how positive pressure ventilation affects vital organs functions shao-hsuan hsia, md. pediatric...
TRANSCRIPT

How Positive Pressure Ventilation Affects Vital Organs Functions
Shao-Hsuan Hsia, MD.Pediatric Critical Care Medicine, Chang Gung Children’s Hospital

Why is this topic important?
One’s meal is another one’s poisonRespiration affects several major body compartments: thorax, abdomen, cranium, muscle tissue spaces.Take care of the whole body, not only one organ systemAdverse effects of mechanical ventilation existRespiratory system dysfunction is potentially a cause of multiple organ dysfunction syndrome (MODS)

How Positive Pressure Ventilation Affect Vital Organs Functions
Respiratory system-cardiovascular system Respiration as exercise Increased lung volume Intrathoracic pressure Respiratory acidosis/alkalosis, inhalation gases
Respiratory system-vital organs Brain Liver Kidney
Oxygen toxicity

DO2=CO(1.34HbSaO2+0.003PaO2)

Increased Lung VolumeVt<12ml/kg: vagal withdrawaltachycardiaVt>15ml/kg: sympathetic withdrawal bradycardiaHumoral factors: cyclo-oxygenase inhibition, NOMechanical compression of LVPulmonary vascular resistanceVentricular interdependence

Pulmonary Vascular Resistence

Ventricular interdependence
*Positive pressure ventilation can restrict RV volume and decrease ventricular interdependence effects
*Ventricular interdependence can be worsened by pulmonary hypertension

Intrathoracic Pressure
Venous returnRV preload and afterloadLV preload and afterloadPulmonary resistence

Systemic Venous Return(RV Preload)
0Systemic Venous Return
Max
RAP
Spontaneous Breathing
PPV increases RAP
Volume expansion shifts the line to right

右心與正壓呼吸
RA
RV
Vena Cava
胸腔內 壓力上升PA
正壓呼吸器壓力
正壓呼吸器壓力

左心與正壓呼吸
LA
LV
Ao
Lung Lung正壓呼吸器壓力
正壓呼吸器壓力
Thoracic pump augmentation

左心與正壓呼吸

正壓呼吸與肺血管阻力
9.4
4.6
9.4
3.8
1.6
3.7
2.32.9
2.4
0
2
4
6
8
10
Paw PVR CI
Pre
HFJV
Post
* *
* ** *
Effect of HFJV on PAH
Meliones Circ 1991
*P<0.01 vs. HFJV
(n=13)

血液酸鹼值與肺血管阻力
0
5
10
15
20
25
30
35
40
CTL
Hypoxia
Resp alkalosis
Meta alkalosis
Hypoxia
**
Lyrene RK 1985
PV
R
*P<0.01 vs hypoxia
Effect of pH on PVR

呼吸氣體與肺血管阻力
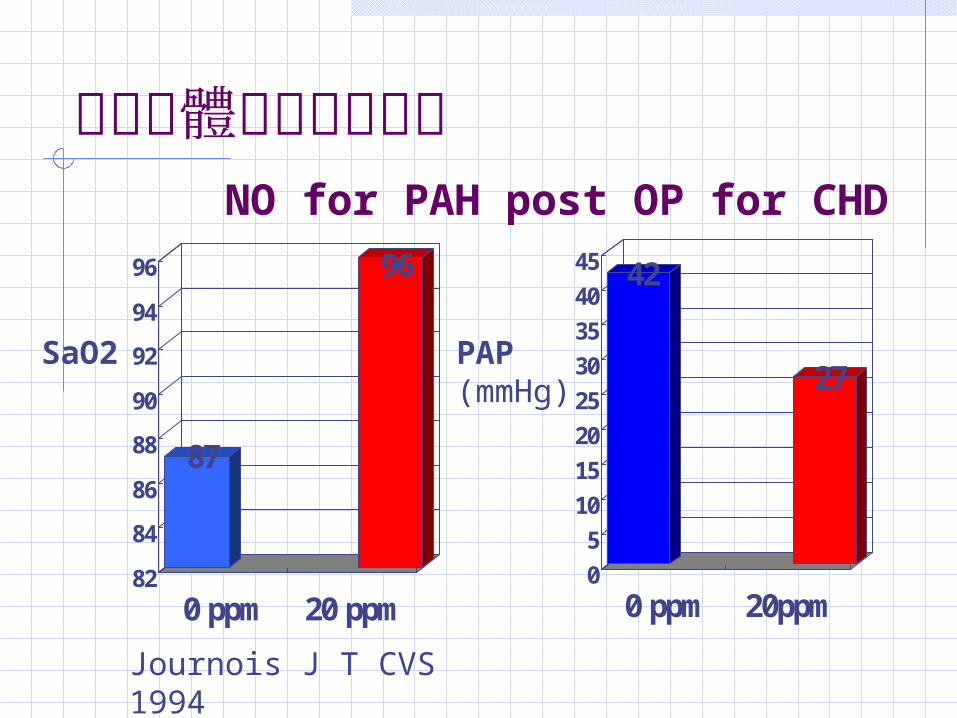
呼吸氣體與肺血管阻力
42
27
0
5
10
15
20
25
30
35
40
45
0 ppm 20ppm
PAP (mmHg)
87
96
82
84
86
88
90
92
94
96
0 ppm 20 ppm
SaO2
Journois J T CVS 1994
NO for PAH post OP for CHD
How Positive Pressure Ventilation Affect Vital Organs Functions
Respiratory system-cardiovascular system Increased lung volume Intrathoracic pressure Respiratory acidosis/alkalosis, inhalation
gases
Respiratory system-vital organs Brain Liver Kidney
Oxygen toxicity

腦血流量監測
010
20304050
6070
Reduced Normal Elevated
GR/MDSD/PVSDead
CBF Groups
% of Patients
CBF vs. Glasgow outcome score: 3 months post injuryRobertson et al. 1992

Positive Pressure Ventilation and Cerebral Perfusion
Cerebral perfusion pressure=mean arterial pressureintracranial pressure CPP=MAP ICP (CVP when CVP>ICP)
PEEP ITP, VR, CVP Normal ICP: PEEP>10cmH2O ICP Increased ICP: PEEP<ICP is safe
McGuire et al 1997
PaCO2

PEEP vs. normal ICP
0
2
4
6
8
10
12
14
16
0 5 10 15PEEP
mm
Hg
79
80
81
82
83
84
85
86
87
ICP
CPP
* *
*p<0.05

PEEP vs. elevated ICP
0
5
10
15
20
25
30
35
0 5 10 15PEEP
mm
Hg
88
88.5
89
89.5
90
90.5
91
ICP
CPP

正壓呼吸與腦血流量
-0.1
-0.05
0
0.05
0.1
0.15
PIP off PIP on
CBV
HbO2
DOHb
Volum
e change(ml/100m
l brain)
Palmer, Acta Paediatr 1995

Impaired Pressure-Flow Autoregulation
Maximal Normal MaximalVasodilation Autoregulation Vasoconstriction
0 25 50 75 100 125 150 CPP (mmHg)
CBFUnexpected Ischemia
Unexpected Hypermia
Normal AutoregulationDisrupted AutoregulationPartial Disrupted Autoreg

經顱骨超音波都卜勒監測 -TCD
40 35 30 25 PaCO2
ICP PulsatilityIndex (PI)
Hyperventilation Vasoconstriction (Ischemia): ICP but PI

腦代謝率 CMRO2之監測
CMRO21.81.51.20.90.60.30
0 0.4 0.8 1.2
2.0
4.0
6.0
CBF(ml/gm/min)
AV
DO
2(m
ol/ml)
ischemia
infarction hyperemia
normal
hypo- perfusion
Robertson J of Neurosurg 1989

Positive Pressure Ventilation and Liver Function
Patients with sepsis, trauma and ARDS usually combine liver dysfunction—endotoxin, shock, hypoxemia and DICCO hepatic artery and portal vein blood flowITPhepatic vein pressure (Phv)hepatic flowDescending diaphragm compression intrahepatic closing pressure (Pc) sinusoidal cell-blood contact timePeak-inspiratory RAP hepatic blood flow pressure gradientabdominal pressure Ppv, and Pc

Pha
Rha
Ppv
Rpv
Ps Pc Phv
Pra
Diaphragm
Pab
Qha
Qpv
QLQvc
Matushak et al J Crit Care 1989
Hepatic blood flow interactions

0
20
40
60
80
100
IPPV1 PEEP1 PEEP2 IPPV2
ml/k
g/m
in CO
QLemf*P<0.001
+p<0.05
N=6
Matuschak et al. J Appl Physiol 1987

Positive Pressure Ventilation and Renal Functions
PPV may decrease CO and MAPThe partial occlusion of IVC increase renal vein pressure (RVP) and retention of Na and waterSympathetic nervous system/renin-angiotensin-aldosterone system/atrial natriuretic factor (ANF) system.

Positive Pressure Ventilation and Renal Functions
venous returndeactivate low pressure baroreceptor reflexesrenal blood flow, reninvenous return ANFNa and water retention

Renal Blood Flow vs. PEEP
-60
-40
-20
0
20
40
60
RVP
CO
RBF
ZEEP PEEP 10
RVP 10 PEEP 20
RVP 20
***
* **
Masahiro et al. CCM 1988

PEEP and Hormones
0
50
100
150
200
250
300
ANF PRAx20 Aldo NEx100 Epi
ZEEP
PEEP
Pierre et al. J Appl Physiol 1991
P<0.0001
P<0.02

PEEP and Natriuresis
0
50
100
150
200
250
300
Urine FeNa%x100 GFR SBP
ZEEP
PEEP
Pierre et al J Appl Physiol 1991
P<0.0003
P<0.0002

Schuller et al. Chest 1991, 100(4): 1068
-4
-3
-2
-1
0
1
2
3
4
5
6
0 12 24 36 48 60 72TIME (HOURS)
TO
TA
L I
/O (
L)
NON-SURVIVORS
SURVIVORS

Schuller et al. Chest 100(4): 1068, 1991
0
20
40
60
80
100
120
140
160
180
200
Survivors Non-survivors
Rat
e of
flui
d ac
cum
ulat
ion
(ml/h
r)
Survivors
Non-survivors
P=0.0005

Schuller et al. Chest 100(4): 1068, 1991

Conclusions (1)DO2 = CO (1.34 Hb SaO2 + 0.003PaO2)
Use heart-lung interactions Restrict airway pressure for RV failure Expand fluid volume to compensate venous
return Use positive pressure ventilation in LV
failure Optimize PEEPFRC to optimize PVR Avoid hypercapnea for pulmonary
hypertension

Conclusions (2)Avoid prolonged use of hyperventilation in IICPMonitor ICP and CPP vs. PEEPAvoid prolonged use of positive pressure ventilation in neonates with risk of ICHWatch liver function and coagulation factors Allow spontaneous (negative pressure) breath (IMV, SIMV)Watch fluid balance and NaUse constant flow in healthy lung

Mean Airway Pressure Decelerating Constant
Flow(l/sec)
AirwayPressure(cmH20)
MAP = Area Under Curve
PIP PIP
Gas Distribution