hospital medicaid 101- the basics and ub-04 billing guidelines
TRANSCRIPT

Department of Medical Assistance Services
Medicaid 101
www.dmas.virginia.gov

This presentation is to facilitate training of the This presentation is to facilitate training of the subject matter in Virginia Medicaid Hospital subject matter in Virginia Medicaid Hospital Manual. Manual.
This training contains only highlights of the This training contains only highlights of the manual and is not meant to substitute for or take manual and is not meant to substitute for or take the place of the manualthe place of the manual..
Providers are responsible for reviewing and Providers are responsible for reviewing and adhering to all Medicaid manual requirements.adhering to all Medicaid manual requirements.
2

3
Agenda
1. DMAS Website 2. Excluded Individuals/Entities
3. Medicaid Eligibility Verification Options
4. Medicaid Programs and Benefit Packages 5. UB-04 Billing Guidelines

4
DMAS Website www.dmas.virginia.gov
• Current, most up-to-date information on Virginia Medicaid programs
• Provider memos available for review• Access to Medicaid manuals• 50 Common Error Reason Codes with
Resolutions• Numeric Insurance Code List• Primary Carrier Coverage Code List

5
DMAS Websitewww.dmas.virginia.gov
• Financial Reason Code Description List
• Hospital DRG Rates • Medicaid Forms• 2010 Medicaid/FAMIS-PLUS
Handbook

6

7
Excluded Individual/Entities
• No payment can be made for any items or services ordered or prescribed by an excluded physician when the furnishing party either knew or should have known of the exclusion
• Medicaid providers may be subject overpayment liability and civil monetary penalties when they do not abide by this Federal Regulation

8
• This ban includes payment for administrative and management services not directly related to patient care
• Providers are required to identify excluded individuals and entities
• This ensures that DMAS is not paying any excluded individuals or entities for services rendered
Excluded Individual/Entities

9
How to Ensure Program Integrity
• Screen all employees and contractors to determine whether they have been excluded
• Search HS-OIG List of Excluded Individuals/Entities (LEIE) website monthly
• Immediately report to DMAS any exclusion information discovered

10
Reporting• Discoveries are to be sent in writing to the
address below and should include the:– individual or business name– provider identification number
• State action, if any, has been taken
DMASAttn: Program Integrity/Exclusions
600 E. Broad St. Ste 1300Richmond, VA 23219

11
Accessing the LEIE
• HHS-OIG maintains the LEIE• Provides information about parties
excluded from participation in Medicare, Medicaid and all other Federal healthcare programs
• The online database is located athttp://www.oig.hhs.gov/fraud/exclusions.asp

12
As A Participating ProviderYou Must-
• Determine the patient’s identity.• Verify the patient’s age.• Verify the patient’s eligibility.• Accept, as payment in full, the
amount paid by Virginia Medicaid.• Bill any and all other third-party
carriers.
13
DOB: 05/09/1964 F CARD# 00001
DEPARTMENT OF MEDICAL ASSISTANCE SERVICESCOMMONWEALTH OF VIRGINIA
V I RG I N I A J. R E C I P I E N T
9 9 9 9 9 9 9 9 9 9 9 9
002286

14
Medicaid Verification Options
• MediCall • Medicaid Web Portal

15
MediCall/Medicaid Web Portal
Information Available• Medicaid member eligibility/benefit verification
• Service limit information• Claim status• Service authorization• Provider check log• Primary Payer Information• Medallion Participation• Managed Care Organization Assignment

16
Copay Indicators• Code A
– Under 21- No copay exists
• Code B– Long Term Care, Home or Community
Based Waiver Services, Hospice-No copay
• Code C– All other members – collect any/all
applicable copays

17
Copay Exemptions
• Members in managed care may not have copays
• Pregnancy related/family planning services
• Emergency services

Copay Amounts
Inpatient hospital $100.00 per admission
Outpatient hospital clinic $3.00 per visit
Clinic visit $1.00 per visit
Physician office visit $1.00 per visit
Other physician visit $3.00 per visit
18

19
General Exclusion • Payment cannot be made under the
Medicaid Program for certain items and services, and Virginia Medicaid will not reimburse providers for these non-covered services.
• Medicaid members have been advised that they may be responsible for payment to providers for non-covered services.

20
General Exclusion - Directive
• Prior to the provision of service, the provider must advise the Medicaid member that he or she may be billed for a non-covered service.
• A directive signed by the patient, meets Virginia Medicaid’s requirement of patient notification of financial responsibility for non-covered services.

21
MediCall
• 800-884-9730• 800-772-9996• 804-965-9732• 804-965-9733

22
Medicaid Web Portal
• Web-based eligibility verification option–Free of Charge.–Information received in “real
time”.–Secure–Fully HIPAA compliant

23
Changes-• A new enhanced web portal will allow
providers to transact all Medicaid business via one central location.
• The web portal will provide access to:– Member Eligibility Status– Payment History– Remittance Advices– Service Authorization

Registration Process• First Time Users
– Go to www.virginiamedicaid.dmas.virginia.gov – Establish an user ID and password– By registering you are acknowledging yourself as a
staff member with administrative rights for the organization
• Established Users- Delegated Administrators– will receive a letter containing their NPI and
instructions on accessing the Web Portal– must access the Web Portal and change their
temporary password no later than June 27, 2010– will be able to add new users beginning June 28,
2010. 24

25
ACS Web Registration Support Call Center
• Questions regarding new user registration, existing user access letter, or temporary password–1-866-352-0496– Available after June 8, 2010– 8 am – 5 pm Monday thru Friday– No holidays

26
Key Dates and Times
• May 26th – New registration to FHS/UAC discontinued
• Through June 27th
– Current FHS/UAC users can continue to request password resets, routine maintenance, or access information as normal
• June 27th – Access to ARS via FHS/UAC will be
discontinued

27
Key Dates and Times
• June 28th – new registration and users can be added
via the new Virginia Medicaid Web Portal– access to eligibility and claims
information will be available in the new Virginia Medicaid Web Portal at 7:01 am
www.virgniniamedicaid.dmas.virginia.gov

28
Provider Call Center
Claims, covered services, billing inquiries:
800-552-8627 804-786-6273
8:30am – 4:30pm (Monday-Friday)
11:00am – 4:30pm (Wednesday)

29
Provider Enrollment NPI enrollment, EFT sign-up, update
facility contact and email, change of address or phone number:
Provider Enrollment UnitP. O. Box 26803Richmond, VA 23261888-829-5373804-270-5105804-270-7027 - Fax

Medicaid Programs/Benefit Packages

31
Medicaid ProgramsMedicaid
Fee-for-Service
• No Primary Care Physician (PCP)
• No mandatory referral from the PCP.
Medallion • Primary Care
Physician who directs all care.
• PCP referral required for all non-emergency services.

32
Medicaid Programs• FAMIS
– Medicaid program for children under age 19
– First 30 days coverage provided under the FAMIS fee-for-service program
– Mandatory Managed Care Organization assignment (where available) after the initial 30 days of coverage

33
Medicaid Programs
• FAMIS MOMS– For pregnant women with incomes
above the Medicaid income guidelines
– Managed Care Organization assignment rules same as FAMIS
– Apply thru local Department of Social Services or Central Processing Unit
– Baby is not covered until application submitted and approved

34
Medallion II MCO ID Cards• Issued by the Managed Care
Organizations• Medicaid member will have both
MCO and Medicaid cards• Eligibility verification is a
REQUIREMENT• Each verification option will give
the MCO enrollment information if applicable

35
Medallion II MCO ID Cards• The Anthem card for Medicaid members
indicates Anthem Health Keepers Plus (PLUS identifies the Medicaid plan).
• The Optima Card for Medicaid members indicates Optima Family Care (FAMILY CARE identifies the Medicaid plan).
• Virginia Premier - anyone presenting a VA Premier Card is a Medicaid client.

36
Medallion II MCO ID Cards
• CareNet identifies the Southern Health Services card for Medicaid members.
• AMERIGROUP of Virginia is for Medicaid members.

Virginia Medicaid MCO ContactsMedicaid HMO Plan Telephone Number
Anthem HealthKeepers Plus
800-901-0020
Optima Family Care 800-881-2166
Virginia Premier 800-727-7536
CareNet 800-279-1878
AMERIGROUP of Virginia 800-600-444137

38
Member Choice - MCO Selection(Areas Where MCO is Available)
• Member will be enrolled in Medicaid fee-for-service plan for the first 30 days.
• Member will then have 90 days to select an MCO plan.
• During the 90 day period, a member can select a new MCO for the upcoming month as long as the request is received by the 15th of the current month.
• At the end of the 90 day period, the member will be enrolled in the chosen MCO until the next open enrollment period.

39
Managed Care Helpline
1-800-643-2273
TDD# 1-800-817-6608
Monday – Friday
8:30 a.m. – 6:00 p.m.
(Translation Services Available)

40
Client Medical Management- CMM
• Mandatory Primary Care Physician (PCP) and Pharmacist who directs all care
• Responsibilities:– coordinating routine medical care– making referrals to specialists as necessary– arrange 24 hour coverage when not
available– explain to members all procedures to follow
when office is closed or there is an urgent or emergency situation

Client Medical Management - CMM • Services received by a CMM member not provided
by the PCP will be reimbursed only:– in a medical emergency/delay in treatment may cause
death, lasting injury or harm– on written referral from PCP using the Practitioner
Referral Form (DMAS-70), includes covering physicians– covered services excluded from CMM program
requirements• If not a medical emergency or no referral form is
attached, hospital emergency room CMM claims will be denied, not paid at a reduced rate
• CMM patient can be billed for these non-emergency services 41

42
Aliens• Section 1903v of the Social Security Act
requires Medicaid to cover emergency services for specified aliens when the services are provided in an emergency room or inpatient hospital setting.
• Hospital outpatient follow-up visits or physician office visits are not included in the covered services.

43
Aliens• Emergency medical treatment only• Eligibility requests should be sent
to the local DSS• Emergency Medical Certification
form required for claim submission

44
Aliens Covered services must meet
emergency treatment criteria and are limited to :
• Emergency room care• Physician services• Inpatient hospitalization not to exceed limits
established for other Medicaid recipients• Ambulance service to the emergency room• Inpatient and outpatient pharmacy services
related to the emergency treatment

45
Early Periodic Screening Diagnosis and Treatment - EPSDT
• The EPSDT Program is Medicaid’s comprehensive and preventative child health program for individuals under the age of 21.
• Federal law requires a broad range of outreach, coordination, and health services under EPSDT distinct from general state Medicaid requirements.
• The goal of EPSDT is to identify and treat health problems as early as possible.
• EPSDT provides examination and treatment at no cost to the individual.

46
Early Periodic Screening Diagnosis and Treatment - EPSDT
• For individuals under age 21, EPSDT must include the services listed below-
• Screening services, which encompass all of the following services:– Comprehensive health and developmental
history– Comprehensive unclothed physical exam– Appropriate immunizations according to age
and health history– Laboratory tests (including blood lead
screening)– Health education

47
Qualified Medicare Beneficiaries- QMB
• Eligible only for Medicaid payment of Medicare premiums, deductibles, coinsurance and Medicare Advantage Plan copays.
• Medicaid will consider the Medicare deductibles, coinsurance and copays for benefits.
• If Medicare does not cover the service, the service cannot be billed to Medicaid.

48
Qualified Medicare Beneficiaries- QMB Extended
• This group is eligible for Medicaid coverage of premiums, deductibles, coinsurance and Medicare Advantage Plans copays, plus all other Medicaid-covered services.
• Medicaid will consider the Medicare deductibles, coinsurance and copays for benefits.
• Members are also eligible for all Medicaid covered services.

49
Medicare Advantage Plans
• VA Medicaid handles and processes Medicare Advantage Plans the same way as traditional Medicare.
• DMAS does not process the Medicare Advantage Plans as Third Party Liability (TPL)
• Advantage Plan deductible, copay or coinsurance amounts submitted, will be considered by VA Medicaid for payment
•

50
Special Low-Income Beneficiaries- SLMB
• This group is only eligible for Medicaid coverage of the Medicare Part B premium only.
• The member will have a Medicaid number, but will not received a Medicaid card.
• Medicaid will not cover any medical services for this member.

51
Plan First• Medicaid fee-for-service family
planning waiver program• Men and women ages 19 years and
older may be eligible• Participant income must be less than
or equal to 133% of federal poverty level
• Must meet citizenship and identity requirements

52
Plan First• Plan First includes coverage of those
services necessary to prevent or delay a pregnancy
• Family planning does not include counseling about, recommendations for or performance of abortions, hysterectomies or procedures performed for medical reasons such as the removal of intrauterine devices due to infections.

53
Plan First
• Not eligible for the waiver:– Individuals who have major medical
insurance– Individuals who are eligible for full
Medicaid benefits coverage– Individuals who have had a
sterilization procedure

54
Plan First- Covered Services• Plan First covers routine and periodic
family planning office visits and related services.
• Medicaid will only reimburse approved procedure codes and the code must be accompanied with a V25 category (family planning) as a primary diagnosis on the claim.
• Please review the Plan First manual, Chapter IV for codes.

55
Spend Down• Medicaid applicants whose income is
over the Medicaid limit, the applicant may become eligible for a limited period of Medicaid coverage if all other eligibility factors are met.
• This process is called a “spend-down”. • The applicant’s medical expenses must
equal or exceed the difference between his or her income and the Medicaid income limit.

56
Spend Down• If the allowable expenses of the applicant
equal this spend-down amount before the end of a budget period (six months for non-institutionalized individuals or a one month period for institutionalized individuals), the applicant may receive a limited period of Medicaid coverage which will stop at the end of the budget period.
• Eligibility must be re-determined in order to establish eligibility in subsequent budget periods.

57
Medicaid Waiver• There are key requirements with which a
state’s Medicaid program must comply.• These basic requirements govern Medicaid
programs nationwide.– State must make services available to
individuals on a comparable basis.– State must guarantee members freedom of
choice in selecting service providers when obtaining Medicaid services.
– State must make Medicaid services available statewide and provide that individuals have ready access to them.

58
Medicaid Waiver• In some cases the states may request
waivers of some of these requirements.• Medicaid home and community-based
service waiver programs operate under these rules.
• The waiver allows Medicaid to pay for additional services not covered by traditional Medicaid.
• The state has the ability to decide who gets funded for what service (criteria for eligibility and coverage).

59
VA Medicaid Waivers• Alzheimer’s Assisted Living Waiver• Assisted Technology and Environmental
Modifications• Elderly or Disabled With Consumer Direction• HIV/AIDS• Individual and Family Developmental
Supports (IFDDS)• Intellectual Disabilities/Mental Retardation
(ID/MR)• Technology Assisted (Tech)

60
Temporary Detention Order• The General Assembly directed DMAS to
process all requests for payment of services rendered as a request of Civil/Criminal Mental Temporary Detention Orders (TDO) effective July 1, 1995.
• Any magistrate may, within the specified guidelines, issue a temporary detention.
• A law enforcement officer executes Temporary Detention Orders.
• Employee of the community services board or its designee shall determine the facility of temporary detention for all individuals.

61
Temporary Detention Order• The duration of the temporary detention
shall not exceed 48 hours prior to a hearing.
• If the forty-eight hour period herein specified terminated on a Saturday or Sunday, or a legal holiday, such person shall be detained until the next day which is not a Saturday, Sunday or legal holiday, but in no event may be detained longer than 96 hours.

Temporary Detention Order• Hospitals and physicians must submit claims to
DMAS as the result of issuance by a court.• DMAS will accept only the original claim forms.• All TDO submissions must have the TDO form
attached to the claim with the pre-printed case identification number.
• Failure to provide the TDO form will result in claims being returned to the provider for incomplete information.
• The Execution section on the TDO form must be signed by the law enforcement officer and dated to be valid. 62

63
Temporary Detention Order• Processing of TDO claims includes both
Medicaid-eligible and non-Medicaid eligible patients.
• TDO is the payer of last resort and attempts must always be made to first bill the primary carrier , including Medicaid, prior to billing TDO.
• Each claim will be researched for coverage by another resource.
• If the patient has other resources, the claim will be returned to the provider.
• The returned claim will have a letter attached, advising the provider to bill primary payer.

Fiscal Agent Transition
Updates and Changes

Paper Claims• Process for submitting claims remains the same• Continue to send to the appropriate P.O. Box• Claims received
– By close of business 6/21 will process as usual• Inquiry on clean claims should be available on or
after 6/28• Should be on 7/2 remit
– From 6/22-6/27 will be held and processed on 6/28• Inquiry on clean claims will not be available until
at least 6/28• Will not be on remit until 7/9 65

66
Paper Claims Requirements• Claims must be submitted on the original
red and white claim form• The National Uniform Billing Committee and
National Uniform Claims Committee standards and specifications must be met for margins, formats, and fonts:
• 10 pitch Pica type• 6 lines per in vertical• 10 characters per inch

67
Electronic Data Interchange (EDI)• EDI Claims received by 5:00 pm June 24
– Will process as usual– Should be available for inquiry 6/28– Should be on 7/9 remit
• EDI Claims received after 5:00 pm June 24– Will be processed starting June 28

68
Electronic Data Interchange (EDI)
• Requirements– You or your designee must have
established and been given a• New user ID• New password• New File Transfer Protocol (FTP)

69
Trader Partner Testing• Communications validation testing is
being conducted– Clearinghouses– Service centers– Software vendors
• Letter sent to all trading partners containing information regarding testing of EDI batch processing

70
Trader Partner Testing
• If you or your designee has not received this letter– email [email protected]– four position submitter ID– contact information

71
Hospital Billing Guidelines

72
MAIL CMS-1450 FORMS TO:
DEPARTMENT OF MEDICAL ASSISTANCE SERVICES
FacilityP. O. Box 27443
Richmond, Virginia 23261-7443

73
TIMELY FILING• ALL CLAIMS MUST BE SUBMITTED AND
PROCESSED WITHIN ONE YEAR FROM THE DATE OF SERVICE
• EXCEPTIONS– Retroactive/Delayed Eligibility– Denied Claims
• NO EXCEPTIONS– Accidents– Other Primary Insurance

74
TIMELY FILING
• Submit claims with documentation attached (to the back of claim) explaining the reason for delayed submission

CMS-1450 CLAIM FORM:Use ONLY the ORIGINAL
RED & WHITEInvoice
Photocopies are not Acceptable
Computer generated claims must match NUBC uniform standards
75

76
Locator 1:Provider’s Name, Address and Phone Number
• Enter the provider’s name, complete mailing address and telephone number of the provider that is submitting the bill and which payment is to be sent.
• NOTE: DMAS will need to have the 9 digit zip code on line four, left justified for adjudicating the claim.

Locator 1: Provider Name, Address and Phone Number
77
1Our Neighborhood Hospital121 Friendly StreetAny Town VA
12345-6456 8049781234

3a PAT.CNTL #b. MEDREC. #
123456789ABCDEFGH012987654321HGFEDCBA1234567
78
Patient Control Number (not to exceed 20 characters) and Medical/Health Record Number (not to exceed 24 characters) are required for all UB-04 claim submissions.
Locators 3a:Patient Control Number3b: Medical Record Number

4 TYPE OF BILL
Locator 4: Type of Bill
0111OriginalBillInp
atien
t Hos
pital
79

• 0111- Original Inpatient Hospital Invoice• 0112- Interim Inpatient Hospital Invoice*• 0113- Continuing Inpatient Hospital Invoice*• 0114- Last Inpatient Hospital Invoice *• 0117- Adjustment Inpatient Hospital • 0118- Void Inpatient Hospital Invoice• Only “APROVED” claims can be adjusted or
voided
Locator 4: Enter the code as appropriate.Valid codes for VA Medicaid
Inpatient Bill Types
1280

81
*The proper use of these codes will enable DMAS to reassemble cycle-billed claims to form DRG cases for purposes of DRG payment calculations and cost settlement.

4 TYPE OF BILL
Locator 4: Type of Bill
0131OriginalBillOutp
atien
t
Hospit
al
0131- Original Outpatient Invoice0131- Original Outpatient Invoice0137- Adjustment Outpatient Invoice0137- Adjustment Outpatient Invoice0138- Void Outpatient Invoice0138- Void Outpatient Invoice 82

83
Locator 6: Statement Covered Period
• For hospital admissions, the billing cycle for general medical surgical services has been expanded to a minimum of 120 days for both children and adults, except for psychiatric services.
• Interim claims (bill types 0112 or 0113) submitted with less than 120 days will be denied.
• Bill types 0111 or 0114 submitted with greater than 120 days will be denied.

6 STATEMENT COVERS PERIOD FROM THROUGH
Enter the beginning and ending service dates reflected by this invoice (include both covered non-covered days). Use both “from” and “to” for a single day.
030710 030710
84
Locator 6: Statement Covers Period

b
8 PATIENT NAME
a
Enter the last name, first name and middle initial of the patient.
Last First M
85
Locator 8: Patient Name/Identifier

10 BIRTHDATE
Enter the date of birth of the patient using thefollowing format - MMDDYYYY.
10011980
86
Locator 10: Patient Birthdate

11 SEX
Enter the sex of the patient as recorded at admission, outpatient or start of care.
M = Male; F = Female; U = Unknown
F
87
Locator 11: Sex

88
Locator 12: Admission/Start of Care
• The start date for this episode of care. For inpatient services this is the date of admission. For all other services, the date the episode of care began:
IP- Day admitted OP- Day episode of care began

030510
ADMISSION 12 DATE
89
Locator 12: Admission/Start of Care

ADMISSION13 HR22
Enter the hour during which the patient was admitted for inpatient or outpatient care. NOTE: Military time is used as defined by NUBC. 90
Locator 13: Admission Hour
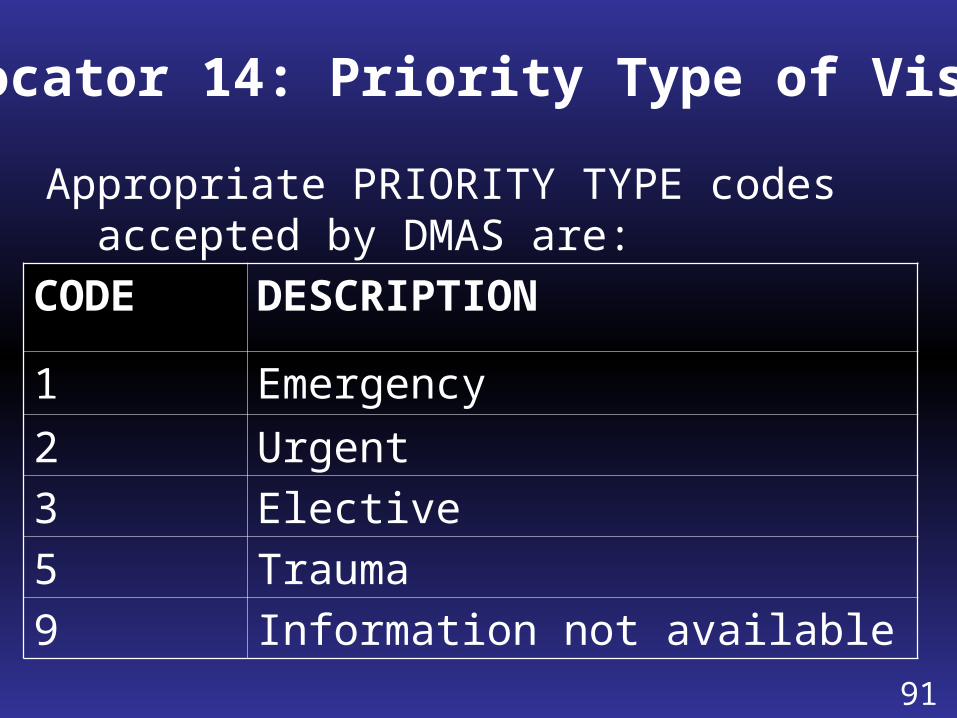
Appropriate PRIORITY TYPE codes accepted by DMAS are:
CODE DESCRIPTION
1 Emergency2 Urgent3 Elective5 Trauma9 Information not available
Locator 14: Priority Type of Visit
91
ADMISSION 14 TYPE
9Enter the code indicating the priority of this admission /visit.
92
Locator 14: Priority Type of Visit

Source of Referral for Admission or VisitAppropriate codes accepted by DMAS are:
Code Description1 Physician Referral
2 Clinic Referral
4 Transfer from Another Acute Care Facility
5 Transfer from a Skilled Nursing Facility
6 Transfer from Another Health Care Facility
7 Emergency Room
8 Court/Law Enforcement
9 Information not available
D Transfer from Hospital Inpatient in the Same Facility

815 SRC
Enter the code indicating the source of theReferral for this admission or visit.
94
Locator 15: Source of Referral for Admission/Visit

16 DHR
15 Enter the code indicating the discharge hour of the patient from inpatient care. NOTE: Military time is used as defined by the NUBC.
Locator 16: Discharge Hour
95

Locator 17:Patient Discharge Status
Appropriate codes accepted by DMAS in claims processing:
Code Description01 Discharge to Home
02 Discharged/transferred to Short Term General Hospital for Inpatient Care
03 Discharged/transferred to SNF
04 Discharged/transferred to ICF
05 Discharged/transferred to Another Facility not Defined Elsewhere

Locator 17:Patient Discharge Status
Appropriate codes accepted by DMAS in claims processing:
Code Description
07 Left Against Medical Advice/Discontinued Care
20 Expired
30 Still a Patient
50 Hospice – Home
51 Hospice – Medical Care Facility

Locator 17:Patient Discharge Status
Code Description
61 Discharge/transfer to Hospital Based Medicare Approved Swing Bed
62 Discharged/transferred to an Inpatient Rehabilitation Facility
63 Discharged/transferred to a Medicare Certified Long Term Care Hospital
64 Discharged/transferred to Nursing Facility Certified Under Medicaid but not Medicare
65 Discharged/transferred to Psychiatric Hospital or Psychiatric Distinct Part Unit of Hospital

99
Locator 17: Patient Status
Correct reporting of patient status code will facilitate quick and accurate determination of DRG reimbursement. In particular, accurate reporting of the values 01,02,05, and 30 will be very important in DRG methodology.

17 STAT
01Enter the code indicating the disposition or Discharge status of the patient at the end for theService period covered on this bill (StatementCovered Period, Locator 6).
NOTE: If the patient was a one-day treatment, enter code “01”.
100
Locator 17: Patient Discharge Status

Locators 18-28: Condition Codes
• These codes are used by DMAS in the adjudication of claims:
Code Description39 Private Room Necessary40 Same Day TransferA1 EPSDTA4 Family PlanningA5 DisabilityA7 Induced Abortion Danger to Life

Locators 18-28:Condition Codes
• These codes are used by DMAS in the adjudication of claims:
Code Description
AA Abortion Performed Due to Rape
AB Abortion Performed Due to Incest
AD Abortion Performed Due to Life Endangering Physical Condition
AH Elective Abortion
AI Sterilization

Condition Codes18 19 20 21 22 23 24 25 26 27 28
Enter the code (s) in alphanumeric sequence Used to identify conditions or events related to this bill that may affect adjudication.NOTE: DMAS limits the number of codes to a maximum of 8 on one claim.
30
103
40
Locators 18-28: Condition Codes(Required if Applicable)

VA29 ACDT
STATE
Enter if known, the state ( two digit Postal State Code abbreviation) where the motorvehicle accident occurred.
104
Locator 29: Accident State
(Conditional)

30
CROSSOVERNOTE: DMAS is requiring for Medicare Part Acrossover claims that the word “CROSSOVER”be in this locator.
105
Locator 30: Crossover Part A Indicator
(Required If Applicable)

31 OCCURRENCE CODE DATE
Enter the code and associated date defininga significant event relating to this bill. Enter codes in alphanumeric sequence.
ab
A3 030110
106
Locators 31-34:Occurrence Codes and Dates
(Required If Applicable)

Enter the code and related dates that identifyan event that relates to the payment of theclaim. Enter codes in alphanumeric sequence.
35 OCCURRENCE SPANCODE FROM THROUGH
ab
107
Locators 35-36:Occurrence Codes and Span Dates
(Required If Applicable)

108
• DMAS will capture the number of covered or non-covered day (s) or units for outpatient services with these required value codes:80 Enter the number of covered days for
inpatient hospitalization or the number of days for re-occurring outpatient claims. 81 Enter the number of non-covered days
for inpatient hospitalization
Locators 39-41:Value Codes and Amounts

Locators 39-41: Value Codes and Amount
• Enter the appropriate code (s) to relate amounts or values to identify data elements necessary to process this claim.
• One of the following codes must be used to indicate coordination of third party insurance carrier benefits
82 No Other Coverage83 Billed and Paid
(Enter Amount Paid by Primary Carrier)85 Billed Not Covered/No Payment
(Documentation Required) 109

110
Locators 39-41: Value Codes and Amount
• For Part A Medicare Crossover Claims, the following codes must be used with one of the third party insurance carrier codes:
A1 Deductible from Part A
A2 Coinsurance from Part A
Other codes may be used if applicable.

a
b
c
d
80 25
39 VALUE CODES
CODE AMOUNT
40 VALUE CODESCODE AMOUNT
41 VALUE CODESCODE AMOUNT
83 A1 1100 00
Value Codes and AmountLOCATORS 39-41:
7841
08
111

112
Locator 42: Revenue Code
Enter the appropriate revenue code (s) for the service provided. Note:
• Multiple services for the same item, providers should aggregate the service under the assigned revenue code and then total the number of units that represent those services
• DMAS has a limit of five pages for one claim
• The Total Charge revenue code (0001) should be the last line of the last page of the claim

42 REV. CD.1
234
0123025103000330Revenue codes are four digits, leading
zero, leftjustified and should be reported in ascendingnumeric order.
113
Locator 42: Revenue Code

114
Outpatient Hospital Setting Billing Requirements for NDC
• CMS requirements related to the Deficit Reduction Act (DRA) of 2005, mandate DMAS to require hospital providers who bill drug products administered in an outpatient hospital setting to include the National Drug Code (NDC) information of the drug dispensed on all claim submissions.

115
Outpatient Hospital Setting NDC Billing Requirements
• The NDC information will be required on all electronic (ASC X12N:837I) and paper (Universal Billing “UB”) claim submissions.
• This requirement also applies to Medicare Crossover claim submissions.
• Outpatient hospital claims submitted without a valid NDC will have the revenue code line reduced to a non-covered service line.

116
Outpatient Hospital Setting NDC Billing Requirements
• Providers billing for compound medication with more than one NDC included in the medication dispensed, each applicable NDC must be submitted on a separate claim line to include both prescription and over-the-counter ingredients.
• Each claim line submitted with pharmacy revenue codes 0250-0259 and 0630-0639 will require the NDC information.

Outpatient Hospital Setting NDC Billing Requirements
• Effective 07/01/08, a valid NDC will be required for all drug products administered in an outpatient hospital setting.
• By definition, a valid NDC is a formatted number using the 5-4-2 format, i.e., 5-digits, followed by 4-digits, followed by 2-digits:– 99999888877
• Each NDC must be an 11-digit code unique to the manufacturer of the specific product administered to the patient.
117

118
Outpatient Hospital Setting NDC Locator 43: Billing Requirements
• Form Locator 43 must have N4 modifier as the first indicator in this field, the corresponding 11-digit NDC number, followed by the Unit of Measure Qualifier and the NDC unit quantity.
• Billing for the same medication dispensed in different packages, each package size MUST be listed separately using N4 modifier, the revenue code, and all the required information on separate lines.
• The DMAS system will not consider these drugs as duplicates.

Outpatient Hospital Setting NDC Billing Requirements
• If available, providers should enter the HCPCS code in Locator 44 (HCPCS/Rate/HIPPS Code) and the HCPCS units in Locator 46 (Serv Unit).
• DMAS will validate all HCPCS codes. • Submission of an invalid HCPCS code will cause
denial of the entire claim.• The NDC number submitted to Medicaid must
be the actual NDC number on the package or container from which the medication was administered.
119

N412345678901UN1234.567RadiologyRadiology
43 DESCRIPTION
Enter the standard abbreviated description of the related revenue code categories included on this bill. 120
Locator 43: Revenue Description

R&B-2 Bed-PediatricDrugs-GenericLaboratory (Lab) General
43 DESCRIPTION
Enter the standard abbreviated description of the related revenue code categories included on this bill. 121
Locator: Revenue Description

44 HCPCS / RATE / HIPPS CODE
Inpatient: Enter the accommodation rate. Outpatient: Enter the applicable code.When billing for outpatient surgery, enter the CPTcode on the same line as revenue code 0490.
112
Locator 44:HCPCS/Rates/HIPPS Rate Codes
122

45 SERV. DATE
Enter the date the outpatient service was provided.
030510
123
Locator 45: Service Date

46 SERV. UNITS
612
Outpatient: Enter the unit (s) of service for physical therapy, occupational therapy or speech-language pathology visit or session(1 visit = 1 unit, even if more than 1 modality is done).
Inpatient: Enter the total number of coveredaccommodation days or ancillary units of service where appropriate.
124
Locator 46: Service Units

47 TOTAL CHARGES
1755 75305 29
Enter the total charge (s) for the primary payer pertaining to the related revenue code for the current billing period as entered in the statement covers period. Total charges include both covered and non-covered charges. Note: Use code “0001” for TOTAL.
125
Locator 47: Total Charges

48 NON-COVERED CHARGES
75 00
To reflect the non-covered charges for the primary payer as it pertains to the relatedrevenue code.
126
Locator 48: Non-Covered Charges

127
Locator 50: Payer Name A-C
• Enter the payer from which the provider may expect some payment for the bill.
• When Medicaid is the only payer, enter “Medicaid” on line A.
• If Medicaid is the secondary or tertiary payer, enter on lines B or C.

50 PAYER NAME
A Primary Payer
B Enter the secondary payer identification, if applicable.
C Enter the tertiary payer if applicable. 128
Medicaid
Locator 50: Payer Name

56 NPI1234567890
129
Providers must list their NPI in this field.
Locator 56: NPINational Provider Identifier

A
B
C
58 INSURED’S NAME
Enter the name of the insured person covered bythe payer in locator 50. The name on the Medicaidline must correspond with the member namewhen eligibility is verified.
Virginia J. Member
130
Locator 58: Insured’s Name

131
• Note: appropriate codes accepted by DMAS are:
Code Description01 Spouse18 Self19 Child21 Unknown39 Organ Donor40 Cadaver Donor53 Life PartnerG8 Other Relationship
Locator: 59 Patient’s Relationship to Insured

52 REL. INFO18
Enter the code indicating the relationship of the insured to the patient.
132
Locator 59: Patient’s Relationship to Insured

60 INSURED’S UNIQUE ID
012345678910
For lines A-C, enter the unique identification number of the person insured that is assigned by the payer organization shown on lines A-C, Locator 50. NOTE: The Medicaid member ID number is 12 numeric digits.
Locator 60: Insured’s Unique Identification

A
B
63 TREATMENT AUTHORIZATION CODES 12345678910
Enter the 11 digit Service Authorization (SA) number
assigned by KePRO for the appropriate inpatient and outpatient services as required
by Virginia Medicaid. 134
Locator 63: Treatment Authorization Codes

135
Locator 64:Document Control Number
• This locator is to be used to list the original Internal Control Number (ICN) for APPROVED claims that are being submitted to adjust or void the original claim.

200936312345670164 DOCUMENT CONTROL NUMBER
The control number (ICN) assigned to the original bill by Virginia Medicaid as part of their internal claims reference number. Only required to adjust or void previously approved claims. 91
Locator 64: Document Control Number

966DX
The qualifier that denotes the version of theInternational Classification of Diseases. Qualifier = 9 for the Ninth Revision. NOTE: Virginia Medicaid currently only accepts a 9 in this locator. 137
Locator 66: Diagnosis and ProcedureCode Qualifier (ICD Version Indicator)

138
Locator 67 Principal Diagnosis CodeLocators 67A-Q
Present on Admission (POA) Indicator• The eighth digit of the Principal, Other and
External Cause of Injury Codes are to indicate if:– the diagnosis was know at the time of
admission, or – the diagnosis was clearly present, but not
diagnosed, until after the admission took place or
– was a condition that developed during an outpatient encounter

Locators 67 A-Q: Present on Admission (POA) Indicator
• The POA indicator should be listed in the shaded area. This field is required for hospitals, (06/30/09 Memo). Reporting codes are:
CODE DEFINITION Y YES N NO U No information in the record W Clinically undetermined
139

67 A B C
I J K L
Enter the diagnosis codes corresponding to allconditions that coexist at the time of admission,that develop subsequently, or that affect the treatment received and/or the length of stay.NOTE: Do not use decimals.
140
Locator 67: Principal Diagnosis Code
Locators A-QPresent on Admission (POA) Indicator

69 ADMIT
DX
Enter the diagnosis code describing the patient’s diagnosis at the time of admission.NOTE: Must be a current ICD-9 code. Do not use decimals.
4019
141
Locator 69: Admitting Diagnosis

34501 b c70 PATIENTREASON DXEnter the diagnosis code describing the patient’s reason for visit at the time of outpatient registration.
142
Locator 70a-c: Patient’s Reason for Visit
(Required If Applicable)

E895 c72ECI b
Enter the diagnosis code pertaining to externalcauses of injuries, poisoning, or adverse effect.
143
Locator 72:External Cause of Injury
(Required If Applicable)

Locator 74: Principal Procedure Code and Date• Note: for outpatient claims, a procedure code
must appear in this locator when revenue codes 0360-0369, 0420-0429, 0430-0439, and 0440-0449 (if covered by Medicaid) are used in Locator 42 or the claim will be rejected.
• For inpatient claims, a procedure code or one of the diagnosis codes of V64.1 through V64.3 must appear in this locator (or Locator 67) when revenue codes 0360-0369 are used in Locator 42 or the claim will be rejected.144

030510
74 PRINCIPAL PROCEDURE CODE DATE
Enter the ICD-9-CM procedure code that identifies the inpatient principal procedurePerformed at the claim level during the periodCovered by this bill and the corresponding date.
6501
145
Locator 74: Principal Procedure Code and Date
(Required If Applicable)

6601 030710
a. OTHER PROCEDURE CODE DATE
Enter the ICD-9-CM procedure codes identifyingall significant procedures other than the principal procedure and the dates on which the procedures were performed. Report those that are most important for the episode of care and specifically any therapeutic procedures closely related to the principal diagnosis.
146
Locator 74a-e: Other Procedure Codes and Date
(Required If Applicable)

76 ATTENDING
NPI 1234567890
Enter the NPI for the physician who has overall responsibility for the patient’s medical care and treatment reported on this claim.
147
Locator 76:Attending Provider

77 OPERATING
NPI 1234567890
Enter the NPI of the individual with the primary responsibility for performing the surgical procedure (s).
148
Locator 77:Attending Provider

149
Locators 78-79:Other Provider Name and Identifiers• This field will be used to list the NPI for
the Primary Care Physician (PCP) who authorized the inpatient stay or outpatient visit.
• For MEDALLION patients referred to an outpatient clinic, enter the NPI for the PCP who authorized the outpatient visit.
• This information is required for all MEDALLION patients treated for non-emergency services.

150
Locators 78-79:Other Provider Name and Identifiers
• For Client Medical Management (CMM) patients referred to the emergency room by the PCP or admitted for non-emergency inpatient stay, enter the provider’s ID number and attach the Practitioner Referral Form (DMAS-70).

78 OTHER NPI 1234567890The NPI of the Primary Care Physician is
required for Medallion and Client Medical Management (CMM) patients admitted for
non-emergency treatment.
151
Locator 78:Other Provider Name and Identifier

80 REMARKS
Enter additional information necessary to adjudicate the claim. Enter a brief description of the reason for the submission of the adjustment or void. If there is a delay in filing, indicate the reason for the delay here and include an attachment. 152
Locator 80: Remarks Field

153
TAXONOMYLocator 81: Code-Code Field
• DMAS will be using this field to capture a taxonomy code for claims that are submitted for one NPI with multiple business types or locations (e.g., Rehabilitative or Psychiatric units within an acute care facility, Home Health Agency with multiple locations).

154
TAXONOMYLocator 81: Code-Code Field
• The taxonomy code will be required for providers who do not have a separate NPI for each different service billed to VA Medicaid.
• The taxonomy code will also be required for providers who have one NPI for multiple business locations.
• Code B3 is to be entered in the first small space and the provider taxonomy code is to be entered in the second large space. The third space should be blank.

81CC a
b
c dEnter the provider taxonomy code for the
billing provider when the adjudication of the claim is known to be impacted.
B3 282N00000X
155
Locator 83: Code-Code Field

DMAS Service Types That May Require a Taxonomy Codes
Service Type Description Taxonomy Code (s)
Hospital, General 282N00000X
Laboratory 291U00000XRehabilitation Unit of Hosp.
273Y00000X
Psychiatric Unit of Hospital
273R00000X
Private Mental Hospital (IP)
283Q00000X
Rehabilitation Hospital 283X00000X 156

Outpatient Surgery• For elective outpatient surgical procedures
which require Service Authorization (SA) by Medicaid Medical Support (Physician’s Manual, Appendix B), submit paper claim.
• Contact the surgeon and request a copy of his SA letter ( the facility services do not required service authorization).
• Attach a copy of the SA letter to the back of your claim form.
• Do not put the Physician’s SA # on your claim.• Charges- including facility- for elective
surgery not approved with a service authorization, will be denied. 157

Medicare Primary
Crossover Claims

159
Medicare Primary Billing Instructions for CMS-1450
• The word “CROSSOVER” must be entered in Block 30 of the UB-04 to identify Medicare crossover claims.
• Coordination of Benefits (COB) codes 83 and 85 must be accurately printed in Blocks 39-41 of the UB-04.

160
Medicare Primary Billing Instructions for CMS-1450
• The first occurrence code 83 indicates that Medicare paid and there should always be a dollar value associated with this code. The A1 indicates Medicare deductible and code A2 indicates Medicare coinsurance

161
Medicare Primary: Blocks 39-41
• Line a 83 = Billed and Paid (enter amount paid by Medicare or other insurance).
• Line a A1 = Deductible Payer A. (enter Medicare Deductible Amount listed on the EOMB).
• Line a A2 = Co-Insurance Payer A. (enter Medicare Co-Insurance amount listed on the EOMB).

Medicare Primary Billing Instructions for CMS-1450
• Note: Complete all information in Locators 39a through 41a first (payments by Medicare or payments by other insurance) before entering information in 39b through 41b locators etc.
• COB code 85 is to be used when another insurance carrier is billed and there is no payment from that carrier.
• For the deductibles and co-insurance due from any other carrier (s) (not Medicare) the code for reporting the amount paid is B1 for the deductibles and B2 for the coinsurance.
162
163
Medicare Exhaust Days
• MEDICARE PRIMARY/Days Exhausted – Service authorization from KePRO
is required.– Proof of exhausted Medicare days
must be submitted with service authorization request.

164
Medicare Exhaust Days
• All days must be billed.• Initial stay less than 120 days, bill type
0111.• First 120 days bill type 0112 – next 120
days bill type 0113 – continue bill type 0113 for any additional 120 day periods.
• Final bill type 0114.

165
Medicare Exhaust Days
• Providers should list the amount Medicare paid on the 0112 bill type (less than 120 days list payment on 0111 bill type).
• Medicare payment should be listed in Block 39a and use COB code 83 (billed and paid).

166
Medicare Exhaust Days• DO NOT WRITE the word
CROSSOVER in Block 30 (Medicare is exhausted and the days billed to Medicaid were not paid by Medicare)
• Block 80- providers MUST put write a statement MEDICARE DAYS EXHAUSTED and attach something showing Medicare are exhausted (Medicare EOB).

167
Medicare Exhaust Days• If Medicaid has considered a crossover
claim for deductible and coinsurance on days Medicare paid or any Part B charges-– If the provider keeps all charges on the
claim submitted for Medicare Exhaust days, all payments must be listed.
– If the provider deletes Part B charges, do not list any Part B payment amounts.

168
Special Note
• If the Medicaid member does not have Part A coverage, the COB code should be 82 (No Other Coverage).

THANK YOU
Department of Medical Assistance Services
www.dmas.virginia.gov