how family communication patterns and conflict …
TRANSCRIPT

HOW FAMILY COMMUNICATION PATTERNS AND CONFLICT MANAGEMENT
AFFECT CANCER PATIENTS’ SUPPORT SATISFACTION AND AVAILABILITY
by
TARA J. ABBOTT
(Under the Direction of Jennifer A. Samp)
ABSTRACT
This study examines the relationship between family communication patterns, conflict
management styles, and cancer patients’ perceptions of received social support. Fifty-three
cancer survivors recruited from online message boards completed an online survey which
assessed their level of family conformity and conversation orientations, their conflict
management styles, their perceptions of the amount and types of support they receive from their
primary support provider, and their perception of optimal matching of support. Results indicated
that although there were not significant relationships between level of conformity and perception
of received social support or optimal matching, there were significant relationships between a
patient’s level of family conversation orientation and his/her amount of communication with
family about the cancer and support needs, perception of received support and optimal matching.
There were also significant relationships between particular conflict management styles and
perceived optimal matching.
INDEX WORDS: Family communication patterns, Conflict styles, Social support, Optimal
Matching, Cancer

HOW FAMILY COMMUNICATION PATTERNS AND CONFLICT MANAGEMENT
AFFECT CANCER PATIENTS’ SUPPORT SATISFACTION AND AVAILABILITY
by
TARA J. ABBOTT
B.A., Boston College, 2006
A Thesis Submitted to the Graduate Faculty of the University of Georgia in Partial Fulfillment of
the Requirements for the Degree
MASTER OF ARTS
ATHENS, GEORGIA
2008

© 2008
TARA J. ABBOTT
All Rights Reserved

HOW FAMILY COMMUNICATION PATTERNS AND CONFLICT MANAGEMENT
AFFECT CANCER PATIENTS’ SUPPORT SATISFACTION AND AVAILABILITY
by
TARA J. ABBOTT
Major Professor: Jennifer A. Samp
Committee: Jerold Hale
Jennifer Monahan
Electronic Version Approved:
Maureen Grasso
Dean of the Graduate School
The University of Georgia
August 2008
iv
DEDICATION
This thesis is dedicated first and foremost to my parents. Their endless encouragement
and support are the foundation of all of my accomplishments. I am both so grateful for and so
inspired by their patience, love, and generosity.
I also dedicate this work to Betsy, Carolyn, and Katie for continuously standing by me
the last two years. I could not have asked for better friends and classmates to experience graduate
school with and to keep me laughing.
This work is also dedicated to Lauren and Danielle, my Georgia family, who have truly
made the South my home. I could not have made it through the last two years without their
humor and compassion. I feel so lucky and honored to call them my friends.
And finally, this thesis is dedicated to Dorothy, the inspiration for this project. She
exuded passion, love and positive energy each day of her life. She may have lost her fight with
cancer, but her amazing spirit and heart continue to live on in all the people whose life she
touched.
v
ACKNOWLEDGEMENTS
I would like extend my sincerest gratitude to Dr. Jennifer Samp for her endless
commitment to this project. Her input and encouragement from start to finish have been
irreplaceable. I am so lucky to have had the opportunity to have her as a teacher and as an
advisor these past two years. I am a stronger student and a more thoughtful individual as a result
of having learned from her.
I would also like to thank Dr. Jennifer Monahan and Dr. Jerold Hale for their insight and
support. I am extremely grateful for all the time and energy they devoted to this project.
vi
TABLE OF CONTENTS
PAGE
ACKNOWLEDGEMENTS.........................................................................................................v
LIST OF TABLES...................................................................................................................viii
CHAPTER
1 INTRODUCTION .....................................................................................................1
2 LITERATURE REVIEW AND PREDICTIONS .......................................................4
Social Support and Well-being ..............................................................................4
Conflict and its Hazardous Effects.......................................................................10
Family Communication Patterns and Conflict Management Styles ......................17
Hypotheses and Research Questions ....................................................................21
3 METHOD................................................................................................................30
Sample and Procedure .........................................................................................30
Measures .............................................................................................................32
4 ANALYSES AND RESULTS .................................................................................39
Preliminary Analyses...........................................................................................39
Tests of Hypotheses.............................................................................................48
6 DISCUSSION, LIMITATIONS AND CONCLUSION............................................60
Observations about Optimal Matching.................................................................60
Observations about Conversation Orientation ......................................................65
Observations about Conformity Orientation.........................................................69
vii
Limitations and Future Research..........................................................................75
Conclusion ..........................................................................................................78
REFERENCES .........................................................................................................................82
APPENDICES ..........................................................................................................................87
A SOLICITATION LETTER ......................................................................................87
B LETTER OF INFORMED CONSENT ....................................................................88
C QUESTIONNAIRE .................................................................................................90
viii
LIST OF TABLES
PAGE
Table 1: Correlations among Independent and Dependent Variables..........................................39
Table 2: Hierarchical Regression of the Family Conversation Orientation and the Family
Conformity Orientation on the Frequency of Family Discussion about the Cancer ......48
Table 3: Hierarchical Regression of the Family Conversation Orientation and the Family
Conformity Orientation on the Perceived Amount of Emotional Support ....................50
Table 4: Hierarchical Regression of the Family Conversation Orientation and the Family
Conformity Orientation on the Perceived Amount of Tangible Support ......................51
Table 5: Hierarchical Regression of the Family Conversation Orientation and the Family
Conformity Orientation on the Perceived Amount of Informational Support ...............52
Table 6: Hierarchical Regression of the Family Conversation Orientation and the Family
Conformity Orientation on the Amount of Patient Talk about Support Needs..............53
Table 7: Hierarchical Regression of the Family Conversation Orientation and the Family
Conformity Orientation on External Support Optimal Matching .................................54
Table 8: Hierarchical Regression of the Family Conversation Orientation and the Family
Conformity Orientation on Within-Family Optimal Matching.....................................55
Table 9: Hierarchical Regression of the Collaboration and Compromise, Avoidance,
Competition, and Accommodation Conflict Management Styles on External Support
Optimal Matching ......................................................................................................57

ix
Table 10: Hierarchical Regression of the Collaboration and Compromise, Avoidance,
Competition, and Accommodation Conflict Management Styles on Within-Family
Optimal Matching.......................................................................................................58
1
CHAPTER 1
INTRODUCTION
When an individual is diagnosed with cancer, the impact of the diagnosis extends far
beyond that individual who is diagnosed. The diagnosis not only marks a change in the physical
health and well-being of the individual, but consequently also marks the beginning of what is
sure to be a drastic change in the overall dynamic of the individual’s family unit. Only recently,
however, have researchers begun focusing their efforts on studying the effects of illness on the
family unit as a whole (Revenson, 1994). Martire, Lustig, Schulz, Miller, and Helgeson (2004)
explain that severity of a patient’s illness is related to strain in family relationships. The stress
experienced by a patient due to such things as physical discomfort, a more restricted lifestyle,
and fear of the future combined with the stress experienced by other family members resulting
from such things as fear of losing their loved one and increased responsibilities can breed a
negative environment that has the potential for much conflict. Glasdam, Jensen, Madsen, and
Rose (1996) explain, for example, that family stress resulting from a patient’s illness is often
accompanied by anger and greater difficulty coping with daily stress. Ell (1996, p. 174) suggests
that, “families are not merely static resource banks from which a seriously ill member withdraws
desirable social supports.” She emphasizes that families, particularly in these trying
circumstances, can be additional sources of stress and can unintentionally hamper both the
communication a support-receiving process (Ell, 1996). Unfortunately, it is during this extremely
stressful time when the potential for conflict, negative energy, and poor communication within
2
the family is so high, that it is also critical that the family unit pulls together and finds some way
to meet the staggering social support needs of the sick individual.
Because a supportive environment is so important to the physical and mental health of a
patient (Albrecht, Burleson, & Goldsmith, 1994), it is imperative that there is an examination of
how patients perceive the type and amount of social support provided by their primary support
providers within their family and what family communication characteristics post diagnosis
influence these perceptions. We must also examine how cancer patients perceive handling
conflict within their family following the diagnosis in order to determine how it could potentially
influence not only the overall family dynamic, but also the ability for the patients’ to feel
satisfied with the support efforts made by their family members.
This thesis proposes that family communication patterns can be used to understand and
predict the types and amount of support that cancer patients receive from their family members
after their diagnosis. It will also be argued that the conflict management used within the families
following the diagnoses will influence the patients’ perceived satisfaction with their support. In
order to carry out this study, 53 adult cancer survivors were asked to answer questions regarding
how their families communicate, the types of support they perceive themselves as receiving since
the diagnosis, their satisfaction with their support and also the way they believe they manage
conflict within their family. The hope is that this research can provide future insight into
protecting the well-being of the family unit during a particularly trying and uncertain time so that
the cancer patient can receive optimal support with minimal burden to the other already
overwhelmed family members. Allowing a cancer patient the best possible opportunity to live a
happy and satisfying life involves much more than just treating the physical symptoms of the
cancer. Hopefully medical staff and professionals will be able to apply the findings of this

3
research to their own professions to ensure that they can provide their patients not only with the
proper medical treatment, but also the proper communication tools and strategies to ensure that
their life and environment at home is positively contributing to the overall health and wellbeing
of the patient.
In the remainder of this paper I will review past literature related to the concepts
underlying this thesis project and explain my predictions that developed out of an analysis of this
past research (Chapter 2). I will then describe the methods (Chapter 3) and results of this study
(Chapter 4). I will conclude by offering an analysis of these findings and their potential
implications (Chapter 5).
4
CHAPTER 2
LITERATURE REVIEW AND PREDICTIONS
This chapter will provide a review of the existing literature on the concepts of social
support (particularly that relating to physical illness), optimal matching, conflict and family
communication patterns. There will also be an overview of the different literature exploring the
relationship and possible interaction between social support and conflict. This chapter will
conclude with a presentation and explanation of the hypotheses and research questions for this
study.
Social Support and Well-being
When an individual within a family unit is diagnosed with a potentially terminal illness,
social support becomes an essential component of the relationship between the family members.
The exchange of social support is a way of ensuring the physical and emotional wellbeing of the
sick family member. Albrecht, Burleson, and Goldsmith (1994) explain that receiving social
support is associated with reduced sorrow or distress, improved recovery from illness, increased
resistance to disease, and improved psychological adjustments. Blanchard, Albrecht,
Ruckdeschel, Grant, and Hemmick (1995) found that social support plays an important role in
reducing and/or buffering hopelessness, depression, and other negative psychological responses
to chronic and terminal illnesses. In an examination of the feelings of hopelessness felt by cancer
patients, it was found that patients who had less social support had more symptoms of
hopelessness. Also, those patients who reported less social support also indicated more
symptoms of depression, thereby suggesting that individuals receiving more social support have
5
a greater likelihood of better psychological adjustment than those with less available support (Gil
& Gilbar, 2001). Therefore, it could be determined from this study that social support is an
important external resource for coping with various stressors, particularly those stressors
resulting from serious illness (Gil & Gilbar, 2001). Ensuring that the support needs of the sick
family member are being met not only helps to improve the well-being of the sick individual but,
in doing so, also helps to prevent the stress and burnout of his/her family members that could
result from the frustration of not being able to adequately address the needs of their loved one.
With this in mind, it is important that we not only have a conceptual understanding of social
support but also an understanding of which types of support are optimal in particular
circumstances. To do this, the concept of social support must be explicated and its critical
components identified.
Since the 1970s, a great deal of research has been done relating to the concept of social
support (Cobb, 1976; Norbeck, Lindsey, & Carrieri, 1981). Even with all the attention paid to the
concept, however, a universal description of social support has yet to be developed. Norbeck,
Lindsey, and Carrieri (1981) explain, “at one extreme, simple contact or presence of another
during a stressful experience is described as social support, at the other extreme, elaborate
formulations about social network properties are suggested as essential properties to study” (p.
264). Cobb (1976) defined social support as information leading to one or more of three
categories: believing one is esteemed and valued, feeling cared for, and believing one belongs to
a reciprocal communication network. Since then, the term social support has been used as a
blanket term to describe many communication styles and networks that aid with coping in a
number of different contexts.
6
Sarason, Levine, Basham, and Sarason (1983) describe social support as “the existence or
availability on people whom we can rely, people who let us know that they care about, value, and
love us” (p. 127). Kahn (1979) developed a general, yet more descriptive and structured
definition that states that social support is an “interpersonal transaction that includes one or more
of the following: the expression of positive affect of one person towards another; the affirmation
or endorsement of another person’s behaviors, perceptions, or expressed views; the giving of
symbolic or material aid to another” (p. 85). Piko (1998) defines social support as an interactive
process in which certain behaviors can positively affect one’s social, physical, and/or
psychological well-being. While there are dozens of other conceptualizations of social support
that recognize its multi-dimensionality, with some emphasizing the structural component (the
actual social network) and others emphasizing the functional component (the perceived types and
amount of available resources), many researchers that examine social support and conflict
interdependently use definitions which align with those just described and, therefore, those are
the ones that will be used for the purposes of this paper.
Several studies have focused on what types of social support and which social support
networks best meet the needs of certain individuals in various contexts. Robinson and Turner
(2001) suggest that the source from which the social support comes can, in some instances, be
just as important as the social support itself. Intimate relationships such as those between family
members have been found to be suitable for providing multiple types of support simultaneously
to meet the changing needs of an individual (Eggert, 1987). Glasdam, Jensen, Madsen and Rose
(1996) specify that most married patients identify their spouses as their most important sources
of support.
7
Judging by past research it appears that, in most cases, the members of the family unit are
the critical support providers. This places a great deal of responsibility in the hands of these
individuals. Not only must the family members be willing and able to offer support, but in order
to be helpful and successful support providers, they must be able to recognize the types and
amount of support desired by those individuals in need. Of course, social support does not look
the same in every situation. Support comes in a variety of different forms and can be manifested
in a variety of ways. It is important to identify these common support types and to recognize that
certain coping situations require particular types of support.
While certain scholars will acknowledge different types of social support, usually
depending on the context of their research, there are three main types of socially supportive
interactions: emotional, tangible, and informational (Helgeson & Cohen, 1996). Emotional
support occurs when individuals interact with others to achieve feelings of comfort or a sense of
belonging in times of difficulty (Cutrona & Russel, 1990). This type of support, therefore,
involves providing love, empathy, and trust to a coping individual (Piko, 1998). Tangible support
involves the provision of goods and services, such as financial assistance or help with daily
chores/errands. Informational support is when information or guidance is provided to the coping
individual by the support provider in order to help solve a problem; for example, when an
individual provides a cancer patient with a list of top oncologists in his/her area.. In recognizing
that there are different types of support, we must also recognize that these support types serve
different purposes and meet different needs of a coping individual. It seems logical to believe
that individuals will perceive certain types of support as more important than others depending
on which needs they find most pressing and will, therefore, be more receptive to those support

8
types. To understand this idea more, we can turn to research by Cutrona and Russel (1990) on
the concept of optimal matching.
Optimal matching. It has been suggested that support that comes from the wrong person
or that is perceived as the wrong kind may, in fact, worsen one’s stress level (Taylor, Falke,
Shoptaw & Lichtman, 1986). Glasdam et al. (1996) identified that those patients satisfied with
the support from family members were significantly less depressed and anxious than those who
were not satisfied with their support. Cutrona and Russel (1990) developed the theoretical model
of optimal matching that suggests that social support is most effective when the type of support
needed is the type of support provided. Optimal matching theory (OMT) recognizes the
distinction between three different types of support: emotional, informational, and tangible.
OMT argues that the relative importance of these support types as social resources depends on
how controllable an individual’s stressors are. When it comes to uncontrollable stressors such as
death and illness, OMT suggests that emotional support will be most important. When it comes
to more controllable stressors, however, OMT argues that tangible and informational support will
be most important. Cutrona and Russel (1990) also explained, however, that an illness is an
uncontrollable event that can influence a variety of aspects of an individual’s life and, therefore,
support that addresses each of these aspects will be most effective. Ell (1996) suggests that
optimal support can only occur when there is clear, accurate communication of need by an
individual and sufficient ability on the part of the support providers to meet that expressed need.
Clearly, during time of serious illness within a family, many circumstances can hinder both the
patient’s communication and the family members’ support-giving abilities, thereby making
optimal matching an extremely challenging and potentially all too rare occurrence.

9
Hazards of not achieving optimal matching. Ensuring that a sick individual gets the type
and amount of support that he/she requires can be challenging for anyone, but it is particularly
challenging for that individual’s family members who are usually experiencing their own anxiety
and hurt over the sickness of their loved one. The sick individual’s family members are usually
trying to cope with their own feelings and challenges while also being a coping devise for their
loved one. A lack of optimal matching of social support, however, can not only be detrimental to
the well-being of the individual in need, but also to the well-being of the support providers and
the familial relationships.
Because it is so difficult for family members to recognize what level of support will be
sufficient for their sick loved ones, they often struggle with how much physical and emotional
assistance to offer. Revenson (1994) suggests that relational partners have difficulty balancing on
the line between being supportive of their sick spouses and being too controlling and smothering.
Ell (1996) argues that well-intentioned support that is misguided can often lead to a decrease in a
patient’s communication about distressful feelings which can, in turn, cause overprotectiveness
on the part of the caregivers and eventually have a negative effect on a patient’s perceived self-
efficacy and coping abilities. Some evidence also shows that the degree to which family
members are willing to engage in supportive behaviors may be influenced by the patient’s ability
to cope with the emotions pertaining to his/her illness. Revenson (1994) suggests that spouses of
seriously ill individuals who are seen as highly distressed and continuously poor at coping may
decrease their supportive efforts with the fear that any efforts will be ineffective.
The concerns that arise from being a primary support provider can have significant
effects on the provider’s lifestyle and well-being. Glasdam et al. (1996) report that spouses of
patients often report greater anxiety, a poor ability to cope with daily stresses, and physical
10
symptoms resulting from fatigue and stress in addition to having strong feelings of anger, guilt,
increased vulnerability. They also found that the spouses rarely talked about or addressed any of
these personal issues with family and/or friends and felt that they had little support provided to
them by others. Revenson (1994) explains that spouses are often reluctant to disclose emotions
or personal concerns to their partners for fear of placing further burden on their already sick
loved ones. As a result, however, it is possible that the emotional needs of both the patient and
the partner are not adequately met.
The stress that results from the obligation family members feel to provide adequate
support to their loved ones, added to the nervousness and fear that is present when there is a life-
threatening illness in the family, can cause an environment that has the potential for extreme
conflict. While conflict always has the potential to cause discomfort and hurt within a family, the
stakes are heightened in families that are dealing with illness. Conflict in families with a sick
family member has the potential not only to add further stress and anxiety to the home
environment, but also to hamper the flow of support within the family unit. To have a better
understanding of this potential, however, we must first conceptualize social conflict and its
recognized relationship to social support.
Conflict and its Hazardous Effects
Much like the conceptualization of social support, the conceptualization of social conflict
has varied significantly depending on the researcher examining it and the context in which it has
been examined. If social support represents the positive aspects of a support network, then social
conflict represents the negative aspects of a support network (MaloneBeach & Zarit, 1995).
Abbey, Abramis, and Caplan (1985) defined conflict using the concept of social support when
they explain, “If social support represents the potentially positive aspects of interpersonal
11
relations, such as expressions of positive affect and affirmation, then social conflict represents
the potentially negative aspects of these relations, such as expressions of negative affect and
disconfirmation” (p.114). Moos and Schaefer (1984) explain that social conflict has sometimes
been defined as the extent to which anger and aggression characterize a relationship.
MaloneBeach and Zarit (1985) further specified that interactions that lack overt aggression and
are, instead, made up more of frustration, hurt and irritation can also be identified as conflictual.
These various interpretations of social conflict suggest that conflictual situations must not always
arise from bad intentions or one individual’s lack of consideration for another; they can also arise
from misguided or poorly executed well-intentioned actions (MaloneBeach & Zarit, 1985).
Social conflict, like social support has been found to have significant ties to well-being.
MaloneBeach and Zarit (1985) explained that social conflict can lead to lower life satisfaction
and cognitive functioning problems. The relationship that social support and social conflict share
with an individual’s well-being is not the only connection these concepts have to one another. In
fact, social support and conflict are often co-existing concepts in the lives of loved ones,
particularly in times of heightened stress and uncertainty.
Relationship between conflict and social support. There are a few different ways in which
the concepts of social support and conflict can be linked to one another. Conflict and distress can
be the result of well-intentioned social support. Support providers can intend to be helpful by
providing various types of aid, but may do so in a way that is perceived as insensitive by the
recipient, thereby causing conflict between the two parties (Barrera, Chassin, & Rogosch, 1993).
This is in line with MaloneBeach and Zarit’s (1985) understanding of social conflict as distress
that results from both good and bad intentions. MaloneBeach and Zarit (1995) observed, for
example, that the pressure a caregiver feels when he/she perceives that the individual being cared
12
for is continuously requesting an alternative approach to the caregiving can lead to significant
conflict.
In addition to conflict being the result of a support providers’ well-intentioned aid, there
are also those situations in which conflict arises from the negative interactions an individual has
with the same people who provide him/her with support (Barrera, Chassin, & Rogosch, 1993).
Barrera (1981) described this as “conflicted support.” Manne and Schnoll (2001), when
examining cancer patients and their support providers, identified three types of unsupportive
responses from support providers that are considered common within this context: overtly critical
and insensitive responses, the avoidance of and withdrawal from the patient, and the
encouragement of the patient to distance him/herself from the cancer experience (i.e., refrain
from discussing it, trying to keep feelings to him/herself). These unsupportive responses may be
a result of burnout on the part of the support provider or perhaps an attempt at emotional
distancing. Carter and Carter (1994) studied marriages in which one partner suffered from cancer
and observed patient-spouse interactions that indicated an oscillation that entailed the partners
interacting up to a critical point of intimacy and then quickly disengaging with force through
interpersonal conflict, only to repeat the cycle.
Research has also been done examining the possible interaction effects between the
presence of social support and conflict on and individual’s wellbeing. Barrera et al. (1993)
examined the potential for “synergistic effects” of interactions between social support and
conflict by looking at effects of social support and conflict on adolescents of alcoholic and
nonalcoholic parents. They argued that synergistic effects occur when high conflict neutralizes
the effectiveness of social support or when low conflict provides situations suitable for
individuals to better reap the benefits of social support. Barrera et al. (1993) found no evidence

13
that conflict in a relationship neutralizes the effectiveness of the social support provided in that
relationship, suggesting that adolescent children have separate appraisals of parental support and
conflict. Their findings reinforce the possibility that increasing the supportiveness of family and
friend relationships is entirely unrelated to decreasing conflict within these relationships and vice
versa.
Research in a number of different contexts has been done to examine the simultaneous
effects of social support and social conflict on individual well-being. Major, Zubek, Cooper,
Cozzarelli, and Richards (1997), for example, looked at the implications of social conflict and
social support within close relationships for post-abortion adjustment. The main goals of the
study were to compare the impacts of perceived support and perceived conflict on adjustment to
stressful life events and to explore the potential for interactive effects of support and conflict on
adjustment. Major et al. (1997) used two pre-established hypotheses to interpret the results: the
social negativity hypothesis and the affect-matching hypothesis. The social negativity hypothesis
assumes that conflict in social relationships is a greater predictor of mental health than is social
support in those relationships, given that a substantial amount of evidence supports the idea that
negative events are weighed more heavily in one’s judgment and, therefore, result in stronger
effects on mental health and well-being than do positive events. The affect-matching hypothesis
assumes that perceptions of social support are stronger predictors of positive indexes of mental
health, whereas perceptions of social conflict are stronger predictors of negative indexes of
mental health. Though neither hypothesis obtained complete support, there was stronger support
for the affect matching hypothesis than the social negativity hypothesis. Pre-abortion conflict
was found to uniquely predict post-abortion distress, whereas pre-abortion support was a unique
predictor of post-abortion wellbeing (Major et al., 1997). Although there was no evidence of an
14
interaction between partner conflict and partner support in terms of mental health, social conflict
from either the mother or the friend interacted with social support from that same individual to
predict psychological distress. For example, women who perceived their mothers as non-
supportive were just as likely to be as distressed if their mothers were a source of high conflict as
if their mothers were a source of no conflict, whereas women who perceived their mothers to be
very supportive were significantly more distressed if they also perceived them as being sources
of high conflict than if they perceived them as sources of no conflict (Major et al., 1997).
Although post-abortion coping is very different than coping with cancer, considering that the act
of abortion is an individual’s choice and not a threat to his/her life, this finding still helps to
illustrate the importance of considering family conflict when examining the satisfaction with
family support and the effect of that support on the cancer patients well-being. It suggests that
during times of heightened sensitivity and stress, the presence of conflict between a patient and
his/her primary support provider could effect the satisfaction with and usefulness of his/her
available support.
Abbey, Abramis, and Caplan (1985) researched the effects of different sources of social
support and social conflict on an individual’s emotional wellbeing. They sought to determine
whether or not the significance of an interaction between social support and social conflict was
related to the type of source an individual was referring to. Each respondent was asked to explain
how much social support and how much conflict he/she experienced with respect to either the
person closest to them, some one person, or people in their personal life (Abbey et al., 1985).
They hypothesized that social conflict and social support would only be negatively and
moderately correlated in those situations where the source was people in their personal life or
some one person, given that individuals can receive both social support and social conflict at the
15
same time from different sources or from the same source (i.e. if someone gives useful
information in an argumentative way). They also hypothesized, however, that the negative
relationship between social support and conflict would be stronger when the source was the
person closest to them. They suggested that this would be because they are less likely to feel
closest to individuals who provide significant conflict along with support. Their hypotheses
regarding the correlation between social support and social conflict were supported (Abbey et al.,
1985). Results of their research also suggested a buffering effect, but only in some conditions.
For respondents who reported receiving low support from some one person, there was a strong,
positive relationship between social conflict and feelings of anxiety, depression, and
interpersonal sensitivity, while there was a strong, negative relationship between social conflict
and quality of life. As for respondents who reported high levels of social support, however, the
relationship between conflict and well-being was not exhibited (Abbey et al., 1985).
All of these findings highlight the importance of continued research on the relationship
between conflict and social support, particularly in situations of high-anxiety. There is strong
evidence suggesting that both social support and conflict are critical factors influencing the well-
being of coping individuals and that supportive relationships have the potential to be breeding
grounds for conflict in situations of high stress and uncertainty. The fact, however, that some
research has found a relationship between conflict and social support, while other results would
imply that there is no direct relationship suggests that further exploration and explanation is
needed. Rather than solely considering the amount of conflict in families in which significant
social support is required, what is needed is an examination of the way in which conflict is
managed when it does arise. A family situation where one individual has been diagnosed with a
life-threatening illness is a particularly important context in which to explore conflict
16
management and social support. This is because the potential for conflict is heightened more so
than in other situations, partly because of fear of the suffering and potential death of the cancer
patient and partly because of the constant support that the diagnosed individual may expect of
family members. Because the individuals in this situation have very little control over the factors
that could easily spark conflict, it is an extremely important context in which to focus on the
effects of conflict management strategies rather than just the amount of conflict. The conflict
management styles the various families in this situation use could have an important connection
to the social support that the sick individuals perceive as being available to them. When conflict
is not managed in a constructive way it could influence the ability for the family members to
provide adequate amounts or types of support. It could also influence the ability the individual in
need has to perceive or be open to the support being offered. Conflict management could also be
a useful predictor of which supportive relationships have the greatest potential to breed conflict.
In a situation where a life-threatening illness is involved and, therefore, where social support is
of the utmost importance, it is important to consider how a variety of the factors influencing the
family dynamic could work together to influence the satisfaction the patient feels with his/her
support.
Given the fact that not all families operate or communicate in the same way, we can not
expect all families to handle a life-threatening diagnosis in a similar manner. The ways in which
families deal with providing support and manage conflict are partially a reflection of their overall
family dynamic and interaction patterns. Therefore, one must have an understanding of the
different communication patterns that characterize families in order to gain insight into their
supportive capabilities.
17
Family Communication Patterns and Conflict Management Styles
Koerner and Fitzpatrick (2002, p. 71) define the term family as, “a group of intimates
who generate a sense of home and group identity and who experience a shared history and a
shared future.” Fitzpatrick and Ritchie (1994) conceptualized two sets of beliefs, known as
conversation orientation and conformity orientation, as beliefs that will determine how family
members will go about communicating and interacting with each other.
Conversation orientation is the degree to which families create an environment in which
all of the members feel unrestrained when it comes to communicating about a wide range of
topics. Members of families that fall on the high end of the conversation orientation encourage
one another to participate in communication frequently and openly. Individuals in these types of
families spend lots of time with one another and discuss a number of different topics regarding
their thoughts, emotions, and individual activities without feeling as though there are restrictions
as to what they are permitted to discuss or how much time they should spend interacting with
one another (Koerner & Fitzpatrick, 2002). Families high in conversation orientation use open
and frequent communication in family decision making and stress that this open communication
is the key to a successful and rewarding family life. Those families on the low end of the
conversation orientation dimension usually don’t spend as much time interacting with one
another and only have a few topics that all the members feel comfortable discussing openly with
one another. The exchange of personal thoughts and feelings does not occur frequently in these
low conversation orientation families because they do not see openness as essential for the
functioning of a family unit.
In addition to conversation orientation, dimension influencing communication within the
family is conformity orientation (Koerner & Fitzpatrick, 2002). The conformity orientation
18
dimension deals with the degree to which family communication stresses every member sharing
similar values, attitudes, and beliefs. Families that are on the high end of this dimension focus on
emphasizing the uniformity and harmony of the family unit through their interactions. As a
result, families high in conformity orientation value the interdependence of family members and
try to avoid conflict as much as possible. High conformity orientation families value the family
relationship over any and all other relationships outside of the family unit and, therefore, try to
maximize the time they spend together. Families high in conformity orientation are also those
families that value a hierarchy and, therefore, often do not involve children (if there are any) in
the decision making process. When it comes to specific speech acts, individuals in families high
in conformity orientation frequently engage in advice giving and evaluating of others’ behaviors
based on their own attitudes and perspectives (Koerner & Cvancara, 2002). Families that are on
the low end of the conformity orientation dimension, on the other hand, emphasize the
individuality of family members and each member’s independence from the family. As a result,
low conformity orientation families do not follow the traditional, hierarchical family structure
but rather believe that it is important to foster individual growth and personal relationships
outside of the family even if it is at the expense of the cohesiveness of the family unit (Koerner
& Fitzpatrick, 2002). When it comes to specific speech acts, individuals in low conformity
families deliver more confirming statements and value-free reflections of others’
communication. Communication within these low conformity families is freer and more
spontaneous (Koerner & Cvancara, 2002).
Family communication patterns also influence how people manage conflict within their
families. I argue that a focus on how families manage conflict, rather than just focusing on the
amount of conflict within the family, may provide insight into the conflicting research regarding
19
the relationship between social support and conflict. As previously mentioned, some research has
found a relationship between conflict and social support, while other results would imply that
there is no direct relationship. A reason for this discrepancy between findings could be that these
past studies explored the amount of conflict within families when, perhaps, the relationship
between conflict and the presence of and satisfaction with social support is actually a result of
how conflict is managed rather than whether or not it is significantly present. In the context of
cancer, where numerous uncontrollable stressors make conflictual situations nearly unavoidable,
conflict management is important to explore in order to determine whether or not satisfactory
support can still be offered and under what circumstances.
Conflict can either be managed constructively or destructively. Noller, Feeney, Sheehan,
and Peterson (2000) explain that constructive conflict management involves openly sharing
differences and supporting one another in joint problem solving so that there can be some sort of
mutually acceptable solution. There have been found to be five important conflict behaviors that
vary along two dimensions- concern for self and concern for the relationship (Rahim, 1983).
Which conflict behaviors individuals typically choose to use within the family unit will
determine whether or not conflict is resolved constructively or destructively (Noller et al., 2000).
Competition involves a high concern for self and a low concern for the relationship. Individuals
that engage in this conflict behavior are concerned with being the “winner” of the conflict rather
than with ensuring that the needs and concerns of all parties involved are being addressed.
Competitive individuals may use their power or expertise to persuade others that they are right
and deserve to have their needs met. Collaboration involves a high concern for both the self and
the relationship. Both parties work together to come up with a solution in which everyone
involved gets what they want and are completely satisfied with the outcome. This style involves

20
high levels of disclosure on the part of the individuals and much discussion regarding the issues.
The accommodating conflict behavior involves a low concern for self but a high concern for the
relationship. Individuals with this conflict behavior give in to others’ wishes and opinions at the
onsite of conflict so as to not have to deal with the issues and so as not to disturb their
relationships. The compromise behavior involves a moderate concern for both the self and the
relationship and entails each person getting part of what they want. As a result, the compromise
style requires moderate to low levels of self disclosure. And lastly, avoidance involves a low
concern for self and the relationship. The avoidant style often involves little self-disclosure and
retreating physically and or emotionally in order to get away from conflict.
Koerner and Fitzpatrick (1997) explored the relationship between family communication
patterns and conflict behaviors. They observed that families high in the conformity orientation
were more likely to practice conflict avoidance while those high in conversation orientation were
less likely to practice avoidance. Koerner and Fitzpatrick (1997) also observed that when conflict
avoidance did occur, it had negative effects on the relationship. This avoidance led to negative
feelings about the family and caused tension among the family members. Botta and Dumlao
(2002) supported these findings when they argued that living in a high conformity family could
cause children to have unresolved conflict with their parents (as a result of being forced to
conform and refrain from communication) and that could then result in unhealthy mindsets and
dangerous behaviors.
From past research we can begin to see that both communication patterns and conflict
management styles are important predictors of how members of different family types are going
to interact with one another on a daily basis. While these concepts have been applied to some
challenging family situations such as a child’s adjustment to college or eating disorders within

21
the family, there is little research on the effects of these communication patterns and conflict
styles on family behaviors in times of serious stress and uncertainty, such as during the presence
of a life-threatening illness. This research will, therefore, explore the relationship between
communication patterns, conflict styles and the amount and type of support that cancer patients
receive following their diagnoses, when social support is necessary and unavoidable. The context
of cancer within the family is a particularly important context in which to study these concepts
because it is in these times of such enormous stress and anxiety that communication and support
are critical, but also that conflict has the greatest potential of occurring. With this in mind, a
number of hypotheses and research questions are proposed.
Hypotheses and Research Questions
Families that are high in conversation orientation spend significant amounts of time
communicating with one another and, therefore, should take comfort in using open and frequent
communication as a coping strategy in the uncertain time following a cancer diagnosis. Once an
individual is diagnosed with cancer, managing the disease becomes an important part of not only
the patient’s life, but his/her family’s life as well. To avoid discussion of the cancer would be to
stop communicating about a significant portion of the family members’ lives. Given that high
conversation orientation families believe communication to be an important contributor to the
success of the family unit, this significant decrease in conversation would not be something that
these families high in conversation would be comfortable with, especially during a time when
they need to feel especially close to one another. Families low in conversation, on the other hand,
are not used to significant amounts of self-disclosure and, therefore, engaging in frequent
communication about feelings and concerns relating to the cancer might be uncomfortable and/or
anxiety producing. It is difficult, however, to predict the relationship between a family’s level of
22
conformity and its frequency of discussion about the cancer. While the heads of a high
conformity household will probably refrain from involving the entire family in the process of
making medical decisions, they wont necessarily refrain from encouraging family members to
discuss facts related to the cancer, feelings associated with the cancer, and other related
information that is not a threat to the hierarchy, particularly since they value interdependence and
are used to focusing on relationships within the family. Therefore, the level of conformity within
a family may not have a significant impact on the amount of disclosure about the illness. With
this rationale, the following prediction and research question are posed:
H1: There will be a positive association between a cancer patient’s level of family
conversation orientation and the patient’s perceived frequency of family discussion about the
cancer.
RQ1: What is the relationship between family conformity orientation and the frequency
of family discussion about the cancer?
In addition to the belief that there is a relationship between a family’s communication
patterns and the amount of communication its members engage in about the cancer, it is also
believed that there is a relationship between family communication patterns and the type and
amount of support that a cancer patient perceives as being available within the family.
Individuals in high conversation orientation families expect high levels of self-disclosure with
one another given that they depend on and encourage frequent communication as well as the
expression of feelings. Individuals in these high conversation orientation families, therefore,
should be best equipped to offer emotional support to the family member in need. The significant
amount of time spent together supportively sharing their thoughts and feelings should make it
easier and more natural for individuals in high conversation families than for individuals in low

23
conversation families to be empathetic towards one another as well as a source of trust and
comfort. As a result, cancer patients in families that are higher in conversation orientation should
perceive more emotional support from their primary support providers than cancer patients in
families that are lower in conversation orientation. It is more difficult to predict the relationship
between family conformity orientation and the amount of emotional support that is perceived by
the cancer patient as being provided. The high conformity orientation family stresses family
interdependence and loyalty and, therefore, individuals in these families, more so than
individuals in low conformity families, should be used to being the primary support providers for
their family members. It may be, however, that the vulnerability that often comes along with
giving and/or receiving emotional support could be perceived by the family as threatening the
power balance within the established family hierarchy. Also, the higher the conformity
orientation, the greater difficulty family members may have being empathetic if they feel a
cancer-related decision made by the patient does not go along with family values or beliefs and,
therefore, the less emotional support that patient will perceive. It is also important, then, to
question if level of family conformity orientation influences family members’ tendencies to
provide other, less vulnerable types of support. Perhaps individuals in high conformity
orientation families use tangible and information support as a way to make sure they are
protecting and being loyal to their family unit even when they do not feel comfortable providing
emotional support. With this rationale, the following hypothesis and research question are
presented:
H2: There will be a positive association between a cancer patient’s family conversation
orientation and his/her perception of the amount of emotional support provided by their primary
support provider.
24
RQ2: What is the relationship between a cancer patient’s family conformity orientation
and the amount of emotional, informational and tangible support he/she perceives him/herself as
receiving from the primary support provider?
Individuals in families that frequently discuss their wants, desires and concerns are more
likely to feel comfortable talking openly with their family about what kind of assistance they
need in coping with cancer. Individuals in families that emphasize open communication are less
likely to feel guilt or hesitation when it comes to being open about the specific ways in which
they want to be supported because they are used to turning to their family members to talk about
their needs and feelings. Individuals in high conversation orientation families should not
consider their disclosure an additional burden for their family members because they recognize
that this method of open and honest communication is what their families rely on and are
comfortable with. In fact, these patients in high conversation orientation families would probably
recognize that not openly communicating their support needs would cause more stress and
concern amongst their family members. Patients in families that are low in conversation, on the
other hand, would probably see their communication of support needs as a heavy burden to their
family members because they are not as used to going to these members to talk about their wants
and needs. Also, because families low in conversation orientation do not engage in as much self-
disclosure, patients within these families might feel embarrassed about or uncomfortable with
being so direct in their expression of need. It is harder to predict the relationship between a
patient’s family conformity orientation and his/her disclosure about support needs. Because
families high in conformity emphasize putting family relationships and the good of the family
unit over all else, one might suspect that the members of these families would encourage their
sick loved ones to express their support needs so that they may be taken care of in the best way
25
possible, consequently preserving the well-being of the family units. However, families high in
conformity orientation also have well-established family roles as well as a strong desire to
maintain harmony. Cancer patients in families that are high in conformity may refrain from
expressing their support needs because they feel as though it will threaten the power structure
established within the family unit or because they feel their support wishes/needs do not align
with the attitudes and values of the family. Given these assumptions, the following hypothesis
and research question are proposed:
H3: There will be a positive association between a cancer patient’s family conversation
orientation and the amount of time that patient spends talking about his/her social support needs
with the other family members.
RQ3: What is the relationship between a cancer patient’s family conformity orientation
and the amount of time that patient spends talking about his/her social support needs with the
other family members?
Because families that are high in conversation orientation engage in so much dialogue
and disclosure, cancer patients in these families can work through figuring out their specific
support needs and concerns through communication with their family members. Also, the more
communication going on, the more up to date the family is on the patient’s challenges, concerns,
etc., and the greater the understanding between the family members about what needs to be done
in order to best cope with the situation. Also, because families that are high in conversation
orientation are used to being honest with and trusting of one another, cancer patients in these
families should feel comfortable expressing when they are not satisfied with the type and/or
amount of support they are receiving and what kind of change they would like to see. With all of
this in mind, it seems that the cancer patients in families that are high in conversation orientation
26
are going to be the most satisfied with the support they are receiving from their family members.
Family members in low conversation orientation families are probably not engaging in as much
communication with their sick loved ones and, therefore, should have a lesser understanding of
what they are going through and what they are in need of. It is more difficult to predict the
relationship between conformity orientation and optimal matching. If the reasons previously
mentioned prevent individuals in these families from expressing their support needs, it may be
that they will not receive the type or amount of support that they are looking for. Also,
individuals in high conformity orientation families are not used to expressing disapproval of or
disagreement with family behaviors and, therefore, may also refrain from expressing
dissatisfaction with support family members have provided because it goes against the family
norms of maintaining harmony. If they do not express this disapproval, it could prevent optimal
matching. Also, during a time of such heightened stress, when the future of the family unit is
threatened, the high conformity family’s emphasis on the importance of family togetherness and
dependence will only be strengthened. Therefore, individuals in these high conformity
orientation families who are dissatisfied with their support will be heavily discouraged to look
outside the family to have their support needs met. With this rationale the following hypothesis
and research question are proposed:
H4: There will be a positive association between a cancer patient’s family conversation
orientation and the degree to which he/she reports optimal matching.
RQ4: What is the relationship between a cancer patient’s family conformity orientation
and the degree to which he/she reports optimal matching?
Based on past research, it is believed that the way conflict is managed within the
household can be a strong predictor of whether or not a cancer patient will feel satisfied with the
27
type of support he/she is receiving within the family. The reason conflict management style is
expected to be an important predictor of optimal matching within this particular context is that
the significant number of uncontrollable stressors resulting from a cancer diagnosis leaves the
family environment prone to conflict-inducing situations. Those cancer patients that practice an
avoidant management style with their family members are going to frequently distance
themselves from those family members. The reason for this is that avoidant individuals are so
concerned with not having to address or deal with conflict that they avoid most situations or
interactions that they fear could potentially result in conflict. This also means that avoidant
individuals will be more cautious when it comes to choosing what to approach their family
members about. As a result, those avoidant individuals with cancer will be less likely to voice
their support needs or to bring up the issue of their support needs not being adequately met for
fear of upsetting or insulting their family members. Individuals with an accommodating
management style should behave similarly to those who practice conflict avoidance when it
comes to dealing with their social support concerns. Almost equally uncomfortable with conflict,
accommodating individuals are so used to appeasing others that they will accept the support
behaviors of their loved ones with little input or suggestions for improvement when they are
unsatisfied. Also, when a specific conflict situation does arise, these individuals with either an
avoidant or accommodating conflict style will usually keep their feelings and wants inside so as
to not perpetuate the conflict. As a result, the individuals with avoidant or accommodating
conflict styles may build up feelings of hurt, frustration and anger that prevent them from being
open to support from their loved ones or from having a realistic perception of the amount or
quality of support they are receiving. Individuals with collaborative or compromising conflict
management styles, on the other hand, should not have these issues. Individuals with
28
collaborative and compromising conflict styles should be use to talking through concerns with
their family members and should not be overly anxious about discussing sensitive issues. As a
result, collaborating and compromising individuals should be more comfortable talking about
their support needs and sharing concerns they have about the support they are receiving with
their loved ones, thereby allowing them a greater opportunity for optimal matching. Also, if a
conflict does arise in the family, it is usually addressed in such a quick and communicative
manner that there are fewer hostile or hurt feelings that could get in the way of the offering
and/or receiving of support. With this information in mind, the following prediction can be
made:
H5: There will be a relationship between cancer patients’ conflict management styles and
optimal matching such that:
(a) Avoidant or accommodative styles will be negatively associated with
perceived optimal matching.
(b) Collaborative or compromising styles will be positively associated with
perceived optimal matching.
Given what we know about the competitive conflict style, it is more challenging to
predict how satisfied cancer patients with this conflict style will be with the social support they
receive from their family members. Individuals with a competitive conflict style have a win-lose
attitude about conflict, meaning that they continue to battle out issues until one individual has
conquered the other and, therefore, gotten his/her way. Therefore, on the one hand we can expect
competitive individuals to be comfortable bringing up issues relating to their social support,
because they are not intimidated by the potential for conflict. On the other hand, however, if
significant conflict does arise (either about social support concerns or another issue), competitive
29
individuals’ intense, often hurtful attempts to get their way and win the battle could cause
negative feelings that would deter their loved ones from providing adequate support. With this in
mind, the following research question is posed:
RQ5: What is the association between competitive conflict management style and
optimal matching?

30
CHAPTER 3
METHOD
Sample and Procedure
Individuals who had been diagnosed with some form of cancer were recruited from
several internet-based cancer discussion forums and message boards. A general explanation of
the research goals were made available for forum and message board visitors with a link to a
questionnaire for those individuals who decided that they would like to participate. The
explanation provided described that I was interested in looking at how those fighting cancer
generally communicate with their family and discuss their support needs for the future goal of
improving the quality of support offered to cancer patients by their loved ones. The solicitation
letter is provided in Appendix A. The online forums that the were used for participant
recruitment were Breast Cancer Support (http://bcsupport.org/), American Cancer Society’s
Cancer Survivor Network (http://www.acscsn.org/), the Lung Cancer Support Community
(http://lchelp.org/), Cancer Compass (http://www.cancercompass.com), Susan G. Komen For the
Cure Message Boards (http://apps.komen.org/Forums/), and the MSN Cancer Message Board
(http://health.msn.com/message-boards.aspx). Before posting the explanation and questionnaire
link on these websites, I contacted the administrators of each forum and message board and gave
them a brief explanation of my intent. Six of ten message board administrators granted
permission to solicit participants for this study. Only those on-line communities that agreed to
post the survey solicitation were used to solicit participants. The solicitation of participants
occurred during the period of February through June 2008.
31
Each individual who decided to participate completed an anonymous questionnaire
hosted by www.surveymonkey.com, after reading a letter of informed consent, and responses
were encrypted and sent over a secure 256-bit secure SSL- socket server. The letter of informed
consent may be found in Appendix B and a copy of the full questionnaire may be found in
Appendix C. Participants did not receive any tangible credit for their participation.
Seventy-eight individuals completed a portion of the survey. Twenty-five of those
people, however, did not complete significant portions of the survey related to the tests of
hypotheses and were, therefore, not used for analysis. Thus, the final sample was comprised of
53 individuals who have, at one time, been diagnosed with cancer and who have at least one
other person in their immediate family. Respondents ranged in age from 32 to 72 with a mean
age of 48.90 (SD = 9.75). Forty-nine respondents (92.5%) were female and 3 (5.7%) were male.
The sample was 94.3% white (n = 50) and 1.9% Asian (n = 1). The majority of the sample
identified themselves as both a wife and a mother in their immediate family (n = 30). Of the
remaining sample, 2 respondents identified themselves as both a husband and a father, 2
identified themselves daughters, and 4 identified themselves as sisters. Participant cancer status
ranged from newly diagnosed (less than 1 month ago) to diagnosed 10 years ago (M = 14.76
months). When asked to indicate on a Likert scale how differently they now manage family
conflict when it arises as compared to before the diagnosis (1 = very differently; 5 = exactly the
same) most participants reported that they managed it fairly similarly (M = 3.58). However, in
response to a three-option question regarding the amount of conflict experienced in the family
since the diagnosis, over half (n = 30, 56.6%) of the participants reported that they engaged in
less conflict. Twenty respondents (37.7%) indicated that they engaged in the same amount of
conflict and 3 respondents (5.7%) indicated they engaged in more conflict.

32
Participants were asked to think about their primary support provider while answering a
series of items. The average age of the respondents’ primary support providers was 47.75 years
old (SD = 12.93, range: 16-70). Of these primary support providers, 38 were male (71.1%) and
14 were female (26.4%). Forty-one (77.4%) of the primary care givers were the spouses of the
cancer patients, whereas 8 (15.1%) were children of the patients, 2 (3.8%) were parents of the
patients, and 2 (3.8%) were siblings of the patients. The average length of time the respondents
had known these support providers was 26.62 years (SD =12.72, range: 5-54).
Measures
Family communication patterns. Family communication patterns were measured using
the Revised Family Communication Pattern Instrument (RFCP; Ritchie & Fitzpatrick, 1990).
The RFCP is 26-item measure designed to assess two dimensions of family communication
patterns: conversation and conformity. For this study, a modified version of the RFCP was
utilized to assess the two dimensions in order to prevent participant burnout. Further, because
participants were not required to have children to complete the questionnaire, those items that
focused exclusively on children were not included. Also, some of the items included in the
questionnaire were reworded so that instead of referring specifically to parents and children they
referred to “heads of the household” and “other family members.” Thus, the following eight
items measuring conversation orientation were used to assess conversation orientation: (i) ‘We
often talk as a family about things we have done during the day’; (ii) ‘My family encourages me
to express my feelings’; (iii) ‘I can tell my family members almost anything’; (iv) ‘I really enjoy
talking to my family members, even when we disagree’; (v) ‘In our family, we often talk about
our plans and hopes for the future’; (vi) ‘I usually tell the people in my family what I am
thinking about things’; (vii) ‘In our family we often talk about our feelings and emotions’; and
33
(viii) ‘The people in my family like to hear my opinion, even when they don’t agree with me’.
Responses were averaged (M = 3.98, SD = .84, range: 1.88-5.00, α = .90). Eight items measured
conformity orientation: (i) ‘My family has established rules that everyone is expected to obey’;
(ii) ‘If the head(s) of the house don’t approve of it, they don’t want to know about it’; (iii) ‘In our
home, the head(s) of the household usually have the last word’; (iv) ‘The head(s) of the house
often say something like, “My ideas are right and you should not question them”’; (v) ‘The
head(s) of my household say something like “You should give in on arguments rather than risk
making people mad”’; (vi) ‘My family members become irritated with my views if they are
different from theirs’; (vii) ‘The head(s) of my household say something like, “There are some
things that just shouldn’t be talked about”’; (viii) ‘The head(s) of the household feel that it is
important to be the boss’. Individuals completing the scale were asked to respond to these items
on a scale ranging from 1 (never) to 5 (frequently). Responses were averaged (M = 2.17, SD =
.91, range = 1.00 – 5.00, α = .89). Although in some past studies (Orrego & Rodriquez, 2001;
Zhang, 2007) four family communication styles have been derived using the mean splits on both
dimensions, I chose to focus solely on the 2 dimensions given the rather limited sample size of
this study.
Frequency of Family Discussion of the Cancer. The cancer patients’ perceived frequency
of family discussion about the cancer was measured with a single item: ‘How often would you
say your family spends talking about the illness and issues surrounding the illness?’ Participants
responded to this item using a scale from 1 (never) to 5 (frequently). Responses were averaged
(M = 3.32, SD = 1.03, range: 1.00-5.00).
Social Support. A portion of the Revised Inventory of Socially Supportive Behaviors
(ISSB; Krause, 1987) was used to measure the type and amount of support patients believed they
34
received from their primary support providers. The ISSB is 41-item measure which measures
four dimensions of support: tangible support, informational support, emotional support, and
support provided to others. Since this study was not focused on support provided to others, the
13 items on the measure that address this type of support were not included in the questionnaire.
Before completing the support items, participants were asked to think of the one family
member that currently provides them with the most support, to write down that person’s
relationship to them, and to keep that person in mind while answering the remaining
questionnaire items. Participants were asked to answer the support questions thinking back as far
as their last diagnosis. Also, some of the items were slightly modified from the original measure
to make them more applicable to the context of coping with cancer.
All 11 of the revised ISSB items measuring emotional support were included in the
questionnaire. Participants were, therefore, asked to respond to the following items on a scale
ranging from 1(never) to 5 (frequently): Since the diagnosis, how often has this person, (i) ‘Been
right there with you (physically) during this stressful situation’; (ii) ‘Told you you were okay just
the way you are, (iii) Comforted you by showing you physical affection’; (iv) ‘Listened to you
talk about your private feelings’; (v) ‘Told you they felt very close to you’; (vi) ‘Joked and
kidded to try to cheer you up’; (vii) ‘Expressed interest in and concern for your well-being’;
(viii) ‘Went with you to see someone who helped you with a problem that you were having
related to the illness/coping with the illness’; (ix) ‘Told you that they would keep the things you
talked about privately just between the two of you’; (x) ‘Did some activity together with you to
help you get your mind off things’; (xi) ‘Told you how they felt in a situation that was similar to
yours’. Responses were averaged (M = 3.92, SD = .87, range = 1.55 to 5.00, α = .90).
35
Out of the original 9 tangible support items, only 3 were selected for the questionnaire,
given that most of the items (i.e. ‘Provided you with a place to stay overnight’) were not
particularly applicable to relationships within the immediate family. Like with the emotional
support items, participants were asked to respond on a scale from 1 (never) to 5 (frequently).
Factor analysis suggested that one item be dropped. Principle components analyses using
varimax rotation indicated the following 2 item measure for the emotional support factor: Since
the diagnosis, how often has this person, (i) ‘pitched in to help you do something that needed to
get done, like household chores or yardwork?’; (ii) ‘helped you with shopping?’ Responses were
averaged (M = 4.42, SD = 1.02, range: 1.00-5.00, α = .75).
All 7 of the informational support items were included in the questionnaire. Like with all
of the other items, participants were asked to respond on a scale from 1 (never) to 5 (frequently).
Factor analysis suggested that one item be dropped. Principle components analyses using
varimax rotation indicated the following 6 item measure for the informational support factor:
Since the diagnosis, how often has this person (i) ‘suggested some action that you should take in
dealing with a problem you were having related to the illness/coping with the illness?’; (ii)
‘given you information that made a difficult situation clearer and easier to understand?’; (iii)
‘helped you understand why you didn't do something well?’; (iv) ‘told you who you should see
for assistance with a problem that you were having relating to the illness/coping with the
illness?’; (v) ‘commented on how you were dealing with a problem related to the illness/coping
with the illness without saying it was good or bad?’; (vi) ‘checked back with you to see if you
followed advice you were given on how to deal with a problem related to the illness/coping with
the illness?’ Responses were averaged (M = 3.48, SD = .91, range = 1.85 – 5.00, α = .82).
36
Amount of Patient Talk about Support Needs. The cancer patients’ perceived amount of
time spent talking about their support needs with their family was measured with the following
item: ‘How often would you say you talk to your family about your support needs?’ Participants
responded to this item using a scale from 1 (never) to 5 (very often). Responses were averaged
(M = 3.24, SD = 1.30, range: 1.00-5.00).
Optimal Matching. Six Likert-type items were created for this study to measure the
degree to which the cancer patients report experiencing optimal matching. Principle components
analyses using varimax rotation suggested a 2 factor measure of optimal matching. One factor
reflected optimal matching that occurs from within-family support (i.e., from the primary support
provider the respondents were asked to think about before answering the revised ISSB items)
which was defined by 4 items: (i) ‘How satisfied are you with the support you are currently
receiving from this individual?’ (answered using a Likert scale ranging from 1 “not at all
satisfied” to 5 “very satisfied”); (ii) ‘I feel like I am getting the support that I need from this
individual’ (answered using a Likert scale ranging from 1 “not at all true” to 5 “very true”); (iii)
‘When it comes to the amount of support I am receiving I am…’ (answered using a Likert scale
ranging from 1 “not at all satisfied” to 5 “very satisfied”); (iv) ‘Sometimes I wish that my family
offered me more support’ (answered using a Likert scale ranging from 1 “not at all true” to 5
“very true”). The final item listed was reverse coded for analyses. Responses were averaged (M
= 3.91, SD = 1.14, α = .91). The second factor reflected optimal matching that occurs from
external support (i.e., support from individuals outside the immediate family) which was defined
by 2 items: (i) ‘I turn to people outside of my immediate family to provide me with support’
(answered using a Likert scale ranging from 1 “never” to 5 “frequently”); (ii) ‘If I can’t get the
support that I need from within my family, I have people outside my family who can provide me

37
with the support I need’ (answered using a Likert scale ranging from 1 “not at all true” to 5 “very
true”). Responses were averaged (M = 2.36, SD = 1.14, range = 1.00 - 5.00, α = .78).
Conflict styles. Conflict styles were measured with the Rahim Organizational Conflict
Inventory- II (ROCI-II; Rahim, 1983). This measure consists of 28 Likert-type items that assess
the five conflict styles: competition, collaboration, compromise, accommodation, and avoidance.
All 28 items were included in the questionnaire along with 4 additional items that had once been
developed by Rahim (1983) to measure conflict styles. Participants responded to these items
using a scale ranging from 1 (never) to 5 (frequently) and were reminded to continue to think of
their primary support providers while responding.
Principle components analyses using varimax rotation suggested a 4 factor measure of
conflict orientation. One factor reflected collaboration and compromise which was defined by 10
items: (i) ‘I try to investigate an issue with ____________ to find a solution acceptable to us’;
(ii) ‘I try to integrate my ideas with those of ____________’s to come up with a decision
jointly’; (iii) ‘I try to work with ___________ to find solutions to a problem which satisfy our
expectations’; (iv) ‘I propose a middle ground for breaking deadlocks’; (v) ‘I exchange accurate
information with ____________ to solve a problem together’; (vi) ‘I negotiate with
____________ so that a compromise can be reached’; (vii) ‘I try to bring all our concerns out in
the open so that the issues can be resolved in the best possible way’; (viii) ‘I use "give and take"
so that a compromise can be made’; (ix) ‘I collaborate with ___________ to come up with
decisions acceptable to us’; (x) ‘I try to work with ____________ for a proper understanding of a
problem’. Responses were averaged (M = 3.82, SD = .85, range = 1.70 – 5.00, α = .93). The
second factor reflected competition and was defined by 5 items: (i) ‘I use my power to win a
competitive situation’; (ii) ‘I use my influence to get my ideas accepted’; (iii) ‘I use my authority

38
to make a decision in my favor’; (iv) ‘I use my expertise to make a decision in my favor’; (v) ‘I
am generally firm in pursuing my side of the issue’. Responses were averaged (M = 2.38, SD =
.80, range = 1.00 – 5.00, α = .86). The third factor reflected accommodation and was defined by
3 items: (i) ‘I generally try to satisfy the needs of ___________’; (ii) ‘I accommodate the wishes
of __________’; (iii) ‘I go along with the suggestions of __________’. Responses were averaged
(M = 3.60, SD = .87, range = 1.33 – 5.00, α = .74). And the final factor reflected avoidance and
was defined by 6 items: (i) ‘I try to keep my disagreement with ___________to myself in order
to avoid hard feelings’; (ii) ‘I try to avoid unpleasant exchanges with ____________’; (iii) ‘I
generally avoid an argument with _____________’; (iv) ‘I attempt to avoid being "put on the
spot" and try to keep my conflict with __________ to myself’; (v) ‘I avoid open discussion of
my differences with _________’; (vi) ‘I try to stay away from disagreement with
____________’. Reponses were averaged (M = 2.80, SD = 1.18, range 1.00 – 5.00, α = .92).
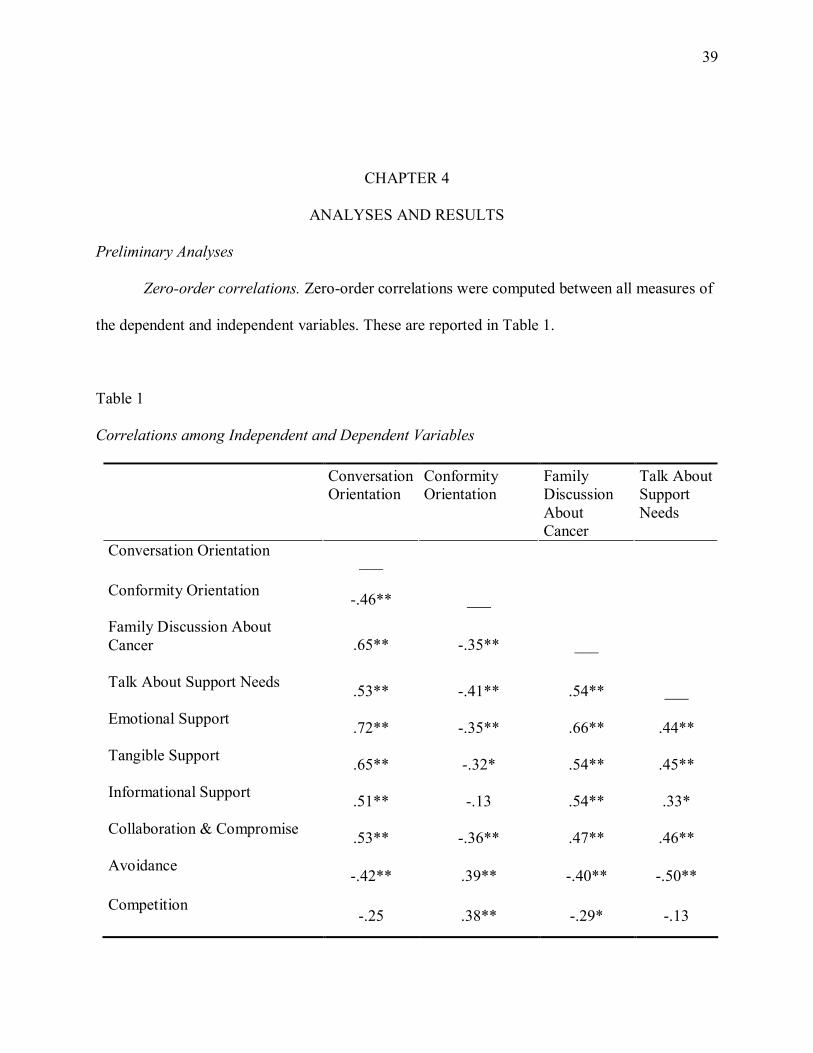
39
CHAPTER 4
ANALYSES AND RESULTS
Preliminary Analyses
Zero-order correlations. Zero-order correlations were computed between all measures of
the dependent and independent variables. These are reported in Table 1.
Table 1
Correlations among Independent and Dependent Variables
Conversation
Orientation
Conformity
Orientation
Family
Discussion
About
Cancer
Talk About
Support
Needs
Conversation Orientation
___
Conformity Orientation
-.46** ___
Family Discussion About
Cancer
.65** -.35** ___
Talk About Support Needs
.53** -.41** .54** ___
Emotional Support
.72** -.35** .66** .44**
Tangible Support
.65** -.32* .54** .45**
Informational Support
.51** -.13 .54** .33*
Collaboration & Compromise
.53** -.36** .47** .46**
Avoidance
-.42** .39** -.40** -.50**
Competition
-.25 .38** -.29* -.13
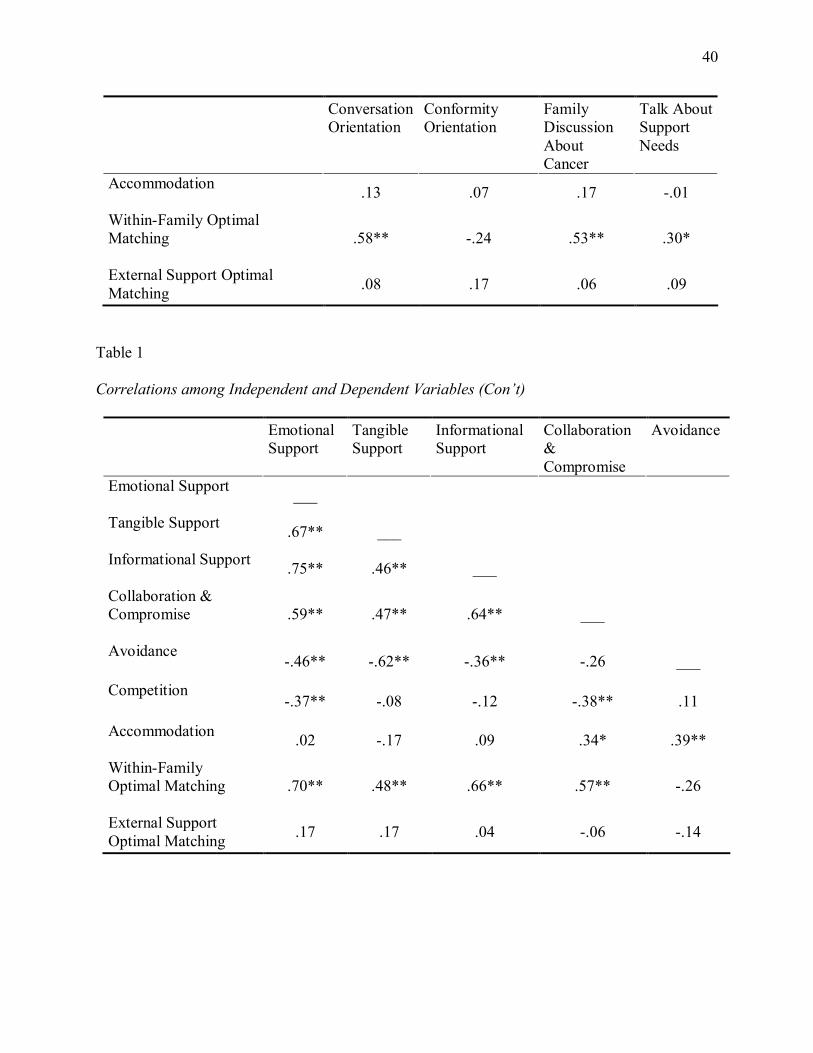
40
Conversation
Orientation
Conformity
Orientation
Family
Discussion
About
Cancer
Talk About
Support
Needs
Accommodation
.13 .07 .17 -.01
Within-Family Optimal
Matching
.58** -.24 .53** .30*
External Support Optimal
Matching .08 .17 .06 .09
Table 1
Correlations among Independent and Dependent Variables (Con’t)
Emotional
Support
Tangible
Support
Informational
Support
Collaboration
&
Compromise
Avoidance
Emotional Support
___
Tangible Support
.67** ___
Informational Support
.75** .46** ___
Collaboration &
Compromise
.59** .47** .64** ___
Avoidance
-.46** -.62** -.36** -.26 ___
Competition
-.37** -.08 -.12 -.38** .11
Accommodation
.02 -.17 .09 .34* .39**
Within-Family
Optimal Matching
.70** .48** .66** .57** -.26
External Support
Optimal Matching .17 .17 .04 -.06 -.14
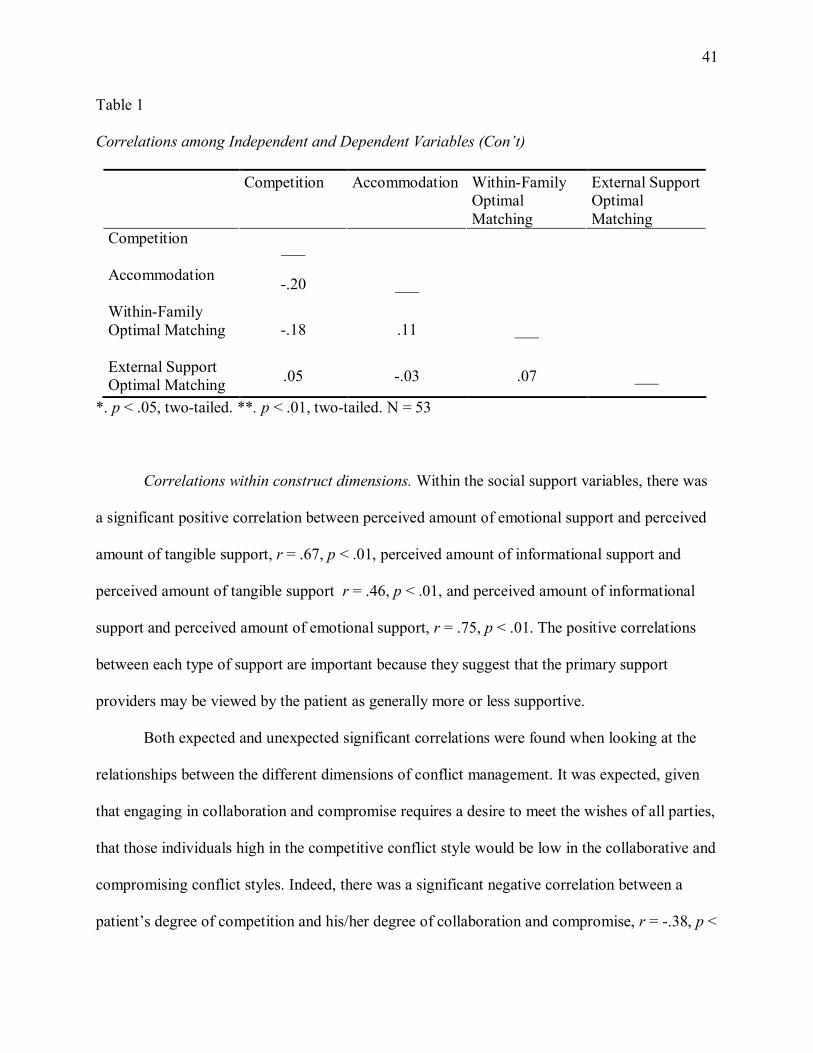
41
Table 1
Correlations among Independent and Dependent Variables (Con’t)
Competition Accommodation Within-Family
Optimal
Matching
External Support
Optimal
Matching
Competition
___
Accommodation
-.20 ___
Within-Family
Optimal Matching
-.18 .11 ___
External Support
Optimal Matching .05 -.03 .07 ___
*. p < .05, two-tailed. **. p < .01, two-tailed. N = 53
Correlations within construct dimensions. Within the social support variables, there was
a significant positive correlation between perceived amount of emotional support and perceived
amount of tangible support, r = .67, p < .01, perceived amount of informational support and
perceived amount of tangible support r = .46, p < .01, and perceived amount of informational
support and perceived amount of emotional support, r = .75, p < .01. The positive correlations
between each type of support are important because they suggest that the primary support
providers may be viewed by the patient as generally more or less supportive.
Both expected and unexpected significant correlations were found when looking at the
relationships between the different dimensions of conflict management. It was expected, given
that engaging in collaboration and compromise requires a desire to meet the wishes of all parties,
that those individuals high in the competitive conflict style would be low in the collaborative and
compromising conflict styles. Indeed, there was a significant negative correlation between a
patient’s degree of competition and his/her degree of collaboration and compromise, r = -.38, p <
42
.01. The unexpected significant relationships that were found were between the avoidance and
accommodation conflict styles and between the accommodation and collaboration conflict styles.
A significant positive correlation was found between a patient’s degree of avoidance and his/her
degree of accommodation, r = .39, p < .01. This indicates that many of those individuals that are
practicing avoidant conflict tactics are also practicing accommodation tactics. There was also a
significant positive correlation between a patient’s degree of accommodation and his/her degree
of collaboration, r = .34, p < .05.
Looking at the associations between family communication patterns, it appears that there
was a significant negative correlation between a patient’s level of family conversation orientation
and his/her reported level of family conformity orientation, r = -.46, p < .01. This negative
association between conversation and conformity provides insight into the finding that nearly all
of the conformity orientation’s relationships to the support-related variables are opposite that of
conversation orientation.
Correlations regarding communication about cancer and social support. One expectation
throughout this research was that those families that practice and encourage open communication
regularly were going to use this skill to cope with and manage their one member’s diagnosis and
fight with cancer. Because these high conversation orientation families value talking through
emotions, concerns and ideas, it was suspected that individuals in these families were going to
feel comfortable frequently discussing the cancer and the physical and psychological needs
associated with the cancer. Preliminary analyses indicated that, in fact, the level of family
conversation orientation was significantly and positively associated with both a patient’s
perceived frequency of family discussion about the cancer, r = .66, p < .01, and a patient’s
amount of talk about his/her support needs, r = .53, p < .01. A significant negative correlation, on

43
the other hand, was found between the level of family conformity orientation and both a patient’s
perceived frequency of family discussion about the cancer, r = -.35, p < .01, and a patient’s
amount of talk about his/her support needs, r = -.41, p < .01.
Because families high in conversation orientation have members that are comfortable
with expressing and responding to emotions, it was suspected that there would be a positive
relationship between a patient’s family conversation orientation and his/her perception of
emotional support provided by his/her primary support provider. A significant positive
association between the level of family conversation orientation and the perceived amount of
emotional support was, in fact, found in preliminary analyses, r = .72, p < .01. In addition, there
was a significant positive relationship found between family conversation orientation and
perceived amount of tangible support, r = .65, p < .01, and between family conversation
orientation and perceived amount of informational support, r = .51, p < .01. Perhaps the more a
family emphasizes open communication, the more information that is exchanged regarding
support needs and, therefore, the more support that is provided (emotional or other). Indeed,
there was also a significant positive relationship between a patient’s amount of discussion about
his/her support needs and his/her perceived amount of emotional support, r = .44, p < .01,
tangible support, r = .45, p < .01, and informational support, r = .33, p < .01.
There was also a positive association between the frequency of family discussion about
the patient’s cancer and the patient’s perceived amounts of all three types of social support. The
zero-order correlations showed a significant positive correlation between the frequency of family
discussion about the patient’s cancer and his/her perceived amount of emotional support, r = .66,
p < .01, tangible support, r = .54, p < .01, and informational support, r = .54, p < .01. In other

44
words, those families that were engaging in more frequent communication about the patient’s
cancer had cancer patient’s that perceived themselves as having more support.
Because families that are high in conformity orientation are less comfortable expressing
emotions and concerns and are particularly careful to maintain the established power hierarchy
(which evidence of vulnerability could threaten), it was also suspected that there would be a
negative relationship between a patient’s family conformity orientation and his/her perception of
the amount of emotional support provided by his/her primary support. The primary analysis
confirmed this suspicion, showing a significant negative association between a patient’s level of
family conformity orientation and his/her perceived amount of emotional support, r = -.35, p <
.01. It also indicated a significant negative association between a patient’s level of family
conformity orientation and his/her perceived amount of tangible support, r = -.32, p < .05.
Zero-order correlations showed that there was a significant positive association between
the level of family conversation orientation and within-family optimal matching, r = .58, p < .01.
In other words, the more open communication seems to allow for what the patients perceive as a
better understanding of their support needs on the part of their primary support providers.
It was previously suspected that the more cancer patients were able to communicate their
support needs to their support providers, the more optimal matching would occur. This belief
stemmed from the idea that the more cancer patients discussed their support needs, the clearer
understanding both the support providers and the patients would have about the amount and
types of support that the patients were finding most helpful and what, if any, changes needed to
be made. The suspected association was indicated in the zero-order correlations. While there
were no significant correlations found between external support optimal matching and any of the

45
other variables, there was a significant positive correlation between the patient’s amount of talk
about his/her support needs and his/her within-family optimal matching, r = .30, p < .05.
A significant positive correlation was identified between the frequency of family
discussion about the cancer and a patient’s amount of talk about his/her support needs to the
family, r = .54, p < .01. This relationship may stem from the fact that the more a cancer patient
discusses the experience of the illness, the more likely his or her support needs will emerge in
discussion. There was also a significant positive association between the frequency of family
discussion about the cancer and the collaborative and compromising conflict style, r = .47, p <
.01 and significant negative associations between the frequency of family discussion about the
cancer and the degree of both avoidant conflict management, r = -.40, p < .01, and competitive
conflict management, r = .29, p < .05. Given the positive relationship between the frequency of
family discussion about the cancer and the patient’s amount of communication about his/her
support needs, it is not surprising that the zero-order correlations also identified a positive
relationship between the patient’s amount of communication about his/her support needs and the
degree of collaborative and compromising conflict management, r = .46, p < .01, and a negative
relationship between the patient’s amount of communication about his/her support needs and the
degree of avoidant conflict management, r = -.50, p < .01.
There was a positive association found between the frequency of family discussion about
the cancer and within-family optimal matching, r = .53, p < .01. This positive association
indicates that the patients who perceive their families as being open to discussing the issues,
concerns, and decisions surrounding their cancer are often the same individuals who are most
satisfied with their within-family support. There were also significant correlations between
within-family optimal matching and the perceived amount emotional support, r = .70, p < .01,
46
tangible support, r = .48, p < .01, and informational support, r = .66, p < .01. Thus, it appears
that the more support received from the primary caregiver (regardless of which type), the more
the patient experienced optimal matching.
Correlations regarding conflict. In regard to the relationship between conversation
orientation and conflict management, because individuals in a family high in conversation
orientation are used to talking through issues and both hearing and expressing different ideas, it
was suspected that these same individuals would be the ones engaging in constructive conflict
management Therefore, there was a suspected positive relationship between family conversation
and the collaborative and compromising conflict style. There was also a suspected negative
relationship between the level of family conversation orientation and the patient’s degree of
conflict avoidance. The suspected associations were indicated in the zero-order correlations, as
there was a significant positive correlation between a patient’s level of family conversation
orientation and the degree of collaborative and compromising conflict management, r = .53, p <
.01, and a significant negative correlation between a patient’s family conversation orientation
and the degree of avoidant conflict management, r = -.42, p < .01.
With regard to family conformity orientation, because individuals in families high in
conformity are discouraged from expressing differing viewpoints and from challenging both
established roles and ideas, it was believed that these individuals actively seek to avoid conflict.
It was also suspected that when conflict is brought into the open, it is solved mainly by those
who have the power in the household in the way they see fit, with little input from the rest of the
family. Therefore, it was believed that there would be a positive relationship between family
conformity and the avoidant conflict style and a negative relationship between family conformity
and the collaboration and compromise conflict style. Indeed, the zero-order correlations
47
indicated a significant positive association between a patient’s level of family conformity
orientation and his/her degree of avoidance, r = .39, p < .01, thus mirroring the relationship
Koerner and Fitzpatrick (1997) identified between these two variables. A significant negative
correlation was also found between a patient’s level of family conformity and his/her degree of
collaboration and compromise, r = -.36, p < .01. In addition, a significant positive correlation
was found between a patient’s level of family conformity orientation and his/her degree of
competition, r = .38, p < .01.
Considering the relationship between social support and conflict styles, the degree of
collaborative and compromising conflict management was positively associated with a patient’s
perceived amount of emotional support, , r = .59, p < .01, tangible support, r = .47, p < .01, and
informational support, r = .64, p < .01. This pattern of significant associations suggests that the
more patients engaged in constructive conflict management styles with their family members, the
more social support they perceived themselves as receiving from those members. The degree of
avoidant conflict management, on the other hand, was negatively associated with a patient’s
perceived amount of emotional support, r = -.45, p < .01, tangible support, r = -.62, p < .01, and
informational support, r = -.36, p < .01. This negative association suggests that the more patients
try to prevent conflict from occurring and/or avoid managing conflict situations with their family
members, the less social support they perceive themselves as receiving from those members.
Finally, a significant negative relationship was found between the degree of competitive conflict
management and the perceived amount of emotional support, r = -.37, p < .01. Perhaps when
competitive tactics are used to handle conflict between the patients and their family members, at
least one (if not both) of the individuals could become hurt or frustrated and, therefore, not open
to giving or receiving emotional support.
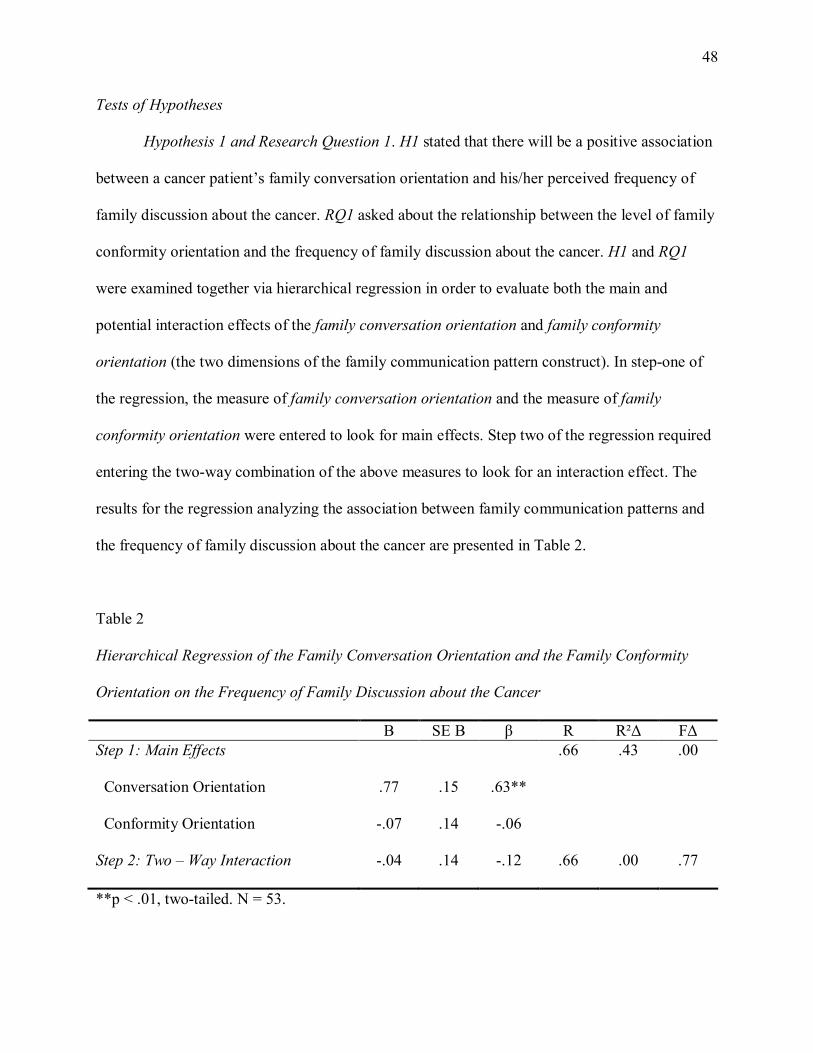
48
Tests of Hypotheses
Hypothesis 1 and Research Question 1. H1 stated that there will be a positive association
between a cancer patient’s family conversation orientation and his/her perceived frequency of
family discussion about the cancer. RQ1 asked about the relationship between the level of family
conformity orientation and the frequency of family discussion about the cancer. H1 and RQ1
were examined together via hierarchical regression in order to evaluate both the main and
potential interaction effects of the family conversation orientation and family conformity
orientation (the two dimensions of the family communication pattern construct). In step-one of
the regression, the measure of family conversation orientation and the measure of family
conformity orientation were entered to look for main effects. Step two of the regression required
entering the two-way combination of the above measures to look for an interaction effect. The
results for the regression analyzing the association between family communication patterns and
the frequency of family discussion about the cancer are presented in Table 2.
Table 2
Hierarchical Regression of the Family Conversation Orientation and the Family Conformity
Orientation on the Frequency of Family Discussion about the Cancer
B SE B β R R²∆ F∆
Step 1: Main Effects
Conversation Orientation
Conformity Orientation
Step 2: Two – Way Interaction
.77
-.07
-.04
.15
.14
.14
.63**
-.06
-.12
.66
.66
.43
.00
.00
.77
**p < .01, two-tailed. N = 53.
49
Analyses indicated that there was a significant main effect for the association between family
conversation orientation and frequency of family discussion about the cancer, β = .63, p < .01.
Therefore, as the preliminary analysis suggested, H1 received support. In regards to RQ1,
however, no significant main effect was found for the association between family conformity
orientation and frequency of family discussion about the cancer. The analyses indicated no
significant two-way interaction effect for the family orientations on frequency of family
discussion about the cancer.
Hypothesis 2. H2 stated that there will be a positive association between a cancer
patient’s family conversation orientation and that patient’s perception of the amount of emotional
support provided by the primary support provider. This hypothesis was examined via multiple
regression with the measure of perceived amount of emotional support as the dependent variable.
Specifically, in step-one of the regression, the measure of family conversation orientation and
the measure of family conformity orientation were entered to look for main effects. Step two of
the regression required entering the two-way combination of the above measures to look for an
interaction effect. The results for the regression analyzing the association between a cancer
patient’s family conversation orientation and his/her perception of the amount of emotional
support provided are presented in Table 3.

50
Table 3
Hierarchical Regression of the Family Conversation Orientation and the Family Conformity
Orientation on the Perceived Amount of Emotional Support
B SE B β R R²∆ F∆
Step 1: Main Effects
Conversation Orientation
Conformity Orientation
Step 2: Two – Way Interaction
.73
-.02
.06
.11
.10
.14
.71**
-.03
.21
.72
.72
.52
.00
.00
.58
**p < .01, two-tailed. N = 53.
Analyses indicated that there was a significant main effect for the association between family
conversation orientation and perceived amount of emotional support, β = .71, p < .01. Therefore,
H2 received support. The analyses indicated no significant two-way interaction effect for the
family orientations on perceived amount of emotional support.
Research Question 2. RQ2 asked about the relationship between a cancer patient’s level
of family conformity orientation and the amount of emotional, tangible and informational
support he/she perceives him/herself as receiving from their primary support provider. The
results shown in Table 3 for the regression described above indicate no significant main effect
for the association between family conformity orientation and perceived emotional support.
Another hierarchical regression was run with the perceived amount of tangible support as the
dependent variable. In step-one of the regression, the measure of family conversation orientation
and the measure of family conformity orientation were entered to look for main effects. Step two
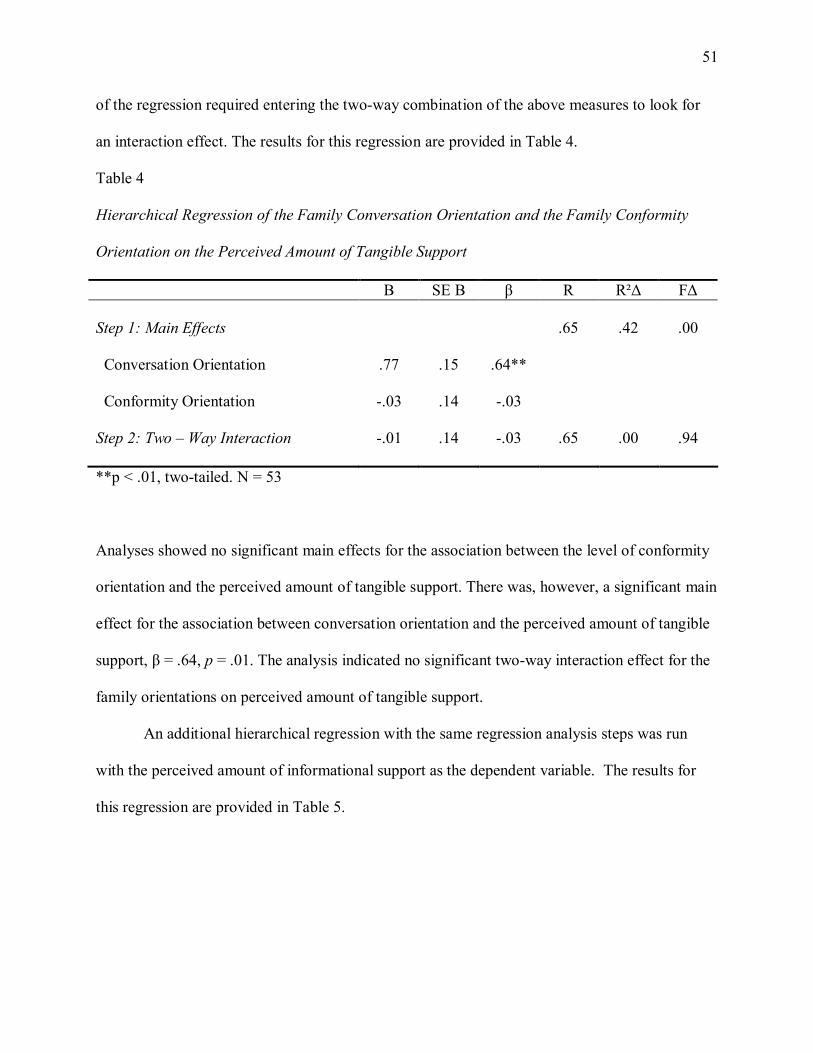
51
of the regression required entering the two-way combination of the above measures to look for
an interaction effect. The results for this regression are provided in Table 4.
Table 4
Hierarchical Regression of the Family Conversation Orientation and the Family Conformity
Orientation on the Perceived Amount of Tangible Support
B SE B β R R²∆ F∆
Step 1: Main Effects
Conversation Orientation
Conformity Orientation
Step 2: Two – Way Interaction
.77
-.03
-.01
.15
.14
.14
.64**
-.03
-.03
.65
.65
.42
.00
.00
.94
**p < .01, two-tailed. N = 53
Analyses showed no significant main effects for the association between the level of conformity
orientation and the perceived amount of tangible support. There was, however, a significant main
effect for the association between conversation orientation and the perceived amount of tangible
support, β = .64, p = .01. The analysis indicated no significant two-way interaction effect for the
family orientations on perceived amount of tangible support.
An additional hierarchical regression with the same regression analysis steps was run
with the perceived amount of informational support as the dependent variable. The results for
this regression are provided in Table 5.

52
Table 5
Hierarchical Regression of the Family Conversation Orientation and the Family Conformity
Orientation on the Perceived Amount of Informational Support
B SE B β R R²∆ F∆
Step 1: Main Effects
Conversation Orientation
Conformity Orientation
Step 2: Two – Way Interaction
.62
.13
.03
.15
.14
.14
.57**
.13
.10
.53
.53
.28
.00
.00
.84
**p < .01, two-tailed. N = 53.
Analyses showed no significant main effects for the association between the level of conformity
orientation and the perceived amounts of informational support. There was, however, a
significant main effect for the association between conversation orientation and the perceived
amount of informational support, β = .57, p = .01. The analyses indicated no significant two-way
interaction effect for the family orientations on perceived amount of informational.
Hypothesis 3 and RQ3: H3 stated that there will be a positive association between a
cancer patient’s family conversation orientation and the amount of time that patient spends
talking about his/her social support needs with the other family members. RQ3 asked about the
relationship between a cancer patient’s family conformity orientation and the amount of time that
patient spends talking about his/her social support needs with the other family members. H3 and
RQ3 were examined together via hierarchical regression with the dependent variable being the
amount of time a patient spends talking about his/her social support needs with the other family
members. In step-one of the regression, the measure of family conversation orientation and the
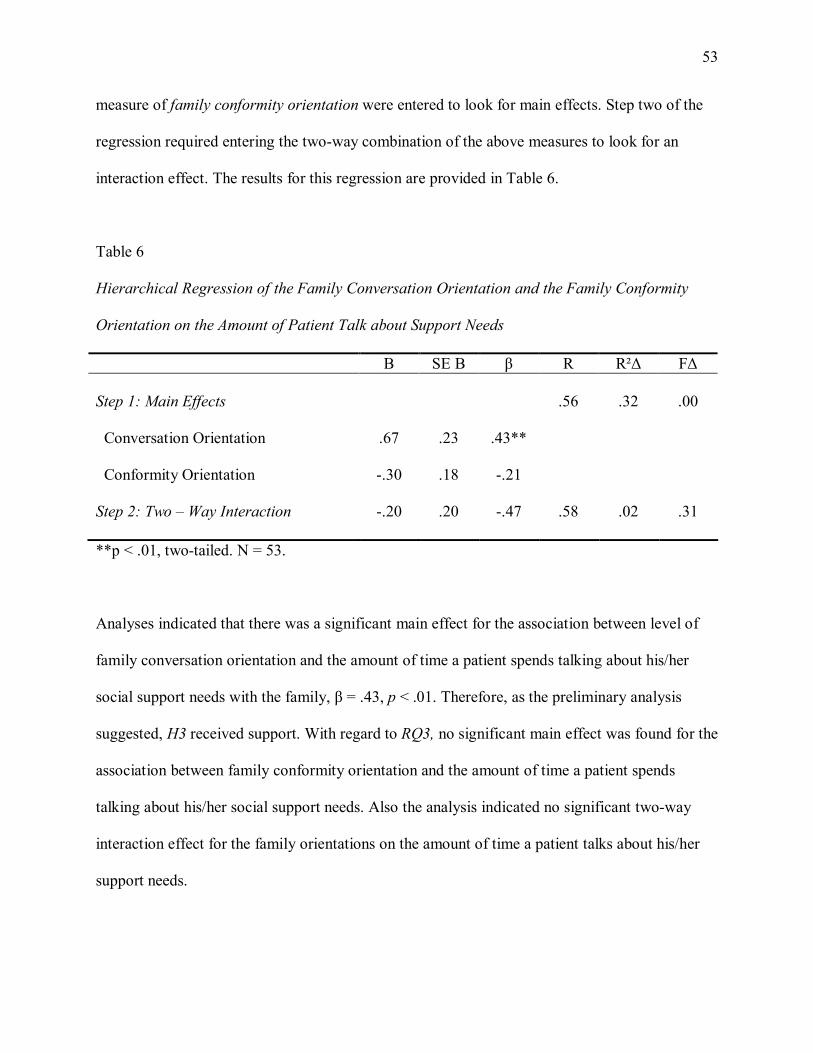
53
measure of family conformity orientation were entered to look for main effects. Step two of the
regression required entering the two-way combination of the above measures to look for an
interaction effect. The results for this regression are provided in Table 6.
Table 6
Hierarchical Regression of the Family Conversation Orientation and the Family Conformity
Orientation on the Amount of Patient Talk about Support Needs
B SE B β R R²∆ F∆
Step 1: Main Effects
Conversation Orientation
Conformity Orientation
Step 2: Two – Way Interaction
.67
-.30
-.20
.23
.18
.20
.43**
-.21
-.47
.56
.58
.32
.02
.00
.31
**p < .01, two-tailed. N = 53.
Analyses indicated that there was a significant main effect for the association between level of
family conversation orientation and the amount of time a patient spends talking about his/her
social support needs with the family, β = .43, p < .01. Therefore, as the preliminary analysis
suggested, H3 received support. With regard to RQ3, no significant main effect was found for the
association between family conformity orientation and the amount of time a patient spends
talking about his/her social support needs. Also the analysis indicated no significant two-way
interaction effect for the family orientations on the amount of time a patient talks about his/her
support needs.
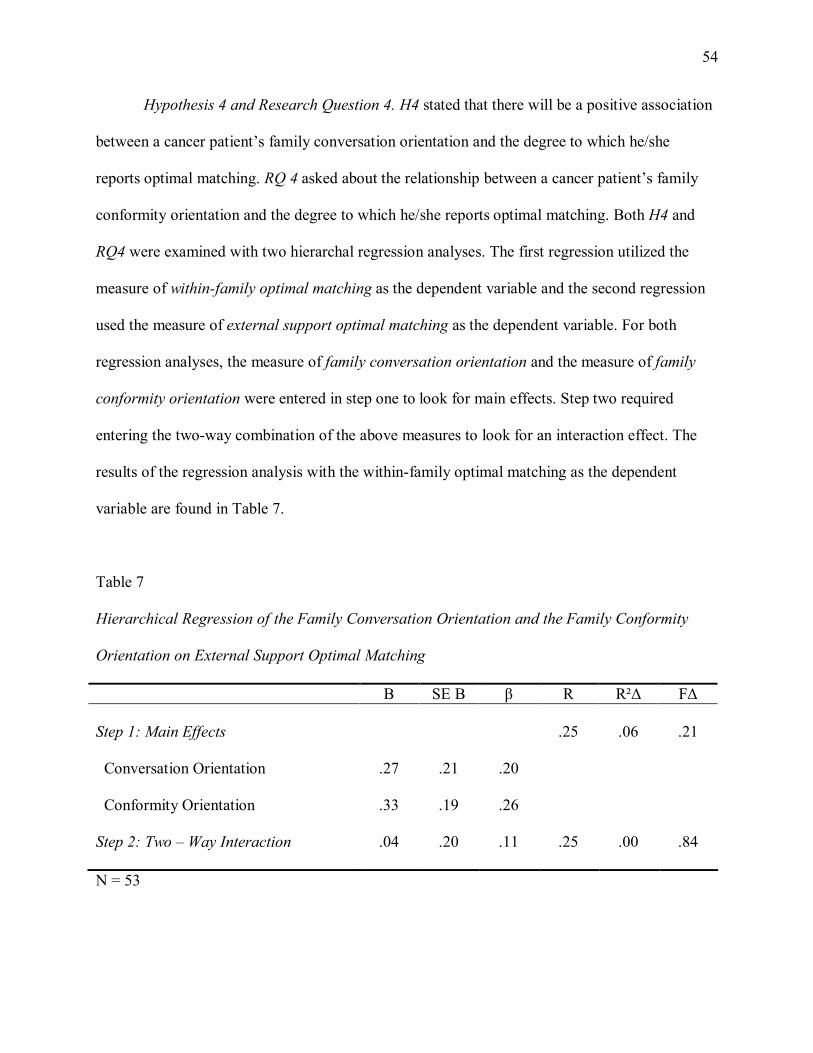
54
Hypothesis 4 and Research Question 4. H4 stated that there will be a positive association
between a cancer patient’s family conversation orientation and the degree to which he/she
reports optimal matching. RQ 4 asked about the relationship between a cancer patient’s family
conformity orientation and the degree to which he/she reports optimal matching. Both H4 and
RQ4 were examined with two hierarchal regression analyses. The first regression utilized the
measure of within-family optimal matching as the dependent variable and the second regression
used the measure of external support optimal matching as the dependent variable. For both
regression analyses, the measure of family conversation orientation and the measure of family
conformity orientation were entered in step one to look for main effects. Step two required
entering the two-way combination of the above measures to look for an interaction effect. The
results of the regression analysis with the within-family optimal matching as the dependent
variable are found in Table 7.
Table 7
Hierarchical Regression of the Family Conversation Orientation and the Family Conformity
Orientation on External Support Optimal Matching
B SE B β R R²∆ F∆
Step 1: Main Effects
Conversation Orientation
Conformity Orientation
Step 2: Two – Way Interaction
.27
.33
.04
.21
.19
.20
.20
.26
.11
.25
.25
.06
.00
.21
.84
N = 53

55
As with the preliminary analysis, the regression analyses examining the relationship between
family communication patterns and external support optimal matching identified no significant
correlations. Also the analyses indicated no significant two-way interaction effect for the family
orientations on the amount of external support optimal matching.
The results of the regression analyses with the within-family optimal matching as the
dependent variable are found in Table 8.
Table 8
Hierarchical Regression of the Family Conversation Orientation and the Family Conformity
Orientation on Within-Family Optimal Matching
B SE B β R R²∆ F∆
Step 1: Main Effects
Conversation Orientation
Conformity Orientation
Step 2: Two – Way Interaction
.81
.04
-.04
.18
.16
.17
.60**
.04
-.11
.58
.59
.34
.00
.00
.81
**p < .01, two-tailed. N = 53.
Analyses examining the relationship between family communication patterns and within-family
optimal matching identified a significant main effect for the relationship between the level of
family conversation orientation and within-family optimal matching, β = .60, p < .01. Therefore,
as indicated in the primary analysis, H4 received support. In regards to RQ4, however, no
significant main effects were found between the level of family conformity orientation and
56
within-family optimal matching. Also the analysis indicated no significant two-way interaction
effect for the family orientations on the amount of within-family optimal matching.
Hypothesis 5 and Research Question 5. H5 stated that there will be a relationship
between cancer patients’ conflict management style and optimal matching such that: (a) Avoidant
or accommodative orientations will be negatively associated with perceived optimal matching
and (b) Collaborative or compromising orientations will be positively associated with perceived
optimal matching. RQ5 asked about the association between the competitive conflict
management style and optimal matching. An examination of the mean scores on the conflict
management styles indicated that several participants could not be categorized into only one
style so regressions based on the dimensional measures of conflict orientation were conducted.
Further, since optimal matching was defined by two factors, two separate regression analyses
were run. For both analyses, the same two steps were followed. In step-one, the measure of the
collaborative and compromising management style, the measure of the avoidant management
style, the measure of the competitive management style, and the measure of the accommodating
management style were all entered to look for main effects. Step two of both regression analyses
required entering all possible two-way combinations of the above measures (collaborative and
compromising and avoidant; collaborative and compromising and competitive; collaborative and
compromising and accommodating; avoidant and competitive; avoidant management style and
accommodating; competitive and avoidant). The results for the regression analyses examining
the relationship between conflict management style and external support optimal matching are
presented in Table 9.
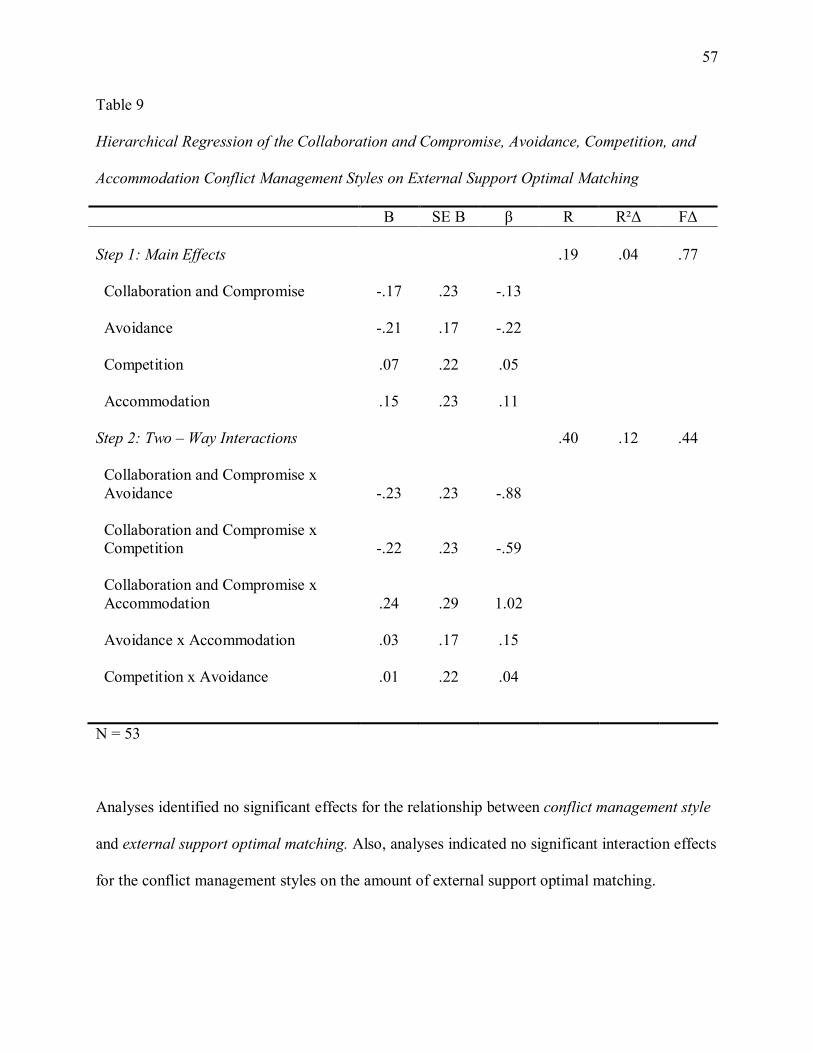
57
Table 9
Hierarchical Regression of the Collaboration and Compromise, Avoidance, Competition, and
Accommodation Conflict Management Styles on External Support Optimal Matching
B SE B β R R²∆ F∆
Step 1: Main Effects
Collaboration and Compromise
Avoidance
Competition
Accommodation
Step 2: Two – Way Interactions
Collaboration and Compromise x
Avoidance
Collaboration and Compromise x
Competition
Collaboration and Compromise x
Accommodation
Avoidance x Accommodation
Competition x Avoidance
-.17
-.21
.07
.15
-.23
-.22
.24
.03
.01
.23
.17
.22
.23
.23
.23
.29
.17
.22
-.13
-.22
.05
.11
-.88
-.59
1.02
.15
.04
.19
.40
.04
.12
.77
.44
N = 53
Analyses identified no significant effects for the relationship between conflict management style
and external support optimal matching. Also, analyses indicated no significant interaction effects
for the conflict management styles on the amount of external support optimal matching.
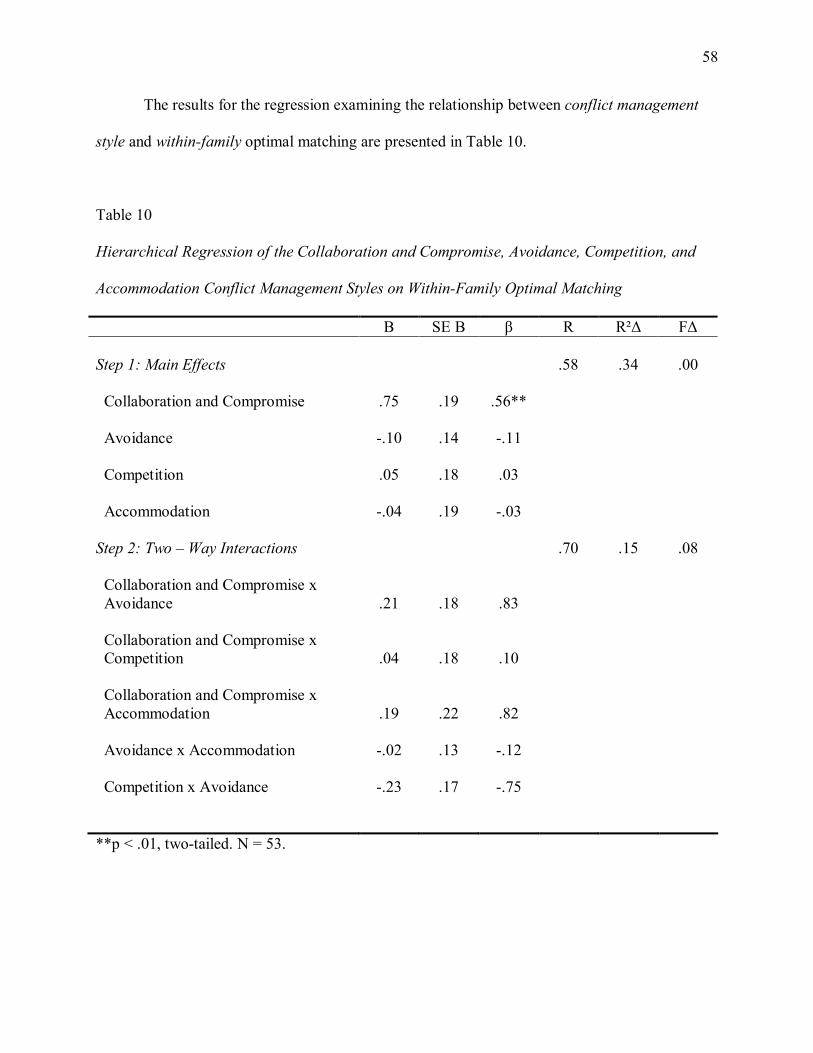
58
The results for the regression examining the relationship between conflict management
style and within-family optimal matching are presented in Table 10.
Table 10
Hierarchical Regression of the Collaboration and Compromise, Avoidance, Competition, and
Accommodation Conflict Management Styles on Within-Family Optimal Matching
B SE B β R R²∆ F∆
Step 1: Main Effects
Collaboration and Compromise
Avoidance
Competition
Accommodation
Step 2: Two – Way Interactions
Collaboration and Compromise x
Avoidance
Collaboration and Compromise x
Competition
Collaboration and Compromise x
Accommodation
Avoidance x Accommodation
Competition x Avoidance
.75
-.10
.05
-.04
.21
.04
.19
-.02
-.23
.19
.14
.18
.19
.18
.18
.22
.13
.17
.56**
-.11
.03
-.03
.83
.10
.82
-.12
-.75
.58
.70
.34
.15
.00
.08
**p < .01, two-tailed. N = 53.

59
Analyses examining the relationship between conflict management styles and within-family
optimal matching identified a significant main effect for the relationship between the
collaborative and compromising management style and within-family optimal matching, β = .56,
p < .01. No other significant main or interaction effects were identified. Therefore, H5 was
partially supported, with evidence being found for H5b but not H5a.
60
CHAPTER 5
DISCUSSION, LIMITATIONS AND CONCLUSION
The purpose of this thesis was to examine the effects of family communication patterns
and conflict management styles on cancer patients’ support satisfaction and availability. Support
was found for the hypotheses predicting positive relationships between the level of family
conversation orientation and each of the following dependent variables: frequency of family
discussion of cancer, the amount of patient communication about support needs, the perception
of the amount of available types of support, and the degree of optimal matching. Preliminary
analyses suggested potential negative relationships between conformity orientation and most of
these same dependent variables. The prediction of a positive relationship between the
collaboration and compromising conflict management styles and a patient’s reported degree of
optimal matching was also supported. Examining all of these results together, some significant
observations can be made regarding the importance of successful, open communication and
constructive conflict management when it comes to the exchanging of social support within the
family. The remainder of this chapter will highlight the significant observations that arose from
this study, discuss potential limitations of the study, and offer a conclusion that addresses the
potential implications of this work.
Observations about Optimal Matching
The theory of optimal matching has been relatively under explored up until this point
and, therefore, it is important to call attention to this study’s significant findings pertaining to the
theory. One of the most insightful findings regarding OMT was the positive association found
61
between the collaboration and compromise conflict style and the degree of optimal matching that
was predicted in H5b. What this finding suggests is that engaging in constructive conflict
management may actually be a tool for families to both become closer as a result of overcoming
challenges and to learn how to be comfortable with open and encouraging communication,
thereby making the members more in tune with one another and, thus, more satisfactory support
providers. Using collaborative and compromising conflict management techniques requires a
heightened level of trust, patience, and self-disclosure amongst the family members and the
presence of these characteristics within the household make for a safer and more effective
environment for support. Therefore, by engaging in collaboration and/or compromise, family
members may be developing the skills needed to grow closer to one another and to make them
more aware of each other’s support needs. Relationships identified in the preliminary analyses
that provided additional support for this idea were the positive relationship between the
collaboration and compromise conflict style and the frequency of family discussion of the cancer
as well as the positive relationship between the collaboration and compromise conflict style and
the cancer patient’s amount of talk about his/her support needs. The findings regarding the
relationship between constructive conflict management and support are particularly important
because they suggest that rather than avoiding conflict, families should be embracing it as tool to
become more successful communicators and social support providers. Thompson and Pitts
(1992) suggest that the nature of the well-established relationship and shared history that
characterize a family influences a sick individuals’ supportive experience. Therefore, individuals
in families that develop a history of handling conflict constructively could have more positive
feelings, feelings of closeness and feelings of trust towards one another, thereby contributing to
satisfactory communication and support. This explanation is also in line with Smetana, Yau, and

62
Hanson’s (1991) belief that collaboration and compromise are associated with healthier family
functioning than unilateral approaches to conflict management (i.e. use of power). The
understanding of the relationship between conflict and social support gained in this study is
particularly important for contexts such as cancer, because it suggests that in situations of
potentially high conflict, there is still the potential for extremely effective support exchange;
therefore, rather than trying to minimize conflict following a cancer diagnosis, families should
confront their issues, as long as they are willing and able to do it in a constructive way.
The suggestion that constructive conflict management provides the tools needed for
successful support exchange is also supported by the positive relationship found between level of
family conversation orientation and the degree of optimal matching observed in tests of H4. The
positive relationship between conversation orientation and optimal matching of within-family
social support suggests that, as expected, family members in high conversation orientation
families are more up to speed on their cancer patients’ challenges, concerns, needs, etc. due to
the more frequent and open communication all the members engage in with one another. These
family members are, therefore, better able to discern the specific types and amounts of support
that their sick loved ones need. Ell (1996) explains that optimal support requires clear
communication of need by the individual in need. The significant relationships found in both the
zero-order correlations and the regression model for the relationship between family
conversation orientation and a patient’s perceived amount of support as well as the significant
positive correlation found between a patient’s amount of talk about support needs and within-
family optimal matching of social support further support Ell’s (1996) argument. Knowing that
collaboration and compromise require significant amounts of clear, encouraging, and free
communication and that, in this study, a positive relationship was found in the preliminary
63
analyses between collaboration and compromise and level of family conversation orientation, it
is evident that constructive conflict management tools can be important to keeping
communication open and free within the family unit, thereby providing a greater opportunity for
successful support exchange.
It should also be mentioned here that zero-order correlations indicated that there were
significant positive relationships between within-family optimal matching and each of the 3
support types. This is an interesting and important finding because it suggests that with this
particular sample, the more social support a cancer patient received, the more satisfied that
patient was with his/her support. This may be because participants were asked to think about
their primary support providers when answering questions about their social support and these
are the people from whom they expect and need to receive a significant amount of assistance.
While significant relationships found in this study offer a great deal of insight into the
important contributing factors to optimal matching, further knowledge can also be gained by
trying to understand and explain the nonsignficant relationships pertaining to conflict and
optimal matching. Contrary to H5a, no significant associations were found between the avoidant
and accommodating conflict styles and within-family optimal matching in either the preliminary
analyses or the regression models. This prediction was developed partially with the belief that
cancer patients who were avoidant or accommodating would be hesitant to express
dissatisfaction with support or to request an adjustment of the support being provided to them for
fear of bringing about conflict. It could be, however, that there was not this initial dissatisfaction
with support that was being assumed and, therefore, a patient’s fear of causing conflict did not
significantly affect the degree of optimal matching. This prediction was also developed with the
belief that individuals with avoidant and accommodating conflict styles bottle up feelings of hurt
64
and frustration from unresolved issues with their family members so as to avoid engaging in
expressed conflict. This belief was in line with Koerner and Fitzpatrick’s (1997) argument that
conflict avoidance leads to negative feelings about the family which, in turn, causes tension
among family members that could result in resentment. It was thought that bottled up feelings of
tension and hurt would make it more difficult for these individuals to be open to support from
their loved ones or to have a realistic perception of the amount and quality of support they are
receiving. Because over half of the sample reported engaging in less conflict since the cancer
diagnosis, the effect of residual feelings of hurt on the perception of social support satisfaction
would not be as strong as predicted, thus potentially helping to explain the lack of significant
results for the relationship between the avoidant and accommodating conflict styles and optimal
matching.
There were also no significant associations between competitive conflict management
and within-family optimal matching, as inquired about in RQ5, in either the preliminary analyses
or the regression model. There was, therefore, no evidence supporting the suspicion that one’s
degree of competition is a strong predictor of how comfortable he/she feels expressing
satisfaction or dissatisfaction and, thus also a strong indicator of optimal matching. In fact, there
was a significant negative relationship found, between competition and frequency of family
discussion about the cancer, suggesting that competitive individuals may actually be less
comfortable engaging in open communication about sensitive topics. There was also no evidence
found lending support to the opposing explanation that competitive conflict management creates
tension and negative feelings between family members that negatively influences a patient’s
perceived reception of support and, thus, his/her degree of optimal matching. This explanation
was in line with Smetana, Yau, and Hanson’s (1991) belief that collaboration and compromise
65
are associated with healthier family functioning than unilateral approaches to conflict
management (i.e. use of power). Lack of significant support for this explanation, however, may
have to do with over half of the sample reporting that their family engaged in less conflict since
the cancer diagnosis.
Observations about Conversation Orientation
It is no surprise that, as mentioned above, the level of conversation orientation was found
to be positively related to optimal matching of support when considering the positive
relationships found between conversation orientation and each of the support-related variables.
One of the most important realizations that can be taken from this study is that open and frequent
communication is crucial within a family if that family environment is going to be one that is
conducive to the exchanging of social support. The emphasis placed on unrestrained
communication and the expression of feelings and ideas, even during times of conflict, in
families that are high in conversation orientation allows for more comfortable discussion about
the cancer and about support needs while also helping to breed trust and closeness amongst the
family members. These positive effects experienced by families high in conversation orientation
allow for optimal support exchange with as few feelings of burden or frustration as can be
expected given the circumstances. In order to offer more detailed evidence for this argument
regarding the positive effects of conversation orientation on the exchange of social support, the
hypotheses not yet discussed regarding family conversation orientation will now be examined
more closely.
As predicted in H1, a significant main effect was found for this relationship between
family conversation orientation and family discussion of cancer. This finding is not surprising
given Koerner and Fitzpatricks’s (2002) argument that the greater the level of family
66
conversation orientation, the more frequent the communication between family members and the
fewer topics family members are uncomfortable discussing with one another. Further, Elwood
and Schrader (1998) observed that conversation orientation was negatively correlated with
communication apprehension in both public and private contexts. Understanding this
observation, one could suspect that because individuals in families higher in conversation
orientation interact and communicate with one another more on a day-to-day basis than
individuals in families lower in conversation orientation, it is natural that they have more
opportunity for the topic of the patients’ cancer to arise. Also, individuals in families high in
conversation orientation feel less restricted when it comes to discussing sensitive topics such as
treatment options and concerns and fears that come along with the cancer than individuals in
families low in conversation orientation because high conversation orientation families
continuously emphasize the importance of each family member expressing his/her feelings and
ideas. Koerner and Fitzpatrick (2002) also argued that families high in conversation orientation
view open and frequent communication as a key to family success; whereas families low in
conversation do not. Therefore, it is reasonable to suspect that coming together to engage in open
family discussion about the cancer is being used as a source of comfort and a type of coping
strategy for the families. This discussion of the cancer may be a way to hold the family together
and ensure their strength during a time of heightened fear and uncertainty. Avoiding discussion
of the cancer might be just as much a coping strategy for individuals in families that are low in
conversation orientation. Because individuals in low conversation orientation families are not as
comfortable discussing ideas and feelings as openly, frequent discussion of issues and feelings
pertaining to the cancer might be too much of an additional emotional burden to take on
following a cancer diagnosis.
67
Not only was there a significant main effect found for the relationship between the level
of conversation orientation and a patient’s perceived amount of emotional support, as was
predicted in H2, but there were also significant main effects found for the relationship between
family conversation orientation and perceived amounts of tangible and information support as
well. The significant positive relationship found between family conversation orientation and
perceived emotional support falls in line with Koerner and Fitzpatrick’s (2002) argument that the
higher the level of family conversation orientation, the more encouraging and supportive
individuals are going to be of their family members’ expression of feelings and attitudes.
Individuals in high conversation orientation families are probably better equipped to be
empathetic towards one another than individuals in low conversation orientation families
because they spend more time together, supportively exchanging thoughts and feelings. For
example, Koesten (2004) found that teenage women from high conversation orientation families
were more likely to be able to offer emotional support to friends and relational partners than
teenage women from low conversation families. It is quite possible that the greater ease with
which individuals in high conversation orientation families can provide emotional support causes
them to be more emotionally supportive than those individuals in low conversation orientation
families. Therefore, patients in high conversation orientation families perceive they are getting
more emotional support from their primary support provider than individuals in low conversation
orientation families. The relationship between level of family conversation orientation and
perceived amount of emotional support could also have to do with the positive relationship
between level of family conversation orientation and frequency of family discussion about the
cancer. It may be that because families high in conversation orientation engage in more
discussion about the cancer than families low in conversation orientation, cancer patients in high
68
conversation families spend more time expressing concerns, challenges, and fears related to the
cancer than those in low conversation families and, therefore, perceive themselves as receiving
more emotional support in response to that communication.
The positive relationships that were found between conversation orientation and tangible
and emotional support might suggest that those primary support providers in high conversation
orientation families are being perceived as generally more willing and able to provide social
support than those support providers in low conversation families. Recognizing the relationship
that was found between family conversation orientation and frequency of family discussion
about the cancer, one could suspect that patients whose families spend more time talking about
their cancer view their primary support providers as generally more in-tune with their needs and
their struggles and, therefore, more supportive. Positive relationships between frequency of
family discussion about cancer and all three support types found in the preliminary analyses offer
further support for this argument.
A significant main effect was also found for the relationship between family conversation
orientation and a patient’s amount of time spent talking about support needs that was predicted in
H3. The support found for this hypothesis is in line with Koerner and Fitzpatrick’s (2002)
argument that individuals in high conversation orientation families are encouraged to freely
express their thought and feelings, whereas individuals in low conversation orientation families
are not as concerned with the thoughts and feelings of their other family members. Therefore,
individuals in families low in conversation orientation probably feel less comfortable being open
and honest with their family members about what support they feel they need than individuals in
high conversation orientation families. Individuals in low conversation orientation families might
also be feeling that directly communicating their support needs would be equally uncomfortable
69
for their family members and an additional burden for them seeing as how they are not used to
going to each other with their wants and needs. Those individuals in high conversation families,
however, probably recognize their families’ dependence on open communication and, therefore,
feel that not directly expressing their support needs would make their family members more
anxious. Further explanation may also lie in the positive correlations identified in the preliminary
analyses between the level of family conversation orientation and the frequency of family
discussion about cancer and between the level of family conversation orientation and a patient’s
amount of talk about his/her support needs. Although speculative, these significant positive
correlations may suggest that because high conversation orientation families spend more time
discussing the cancer in general, there is greater opportunity for a patient’s support needs to be
brought up and expressed in these families than in families with a low conversation orientation.
Observations about Conformity Orientation
The results found in this study regarding the effects of conformity orientation are
particularly intriguing. Looking at the preliminary analyses, it appears that nearly all of the
relationships between conformity orientation and the support-related variables are directly
opposite those relationships between conversation orientation and the support-related variables.
This makes great sense when considering the significant negative relationship found in the
preliminary relationship between the conversation orientation and the conformity orientation.
When run in regressions with conversation orientation, however, significant main effects were
always found for conversation orientation only. There are a few possible explanations for this
observation. One explanation, which will be brought up again in the Limitations and Future
Research section of this paper may be the sample size. There may not have been enough power,
as a result of the small, relatively homogeneous sample, to find significant main effects of
70
conformity orientation. Had there been a larger and more diverse sample, the pattern that
appeared in the zero-order correlations may have carried through to the results of the regressions.
The lack of a larger, more diverse sample would also potentially explain the fact that no
significant relationship was found in either the preliminary analyses or the regressions between
conformity orientation and the degree of optimal matching of support, when the other significant
correlations would suggest there possibly should be. The majority of the participants in this
sample were both parents and spouses and thus probably one of the heads (if not the head) of
his/her household. Therefore, while a shared desire with their other family members to maintain
family harmony and hierarchy may have prevented the cancer patients from frequently
discussing their support needs, having the role of a leader in their family may have made the
degree of family conformity a less significant factor in determining optimal matching. This is
because these individuals have the power within the family to express dissatisfaction with
support or alternative approaches to support, even if they do not enjoy doing so, when they feel
like their needs are not being adequately met. A larger, more diverse sample including cancer
patients that were not heads of their households may have revealed a significant negative
correlation between conformity and optimal matching that would be in line with those negative
relationships found in the preliminary analyses between conformity orientation and the other
support-related variables.
The other possible explanation for the significant negative relationships between
conformity orientation and support-related variables not carrying over into the regression results
is that, perhaps, conversation orientation is the real driving force behind the effects of family
communication patterns on family behaviors. It may be, therefore, that the theoretical
conceptualization of the family communication pattern variables needs some refining in order to
71
most accurately reflect the presence and role of each orientation within the family. In the future,
theorists should spend some time examining the potential theoretical issue with the family
communication patterns.
If we consider the small sample size to be a reason for the lack of significant main effects
of conformity, then significant relationships found in the preliminary analyses are important to
look at because they offer insight into the relationships that may truly exist between conformity
and support-related variables that were inquired about in RQ1-RQ3. In the remained of this
section, therefore, results of the preliminary analyses will be looked at in order to begin to
understand the possible relationships that were found with this particular sample between
conformity orientation and support-related variables. Preliminary analyses showed a significant
negative correlation between conformity orientation and frequency of family discussion about
cancer. This negative relationship is surprising to some degree, given Koerner and Fitzpatrick’s
(2002) research suggesting that families higher in conformity emphasize family togetherness and
cohesiveness whereas families lower in conformity emphasize the strengthening of relationships
outside of the family. One would not suspect that individuals in families that focus their efforts
on relationships outside of the family unit would discuss the cancer with their family members
more than individuals in families that place familial relationships above all other relationships.
However, the negative relationship between level of family conformity orientation and frequency
of family discussion about cancer may be better understood by considering past research by
Koerner and Cvancara (2002) regarding the type of communication that occurs within low and
high family conformity orientations. Koerner and Cvancara (2002) found that communication in
families that are low in conformity is freer and more spontaneous than communication in
families that are high in conformity because individuals in low conformity orientation families

72
use more confirming statements and value-free reflections of others’ communication than
individuals in high conformity orientation families. Thus, the low conformity orientation families
may offer a more supportive, encouraging environment for individuals to freely discuss their
feelings and ideas concerning the cancer than the high conformity orientation families. The
negative relationship between family conformity orientation and family discussion of illness
found in the preliminary analyses could also be because of the value placed on the family
hierarchy. Koerner and Fitzpatrick (2002) explain that high conformity families value the idea
that children should be seen and not heard and, therefore, the head(s) of the household make(s)
the decisions regarding the well-being of the family. Since the majority of the sample identified
themselves as a parent and a spouse, perhaps those participants in the high conformity families
believe that their children need not be kept informed of all the details pertaining to their parents’
cancer, nor involved in making decisions regarding the cancer.
Preliminary analyses indicated significant negative relationships between conformity
orientation and emotional support and between conformity orientation and tangible support.
Preliminary analyses did not, however, indicate a relationship between conformity orientation
and informational support. These negative relationships between family conformity orientation
and emotional support and between family conformity orientation and tangible support are, to
some extent, surprising given Koerner and Fitzpatrick’s (2002) argument that high conformity
families value the family unit and family relationships above all else. Because of Koerner and
Fitzpatrick’s (2002) argument, one could suspect that individuals in these high conformity
families who are used to relying more on family members than on individuals outside the family
would perceive more support from their loved ones than individuals in low conformity families
that do not emphasize familial interdependence. The negative relationship between conversation
73
orientation and emotional support is better understood, however, if one considers the high
conformity family’s goals of maintaining homogeneity of attitudes and beliefs as well as the
established family hierarchy. Again considering Koerner and Cvancara’s (2002) finding that
communication in families that are low in conformity is freer and more spontaneous than
communication in families that are high in conformity, it is possible that the more a family
values conformity, the more taboo topics there are within the family and, therefore, the less
comfortable its members are being honest and free with their communication of feelings. A lack
of comfort with honest and free communication of feelings in families high in conformity could
make it more challenging for members of these families to be empathetic and/or emotionally
supportive towards one another, thus causing patients in these families to perceive less emotional
support. The negative correlation between conformity and emotional support could also be a
result of the sample. Almost all of the participants were women and the majority of these women
indicated that their primary support providers were their husbands. Koerner and Fitzpatrick
(2002) explain that high conformity families value a traditional, hierarchical family structure.
Perhaps, therefore, families that are higher in conformity adhere more to traditional family roles
where the husband and father figure is the “rock” of the family and, thus, less likely to show
vulnerability by showing emotion and providing emotional support.
The negative relationship between conformity orientation and tangible support found in
the primary analyses is more difficult to understand, especially given the negative relationship
between conformity and emotional support. It was thought that if emotional support was difficult
for individuals in high conformity families, perhaps they would compensate for this lack of
emotional support by engaging in less vulnerable types of support. Perhaps as mentioned above,
however, the more a family emphasizes conformity, the more emphasis it places on maintaining
74
the established family roles and, thus, the less comfortable and/or capable the primary support
provider is assisting in or taking over responsibilities that fall in the cancer patient’s domain.
The lack of a significant positive relationship between conformity orientation and
informational support is somewhat surprising seeing that Koerner and Cvancara (2002) found
that individuals in high conformity families engage in advice giving more than individuals in low
conformity families. Perhaps their predisposition to engage in advice giving is tempered in the
context of cancer because the family members do not feel knowledgeable enough about the
disease and what the patient is going through.
Finally, preliminary analyses indicated a significant negative correlation between
conformity orientation and a patient’s amount of talk about his/her support needs. Perhaps,
therefore, cancer patients in high conformity families are more hesitant to discuss their support
needs with their family members because they fear the requesting of certain types of support
(i.e., emotional support) would threaten the power structure and/or family roles that are already
established in the family. It could also be that cancer patients in high conformity families are less
likely to talk about their support needs than patients in low conformity families because they feel
that their family members are more likely to judge their perception of need if it is not in line with
the traditional attitudes and beliefs of the family unit. This explanation is in line with Koerner
and Cvancara’s (2002) finding that families high in conformity orientation engage in more
advice giving and evaluating of others’ behaviors based on their own attitudes and perspectives,
whereas families low in conformity engage in more confirming statements and value-free
reflections of others’ communication.
The above interpretation of the zero-order correlations suggest that being high in
conformity orientation may prevent a family from creating an environment that is conducive to
75
the type of communication and trust amongst family members that is required for successful
support exchange. Further research is needed with a larger, more diverse sample is needed to
confirm if this suspicion is correct or if the conceptualization of the family communication
patterns requires further theorizing.
Limitations and Future Research
One of the chief limitations of this study concerns the sample. Although 78 individuals
completed a portion of the survey, 25 of those people did not complete significant portions of the
survey related to the tests of hypotheses and, therefore, were not used in the analyses. As a result,
there was a relatively small sample size (N = 53). As previously mentioned, a lack of power as a
result of the smaller sample may account for the lack of significant main effects for the
conformity orientation on the dependent variables. It is important to note here that recruitment
was particularly challenging given that the limited available funds for the project prevented there
from being a monetary reward for participants and that local hospitals would not permit
recruitment at their social support group meetings given the number of research projects they
already had underway. Future research with a larger number of participants should be done to see
if similar significant results are found. Also, with a larger sample it may be possible to use the
four categories of family communication patterns that past studies (Orrego & Rodriquez, 2001;
Zhang, 2007) have derived using the mean splits on both the conformity and conversation
dimensions. Using the four category system would allow for a comparison between family types
to determine which combinations of conversation and conformity orientation allow for optimal
support. It would also allow for a more nuanced understanding of the connection between the
conversation and conformity orientations that was not possible in this particular study.
76
Another limitation of the sample is its lack of diversity. Nearly all of the participants
were women who identified themselves as both a wife and a mother in their immediate families.
This may be a result of two of the message boards used for recruiting being solely about breast
cancer. The results of this research, therefore, may not be as applicable for families that have
male cancer patients or whose cancer patients are not one of the heads of the household. Also, as
mentioned earlier, the fact that the majority of participants are heads of their household may have
played a role in the lack of significant main effects of conformity found in the study. Also, the
sample was significantly lacking in racial diversity with 94.3% of the respondents identifying
themselves as white. This is probably a result of the recruitment medium. Im, Chee, Tsai, Lin,
and Cheng (2005) explained that online help and support for cancer is used primarily by white,
highly educated individuals. Results of this research, therefore, may not be applicable for
families of different ethnic backgrounds. Future research should be done on a more diverse
sample so that results can extend to these other groups.
Because individuals that use online message boards are clearly getting some other
support outside of their family unit, their perception of within-family support and optimal
matching might be impacted by this external support. Also, individuals who use online support
tools may share certain individual or familial characteristics that influence the perceived amount
and quality of support available in their households. Future research should be done using
participants who do not have this additional external support so that results can be applied to a
larger population.
Another potential limitation is that, in order to increase sample size, individuals who
were in remission were also asked to complete the survey. For some participants, it has been
over 10 years since they have needed the sort of support that was required following their last

77
diagnosis and, therefore, they may not accurately recall the amount or type of support they felt
they were receiving at the time or how much they felt they discussed cancer and support with
their family members. As a result, retrospection error may have impacted some of the results.
Future research should try to examine individuals who are not yet in remission, and thus still in
great need of social support. It may be extremely beneficial to do a longitudinal study of cancer
patients directly following their cancer diagnoses to see how their support needs change and also
how their support providers’ abilities to provide support change with the passing of time.
How participants conceptualized the term conflict may be an additional limitation to the
study. When asked to identify whether the amount of conflict within their families had changed
since the diagnosis, they may have only been considering competitive conflict, or conflict that
was managed poorly or resulted in a fight, thus causing the majority of the participants to
unexpectedly report engaging in less conflict during a time of such stress and uncertainty. If it
was made evident to the participants that conflict referred to any situation involving misaligning
goals or a struggle over scarce resources, regardless of how the situation was handled
(constructively or not), it may be that they would have reported engaging in more conflict.
A final limitation to this study is that results were mostly based off of the participants’
views of their primary support providers in their family. In families larger than 2 people,
however, it is likely that important support is also coming from those other family members. For
a more thorough understanding of the kind of supportive atmosphere perceived by the patients as
being provided by their families, future research should examine all of the support providers in
the household. Future research might also survey the family members of the cancer patients so
that one can better examine how family communication patterns and conflict management styles
78
may cause discrepancies between the support that is being provided by the family members and
the support that the cancer patient perceives as being provided by the family members.
Despite these limitations, the significant findings of this study provide valuable insight
into the relationship between communication patterns, conflict styles, and social support in the
context of coping with cancer within the family. The remainder this thesis offers a summary of
this work and its greater importance for improving the well-being of cancer patients and their
loved ones.
Conclusion
This thesis sought to gain further insight into the capability of a family to be a positive,
supportive environment for a cancer patient while members try to cope with the cancer diagnosis
of their loved one. The relationships between family communication patterns, conflict
management styles, perceived social support and optimal matching of support were discovered
by having cancer survivors complete a self-report questionnaire in which they reported how their
family communicates, how they handle conflict within their family, and their perception of and
satisfaction with the social support they receive from their primary support provider.
Hierarchical regression modeling was used to analyze the data.
A cancer diagnosis is not only a life-altering event for the individual diagnosed, but
rather a life-altering event for that individual’s entire family unit. When an individual is
diagnosed with cancer, social support becomes a critical component of the relationship between
the family members. It is unreasonable to suspect, however, that all families are equally
equipped to provide what the cancer patients perceive as adequate support, especially while they
themselves are trying to cope with the fear and sadness that result from having a sick loved one.
Several factors relating to how individuals within a family unit inherently communicate with and
79
relate to one another can influence their ability to exchange support. A cancer patient’s
dissatisfaction with family support is not only a physical and psychological threat to his/her well-
being, but also an additional stressor in the family environment and another disappointment for
their already anxious family members. Ensuring that the support needs of the sick family
member are being met thus helps to both improve the well-being of the sick individual and
prevent stress and burnout on the part of the family members. When an individual is fighting
cancer, the presence of so many uncontrollable stressors related to illness in the family
environment makes this environment a breeding ground for conflict. It is important, therefore, to
try to ensure that the management of conflict within the family does not prevent the successful
exchange of support and that any inadequate offering of support does not become an additional
source of tension and potential conflict within the family during this stressful time.
Because both family communication patterns and conflict management styles are
significant influences on familial behavior and relationships, both were suggested to be
significant predictors of available support and optimal matching. As expected, significant results
were found for both of these constructs, suggesting that they were, in fact, useful constructs to
explore within this context. Preliminary analyses showed evidence of negative relationships
between level of family conformity orientation and the frequency of family discussion of cancer,
the amount of patient communication about his/her support needs, and the patient’s perceived
amount of emotional and tangible support. Further research should be done with a larger sample
size to gain further insight into the actual influence of conformity orientation on these variables.
Support was found for the hypotheses predicting positive relationships between the level of
family conversation orientation and each of the following dependent variables: frequency of
family discussion of cancer, the amount of patient communication about support needs, the
80
perception of the amount of available types of support, and the degree of optimal matching. The
prediction of a positive relationship between the collaboration and compromising conflict
management styles and a patient’s reported degree of optimal matching was also supported.
The support found for the hypotheses is important evidence that family environments
conducive to frequent open and clear communication are most suitable for providing substantial
support that a cancer patient deems satisfying. In other words, during this time of heightened
uncertainty and fear, constructive and consistent family communication is critical to meet the
demanding needs of the cancer patient and, consequently, decrease the potential for additional
strain within the family thus preserving the well-being of the all of the family members. The
findings regarding conflict management is also particularly important because they emphasize
that engaging in constructive conflict is an important tool for gaining experience and skill at
communicating in a way that will allow for optimal support exchange.
The findings of this research highlight the importance of making sure that medical staff
and professionals are doing more than just treating the physical symptoms of cancer. It can not
be assumed that families of cancer patients inherently have the communication tools needed to
be successful support providers during such a vulnerable time. Also, the potential threat to the
patient and his/her family members’ well-being that can result from inadequate supportive
exchange can not be overlooked. Medical staff and professionals must, therefore, not only
concern themselves with providing patients with the best possible medical treatment, but also
with making sure patients’ families get educated about the communication and conflict
management strategies that can be used to provide the most supportive and constructive home
environment possible. An individual’s cancer diagnosis puts the well-being of every family

81
member at risk and, therefore, every step must be taken to ensure that the environment at home is
both positive and supportive.
82
REFERENCES
Abbey, A., Abramis, D. J., & Caplan, R. D. (1985). Effects of different sources of social support
and social conflict on emotional well-being. Basic and Applied Social Psychology, 6(2),
111-129.
Albrecht, T.L., Burleson, B.R., & Goldsmith, D. (1994). Supportive communication. In M. L.
Knapp, & G. R. Miller (Eds.), Handbook of interpersonal communication (rev. ed., p.
419-449). Newbury Park, CA: Sage.
Barrera, M., Chassin, L. & Rogosch, F. (1993). Effects of social support and conflict on
adolescent children of alcoholic and nonalcoholic fathers. Journal of Personality and
Social Psychology, 64(4), 602-612.
Barrera, M., Sandler, I.N. & Ramsey, T.B. (1981). Preliminary development of a scale of social
support: Studies on college students. American Journal of Community Psychology, 9,
435-447.
Blanchard, C.G., Albrecht, T.L., Ruckdeschel, J.C., Grant, C.H., & Hemmick, R.M. (1995). The
role of social support in adaptation to cancer and to survival. Journal of Psychosocial
Oncology, 13(1-2), 75-95.
Chaffee, S.H., McLeod, J.M., & Atkin, C.K. (1971). Parental influences on adolescent media
use. American Behavioral Scientist, 14, 323-340.
Cobb, S. (1976). Social support as a moderator of life stress. Psychosomatic Medicine, 38, 300-
314
83
Cutrona, C. & Russell, D. (1990). Social Support: An Interactional View. In B. Sarason & G.
Pierce (Eds.), Type of social support and specific stress: Toward a theory of optimal
matching (p. 319-366). New York: Wiley.
Dumlao, R. & Botta, R.A. (2000). Family communication patterns and the conflict young adults
use with their fathers. Communication Quarterly, 48(2), 174-189.
Eggert, L.L. (1987). Support in the family. In T. Albrecht & M. Adelman (Eds.), Communicating
social support (p. 240-254). Newbury Park, CA: SAGE Publications.
Ell, K. (1996). Social networks, social support and coping with serious illness: The family
connection. Social Science and Medicine, 42(2), 173-183.
Elwood, T. & Schrader, D. (1998). Family communication patterns and communication
apprehension. Journal of Social Behavior and Personality, 13(3), 493-502.
Gil, S., & Gilbar, O. (2001). Hopelessness among cancer patients. Journal of Psychosocial
Oncology, 19(1), 21-33.
Glasdam, S., Jensen, A.B., Madsen, E.L., & Rose, C. (1996). Anxiety and depression in cancer
patients’ spouses. Psycho-oncology, 5, 23-29.
Hagerty, B. M. & Williams, A. R. (1999). Sense of belonging, social support, conflict, and
loneliness on depression. Nursing Research, 48(4), 215-219.
Im, E., Chee, W., Tsai, H., Lin, L., Cheng, C. (2005). Internet cancer support groups. Cancer
Nursing, 28(1), 1-7
Kahn, R. L. (1979). Aging and social support. In M. W. Riley (Ed.), Aging from Birth to Death:
Interdisciplinary Perspectives (p. 77-91). Boulder, CA: Westview Press.
84
Kenen, R., Ardern-Jones, A., & Eeles, R. (2004). We are talking, but are they listening?
Communication patterns in families with a history of breast/ovarian cancer (HBOC).
Psycho-Oncology, 13, 335-345.
Krause, N. (1987). Chronic financial strain, social support, and depressive symptoms among
older adults. Psychology and Aging, 2(2), 185-192.
Koerner, A.F. & Cvancara, K.E. (2002). The influence of conformity orientation on
communication patterns in family conversations. Journal of Family Communication,
2(3), 133-152.
Koerner, A.F. & Fitzpatrick, M. (1997). Family type and conflict: The impact of conversation
orientation and conformity orientation on conflict in the family. Communication Studies,
48, 59.
Koerner, A.F. & Fitzpatrick, M. (2002). Toward a theory of family communication.
Communication Theory, 12(1), 70-91.
Koesten, J. (2004). Family communication patterns, sex of subject and communication
competence. Communication Monographs, 71(2), 226-244.
Major, B., Cooper, M. L., Zubek, J. M., Cozzarelli, C., & Richards, C. (1997). Mixed Messages:
Implications of social conflict and social support within close relationships for
adjustment to a stressful life event. Journal of Personality and Social Psychology, 72(6),
1349-1363.
MaloneBeach, E. E. & Zarit, S. H. (1995). Dimensions of social support and social conflict as
predictors of caregiver depression. International Psychogeriatrics, 7(1), 25-38.

85
Manne, S. & Schnoll, R. (2001). Measuring supportive and unsupportive responses during
cancer treatment: A factor analytical assessment of the partner responses to cancer
inventory. Journal of Behavioral Medicine, 24(4), 297-321.
Martire, L. M., Lustig, A.P., Schulz, R., Miller, G.E., & Helgeson, V.S. (2004). Is it beneficial to
involve a family member? A meta-analysis of psychosocial interventions for chronic
illness. Health Psychology, 23(6), 599-611.
Moos, R. H., & Schaefer, J. A. (1984). The crisis of physical illness: An overview and
conceptual approach (Vol. 2, pp. 3-23). New York: Plenum.
Noller, P., Feeney, J.A., Sheehan, G., & Peterson, C. (2000). Marital conflict patterns: Links
with family conflict and family members’ perceptions of one another. Personal
Relationships, 7(1), 71-94.
Norbeck, J. S., Lindsey, A. M., & Carrieri, V. L. (1987). Further development of the Norbeck
Social Support Questionnaire: Normative data and validity testing. Nursing Research,
32(1), 4-10.
Orrego, V.O. & Rodriguez, J. (2001). Family communication patterns and college adjustment:
The effects of communication and conflictual independence on college students. Journal
of Family Communication, 1(3), 175-189.
Piko, B. (1998). Social support and health in adolescence: A factor analytical study. British
Journal of Health Psychology, 3, 333-344.
Rahim, M. A. (1983). A measure of styles of handling interpersonal conflict. Academy of
Management Journal, 26, 368-376.
Revenson, T. A. (2004). Social support and marital coping with chronic illness. Annals of
Behavioral Medicine, 16(2), 122-130.
86
Ritchie, L. D. & Fitzpatrick, M. (1990). Family communication patterns. Communication
Research, 17(4), 523-544.
Robinson, J. D. & Turner, J. (2003). Impersonal, interpersonal, and hyperpersonal social support:
Cancer and older adults. Health Communication, 15(2), 227-234.
Sarason, I. G., Levine, H. M., Basham, R. B., & Sarason, B. R. (1983). Assessing social support:
The Social Support Questionnaire. Journal of Personality and Social Psychology, 44(1),
127-139.
Smetana, J. G., Yau, J. & Hanson, S. (1991). Conflict resolution in families with adolescents.
Journal of Research on Adolescents, 1(2), 189-206.
Taylor, S. E., Falke, R. L., Shoptaw, S. J., & Lichtman, R. R. (1986). Social support, support
groups, and the cancer patient. Journal of Consulting and Clinical Psychology, 54(5),
608-615.
Thompson, S. & Pitts, J.S. (1992). In sickness and in health: Chronic illness, marriage, and
spousal caregiving. In S. Spacapan & S. Oskamp (Eds.), Helping and Being Helped (pp
115-151). Newbury Park, CA: Sage
Turner, J. W., Grube, J. A., & Meyers, J. (2001). Developing an optimal match within online
communities: An exploration of CMC support communities and traditional support.
Journal of Communication, 51(2), 231-251.
Zang, Q. (2007). Family communication patterns and conflict styles in Chinese parent-child
relationships. Communication Quarterly, 55(1), 113-128.
87
APPENDIX A
SOLICITATION LETTER
Hello,
I am a graduate student at the University of Georgia studying Speech Communication. I
am particularly interested in communication related to health and families. I am in my second
year of my Master’s program and, therefore, working on my thesis. My project is entitled, “How
Family Communication Patterns and Conflict Management Affect Cancer Patients’ Support
Satisfaction and Availability.” I am examining the communication styles and strategies in
families in which one individual is fighting cancer. More specifically, I am looking at how those
fighting cancer communicate/discuss their support needs with their loved ones. The future goal
of this research is to obtain the information necessary to improve the type and quality of support
that is offered to cancer patients, and to ensure that the type of support that they want/need is the
type that their family and loved ones are able to provide.
In order to carry out my research, I need individuals who are currently fighting cancer to
fill out a questionnaire about how they communicate with their families, particularly in regards
to the illness. Therefore, I am asking for your assistance. Any individuals over the age of 18
who have, at one time, been diagnosed with cancer and who have at least one other individual
in their immediate families are welcome and encouraged to click on the link below, read the
consent form explaining the study and questionnaire in more detail, and then fill out and submit
the anonymous questionnaire online. You are free to contact me if you have any
questions/concerns regarding your decision to participate. Further contact information is
available on the informational letter at the beginning of the survey (you will have the opportunity
to read through the letter and make your decision before you are asked to look at/answer any of
the questions).
Many of my loved ones have fought and continue to fight cancer and for this reason I am
extremely passionate about my project. I believe that my work could potentially make a
significant difference and, therefore, I would love the opportunity to get a decent number of
individuals involved. Thank you so much in advance for your time and consideration.
Link to the questionnaire:
http://www.surveymonkey.com/s.aspx?sm=3eydO24u5OJ6qDwA_2bR_2bmOg_3d_3d

88
APPENDIX B
LETTER OF INFORMED CONSENT
To Whom It May Concern,
I am a graduate student in the department of Speech Communication at the University of Georgia
working under the direction of Dr. Jennifer Samp (706-542-4893, [email protected]). I invite you
to participate in a research study titled "HOW FAMILY COMMUNICATION PATTERNS
AND CONFLICT MANAGEMENT AFFECT CANCER PATIENTS’ SUPPORT
SATISFACTION AND AVAILABILITY." Your participation is entirely voluntary. You can
refuse to participate or stop taking part without giving any reason, and without penalty. You can
ask to have all of the information about you returned to you, removed from the research records,
or destroyed.
The reason for this study is to see if the different ways family members communicate with one
another and handle conflict influence the giving and receiving of support when one family
member has cancer. If you volunteer to take part in this study, you will be asked to do the
following things:
1) Answer questions about how your family communicates, how your family handles conflict,
and the amount and type of support available within your family which will take 20-40 minutes
While there are no direct benefits for participating in this study, you may gain a better
understanding of your support needs as a result of participating in this research. As the
researcher, I also hope to learn more about the impact of family communication and conflict
styles on cancer patient support.
No risk is expected but there is a slim chance that you may experience some psychological stress
when completing the questionnaire as a result of having to think about situations of conflict in
your family. These risks will be reduced in the following way: by the questionnaire refraining
from asking for detailed information about specific conflicts or instances of poor support-giving
within the family.
Please note that Internet communications are insecure and there is a limit to the confidentiality
that can be guaranteed due to the technology itself. However, once we receive the completed
surveys, the surveys will be anonymous, meaning that no one will be able to trace your responses
back to me. If you are not comfortable with the level of confidentiality provided by the Internet,
please feel free to print out a copy of the survey, fill it out by hand, and mail it to me at the
address given below, with no return address on the envelope.
Thank you for your consideration! If you have any questions about this research project, please
feel free to call me at (706) 542-4893 or send an e-mail to [email protected]. Questions or
89
concerns about your rights as a research participant should be directed to The Chairperson,
University of Georgia Institutional Review Board, 612 Boyd GSRC, Athens, Georgia 30602-
7411; telephone (706) 542-3199; email address [email protected].
90
APPENDIX C
QUESTIONNAIRE
Please think about your immediate family and how you typically go about talking to one
another and then answer the following questions.
1.) My family has established rules that everyone is expected to obey.
1 2 3 4 5
Never
2.) If the head(s) of the house don’t approve of it, they don’t want to know about it.
1 2 3 4 5
Never Frequently
3.) We often talk as a family about things we have done during the day.
1 2 3 4 5
Never Frequently
4.) My family encourages me to express my feelings.
1 2 3 4 5
Never Frequently
5.) In our home, the head(s) of the household usually have the last word.
1 2 3 4 5
Never Frequently
6.) I can tell my family members almost anything.
1 2 3 4 5
Never Frequently
91
7.) The head(s) of the house often say something like “My ideas are right and you should not
question them.”
1 2 3 4 5
Never Frequently
8.) The head(s) of my household say something like “You should give in on arguments rather
than risk making people mad.”
1 2 3 4 5
Never Frequently
9.) I really enjoy talking to my family members, even when we disagree.
1 2 3 4 5
Never Frequently
10.) My family members become irritated with my views if they are different from theirs.
1 2 3 4 5
Never Frequently
11.) The head(s) of my household say something like “There are some things that just shouldn’t
be talked about.”
1 2 3 4 5
Never Frequently
12.) In our family, we often talk about our plans and hopes for the future.
1 2 3 4 5
Never Frequently
13.) I usually tell the people in my family what I am thinking about things.
1 2 3 4 5
Never Frequently
14.) In our family we often talk about our feelings and emotions.
1 2 3 4 5
Never Frequently

92
15.) The people in my family like to hear my opinion, even when they don’t agree with me.
1 2 3 4 5
Never Frequently
16.) The head(s) of the household feel that it is important to be the boss.
1 2 3 4 5
Never Frequently
17.) How often would you say your family spends talking about the illness and issues
surrounding the illness?
1 2 3 4 5
Never Frequently
18.) How often would you say your family spends talking about each other’s support needs?
1 2 3 4 5
Never Frequently
Now, please think of the most important person in your immediate family as you are
dealing with your illness.
19.) How is this person related to you? ____________________________
Please continue to think of this person as you answer the following questions:
Since the diagnosis, how often has this person. . .
20.) Told you what they did in a stressful situation that was similar to
one you were experiencing?
1 2 3 4 5
Never Frequently
21.) Been right there with you (physically) during this stressful situation?
1 2 3 4 5
Never Frequently
22.) Suggested some action that you should take in dealing with a problem you were having
related to the illness/coping with the illness?
1 2 3 4 5
Never Frequently

93
23.) Told you you were okay just the way you are?
1 2 3 4 5
Never Frequently
24.) Given you information that made a difficult situation clearer and easier to understand?
1 2 3 4 5
Never Frequently
25.) Comforted you by showing you physical affection?
1 2 3 4 5
Never Frequently
26.) Helped you understand why you didn't do something well?
1 2 3 4 5
Never Frequently
27.) Provided you with some transportation?
1 2 3 4 5
Never Frequently
28.) Listened to you talk about your private feelings?
1 2 3 4 5
Never Frequently
29.) Told you who you should see for assistance with a problem that you were having relating to
the illness/coping with the illness?
1 2 3 4 5
Never Frequently
30.) Told you they felt very close to you?
1 2 3 4 5
Never Frequently
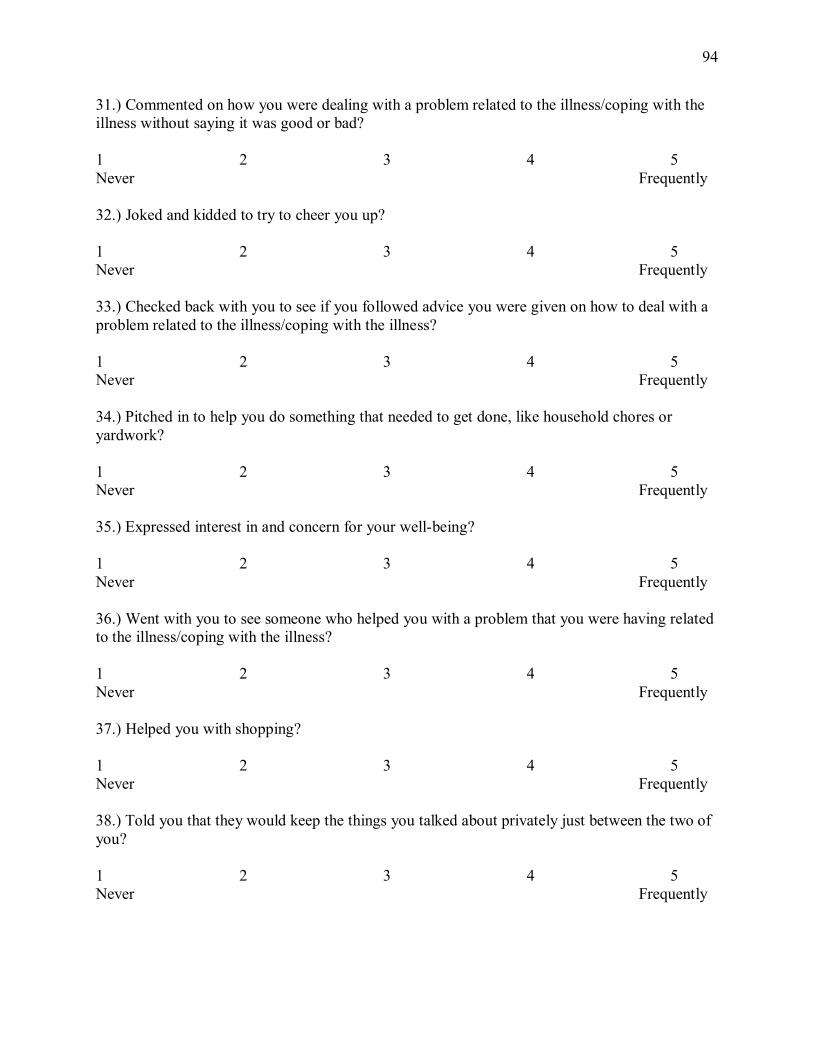
94
31.) Commented on how you were dealing with a problem related to the illness/coping with the
illness without saying it was good or bad?
1 2 3 4 5
Never Frequently
32.) Joked and kidded to try to cheer you up?
1 2 3 4 5
Never Frequently
33.) Checked back with you to see if you followed advice you were given on how to deal with a
problem related to the illness/coping with the illness?
1 2 3 4 5
Never Frequently
34.) Pitched in to help you do something that needed to get done, like household chores or
yardwork?
1 2 3 4 5
Never Frequently
35.) Expressed interest in and concern for your well-being?
1 2 3 4 5
Never Frequently
36.) Went with you to see someone who helped you with a problem that you were having related
to the illness/coping with the illness?
1 2 3 4 5
Never Frequently
37.) Helped you with shopping?
1 2 3 4 5
Never Frequently
38.) Told you that they would keep the things you talked about privately just between the two of
you?
1 2 3 4 5
Never Frequently
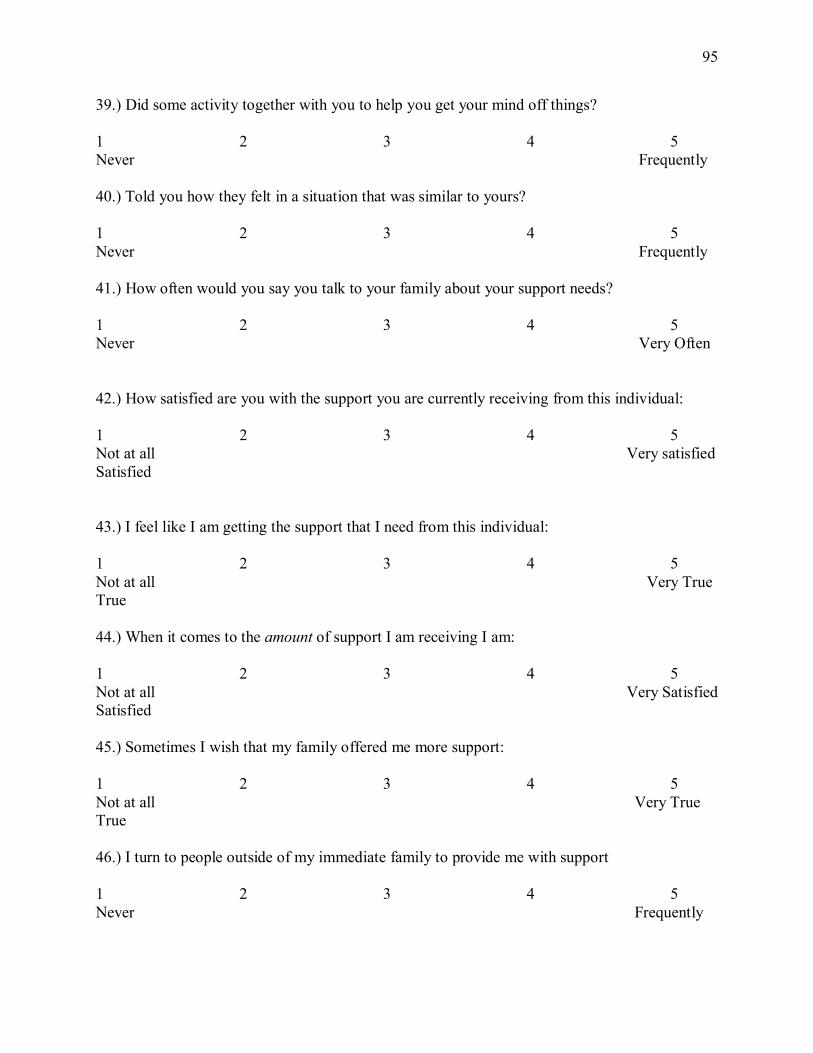
95
39.) Did some activity together with you to help you get your mind off things?
1 2 3 4 5
Never Frequently
40.) Told you how they felt in a situation that was similar to yours?
1 2 3 4 5
Never Frequently
41.) How often would you say you talk to your family about your support needs?
1 2 3 4 5
Never Very Often
42.) How satisfied are you with the support you are currently receiving from this individual:
1 2 3 4 5
Not at all Very satisfied
Satisfied
43.) I feel like I am getting the support that I need from this individual:
1 2 3 4 5
Not at all Very True
True
44.) When it comes to the amount of support I am receiving I am:
1 2 3 4 5
Not at all Very Satisfied
Satisfied
45.) Sometimes I wish that my family offered me more support:
1 2 3 4 5
Not at all Very True
True
46.) I turn to people outside of my immediate family to provide me with support
1 2 3 4 5
Never Frequently
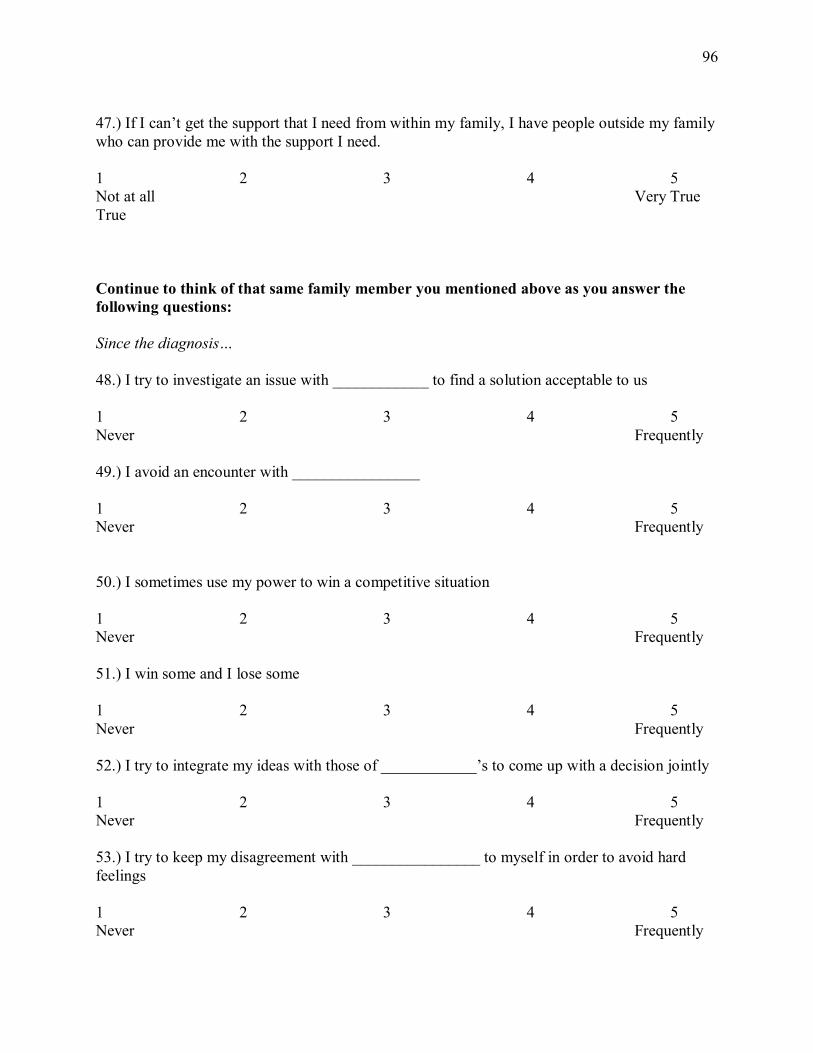
96
47.) If I can’t get the support that I need from within my family, I have people outside my family
who can provide me with the support I need.
1 2 3 4 5
Not at all Very True
True
Continue to think of that same family member you mentioned above as you answer the
following questions:
Since the diagnosis…
48.) I try to investigate an issue with ____________ to find a solution acceptable to us
1 2 3 4 5
Never Frequently
49.) I avoid an encounter with ________________
1 2 3 4 5
Never Frequently
50.) I sometimes use my power to win a competitive situation
1 2 3 4 5
Never Frequently
51.) I win some and I lose some
1 2 3 4 5
Never Frequently
52.) I try to integrate my ideas with those of ____________’s to come up with a decision jointly
1 2 3 4 5
Never Frequently
53.) I try to keep my disagreement with ________________ to myself in order to avoid hard
feelings
1 2 3 4 5
Never Frequently
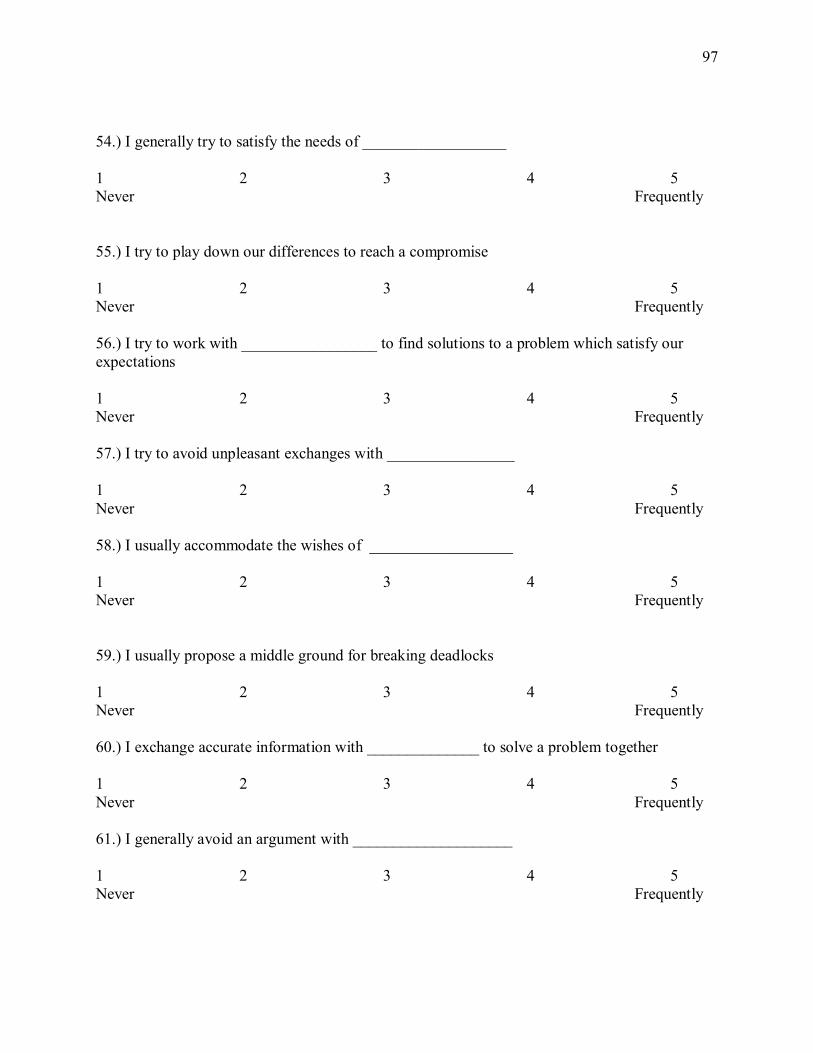
97
54.) I generally try to satisfy the needs of __________________
1 2 3 4 5
Never Frequently
55.) I try to play down our differences to reach a compromise
1 2 3 4 5
Never Frequently
56.) I try to work with _________________ to find solutions to a problem which satisfy our
expectations
1 2 3 4 5
Never Frequently
57.) I try to avoid unpleasant exchanges with ________________
1 2 3 4 5
Never Frequently
58.) I usually accommodate the wishes of __________________
1 2 3 4 5
Never Frequently
59.) I usually propose a middle ground for breaking deadlocks
1 2 3 4 5
Never Frequently
60.) I exchange accurate information with ______________ to solve a problem together
1 2 3 4 5
Never Frequently
61.) I generally avoid an argument with ____________________
1 2 3 4 5
Never Frequently
98
62.) I give in to the wishes of _________________
1 2 3 4 5
Never Frequently
63.) I negotiate with _______________ so that a compromise can be reached
1 2 3 4 5
Never Frequently
64.) I try to bring all our concerns out in the open so that the issues can be resolved in the best
possible way
1 2 3 4 5
Never Frequently
65.) I usually hold on to my solution to a problem
1 2 3 4 5
Never Frequently
66.) I use "give and take" so that a compromise can be made
1 2 3 4 5
Never Frequently
67.) I collaborate with _____________ to come up with decisions acceptable to us
1 2 3 4 5
Never Frequently
68.) I use my influence to get my ideas accepted
1 2 3 4 5
Never Frequently
69.) I try to work with _______________for a proper understanding of a problem
1 2 3 4 5
Never Frequently
70.) I use my authority to make a decision in my favor
1 2 3 4 5
Never Frequently
99
71.) I often go along with the suggestions of ____________________
1 2 3 4 5
Never Frequently
71.) I attempt to avoid being "put on the spot" and try to keep my conflict with _____________
to myself
1 2 3 4 5
Never Frequently
72.) I try to satisfy the expectations of _________________
1 2 3 4 5
Never Frequently
73.) I usually avoid open discussion of my differences with ______________
1 2 3 4 5
Never Frequently
74.) I use my expertise to make a decision in my favor
1 2 3 4 5
Never Frequently
75.) I give some to get some
1 2 3 4 5
Never Frequently
76.) I try to stay away from disagreement with _______________
1 2 3 4 5
Never Frequently
77.) I am generally firm in pursuing my side of the issue
1 2 3 4 5
Never Frequently
78.) I try to find a middle course to resolve an impasse
1 2 3 4 5
Never Frequently
100
79.) Before the diagnosis, I handled conflict:
1 2 3 4 5
Very differently Exactly the Same
80.) Since the diagnosis I engage in:
______________ Less Conflict __________ The same amount ___________ More Conflict
Of Conflict
Please tell us about yourself:
Your gender (circle): Male or Female
Your age:________
The age of your primary support provider _________.
The sex of your primary support provider: Male or Female
How long have you know your primary support provider: __________________.
The racial/ethnic identification that best describes you is:_________________________
How would you define the role you play in your immediate family (please circle all that apply):
Husband Father Daughter Sister Other_____________
Wife Mother Son Brother
When were you last diagnosed with cancer? ____________________________.
THANK YOU FOR YOUR PARTICIPATION