hospital simulated patient programme: a guide
TRANSCRIPT
Hospital simulatedpatient programme:a guideJenny Barrett and Jan Hodgson, Department of Paediatrics, University of Melbourne,Melbourne, Victoria, Australia
SUMMARYContext: Many university coursesemploy simulated patients towork with students in the devel-opment of communication skills.Our challenge was to build asustainable programme that couldbe adapted for medical, nursingand allied health staff, andgroups of students, on our hos-pital campus.Innovation: In recognition of theneed to provide practice oppor-tunities for junior medical staff tohone their capacity to communi-
cate effectively with parents, weemployed professional actors whoare also qualified teachers. Juniordoctors have multiple opportuni-ties over their training time towork one-to-one with an actor-tutor in the role of simulatedparent. The simulated parents areskilled in helping the traineesreflect on the conversation, andthe trainees are given a recordingof their sessions for furtherreflection and feedback from acolleague. This model has beenadapted to meet the ‘topic’ needs
and scheduling requirements ofother staff and hospital-basedstudent groups.Discussion: In adapting the ori-ginal medical staff programme, wecame to appreciate not only thelogistical but also the ethicalconsiderations inherent in a sim-ulated parent ⁄ patient programme.Our guide highlights the impor-tance of safeguarding the educa-tional integrity of the design,maintaining the fidelity of thesimulations and ensuring thesafety of all involved.
Many universitycourses employsimulatedpatients to workwith students indevelopment ofcommunicationskills
How todo it
� Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 217–221 217

INTRODUCTION
The pursuit of excellence ininteractions with patientsand their families remains a
high priority for clinicians andtheir educators, and simulation isa popular method for learningabout communication. In thecontext of busy hospitals, creat-ing and sustaining a clinicalcommunications educationprogramme is particularlychallenging.
Over the last decade, we haverefined a simulated patient ⁄ parenteducation programme for medicaland nursing staff in a large teach-ing hospital.1 Initially, we soughtwisdom from the education andclinical education literature,2–5
and eventually, through trial anderror, and systematic evalua-tions,6,7 developed a workablemodel that is well regarded by thehundreds of clinical staff and stu-dents who have participated.Based on this experience, we cannow offer to other hospital educa-tors a concise practical guide torunning such a programme.
Over time, we have come tounderstand some of the subtletiesthat were not apparent at thebeginning. Therefore, underlyingthe operational steps explainedbelow are three principles thatneed to be considered in thecomplex and time-pressuredenvironment of hospital educa-tion for professionals: the educa-tional integrity of the whole(participating in the workshopand the simulations with multiplereflection and feedback); thefidelity of the simulations(authentic acting, protectedindividual learning time); and thesafety of participating staff (pri-vacy for practice, and confidenti-ality of records and recordings)and actor-tutors. Our experiencehas repeatedly reinforced theimportance of these principles.
We use the term ‘actor-tutor’to denote the person who isemployed in the role of ‘simulatedparent ⁄ patient’. Although theterms ‘standardised patient’ and‘standardised family member’ areused elsewhere,1,6 our terminol-ogy attempts to acknowledge thespecial roles of both the profes-sional actor-tutors and parents.
PROGRAMME OVERVIEW
In our programme we first conducta workshop on a particular topicof clinical communication (e.g.giving bad news to parents), atwhich, through group discussion,we deconstruct a DVD that wehave previously made that modelsgood communication on that to-pic. We provide written notes andsuitable references for individualfollow-up and reinforcement. Theworkshop facilitator stresses theimportance of practising what hasbeen modelled and discussed inthe workshop. Learners areencouraged to register to have aone-to-one simulation sessionwith one of the actor-tutors at ascheduled time in the forthcom-ing week or two. The simulation isrecorded and the learner is givena DVD of their work for self-appraisal and subsequent discus-sion with a colleague.
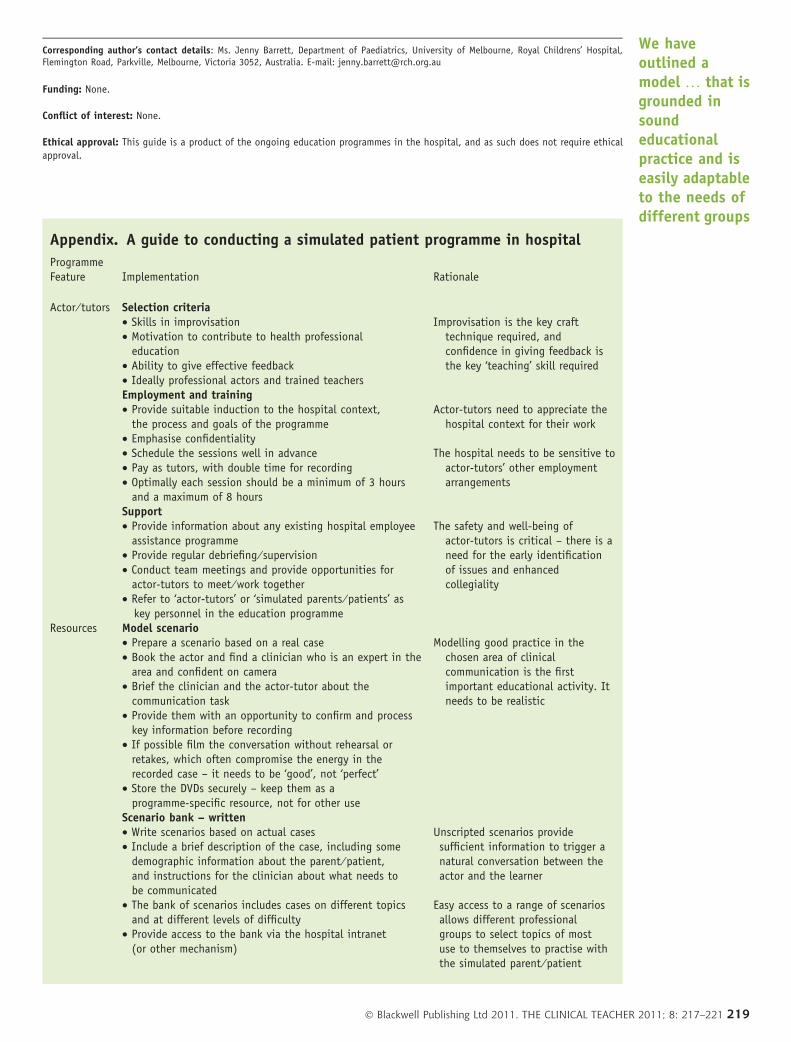
The appendix provides a guideto conducting a programme in ahospital, and highlights practicalsuggestions and the educationalrationale based on ourexperience.
CONCLUSION
We have outlined a model basedon our experience of conducting asimulated parent programme formedical staff in a hospital thathas been adapted and furtherrefined for graduate nurses andMaster of Genetic Counsellingstudents. This is grounded insound educational practice and
has proven to be easily adaptableto the needs of different groupswithout compromising its valueand integrity.
REFERENCES
1. Gough J, Roseby R, Marks M.
Rehearsing the art of clinical practice.
Med Educ 2004;38:545–546.
2. Kurtz S, Silverman J, Draper J. Teach-
ing and learning communication skills
in medicine. 2nd ed. Abingdon, Oxon,
UK: Radcliffe Publishing; 2005.
3. Lorin S, Rho L, Wisnivesky JP, Nier-
man DM. Improving medical student
intensive care unit communication
skills: A novel educational initiative
using standardized family members
2006;34:2386–2391.
4. Nikendei C, Bosse HM, Hoffmann K,
Moltner A, Hancke R, Conrad C,
Huwendiek S, Hoffmann GF, Herzog W,
Junger J, Schultz JH. Outcome of
parent–physician communication
skills training pediatric residents.
Patient Education and Counseling
2006;82:94–99.
5. Chur-Hansen A, Burg F. Working with
standardized patients for teaching
and learning. Clin Teach 2006;3:220–
224.
6. Gough J, Waldron S, Johnston L, Tyler
P. Rehearsing clinical communication:
Innovative education in a graduate
nurse programme in paediatrics. Nurse
Education in Practice 2009;9:209–214.
7. Gough J, Frydenberg A, Donath S,
Marks M. Simulated parents:
Developing paediatrics trainees’
communication skills in giving bad
news. Journal of Paediatrics and Child
Health 2009;45:133–138.
Creating andsustaining a
clinicalcommunications
educationprogramme is
particularlychallenging
218 � Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 217–221
Corresponding author’s contact details: Ms. Jenny Barrett, Department of Paediatrics, University of Melbourne, Royal Childrens’ Hospital,Flemington Road, Parkville, Melbourne, Victoria 3052, Australia. E-mail: [email protected]
Funding: None.
Conflict of interest: None.
Ethical approval: This guide is a product of the ongoing education programmes in the hospital, and as such does not require ethical
approval.
Appendix. A guide to conducting a simulated patient programme in hospital
ProgrammeFeature Implementation Rationale
Actor ⁄ tutors Selection criteria• Skills in improvisation• Motivation to contribute to health professional
education• Ability to give effective feedback• Ideally professional actors and trained teachers
Improvisation is the key crafttechnique required, andconfidence in giving feedback isthe key ‘teaching’ skill required
Employment and training• Provide suitable induction to the hospital context,
the process and goals of the programme• Emphasise confidentiality• Schedule the sessions well in advance• Pay as tutors, with double time for recording• Optimally each session should be a minimum of 3 hours
and a maximum of 8 hours
Actor-tutors need to appreciate thehospital context for their work
The hospital needs to be sensitive toactor-tutors’ other employmentarrangements
Support• Provide information about any existing hospital employee
assistance programme• Provide regular debriefing ⁄ supervision• Conduct team meetings and provide opportunities for
actor-tutors to meet ⁄ work together• Refer to ‘actor-tutors’ or ‘simulated parents ⁄ patients’ as
key personnel in the education programme
The safety and well-being ofactor-tutors is critical – there is aneed for the early identificationof issues and enhancedcollegiality
Resources Model scenario• Prepare a scenario based on a real case• Book the actor and find a clinician who is an expert in the
area and confident on camera• Brief the clinician and the actor-tutor about the
communication task• Provide them with an opportunity to confirm and process
key information before recording• If possible film the conversation without rehearsal or
retakes, which often compromise the energy in therecorded case – it needs to be ‘good’, not ‘perfect’
• Store the DVDs securely – keep them as aprogramme-specific resource, not for other use
Modelling good practice in thechosen area of clinicalcommunication is the firstimportant educational activity. Itneeds to be realistic
Scenario bank – written• Write scenarios based on actual cases• Include a brief description of the case, including some
demographic information about the parent ⁄ patient,and instructions for the clinician about what needs tobe communicated
• The bank of scenarios includes cases on different topicsand at different levels of difficulty
• Provide access to the bank via the hospital intranet(or other mechanism)
Unscripted scenarios providesufficient information to trigger anatural conversation between theactor and the learner
Easy access to a range of scenariosallows different professionalgroups to select topics of mostuse to themselves to practise withthe simulated parent ⁄ patient
We haveoutlined amodel … that isgrounded insoundeducationalpractice and iseasily adaptableto the needs ofdifferent groups
� Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 217–221 219
Appendix. (Continued)
ProgrammeFeature Implementation Rationale
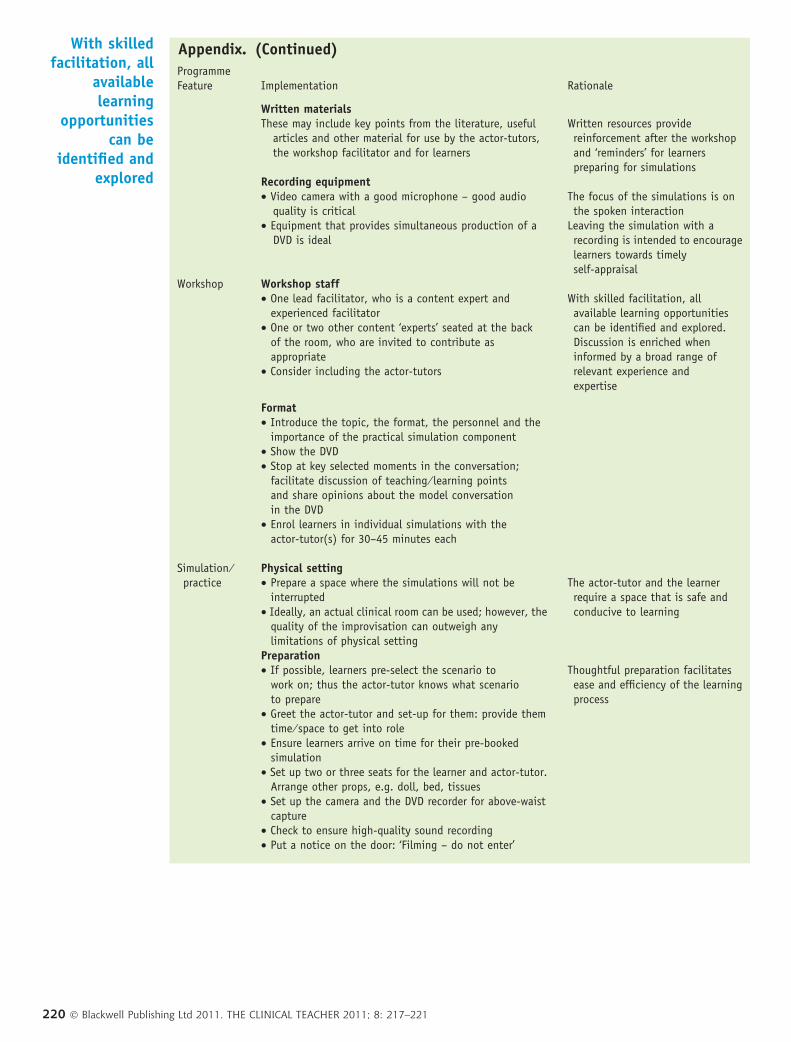
Written materialsThese may include key points from the literature, useful
articles and other material for use by the actor-tutors,the workshop facilitator and for learners
Written resources providereinforcement after the workshopand ‘reminders’ for learnerspreparing for simulations
Recording equipment• Video camera with a good microphone – good audio
quality is critical• Equipment that provides simultaneous production of a
DVD is ideal
The focus of the simulations is onthe spoken interaction
Leaving the simulation with arecording is intended to encouragelearners towards timelyself-appraisal
Workshop Workshop staff• One lead facilitator, who is a content expert and
experienced facilitator• One or two other content ‘experts’ seated at the back
of the room, who are invited to contribute asappropriate
• Consider including the actor-tutors
With skilled facilitation, allavailable learning opportunitiescan be identified and explored.Discussion is enriched wheninformed by a broad range ofrelevant experience andexpertise
Format• Introduce the topic, the format, the personnel and the
importance of the practical simulation component• Show the DVD• Stop at key selected moments in the conversation;
facilitate discussion of teaching ⁄ learning pointsand share opinions about the model conversationin the DVD
• Enrol learners in individual simulations with theactor-tutor(s) for 30–45 minutes each
Simulation ⁄practice
Physical setting• Prepare a space where the simulations will not be
interrupted• Ideally, an actual clinical room can be used; however, the
quality of the improvisation can outweigh anylimitations of physical setting
The actor-tutor and the learnerrequire a space that is safe andconducive to learning
Preparation• If possible, learners pre-select the scenario to
work on; thus the actor-tutor knows what scenarioto prepare
• Greet the actor-tutor and set-up for them: provide themtime ⁄ space to get into role
• Ensure learners arrive on time for their pre-bookedsimulation
• Set up two or three seats for the learner and actor-tutor.Arrange other props, e.g. doll, bed, tissues
• Set up the camera and the DVD recorder for above-waistcapture
• Check to ensure high-quality sound recording• Put a notice on the door: ‘Filming – do not enter’
Thoughtful preparation facilitatesease and efficiency of the learningprocess
With skilledfacilitation, all
availablelearning
opportunitiescan be
identified andexplored
220 � Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 217–221
Appendix. (Continued)
ProgrammeFeature Implementation Rationale
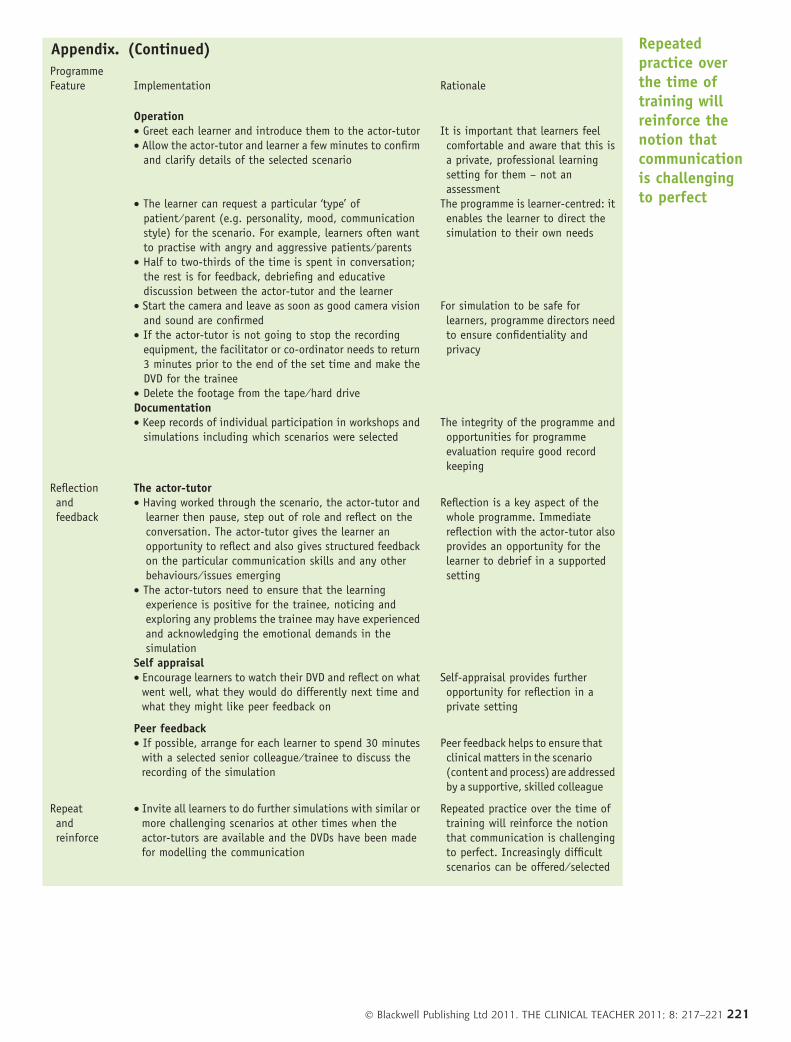
Operation• Greet each learner and introduce them to the actor-tutor• Allow the actor-tutor and learner a few minutes to confirm
and clarify details of the selected scenario
• The learner can request a particular ‘type’ ofpatient ⁄ parent (e.g. personality, mood, communicationstyle) for the scenario. For example, learners often wantto practise with angry and aggressive patients ⁄ parents
• Half to two-thirds of the time is spent in conversation;the rest is for feedback, debriefing and educativediscussion between the actor-tutor and the learner
• Start the camera and leave as soon as good camera visionand sound are confirmed
• If the actor-tutor is not going to stop the recordingequipment, the facilitator or co-ordinator needs to return3 minutes prior to the end of the set time and make theDVD for the trainee
• Delete the footage from the tape ⁄ hard drive
It is important that learners feelcomfortable and aware that this isa private, professional learningsetting for them – not anassessment
The programme is learner-centred: itenables the learner to direct thesimulation to their own needs
For simulation to be safe forlearners, programme directors needto ensure confidentiality andprivacy
Documentation• Keep records of individual participation in workshops and
simulations including which scenarios were selectedThe integrity of the programme andopportunities for programmeevaluation require good recordkeeping
Reflectionandfeedback
The actor-tutor• Having worked through the scenario, the actor-tutor and
learner then pause, step out of role and reflect on theconversation. The actor-tutor gives the learner anopportunity to reflect and also gives structured feedbackon the particular communication skills and any otherbehaviours ⁄ issues emerging
• The actor-tutors need to ensure that the learningexperience is positive for the trainee, noticing andexploring any problems the trainee may have experiencedand acknowledging the emotional demands in thesimulation
Reflection is a key aspect of thewhole programme. Immediatereflection with the actor-tutor alsoprovides an opportunity for thelearner to debrief in a supportedsetting
Self appraisal• Encourage learners to watch their DVD and reflect on what
went well, what they would do differently next time andwhat they might like peer feedback on
Self-appraisal provides furtheropportunity for reflection in aprivate setting
Peer feedback• If possible, arrange for each learner to spend 30 minutes
with a selected senior colleague ⁄ trainee to discuss therecording of the simulation
Peer feedback helps to ensure thatclinical matters in the scenario(content and process) are addressedby a supportive, skilled colleague
Repeatandreinforce
• Invite all learners to do further simulations with similar ormore challenging scenarios at other times when theactor-tutors are available and the DVDs have been madefor modelling the communication
Repeated practice over the time oftraining will reinforce the notionthat communication is challengingto perfect. Increasingly difficultscenarios can be offered ⁄ selected
Repeatedpractice overthe time oftraining willreinforce thenotion thatcommunicationis challengingto perfect
� Blackwell Publishing Ltd 2011. THE CLINICAL TEACHER 2011; 8: 217–221 221