hyperglycemia as a risk factor in the perioperative patient€¦ · mortality after coronary artery...
TRANSCRIPT
r in
Hyperglycemia as a Risk Factothe Perioperative Patient LINDA RUTAN, MSN, RN, CNS-BC, CNOR, CRNFA; KATHLEEN SOMMERS, EdD, RNwww.aorn.org/CE
2.1
e glucosein patientslycemia iscomes. Anhe body’ssely mon-a through-borativelyioperative
2012. doi:
mellitus.
ABSTRACT
Bodily injury and stress associated with surgical interventions increaslevels not only in individuals diagnosed with diabetes mellitus but alsowithout a preoperative diagnosis of diabetes. Whatever the cause, hypergbecoming an increasingly important indicator of perioperative patient outelevated blood glucose level affects the body’s defense systems and tability to heal after surgical intervention. Perioperative nurses should cloitor the patient’s blood glucose levels and watch for signs of hyperglycemiout the perioperative experience. Perioperative nurses should work collawith other perioperative team members to identify and treat perhyperglycemia. AORN J 95 (March 2012) 352-361. © AORN, Inc,10.1016/j.aorn.2011.06.010
Key words: hyperglycemia, diabetes of injury, stress diabetes, diabetes
prochypergnoslic aptionlt of
s, theintervsruptrglyce
00 mg/dL).2
ses to un-cess thatat hypergly-ic levels,glycemia
rioperativeare practicess and im-.
injury andntions in-iagnosedents withoutperative hy-on for hy-ls have ledpatient.4 The
contac
rn the
wing
leting
ation
hours
Individuals undergoing a surgicalare at risk for complications ofmia even in the absence of a dia
diabetes mellitus.1 Complex metabodocrine changes, including the disruglucose metabolism, occur as a resudividual’s preoperative health statution requiring surgery, the surgicaland postoperative processes. The diglucose metabolism results in hype
indicates that continuing education
hours are available for this activity. Ea
tact hours by reading this article, revie
purpose/goal and objectives, and comp
online Examination and Learner Evalu
http://www.aorn.org/CE. The contact
this article expire March 31, 2015.
352 AORN Journal ● March 2012 Vol 95
edureglyce-is ofnd en-
ofan in-condi-ention,
ion ofmia
(ie, blood sugar level greater than 2It is important for perioperative nurderstand the pathophysiological prodrives hyperglycemia, the effects thcemia has at the cellular and systemresearch correlations between hyperand patient complications in the pesetting, and recommended patient cthat disrupt the pathological procesprove patient healing and outcomes
According to Berkers et al,3 bodilystress associated with surgical intervecrease glucose levels in individuals dwith diabetes mellitus. However, patidiabetes also may experience postoperglycemia. Regardless of the reasperglycemia, increased glucose leveto impaired healing in the surgical
t
con-
the
the
at
for
National Nosocomial Infections Surveillance
doi: 10.1016/j.aorn.2011.06.010
No 3 © AORN, Inc, 2012
emiafectioetes od glu
llnessial adositivoperated unHow
glycemed mhat n
blooyper
eriencrativelatedia in
us.
en dibetests in
nsulin.8
e stress
critical
profound
atients can
hyperglyce-
for perioper-
of many
at result in
ndant endog-
ed glucose
t tissues.9
immune re-
mechanism.3
ted stress
ant increased
ed insulin
ance produce
n of the ad-
tisol, which
muscle pro-
ive hepatic
lly, there is
PERIOPERATIVE HYPERGLYCEMIA www.aornjournal.org
System risk index included hyperglycleading risk factor for surgical site in
In the past, stress diabetes, or diabjury1 (ie, a transitory increase of bloolevel in response to the stress of an ijury), was considered to be a beneficresponse that promotes healing and poperative outcomes.3 Generally, postblood glucose levels were left untrealevels were greater than 200 mg/dL.3
recent research has correlated normothe perioperative patient with decreasand mortality.6 Evidence suggests tshould closely monitor the patient’scose levels and watch for signs of hmia throughout the perioperative expTherefore, it is important for periopeto understand the pathophysiology regical insult and resulting hyperglycemtients with or without diabetes mellit
PATHOPHYSIOLOGYThere are several similarities betwemellitus and diabetes of injury. Diatus is a pancreatic failure that resul
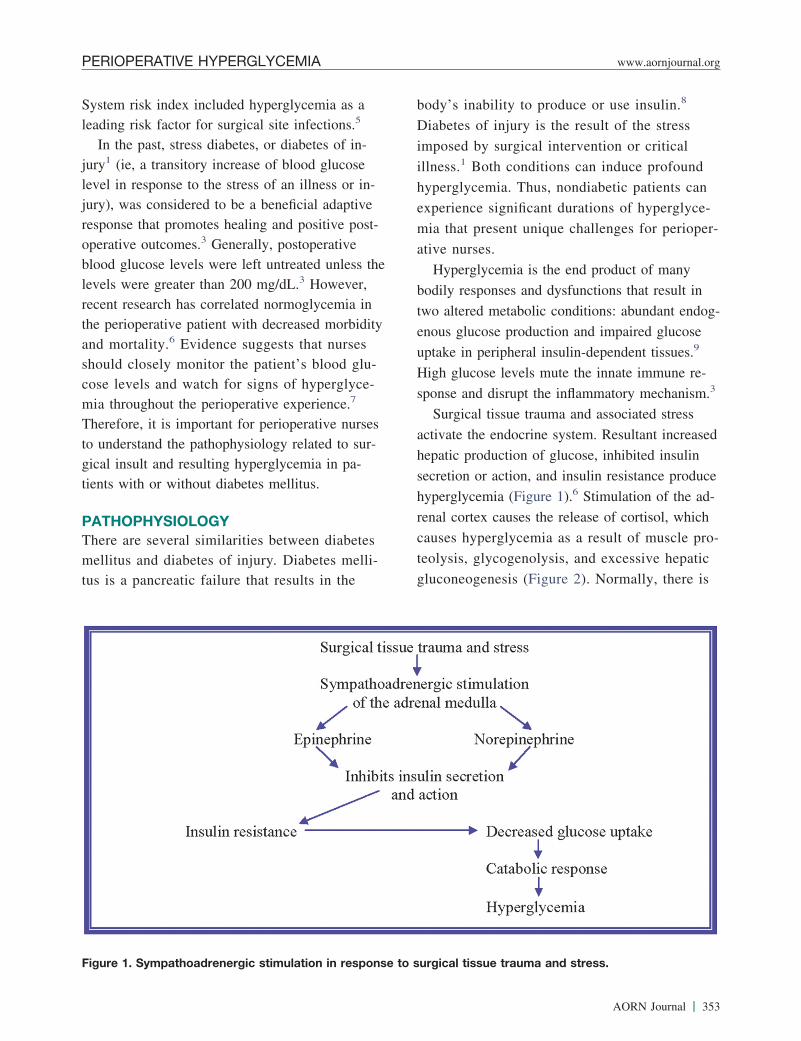
Figure 1. Sympathoadrenergic stimulation in
as ans.5
f in-coseor in-
aptivee post-tiveless theever,ia in
orbidityursesd glu-glyce-e.7
nursesto sur-pa-
abetesmelli-
the
body’s inability to produce or use i
Diabetes of injury is the result of th
imposed by surgical intervention or
illness.1 Both conditions can induce
hyperglycemia. Thus, nondiabetic p
experience significant durations of
mia that present unique challenges
ative nurses.
Hyperglycemia is the end product
bodily responses and dysfunctions th
two altered metabolic conditions: abu
enous glucose production and impair
uptake in peripheral insulin-dependen
High glucose levels mute the innate
sponse and disrupt the inflammatory
Surgical tissue trauma and associa
activate the endocrine system. Result
hepatic production of glucose, inhibit
secretion or action, and insulin resist
hyperglycemia (Figure 1).6 Stimulatio
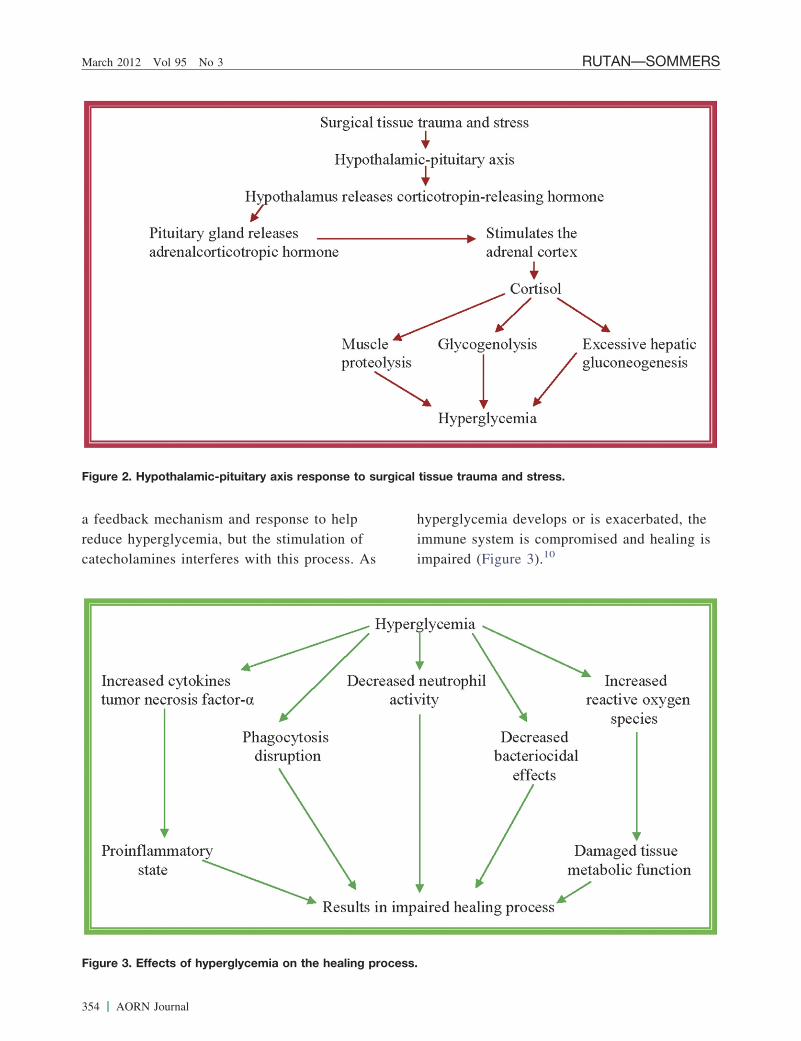
renal cortex causes the release of cor
causes hyperglycemia as a result of
teolysis, glycogenolysis, and excess
gluconeogenesis (Figure 2). Norma
response to surgical tissue trauma and stress.
AORN Journal 353
e to hulatioproce
rbated, thed healing is
spon
March 2012 Vol 95 No 3 RUTAN—SOMMERS
a feedback mechanism and responsreduce hyperglycemia, but the stimcatecholamines interferes with this
Figure 2. Hypothalamic-pituitary axis re
Figure 3. Effects of hyperglycemia on the he
354 AORN Journal
elpn ofss. As
hyperglycemia develops or is exaceimmune system is compromised animpaired (Figure 3).10
se to surgical tissue trauma and stress.
aling process.
d randnorma
hospsurgicortalt stu
hat is
pogly
uences,13,16
emia as an
outcomes,
of glucose
1% decreaseinsulin titrate
L versus ainsulin titrate
Lorrelated withindependent
putations inents without
� 180atients whose108 mg/dL
glycemictor foryieldedtraditional
mg/dL withality
reced patient
8(3):506-523.creases in
hemia is poor in
nts. N Engl
after cardiac
ed. 2005;33(7):
):933-944.
PERIOPERATIVE HYPERGLYCEMIA www.aornjournal.org
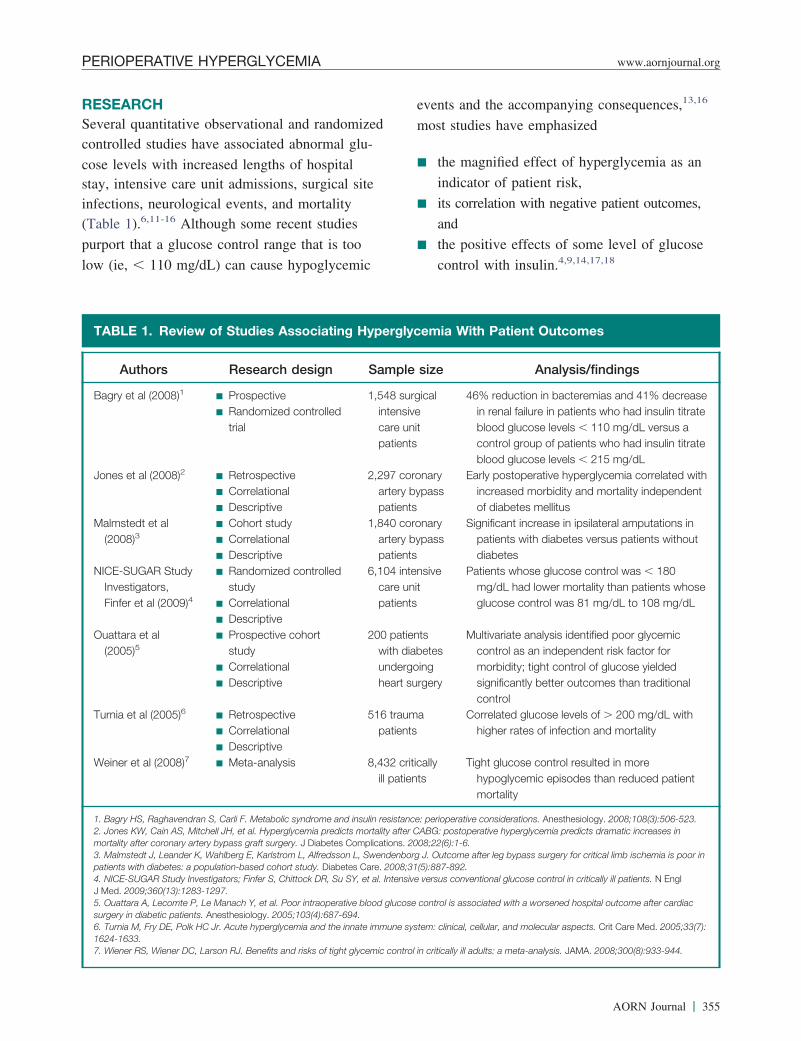
RESEARCHSeveral quantitative observational ancontrolled studies have associated ab
cose levels with increased lengths ofstay, intensive care unit admissions,infections, neurological events, and m(Table 1).6,11-16 Although some recen
purport that a glucose control range t
low (ie, � 110 mg/dL) can cause hy
TABLE 1. Review of Studies Asso
Authors Research de
Bagry et al (2008)1 � Prospective� Randomized co
trial
Jones et al (2008)2 � Retrospective� Correlational� Descriptive
Malmstedt et al(2008)3
� Cohort study� Correlational� Descriptive
NICE-SUGAR StudyInvestigators,Finfer et al (2009)4
� Randomized costudy
� Correlational� Descriptive
Ouattara et al(2005)5
� Prospective cohstudy
� Correlational� Descriptive
Turnia et al (2005)6 � Retrospective� Correlational� Descriptive
Weiner et al (2008)7 � Meta-analysis
1. Bagry HS, Raghavendran S, Carli F. Metabolic syn2. Jones KW, Cain AS, Mitchell JH, et al. Hyperglycemortality after coronary artery bypass graft surgery. J3. Malmstedt J, Leander K, Wahlberg E, Karlstrom Lpatients with diabetes: a population-based cohort st4. NICE-SUGAR Study Investigators; Finfer S, ChittoJ Med. 2009;360(13):1283-1297.5. Ouattara A, Lecomte P, Le Manach Y, et al. Poorsurgery in diabetic patients. Anesthesiology. 2005;106. Turnia M, Fry DE, Polk HC Jr. Acute hyperglycemi1624-1633.7. Wiener RS, Wiener DC, Larson RJ. Benefits and ri
omizedl glu-
italal siteitydies
too
cemic
events and the accompanying conseq
most studies have emphasized
� the magnified effect of hyperglyc
indicator of patient risk,
� its correlation with negative patient
and
� the positive effects of some level
control with insulin.4,9,14,17,18
ng Hyperglycemia With Patient Outcomes
Sample size Analysis/findings
d1,548 surgical
intensivecare unitpatients
46% reduction in bacteremias and 4in renal failure in patients who hadblood glucose levels � 110 mg/dcontrol group of patients who hadblood glucose levels � 215 mg/d
2,297 coronaryartery bypasspatients
Early postoperative hyperglycemia cincreased morbidity and mortalityof diabetes mellitus
1,840 coronaryartery bypasspatients
Significant increase in ipsilateral ampatients with diabetes versus patidiabetes
d 6,104 intensivecare unitpatients
Patients whose glucose control wasmg/dL had lower mortality than pglucose control was 81 mg/dL to
200 patientswith diabetesundergoingheart surgery
Multivariate analysis identified poorcontrol as an independent risk facmorbidity; tight control of glucosesignificantly better outcomes thancontrol
516 traumapatients
Correlated glucose levels of � 200higher rates of infection and mort
8,432 criticallyill patients
Tight glucose control resulted in mohypoglycemic episodes than redumortality
and insulin resistance: perioperative considerations. Anesthesiology. 2008;10dicts mortality after CABG: postoperative hyperglycemia predicts dramatic ins Complications. 2008;22(6):1-6.
son L, Swendenborg J. Outcome after leg bypass surgery for critical limb iscbetes Care. 2008;31(5):887-892.u SY, et al. Intensive versus conventional glucose control in critically ill patie
rative blood glucose control is associated with a worsened hospital outcome-694.
e innate immune system: clinical, cellular, and molecular aspects. Crit Care M
ht glycemic control in critically ill adults: a meta-analysis. JAMA. 2008;300(8
ciati
sign
ntrolle
ntrolle
ort
dromemia preDiabete
, Alfredsudy. Diack DR, S
intraope3(4):687a and th
sks of tig
AORN Journal 355

ptimaycemiks.4 Rwith(ie,
olonglucos
plicais recbloodthouthat shsk of
hypemnon.19
issioose ldiseaand
creenng onenz2
emicrativituted
r recom-
1c test that
; if the result
ician is con-
ostponing a
levels im-
ommends
120 mg/dL
d glucose
er the pa-
ications. If
, peak, and
the nurse
od glucose
und stress
f nursing
ive care.
abolic
ase blood
s who have
ly prone to
ose tissue
ocrine organ
l cellular
rglycemia.23
surgical
ed within the
ol is obtainedervention if
erativeccessed
March 2012 Vol 95 No 3 RUTAN—SOMMERS
Study results conflict regarding the ocose control range to prevent hypoglas well as to avoid hyperglycemic rissearch has yet to correlate outcomesglycated hemoglobin (HbA1c) resultsplasma glucose concentration over prods) or hospital stay average blood g
IMPLICATIONSResearch results have a number of imfor perioperative nurses (Table 2). Itmended that nurses obtain a baselinecose level for the patient. Patients widiabetes can demonstrate symptoms talert the perioperative nurse to the riglycemia or developing perioperativemia. These symptoms may include sofruity breath, itchy skin, and confusio
Some hospitals have instituted adming that includes an initial blood glucall patients, regardless of preexistingThe Agency for Healthcare Researchrecommends preoperative glycemic ssubsequent control measures dependifindings.20 A study by Gurkan and Wported maintaining preoperative glyc� 200 mg/dL. A protocol for periopecose management developed and inst
TABLE 2. Glycemic Control: Rec
Admission bloodglucose level
� 100 mg/dL � N100 mg/dL � 220 mg/dL � R
p� M� C
� 220 mg/dL � C� P
s
1. Committee on Perioperative Evaluation (CAPO), Bevaluation. Arq Bras Cardiol. 2007;89(6):e197-208. hOctober 16, 2011.
356 AORN Journal
l glu-c crisise-
eitheraverageed peri-e levels.
tionsom-
glu-knownould
hyper-rglyce-lence,
n test-evel forses.Qualitying and
the1 sup-levelse glu-
by the
Ohio State University Medical Cente
mends reviewing a preoperative HbA
was obtained within the past 30 days
is greater than 9%, the referring phys
tacted and consideration is given to p
nonemergent procedure until glucose
prove.22 In addition, the protocol rec
maintaining a target glucose level of
to 150 mg/dL intraoperatively.
When evaluating a patient’s bloo
level, it is important to know wheth
tient is taking any antidiabetic med
so, knowledge of the last dose, onset
duration of that medication can give
insight into the direction that the blo
level is likely to follow.
Identifying factors that can compo
hyperglycemia is an important part o
assessment, judgment, and perioperat
Corticosteroids, catecholamines, an
agents, and other medications incre
glucose levels. Furthermore, patient
central visceral obesity are particular
insulin resistance. The excessive adip
around the abdomen works as an end
and is an indication of dysfunctiona
metabolism that contributes to hype
Acute pain, blood loss, and lengthy
endations for the Perioperative Period1
Perioperative recommendations
cific preoperative measurescreatinine test results and a baseline electrocardiogram obtains 12 monthsr blood pressure closelyer referring the patient to an endocrinologist after surgeryer postponing nonemergent surgery until better glycemic contr
a blood glucose test at induction and consider insulin drip intlasts longer than 1 hour
ociety of Cardiology. Steps to reduce surgical risk. In: I guidelines for periopideline.gov/content.aspx?id�12237&search�perioperative�patient�care. A
omm
o speeviewreviouonitoonsidonsiderformurgery
razilian Sttp://gu
statement
t’s endocrineaintained atd fromvels.
PERIOPERATIVE HYPERGLYCEMIA www.aornjournal.org
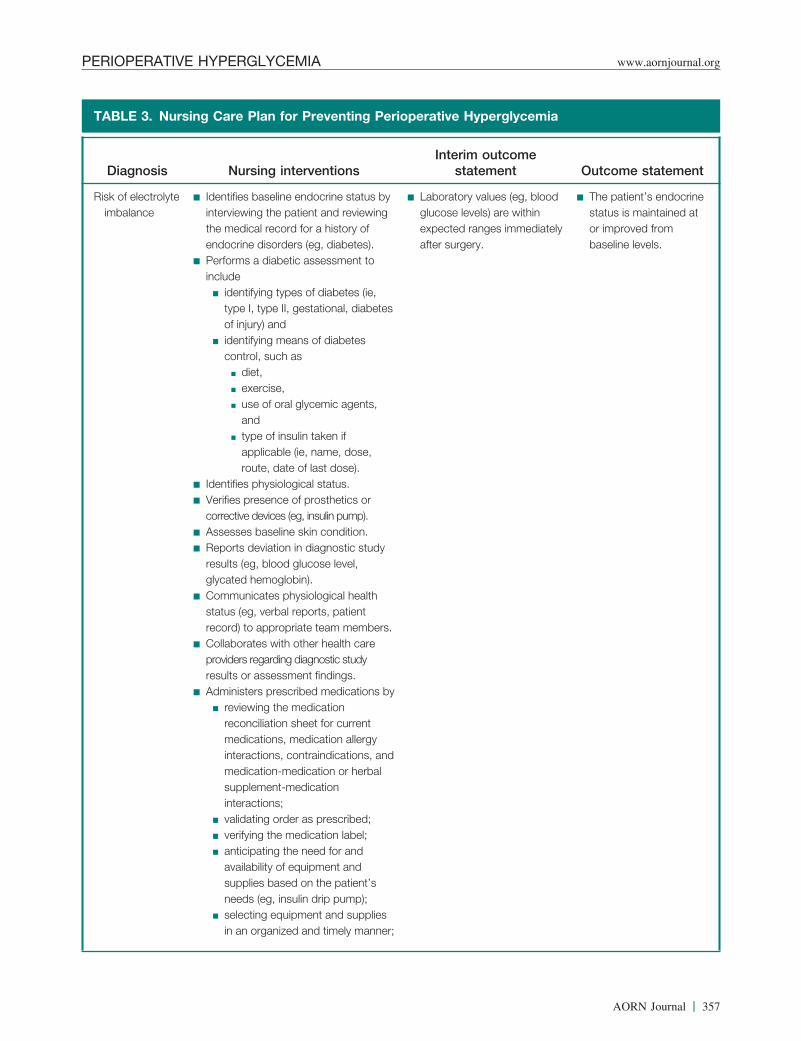
TABLE 3. Nursing Care Plan for Preventing Perioperative Hyperglycemia
Diagnosis Nursing interventionsInterim outcome
statement Outcome
Risk of electrolyteimbalance
� Identifies baseline endocrine status byinterviewing the patient and reviewingthe medical record for a history ofendocrine disorders (eg, diabetes).
� Performs a diabetic assessment toinclude
� identifying types of diabetes (ie,type I, type II, gestational, diabetesof injury) and
� identifying means of diabetescontrol, such as
� diet,� exercise,� use of oral glycemic agents,
and� type of insulin taken if
applicable (ie, name, dose,route, date of last dose).
� Identifies physiological status.� Verifies presence of prosthetics or
corrective devices (eg, insulin pump).� Assesses baseline skin condition.� Reports deviation in diagnostic study
results (eg, blood glucose level,glycated hemoglobin).
� Communicates physiological healthstatus (eg, verbal reports, patientrecord) to appropriate team members.
� Collaborates with other health careproviders regarding diagnostic studyresults or assessment findings.
� Administers prescribed medications by� reviewing the medication
reconciliation sheet for currentmedications, medication allergyinteractions, contraindications, andmedication-medication or herbalsupplement-medicationinteractions;
� validating order as prescribed;� verifying the medication label;� anticipating the need for and
availability of equipment andsupplies based on the patient’sneeds (eg, insulin drip pump);
� selecting equipment and suppliesin an organized and timely manner;
� Laboratory values (eg, bloodglucose levels) are withinexpected ranges immediatelyafter surgery.
� The patienstatus is mor improvebaseline le
AORN Journal 357

sistan
sixthe comis tosion t). If tmg/dLff meese re
aboraol foith aod g
mic tergen
ry tw
ative blood
lin drip if
ose checksnts in the
g protocolse level of �
hing abouthyperglyce-hat would
n endocrinol-
and re-sk factor for4 However,
statement
March 2012 Vol 95 No 3 RUTAN—SOMMERS
procedures also can induce insulin rewell as decrease glucose disposal.6
RECOMMENDATIONSGlucose level is often considered thesign.24 The first step in preventing thtions of perioperative hyperglycemiaprove clinical assessment with admisof glucose level and HbA1c (Table 3tient’s blood glucose level is � 180nurse should consult with medical staPerioperative nurses should follow thmendations:
� Initiate and become part of a colleffort to develop a hospital protoccose control in surgical patients wwithout diabetes to maintain a blolevel of � 140 mg/dL.
� Collaborate to set a specific glyce� 80 mg/dL for scheduled nonemcal interventions.
� Perform blood glucose checks eve
TABLE 3. (continued) Nursing Ca
Diagnosis Nursing inte
� determining that afunctioning before
� performing patienusing at least two
� ensuring the seveadministration aremedication admin
� right patient,� right medicatio� right dose,� right route,� right time,� right reason, a� right documen
� Monitors physiologic� Evaluates endocrine� Reviews pertinent la
results (eg, serum gl
during surgery if surgery lasts longer t
358 AORN Journal
ce as
vitalplica-
im-estinghe pa-, thembers.com-
tiver glu-ndlucose
arget oft surgi-
o hours
hours and if the patient’s preoperglucose level was � 110 mg/dL.
� Be prepared to implement an insuneeded.
� Perform postoperative blood glucwith initial vital signs on all patiepostanesthesia care unit.
� Develop postoperative monitorinfor patients with a blood glucos180 mg/dL.
� At discharge, provide patient teacsigns and symptoms of increasedmia and infection or nonhealing trequire medical attention.
� Consider obtaining a referral to aogist if necessary.19
CONCLUSIONThere is a consensus among expertssearchers that hyperglycemia is a rinegative surgical outcomes.2,3,6,11,1
an for Preventing Perioperative Hyperglycemia
ionsInterim outcome
statement Outcome
ment is
ficationers;of solution
ed duringn:
meters..ry testlevels).
re Pl
rvent
ll equipuse;
t identiidentifin rightsfollow
istratio
n,
ndtation.al parastatus
boratoucose
han two experts disagree on target blood glucose levels
s of high blood
levels, if
edicine, if
igh bloodery?
.ay experience, and heart; in-r circulation;be prevented
0 days. Thenume-free soapor powder di-pletely healed.lood sugar.structed by your
by your doctor.
xperience any
r weakness;t your incision
ills;ith medication;
above 240
n the desired
tp://www168/TAB�
ealth Care.ucation/0Sugar%
PERIOPERATIVE HYPERGLYCEMIA www.aornjournal.org
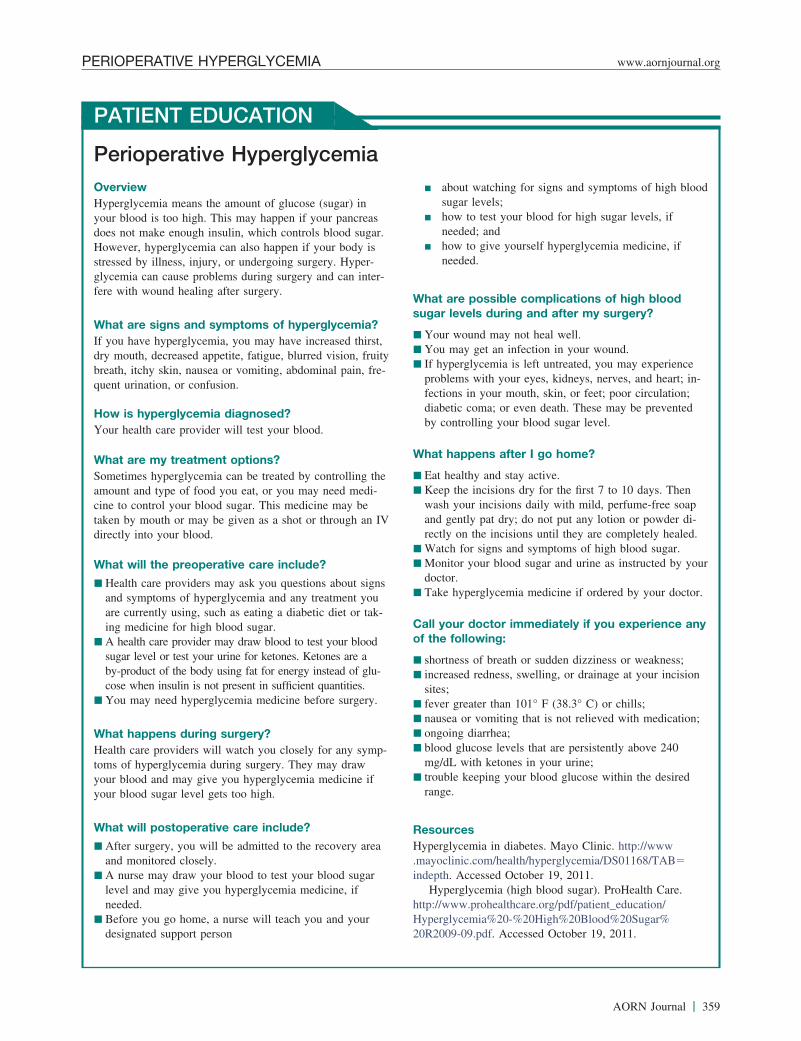
PATIENT EDUCATION
Perioperative HyperglycemiaOverviewHyperglycemia means the amount of glucose (sugar) inyour blood is too high. This may happen if your pancreasdoes not make enough insulin, which controls blood sugar.However, hyperglycemia can also happen if your body isstressed by illness, injury, or undergoing surgery. Hyper-glycemia can cause problems during surgery and can inter-fere with wound healing after surgery.
What are signs and symptoms of hyperglycemia?If you have hyperglycemia, you may have increased thirst,dry mouth, decreased appetite, fatigue, blurred vision, fruitybreath, itchy skin, nausea or vomiting, abdominal pain, fre-quent urination, or confusion.
How is hyperglycemia diagnosed?Your health care provider will test your blood.
What are my treatment options?Sometimes hyperglycemia can be treated by controlling theamount and type of food you eat, or you may need medi-cine to control your blood sugar. This medicine may betaken by mouth or may be given as a shot or through an IVdirectly into your blood.
What will the preoperative care include?
� Health care providers may ask you questions about signsand symptoms of hyperglycemia and any treatment youare currently using, such as eating a diabetic diet or tak-ing medicine for high blood sugar.
� A health care provider may draw blood to test your bloodsugar level or test your urine for ketones. Ketones are aby-product of the body using fat for energy instead of glu-cose when insulin is not present in sufficient quantities.
� You may need hyperglycemia medicine before surgery.
What happens during surgery?Health care providers will watch you closely for any symp-toms of hyperglycemia during surgery. They may drawyour blood and may give you hyperglycemia medicine ifyour blood sugar level gets too high.
What will postoperative care include?
� After surgery, you will be admitted to the recovery areaand monitored closely.
� A nurse may draw your blood to test your blood sugarlevel and may give you hyperglycemia medicine, ifneeded.
� Before you go home, a nurse will teach you and your
� about watching for signs and symptomsugar levels;
� how to test your blood for high sugarneeded; and
� how to give yourself hyperglycemia mneeded.
What are possible complications of hsugar levels during and after my surg
� Your wound may not heal well.� You may get an infection in your wound� If hyperglycemia is left untreated, you m
problems with your eyes, kidneys, nervesfections in your mouth, skin, or feet; poodiabetic coma; or even death. These mayby controlling your blood sugar level.
What happens after I go home?
� Eat healthy and stay active.� Keep the incisions dry for the first 7 to 1
wash your incisions daily with mild, perfand gently pat dry; do not put any lotionrectly on the incisions until they are com
� Watch for signs and symptoms of high b� Monitor your blood sugar and urine as in
doctor.� Take hyperglycemia medicine if ordered
Call your doctor immediately if you eof the following:
� shortness of breath or sudden dizziness o� increased redness, swelling, or drainage a
sites;� fever greater than 101° F (38.3° C) or ch� nausea or vomiting that is not relieved w� ongoing diarrhea;� blood glucose levels that are persistently
mg/dL with ketones in your urine;� trouble keeping your blood glucose withi
range.
ResourcesHyperglycemia in diabetes. Mayo Clinic. ht.mayoclinic.com/health/hyperglycemia/DS01indepth. Accessed October 19, 2011.
Hyperglycemia (high blood sugar). ProHhttp://www.prohealthcare.org/pdf/patient_edHyperglycemia%20-%20High%20Blood%2
designated support person 20R2009-09.pdf. Accessed October 19, 2011.
AORN Journal 359
entionealin
contric evatiention wa reincr
italstocoltrolical
moni
al. Tye to su
HC. Sstudy
06;24
n dene orga2008;
l on pn cardnce Nu
illanceuary 1. http:.pdf. A
etaboliive co-523.ernikessiveardiactudy..
sociati�WW
_comp
Berghe a rol
iaz JJ.Nutr C
Hyperglycemiarative hypergly-rtality after cor-betes Complica-
arlstrom L,after leg by-
s poor in pa-cohort study.
fer S, Chittockentional glucoseJ Med. 2009;
, et al. Poorassociated
r cardiac sur-gy. 2005;
hyperglycemial, cellular, and
05;33(7):1624-
nefits and risksadults: a meta-
DR, et al. Hy-bral aneurysmross neurologicClin Proc.
You X, Thalerdependentts with undiag-
b. 2002;87(3):
ve management/emedicine#showall. Ac-
(CAPO), Bra-duce surgical
valuation. Arq://guideline
erioperative�1.ion control: anurgery. Ortho-
videnced-based’s Guide toManagement.University
et al. Increasedue productionsurgery
nsulin resis-1(11):
h vital sign.
March 2012 Vol 95 No 3 RUTAN—SOMMERS
and duration and methods of intervachieve optimal patient safety and hvious trends toward tight glycemicbeen shown to produce hypoglycemthat generate unintended negative pcomes.13 Consequently, in combinaevidence that hyperglycemia can bedictor of surgical site infections andmorbidity and mortality, many hospproducing glucose management progeared toward a more moderate conRegardless, hyperglycemia is a surgthat demands attention and carefulby perioperative nurses.
References1. Schricker T, Gougeon R, Eberhart L, et
betes mellitus and the catabolic responsAnesthesiology. 2005;102(2):320-326.
2. Turina M, Miller FN, Tucker CF, Polkhyperglycemia in surgical patients and alated cellular mechanisms. Ann Surg. 20851.
3. Berkers J, Gunst J, Vanhorebeek I, VaG. Glycaemic control and perioperativtion. Best Pract Res Clin Anesthesiol.135-149.
4. Patel KL. Impact of tight glucose controtive infection rates and wound healing igery patients. J Wound Ostomy Contine35(4):397-404.
5. National Nosocomial Inspections SurveSystem Report, Data Summary from Janthrough June 2004, issued October 2004.cdc.gov/nhsn/PDFs/datastat/NNIS_2004December 2, 2011.
6. Bagry HS, Raghavendran S, Carli F. Mdrome and insulin resistance: perioperatations. Anesthesiology. 2008;108(3):506
7. Prasad AA, Kline SM, Schuler HG, SukClinical and laboratory correlates of excsistent blood glucose elevation during cin nondiabetic patients: a retrospective sthorac Vasc Anesth. 2007;21(6):843-846
8. Diabetes Basics. American Diabetes Asdiabetes.org/diabetes-basics/?utm_sourceutm_contents�Keymathc-diabetes&utmCON. Accessed December 2, 2011.
9. Langouche L, Vanhorebeek I, Van Dencemic control in trauma patients, is therTrauma. 2006;8:13-19.
10. Collier B, Dossett LA, Addison KM, Dcontrol and the inflammatory response.
2008;23(1):3-15.360 AORN Journal
tog. Pre-ol haveentst out-
ithal pre-easedare
slevel.risktoring
pe 2 dia-rgery.
hort-termof re-
3(6):845-
Berghen protec-22(1):
ostopera-iac sur-rs. 2008;
(NNIS)992
//wwwccessed
c syn-nsider-
MR.and per-surgeryJ Cardio-
on. http://W&
aign�
e G. Gly-e?
Glucoselin Pract.
11. Jones KW, Cain AS, Mitchell JH, et al.predicts mortality after CABG: postopecemia predicts dramatic increases in moonary artery bypass graft surgery. J Diations. 2008;22(6):1-6.
12. Malmstedt J, Leander K, Wahlberg E, KAlfredsson L, Swendenborg J. Outcomepass surgery for critical limb ischemia itients with diabetes: a population-basedDiabetes Care. 2008;31(5):887-892.
13. NICE-SUGAR Study Investigators, FinDR, Su SY, et al. Intensive versus convcontrol in critically ill patients. N Engl360(13):1283-1297.
14. Ouattara A, Lecomte P, Le Manach Yintraoperative blood glucose control iswith a worsened hospital outcome aftegery in diabetic patients. Anesthesiolo103(4):687-694.
15. Turnia M, Fry DE, Polk HC Jr. Acuteand the innate immune system: clinicamolecular aspects. Crit Care Med. 201633.
16. Wiener RS, Wiener DC, Larson RJ. Beof tight glycemic control in critically illanalysis. JAMA. 2008;300(8):933-944.
17. Pasternak JJ, McGregor DG, Schroederperglycemia in patients undergoing ceresurgery: Its association with long-term gand neuropsychological function. Mayo2008;83(4):406-417.
18. Umpierrez GE, Isaacs SD, Bazargan N,LM, Kitabchi AE. Hyperglycemia: an inmarker of in-hospital mortality in patiennosed diabetes. J Clin Endocrinol Meta978-982.
19. Loh-Trivedi M, Shwer WA. Perioperatiof the diabetic patient. Medscape. http:/.medscape.com/article/284451-overviewcessed December 2, 2011.
20. Committee on Perioperative Evaluationzilian Society of Cardiology. Steps to rerisk. In: I guidelines for perioperative eBras Cardiol. 2007;89(6):e197-208. http.gov/content.aspx?id�12237&search�ppatient�care. Accessed October 16, 201
21. Gurkan I, Wenz JF. Perioperative infectupdate for patient safety in orthopedic spedics. 2006;29(4):329-339.
22. Ohio State University Medical Center. Epractice clinical resources. In: ClinicianPeri-Operative/Peri-Procedure GlucoseRevised ed. Columbus, OH: Ohio StateMedical Center; 2010: 5, 13-16.
23. Kremen J, Dolinkova M, Krajickova J,subcutaneous and epicardial adipose tissof proinflammatory cytokines in cardiacpatients: possible role in postoperative itance. J Clin Endocrinol Metab. 2008;94620-4627.
24. Bierman AS. Functional status: the sixt
J Gen Intern Med. 2001;16(11):785-786.
Metaburr Op
patien
amar Gic manrgery
n the prdiac sPract.
t al. Thr duri
ediatedplicatites. J
CNOR,d RN firstarmel Sts Rutan
d be per-of interest
an assis-at Mountbus, OH.
iation thattentialon of this
PERIOPERATIVE HYPERGLYCEMIA www.aornjournal.org
ResourcesLjungqvist O, Nygren J, Soop M, Thorell A.
operative management: novel concepts. CCare. 2005;11(4):295-299.
Moitra VK, Meiler SE. The diabetic surgicalOpin Anaesthesiol. 2006;19(3):339-345.
Pennell L, Smith-Synder CM, Hudson LR, HWesterfield J. Practice changes in glycemand outcomes in coronary artery bypass suJ Cardiovasc Nurs. 2005;20(1):26-34.
Wellard SJ, Cox H, Bhujoharry C. Issues iof nursing care to people undergoing cawho also have type 2 diabetes. Int J Nurs13(4):222-228.
Yamashita K, Okabayashi T, Yokoyama T, eracy of a continuous blood glucose monitogery. Anesth Analg. 2008;106(1):160-163.
Zimmerman MA, Flores SC. Autoimmune-mtive stress and endothelial dysfunction: Imaccelerated vascular injury in type 1 diabe
2009;155(1):173-178.olic peri-in Crit
t. Curr
B,agementpatients.
rovisionurgery2007;
e accu-ng sur-
oxida-ons ofSurg Res.
Linda Rutan, MSN, RN, CNS-BC,CRNFA, is a clinical level 5 certifieassistant and staff nurse at Mount CAnne’s Hospital, Westerville, OH. Mhas no declared affiliation that coulceived as posing a potential conflictin the publication of this article.
Kathleen Sommers, EdD, RN, istant professor of graduate studiesCarmel College of Nursing, ColumDr Sommers has no declared affilcould be perceived as posing a poconflict of interest in the publicati
article.AORN Journal 361
.1.aorn.org/CE
EXAMINATION
CONTINUING EDUCATION PROGRAM2wwwHyperglycemia as a Risk Factor in
the Perioperative Patient
ioperative
ve
ur conve-e Exami-
PURPOSE/GOAL
To educate perioperative nurses about the risks of complication from perhyperglycemia in patients with and without a diagnosis of diabetes.
OBJECTIVES
1. Explain the causes of hyperglycemia.2. Discuss the effects of hyperglycemia.3. Identify symptoms of hyperglycemia.4. Describe interventions that nurses should consider to treat perioperati
hyperglycemia.
The Examination and Learner Evaluation are printed here for yonience. To receive continuing education credit, you must complete thnation and Learner Evaluation online at http://www.aorn.org/CE.
roceduemia etes me
y, wasadaptositive
cose
eral insulin-
ly responsestered meta-
se.
2, and 32, 3, 4, and 5
uses release ofas a result of
is.
nd 4
QUESTIONS
1. Individuals undergoing a surgical prisk for complications of hyperglycthe absence of a diagnosis of diabea. true b. false
2. Stress diabetes, or diabetes of injurmerly considered to be a beneficialsponse that promotes healing and perative outcomes.a. true b. false
3. Hyperglycemia1. causes abundant endogenous glu
production.
2. disrupts the inflammatory mechanism.362 AORN Journal ● March 2012 Vol 95
re are atven inllitus.
for-ive re-
postop-
3. impairs glucose uptake in periphdependent tissues.
4. is the end product of many bodiand dysfunctions that result in albolic conditions.
5. mutes the innate immune respon
a. 4 and 5 b. 1,c. 1, 2, 3, and 4 d. 1,
4. Stimulation of the adrenal cortex cacortisol, which causes hyperglycemia
1. muscle proteolysis.2. glycogenolysis.3. excessive hepatic gluconeogenes4. enzymatic glycosylation.
a. 1 and 3 b. 2 a
c. 1, 2, and 3 d. 1, 2, 3, and 4No 3 © AORN, Inc, 2012

feres wthat isa.
lucose
.ission
3, and2, 3, 4
operae dev
nd 42, 3, a
abdo
cellul
reas.
nd 42, 3, and 4
ioperative
ers if the pa-e level is
ery two hours’s preoperative
g/dL.ulin drip if
ose checksents in the
gns and symp-and infectionmedical
n endocrinolo-
4, and 6, 3, 4, 5, and 6
me to a con-emia is a risks.
linical editor,
have no de-
CE EXAMINATION www.aornjournal.org
5. Stimulation of catecholamines interfeedback mechanism and responsetended to help reduce hyperglycemia. true b. false
6. Studies have associated abnormal gwith1. increased lengths of hospital stay2. increased intensive care unit adm3. surgical site infections.4. neurological events.5. mortality.
a. 1 and 3 b. 2,c. 1, 2, 4, and 5 d. 1,
7. Symptoms that should alert the perinurse that the patient may have or bperioperative hyperglycemia include1. confusion.2. fruity breath.3. itchy skin.4. somnolence.
a. 1 and 3 b. 2 ac. 1, 2, and 4 d. 1,
8. Excessive adipose tissue around the1. contributes to hyperglycemia.2. is an indication of dysfunctional
metabolism.3. diverts blood flow from the panc
The behavioral objectives and examination fo
with consultation from Susan Bakewell, MS,
clared affiliations that could be perceived as posing
ith ain-
levels
s.
4, and 5
tiveeloping
nd 4
men
ar
4. works as an endocrine organ.a. 1 and 3 b. 2 ac. 1, 2, and 4 d. 1,
9. To prevent the complications of perhyperglycemia, nurses should1. consult with medical staff memb
tient’s preoperative blood glucos� 180 mg/dL.
2. perform blood glucose checks evduring surgery and if the patientblood glucose level was � 110 m
3. be prepared to implement an insneeded.
4. perform postoperative blood glucwith initial vital signs on all patipostanesthesia care unit.
5. provide patient teaching about sitoms of increased hyperglycemiaor nonhealing that would requireattention.
6. consider obtaining a referral to agist if necessary.a. 1, 3, and 5 b. 2,c. 2, 3, 5, and 6 d. 1, 2
10. Experts and researchers have not cosensus regarding whether hyperglycfactor for negative surgical outcomea. true b. false
program were prepared by Rebecca Holm, MSN, RN, CNOR, c
, director, Perioperative Education. Ms Holm and Ms Bakewell
r this
RN-BC
potential conflicts of interest in the publication of this article.
AORN Journal 363

.1.aorn.org/CE
LEARNER EVALUATION
CONTINUING EDUCATION PROGRAM2wwwHyperglycemia as a Risk Factor in
the Perioperative Patiente therograms as d
tives o
.
.
.
ould.
ase yo
l objec
tion fr
result ofr question
e? (Select all
team regard-
to change/ure.
eeting withand acceptance
valuate theintervals untilest practice.
e as a resultt all that
t relevant to
teach othersd change.port to make
we verifyhe 2.1 con-6-minute)
This evaluation is used to determinwhich this continuing education pyour learning needs. Rate the item
below.
OBJECTIVES
To what extent were the following objeccontinuing education program achieved?
1. Explain the causes of hyperglycemiaLow 1. 2. 3. 4. 5. High
2. Discuss the effects of hyperglycemiaLow 1. 2. 3. 4. 5. High
3. Identify symptoms of hyperglycemiaLow 1. 2. 3. 4. 5. High
4. Describe interventions that nurses shto treat perioperative hyperglycemiaLow 1. 2. 3. 4. 5. High
CONTENT
5. To what extent did this article increknowledge of the subject matter?Low 1. 2. 3. 4. 5. High
6. To what extent were your individuamet? Low 1. 2. 3. 4. 5. High
7. Will you be able to use the informaarticle in your work setting?
applicant who successfully completes this program
364 AORN Journal ● March 2012 Vol 95
extent tomet
escribed
f this
consider
ur
tives
om this
8. Will you change your practice as areading this article? (If yes, answe#8A. If no, answer question #8B.)
8A. How will you change your practicthat apply)1. I will provide education to my
ing why change is needed.2. I will work with management
implement a policy and proced3. I will plan an informational m
physicians to seek their inputof the need for change.
4. I will implement change and eeffect of the change at regularthe change is incorporated as b
5. Other:8B. If you will not change your practic
of reading this article, why? (Selecapply)1. The content of the article is no
my practice.2. I do not have enough time to
about the purpose of the neede3. I do not have management sup
a change.4. Other:
9. Our accrediting body requires thatthe time you needed to complete ttinuing education contact hour (12
dentialing Center
eptance of this
ers. Each
1. Yes 2. No program:
This program meets criteria for CNOR and CRNFA recertification, as well as other continuing education requirements.
AORN is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
AORN recognizes these activities as continuing education for registered nurses. This recognition does not imply that AORN or the American Nurses Creapproves or endorses products mentioned in the activity.
AORN is provider-approved by the California Board of Registered Nursing, Provider Number CEP 13019. Check with your state board of nursing for accactivity for relicensure.
Event: #12509 Session: #0001; Fee: Members $10.50, Nonmembers $21
The deadline for this program is March 31, 2015.
A score of 70% correct on the examination is required for credit. Participants receive feedback on incorrect answ
can immediately print a certificate of completion.No 3 © AORN, Inc, 2012