hosted by: center for advocacy and leadership training a project of time for change foundation...
TRANSCRIPT

Hosted by: Center for Advocacy and Leadership Training
A project of Time for Change Foundation
Strengths-Based
Case Management
Presented by Dr. Richard Rapp June 12th & 13th , 2014
Richard C. Rapp, M.S.W., Ph.D.
Wright State University
Boonshoft School of Medicine

Objectives• Understand principles and practice
activities important in Strengths-Based Case Management
• Engage in practice scenarios & role plays• Discuss adaptation and implementation
issues for your setting

Terms
• Strengths-based Case Management (SBCM)– Treatment Linkage Case Management (TLCM)
• Persons with substance abuse problems
– ARTAS Linkage Case Management (ALCM)• Persons newly diagnosed with HIV
– Emergency Department SBCM (ED-SBCM)• Opiod addicts being treated in emergency departments
• “Linkage”; “Care Coordination”

Case Management & Substance Abuse
• Prior to 1990 case management used almost exclusively with mental health populations
• 1990 – four case management studies proposed as part of a National Institute on Drug Abuse initiative to improve treatment retention and outcomes
Case Management & Substance Abuse
• Models adapted from mental health field– Strengths-based: Wright State University;
University of Iowa– Assertive Community Treatment: University of
Delaware– Generalist: UCLA
• Since 1990, mostly generalist case management

Case Management

Barriers to Treatment
Persons who have
substance abuse
problems & are HIV positive
Personal
• Practical • Transportation• Financial• Childcare
•Lifestyle• Substance abuse &
mental health• High risk
behaviors• Homeless• Incarceration
•Internal• Fear of discovery• Stigma• Denial• Fatalism• Lack of trust
•Physical• Side effects
System
•Location•Rural providers•Affordability•Eligibility criteria•Inflexible hours•Admission process•Cultural competence•Impersonal•Intimidating•Staff skills•Waiting lists
Substance abuse
treatment & medical care
Case Management Functions
• Assesses – Identifies service(s) the client needs
• Arranges – Makes plans to get service(s)• Coordinates – Makes sure that service(s)
are received• Monitors – Follows the progress of client –
service(s) interactions
Case Management Functions
• Evaluates – Makes sure that client gets services as intended
• Advocates – Intervenes to assure that client gets the services they needed

Duration of Case Management
• On-going support of clients over a protracted period of time; long-term support of mental health clients reintegrated into community
AND/OR• Support in achieving specific, short-term
goals; assisting clients to link with services

Strengths Perspective

Barriers to Treatment
Persons who have
substance abuse
problems & are HIV positive
Substance abuse
treatment & medical care
Personal
• Practical • Transportation• Financial• Childcare
•Lifestyle• Substance abuse &
mental health• High risk
behaviors• Homeless• Incarceration
•Internal• Fear of discovery• Stigma• Denial• Fatalism• Embarrassment• Lack of trust
System
•Location•Rural providers•Affordability•Eligibility criteria•Inflexible hours•Admission process•Cultural competence•Impersonal•Intimidating•Staff skills•Waiting lists
CASE MANAGEMENT
STRENGTHS PERSPECTIVE
Principle I: Focus on Client Strengths
• Emphasize client strengths, positives, assets, skills, abilities, etc.
• De-emphasize client recounting of what they’ve done wrong
• Recognize motivation and personal efforts• Base goal-setting on past assets

Principle II: Client Driven
• Establish client as responsible for identifying own goals and path to accomplish those goals
• Increase client investment in goals• Promote self-determination• Reduces resistance and denial
Principle III: Case Manager as Primary Relationship
• Development of working alliance, relationship is critical
• Provides the short-term foundation for client taking risks
• Primary, but not exclusive relationship

Principle IV: Community as a Resource
• Selective use of formal, informal, and created resources
• Formal – specialized, entitlements• Informal – day to day functioning and
community involvement• Created – Expand personal interests, skills
Principle V: Assertive Outreach
• Encourages understanding of client’s life• Helps case manager to help client formulate
plans• Promotes relationship between client and
case manager
Combining Case Management & Strengths Perspective

ITARC Center for Interventions
Treatment & Addictions Research
Case Management + Strengths Focus
Case Management• Assessment• Planning• Linking• Coordinating• Advocacy
Strengths Perspective• Focus on strengths• Client driven• Primary relationship• Assertive outreach• Creative use of
resources
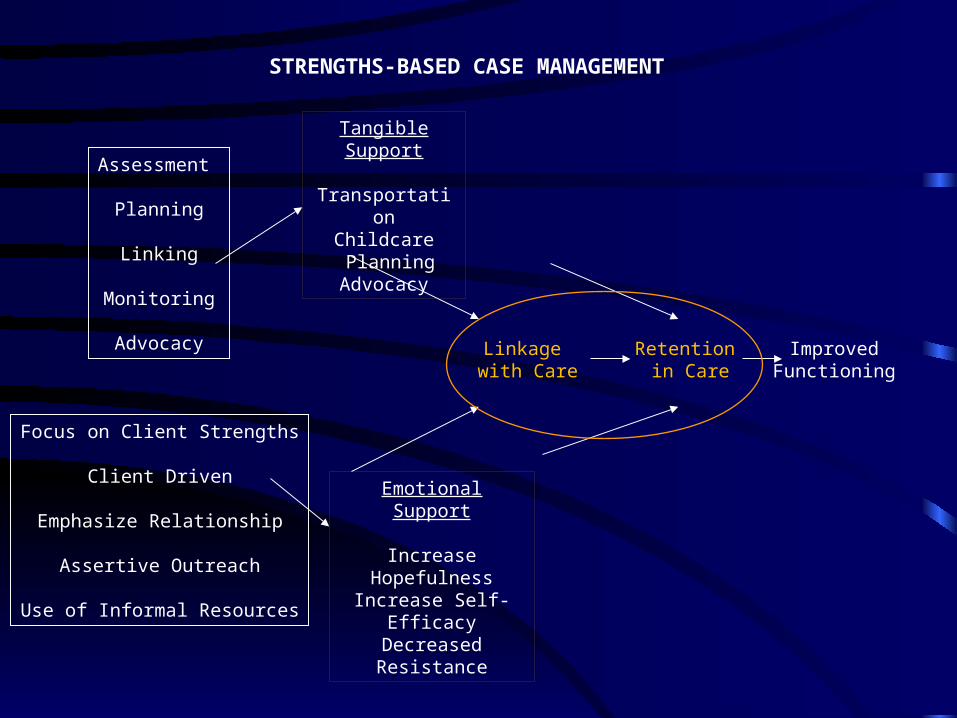
Focus on Client Strengths
Client Driven
Emphasize Relationship
Assertive Outreach
Use of Informal Resources
Assessment
Planning
Linking
Monitoring
Advocacy
STRENGTHS-BASED CASE MANAGEMENT
Linkage with Care
Retention in Care
Improved Functioning
Tangible Support
TransportationChildcare
PlanningAdvocacy
Emotional Support
Increase HopefulnessIncrease Self-EfficacyDecreased Resistance
Strengths-Based Case Management
• A value-added intervention in that:– Case management provides concrete support in
getting resources– Strengths perspective provides emotional
support in identifying abilities

Strengths Perspective and Medical Model
Strengths Perspective• Basic position is to find strengths, assets,
and abilities• Diagnosis and labeling is avoided• Full discussion of client’s story is
encouraged
Medical/Disease Model
• Basic position is to find sickness, problems, disease & pathology
• Diagnosis is required; labeling is frequent
• Client/patient usually seen as less capable, needs to be helped/fixed

Strengths Perspective and Medical Model
Strengths Perspective
• Individual is asked about needs• Individual seen as “able” and necessary
participant in addressing needs• Active involvement encouraged• Goals are (almost) always supported
Medical/Disease Model
• Worker supports “party line” and agency role
• Client/patient goes to services
• Solutions usually involve formal resources
• Doctor-patient relationship

Activity #1
• Scenario A & Scenario B

Outcomes
Linkage & Retention

Percent linkage by intervention and modality
Treatment Modality
Standard of Care
Motivational Interviewing
Strengths-Based Case
Management(n=222)
Total
Residential 39.0 43.9 56.2 46.3 a
Outpatient 28.7 c 43.4 52.3 c 41.2 b
Methadone 68.4 48.9 60.0 58.4 a,b
Total 38.7 d 44.7 e 55.0 d,e ++ 46.0
Percentages with same superscript are significantly different. a, e p < .05; c p < .01; b, d p <.001
++When substance abusers who attended no case management are removed the total linkage rate was 63.1%.
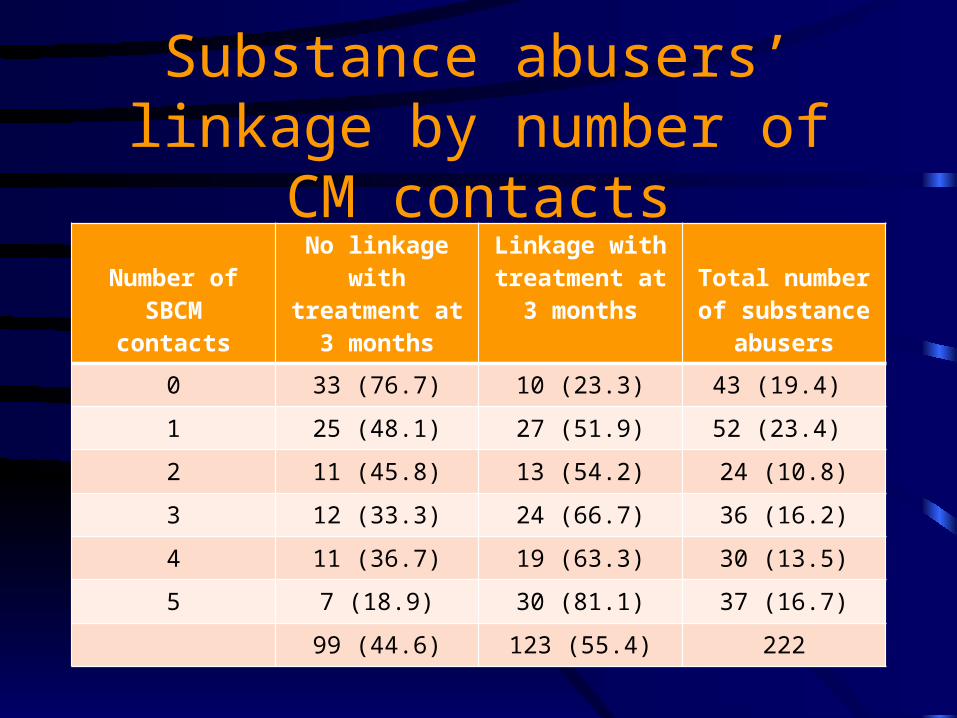
Substance abusers’ linkage by number of CM contacts
Number of SBCM contacts
No linkage with treatment at 3
months
Linkage with treatment at 3
monthsTotal number of
substance abusers
0 33 (76.7) 10 (23.3) 43 (19.4)
1 25 (48.1) 27 (51.9) 52 (23.4)
2 11 (45.8) 13 (54.2) 24 (10.8)
3 12 (33.3) 24 (66.7) 36 (16.2)
4 11 (36.7) 19 (63.3) 30 (13.5)
5 7 (18.9) 30 (81.1) 37 (16.7)
99 (44.6) 123 (55.4) 222

Path Model of Significant Factors on Post-Treatment Contact and Drug Severity
Unemployed
Fewer Arrests
Case Manager
Less Drug Use
Lower Drug Severity(Six Months)
More Weeks in Aftercare Treatment
.251
.122
.165
.129
.136
.399
.113 .120
(Baseline)
Less Depression
Less Use of Crack
Cocaine
Fewer Treatments

Path Model of Significant Factors on Post-Treatment Contact and Legal Severity
Unemployed
Lower Legal Severity
Case Manager
Readiness for Treatment
Lower Legal Severity
(Twelve Months)
More Weeks in Aftercare Treatment
.251
.242
.104
.425 .112.092 .089
(Baseline)

Practice of SBCM
A Word About Motivational Interviewing
• Some of basic skills of MI can be very useful as part of SBCM– Reflective comments vs. open and closed
questions – Recognizing stage of change – Rolling with resistance; empathy– Using discrepancy
Strengths-Based Case Management
• Preparation – Getting ready• Engagement – First impressions are
everything• Strengths Assessment – Changing the
discussion• Case Management Planning – Following
the client• Disengagement – Letting go

Preparation (System)
• Learn about & make a directory of both formal and informal resources
• Examine structure of own agency, what interferes with linkage
• Visit all resources where you might refer clients• Shadow program staff; Be the client• Establish informal relationships with staff• Encourage your agency to develop MOUs with other
programs

Preparation (Clients)
• Have a strengths “attitude”• Have knowledge necessary to assist clients• Understand situation of your potential clients• Interview clients who have been successful• Have basic support/counseling skills• Stay open to learning new ways of helping
people

Note on Preparation
• If you aren’t prepared, you put clients’ ability to be successful at risk
• Especially true when it comes to:– “Strengths attitude”– Fully knowing the resources where you refer
clients
Engagement
• Find out about client; Talk, don’t interview• Ask about their reaction to their situation• Don’t worry about apparent motivation• Recognize and state strengths as soon as
possible• Provide a summary of what you can and
can’t do for client• Be cautious about self-disclosure too early

Example ofStrengths-Related Assessment Tools
Strengths Assessment
• Benefits– Help client identify strengths, abilities, assets,
skills, dreams, interests– Provide improved sense of self-efficacy and
hopefulness– Use strengths, etc. in planning– Develop relationship– Reduce client resistance
Strengths Assessment
• Provides constructive challenge – Can’t do “autopilot” on reciting pathology– Encourages thoughts about, and practice of,
strengths (rather than practicing pathology)– Inoculates case manager against hopelessness
and skepticism
Strengths Assessment
• Initially may be difficult for both worker and client
• Usually unstructured; may have a list of strengths to prompt client’s thinking
• Always dynamic and interactive • On-going throughout the relationship
Strengths Assessment
• Summarize and write strengths down, give to clients
• Help client take credit for things going well• Continually connect client strengths and
current challenges they face
Strengths Assessment Questions
• What are your strengths/positives/good points/abilities?
• When have you faced challenges successfully?
• When were things going well and what were you doing to make them go well?
Strengths Assessment - Relationships
• Who do you trust? What is it about them?• What has been the most successful
relationship you’ve had, successful for both parties? What made it successful?
• When have you been able to just give to others without expecting anything in return?

Strengths Assessment -Internal Resources
• What was an example of your solving a problem effectively?
• When did you successfully identify and complete a goal? What helped you complete that goal?
• When did you feel most in control of your own life? What were you doing to make that happen?
Strengths Assessment - Recovery
• When was a time that you stayed sober? What were you doing that helped you stay sober?
• When was a time that you controlled your drug use? What were you doing that helped you stay in control?
• What have you done to try and deal with your drug use?
Non-Strengths Information
• Suicidal ideation or attempts• Risk to do harm to others• Physical problems associated with drug use,
HIV status, general health concerns• Intrinsic limitations such as learning
difficulties, not reading well

Activity #2
• Conducting strengths-based assessments

Example of a Goal-Setting Tool
Goal Setting/Treatment Planning
• Benefits– When client identifies own goals (objectives,
strategies) they are more likely to accomplish them
– Places responsibility for action on client– Enhances client investment in own care– Teaches a process that can be used in the future
Goal Setting/Treatment Planning• Provides a constructive challenge
– Can’t do “autopilot”, expecting someone else to do for them
• Minimizes chances of not being successful• Worker only helps shape the process and
asks the right questions• Builds in accountability for client (and
worker)

Goal Setting/Treatment Planning
• Initially may be difficult for both worker and client
• Plan based on demonstrated successes whenever possible
• Engages clients who function at various reading and cognitive levels
Goal Setting/Treatment Planning
• Process includes:– Identifying Goals, Objectives, Strategies– Target dates– Review of plan at every meeting
Goal Setting/Treatment Planning
• Goals: – “What do you need/want to accomplish?”– Broad statement in client’s own words– Not for case manager to decide– CM will work on any goal, unless its illegal or
hurtful to self or other
Goal Setting/Treatment Planning
• Objectives– Specific, measurable actions; no doubt if it has
been accomplished or not– Allows client to see success in tangible terms,
or if not successful make specific alternative plans
– Case manager may provide feedback, help client consider pros/cons, put objectives in best order, etc.

Goal Setting/Treatment Planning
• Strategies– Specific, measurable actions– The action or “baby steps” for accomplishing an
objective and thereby a goal– Allows client to see success in tangible terms, or if not
successful make specific alternative plans– Case manager may provide feedback, help client
consider pros/cons, put objectives in best order, etc.
Goal Setting/Treatment Planning
• Target Dates– Help client to identify realistic time frame for
accomplishing objectives and strategies– Use to discourage procrastination or overly
eager expectations
• Regular Review– Encourages follow-through– Provides prompt assistance if needed

Activity #3
• Developing a Personal Roadmap

One Example of SBCM
Structured 5 Contacts
#1: Building the Relationship• Describe the goals and objectives of SBCM• Review incident that led to ED treatment• Introduce the concept of strengths, abilities, and
skills and begin strengths assessment • Encourage linkage with substance abuse treatment
or identification of goals that are important to the individual
• Identify barriers to linkage or accomplishing goals of importance
• Summarize the session• Accomplish tasks on behalf of individual
#2: Assessing Personal Strengths• Discuss issues from last session; follow-up
on task since previous session• Continue strengths assessment• Encourage linkage with treatment or
identifying personal goals• Identify barriers to linkage and personal
goals• Summarize the session• Accomplish tasks on behalf of individual
#3: Learning to Make Contact• Discuss issues from last session; follow-up
on any plans• Continue to emphasize strengths• Encourage linkage with treatment and
personal goals• Identify barriers to linkage & personal goals• Begin disengagement process• Summarize the session• Accomplish tasks on behalf of individual

#4: Reviewing Progress• Discuss issues from last session; follow-up
on any plans• Engage in a summary of strengths &
accomplishments• Emphasize disengagement• Identify remaining barriers to linkage &
personal goals• Summarize the session• Accomplish tasks on behalf of individual

#5: Completing the Work
• Discuss issues from last session; follow-up on any plans
• Finalize disengagement process• Encourage client’s independent contact with
treatment and other resources• Summarize the relationship

Activity #4
• Staffing cases ala strengths-based case management

Implementing SBCM your organization
First 5 Questions to Answer
Question #1
• How completely do you want to implement SBCM?– Individual staff– Agency-wide– Agency-wide for certain population(s)– Community-wide
Question #2
• If agency-wide for certain populations, which population(s)?– Consider strategically – Define precisely

Question #3
• Do you want SBCM to be:– Brief, to help individuals with a specific
objective(s)? Or – Long-term with on-going support?
– Based on selected population– Based on agency and community services– Very different structures
Question #4
• Having answered questions #1 through #3, what objectives would you assign to each case management contact?

Question #5
• What current policies and procedures of your organization will interfere with implementing SBCM?– That’s not how we do it here– The intake process– Lack of clinical supervision focused on SBCM– Others
Steps in the Staffing Process
• Few facts – name, age, living situation, medical conditions
• Strengths, assets, skills, positives, etc.• Goals, Objectives, Strategies• Barriers to Objectives and Strategies• Inherent limitations