how to improve engagement with community physicians
TRANSCRIPT

How to Improve Engagement with Community Physicians
Thursday, May 21st 2015 | 1:00PM - 2:00PM CDT
2
Your Presenters
Francisco Loya, MD, MBACEO, EmCare Hospital [email protected]
Mirza BaigChief Technology Officer, EmCare Hospital [email protected]

3
Attendees Will Learn:
The opportunity cost associated with unmanaged
referral processes
Best practices for managing direct admissions for
hospital care and referrals from physician to physician
New tools which can impact referral preference as well
as satisfaction

4
Types of Integration• technology, branding, process flow,
management information systems, physicians' liaisons, referral services, medical staff development
Non-economic
• monetary payments to physicians for services, improvementsEconomic
• systems to coordinate patient care, scheduling and registration, information systems, care standards, quality programs, service lines, case management
ClinicalSource: Milbank Q. 2008 Sep; 86(3): 375–434. doi: 10.1111/j.1468-0009.2008.00527.x PMCID: PMC2690342 Hospital-Physician Collaboration: Landscape of Economic Integration and Impact on Clinical Integration. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2690342/

5
Types of Referrals
MANY TO ONE
MANY TO ONE
MANY TO MANY
MANY TO MANY

6
The Impact of an Unmanaged Referral Process
Poor continuity
of care
Delayed care
Medical errors
Redundant testing
Wasted resources
Lower patient
satisfaction
Lower rate of referrals/ admissions

7
Poor Communication Impact on Sentinel Events
“The Joint Commission Sentinel Event database suggests poor communication contributes to nearly 70% of sentinel events, surpassing other commonly identified issues such as patient assessment and procedure compliance.”
Source: http://www.ncbi.nlm.nih.gov/books/NBK43683/

8
Direct vs. E.D. Admissions136.3 million
E.D. visits annually in the US (44.5 visits per 100
persons) 1
11.9% of visits result in
hospital admission1
Only 27% of patients are seen
in fewer than 15 minutes1
According toER Wait Watcher 2
National average24 minutes
Wyoming = 15 min.Washington D.C. = 53 min
Overcrowding in the E.D.
1 CDC: Emergency Department Statistics (2011) http://www.cdc.gov/nchs/fastats/emergency-department.htm2 ProPublica: https://projects.propublica.org/emergency/

9
Transition to More Direct Admissions
Direct admission
can improve:E.D. wait
timesPatient
experienceQuality and continuity
of care

10
Physician Referrals as a Measure of Engagement: Gallup Study
“Engaged physicians gave the hospital an average of 3% more outpatient referrals and 51% more inpatient referrals than physicians who were not engaged or who were actively disengaged.”
Gallup Article: Want to Increase Hospital Revenues? Engage Your Physicians. By Jeff Burger and Andrew Giger.http://www.gallup.com/businessjournal/170786/increase-hospital-revenues-engage-physicians.aspx

11
Physician Referrals: The Opportunity
Source: Projecting US Primary Care Physician Workforce Needs: 2010-2025 http://annfammed.org/content/10/6/503.full Alternate Source: NCHS Data Brief Number 105, September 2012: Generalist and Specialty Physicians: Supply and Access, 2009–2010 http://www.cdc.gov/nchs/data/databriefs/db105.htm calculations indicate PCP visits at 533,612 and specialist visits at 1,129,794 for a population of 320,873,156 (http://www.census.gov/popclock/)
462 Million PCP Visits
161 Million
Referrals 516 Million Specialist
Visits
(Projecting 565 Million by 2025)

12
Referral Management in the U.S.
Exchanging patient
information
PCP to Specialist66% refer to a
colleague
Specialist to PCP50% refer to a
colleague
Non-Colleague
34%Colleague66%
Non-Colleague
50%Colleague
50%
Often citing reasons such as of “ease of communication” and “share my medical record system”
Source: J Gen Intern Med. 2012 May;27(5):506-12. doi: 10.1007/s11606-011-1861-z. Epub 2011 Sep 16. Reasons for choice of referral physician among primary care and specialist physicians. Retrieved May 11, 2015 at http://www.ncbi.nlm.nih.gov/pubmed/21922159

13
The Problem with Referrals…
Only 16% of referrals are completed
electronically1
3 of every 10 tests are
reordered3
Redundant tests cost $8 billion per
year (2.7% of inpatient costs)4
20% of patients
referred to a specialist don’t
show up where they’re
referred2
Direct communication
between hospitalist and
PCP only in 3% - 20% of discharges5
Sources:1. Gaps in Referral Process between US Medical Providers http://www.practicefusion.com/pages/pr/survey-gaps-in-referral-process-between-us-medical-
providers.html?_sm_byp=iVVfD1PnJkMktqqV 2. Specialty Referral Completion among Primary Care Patients http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1934973/ 3. A Healthy System,” Technology CEO Council http://www.techceocouncil.org/reports/tcc_reports/ 4. Health Affairs. Improving Safety And Eliminating Redundant Tests: Cutting Costs In U.S. Hospitals. http://content.healthaffairs.org/content/28/5/1475.full and J Am Med
Inform Assoc. 2010 May-Jun;17(3):341-4. doi: 10.1136/jamia.2009.001750.A preliminary look at duplicate testing associated with lack of electronic health record interoperability for transferred patients. http://www.ncbi.nlm.nih.gov/pubmed/20442154
5. Deficits in communication and information transfer between hospital-based and primary care physicians http://www.ncbi.nlm.nih.gov/pubmed/17327525

14
Poor Follow-up Leads to Readmissions and Medication Errors
Source: http://www.commonwealthfund.org/~/media/Files/Publications/Case%20Study/2011/Apr/1473_SilowCarroll_readmissions_synthesis_web_version.pdfHiMSS paper Reducing Readmissions Top Ways Information Technology Can Help The Hospital Readmission (sources New England Journal of Medicine, Journal of Hospital Medicine and The Commonwealth Fund) http://www.himss.org/files/himssorg/content/files/controlreadmissionstechnology.pdf
50.2% of those readmitted never had a follow-up visit with a PCP
Patients lacking PCP follow up were 10 times more likely to be readmitted (adjusted 21% readmission) versus 3% with timely PCP follow-up
About 23% of follow-up patient appointments were missing test results and medical records
About 60% of medication errors occur during transitions of care (annual cost of $3.5 billion)

15
Reducing Readmissions Through Integration and Technology
Source: http://www.commonwealthfund.org/~/media/Files/Publications/Case%20Study/2011/Apr/1473_SilowCarroll_readmissions_synthesis_web_version.pdfHiMSS paper Reducing Readmissions Top Ways Information Technology Can Help The Hospital Readmission (sources New England Journal of Medicine, Journal of Hospital Medicine and The Commonwealth Fund) http://www.himss.org/files/himssorg/content/files/controlreadmissionstechnology.pdf
“Integrating hospital and outpatient care is key to reducing readmissions.”
The Commonwealth Fund

16
Solution?
Need a solution to:
Enhance communication
between physicians
Create “stickiness” in your referral
network
Expand your referral footprint
Close the loop at time of discharge

17
Solution: Many to Many Referrals
• Enhance communication between physicians
• Create “stickiness” in your referral network
• Expand referral footprint
• Enhance communication between physicians
• Create “stickiness” in your referral network
• Expand referral footprint
18
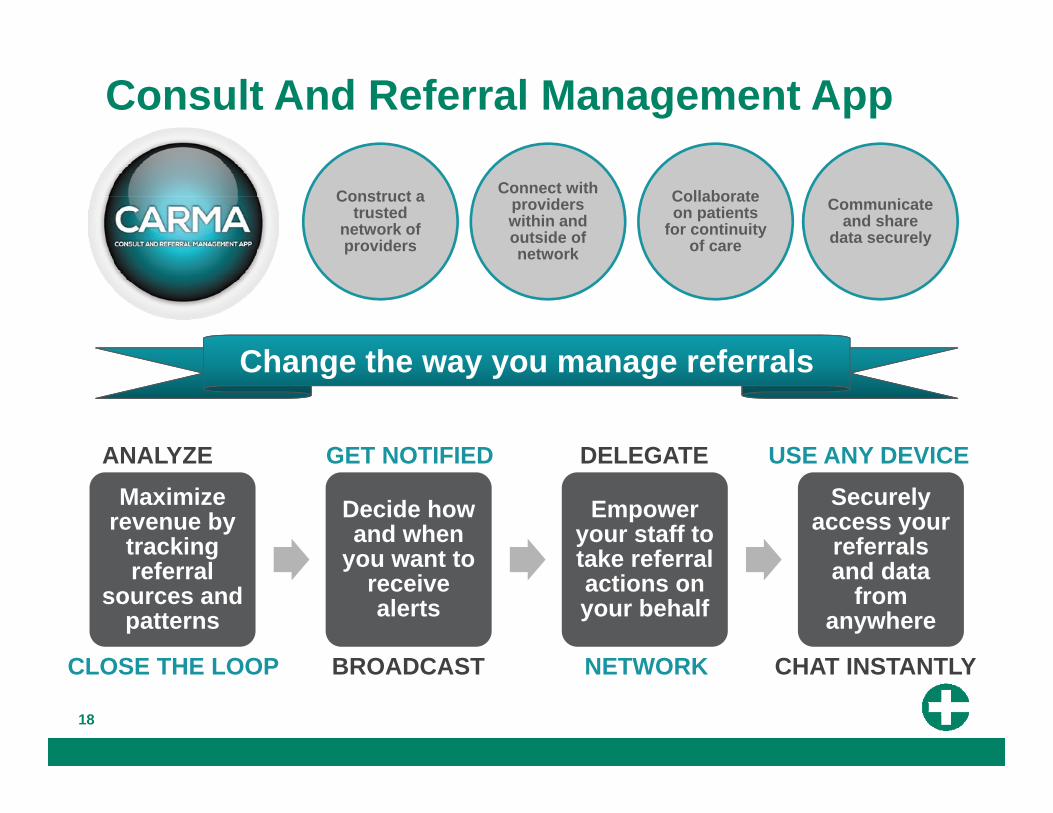
Consult And Referral Management App
Communicate and share
data securely
Collaborate on patients
for continuity of care
Connect with providers within and outside of network
Construct a trusted
network of providers
CLOSE THE LOOP BROADCAST NETWORK CHAT INSTANTLY
Maximize revenue by
tracking referral
sources and patterns
Decide how and when
you want to receive alerts
Empower your staff to take referral actions on your behalf
Securely access your
referrals and data
from anywhere
Change the way you manage referrals
ANALYZE GET NOTIFIED DELEGATE USE ANY DEVICE

19
CARMA Home Health Process Flow
Under Review
Step 2
TCM
MCC
InitiatedCase Manager Evolution
Health
Step 1
AcceptedAssign
NP
Step 3
Forward Schedule Visit
NP Visit on XX/XX
Step 4
NP
5 users, 20+ distinct actions5 users, 20+ distinct actions

20
Relevant stakeholders receive real-time updatesRelevant stakeholders receive real-time updates
CARMA Process Flow: Hospice
“PANIC” Hospice Center
MIH ParamedicMedical Care Coordinator
GOALPatient remains in
Care Plan
HospiceNurse
Patient’s Caretaker

21
Solution: Many to One Referrals
• Reduce E.D. wait times and overcrowding
• Enhance patient satisfaction
• Improve quality and continuity of care
• Reduce E.D. wait times and overcrowding
• Enhance patient satisfaction
• Improve quality and continuity of care

22
22
Referring Medical Facility
• Primary/Specialty Clinics
• Lower Acuity Hospitals
• Urgent Care• Free Standing E.D.• Extended Care
Facilities• NH/LTAC• ALF/SNF/Rehab
Assign BedAssign Bed
Scenario: An ill patient is seen in a referring medical facility and requires hospital admission.
Hospital
House Supervisor
Direct ADMIT
Alert
Admitting Physician
AcceptAccept
Patient
Hospital Boarding
Pass
1
3
2
Direct Admit System for HospitalsDASH
23
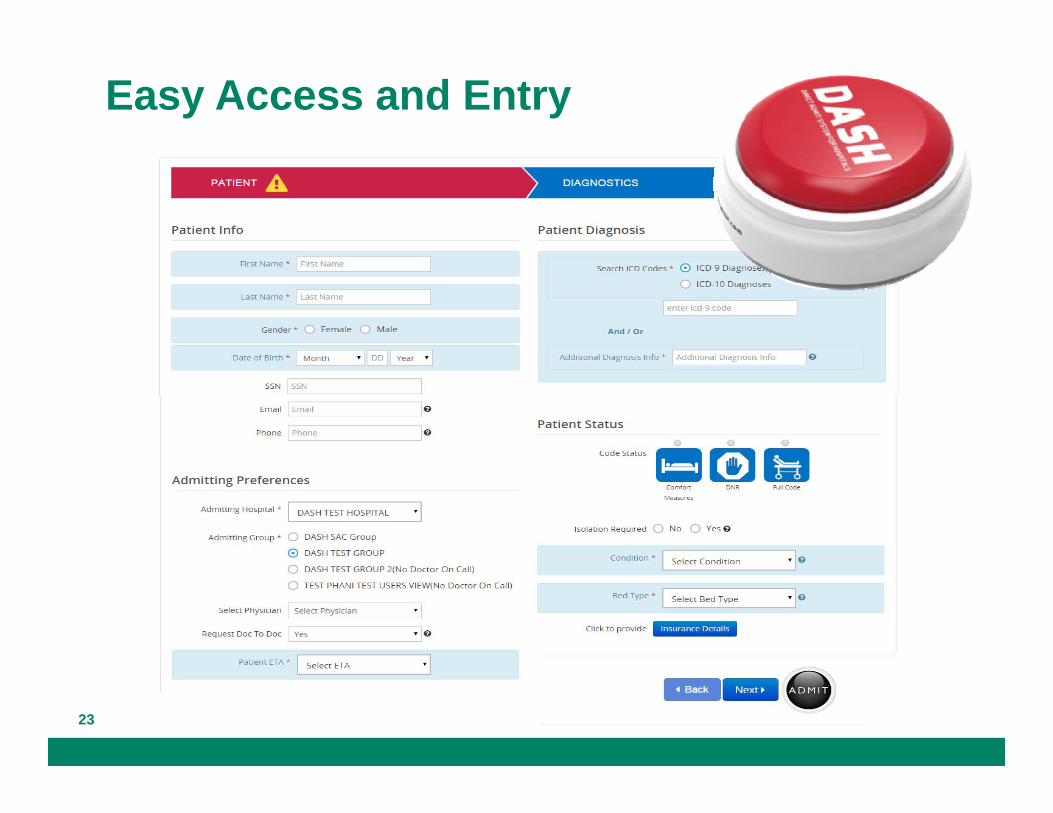
Easy Access and Entry

24
Real-time Communication

25
Tracking
DASHBOARD

26
0 1 2 4
72
84
140
27
1221
99108
170
0
20
40
60
80
100
120
140
160
180
Before and After DASH
DASH Impact on Referrals

Case Study: DASH Implementation at a 360-Bed Hospital

28
Hospital Case Study360-bed, acute care transforming rural hospital45 minutes from a major city in the SouthHas 9 acute care hospitals in a 25 mile radius with the closest one < 6 miles awayHad an occupancy rate of 75% in 2013Averaged 60 direct admit patients in 2013
Main desired outcomes • Build loyalty among high volume referrers• Streamline their admission process

29
Challenges Identified During DASH Implementation
Long response times – at times reached over 10 hoursBed Unavailable: Inefficient admission process Highlight other inefficiencies in admit, discharge and
transfer Peaked in the sixth month with 23 “bed not available”
responses
Implemented direct admit unit - immediate results

30
DASH Results
586
1380
592
84
115
148
0
20
40
60
80
100
120
140
160
0
200
400
600
800
1000
1200
1400
1600
2013 2014 2015
Direct Admissions
Total Admissions Avg # of admissions/mo
8:51
4:393:07
0:001:122:243:364:486:007:128:249:36
2013 2014 2015
Click to Arrival Time
Click to Arrival Time

31
Results*
Increased referrals from existing
sources as much as 27 percent, earning more loyalty from those who may
typically split their referrals between multiple hospitals
Reduced phone calls required to complete a direct admission by
over 90 percent
Reduced time to generate a direct admit form to 3
minutes
Captured actual key performance metrics like bed assignment
time to increase operational efficiencies
*Actual results may vary.
32
What We’ve Learned
Types of referrals
Impact of unmanaged referral processes
Referral management in the U.S. – problems and solutions
Physician referrals and engagement
Use of referral management technology
Case study

Q & A
Francisco Loya, MD, MBACEO, EmCare Hospital [email protected]
Mirza BaigChief Technology Officer, EmCare Hospital [email protected]
Call (855) 878-7326 or visit www.emcare.com/dash