research will also help toidentify gaps and challenges in care.
Future research on social workers in hospice care would also benefit from considering elements ofcost effectiveness. Cost effectiveness research can focus at multiple levels including examiningoutcomes related to the well-being of the family and loved ones after the patient dies.
Building a sufficient body of research so that there is opportunity to complete systematic reviewswill also help build the evidence-base for hospice social work services. Entities like the CampbellCollaboration (www.campbellcollaboration.org) with active involvement of social workresearchers can provide a venue for undertaking such a rigorous and transparent review.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 15
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 15
Interdisciplinary ResearchSince hospice is an interdisciplinary team model, interdisciplinary research is a critical avenue thatshould be used to examine service delivery that can result in outcomes and insights to achieveoptimal quality care. Joint research teams that use multiple practice philosophies can also providea multi-faceted view of interdisciplinary team functioning, and could help solve current gaps andchallenges.
DisseminationDissemination of research to practitioners is a dilemma in many fields. Although many hospicesocial workers acquire information used in clinical practice from books, most new research ispublished in peer-reviewed journals and is not necessarily or readily seen by practitioners.Enhanced tools for dissemination are needed to get pertinent research into the hands ofpractitioners and better use might be made of various on-line web resources and newsletters to getresearch interpreted for practice.
Addressing Disparities in Access to and Use of Hospice CareThere are demographic disparities in both the hospice workforce and for those who choose to,have access to, and/or receive hospice care. Social workers should explore the nature of thedemographic disparities in both the worker and patient populations. Policy makers can use thisresearch to develop new methods for reaching these underserved populations and recruiting amore diverse workforce. As one step to give greater visibility to this need the 2010 SWHPNpreconference that was held in conjunction with the annual AAHPM/HPNA Annual Assemblyincluded the session Understanding Diversity: How culturally based interventions impact hospiceand palliative care with presenters Karen Bullock, Karen Kayser, and J. Ernest Aguilar.
Hospice Social Work/Policy Connections
The symposium highlighted the value of building and strengthening the connections betweensocial work and federal agencies in regard to social work’s role in hospice. The representativesfrom CMS were actively engaged in the think tank and valued the opportunity to become morefamiliar with the social work researchers and practitioners who were their fellow participants.There is the potential for forming new exchanges among federal agencies, hospice researchers,practitioners, and national organizations with the goal of advancing quality hospice servicedelivery and the role of various members of the interdisciplinary team. While CMS staff areregularly engaged with representatives from NHPCO and other hospice provider organizations, itwould be extremely beneficial to enhance the involvement of social workers and social workorganizations with CMS and other federal agencies. This would highlight the social work role aswell as outcomes from social work research.
CMS’s development of new quality measures is a prime area for hospice social work practitionersand researchers to contribute. Social work ethics and standards for practice align closely with theCMS goals of providing patient-centered and quality care. Therefore, social workers are poised toprovide valuable insight to quality indicators, specifically in evaluating the psychosocial elementsand outcomes of hospice care.
Since the National Institutes of Health (NIH) already has a plan to enhance social work research(see http://obssr.od.nih.gov/pdf/SWR_Report.pdf) highlighting the fit of that agenda with the needto build hospice social work research is relevant to multiple institutes and offices beyond NINR.This would include the National Cancer Institute, the National Institute on Aging, the National
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 16
searchavailable through the Hartford Scholars and Fellows
ding available for hospice social work researchers. While theient Protection and Affordable Care Act (PPACA (Pub.L.o hospice services for children, there is little research bychildren in hospice.
ave been successful in garnering National Institutes of Health.g., Social Work Principal Investigators Otis-Green,nd Zimmerman). In most instances, the successful applicantsartford Faculty Scholars and/or Hartford Doctoral Fellows,nstitutes offered to social work researchers to enhance theirfunding.
cience Consensus meeting on End of Life Care in 2004ndOfLifeCareSOS024html.htm), social work research wasfort. The National Institute on Nursing Research (NINR)s related to end-of-life care. However, there is nos grant submissions on hospice and end-of-life care nor isvelop the research careers of end-of-life and hospiceross multiple disciplines.
mposium included the oft identified problem of theresearchers might seek to ask and the concerns thate and/or patient care. Practitioner involvement in researchquestions that are relevant for practice. Incorporating theithin hospice research is also important. However patientdeteriorating physical and mental health of the patient.
t and applicable to practice will encourage hospice socialand help to legitimize the field of social work as driven by
important in order to expand and better define ourons of hospice social work. Qualitative research methods cancators and better understand the nuances of hospice.help to establish the effectiveness of hospice social workersspice patients and families. Further research will also help to
hospice care would also benefit from considering elements ofesearch can focus at multiple levels including examiningthe family and loved ones after the patient dies.
so that there is opportunity to complete systematic reviewsfor hospice social work services. Entities like the Campbellration.org) with active involvement of social workndertaking such a rigorous and transparent review.
NKING POLICY, PRACTICE, AND RESEARCH REPORT
15
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 16

RECOMMENDATIONS FOR ACTION
To Advance the Role of Hospice Social Work and Addres
• Hospice social workers can:
◊ Continually reinforce their role on the interdiscipand co-workers, and with other organizations tha
◊ Utilize information provided in the NASW Standprofessional development strategies to implement
◊ Advocate for hospice administrators to promote ttools to provide quality documentation (electroniplan of care. This will help CMS better documentsocial workers.
◊ Participate in research on hospice social work toto identify practice challenges and develop eviden
◊ Remain abreast of hospice social work research atheir own practice.
◊ Develop group supervision and peer support netwand increase skills for practice.
◊ Partner with social workers in other areas (e.g., hsocial workers, oncology social workers) to promasset in providing quality care at the end of life.
• Hospice agencies can enhance the quality of services p
◊ Decreasing caseloads.
◊ Offering competitive salaries that reward social wand acquired licenses and credentials.
◊ Offering incentives for social workers that seek trincorporate research into practice.
◊ Providing quality and consistent supervision andsocial workers to help build practice skills and effevaluate performance to increase effectiveness an
◊ Helping define and support the social worker’s rointerdisciplinary care team.
◊ Ensuring electronic case notes have sections desigwork service delivery.
• National social work organizations can:
◊ Work with CMS and other federal agencies in ordvalue of hospice social work in efficiently admini
◊ Work with NIH to support research to evaluate tinterdisciplinary care teams and explore innovativ
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
Center for Complementary and Alternative Medicine, the National Center for Minority Healthand Health Disparities, the Office of Behavioral and Social Sciences Research, the Office of AIDSResearch, etc.
In addition, health care reform include provisions related to endorsing pediatric hospices,identification of a funding model for providing concurrent care of hospice and curative treatment,along with some potential funding cuts. Thus, the need for social work’s voice on developing andimplementing policy continues to be important and potentially powerful.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 17
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 17
RECOMMENDATIONS FOR ACTION
To Advance the Role of Hospice Social Work and Address Practice Issues
• Hospice social workers can:
◊ Continually reinforce their role on the interdisciplinary care team with administratorsand co-workers, and with other organizations that serve hospice patients.
◊ Utilize information provided in the NASW Standards as a guide, including creation ofprofessional development strategies to implement social work competencies.
◊ Advocate for hospice administrators to promote the need for social work relevanttools to provide quality documentation (electronic or paper format) of the patient’splan of care. This will help CMS better document and recognize the role of hospicesocial workers.
◊ Participate in research on hospice social work to better establish its effectiveness andto identify practice challenges and develop evidence-based practices.
◊ Remain abreast of hospice social work research and how its outcomes are relevant totheir own practice.
◊ Develop group supervision and peer support networks in order to decrease isolationand increase skills for practice.
◊ Partner with social workers in other areas (e.g., hospital social workers, nursing homesocial workers, oncology social workers) to promote hospice services as a valuableasset in providing quality care at the end of life.
• Hospice agencies can enhance the quality of services provided by social workers by:
◊ Decreasing caseloads.
◊ Offering competitive salaries that reward social workers for educational achievementsand acquired licenses and credentials.
◊ Offering incentives for social workers that seek training opportunities and continuallyincorporate research into practice.
◊ Providing quality and consistent supervision and consultation of social workers bysocial workers to help build practice skills and efficacy; document outcomes; andevaluate performance to increase effectiveness and efficiency of service delivery.
◊ Helping define and support the social worker’s roles and responsibilities on theinterdisciplinary care team.
◊ Ensuring electronic case notes have sections designed for capturing elements of socialwork service delivery.
• National social work organizations can:
◊ Work with CMS and other federal agencies in order for them to better understand thevalue of hospice social work in efficiently administering hospice services.
◊ Work with NIH to support research to evaluate the social work role oninterdisciplinary care teams and explore innovative techniques in practice.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 18
native Medicine, the National Center for Minority HealthBehavioral and Social Sciences Research, the Office of AIDS
e provisions related to endorsing pediatric hospices,providing concurrent care of hospice and curative treatment,ts. Thus, the need for social work’s voice on developing andmportant and potentially powerful.
NKING POLICY, PRACTICE, AND RESEARCH REPORT
17
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 18
To Promote Interdisciplinary Team Functioning
• Social workers can help build a dialogue with agencieto understand the nature of each role on the care team
◊ Work to build trust and communication with othcare team.
◊ Conduct trainings on the role of social work andmembers about their role in hospice service delive
◊ Partner with other hospice agencies and nationalinterdisciplinary collaboration in practice.
• Hospice agencies can:
◊ Develop quarterly or annual team building exerciall disciplines understand the value of each teamphilosophies.
◊ Provide tools to increase collaboration in treatmedisciplines on elements of the plan of care.
◊ Model expectations for mutual respect of interdisthe uniqueness and importance of each team memfor providing quality and comprehensive hospice
◊ Provide tools that increase trust and communicat
◊ Provide incentives to team members for taking ef
• National social work and hospice organizations can:
◊ Develop and disseminate tools to hospice leadersinterdisciplinary collaboration and team function
◊ Advocate for federal agencies involved in hospicemethods for increasing interdisciplinary team fun
◊ Advocate for federal agencies involved in hospicecollaboration and valuing different practice philoplans of care.
• Hospice social worker researchers can:
◊ Conduct rigorous research and systematic reviewinterdisciplinary team functioning.
◊ Engage in interdisciplinary research on hospice catreatment philosophies in treatment planning andalso help discover the reasons for gaps and challecollaboration in hospice care.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
◊ Engage in partnerships with national hospice organizations and accrediting bodies toeducate and promote the role of the social worker and the value it provides in hospiceservice delivery.
• Hospice social work researchers can:
◊ Develop research agendas that incorporate evaluations of hospice social workereffectiveness including cost effectiveness.
◊ Conduct rigorous systematic research that examines the effectiveness and costeffectiveness of hospice social workers at different level of qualification (e.g., MSW v.BSW, related degree v. social work degree, supervised v. not supervised, etc.).
◊ Use mixed methods to explore and conclusively define the roles and responsibilities ofhospice social workers.
◊ Seek to develop tools for capturing and evaluating quality indicators related topsychosocial needs that can be useful to CMS’s development and implementation ofthe QAPI program.
• Social work educators can:
◊ Develop a curriculum track that prepares social workers for a career in end-of-lifecare.
◊ Increase infusion of information about hospice services into the curriculum.
To Enhance Diversity in Hospice Services
• Hospice social workers and social work and hospice organizations can:
◊ Advocate for the expansion of services and outreach to more ethnically and culturallydiverse populations by engaging with members of the local community and otherhealth care professionals to educate them on the value of hospice.
◊ Incorporate patient’s and family’s involvement in developing a plan of care, whichincludes the patient’s and family’s cultural considerations of care.
◊ Partner with other hospice organizations to develop awareness campaigns geared atpopulations that are not utilizing hospice services to demonstrate the benefits ofhospice care.
◊ Encourage hospice agencies to increase access of services to populations not utilizinghospice services.
◊ Encourage hospice agencies to seek out employees from diverse backgrounds to helpenrich the cultural richness of their care teams.
◊ Help recruit qualified social workers from diverse backgrounds to explore careers inend-of-life care.
• Social work researchers can:
◊ Explore the reasons for racial and ethnic disparities in both the hospice workforce andpatient population and seek to develop methods for adding cultural diversity to thehospice care environment.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 19
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 19
To Promote Interdisciplinary Team Functioning
• Social workers can help build a dialogue with agencies and interdisciplinary team membersto understand the nature of each role on the care team. For example, social workers could:
◊ Work to build trust and communication with other members of the interdisciplinarycare team.
◊ Conduct trainings on the role of social work and develop trainings with other teammembers about their role in hospice service delivery including treatment philosophies.
◊ Partner with other hospice agencies and national organizations seeking to fosterinterdisciplinary collaboration in practice.
• Hospice agencies can:
◊ Develop quarterly or annual team building exercises to foster team cohesion and helpall disciplines understand the value of each team member and differing treatmentphilosophies.
◊ Provide tools to increase collaboration in treatment planning and include alldisciplines on elements of the plan of care.
◊ Model expectations for mutual respect of interdisciplinary team members by stressingthe uniqueness and importance of each team members’ roles and their responsibilitiesfor providing quality and comprehensive hospice services.
◊ Provide tools that increase trust and communication among team members
◊ Provide incentives to team members for taking efforts to increase collaboration.
• National social work and hospice organizations can:
◊ Develop and disseminate tools to hospice leaders and employees to fosterinterdisciplinary collaboration and team functioning.
◊ Advocate for federal agencies involved in hospice regulation and research to evaluatemethods for increasing interdisciplinary team functioning.
◊ Advocate for federal agencies involved in hospice regulation to stress interdisciplinarycollaboration and valuing different practice philosophies in developing comprehensiveplans of care.
• Hospice social worker researchers can:
◊ Conduct rigorous research and systematic reviews that evaluate elements of successfulinterdisciplinary team functioning.
◊ Engage in interdisciplinary research on hospice care to better understand the varyingtreatment philosophies in treatment planning and implementation. This research canalso help discover the reasons for gaps and challenges to interdisciplinarycollaboration in hospice care.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 20
th national hospice organizations and accrediting bodies torole of the social worker and the value it provides in hospice
rs can:
that incorporate evaluations of hospice social workert effectiveness.
tic research that examines the effectiveness and costcial workers at different level of qualification (e.g., MSW v.ial work degree, supervised v. not supervised, etc.).
plore and conclusively define the roles and responsibilities of
capturing and evaluating quality indicators related toan be useful to CMS’s development and implementation of
k that prepares social workers for a career in end-of-life
mation about hospice services into the curriculum.
rvices
cial work and hospice organizations can:
on of services and outreach to more ethnically and culturallygaging with members of the local community and othero educate them on the value of hospice.
family’s involvement in developing a plan of care, whichfamily’s cultural considerations of care.
e organizations to develop awareness campaigns geared attilizing hospice services to demonstrate the benefits of
es to increase access of services to populations not utilizing
es to seek out employees from diverse backgrounds to helps of their care teams.
al workers from diverse backgrounds to explore careers in
cial and ethnic disparities in both the hospice workforce andek to develop methods for adding cultural diversity to the
NKING POLICY, PRACTICE, AND RESEARCH REPORT
19
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 20

• Hospice social work researchers can:
◊ Develop relationships with CMS to regularly andoutcomes of research on hospice social work and
◊ Seek dissemination methods that will most effectiNASW member updates, webinars, tele-training,practice books, inclusion in newsletters, and othe
To Promote Collaborations with Federal Agencies
• Hospice social workers can:
◊ Engage with CMS surveyors to illustrate areas ofensure that quality indicators represent the servic
◊ Report concerns and violations of the regulationworkers are not asked to perform duties outside o
◊ Hospice agencies can work with CMS to developassess all areas of service delivery including psych
◊ Hospice social work researchers and national orgconnections for researchers with CMS to better inchanges.
Hospice is a patient and family-centered service delivery parainterdisciplinary collaboration and highlights the importancequality of life needs. Social workers are a key part of that serwill help not only those current and future social workers inpatients and families served by hospice as well.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
To Promote Research-Practice Linkages
• Hospice social workers can:
◊ Seek out connections with local or prominent hospice social work researchers to helporiginate relevant practice research questions and develop valuable and effectiveresearch methodologies.
◊ Maintain quality patient records that can be used in larger evaluations of hospicesocial work outcomes, and also in the social workers’ own practice evaluations.
◊ Develop strategies for conducting outcome evaluations in the agency and then usingthe findings to enhance practice.
• Hospice agencies can:
◊ Increase accessibility for practitioners to research journals.
◊ Provide incentives to clinicians that incorporate research into practice.
• National hospice social work organizations could incentivize credentials, such as theAdvanced Certified Hospice and Palliative Social Worker (ACHP-SW) by offering access tojournals targeted at social work in hospice and palliative care.
• Hospice social work researchers can:
◊ Incorporate practitioners in the research design process from the outset, including indevelopment of the research questions.
◊ Promote the use of community-based participatory research strategies.
◊ Structure journal articles to be geared toward implementation in or consideration forpractice.
To Promote Research on Hospice Social Work
• National hospice and social work organizations can:
◊ Advocate for increased funding from Congress to explore and enhance the social workrole in research (e.g. The National Center for Social Work Research Act, S.114).
◊ Develop a network of researchers that can collaborate to design high quality studiesthat may be more eligible for grant funding, and that would also increase the scale andrigor of the research.
◊ Promote the value of research to its members who are clinicians as essential forincreasing the value and legitimacy of the social work profession in hospice care.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 21
Psychosocial Outcomes
“Hospice is one (if not the only) area of health care in which psychosocial outcomes out shadow physiological outcomes in a profound anddemonstrable way. If the research bridge can be built, the standing of social work/psychosocial intervention in this and other areas ofhealth care will rise significantly.” — A think tank participant
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 21
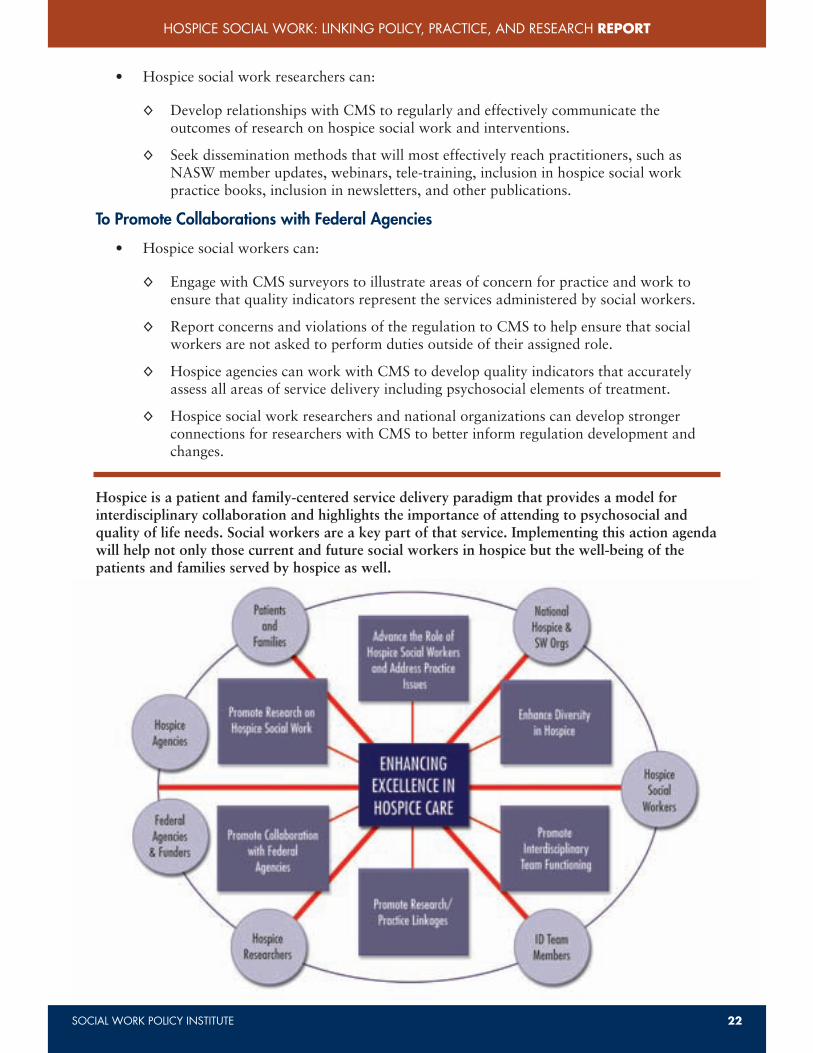
• Hospice social work researchers can:
◊ Develop relationships with CMS to regularly and effectively communicate theoutcomes of research on hospice social work and interventions.
◊ Seek dissemination methods that will most effectively reach practitioners, such asNASW member updates, webinars, tele-training, inclusion in hospice social workpractice books, inclusion in newsletters, and other publications.
To Promote Collaborations with Federal Agencies
• Hospice social workers can:
◊ Engage with CMS surveyors to illustrate areas of concern for practice and work toensure that quality indicators represent the services administered by social workers.
◊ Report concerns and violations of the regulation to CMS to help ensure that socialworkers are not asked to perform duties outside of their assigned role.
◊ Hospice agencies can work with CMS to develop quality indicators that accuratelyassess all areas of service delivery including psychosocial elements of treatment.
◊ Hospice social work researchers and national organizations can develop strongerconnections for researchers with CMS to better inform regulation development andchanges.
Hospice is a patient and family-centered service delivery paradigm that provides a model forinterdisciplinary collaboration and highlights the importance of attending to psychosocial andquality of life needs. Social workers are a key part of that service. Implementing this action agendawill help not only those current and future social workers in hospice but the well-being of thepatients and families served by hospice as well.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 22
ages
local or prominent hospice social work researchers to helpresearch questions and develop valuable and effective
ecords that can be used in larger evaluations of hospiced also in the social workers’ own practice evaluations.
ducting outcome evaluations in the agency and then usingactice.
ractitioners to research journals.
cians that incorporate research into practice.
organizations could incentivize credentials, such as thend Palliative Social Worker (ACHP-SW) by offering access tok in hospice and palliative care.
rs can:
n the research design process from the outset, including inch questions.
unity-based participatory research strategies.
o be geared toward implementation in or consideration for
ocial Work
ork organizations can:
nding from Congress to explore and enhance the social workNational Center for Social Work Research Act, S.114).
earchers that can collaborate to design high quality studiesfor grant funding, and that would also increase the scale and
arch to its members who are clinicians as essential foregitimacy of the social work profession in hospice care.
NKING POLICY, PRACTICE, AND RESEARCH REPORT
21
in which psychosocial outcomes out shadow physiological outcomes in a profound andlt, the standing of social work/psychosocial intervention in this and other areas ofarticipant
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 22

APPENDIXAppendix A: List of Participants
Appendix B: Symposium Agenda
Appendix C: Presenter Biographies
Appendix D: Social Security Act – Hospice Section
Appendix E: CMS Conditions of Participation
Appendix F: CMS Quality Assessment and Performance Im
Appendix G: CMS Approved Hospice Deemed Status Progr
Appendix H: NHPCO Standards for Practice
Appendix I: NASW Standards for Palliative and End-of-Li
Appendix J: Credentials and Training for Hospice Social W
Appendix K: Citations for “Current Status of Social Work R
Appendix L: Annotated Bibliography
Appendix M: Hospice Resources
Appendix N: Pending Legislation
Appendix O: Social Work Researchers on End-of-Life CareFellows)
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
REFERENCESHFA [Hospice Foundation of America]. (n.d.) What is Hospice. Retrieved from
www.hospicefoundation.org/pages/page.asp?page_id=47055.
Cicely Saunders International. (n.d). Dame Cicely Saunders Biography. Retrieved fromwww.cicelysaundersfoundation.org/about-us/dame-cicely-biography.
Medicare and Medicaid Programs: Hospice Conditions of Participation; Final Rule, 73 Fed.Reg. 32159-31260; 32218 (2008) (to be codified at 42 C.F.R. pt. 418).
NASW Center for Workforce Studies. (2006). Assuring the Sufficiency of a Frontline Workforce:A National Study of Licensed Social Workers – Special Report: Social Work Services inHealth Care Settings. Washington, DC: NASW. Retrieved fromhttp://workforce.socialworkers.org/studies/prac_area.asp#health.
National Hospice and Palliative Care Organization. (2009). NHPCO Facts and Figures:Hospice Care in America. Retrieved from: www.nhpco.org/files/public/Statistics_Research/NHPCO_facts_and_figures.pdf.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 23
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 23
APPENDIXAppendix A: List of Participants
Appendix B: Symposium Agenda
Appendix C: Presenter Biographies
Appendix D: Social Security Act – Hospice Section
Appendix E: CMS Conditions of Participation
Appendix F: CMS Quality Assessment and Performance Improvement (QAPI)
Appendix G: CMS Approved Hospice Deemed Status Programs
Appendix H: NHPCO Standards for Practice
Appendix I: NASW Standards for Palliative and End-of-Life Care
Appendix J: Credentials and Training for Hospice Social Workers
Appendix K: Citations for “Current Status of Social Work Research” Section
Appendix L: Annotated Bibliography
Appendix M: Hospice Resources
Appendix N: Pending Legislation
Appendix O: Social Work Researchers on End-of-Life Care (Hartford Scholars and DoctoralFellows)
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 24
a]. (n.d.) What is Hospice. Retrieved fromages/page.asp?page_id=47055.
Dame Cicely Saunders Biography. Retrieved fromn.org/about-us/dame-cicely-biography.
ospice Conditions of Participation; Final Rule, 73 Fed.08) (to be codified at 42 C.F.R. pt. 418).
(2006). Assuring the Sufficiency of a Frontline Workforce:Social Workers – Special Report: Social Work Services inton, DC: NASW. Retrieved froms.org/studies/prac_area.asp#health.
Organization. (2009). NHPCO Facts and Figures:rieved from: www.nhpco.org/files/public/acts_and_figures.pdf.
NKING POLICY, PRACTICE, AND RESEARCH REPORT
23
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 24
Judi Lund Person, MPHVice-PresidentCompliance and Regulatory LeadershipNational Hospice and Palliative Care Organization
Jeri Miller, PhDHeadNINR Office of End-of-Life Palliative Care Science,Investigator Training, and EducationNational Institute of Nursing Research
Sherri Morgan, JD, MSWAssociate CounselLDF and Office of Ethics and Professional ReviewNational Association of Social Workers
Rebecca Myers, LSW, ACSWDirectorExternal RelationsNational Association of Social Workers
Bekki Ow-Arhus, ACSW, DCSW, C-ACYFSWSenior Practice AssociateProfessional DevelopmentNational Association of Social Workers
Debra Parker Oliver, PhD, MSWAssociate ProfessorRural Sociology, Social WorkUniversity of Missouri
Judith Peres, MSW, LCSW-CSupporting Successful Transitions
Kim Roche, BSN, MANurse ConsultantSurvey and Certification GroupCenters for Medicare and Medicaid Services
Mary Rossi-Coajou, MS, RNCaptain, U.S. Public Health ServiceSenior Nurse ConsultantCenters for Medicare and Medicaid Services
Annette SchmidtDirectorU.S. External Affairssanofi-aventis U.S.
Tracy SchroAssistant ProSchool of SoUniversity of
J. Donald SPresident &National Ho
Danielle ShSenior HealtCenters for M
Deborah WAssociate ProSchool of SoUniversity at
Karyn WalsSenior PractiCenter for WNational Ass
Briana WalMSW InternSocial WorkNational Ass
Jennifer WaAssistant DirNational Ass
Sherri WeisAssociate ClHospice of th
Tracy WhitaDirectorCenter for WNational Ass
Gail WoodsDirector of CNational Ass
Joan Levy ZDirectorSocial WorkNational Ass
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
Suzanne Adelman, DCSWClinical SupervisorHospice of Jewish Social Services Agency
Robert Arnold, MPSDirectorNational Association of Social Workers Foundation
Samira Beckwith, ACSW, LCSW, FACHEPresident & CEOHope Hospice
Pamela Bennett, RNExecutive Director of Healthcare Alliance DevelopmentPurdue Pharma
Kathy Brandt, MSVice PresidentInnovation and AccessNational Hospice and Palliative Care Organization
Laura Bronstein, PhD, ACSWAssociate Professor & Department ChairCollege of Community and Public AffairsBinghamton University
Gretchen Brown, MSWBoard ChairNational Hospice and Palliative Care OrganizationPresident & CEOHospice of the Bluegrass - Lexington
Karen Bullock, PhDAssociate ProfessorSchool of Social WorkUniversity of Connecticut
Elizabeth J. Clark, PhD, ACSW, MPHExecutive DirectorNational Association of Social Workers
Paul Clark, PhDAssistant ProfessorDepartment of Social WorkGeorge Mason University
Mirean Coleman, MSW, LICSWSenior Practice Associate – Clinical Social WorkCenter for Workforce Studies and Social Work PracticeNational Association of Social Workers
Stacy Collins, MSWSenior Practice Associate – Children and Adolescent
HealthCenter for Workforce Studies and Social Work PracticeNational Association of Social Workers
Deirdre Downes, MSW, LCSWSocial Work ManagerJewish Home Life Care
Michael FrancumMSW InternNational Association of Social Workers
Ronald FriedVice-PresidentPublic AffairsVITAS Innovative Hospice Care
Barbara Guest, MSW, MPHProgram AnalystOffice of the Associate DirectorNational Cancer Institute
Bernice Harper, MSW, MSPh, LLDNASW Pioneer
Chris Herman, MSW, LICSWSenior Practice Associate – AgingCenter for Workforce Studies and Social Work PracticeNational Association of Social Workers
Elizabeth Hoffler, MSW, ACSWSpecial Assistant to the Executive DirectorLobbyistNational Association of Social Workers
Ayisha JonesMSW InternNational Association of Social Workers
James J. Kelly, PhD, ACSWPresidentNational Association of Social Workers
Donald List, LCSW-CPalliative Care Social WorkerThe Harry J. Duffey Family Pain and Palliative
Care ProgramJohns Hopkins Medicine
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 25
APPENDIX A: PARTICIPANT LIST
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 25

Judi Lund Person, MPHVice-PresidentCompliance and Regulatory LeadershipNational Hospice and Palliative Care Organization
Jeri Miller, PhDHeadNINR Office of End-of-Life Palliative Care Science,Investigator Training, and EducationNational Institute of Nursing Research
Sherri Morgan, JD, MSWAssociate CounselLDF and Office of Ethics and Professional ReviewNational Association of Social Workers
Rebecca Myers, LSW, ACSWDirectorExternal RelationsNational Association of Social Workers
Bekki Ow-Arhus, ACSW, DCSW, C-ACYFSWSenior Practice AssociateProfessional DevelopmentNational Association of Social Workers
Debra Parker Oliver, PhD, MSWAssociate ProfessorRural Sociology, Social WorkUniversity of Missouri
Judith Peres, MSW, LCSW-CSupporting Successful Transitions
Kim Roche, BSN, MANurse ConsultantSurvey and Certification GroupCenters for Medicare and Medicaid Services
Mary Rossi-Coajou, MS, RNCaptain, U.S. Public Health ServiceSenior Nurse ConsultantCenters for Medicare and Medicaid Services
Annette SchmidtDirectorU.S. External Affairssanofi-aventis U.S.
Tracy Schroepfer, PhDAssistant ProfessorSchool of Social WorkUniversity of Wisconsin-Madison
J. Donald Schumacher, PsyDPresident & CEONational Hospice and Palliative Care Organization
Danielle ShearerSenior Health Insurance SpecialistCenters for Medicare and Medicaid Services
Deborah Waldrop, PhD, MSWAssociate ProfessorSchool of Social WorkUniversity at Buffalo
Karyn Walsh, MSW, LCSW, ACSWSenior Practice Associate – Health, Cancer, & WebEdCenter for Workforce Studies and Social Work PracticeNational Association of Social Workers
Briana WaltersMSW InternSocial Work Policy InstituteNational Association of Social Workers Foundation
Jennifer WattAssistant DirectorNational Association of Social Workers Foundation
Sherri Weisenfluh, MSW, LCSW, ACHP-SWAssociate Clinical Officer of Counseling ServicesHospice of the Bluegrass
Tracy Whitaker, DSWDirectorCenter for Workforce Studies and Social Work PracticeNational Association of Social Workers
Gail Woods-Waller, MSDirector of CommunicationsNational Association of Social Workers
Joan Levy Zlotnik, PhD, ACSWDirectorSocial Work Policy InstituteNational Association of Social Workers Foundation
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 26
dation
elopment
ation
ation
rkPractice
Stacy Collins, MSWSenior Practice Associate – Children and Adolescent
HealthCenter for Workforce Studies and Social Work PracticeNational Association of Social Workers
Deirdre Downes, MSW, LCSWSocial Work ManagerJewish Home Life Care
Michael FrancumMSW InternNational Association of Social Workers
Ronald FriedVice-PresidentPublic AffairsVITAS Innovative Hospice Care
Barbara Guest, MSW, MPHProgram AnalystOffice of the Associate DirectorNational Cancer Institute
Bernice Harper, MSW, MSPh, LLDNASW Pioneer
Chris Herman, MSW, LICSWSenior Practice Associate – AgingCenter for Workforce Studies and Social Work PracticeNational Association of Social Workers
Elizabeth Hoffler, MSW, ACSWSpecial Assistant to the Executive DirectorLobbyistNational Association of Social Workers
Ayisha JonesMSW InternNational Association of Social Workers
James J. Kelly, PhD, ACSWPresidentNational Association of Social Workers
Donald List, LCSW-CPalliative Care Social WorkerThe Harry J. Duffey Family Pain and Palliative
Care ProgramJohns Hopkins Medicine
NKING POLICY, PRACTICE, AND RESEARCH REPORT
25
ANT LIST
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 26
1:45 PM Report Out on Gaps, Challenges, and Emerging
2:15 PM PART 3: DEVELOPING AN ACTION PLAN
Action Planning Work Groups
• Building the Science – Agenda and Research
• National Collaborations and Partnerships
• Creating Research-Practice Bridges
• Implications and Recommendations for Polic
3:00 PM Break
3:15 PM Report Out and Identification of Action Steps an
3:45 PM Wrap-up & Next Steps
4:00 PM Adjourn
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
APPENDIX B: SYMPOSIUM AGENDAThursday, March 25, 2010NASW National Office7th Floor Conference Center
8:30 AM REGISTRATION & CONTINENTAL BREAKFAST
9:00 AM GREETINGS & INTRODUCTIONS
Joan Levy Zlotnik, PhD, ACSW, Director, Social Work Policy InstituteElizabeth J. Clark, PhD, ACSW, MPH, Executive Director, National Association ofSocial WorkersGretchen Brown, MSW, Chair, National Hospice and Palliative Care Organization
9:30 AM PART 1: FRAMING THE ISSUES
Building Comprehensive Community-Based End-of-Life Care – Social WorkContributions and Challenges for the Future
Samira Beckwith, ACSW, Hope Hospice, Fort Myers, FloridaRonald Fried, Vitas Innovative Hospice Care, Washington, DC
Social Work’s Role in Hospice – An Overview of ResearchDeborah Waldrop, PhD, School of Social Work, University at Buffalo
Promoting the High Quality Psychosocial Care in HospiceMary Rossi-Coajou, MS, RN & Danielle Shearer,Centers for Medicare and Medicaid Services, Office of Standards and Quality
11:00 AM Break
11:15 AM Questions and Discussion
11:45 AM Overview of NASW Hospice and Palliative Care Resources and ActivitiesElizabeth J. Clark, PhD, ACSW, MPH
12:00 PM Lunch (Provided)
12:45 PM PART 2: IDENTIFYING GAPS, CHALLENGES, AND EMERGING PRACTICES
Roundtable Facilitated Discussions
• Current Status of Hospice Psychosocial Research – Answered and UnansweredQuestions
• Emerging Practices in End-of-Life Care – Opportunities for Social Work
• Enhancing Social Worker’s Role on the Interdisciplinary Team
• Enhancing Researcher/Practitioner/Policy Connections
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 27
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 27

1:45 PM Report Out on Gaps, Challenges, and Emerging Practices for Hospice Social Workers
2:15 PM PART 3: DEVELOPING AN ACTION PLAN
Action Planning Work Groups
• Building the Science – Agenda and Research Training
• National Collaborations and Partnerships
• Creating Research-Practice Bridges
• Implications and Recommendations for Policy
3:00 PM Break
3:15 PM Report Out and Identification of Action Steps and Targets
3:45 PM Wrap-up & Next Steps
4:00 PM Adjourn
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 28
UM AGENDA
NTINENTAL BREAKFAST
DUCTIONS
ACSW, Director, Social Work Policy InstituteACSW, MPH, Executive Director, National Association of
Chair, National Hospice and Palliative Care Organization
E ISSUES
Community-Based End-of-Life Care – Social Workenges for the FutureCSW, Hope Hospice, Fort Myers, Floridannovative Hospice Care, Washington, DC
spice – An Overview of ResearchhD, School of Social Work, University at Buffalo
lity Psychosocial Care in HospiceMS, RN & Danielle Shearer,
e and Medicaid Services, Office of Standards and Quality
n
pice and Palliative Care Resources and ActivitiesACSW, MPH
GAPS, CHALLENGES, AND EMERGING PRACTICES
iscussions
spice Psychosocial Research – Answered and Unanswered
End-of-Life Care – Opportunities for Social Work
rker’s Role on the Interdisciplinary Team
r/Practitioner/Policy Connections
NKING POLICY, PRACTICE, AND RESEARCH REPORT
27
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 28

Deborah Waldrop, PhD, LMSW
Deborah Waldrop, PhD, LMSW is an Associate Professor at tSocial Work. Deborah joined the UBSSW faculty after spendivariety of healthcare settings. Drawing from the experiencesfamilies Dr. Waldrop now conducts research about the needsend. Deborah is currently studying how people make decisiontiming of that decision. She is also involved in an ongoing decare, a newly emerging model for care at life’s end.
Captain Mary Rossi-Coajou, MS, RN
Captain Mary Rossi-Coajou serves as a Senior Nurse Consuland Medicaid Services (CMS), Office of Clinical Standards andegree in Science and Nursing from the State University of Ndegree in Community Health from the University of MarylanFederal service in 1989 at the National Institutes of Health, Bin the areas of occupational health, clinical staff nursing, nuris currently employed at CMS, Baltimore office as a senior nuhospice and community mental health programs, were she isParticipation (CoPs).
Danielle Shearer
Danielle Shearer is a senior health insurance specialist at theServices. She has worked with the Medicare hospice programproposed and final hospice rules, teaching hospice surveyors,develop hospice quality measures. Danielle is also responsibleAgency CoPs and Life Safety Code CoPs for all Medicare andfacilities.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
APPENDIX C: PRESENTER BIOGRAPHIES
Samira Beckwith, ACSW, LCSW, FACHE
Samira K. Beckwith, ACSW, LCSW, FACHE, has over 30 years’ experience in professional healthcare and social services. She has served as President and CEO of Hope Healthcare Services, basedin Fort Myers, Florida, since 1991. When she joined Hope, the agency was caring for a smallnumber of hospice patients in the immediate Fort Myers area. Under her leadership, Hope hascreated an array of services for the frail elderly and children and today serves more than 2,200people and their families in a 10,000 square-mile area throughout southwest and mid-Florida. Sheearned her BA in Sociology and Master’s in Social Work at The Ohio State University. Ms.Beckwith has become a leader in improving and advancing health care on the local, state andnational levels. She has broadened the continuum of health care, enabling adults to livecomfortably and with dignity through old age and into the final chapter of life. Former GovernorJeb Bush appointed Samira to the state’s Long-Term Care Policy Board and she is a frequentparticipant in national health policy forums and has provided expert testimony before governmentbodies including the US House Judiciary Committee. Ms. Beckwith is serving for a third time onthe Board of the National Hospice and Palliative Care Organization and is the 2009 recipient ofthe NASW Foundation’s Knee/Wittman Lifetime Achievement Award for Health & Mental HealthPractice.
Ronald Fried
Ron Fried brings more than 15 years of hospice management and administrative responsibilitiesand more than 30 years of experience in legislative and regulatory affairs to his role as Senior VicePresident of Development and Public Affairs for VITAS Innovative Hospice Care. Ron identifiesand develops partnership opportunities with hospices around the country. In addition, he handlesstrategic growth opportunities, such as relationships with health care providers that complementVITAS’ service such as disease management and palliative care. Ron also oversees public policyissues for VITAS and manages those activities at both the state and federal level. Ron serves on theBoards of Directors of the National Hospice and Palliative Care Organization and FloridaHospices and Palliative Care. He is a member of the Executive Committee for each organization.Ron brings to VITAS more than 15 years of experience in domestic and international strategicdevelopment, including eight years previously spent with VITAS – first, as a public policyconsultant and, subsequently, as Director of Development. Ron’s areas of expertise includestrategic business planning, public policy, acquisition strategy, analysis, negotiation and operationsintegration. Ron served as Director of Development for VITAS from 1992-1997 and providedpublic policy guidance to VITAS from 1988-1992. During his tenure, VITAS successfully addedthe California hospice programs—formerly known as Community Hospice Care—as well asHospice of Miami Valley in Cincinnati and Florida’s first not for profit hospice program, Hospiceof Central Florida in Orlando. Those programs have continued to grow as a part of VITAS andtoday care for more than 3,000 patients and families each day. Early in Ron’s career, he served onCapitol Hill as Legislative Assistant to Congressman Claude Pepper, public health policy advisorto former Florida Governor Bob Graham and National Finance Director for Senator Bob Kerrey’s1992 Presidential Campaign. Ron received his bachelor’s degree in government and politics fromthe University of Maryland in College Park, MD.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 29
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 29

Deborah Waldrop, PhD, LMSW
Deborah Waldrop, PhD, LMSW is an Associate Professor at the University at Buffalo School ofSocial Work. Deborah joined the UBSSW faculty after spending 20 years as a social worker in avariety of healthcare settings. Drawing from the experiences of older adult patients and theirfamilies Dr. Waldrop now conducts research about the needs and concerns that emerge at life’send. Deborah is currently studying how people make decisions about hospice utilization and thetiming of that decision. She is also involved in an ongoing descriptive study of residential hospicecare, a newly emerging model for care at life’s end.
Captain Mary Rossi-Coajou, MS, RN
Captain Mary Rossi-Coajou serves as a Senior Nurse Consultant with the Centers for Medicareand Medicaid Services (CMS), Office of Clinical Standards and Quality. She holds a Baccalaureatedegree in Science and Nursing from the State University of New York at Brockport and a Mastersdegree in Community Health from the University of Maryland. CAPT Rossi-Coajou began herFederal service in 1989 at the National Institutes of Health, Bethesda Maryland. She has workedin the areas of occupational health, clinical staff nursing, nurse manager, and nurse consultant. Sheis currently employed at CMS, Baltimore office as a senior nurse consultant and analyst for thehospice and community mental health programs, were she is responsible for the Conditions ofParticipation (CoPs).
Danielle Shearer
Danielle Shearer is a senior health insurance specialist at the Centers for Medicare & MedicaidServices. She has worked with the Medicare hospice program for the past seven years, drafting theproposed and final hospice rules, teaching hospice surveyors, and managing a special project todevelop hospice quality measures. Danielle is also responsible for writing the Home HealthAgency CoPs and Life Safety Code CoPs for all Medicare and Medicaid-certified health carefacilities.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 30
ER BIOGRAPHIES
ACHE
ACHE, has over 30 years’ experience in professional healthd as President and CEO of Hope Healthcare Services, basedhen she joined Hope, the agency was caring for a small
mediate Fort Myers area. Under her leadership, Hope hasil elderly and children and today serves more than 2,200square-mile area throughout southwest and mid-Florida. Sheer’s in Social Work at The Ohio State University. Ms.oving and advancing health care on the local, state andcontinuum of health care, enabling adults to liveold age and into the final chapter of life. Former Governor
e’s Long-Term Care Policy Board and she is a frequentorums and has provided expert testimony before governmentary Committee. Ms. Beckwith is serving for a third time ond Palliative Care Organization and is the 2009 recipient ofan Lifetime Achievement Award for Health & Mental Health
of hospice management and administrative responsibilitiesin legislative and regulatory affairs to his role as Senior ViceAffairs for VITAS Innovative Hospice Care. Ron identifieses with hospices around the country. In addition, he handless relationships with health care providers that complementement and palliative care. Ron also oversees public policyctivities at both the state and federal level. Ron serves on the
Hospice and Palliative Care Organization and Floridamember of the Executive Committee for each organization.ars of experience in domestic and international strategiceviously spent with VITAS – first, as a public policyctor of Development. Ron’s areas of expertise includeicy, acquisition strategy, analysis, negotiation and operationsDevelopment for VITAS from 1992-1997 and provided1988-1992. During his tenure, VITAS successfully added
merly known as Community Hospice Care—as well asi and Florida’s first not for profit hospice program, Hospiceprograms have continued to grow as a part of VITAS and
nts and families each day. Early in Ron’s career, he served ono Congressman Claude Pepper, public health policy advisorham and National Finance Director for Senator Bob Kerrey’seived his bachelor’s degree in government and politics fromPark, MD.
NKING POLICY, PRACTICE, AND RESEARCH REPORT
29
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 30
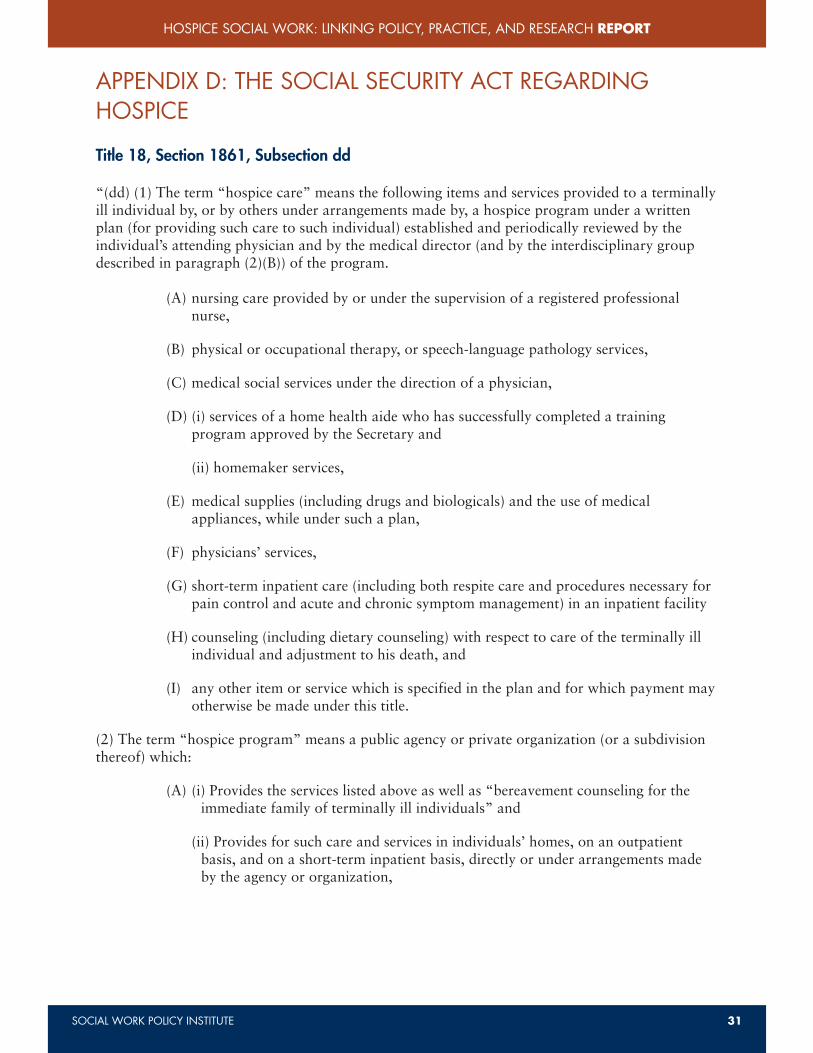
(B) has an interdisciplinary group of personnel wh
(I) one physician (as defined in subsection (r)(1))
(II) one registered professional nurse, and
(III) one social worker”
(3) (A) An individual is considered to be “terminally ill” if ththat the individual’s life expectancy is 6 months or less” (SociSection 1861,Subsection dd)
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
APPENDIX D: THE SOCIAL SECURITY ACT REGARDINGHOSPICE
Title 18, Section 1861, Subsection dd
“(dd) (1) The term “hospice care” means the following items and services provided to a terminallyill individual by, or by others under arrangements made by, a hospice program under a writtenplan (for providing such care to such individual) established and periodically reviewed by theindividual’s attending physician and by the medical director (and by the interdisciplinary groupdescribed in paragraph (2)(B)) of the program.
(A) nursing care provided by or under the supervision of a registered professionalnurse,
(B) physical or occupational therapy, or speech-language pathology services,
(C) medical social services under the direction of a physician,
(D) (i) services of a home health aide who has successfully completed a trainingprogram approved by the Secretary and
(ii) homemaker services,
(E) medical supplies (including drugs and biologicals) and the use of medicalappliances, while under such a plan,
(F) physicians’ services,
(G) short-term inpatient care (including both respite care and procedures necessary forpain control and acute and chronic symptom management) in an inpatient facility
(H) counseling (including dietary counseling) with respect to care of the terminally illindividual and adjustment to his death, and
(I) any other item or service which is specified in the plan and for which payment mayotherwise be made under this title.
(2) The term “hospice program” means a public agency or private organization (or a subdivisionthereof) which:
(A) (i) Provides the services listed above as well as “bereavement counseling for theimmediate family of terminally ill individuals” and
(ii) Provides for such care and services in individuals’ homes, on an outpatientbasis, and on a short-term inpatient basis, directly or under arrangements madeby the agency or organization,
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 31
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 31

(B) has an interdisciplinary group of personnel which—(i) includes at least—
(I) one physician (as defined in subsection (r)(1)),
(II) one registered professional nurse, and
(III) one social worker”
(3) (A) An individual is considered to be “terminally ill” if the individual has a medical prognosisthat the individual’s life expectancy is 6 months or less” (Social Security Act, 2008, Title 18,Section 1861,Subsection dd)
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 32
AL SECURITY ACT REGARDING
dd
ans the following items and services provided to a terminallyrangements made by, a hospice program under a writtenndividual) established and periodically reviewed by they the medical director (and by the interdisciplinary groupprogram.
by or under the supervision of a registered professional
al therapy, or speech-language pathology services,
under the direction of a physician,
health aide who has successfully completed a trainingthe Secretary and
s,
ding drugs and biologicals) and the use of medicalr such a plan,
are (including both respite care and procedures necessary forand chronic symptom management) in an inpatient facility
dietary counseling) with respect to care of the terminally illment to his death, and
ce which is specified in the plan and for which payment mayder this title.
ns a public agency or private organization (or a subdivision
s listed above as well as “bereavement counseling for theterminally ill individuals” and
are and services in individuals’ homes, on an outpatient-term inpatient basis, directly or under arrangements madeanization,
NKING POLICY, PRACTICE, AND RESEARCH REPORT
31
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 32

with the attending physician within 5 calendar days of the elecomprehensive assessments should be updated by the IDG asrequires and at a minimum of every 15 days.
Comprehensive assessments must include an evaluation of th
• Physical, psychosocial, emotional, and spiritual needs
• Nature and condition causing admission
• Complications and risk factors
• Functional status
• Imminence of death
• Symptom severity
• Drug profile
• Bereavement
• Referrals
Hospices organizations must include patient level data from eindividual patient outcomes. These data elements must be useevaluation and in the hospice’s quality assessment performanThe data elements collected must be documented in a consist
§ 418.56 Interdisciplinary group, care planning, and coordin
The interdisciplinary group (IDG) includes a doctor of medicworker, and a pastoral or other counselor and works togethefamily. The RN is tasked with coordinating care, ensuring coand family’s needs, and ensuring the implementation and reviof care is developed, it must include consultation with the attor representative, and the primary caregiver. All hospice serviplan of care, and patients and primary caregiver(s) are instrucresponsibilities. The plan of care should include:
• Patient and family goals
• Interventions for identified problems
• All services necessary for palliation and managementconditions
• Scope and frequency of services
• Measurable outcomes
• Drugs and treatments
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
APPENDIX E: CMS CONDITIONS OF PARTICIPATION
Conditions of Participation Development Process:
The CoPs were drafted during the regulation development period and then proceed to a clearanceprocess within CMS to ensure the new regulations concur with other CMS components. After aninternal review, the CoPs are approved and sent to regulatory clearance process within DHHS toensure that the CoPs concur by other department agencies and are then approved by the Secretaryof the DHHS. Finally, the Office of Management and Budget (OMB) reviews and approves theCoPs and are then published in the Federal Register.
Overview of the Conditions of Participation Requirements
The CoPs focus on enhancing patient rights; initial and comprehensive assessment of the patient;interdisciplinary group, care planning, and coordination of services; and quality assessment andperformance improvement.
§ 418.52 Patient’s rights
The patient must be given a notice of their rights and responsibilities during the initial assessmentvisit and in advance of furnishing care, both verbally and in writing in a language that the patientunderstand. The patient must also be informed about developing advanced directives and thenotice of rights and responsibilities must be signed by the patient or representative. Patients havethe right to exercise their rights, be treated with respect, voice grievances, and be protected fromdiscrimination or reprisal for exercising their rights. Hospices must immediately investigate allalleged violations and complaints, take appropriate corrective action, and report all verifiedviolations. The rights of the patient include:
• Pain management and symptom control
• Be involved in developing plan of care
• Refuse care or treatment
• Choose attending physician
• Confidential clinical record/ HIPAA
• Be free of abuse
• Receive information about hospice benefit
• Receive information about scope and limitations of hospice services
§ 418.54 Initial and comprehensive assessment of the patient
The patient must receive an initial assessment by a registered nurse (RN) within 48 hours of theelection of hospice care. Assessments are frequently done in conjunction with a social worker, butsocial workers are not required to be present during the initial assessment. Other members of theinterdisciplinary group (IDG), including social workers, may visit the patient prior to the nurse’sassessment. A comprehensive assessment must be completed by the hospice IDG in consultation
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 33
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 33
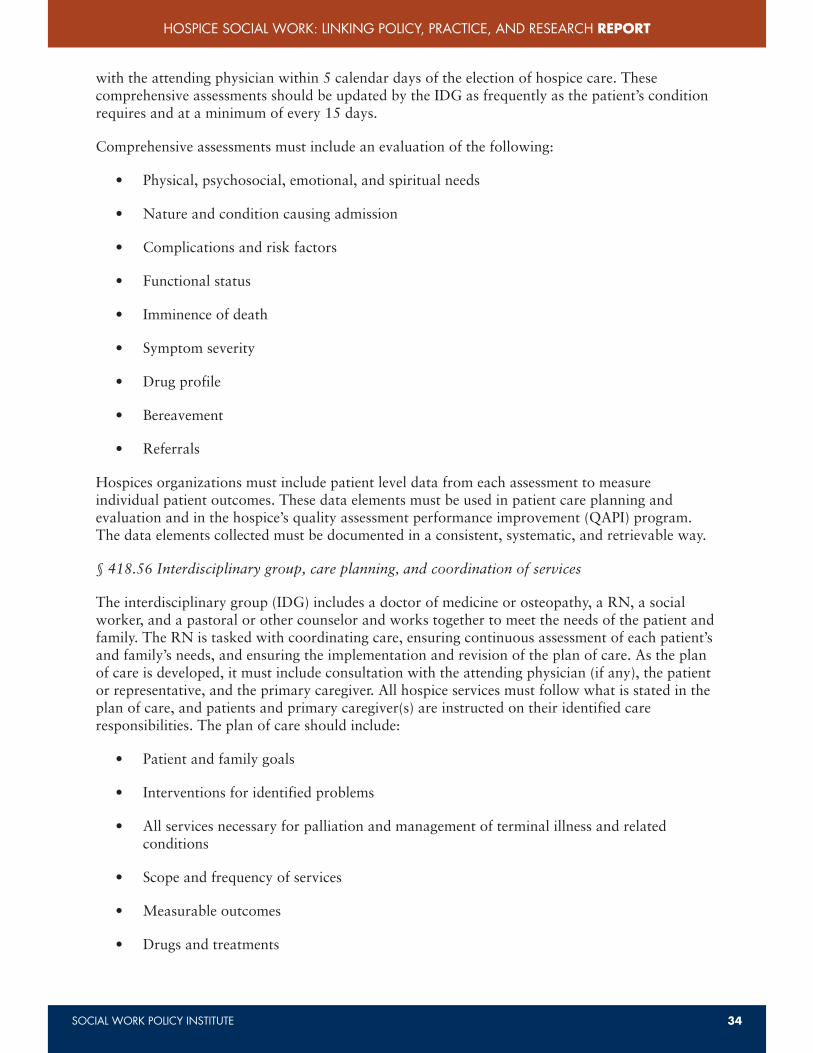
with the attending physician within 5 calendar days of the election of hospice care. Thesecomprehensive assessments should be updated by the IDG as frequently as the patient’s conditionrequires and at a minimum of every 15 days.
Comprehensive assessments must include an evaluation of the following:
• Physical, psychosocial, emotional, and spiritual needs
• Nature and condition causing admission
• Complications and risk factors
• Functional status
• Imminence of death
• Symptom severity
• Drug profile
• Bereavement
• Referrals
Hospices organizations must include patient level data from each assessment to measureindividual patient outcomes. These data elements must be used in patient care planning andevaluation and in the hospice’s quality assessment performance improvement (QAPI) program.The data elements collected must be documented in a consistent, systematic, and retrievable way.
§ 418.56 Interdisciplinary group, care planning, and coordination of services
The interdisciplinary group (IDG) includes a doctor of medicine or osteopathy, a RN, a socialworker, and a pastoral or other counselor and works together to meet the needs of the patient andfamily. The RN is tasked with coordinating care, ensuring continuous assessment of each patient’sand family’s needs, and ensuring the implementation and revision of the plan of care. As the planof care is developed, it must include consultation with the attending physician (if any), the patientor representative, and the primary caregiver. All hospice services must follow what is stated in theplan of care, and patients and primary caregiver(s) are instructed on their identified careresponsibilities. The plan of care should include:
• Patient and family goals
• Interventions for identified problems
• All services necessary for palliation and management of terminal illness and relatedconditions
• Scope and frequency of services
• Measurable outcomes
• Drugs and treatments
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 34
NDITIONS OF PARTICIPATION
pment Process:
ulation development period and then proceed to a clearancew regulations concur with other CMS components. After and and sent to regulatory clearance process within DHHS todepartment agencies and are then approved by the Secretaryanagement and Budget (OMB) reviews and approves thederal Register.
icipation Requirements
rights; initial and comprehensive assessment of the patient;, and coordination of services; and quality assessment and
their rights and responsibilities during the initial assessmente, both verbally and in writing in a language that the patientinformed about developing advanced directives and theust be signed by the patient or representative. Patients haveeated with respect, voice grievances, and be protected fromng their rights. Hospices must immediately investigate alle appropriate corrective action, and report all verifiedclude:
m control
n of care
IPAA
spice benefit
pe and limitations of hospice services
ssessment of the patient
essment by a registered nurse (RN) within 48 hours of theare frequently done in conjunction with a social worker, butpresent during the initial assessment. Other members of theng social workers, may visit the patient prior to the nurse’sent must be completed by the hospice IDG in consultation
NKING POLICY, PRACTICE, AND RESEARCH REPORT
33
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 34

APPENDIX F: CMS QUALITY ASSESSMPERFORMANCE IMPROVEMENT (QAP§ 418.58 Quality assessment and performance improvement
As the core of the patient-focused and outcome oriented revisParticipation, CMS developed the Quality Assessment and PeThe goal is to achieve desired outcomes by monitoring qualitopportunities for improvement, and making changes to achieoutcomes are specifically tied to the other regulations (e.g., pcomprehensive assessments, interdisciplinary group, care plan
QAPI operates on both a patient level and a hospice agency lto assess quality, use the data to identify opportunities for imperformance improvement in one or more areas. The goal is tclinical and managerial expertise and experience to drive decihospice agency level. CMS is currently testing multiple qualitservices that hospices may be able to use in their future QAPIQAPI collects data on an individual patient’s assessment/reaswith the goal of improving patient outcomes. The hospice levclinically focused aggregate data of the patients, and other dadata, administrative data, marketing data, etc. for the entire himproving clinical and non-clinical operations.
The method and quality of reporting by hospice social workeoutcomes of a hospice’s QAPI. Decreased access to electronicelectronic record formats can diminish the quality of recordsinterdisciplinary care files.
The hospice must ensure the development, implementation, aongoing, hospice-wide, data-driven QAPI program that:
• Reflects the complexity of its organization and service
• Involves all hospice services (including those services farrangement)
• Focuses on indicators related to palliative outcomes
• Takes actions to demonstrate improvement in hospice
Additionally, the hospice must maintain documentary evidento demonstrate its operation to CMS
• Program Scope
◊ Measure, analyze and track indicators to assess poperations
◊ Show measurable improvement in indicators of pservices
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
• Medical supplies and appliances
• Documentation of the patient’s or representative’s level of understanding, involvement andagreement with the plan of care
A revised plan of care includes information from the updated comprehensive assessment and trackprogress toward specified outcomes and goals and should be completed as frequently as thepatient’s condition requires, but no less frequently than every 15 calendar days. The hospice willcoordinate the services administered to the patient and should develop and maintain a system ofcommunication. The IDG is responsible for directing, coordinating, and supervising the care andservices provided, and ensuring that the plan of care is followed. Information about a patient’scondition and needs should be shared between all disciplines involved in care and with othernon-hospice healthcare providers.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 35
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 35
APPENDIX F: CMS QUALITY ASSESSMENT ANDPERFORMANCE IMPROVEMENT (QAPI)§ 418.58 Quality assessment and performance improvement
As the core of the patient-focused and outcome oriented revision of the Conditions ofParticipation, CMS developed the Quality Assessment and Performance Improvement (QAPI) CoP.The goal is to achieve desired outcomes by monitoring quality and performance, identifyingopportunities for improvement, and making changes to achieve improvement. These desiredoutcomes are specifically tied to the other regulations (e.g., patient’s rights, initial andcomprehensive assessments, interdisciplinary group, care planning, and coordination of services).
QAPI operates on both a patient level and a hospice agency level, both of which must collect datato assess quality, use the data to identify opportunities for improvement, and demonstrateperformance improvement in one or more areas. The goal is to use data in conjunction withclinical and managerial expertise and experience to drive decision making at the patient level andhospice agency level. CMS is currently testing multiple quality measures to evaluate hospiceservices that hospices may be able to use in their future QAPI efforts. The patient level portion ofQAPI collects data on an individual patient’s assessment/reassessment, care plan, and clinical noteswith the goal of improving patient outcomes. The hospice level portion of QAPI looks at theclinically focused aggregate data of the patients, and other data sources such as client satisfactiondata, administrative data, marketing data, etc. for the entire hospice agency with the goal ofimproving clinical and non-clinical operations.
The method and quality of reporting by hospice social workers will have a direct impact on theoutcomes of a hospice’s QAPI. Decreased access to electronic case files and inappropriateelectronic record formats can diminish the quality of records social workers can contribute tointerdisciplinary care files.
The hospice must ensure the development, implementation, and maintenance an effective,ongoing, hospice-wide, data-driven QAPI program that:
• Reflects the complexity of its organization and services
• Involves all hospice services (including those services furnished under contract orarrangement)
• Focuses on indicators related to palliative outcomes
• Takes actions to demonstrate improvement in hospice performance
Additionally, the hospice must maintain documentary evidence of its QAPI program and be ableto demonstrate its operation to CMS
• Program Scope
◊ Measure, analyze and track indicators to assess processes of care, hospice services andoperations
◊ Show measurable improvement in indicators of palliative outcomes and hospiceservices
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 36
es
s or representative’s level of understanding, involvement andre
ation from the updated comprehensive assessment and tracknd goals and should be completed as frequently as thess frequently than every 15 calendar days. The hospice willo the patient and should develop and maintain a system of
ble for directing, coordinating, and supervising the care andhe plan of care is followed. Information about a patient’sbetween all disciplines involved in care and with other
NKING POLICY, PRACTICE, AND RESEARCH REPORT
35
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 36
Two Levels of QAPI
• Patient-level QAPI: Individual patient’s outcomes or e
◊ Collect data on what happened for an individual
◊ Assessment/reassessment (§418.54)
◊ Care plan (§418.56)
◊ Clinical notes
◊ Use the data to improve quality of care and outco
• Hospice-Level QAPI
◊ Clinically focused
■ Aggregate (patient-level) data
■ Collect satisfaction data
◊ Non-clinically focused
■ Administrative data
■ Marketing - Referral source contact
■ Outreach to community
■ Profitability
■ Fundraising
• Data from both levels is used to improve clinical oper
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
• Program Data
◊ Collect data
■ Timing and detail approved by governing body
◊ Use data
■ Monitor effectiveness, safety of services, and quality of care
■ Identify opportunities and priorities for improvement
• Program activities
◊ The hospice’s performance improvement activities must:
■ Focus on high risk, high volume, problem prone areas affecting palliativeoutcomes, patient safety and quality of care (consider incidence, prevalence,severity)
■ Track adverse events; analyze causes and develop processes and training toprevent them
■ Take action to improve where and when necessary, AND measure (assess) toensure that improvement is sustained
• Performance improvement projects
◊ Number and scope must be based on needs, and reflect scope, complexity and pastperformance of hospice
◊ Document what, why and how successful (measurable improvement)
• Executive responsibilities
◊ QAPI program is defined, implemented and maintained
◊ Quality of care and patient safety priorities are identified and addressed effectively
◊ Individual(s) are designated to be responsible for operating the QAPI program
Other CoPs that Integrate QAPI
418.54 Comprehensive Assessment of the Patient (e) Standard: Patient outcome measures
418.60 Infection Control (b) Standard: Control
418.62 Licensed Professional Services (c) Licensed professionals must participate inthe hospice’s quality assessment andperformance improvement program
418.76 Hospice aide and homemaker services (g) Standard: Hospice aide assignments andduties
418.100 Organization and administration of (b) Standard: Governing body andservices administrator
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 37
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 37

Two Levels of QAPI
• Patient-level QAPI: Individual patient’s outcomes or events. Tasks include:
◊ Collect data on what happened for an individual patient
◊ Assessment/reassessment (§418.54)
◊ Care plan (§418.56)
◊ Clinical notes
◊ Use the data to improve quality of care and outcomes for that patient (§418.56)
• Hospice-Level QAPI
◊ Clinically focused
■ Aggregate (patient-level) data
■ Collect satisfaction data
◊ Non-clinically focused
■ Administrative data
■ Marketing - Referral source contact
■ Outreach to community
■ Profitability
■ Fundraising
• Data from both levels is used to improve clinical operations and non-clinical operations
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 38
proved by governing body
s, safety of services, and quality of care
s and priorities for improvement
e improvement activities must:
igh volume, problem prone areas affecting palliativefety and quality of care (consider incidence, prevalence,
; analyze causes and develop processes and training to
ve where and when necessary, AND measure (assess) toment is sustained
ojects
be based on needs, and reflect scope, complexity and past
how successful (measurable improvement)
implemented and maintained
nt safety priorities are identified and addressed effectively
ed to be responsible for operating the QAPI program
I
the Patient (e) Standard: Patient outcome measures
(b) Standard: Control
(c) Licensed professionals must participate inthe hospice’s quality assessment andperformance improvement program
services (g) Standard: Hospice aide assignments andduties
tion of (b) Standard: Governing body andadministrator
NKING POLICY, PRACTICE, AND RESEARCH REPORT
37
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 38
■ M9: Provision of interpreter or translator fopatients.
■ M10: Percentage of patients who had moderrating scale at any time in the last week of li
■ M11: Percentage of patients with chart docudiscussion that there is no advance directive.
■ M12: Selected number of occurrences per 10
– Four types of issues are tracked: falls, medicmalfunction, or error), and patient/family co
◊ The AIM Project is divided into 8 tasks and will r
1. A comprehensive literature review of existinend-of-life care.
2. An intervention package, including the apprcollection tools, and education and instructiQIOs can use to measure and improve the qpatients.
3. A report on the quality measures and data crelevant information for the quality measurenational consensus body.
4. A final report that describes the entire projecparticipating sites, challenges encountered anpossibilities for future hospice quality measu
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
QAPI Next Steps
• PEACE Project (Prepare. Embrace. Attend. Communicate. Empower.)
◊ Completed in February 2008
◊ Listed 34 suggested measures along with data definitions and a tool for data collection
◊ Available at www.medqic.org
◊ Completed by the Carolinas Center for Medical Excellence, the North Carolina QIO
• AIM Project (Assessment. Intervention. Measurement.)
◊ Uses the PEACE quality measures and a modified version of the PEACE datacollection tool to assess the quality of care in participating hospice sites, identify areasfor performance improvement, and measure quality of care improvements afterperformance improvement projects are implemented.
◊ Examines various factors related to the quality of the data collection tool and qualitymeasures in accordance with NQF standards.
◊ Identifies factors contributing to disparate and inequitable access to and use of hospiceservices.
◊ August 2009 – November 2010
◊ Conducted by IPRO, the New York State QIO
◊ Implemented in 7 hospices and 1 palliative care site within the state of New York thatvolunteered to participate in the project. The participating sites are representative ofhospices nationwide.
◊ AIM Project is testing 12 quality measures
■ M1: Percentage of patients admitted to hospice who had a screening forsymptoms during the admission visit.
■ M2: Percentage of patients who had a comprehensive assessment completedwithin 5 days of admission.
■ M3: For patients who screened positive for pain, the percentage whose pain wasat a comfortable level within 2 days of screening.
■ M4: For patients who screened positive for dyspnea, the percentage whoimproved within 1 day of screening.
■ M5: For patients who screened positive for nausea, the percentage of patientswho received treatment within 1 day of screening.
■ M6: Percentage of patients on opioids who have a bowel regimen initiated within1 day of opioid initiation.
■ M7: For patients who screened positive for anxiety, the percentage of patientswho received treatment within 2 weeks of diagnosis.
■ M8: Percentage of families reporting the hospice attended to family needs forinformation about medication, treatment, and symptoms.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 39
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 39
■ M9: Provision of interpreter or translator for non-English-speaking or deafpatients.
■ M10: Percentage of patients who had moderate to severe pain on a standardrating scale at any time in the last week of life.
■ M11: Percentage of patients with chart documentation of an advance directive ordiscussion that there is no advance directive.
■ M12: Selected number of occurrences per 1000 patient days
– Four types of issues are tracked: falls, medication errors, DME issues (complaint,malfunction, or error), and patient/family complaints
◊ The AIM Project is divided into 8 tasks and will result in 4 major products:
1. A comprehensive literature review of existing research related to disparities inend-of-life care.
2. An intervention package, including the appropriate quality measures, datacollection tools, and education and instruction materials, which hospices andQIOs can use to measure and improve the quality of care provided to hospicepatients.
3. A report on the quality measures and data collection tools that provides allrelevant information for the quality measure and tool endorsement process by anational consensus body.
4. A final report that describes the entire project, including the experiences ofparticipating sites, challenges encountered and overcome, lessons learned, andpossibilities for future hospice quality measure and improvement efforts.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 40
race. Attend. Communicate. Empower.)
008
ures along with data definitions and a tool for data collection
org
as Center for Medical Excellence, the North Carolina QIO
rvention. Measurement.)
measures and a modified version of the PEACE datae quality of care in participating hospice sites, identify areas
ment, and measure quality of care improvements aftert projects are implemented.
related to the quality of the data collection tool and qualityith NQF standards.
ting to disparate and inequitable access to and use of hospice
2010
New York State QIO
s and 1 palliative care site within the state of New York thatin the project. The participating sites are representative of
quality measures
atients admitted to hospice who had a screening foradmission visit.
atients who had a comprehensive assessment completedission.
o screened positive for pain, the percentage whose pain wasl within 2 days of screening.
o screened positive for dyspnea, the percentage whoay of screening.
o screened positive for nausea, the percentage of patientsent within 1 day of screening.
atients on opioids who have a bowel regimen initiated withintion.
o screened positive for anxiety, the percentage of patientsent within 2 weeks of diagnosis.
milies reporting the hospice attended to family needs foredication, treatment, and symptoms.
NKING POLICY, PRACTICE, AND RESEARCH REPORT
39
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 40
5. Step 5: Board of Review: A board will review the hospmaterials completed and make a final accreditation de
6. Step 6: Accreditation: If the hospice organization is apof accreditation and marketing materials.
Accreditation Commission for Health Care (ACHC)www.achc.org/index.php
ACHC has accreditation for programs in:
• Home Health
• Infusion Nursing
• Hospice
• Sleep Lab
• Home/Durable Medical Equipment Services
• Clinical Respiratory Care
• Medical Supply Provider
• Complex Rehabilitation and Assistive Technology Sup
• Fitter Services
• Pharmacy Services
• Non-Certified/Private Duty Program
• Private Duty Nursing
• Private Duty Aide
The accreditation process is as follows:
1. Determine if Program meets the Eligibility Criteria
◊ Your organization has been actively providing in-and has served a minimum of ten (10) clients withsubmitting an application.
◊ Your organization agrees to grant ACHC and/orrecords (including client and personnel) that are nwith the standards.
◊ Your organization agrees to pay fees according tofor Survey.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
APPENDIX G: CMS APPROVED HOSPICE DEEMED STATUSPROGRAMS
The Joint Commission’s 2010 Standards for Home Health, Personal Care and SupportServices, and Hospicewww.jcrinc.com/Accreditation-Manuals/2010-Standards-for-Home-Health-Personal-Care-and-Support-Services-and-Hospice/1826/
Since 1999, The Joint Commission has been the organization authorized to administeraccreditation for hospice programs in the United States. Accreditation is granted to programs thatare in compliance with the CMS’s Conditions of Participation and meet the Joint Commission’s2010 Standards for Home Health, Personal Care and Support Services, and Hospice. Theseaccreditation requirements focus on the following areas:
• Ethics, rights and responsibilities
• Provision of care, treatment, and services
• Medication management
• Surveillance, prevention, and control of infection
• Improving organization performance
• Leadership
• Environmental safety and equipment management
• Management of human resources
• Management of information
Community Health Accreditation Program (CHAP)www.chapinc.org/
CHAP has also been accrediting hospice programs since 1999. Their accreditation process involvesix steps:
Step 1: Application/Contract: An application and $500 fee are submitted and upon approval,an accreditation service agreement (contract) is sent back to the agency.
Step 2: Self Study: Core services and service-specific services are evaluated by the hospiceagency, using tools provided by CHAP. Additional documents and evaluations are requiredfor home health and hospice programs.
Step 3: CHAP will then assign a reviewer to conduct a site visit and take a census of thepatients being served.
Step 4: Plan of Correction: If any deficiencies or required actions are determined, the hospiceprogram receives a tool kit and has about 3-4 weeks to make corrections. Another site visitwill be conducted.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 41
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 41

5. Step 5: Board of Review: A board will review the hospice organization based on thematerials completed and make a final accreditation determination.
6. Step 6: Accreditation: If the hospice organization is approved, they will receive a certificateof accreditation and marketing materials.
Accreditation Commission for Health Care (ACHC)www.achc.org/index.php
ACHC has accreditation for programs in:
• Home Health
• Infusion Nursing
• Hospice
• Sleep Lab
• Home/Durable Medical Equipment Services
• Clinical Respiratory Care
• Medical Supply Provider
• Complex Rehabilitation and Assistive Technology Supplier
• Fitter Services
• Pharmacy Services
• Non-Certified/Private Duty Program
• Private Duty Nursing
• Private Duty Aide
The accreditation process is as follows:
1. Determine if Program meets the Eligibility Criteria
◊ Your organization has been actively providing in-home and/or alternate site servicesand has served a minimum of ten (10) clients with seven (7) active clients beforesubmitting an application.
◊ Your organization agrees to grant ACHC and/or its designated agent’s full access to allrecords (including client and personnel) that are necessary to ascertain compliancewith the standards.
◊ Your organization agrees to pay fees according to the terms specified in the Contractfor Survey.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 42
ROVED HOSPICE DEEMED STATUS
dards for Home Health, Personal Care and Support
nuals/2010-Standards-for-Home-Health-Personal-spice/1826/
s been the organization authorized to administerthe United States. Accreditation is granted to programs that
nditions of Participation and meet the Joint Commission’srsonal Care and Support Services, and Hospice. Thesehe following areas:
ies
nd services
control of infection
mance
pment management
ces
rogram (CHAP)
ice programs since 1999. Their accreditation process involve
pplication and $500 fee are submitted and upon approval,ment (contract) is sent back to the agency.
d service-specific services are evaluated by the hospicey CHAP. Additional documents and evaluations are requiredrograms.
viewer to conduct a site visit and take a census of the
deficiencies or required actions are determined, the hospiced has about 3-4 weeks to make corrections. Another site visit
NKING POLICY, PRACTICE, AND RESEARCH REPORT
41
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 42
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 43
◊ Your organization agrees to submit applications for all branch offices.
◊ Your organization must be operating within the United States and/or its territories.
2. Register for the ACHC Interpretive Guide for Accreditation Standards
3. Preparing your Preliminary Evidence Report (PER)
4. Submission of the Application, Deposit and PER
5. Fee Estimate and Contract
6. Scheduling the Survey (3-7 months)
7. Desk Review
8. On Site Survey. A survey agenda consists of the following:
◊ Opening Conference
◊ Tour of the Facility
◊ Company QI/Performance Improvement Presentation
◊ Review any PER correction (if applicable)
◊ Client/Patient Home Visits
◊ Client/Patient record reviews
◊ Personnel record reviews
◊ Interview with staff and management
◊ Exit conference
9. Scoring Your Survey and Decision. Outcomes:
◊ Accredited – Very minimal or no deficiencies found. Overall the company is compliantwith ACHC standards. Accreditation is granted, but a POC (Plan of Correction) forany deficiencies found must be developed and sent to your Account Manager within30 days.
◊ Deferred – Enough deficiencies that the company did not score high enough foraccreditation status. The company will have an opportunity to submit a POC (Plan ofCorrection) for all standards that were “partially met” or “not met” and this POCwill be reviewed by a clinical advisor. If all deficiencies have been resolved, thecompany will be granted accreditation.
◊ Denied – Many severe deficiencies that cause a company to be outside of the deferredrange. In this instance, the company is out of compliance with ACHC standards andmust re-apply for accreditation. All fees and application documents must bere-submitted in order to re-apply.
10. Accreditation Status
11. Renewal
APPENDIX H: NHPCO STANDARDS FO
National Hospice and Palliative Care Organization (NHPwww.nhpco.org/i4a/pages/Index.cfm?pageID=4900
1. Patient and Family Centered Care: Providing care andneeds and exceed the expectations of those we serve.
2. Ethical Behavior and Consumer Rights: Upholding hiadvocating for the rights of the patients and family ca
3. Clinical Excellence and Safety: Ensuring clinical excelstandards of practice.
4. Inclusion and Access: Promoting inclusiveness in ourpeople - regardless of race, ethnicity, color, religion, gage, disease or other characteristics – have access to o
5. Organizational Excellence: Building a culture of qualorganization that values collaboration and communicpractices.
6. Workforce Excellence: Fostering a collaborative, interpromotes inclusion, individual accountability and woprofessional development, training, and support to al
7. Standards: Adopting the NHPCO Standards for HospConsensus Project’s Clinical Practice Guidelines for Qfoundation for our organization.
8. Compliance with Laws and Regulations: Ensuring coregulations, and professional standards of practice, imthat prevent fraud and abuse.
9. Stewardship and Accountability: Developing a qualifiand senior leadership who share the responsibilities o
10. Performance Measurement: Collecting, analyzing, andmeasurement data to foster quality and performanceservices.
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 43

HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 44
NKING POLICY, PRACTICE, AND RESEARCH REPORT
43
to submit applications for all branch offices.
e operating within the United States and/or its territories.
retive Guide for Accreditation Standards
idence Report (PER)
, Deposit and PER
nths)
da consists of the following:
e Improvement Presentation
n (if applicable)
s
ws
management
sion. Outcomes:
l or no deficiencies found. Overall the company is compliantccreditation is granted, but a POC (Plan of Correction) forst be developed and sent to your Account Manager within
ncies that the company did not score high enough forcompany will have an opportunity to submit a POC (Plan ofrds that were “partially met” or “not met” and this POCcal advisor. If all deficiencies have been resolved, theaccreditation.
iciencies that cause a company to be outside of the deferrede company is out of compliance with ACHC standards andation. All fees and application documents must bee-apply.
APPENDIX H: NHPCO STANDARDS FOR PRACTICE
National Hospice and Palliative Care Organization (NHPCO) Standards for Practicewww.nhpco.org/i4a/pages/Index.cfm?pageID=4900
1. Patient and Family Centered Care: Providing care and services that are responsive to theneeds and exceed the expectations of those we serve.
2. Ethical Behavior and Consumer Rights: Upholding high standards of ethical conduct andadvocating for the rights of the patients and family caregivers.
3. Clinical Excellence and Safety: Ensuring clinical excellence and promoting safety throughstandards of practice.
4. Inclusion and Access: Promoting inclusiveness in our community by ensuring that allpeople - regardless of race, ethnicity, color, religion, gender, disability, sexual orientation,age, disease or other characteristics – have access to our programs and services.
5. Organizational Excellence: Building a culture of quality and accountability within ourorganization that values collaboration and communication and ensures ethical businesspractices.
6. Workforce Excellence: Fostering a collaborative, interdisciplinary environment thatpromotes inclusion, individual accountability and workforce excellence, throughprofessional development, training, and support to all staff and volunteers.
7. Standards: Adopting the NHPCO Standards for Hospice Programs and/or the NationalConsensus Project’s Clinical Practice Guidelines for Quality Palliative Care as thefoundation for our organization.
8. Compliance with Laws and Regulations: Ensuring compliance with applicable laws,regulations, and professional standards of practice, implementing systems and processesthat prevent fraud and abuse.
9. Stewardship and Accountability: Developing a qualified and diverse governance structureand senior leadership who share the responsibilities of fiscal and managerial oversight.
10. Performance Measurement: Collecting, analyzing, and actively using performancemeasurement data to foster quality and performance improvement in all areas of care andservices.
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 44

10. Continuing Education – Social workers shall assume pcontinued professional development in accordance wiContinuing Professional Education (NASW, 2002) an
11. Supervision, Leadership, and Training – Social workeof life care should lead educational, supervisory, admiindividuals, groups, and organizations.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
APPENDIX I: NASW STANDARDS FOR PALLIATIVE ANDEND-OF-LIFE CARE
National Association of Social Workers Standards for Palliative and End-of-Life Carewww.socialworkers.org/practice/bereavement/standards/default.asp
The NASW has eleven standards for practitioners working in palliative and end of life care:
1. Ethics and Values – The values, ethics, and standards of both the profession andcontemporary bioethics shall guide social workers practicing in palliative and end of lifecare. The NASW Code of Ethics (NASW, 2000) is one of several essential guides to ethicaldecision making and practice.
2. Knowledge – Social workers in palliative and end of life care shall demonstrate a workingknowledge of the theoretical and biopsychosocial factors essential to effectively practicewith clients and professionals.
3. Assessment – Social workers shall assess clients and include comprehensive information todevelop interventions and treatment planning.
4. Intervention/Treatment Planning – Social workers shall incorporate assessments indeveloping and implementing intervention plans that enhance the clients’ abilities anddecisions in palliative and end of life care.
5. Attitude/Self-Awareness – Social workers in palliative and end of life care shalldemonstrate an attitude of compassion and sensitivity to clients, respecting clients’ rightsto self-determination and dignity. Social workers shall be aware of their own beliefs,values, and feelings and how their personal self may influence their practice.
6. Empowerment and Advocacy – The social worker shall advocate for the needs, decisions,and rights of clients in palliative and end of life care. The social worker shall engage insocial and political action that seeks to ensure that people have equal access to resources tomeet their biopsychosocial needs in palliative and end of life care.
7. Documentation – Social workers shall document all practice with clients in either the clientrecord or in the medical chart. These may be written or electronic records.
8. Interdisciplinary Teamwork – Social workers should be part of an interdisciplinary effortfor the comprehensive delivery of palliative and end of life services. Social workers shallstrive to collaborate with team members and advocate for clients’ needs with objectivityand respect to reinforce relationships with providers who have cared for the patient alongthe continuum of illness.
9. Cultural Competence – Social workers shall have, and shall continue to develop,specialized knowledge and understanding about history, traditions, values, and familysystems as they relate to palliative and end of life care within different groups. Socialworkers shall be knowledgeable about, and act in accordance with, the NASW Standardsfor Cultural Competence in Social Work Practice (NASW, 2001).
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 45
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 45

10. Continuing Education – Social workers shall assume personal responsibility for theircontinued professional development in accordance with the NASW Standards forContinuing Professional Education (NASW, 2002) and state requirements.
11. Supervision, Leadership, and Training – Social workers with expertise in palliative and endof life care should lead educational, supervisory, administrative, and research efforts withindividuals, groups, and organizations.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 46
ANDARDS FOR PALLIATIVE AND
rkers Standards for Palliative and End-of-Life Carebereavement/standards/default.asp
practitioners working in palliative and end of life care:
s, ethics, and standards of both the profession andguide social workers practicing in palliative and end of lifecs (NASW, 2000) is one of several essential guides to ethical
n palliative and end of life care shall demonstrate a workingnd biopsychosocial factors essential to effectively practice
hall assess clients and include comprehensive information totment planning.
ng – Social workers shall incorporate assessments inintervention plans that enhance the clients’ abilities andof life care.
al workers in palliative and end of life care shallmpassion and sensitivity to clients, respecting clients’ rightsity. Social workers shall be aware of their own beliefs,heir personal self may influence their practice.
– The social worker shall advocate for the needs, decisions,ve and end of life care. The social worker shall engage inseeks to ensure that people have equal access to resources tods in palliative and end of life care.
ers shall document all practice with clients in either the clientThese may be written or electronic records.
Social workers should be part of an interdisciplinary efforty of palliative and end of life services. Social workers shallm members and advocate for clients’ needs with objectivitynships with providers who have cared for the patient along
workers shall have, and shall continue to develop,derstanding about history, traditions, values, and familytive and end of life care within different groups. Socialle about, and act in accordance with, the NASW Standardscial Work Practice (NASW, 2001).
NKING POLICY, PRACTICE, AND RESEARCH REPORT
45
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 46

APPENDIX K: CITATIONS FROM CURRHOSPICE SOCIAL WORK RESEARCH S(prepared by Deborah Waldrop - see pages 6 to 9)
Ai, A.L., Hopp, F.P., & Sherer, M. (2006). Getting affairs in oand religious coping on end-of-life planning among oSocial Work in End-of-Life and Palliative Care, 2(1),
Arnold, E.M., Artin, K.A., Griffith, D., Person, J.L., & Grahaend of life: Perceptions of hospice social workers. JouPalliative Care 2(4), 61-83.
Bern Klug, M., & Forbes-Thompson S. (2008). Family membresidents: “She’s the only mother I got.” Journal of G
Bern-Klug M. (2006). Calling the question of “possible dyingTriggers, barriers and facilitators. Journal of Social WCare 2(3), 61-85.
Bern-Klug, M. (2004). “Getting everyone on the same page:”perspectives on end-of-life care. Journal of Palliative M
Bern-Klug, M. (2004). The ambiguous dying syndrome. Heal
Bern-Klug, M. (2008). State variations in nursing home sociaGerontological Social Work 51(3-4), 379-409.
Bern-Klug, M. (2009). A framework for categorizing social inin nursing homes. The Gerontologist 49(4), 495-507.
Bern-Klug, M., Kramer, B.J., & Linder, J.F. (2005). All aboarresearch agenda in end-of-life and palliative care. Jou& Palliative Care 1(2), 71-86.
Bullock, K. (2006). Promoting advance directive among AfricJournal of Palliative Medicine, 9(1), 183-195.
Bullock, K., McGraw, S.A., Blank, K., & Bradley, E.H. (2005Americans facing end-of-life decisions? A focus groupEnd-of-Life & Palliative Care, 1(3), 3-19.
Cagle J.G. & Bolte, S. (2009). Sexuality and life-threatening iand palliative care. Health & Social Work 34(3), 223
Cagle, J.G., (2009). Education: A complex and empowering slife. Health & Social Work 34(1), 17-27.
Chapin, R., Gordon, T., Landry, S., Rachlin, R. (2007). Hospthe door of the nursing facility: Implications for sociaEnd-of-Life & Palliative Care 3(2), 19-38.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
APPENDIX J: TRAINING AND CREDENTIALS FOR HOSPICESOCIAL WORKERS
Credentials
• Advanced Certified Hospice and Palliative Social Worker (ACHP-SW)www.socialworkers.org/credentials/credentials/chpsw.asp
• Certified Hospice and Palliative Social Worker (CHP-SW)www.socialworkers.org/credentials/credentials/chpsw.asp
Training and Education
• NASW WebEd Continuing Education (CEU) on End-of-Life Carewww.naswwebed.org/
◊ Understanding End-of-Life Care: The Social Worker’s Role
◊ Understanding Cancer Caregiving: The Social Worker’s Role
◊ Achieving Cultural Competence to Reduce Health Disparities in End of Life Care
◊ A daganatos betegségek megismertetése Magyarországon: A szociális munkások(Understanding Cancer in Hungary: The Social Worker’s Role)
• NASW’s continuing education program also approves CEUs on hospice social work andother end-of-life issues provided by other organizationshttp://socialworkers.org/ce/approval.asp
• NHCPO’s Competency-Based Education for Social Workers –www.nhpco.org/i4a/pages/index.cfm?pageid=3913
The purpose of NHPCO’s social work competencies module provides a self-administeredinteractive program that helps social workers master skills for practice, foster continuallearning, and establish a strong sense of professionalism and accountability, which willhelp increase quality of services for patients and caregivers. The competencies module hasthe following goals:
◊ “To offer individual practitioners a tool for interactive on-line study and competencyevaluation related to grief and depression;
◊ To provide a sample format for agencies seeking to develop programs of competencyeducation.”
• The Hospice Foundation of America (HFA) 2010 National Bereavement Teleconference:Living with Grief®: Cancer and End-of Life Carewww.hospicefoundation.org/pages/page.asp?page_id=65770
The NASW supports HFA each year for its National Bereavement Teleconference. Socialworkers may obtain continuing education units by participating in this event. This year’sconference is on March 24 and is available online.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 47
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 47
APPENDIX K: CITATIONS FROM CURRENT STATUS OFHOSPICE SOCIAL WORK RESEARCH SECTION(prepared by Deborah Waldrop - see pages 6 to 9)
Ai, A.L., Hopp, F.P., & Sherer, M. (2006). Getting affairs in order: Influences of social supportand religious coping on end-of-life planning among open-heart surgery patients. Journal ofSocial Work in End-of-Life and Palliative Care, 2(1), 71-94.
Arnold, E.M., Artin, K.A., Griffith, D., Person, J.L., & Graham, K.G. (2006). Unmet needs at theend of life: Perceptions of hospice social workers. Journal of Social Work in End-of-Life &Palliative Care 2(4), 61-83.
Bern Klug, M., & Forbes-Thompson S. (2008). Family members’ responsibilities to nursing homeresidents: “She’s the only mother I got.” Journal of Gerontological Nursing 34(2), 43-52.
Bern-Klug M. (2006). Calling the question of “possible dying” among nursing home residents;Triggers, barriers and facilitators. Journal of Social Work in End-of-Life & PalliativeCare 2(3), 61-85.
Bern-Klug, M. (2004). “Getting everyone on the same page:” Nursing home physicians’perspectives on end-of-life care. Journal of Palliative Medicine 7(4), 533-544.
Bern-Klug, M. (2004). The ambiguous dying syndrome. Health & Social Work 29(1), 55-65.
Bern-Klug, M. (2008). State variations in nursing home social worker qualifications. Journal ofGerontological Social Work 51(3-4), 379-409.
Bern-Klug, M. (2009). A framework for categorizing social interactions related to end-of-life carein nursing homes. The Gerontologist 49(4), 495-507.
Bern-Klug, M., Kramer, B.J., & Linder, J.F. (2005). All aboard: Advancing the social workresearch agenda in end-of-life and palliative care. Journal of Social Work in End-of-Life& Palliative Care 1(2), 71-86.
Bullock, K. (2006). Promoting advance directive among African Americans: A faith-based model.Journal of Palliative Medicine, 9(1), 183-195.
Bullock, K., McGraw, S.A., Blank, K., & Bradley, E.H. (2005). What matters to older AfricanAmericans facing end-of-life decisions? A focus group study. Journal of Social Work inEnd-of-Life & Palliative Care, 1(3), 3-19.
Cagle J.G. & Bolte, S. (2009). Sexuality and life-threatening illness: Implications for social workand palliative care. Health & Social Work 34(3), 223-233.
Cagle, J.G., (2009). Education: A complex and empowering social work intervention at the end oflife. Health & Social Work 34(1), 17-27.
Chapin, R., Gordon, T., Landry, S., Rachlin, R. (2007). Hospice use by older adults knocking onthe door of the nursing facility: Implications for social work in Journal of Social Work inEnd-of-Life & Palliative Care 3(2), 19-38.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 48
AND CREDENTIALS FOR HOSPICE
nd Palliative Social Worker (ACHP-SW)ntials/credentials/chpsw.asp
ve Social Worker (CHP-SW)ntials/credentials/chpsw.asp
ucation (CEU) on End-of-Life Care
e Care: The Social Worker’s Role
regiving: The Social Worker’s Role
etence to Reduce Health Disparities in End of Life Care
megismertetése Magyarországon: A szociális munkásokHungary: The Social Worker’s Role)
program also approves CEUs on hospice social work anded by other organizationsproval.asp
Education for Social Workers –ex.cfm?pageid=3913
al work competencies module provides a self-administeredsocial workers master skills for practice, foster continualg sense of professionalism and accountability, which wills for patients and caregivers. The competencies module has
itioners a tool for interactive on-line study and competencyand depression;
at for agencies seeking to develop programs of competency
merica (HFA) 2010 National Bereavement Teleconference:d End-of Life Careages/page.asp?page_id=65770
h year for its National Bereavement Teleconference. Socialg education units by participating in this event. This year’sd is available online.
NKING POLICY, PRACTICE, AND RESEARCH REPORT
47
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 48
Kramer, B.J., Kavanaugh, M., Trentham-Dietz, Walsh, M., &Family Conflict at the End of Life: The experience ofwith lung cancer. The Gerontologist 50(2), 215-225.
Lawson, R. (2007). Home and hospital: Hospice and palliativimpacts the social work role. Journal of Social Work3-17.
Miller, P.J., Hedlund, S.C., & Soule, A.B. (2006). The challendeath with dignity in Oregon. Journal of Social Work2(2), 25-43.
Moon, R.P. & Cagle, J.G. (2009). An analysis of end-of-life cproceedings. Gerontology & Geriatrics Education 30
Munn, J. & Zimmerman, S. (2006). A good death for residenmembers speak. Journal of Social Work in End-of-Lif
Munn, J.C., Dobbs, D., Meier, A., Williams, C.S., Biola, H.,end-of-life experience in long-term care: Five themes iresidents, family members and staff. The Gerontologi
National Hospice and Palliative Care Organization (2004). DAgenda. Journal of Pain and Symptom Management 2
Parker Oliver & Peck, M. (2006). Inside the interdisciplinaryworkers. Journal of Social Work in End-of-Life & Pa
Parker Oliver, D., Bronstein, L.R., & Kurzejeski, L. (2005). Esuccessful collaboration on the hospice team. Health
Parker Oliver, D., Wittenberg-Lyles, E., Washington, K.T., &role in hospice pain management: A national survey. J& Palliative Care 5, 61-74.
Ratner, E.R., Norlander, L., McSteen, K. (2001). Death at hoplanning process in the home setting: The kitchen tabAmerican Geriatrics Society 49(6), 778-781.
Reese, D.J., Raymer, M. (2004). Relationships between sociaoutcomes: Results of a national hospice social work s
Sanders, S. & Power, J. (2009). Roles, responsibilities and relcaring for wives with progressive dementia and otherWork 34(1), 41-51.
Sanders, S., Butcher, H.K., Swails, P., & Power, J. (2009). Pordementia patients receiving hospice care. Death Studi
Sanders, S., Ott, C.H., Kelber, S.T., & Noonan, P. (2008) Thecaregivers of persons with Alzheimer’s disease and rel495-523.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
Csikai, E. (1999). The role of values and experience in determining social workers’ attitudestoward euthanasia and assisted suicide. Social Work in Health Care 30(1), 75-95.
Csikai, E.L. & Raymer, M. (2005). Social workers’ educational needs in end-of-life care. SocialWork in Health Care 41(1), 53-72.
Csikai, E.L. (1999. Euthanasia and assisted suicide: Issues for social work practice. Journal ofGerontological Social Work 31(3-4), 49-63.
Csikai, E.L. (2004). Social workers’ participation in the resolution of ethical dilemmas in hospicecare. Health & Social Work 29(1), 67-76.
Doherty, J.B. & DeWeaver, K.L. (2004). A survey of evaluation practices for hospice socialworkers. Home Health Care Services Quarterly 23(4), 1-13.
Francoeur, R.B., Payne, R., Raveis, V. H., & Shim, H. (2007, 1). Palliative care in the inner-city:Patient religious affiliation, underinsurance, and symptom attitude. Cancer, 109 (2 Suppl),425-434.Francoeur, R. B. (2006, 3). A flexible item to screen for depression in inner-cityminorities during palliative care symptom assessment. American Journal of GeriatricPsychiatry, 14(3), 227-235.
Gardner, D.S. (2008). Cancer in a dyadic context: Older couples’ negotiation of ambiguity andsearch for meaning at the end of life. Journal of Social Work in End-of-Life & PalliativeCare 4(2), 135-159.
Gwyther, L.P., Altilio, T., Blacker, S., Christ, G., Csikai, E.L., Hooyman, N., Kramer, B.J., Linton,J., Raymer, M. & Howe, J. (2005). Social work competencies in palliative and end-of-lifecare. Journal of Social Work in End-of-Life & Palliative Care 1(1), 87-120.
Head, B. & Faul, A. (2005). Terminal restlessness as perceived by hospice professionals. AmericanJournal of Hospice and Palliative Care 22(4), 277-282.
Hopp, F.P. & Duffy, S. (2000). Racial variations in end-of-life care. Journal of the AmericanGeriatrics Society, 48(6), 658-663.
Hopp, F.P. (2000). Preferences for surrogate decision-makers, informal communication, andadvance directives among community-dwelling elderly: Results from a national study. TheGerontologist, 40(4), 449-457.
Huff, M.B., Weisenfluh, S., Murphy, M., & Black, P.J. (2006). End-of-life care and social workeducation: What do students need to know? Journal of Gerontological Social Work48(1-2), 219-231.
Kramer, B.J., & Auer, C. (2005). Challenges to providing end-of-life care to low-income elderswith advanced chronic disease: Lessons learned from a model program. The Gerontologist45(5), 651-660.
Kramer, B.J., Boelk, A.Z., & Auer, C. (2006). Family conflict at the end of life: Lessons learned ina model program for vulnerable adults. Journal of Palliative Medicine 9(3), 791-801.
Kramer, B.J., Christ, G.H., Bern-Klug, M., & Francoeur, R.F. (2005) A national agenda for socialwork research in palliative and end-of-life care. Journal of Palliative Medicine 8(2),418-431.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 49
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 49
Kramer, B.J., Kavanaugh, M., Trentham-Dietz, Walsh, M., & Yonker, J.A. (2010). Predictors ofFamily Conflict at the End of Life: The experience of spouses and adult children of personswith lung cancer. The Gerontologist 50(2), 215-225.
Lawson, R. (2007). Home and hospital: Hospice and palliative care: How the environmentimpacts the social work role. Journal of Social Work in End-of-Life & Palliative Care 3(2),3-17.
Miller, P.J., Hedlund, S.C., & Soule, A.B. (2006). The challenge to support patients who considerdeath with dignity in Oregon. Journal of Social Work in End-of-Life & Palliative Care2(2), 25-43.
Moon, R.P. & Cagle, J.G. (2009). An analysis of end-of-life content in Aging Network conferenceproceedings. Gerontology & Geriatrics Education 30(2), 130-145.
Munn, J. & Zimmerman, S. (2006). A good death for residents of long-term care: Familymembers speak. Journal of Social Work in End-of-Life & Palliative Care 2, 45-59.
Munn, J.C., Dobbs, D., Meier, A., Williams, C.S., Biola, H., & Zimmerman, S. (2008) Theend-of-life experience in long-term care: Five themes identified from focus groups withresidents, family members and staff. The Gerontologist 48(4), 485-494.
National Hospice and Palliative Care Organization (2004). Development of the NHPCO ResearchAgenda. Journal of Pain and Symptom Management 28(5), 488-496.
Parker Oliver & Peck, M. (2006). Inside the interdisciplinary team experience of hospice socialworkers. Journal of Social Work in End-of-Life & Palliative Care 2(3), 7-21.
Parker Oliver, D., Bronstein, L.R., & Kurzejeski, L. (2005). Examining variables related tosuccessful collaboration on the hospice team. Health & Social Work 30(4), 279-286.
Parker Oliver, D., Wittenberg-Lyles, E., Washington, K.T., & Sehrawat, S. (2009). Social workrole in hospice pain management: A national survey. Journal of Social Work in End-of-Life& Palliative Care 5, 61-74.
Ratner, E.R., Norlander, L., McSteen, K. (2001). Death at home following a targeted advance careplanning process in the home setting: The kitchen table discussion. Journal of theAmerican Geriatrics Society 49(6), 778-781.
Reese, D.J., Raymer, M. (2004). Relationships between social work involvement and hospiceoutcomes: Results of a national hospice social work survey. Social Work 49(3), 415-422.
Sanders, S. & Power, J. (2009). Roles, responsibilities and relationships among older husbandscaring for wives with progressive dementia and other chronic conditions. Health & SocialWork 34(1), 41-51.
Sanders, S., Butcher, H.K., Swails, P., & Power, J. (2009). Portraits of caregivers of end-stagedementia patients receiving hospice care. Death Studies 33(6), 521-556.
Sanders, S., Ott, C.H., Kelber, S.T., & Noonan, P. (2008) The experience of high levels of grief incaregivers of persons with Alzheimer’s disease and related dementia. Death Studies 32(6),495-523.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 50
nd experience in determining social workers’ attitudesd suicide. Social Work in Health Care 30(1), 75-95.
ocial workers’ educational needs in end-of-life care. Social3-72.
sisted suicide: Issues for social work practice. Journal of1(3-4), 49-63.
articipation in the resolution of ethical dilemmas in hospice9(1), 67-76.
4). A survey of evaluation practices for hospice socialervices Quarterly 23(4), 1-13.
H., & Shim, H. (2007, 1). Palliative care in the inner-city:derinsurance, and symptom attitude. Cancer, 109 (2 Suppl),
06, 3). A flexible item to screen for depression in inner-cityre symptom assessment. American Journal of Geriatric
dic context: Older couples’ negotiation of ambiguity andof life. Journal of Social Work in End-of-Life & Palliative
Christ, G., Csikai, E.L., Hooyman, N., Kramer, B.J., Linton,005). Social work competencies in palliative and end-of-lifen End-of-Life & Palliative Care 1(1), 87-120.
restlessness as perceived by hospice professionals. Americantive Care 22(4), 277-282.
variations in end-of-life care. Journal of the American663.
rogate decision-makers, informal communication, andmmunity-dwelling elderly: Results from a national study. The
.
M., & Black, P.J. (2006). End-of-life care and social workneed to know? Journal of Gerontological Social Work
lenges to providing end-of-life care to low-income elders: Lessons learned from a model program. The Gerontologist
(2006). Family conflict at the end of life: Lessons learned inle adults. Journal of Palliative Medicine 9(3), 791-801.
M., & Francoeur, R.F. (2005) A national agenda for sociald end-of-life care. Journal of Palliative Medicine 8(2),
NKING POLICY, PRACTICE, AND RESEARCH REPORT
49
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 50
Wesley, C., Tunney, K., Duncan, E. (2004). Educational needassessment and interventions with diverse populationPalliative Medicine 21(1), 40-46.
Williams, S.W., Williams, C.S., Zimmerman, S., Munn, J., DoEmotional and physical health of informal caregiversrole of social support. Journals of Gerontology SeriesSciences 63(3), S171-183.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
Schroepfer, T.A. (2007). Critical events in the dying process: The potential for physical andpsychosocial suffering. Journal of Palliative Medicine 10(1), 136-147.
Schroepfer, T.A. (2006). Mind frames towards dying and factors motivating their adoption byterminally ill elders. Journals of Gerontology Series B-Psychological Sciences & SocialSciences 61(3), S129-139.
Schroepfer, T.A. (2008). Social relationships and their role in the consideration to hasten death.The Gerontologist 48(5), 612-621.
Schroepfer, T.A., Noh, H., & Kavenaugh, M. (2009). The myriad strategies for seeking control inthe dying process. The Gerontologist 49(6), 755-766.
Townsend, A.L., Ishler, K.J., Vargo, E.H., Shapiro, B.M., Pitorak, E.F., & Matthews, C.R. (2007).The FACES Project: An academic-community partnership to improve end-of-life care forfamilies. Journal of Gerontological Social Work 50(1-2), 7-20.
Waldrop D.P. (2008). Evidence–based psychosocial treatment at the end of life. Journal ofGerontological Social Work 50, Suppl 1, 267-292.
Waldrop, D.P. & Kirkendall, A. (2009). Comfort measures: A qualitative study of nursinghome-based end-of-life care. Journal of Palliative Medicine 12(8), 719-724.
Waldrop, D.P. & Rinfrette, E.S. (2009). Can short hospice enrollment be long enough? Comparingthe perspectives of hospice professionals and family caregivers. Palliative and SupportiveCare 7(1), 37-47.
Waldrop, D.P. & Rinfrette, E.S. (2009). Making the transition to hospice: Exploring hospiceprofessionals’ perspectives. Death Studies 33(6), 557-580.
Waldrop, D.P. (2006). At the eleventh hour: Psychosocial dynamics in short hospice stays. TheGerontologist 46(1), 106-114.
Waldrop, D.P. (2007). Caregiver grief in terminal illness and bereavement: A mixed methodsstudy. Health & Social Work 32(2), 197-206.
Waldrop, D.P., Kramer, B.J., Skretny, J.A., Milch, R. & Finn, B. (2005). Final transitions: Familycaregiving at the end of life. Journal of Palliative Medicine 8(3), 623-638.
Waldrop, D.P., Milch R.A., & Skretny, J.A. (2005). Understanding family responses to life-limitingillness: In-depth interviews with hospice patients and their family members. Journal ofPalliative Care 21(2), 88-96.
Walsh-Burke, K., & Csikai, E.L. (2005). Professional social work education in end-of-life care:Contribution of the Project on Death in America’s Social Work Leadership Developmentprogram. Journal of Social Work in End-of-Life & Palliative Care 1(2), 11-26.
Washington, K.T., Bickel-Swenson, D., & Stephens, N. (2008). Barriers to hospice use amongAfrican Americans: A systematic review. Health & Social Work 33(4), 267-274.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 51
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 51

Wesley, C., Tunney, K., Duncan, E. (2004). Educational needs of hospice social workers: Spiritualassessment and interventions with diverse populations. American Journal of Hospice andPalliative Medicine 21(1), 40-46.
Williams, S.W., Williams, C.S., Zimmerman, S., Munn, J., Dobbs, D., & Sloane, P. 2008).Emotional and physical health of informal caregivers of residents at the end of life: Therole of social support. Journals of Gerontology Series B-Psychological Sciences & SocialSciences 63(3), S171-183.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 52
s in the dying process: The potential for physical andl of Palliative Medicine 10(1), 136-147.
towards dying and factors motivating their adoption byof Gerontology Series B-Psychological Sciences & Social
nships and their role in the consideration to hasten death.621.
ugh, M. (2009). The myriad strategies for seeking control inologist 49(6), 755-766.
.H., Shapiro, B.M., Pitorak, E.F., & Matthews, C.R. (2007).mic-community partnership to improve end-of-life care forgical Social Work 50(1-2), 7-20.
psychosocial treatment at the end of life. Journal of0, Suppl 1, 267-292.
9). Comfort measures: A qualitative study of nursingournal of Palliative Medicine 12(8), 719-724.
). Can short hospice enrollment be long enough? Comparingofessionals and family caregivers. Palliative and Supportive
). Making the transition to hospice: Exploring hospiceeath Studies 33(6), 557-580.
hour: Psychosocial dynamics in short hospice stays. The
in terminal illness and bereavement: A mixed methods32(2), 197-206.
J.A., Milch, R. & Finn, B. (2005). Final transitions: Familyournal of Palliative Medicine 8(3), 623-638.
y, J.A. (2005). Understanding family responses to life-limitingth hospice patients and their family members. Journal of
5). Professional social work education in end-of-life care:Death in America’s Social Work Leadership Development
ork in End-of-Life & Palliative Care 1(2), 11-26.
, & Stephens, N. (2008). Barriers to hospice use amongtic review. Health & Social Work 33(4), 267-274.
NKING POLICY, PRACTICE, AND RESEARCH REPORT
51
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 52

care. Home care hospice social workers have exposure to thetherefore should adapt care to carefully consider this environmay be administering care) in the assessment and planning ofteamwork is required in both environments. However, hospicbalanced role of care planning than hospital palliative care sothat social workers’ skills and knowledge base for each envirdefined in order to focus the scope of practice for palliative cstandards.
Reese, D.J. & Raymer, M. (2004). Relationships between socoutcomes: results of the national hospice social work
The researchers conducted a quantitative survey with patientdirectors to explore outcomes related to social workers’ levelteams. The sample included 330 patients, 66 social workers,agencies (registered with NHPCO) throughout the country. Equestionnaire about social work involvement in care, hospiceoutcomes. Results show that social workers have little involv38% include social workers at intake). However, when socialit increases their ability to plan for potential barriers to treatmthereby decreasing future costs of care. Results also indicate afunctioning as a social worker’s credentials increase (e.g., BSWcontinue to have higher case loads (16.7 patients to 1 social wand only 18% are supervised by a social worker. Social workintegration and feeling equally respected as other team membrecommend establishing higher social work salaries, hiring soand experience, obtaining social work supervision for social wintake interviews, and hiring a sufficient number of social wo
Parker Oliver, D., Wittenberg-Lyles, E., Washington, K.T., &role in hospice pain management: A national survey. J& Palliative Care, 5, 61-74. doi: 10.1080/155242509
These authors evaluated hospice social workers delivery of seinterdisciplinary team, specifically how they assessed and treacaregivers. A mail survey was sent to social workers using theResearch Network (PopCRN), which yielded 90 respondentsQuestions focused on social workers’ delivery of services, intemembers, and interdisciplinary team structure. Results showhad an MSW, an average of 6 years experience, and an averaaverage of 11.2 cases). Additionally, social workers can, but dattitudes in pain management. However, they are regularly cocolleagues and feel like active team participants in team meetabout the increased focus on the medicalization of hospice, thaddress, and interface with caregivers about beliefs and abouof care. While this study and others by the lead author descrisocial work integration with hospice teams, the findings are nwas drawn from a network of hospice organizations that areresearch and encourage progressive hospice care practices. Nthe growing body of knowledge on hospice social work.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
APPENDIX L: ANNOTATED BIBLIOGRAPHY
Social Work’s Role in Hospice Care
Bradsen, C.K. (2005). Social work and end-of-life care: reviewing the past and moving forward.Journal of Social Work in End-of-Life and Palliative Care, 1(2), 45-70. doi:10.1300/J457v01n0205.
This article summarizes research on social work in hospice care from 1990 through July 2004 andprovides a deeper background to the more recent articles listed in this bibliography. Discussioncenters on articles that evaluate the roles, practices, and core values of social workers, and thebarriers they experience in providing end-of-life care. Social workers provide psychosocial supportto patients and families including counseling, assessment and referrals to further services,developing and implementing Advanced Directives, patient advocacy with other careprofessionals, case management (e.g., financial information, referrals to community resources,etc.), bereavement care, ethical considerations for treatment plans, education about death anddying, assistance with funeral arrangements, and at times spiritual counseling.
When working with other professionals in organizations, social workers assist in giving difficultdiagnoses, assessing a client system to develop treatment plans, facilitating communicationbetween staff, mentoring and supervising other social workers, educating colleagues on a client’ssocial context, developing policies and programs for services related to end-of-life care andmanaging staff development and volunteer training. Social workers identify core values asadvocating for a patient’s right to self-determination, pursuing care for the common good,providing care for patients that address all areas of pain (physical, social, emotional, spiritual),and maintain respect for those who are dying or are important to the dying person.
Research highlights the need for social workers to be involved at the policy level in educatinghospice stakeholders and decision-makers about the social work roles, values, and barriers toproviding quality end-of-life care. Research also lists the barriers to service delivery as insufficienteducational preparation, role conflicts with other staff in delivering services, ambiguities inhospice agency policies regarding service delivery, and varying expectations from administrators.Further, a lack of knowledge between professions about each others’ roles leads tointerdisciplinary communication challenges and differing goals. Lastly, there is an overall lack ofempirical research and funding for research, which can result in the devaluing of social workers asa hospice care team members. The author concludes from the review that social workers havebeen integral members of end-of-life care teams for quite some time, although empirical evidenceshowing the importance of their roles is missing. She suggests adding more end-of-life care issuesto the social work BSW and MSW curriculum and setting a research agenda that builds on workon end-of-life care from other professions and focuses on social workers’ contribution to careteams.
Lawson, R. (2007). Home and hospital: Hospice and palliative care: How the environmentimpacts the social work role. Journal of Social Work in End-of-Life & Palliative Care,3(2),3-17. doi: 10.1300/J457v03n02_02.
This invited article summarizes the various aspects of coordination of care, teamwork, andcollaboration of social workers in hospital palliative care and home hospice care environments.Palliative care social workers provide consistency of care in an unfamiliar and regularly changingenvironment, balance a physician-centered treatment model while assessing and advocating for thewhole client, and help ensure that patients are referred to hospice care at the end-of-life stage of
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 53
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 53

care. Home care hospice social workers have exposure to the patient’s home environment andtherefore should adapt care to carefully consider this environment, and include caregivers (whomay be administering care) in the assessment and planning of care process. Interdisciplinaryteamwork is required in both environments. However, hospice social work allows for a morebalanced role of care planning than hospital palliative care social workers. The author suggeststhat social workers’ skills and knowledge base for each environment are different and should bedefined in order to focus the scope of practice for palliative care and hospice social work practicestandards.
Reese, D.J. & Raymer, M. (2004). Relationships between social work involvement and hospiceoutcomes: results of the national hospice social work survey. Social Work, 49(3), 415-422.
The researchers conducted a quantitative survey with patients, social workers, and hospicedirectors to explore outcomes related to social workers’ level of involvement in hospice careteams. The sample included 330 patients, 66 social workers, and 66 hospice directors from 66agencies (registered with NHPCO) throughout the country. Each participant was mailed aquestionnaire about social work involvement in care, hospice care processes, and hospiceoutcomes. Results show that social workers have little involvement during the intake process (only38% include social workers at intake). However, when social workers are involved in assessment,it increases their ability to plan for potential barriers to treatment as well as prevent future crises,thereby decreasing future costs of care. Results also indicate a positive correlation in teamfunctioning as a social worker’s credentials increase (e.g., BSW to MSW). Social workers alsocontinue to have higher case loads (16.7 patients to 1 social worker vs. 5.5 patients to 1 nurse)and only 18% are supervised by a social worker. Social workers report frustrations with teamintegration and feeling equally respected as other team members in the care process. The authorsrecommend establishing higher social work salaries, hiring social workers with more educationand experience, obtaining social work supervision for social workers, including social workers inintake interviews, and hiring a sufficient number of social workers dedicated to client care.
Parker Oliver, D., Wittenberg-Lyles, E., Washington, K.T., & Sehrawat, S. (2009). Social workrole in hospice pain management: A national survey. Journal of Social Work in End-of-Life& Palliative Care, 5, 61-74. doi: 10.1080/15524250903173900.
These authors evaluated hospice social workers delivery of services as a member of aninterdisciplinary team, specifically how they assessed and treated pain as described by patients andcaregivers. A mail survey was sent to social workers using the Population Based Palliative CareResearch Network (PopCRN), which yielded 90 respondents from 19 states across the US.Questions focused on social workers’ delivery of services, interaction with caregivers and teammembers, and interdisciplinary team structure. Results show that 74% of social workers surveyedhad an MSW, an average of 6 years experience, and an average of 23.4 cases (compared to nurses’average of 11.2 cases). Additionally, social workers can, but do not regularly assess caregiverattitudes in pain management. However, they are regularly consulted by non-social workercolleagues and feel like active team participants in team meetings. There were some concernsabout the increased focus on the medicalization of hospice, the need to preventatively assess,address, and interface with caregivers about beliefs and about pain management and other aspectsof care. While this study and others by the lead author describes higher perceived levels of hospicesocial work integration with hospice teams, the findings are not generalizable, because the samplewas drawn from a network of hospice organizations that are more likely to participate in hospiceresearch and encourage progressive hospice care practices. Nonetheless, this research still adds tothe growing body of knowledge on hospice social work.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 54
ED BIBLIOGRAPHY
d end-of-life care: reviewing the past and moving forward.-of-Life and Palliative Care, 1(2), 45-70. doi:
ocial work in hospice care from 1990 through July 2004 andmore recent articles listed in this bibliography. Discussionles, practices, and core values of social workers, and theend-of-life care. Social workers provide psychosocial supportnseling, assessment and referrals to further services,ed Directives, patient advocacy with other carefinancial information, referrals to community resources,erations for treatment plans, education about death andments, and at times spiritual counseling.
als in organizations, social workers assist in giving difficultdevelop treatment plans, facilitating communicationing other social workers, educating colleagues on a client’s
d programs for services related to end-of-life care andnteer training. Social workers identify core values as-determination, pursuing care for the common good,ss all areas of pain (physical, social, emotional, spiritual),re dying or are important to the dying person.
l workers to be involved at the policy level in educatingkers about the social work roles, values, and barriers toearch also lists the barriers to service delivery as insufficientwith other staff in delivering services, ambiguities in
ice delivery, and varying expectations from administrators.professions about each others’ roles leads toenges and differing goals. Lastly, there is an overall lack ofearch, which can result in the devaluing of social workers asthor concludes from the review that social workers haveare teams for quite some time, although empirical evidenceis missing. She suggests adding more end-of-life care issuesrriculum and setting a research agenda that builds on workons and focuses on social workers’ contribution to care
al: Hospice and palliative care: How the environmentJournal of Social Work in End-of-Life & Palliative Care,3(2),2_02.
rious aspects of coordination of care, teamwork, andpital palliative care and home hospice care environments.consistency of care in an unfamiliar and regularly changingtered treatment model while assessing and advocating for theients are referred to hospice care at the end-of-life stage of
NKING POLICY, PRACTICE, AND RESEARCH REPORT
53
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 54
and caregivers had many unmet needs that lead to a decreasethese unmet needs were patient-related psychosocial and famlosing independence and being a burden on family and friendunmet needs are treatable with psychosocial interventions ancare professionals need to assess and intervene effectively to ito addressing unmet needs include societal and cultural issueslack of understanding or knowledge about dying or the hospi
Doherty, J.B. & DeWeaver, K.L. (2004). A survey of evaluatiworkers. Home Health Care Services Quarterly, 23(410.1300/J027v23n04_01.
The authors assessed the methods of supervision for hospicestates. A mail questionnaire was collected from 109 social wo99% of social workers are evaluated in some way with a greaevaluation. The most common evaluation methods were reviework (92%), input from other hospice team members (86%)direct observation (70%), with 53% being evaluated once a ypatient input because of concerns that it is not a useful methoand emotional conditions of some patients. The authors idenindirect evaluation methods, which may be attributed to lackor the social worker. Suggestions for enhanced quality of caresupervisors to directly observe social workers and to seek patsatisfaction. They use the NASW code of ethics to cite the socadvocate for a client’s self-determination as a justification for
Kramer, B.T., Kavanaugh, M., Trentham-Dietz, A., Walsh, Mof Family Conflict at the End of Life: The ExperiencePersons with Lung Cancer, The Gerontologist, 50(2),
Purpose: Guided by an explanatory matrix of family conflictarticle was to examine the correlates and predictors of familyadult children of persons with lung cancer.Design and Methods: A cross-sectional statewide survey of fafrom lung cancer was conducted as part of the larger study oSatisfaction in Wisconsin.Results: Significant bivariate correlations were found betweenvariables (i.e., a history of conflict, younger respondent age, rwishes of the patient), conditions (i.e., greater physical and ppatient), and contributing factors (i.e., communication constrIn the multivariate model, significant predictors of family conrace, communication constraints, and family members assertiof the variance in conflict.Implications: Implications for routine assessment and screenirecommendations for the development and testing of intervenmaking and enhance open communication among at-risk fam
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
Interdisciplinary Collaboration
Parker Oliver, D., Bronstein, L.R., & Kurzejeski, L. (2005). Examining variables related tosuccessful collaboration on the hospice team. Health & Social Work, 30(4), 279-286.
The authors evaluated hospice social workers to determine aspects of successful interdisciplinarycollaboration within hospice care teams. The sample consisted of 146 social workers that weremailed quantitative surveys. All participants were from state licensed hospice agencies in Missouri.Results show that 53% of respondents had an MSW and 31% were the only social worker in theiragency. The overall perception of interdisciplinary collaboration was high, but with a wide rangein responses. Perceptions of interdisciplinary collaboration were not related to the social worker’slevel of education, the make-up of the hospice agency staff, or the quality of care delivered by thehospice program. The authors cite many limitations to their study, such as a low response rate andthe use of a sample from only one state. The article calls for more research on the topic to explainthe lack of correlation among variables. Parker Oliver (2006) later uses a qualitative study toevaluate similar topics (Parker Oliver & Peck, 2006).
Parker Oliver, D. & Peck, M. (2006). Inside the interdisciplinary team experiences of hospicesocial workers. Journal of Social Work in End-of-Life & Palliative Care, 2(3), 7-21. doi:10.1300/J457v02n03_03.
Under the conceptual framework of the Bronstein Model for Interdisciplinary Communication(Bronstein, 2003), the authors used a qualitative research design to randomly evaluate aconvenient sample to determine self-identified strengths and challenges of teamwork for hospicesocial workers. Bronstein’s model views successful collaboration through (1) interdependence, (2)newly created professional activities, (3) flexibility in traditional roles, (4) collective ownership ofgoals, and (5) reflection on process. The sample included 23 social workers from 20 hospiceprograms who discussed their employment and involvement with hospice programs, educationalpreparation for employment, supervision of performance, and the make-up of the hospice careteam. Results show that teamwork is enhanced when team members have strong communicationand trust among the group, engage in joint home visits with other colleagues, participate in teambuilding activities, feel equally respected as a member of the team, and receive support fromhospice administration. Challenges of interdisciplinary work for hospice social workers includelarge caseloads, the medicalization of hospice care diminishing the social work role, a limitednumber of allowed visits, the lack of staff flexibility and administrative support, and personalityconflicts among team members. Lastly, the authors highlight the importance of evaluation todetermine team effectiveness. Only four social workers said this was done at their agency, butindicated that it was helpful in making changes to enhance the effectiveness of the interdisciplinaryteam.
Hospice Services with Families
Arnold, E.M., Artin, K.A., Griffith, D., Person, J.L., & Graham, K.G. (2006). Unmet needs at theend of life: Perceptions of hospice social workers. Journal of Social Work in End-of-Life &Palliative Care, 2(4), 61-83.
The authors evaluated hospice social workers in two Southeastern states to determine the unmetneeds of patients at the end of life. A total of 212 surveys were collected from social workersasking them to identify patients’ and caregivers’ unmet needs, and the reasons, interventions andoutcomes, and barriers to addressing these unmet needs. Findings show that the majority of socialworkers responding were Caucasian (91.9%), females (91.7%), had a MSW (71.2%) , and wereemployed with a hospice agency for an average of 4.24 years. Social workers stated that patients
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 55
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 55

and caregivers had many unmet needs that lead to a decrease enjoyment of daily life. Many ofthese unmet needs were patient-related psychosocial and family conflict issues, such as a fear oflosing independence and being a burden on family and friends. Social workers perceive that theseunmet needs are treatable with psychosocial interventions and referrals, and suggest that hospicecare professionals need to assess and intervene effectively to increase the quality of care. Barriersto addressing unmet needs include societal and cultural issues related to death and dying, such aslack of understanding or knowledge about dying or the hospice care philosophy.
Doherty, J.B. & DeWeaver, K.L. (2004). A survey of evaluation practices for hospice socialworkers. Home Health Care Services Quarterly, 23(4), 1-13. doi:10.1300/J027v23n04_01.
The authors assessed the methods of supervision for hospice social workers in five Southeasternstates. A mail questionnaire was collected from 109 social work supervisors. Results indicate that99% of social workers are evaluated in some way with a great variability in the method ofevaluation. The most common evaluation methods were review of the social workers’ writtenwork (92%), input from other hospice team members (86%), individual supervision (81%), anddirect observation (70%), with 53% being evaluated once a year. Supervisors do not often look topatient input because of concerns that it is not a useful method of evaluation given the physicaland emotional conditions of some patients. The authors identify that supervisors more often useindirect evaluation methods, which may be attributed to lack of time on the part of the supervisoror the social worker. Suggestions for enhanced quality of care include increased efforts ofsupervisors to directly observe social workers and to seek patient feedback to learn about clientsatisfaction. They use the NASW code of ethics to cite the social work profession’s commitment toadvocate for a client’s self-determination as a justification for obtaining patient feedback.
Kramer, B.T., Kavanaugh, M., Trentham-Dietz, A., Walsh, M., & Yonker, J.A., (2010). Predictorsof Family Conflict at the End of Life: The Experience of Spouses and Adult Children ofPersons with Lung Cancer, The Gerontologist, 50(2), 215-225.
Purpose: Guided by an explanatory matrix of family conflict at the end of life, the purpose of thisarticle was to examine the correlates and predictors of family conflict reported by 155 spouses andadult children of persons with lung cancer.Design and Methods: A cross-sectional statewide survey of family members of persons who diedfrom lung cancer was conducted as part of the larger study on the Assessment of Cancer Care andSatisfaction in Wisconsin.Results: Significant bivariate correlations were found between family conflict and family contextvariables (i.e., a history of conflict, younger respondent age, race, and specified end-of-life carewishes of the patient), conditions (i.e., greater physical and psychological clinical care needs of thepatient), and contributing factors (i.e., communication constraints and family asserting control).In the multivariate model, significant predictors of family conflict included prior family conflict,race, communication constraints, and family members asserting control; the model explained 72%of the variance in conflict.Implications: Implications for routine assessment and screening to identify families at risk andrecommendations for the development and testing of interventions to facilitate shared decisionmaking and enhance open communication among at-risk families are highlighted.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 56
Kurzejeski, L. (2005). Examining variables related toe hospice team. Health & Social Work, 30(4), 279-286.
workers to determine aspects of successful interdisciplinaryms. The sample consisted of 146 social workers that wereipants were from state licensed hospice agencies in Missouri.s had an MSW and 31% were the only social worker in theirrdisciplinary collaboration was high, but with a wide rangeplinary collaboration were not related to the social worker’shospice agency staff, or the quality of care delivered by theny limitations to their study, such as a low response rate andte. The article calls for more research on the topic to explaines. Parker Oliver (2006) later uses a qualitative study to& Peck, 2006).
Inside the interdisciplinary team experiences of hospiceial Work in End-of-Life & Palliative Care, 2(3), 7-21. doi:
he Bronstein Model for Interdisciplinary Communicationqualitative research design to randomly evaluate adentified strengths and challenges of teamwork for hospicews successful collaboration through (1) interdependence, (2)3) flexibility in traditional roles, (4) collective ownership ofhe sample included 23 social workers from 20 hospicement and involvement with hospice programs, educationalion of performance, and the make-up of the hospice careenhanced when team members have strong communicationjoint home visits with other colleagues, participate in teamed as a member of the team, and receive support frominterdisciplinary work for hospice social workers includehospice care diminishing the social work role, a limitedtaff flexibility and administrative support, and personalityy, the authors highlight the importance of evaluation tour social workers said this was done at their agency, butg changes to enhance the effectiveness of the interdisciplinary
., Person, J.L., & Graham, K.G. (2006). Unmet needs at thepice social workers. Journal of Social Work in End-of-Life &
workers in two Southeastern states to determine the unmettotal of 212 surveys were collected from social workerscaregivers’ unmet needs, and the reasons, interventions andthese unmet needs. Findings show that the majority of social91.9%), females (91.7%), had a MSW (71.2%) , and weren average of 4.24 years. Social workers stated that patients
NKING POLICY, PRACTICE, AND RESEARCH REPORT
55
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 56
APPENDIX M: HOSPICE RESOURCES
Government Agencies
Centers for Medicare and Medicaid Services (CMS)www.cms.hhs.gov/
• Hospice Centerwww.cms.gov/center/hospice.asp
This website provides links to reports and resources ohospice care.
• Data on Medicare Hospice Carewww.cms.gov/Hospice/Downloads/Hospice_Data_19
This link include the 20 most frequent diagnoses, thestay, and trends over time in length of stay, by diagnodocument of the research is also included.
• Regulations (excerpts listed in brief):
◊ Department of Health and Human Services (DHHMedicaid Services (CMS), Federal Register Part IIMedicaid Programs: Hospice Conditions of Particdetails personnel qualifications for hospice socialhttp://edocket.access.gpo.gov/2008/pdf/08-1305.p
◊ Social Security Act, Title 18, Section 1861 (Subsewww.ssa.gov/OP_Home/ssact/title18/1861.htm
Agency for Healthcare Research and Quality (AHRQ)www.ahrq.gov
• Research in Action Newsletter – (March 2003, Issue 1Preferences for Care at the End of Lifewww.ahrq.gov/research/endliferia/endria.pdf
Accreditation Organizations
The Joint Commissionwww.jointcommission.org/
• 2010 Standards for Home Health, Personal Care andwww.jcrinc.com/Accreditation-Manuals/2010-Standaand-Support-Services-and-Hospice/1826/
Community Health Accreditation Program (CHAP)www.chapinc.org/
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
Munn, J., & Zimmerman, S. (2006). A good death for residents of long-term care: Familymembers speak. Journal of Social Work in End of Life & Palliative Care, 2, 45-59.
The authors examine family members of recently deceased patients from nursing homes andresidential care/assisted living facilities to determine aspects of care that lead to positive quality ofend-of-life care outcomes in long-term care environments. Family members of 437 recentlydeceased residents from 26 nursing homes and 105 from residential care/assisted living facilitieswere interviewed by telephone about the residents’ experiences, care provided during the lastmonth of life, the expectation of death, the process of death, the family and staff involvement, andthe satisfaction of care. The sample was mostly white (91%), female (73%), an average age of 61years old, and the adult children of the resident (66%). Results indicate outcome measures as thestructure of services, the process of dying, and the outcome of services up until death. Understructure of services, family members cited a need for more staff, specifically those that are moreeducated about end-of-life issues. In regard to the process of care prior to death, social supportfrom family and staff was seen as instrumental in increasing the quality of care at the end of life.The highest levels of dissatisfaction in any area were due to a lack of attention and positivesupport from staff. Third party care providers (e.g., hospice care providers) were described as evenmore helpful in increasing the quality of end-of-life care because of the increased attention thepatient received. The most frequent outcome of services up until death for each patient was “beingcomfortable” at the time of death and one-third indicated no additional service would haveincreased the quality of care the resident received. The authors cited the need for emotional andsocial support during end-of-life care and highlighted many ways in which social workers aretrained to provide these services. However, because of diminished federal care requirements fornursing homes and residential care/assisted living facilities, social workers are not often enoughinvolved in administering these services. The article also suggests that hospice care social workersshould consider these elements when working with families in nursing homes and residentialcare/assisted living facilities.
Waldrop, D.P. (2008). Evidence-based psychosocial treatment at end of life. Journal ofGerontological Social Work, 50(S1), 267-292
End-of-life care has gained recognition as an important interdisciplinary clinical domain duringthe past three decades largely because scientific and medical advances have changed the nature ofdying in the US. Advances in the treatment of life-limiting illness have typically focused on medicalissues and on treating the physical symptoms that accompany the final stage of a terminal illness.However, because the lengthening life span has made more choices available at the end of life,there is also greater need for evidence-based psychosocial treatment to diminish some of theprolonged emotional, psychological, social, and spiritual distress that accompanies dying. Bothterminally ill older adults and their caregivers can be helped by interventions that address the needfor information, education, preparation, communication, emotional support, and advocacy. Thispaper presents a review of evidence-based psychosocial treatments at the end of life for both olderadults and their caregivers.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 57
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 57
APPENDIX M: HOSPICE RESOURCES
Government Agencies
Centers for Medicare and Medicaid Services (CMS)www.cms.hhs.gov/
• Hospice Centerwww.cms.gov/center/hospice.asp
This website provides links to reports and resources on a variety of issues related tohospice care.
• Data on Medicare Hospice Carewww.cms.gov/Hospice/Downloads/Hospice_Data_1998-2008.zip
This link include the 20 most frequent diagnoses, the number of patients, average length ofstay, and trends over time in length of stay, by diagnosis from 1998-2008. A summarydocument of the research is also included.
• Regulations (excerpts listed in brief):
◊ Department of Health and Human Services (DHHS), Centers for Medicare &Medicaid Services (CMS), Federal Register Part II, 42 CFR Part 418, Medicare andMedicaid Programs: Hospice Conditions of Participation; Final Rule (Page 32218details personnel qualifications for hospice social workers)http://edocket.access.gpo.gov/2008/pdf/08-1305.pdf
◊ Social Security Act, Title 18, Section 1861 (Subsection dd)www.ssa.gov/OP_Home/ssact/title18/1861.htm
Agency for Healthcare Research and Quality (AHRQ)www.ahrq.gov
• Research in Action Newsletter – (March 2003, Issue 12) – Advance Care Planning:Preferences for Care at the End of Lifewww.ahrq.gov/research/endliferia/endria.pdf
Accreditation Organizations
The Joint Commissionwww.jointcommission.org/
• 2010 Standards for Home Health, Personal Care and Support Services, and Hospicewww.jcrinc.com/Accreditation-Manuals/2010-Standards-for-Home-Health-Personal-Care-and-Support-Services-and-Hospice/1826/
Community Health Accreditation Program (CHAP)www.chapinc.org/
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 58
A good death for residents of long-term care: Familycial Work in End of Life & Palliative Care, 2, 45-59.
of recently deceased patients from nursing homes ands to determine aspects of care that lead to positive quality of
m care environments. Family members of 437 recentlyomes and 105 from residential care/assisted living facilitiesthe residents’ experiences, care provided during the lasth, the process of death, the family and staff involvement, andas mostly white (91%), female (73%), an average age of 61e resident (66%). Results indicate outcome measures as theing, and the outcome of services up until death. Undercited a need for more staff, specifically those that are moreegard to the process of care prior to death, social supportrumental in increasing the quality of care at the end of life.any area were due to a lack of attention and positiveroviders (e.g., hospice care providers) were described as evenof end-of-life care because of the increased attention theutcome of services up until death for each patient was “beingone-third indicated no additional service would have
ent received. The authors cited the need for emotional andand highlighted many ways in which social workers are
wever, because of diminished federal care requirements forsisted living facilities, social workers are not often enoughes. The article also suggests that hospice care social workersworking with families in nursing homes and residential
psychosocial treatment at end of life. Journal of0(S1), 267-292
n as an important interdisciplinary clinical domain duringscientific and medical advances have changed the nature ofment of life-limiting illness have typically focused on medical
mptoms that accompany the final stage of a terminal illness.span has made more choices available at the end of life,-based psychosocial treatment to diminish some of theocial, and spiritual distress that accompanies dying. Bothregivers can be helped by interventions that address the needon, communication, emotional support, and advocacy. Thisased psychosocial treatments at the end of life for both older
NKING POLICY, PRACTICE, AND RESEARCH REPORT
57
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 58

Hospice Foundation of America (HFA)www.hospicefoundation.org/
Social Work Hospice and Palliative Care Network (SWHPN)www.swhpn.org/
Specialty Journal
Journal of Social Work in End-of-Life & Palliative Carewww.haworthpress.com/store/product.asp?sku=J457
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
Accreditation Commission for Health Care (ACHC)www.achc.org/index.php
National Organizations
National Hospice and Palliative Care Organization (NHPCO)www.nhpco.org/templates/1/homepage.cfm
• NHPCO Facts and Figures: Hospice Care in Americawww.nhpco.org/files/public/Statistics_Research/NHPCO_facts_and_figures.pdf
• Social Work Competencies Modulewww.nhpco.org/i4a/pages/index.cfm?pageid=3913
National Association of Social Workers (NASW)www.socialworkers.org
• Credentials
◊ Advanced Certified Hospice and Palliative Social Worker (ACHP-SW)www.socialworkers.org/credentials/credentials/chpsw.asp
◊ Certified Hospice and Palliative Social Worker (CHP-SW)www.socialworkers.org/credentials/credentials/chpsw.asp
• Standards
◊ NASW Standards for Social Work Practice in Palliative and End of Life Carewww.socialworkers.org/practice/bereavement/standards/default.asp
• NASW Policy Statementswww.naswpress.org/publications/practice/speaks.html
◊ End-of-Life Care
◊ Hospice Care
• Help Starts Herewww.helpstartshere.org
◊ Death and Dyingwww.helpstartshere.org/health-and-wellness/death-and-dying-overview.html
◊ Death and Dying – How Social Workers Help – The Role of Social Work in Hospiceand Palliative Care by Mary Raymer, MSW, ACSWwww.helpstartshere.org/health-and-wellness/death-and-dying-how-social-workers-help.html
◊ Death and Dying – How Social Workers Help: How Social Workers Keep the HOPEAlive in Hospice by Margo W. Steinberg, MSW, LCSWwww.helpstartshere.org/health-and-wellness/hope-and-hospice.html
◊ Death and Dying Trends – Creativity at the End of Life by Hannah Fiskewww.helpstartshere.org/health-and-wellness/death-and-dying-trends.html
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 59
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 59

Hospice Foundation of America (HFA)www.hospicefoundation.org/
Social Work Hospice and Palliative Care Network (SWHPN)www.swhpn.org/
Specialty Journal
Journal of Social Work in End-of-Life & Palliative Carewww.haworthpress.com/store/product.asp?sku=J457
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 60
Care (ACHC)
Organization (NHPCO)e.cfm
ospice Care in Americaatistics_Research/NHPCO_facts_and_figures.pdf
oduleex.cfm?pageid=3913
rs (NASW)
ce and Palliative Social Worker (ACHP-SW)edentials/credentials/chpsw.asp
iative Social Worker (CHP-SW)edentials/credentials/chpsw.asp
al Work Practice in Palliative and End of Life Careractice/bereavement/standards/default.asp
ons/practice/speaks.html
ealth-and-wellness/death-and-dying-overview.html
Social Workers Help – The Role of Social Work in Hospicery Raymer, MSW, ACSWealth-and-wellness/death-and-dying-how-social-workers-help
Social Workers Help: How Social Workers Keep the HOPEo W. Steinberg, MSW, LCSWealth-and-wellness/hope-and-hospice.html
– Creativity at the End of Life by Hannah Fiskeealth-and-wellness/death-and-dying-trends.html
NKING POLICY, PRACTICE, AND RESEARCH REPORT
59
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 60

APPENDIX O: SOCIAL WORK RESEAREND-OF-LIFE CARE
Hartford Faculty Scholars and Doctoral Fellows Research
Mercedes Bern-Klug, PhDUniversity of IowaResearch Topic: National Survey of Nursing Home Social Wo
Karen Bullock, PhDUniversity of ConnecticutResearch Topic: Preference for Utilization of Medical Treatmat End of Life
Jean Correll Munn, PhDFlorida State UniversityResearch Topic: Social Work Involvement at the End of Life i
Daniel S. Gardner, PhDNew York UniversityResearch Topic: An Exploratory Evaluation of a PsychoeducaAdults with Advanced Cancer and their Family Caregivers
Betty J. Kramer, PhDUniversity of Wisconsin, MadisonResearch Topic: Innovations in End-of-Life Care for Elders w
Hong Li, PhDUniversity of Illinois, Urbana-ChampaignResearch Topic: Study of Providers of End of Life Care for Fr
Sara Sanders, PhDUniversity of IowaResearch Topic: Hospice Care for Individuals with ProgressivSocial Work Providers and Familial Caregivers
Tracy Schroepfer, PhDUniversity of Wisconsin, MadisonResearch Topic: Assessing the Psychosocial Needs of Termina
Deborah Waldrop, PhDUniversity at BuffaloResearch Topic: At the Eleventh Hour: Psychosocial Factors tCare for Terminally Ill Older Adults
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTIC
SOCIAL WORK POLICY INSTITUTE
APPENDIX N: PENDING LEGISLATION
The Senior Navigation and Planning Act of 2009 (S. 1263 – May 2009)http://warner.senate.gov/public/index.cfm?p=PressReleases&ContentRecord_id=8aa800a1-5eff-42cf-af5f-f42ae841093d&ContentType_id=0956c5f0-ef7c-478d-95e7-f339e775babf&MonthDisplay=6&YearDisplay=2009
Senator Mark Warner has introduced legislation that would expand education and services forfamilies and individuals dealing with terminal illnesses. The bill calls for patients with Medicare toreceive hospice services when diagnosed with 18 months to live as opposed the current standard of6 months to live. Services such as palliative care consultation, patient and family counseling,respite care, and in-home caregiver training would be provided while allowing the patient to stillseek curative treatments. Medicare payments would also be withheld from physicians andhealthcare providers until a patient diagnosed with a terminal illness receives advanced careplanning information. Incentives would be offered from 2011 to 2020 to in-patient hospitals,nursing homes, etc. who obtain accreditation and certification to implement a hospice andpalliative care program. After 2020, these providers would receive a decrease in Medicarepayments (with exceptions) until the accredited and certified hospice and palliative care programis in place. Even more comprehensive discharge planning would be required for hospitals, skillednursing facilities, home health agencies, and hospice programs. Lastly, the Department of Healthand Human Services would develop a public awareness campaign to highlight the importance ofend-of-life planning.
The National Center for Social Work Research Act (S.114 – January 2009)www.govtrack.us/congress/bill.xpd?bill=s111-114
Senator Daniel Inouye has introduced this legislation in each Congress since 1999. It amends thePublic Health Service Act to establish the National Center for Social Work Research as an agencyof the National Institutes of Health (NIH) to conduct, support, and disseminate targeted researchon social work methods and outcomes related to problems of significant social concern. Thelegislation authorizes the Director of the Center to: (1) provide research training and instruction;(2) establish research traineeships and fellowships; (3) provide stipends and allowances; and(4) make grants to nonprofit institutions to provide such training, instruction, traineeships,and fellowships. It directs the Secretary of Health and Human Services to establish an advisorycouncil for the Center.
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 61
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 61

APPENDIX O: SOCIAL WORK RESEARCHERS ONEND-OF-LIFE CARE
Hartford Faculty Scholars and Doctoral Fellows Researching End-of-Life Care
Mercedes Bern-Klug, PhDUniversity of IowaResearch Topic: National Survey of Nursing Home Social Workers
Karen Bullock, PhDUniversity of ConnecticutResearch Topic: Preference for Utilization of Medical Treatment among Older African Americansat End of Life
Jean Correll Munn, PhDFlorida State UniversityResearch Topic: Social Work Involvement at the End of Life in Long-Term Care
Daniel S. Gardner, PhDNew York UniversityResearch Topic: An Exploratory Evaluation of a Psychoeducational Multifamily Group for OlderAdults with Advanced Cancer and their Family Caregivers
Betty J. Kramer, PhDUniversity of Wisconsin, MadisonResearch Topic: Innovations in End-of-Life Care for Elders with Advanced Chronic Disease.
Hong Li, PhDUniversity of Illinois, Urbana-ChampaignResearch Topic: Study of Providers of End of Life Care for Frail Elders in Managed Care.
Sara Sanders, PhDUniversity of IowaResearch Topic: Hospice Care for Individuals with Progressive Dementia: Beliefs and Practices ofSocial Work Providers and Familial Caregivers
Tracy Schroepfer, PhDUniversity of Wisconsin, MadisonResearch Topic: Assessing the Psychosocial Needs of Terminally Ill Elders
Deborah Waldrop, PhDUniversity at BuffaloResearch Topic: At the Eleventh Hour: Psychosocial Factors that Contribute to Delayed HospiceCare for Terminally Ill Older Adults
HOSPICE SOCIAL WORK: LINKING POLICY, PRACTICE, AND RESEARCH REPORT
SOCIAL WORK POLICY INSTITUTE 62
G LEGISLATION
ng Act of 2009 (S. 1263 – May 2009)cfm?p=PressReleases&ContentRecord_id=8aa800a1-5eff-pe_id=0956c5f0-ef7c-478d-95e7-f339e775babf&Month
legislation that would expand education and services forterminal illnesses. The bill calls for patients with Medicare toed with 18 months to live as opposed the current standard ofiative care consultation, patient and family counseling,aining would be provided while allowing the patient to stillyments would also be withheld from physicians andagnosed with a terminal illness receives advanced careld be offered from 2011 to 2020 to in-patient hospitals,ditation and certification to implement a hospice andhese providers would receive a decrease in Medicareaccredited and certified hospice and palliative care programdischarge planning would be required for hospitals, skilleds, and hospice programs. Lastly, the Department of Healthpublic awareness campaign to highlight the importance of
rk Research Act S.114 – January 2009ll=s111-114
this legislation in each Congress since 1999. It amends thethe National Center for Social Work Research as an agency
NIH) to conduct, support, and disseminate targeted researchs related to problems of significant social concern. Thehe Center to: (1) provide research training and instruction;fellowships; (3) provide stipends and allowances; and
ons to provide such training, instruction, traineeships,y of Health and Human Services to establish an advisory
NKING POLICY, PRACTICE, AND RESEARCH REPORT
61
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 62

ABOUT THE SOCIAL WORK POLICY INSTITUTE
The Social Work Policy Institute was established in 2009NASW Foundation. Its mission is:
• To strengthen social work’s voice in public policy delib• To inform policy-makers through the collection and d
work effectiveness.• To create a forum to examine current and future issues
Social Work Policy Institute / NASW Foundation750 First Street NE, Suite 700 • Washington, DC 2000Director: Joan Levy Zlotnik, PhD, ACSWwww.SocialWorkPolicy.org • [email protected]
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 63
ABOUT THE SOCIAL WORK POLICY INSTITUTE
The Social Work Policy Institute was established in 2009 and is a division of theNASW Foundation. Its mission is:
• To strengthen social work’s voice in public policy deliberations.• To inform policy-makers through the collection and dissemination of information on social
work effectiveness.• To create a forum to examine current and future issues in health care and social service delivery.
Social Work Policy Institute / NASW Foundation750 First Street NE, Suite 700 • Washington, DC 20002-4241Director: Joan Levy Zlotnik, PhD, ACSWwww.SocialWorkPolicy.org • [email protected]
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:33 PM Page 64
HOSPICE SOCIAL WORK: LIPRACTICE, AND RE
A REPORT FROM THE MARCSYMPOSIUM
750 First Street NE, Suite 700Washington, DC 20002-4241www.SocialWorkPolicy.org
SWPI-RPT-51710.Hospice-Report:Layout 2 9/14/10 1:32 PM Page 1