how psychological profiles differ in ss with varying eye...
TRANSCRIPT

1
Keynote Address:
How Psychological Profiles Differ
in Ss with Varying Eye Diagnoses
European Conference on Psychology and
Visual Impairment
Heidelberg, Germany
March 29-30, 2012

2
“Fashions” in Psychology
The era of tabula rasa (nurture lovers)
The eugenics movement (nature lovers)
The rise of psychoanalytic approaches (lovers)
Behaviorism and Skinner effects (reward lovers)
The influence of Spock (Star Trek lovers?)
Brain studies (head & science lovers)
Interactive effects (fickle lovers…)

3
A Bit of History
Diagnosis and etiology as possible determinants of
learning style in Ss with visual impairment
The “RLF” Wave: Technology, incubators & research
Retinoblastoma: Observations &findings
Cataracts, lenses and vision: Changes over years
Albinism: Culture and achievement
Neurobiology: Brain development, visual, tactile &
auditory acquisition of information

4
‡ See reference

5

6

7
Research Questions
Are there differences in the way people with visual
impairment learn, develop, behave?
Are these factors affected by eye diagnosis, etiology,
age of onset or learning modes?
What approaches promote best outcomes in people
with these diagnoses or impairments?
How can professionals who render assistance to people
with visual loss apply this knowledge?
8
Dimensions
Cognitive quotients and profiles
Measures of „intelligence‟ & limitations
Verbal and Performance subtest analyses
Academic
Reading, „riting & 'rithmetic scores (3R‟s)
Body and environmental imagery
Figures drawn, described, modeled in clay
Social/Adaptive
Data entry/analysis in process

9
Sampling Issues
Low incidence
“Smallest” major group of disabled students
Blind Ss comprise <15% of vi students
High variability in samples
Behavioral styles around vision
Finding participants: non-random samples
Those who are referred or willing
Risk of stereotyping

10
Quantitative View of Dataset
2, 401 participant assessments*
1,366 unique individuals
- 141 sighted controls
- 110 sleep study participants
*Differing measures by study and source
**N’s vary for dimensions & measures
up to 1,115 VI/NV Ss** included to date

11
Cognitive Measures
Early: Binet-based, M.A. approach
Hayes and Perkins adaptations for VI/NV
Then: Wechsler Scales, Verbal & Performance
Ss with vision, modifications & allowances
Ss without vision, reliance on verbal items
Tactile Assessment of Performance
Now: Profile analysis via an array of methods
Few specifically adapted for VI/NV groups

12
VIQ Contrasts, VI vs. NV/LP
70
75
80
85
90
95
100
Sighted
Norms
VI NV/LP
n = 348 n = 476
Mean SD
Sighted 100 15
VI 84.36 27.15
NV/LP 93.19 29.33
Significantly different
p < .001

13
Subtest Contrasts VI vs. NV/LP Wechsler Verbal Scale
0
2
4
6
8
10
12
14
VI
NV/LP
* p < .05
** p < .001 Scale
d S
co
re

14
Factors
Diagnosis
Original roster of diagnoses (107 entries)
Problems of grouping
Analyses of development by eye conditions
Etiology
Heredity and family history are relevant
Retina as brain extension (neurology)
Infection, accident, other causes
Congenital or Acquired
Age of onset has impact for latter group

15
Diagnostic Group 1
Retrolental Fibroplasia/Retinopathy of Prematurity
Retinoblastoma
Leber‟s Congenital Amaurosis
Other Retinal Disorders
Optic Atrophy
Optic Nerve Hypoplasia
‡ See reference

16
90
117
102
97
7782
60
70
80
90
100
110
120
Rlf/Rop Rb Leber's Retinal Opt Atr Opt Hypn = 294 n = 70 n = 20 n = 67 n = 81 n = 18
Diagnostic Group 1
Me
an
VIQ
Cognitive Findings: Group 1

17
Diagnostic Group 2
Albinism
Glaucoma
Micro/Anophthalmos
Cortical/Visualmotor/Perceptual
Exotropia/Esotropia/Strabismus

18
93 94
87
81
73
60
70
80
90
100
110
120
Albinism
n = 26
Glaucoma
n = 39
Micro/Ano
n = 29
Cort Bl
n = 42
Exo/Eso/Strab
n = 10
Diagnostic Group 2
Mean
VIQ
Cognitive Findings: Group 2

19
Diagnostic Group 3
Congenital/Acquired Cataracts
The Myopias
Cornea/Iris/Choroid/Uvea

20
7478
91
60
70
80
90
100
110
120
Cataract Myopia C.I.C.Un = 72 n = 25 n = 16
Mean
VIQ
Diagnostic Group 3
Cognitive Findings: Group 3

21
Comparing Ability
Significant variability in VIQ by diagnosis
ANOVA: F (17, 806) = 9.09, p < .001
Significant variability in AQ* by etiology
ANOVA: F (17, 691) = 9.73, p < .001
*AQ = Ability Quotient from several sources

22
Etiology Groups
n %
Prematurity 374 38.8
Other/Unknown 212 22.0
Heredity 200 20.7
Pre- & Peri- natal 103 10.7
Neurological 53 5.5
Accident 22 2.3
Total 964 100

23
AQ by Etiology
92
81
109
89
78
93
60
70
80
90
100
110
120
AQ

24
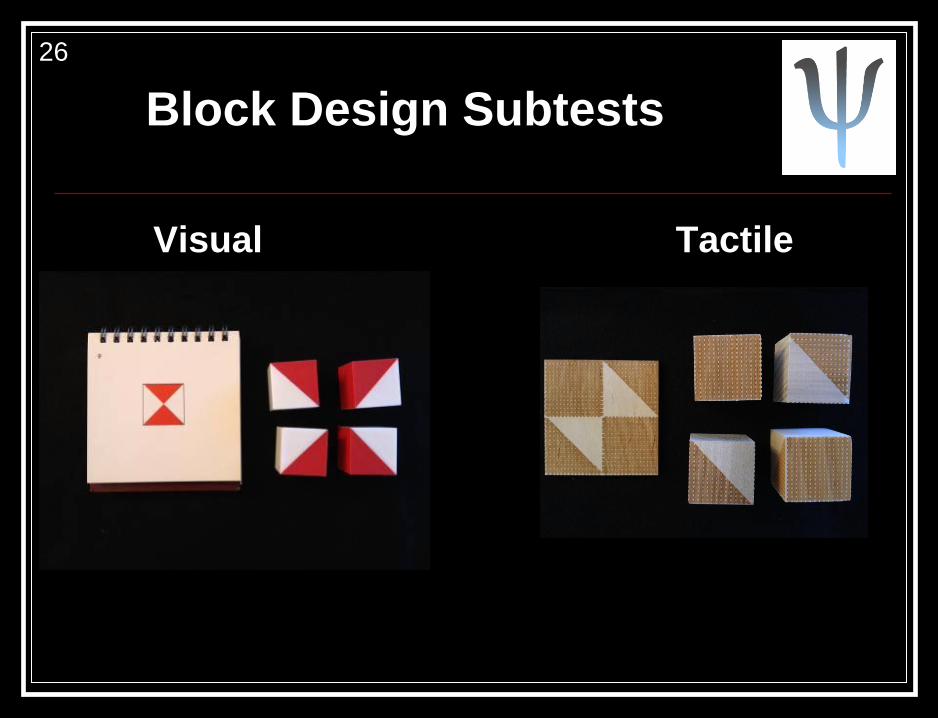
Performance Findings
Visual/Tactile Contrasts
Pictorial display: those with vision
Figures, graphs, other visual methods
Tactile graphic display: NV/LP & Low Vision
Meaningful ways of accessing information
Application for assessment/research
Block Design as example

25
PIQ by Acuity, VI Group
6975
84
92
84
40
50
60
70
80
90
100
110
120
PIQ
20/1000
– 20/501 20/500
– 20/351
20/350
– 20/201
20/200
– 20/101
20/100
– 20/40
n = 9 n = 9 n = 18 n = 32 n = 23
26
Block Design Subtests
Visual Tactile

27
Visual vs. Tactile Block Design by Age
0
5
10
15
20
25
30
35
Raw
Sco
re
Vis
BD
Tact
BD
1 17 13
2 24 17
3 20 36
4 11 61
5 8 66
6 4 37

28
Male student @
residential school
Dx: ROP
C.A.: 20-2
O.S.: no vision
O.D.: 20/240 distance
Reads J10 at 3” near
Couldn‟t see graphics
(black & white) for PA

29
WPPSI
Female
C.A.: 5-10
Dx: Albinism
O.U.: 20/200

30

31
Environmental & Body Image
Measures
Goodenough-Harris Drawing Test
Verbal Draw-A-Person (VDAP)
Expansion to person, house, car
Clay Models: Person, house, car
Analyses
No significant variability by age
Clinical inquiry: Provides developmental insight
Insufficient data for comparisons by diagnosis
‡ See reference

32
Goodenough – Harris Drawings
Female
8 years old
Achromatopsia
Acuity: 20/200

33
Clay Models, Rb
Rb Male
Age 17 ½
Rb Female
Age 15½ Rb Female
Age 11½

34
Clay Models ROP
ROP Male Age 15
ROP Female
Age 15½
ROP Female
Age 12¾ ROP Male
Age 12
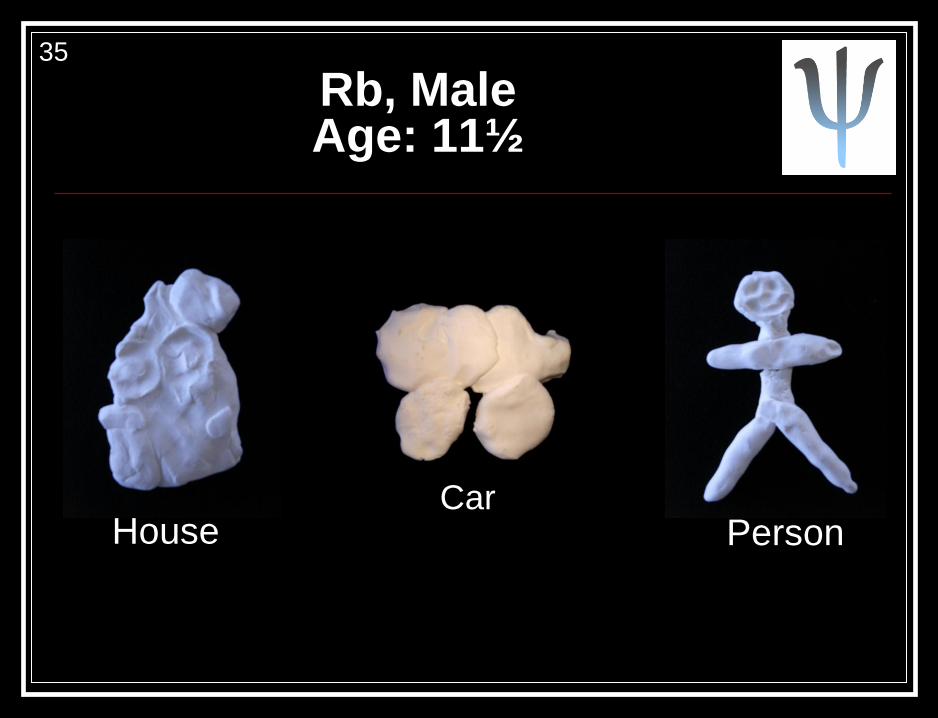
35
Rb, Male Age: 11½
Car House Person

36
Congenital Buphthalmos, Female Age: 12½
(decreasing vision from 3 to 6 years)
Car
House
Person

37
Cortical Blindness, Male Age: 12¼
Car
Person
House

38
ROP, Female 12 Years Old
House
#1
House
#2
Car
#1
Car
#2

39
Summary
Data in process, trends are evident
Social scale & other findings to be added
Sampling difficulties & challenges
Hereditary vs. non genetic disorders
Brain & neurological involvement
Impact of amount & use of vision
Perceptual features of NV/LP & VI groups
40
Meaning for Practitioners
There are no “rules” in development;
differences occur in patterns
Know the diagnosis, etiology and possible
implications as guides in planning
If vision is retained, consider practicing with
lenses that estimate acuity and field
Organize interventions around general
expectations for each group, but be adaptable

41
Meaning for Researchers & Clinicians
Collect standardized data where possible,
-visual and diagnostic observations can be
cited when interpreting or reporting results
-Ss may describe their own perceptions &
understanding of the environment
-where possible, find tangible ways of
evaluating their verbal reports.