how to manage the pregnant woman with heart disease · 2005-06-28 · repaired tof 62 14 0 8.1 100...
TRANSCRIPT

How to manage the pregnant
woman with heart disease
Dr Fiona Walker, The Heart Hospital,UCLH, London
Dr Sara Thorne, University Hospital Birmingham
Dr Cathy Head, The Heart Hospital, UCLH, London
Dr Kate English, The Yorkshire Heart Centre, Leeds

Why you need to know
Dr Fiona Walker
Consultant Cardiologist
The Heart Hospital, UCLH NHS Trust, London
No conflict of interest

Prevalence maternal heart disease ~ 1-3%
Author / Year Country No Preg Prev of Rh HD Congenital HD Other HD Maternal
with HD Maternal HD Mort
Etheridge
1950-75 Australia 764 0.5% 83% 13% 4% 1.3%
Sugrue
1969-7 Ireland 387 0.5% 84 13 3 0.5
Mc Faul N.Ireland 519 1.3% 60 31 9 0.6
1970-83
Bitsch Denmark 87 0.3% 8 81 11 2.3
1977-86

Maternal heart disease
UCL High-Risk Obstetric service 2001-2004
14
131
Acquired heart disease
Congenital heart disease

Impact of Infant Heart SurgeryImpact of Infant Heart Surgery
0
50
100
0
1 mnth 1 y
r5 y
rs15 yrs
% alive
Surgery GOS 1955 - 95
Natural history
new population
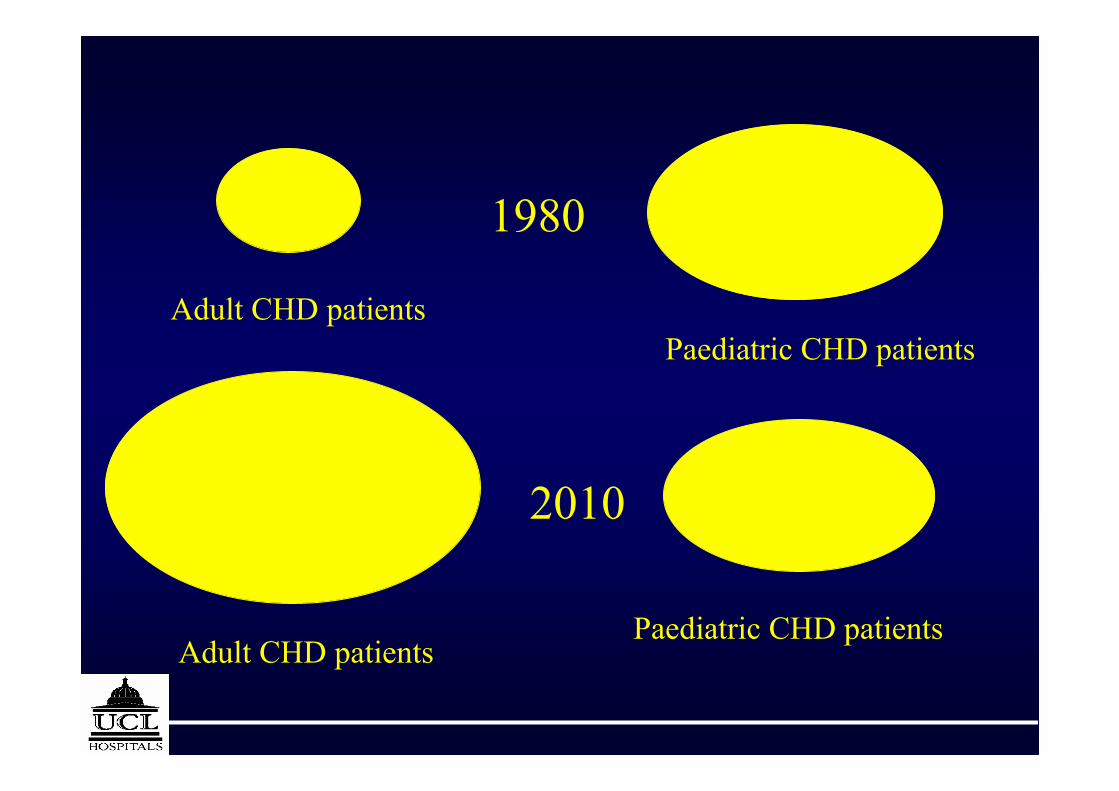
1980
Adult CHD patientsPaediatric CHD patients
2010
Adult CHD patients
Paediatric CHD patients

North East Regional Database
O’Sullivan, Wren BCS 2000
1 year16 years
251Birth
Infants >Infants
72
Follow-up
91/year
+ =
1877 new cases per year
require LTFU in UK
~ 16000 - 20000 patients in UK

GUCH PopulationGUCH Population
�More adults than children with
Fallot’s Tetralogy!
�Almost no children with Mustard or
Senning

28 weeks9%↓SBP
↓DBP
Term30-50%↑CO
Term10-30%↑SV
term20-30%↑HR
34weeks34%↓PVR
24 weeks20%↓SVR
32 weeks45-50%↑↑Plasma
volume
Term20%↑Oxygen
consumption
Circulatory changes in pregnancy

The haemodynamic changes of pregnancy
Labour & delivery puerperiumpregnancy
Baseline CO
Peripheral vascular resistance COPVR

0
5
10
15
20
25
1975 1978 1981 1984 1987 1990 1993 1996 1999 2002
mortality per 100,000 m
atern
ities
maternal mortality
direct mortality
indirect mortality
cardiac
Maternal mortality

Indirect maternal mortality (deaths per 100,000 maternities) 1967-2002
0
2
4
6
8
10
12
1969 1972 1975 1978 1981 1984 1987 1990 1993 1996 1999 2002
all indirect
cardiac
suicide
cancer
other indirect
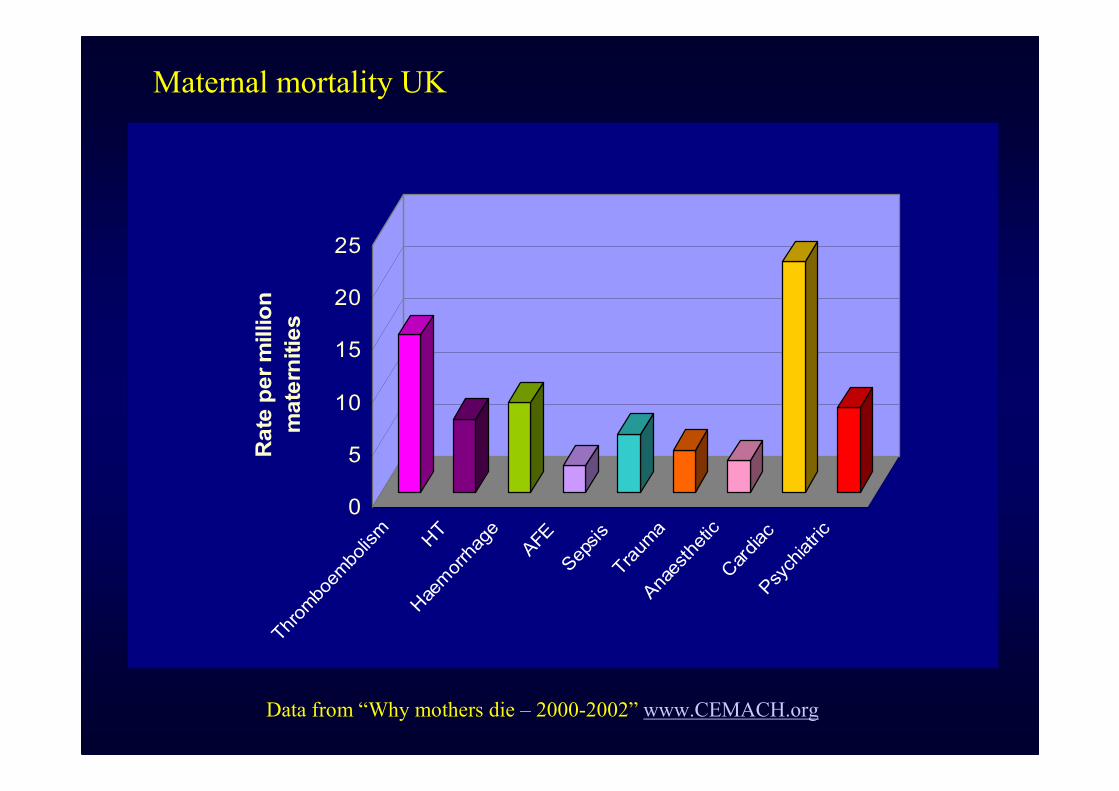
Data from “Why mothers die – 2000-2002” www.CEMACH.org
0
5
10
15
20
25Rate per million
maternities
Thromboembolism
HT
Haemorrhage
AFE
Sepsis
Trauma
Anaesthetic
Cardiac
Psychiatric
Maternal mortality UK

Deaths from heart disease
1952-60 & 1985-93
0
50
100
150
200
250
Rheumatic SBE Coronary Other
1952-60
1985-93

Maternal Cardiac deaths 1993-99
cardiomyopathy
aneurysm
MI
PHT
other
CHD 20%
Substandard care in 40%
CEMACH 2000-2002 - 44 deaths from heart disease

Lesion specific pregnancy outcome data
943.30960Tissue valve
8313 (c)2.978240Mechanical
Valve
87291.04996Cy + / no PHT
845.73553PHT
865.4221074Marfan (a)
1006.101832Fontan
9200215Mustard
1008.101462Repaired TOF
1004.80221Repaired CoA
94696.3016Severe AS
68011938AS (a)
161.50408MS
Live births %Maternal
CVS comp %
Maternal
mortality %
No abhortionNo
pregnancies
Maternal
lesion
U. Thilen, SB Olsson. Eur J Obs & Gynae and Reproductive biology 75(1997) 43-50

Toronto prospective multicentre study of pregnancy
outcomes in women with heart disease
562 women, 599 pregnancies, 13 centres
Review at <28/40, 28-37/40, peripartum,6/52 postpartum, 6/12 post
CHD (445) 74%, acquired (127) 24%, arrhythmia (27) 4%, PHT
(25) 4%
Baseline: 21 (4%) NYHA III, Cy+ 4
13% pregnancies complicated by pulmonary oedema, arrhythmia
or stroke
0% mortality
(Sui et al ; Circulation;104:July 2002)

The 4 predictors of maternal cardiac events are ;
• Prior episode of heart failure, TIA, CVA, or arrhythmia
• NYHA ≥ II or cyanosis
• Left heart obstruction (MVA < 2 cm2, AVA < 1.5 cm2,
Peak LVOTO > 30 mmHg on echo)
• Reduced LV function (EF < 40%)
0 predictors - risk of a cardiac event is 5%
1 predictor - risk of cardiac event 27%
(Sui et al, Circulation;104:July 2002)
> 1- risk of cardiac event is 75%
Obstetric Problems which increase
Maternal risk
> Twins
Pre-eclampsia
Haemorrhage
Premature Labour
Hydramnios

Motto; 6P’s
Prior planning,
prevents
poor performance (outcome)

Pre-Pregnancy counselling ;
1. The complexity of the heart lesion
2. Appreciate impact of normal haemodynamic changes on lesion
3. Detailed knowledge of prior surgical correction(s)/interventions
4. Detailed knowledge of residua / sequelae
5. A discussion re ; long-term prognosis & risk of recurrence in
offspring ? 22q11
6. Optimisation of clinical status including drugs
7. Knowledge of other co-morbid medical problems

Pre - Pregnancy work-up
�Clinical review and examination
�Up to date TTE / stress echo
�ETT or CPEX
�Optimise and change Meds
�Communicate with obstetric team & local cardiologist
�Plan place & frequency of reviews

• Obstetric unit or cardiac unit
• Early or term
• Vaginal delivery v’s C-section
• Epidural / Spinal/ Natural
• Haemodynamic monitoring - invasive / non-invasive
• CVS drugs
• Endocarditis prophylaxis
• Duration of monitoring / observation post-partum
Labour & delivery planning

“If single do not allow marriage,
If fertile do not allow pregnancy
If pregnant do not allow delivery(!?)
If delivered do not allow breast feeding”
XIX century Obstetric aphorism referring to
women with heart disease
Neonatologist
Haematologist
Anaesthesia
GUCH cardiologist Obstetrician
Foetal medicine
Intensive careSpecialist nurse
Obstetric physician
Manpower for the high risk cardiac obstetric service
