hyperplastic lesions and metaplastic changes of the ... · the muscle layer and extensive...
TRANSCRIPT

Hyperplastic Lesions and MetaplasticChanges of the Gallbladder
Contents
Adenomatous Hyperplasia of the Gallbladder . . . . 2Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Pathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Histopathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Differential Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2
Mucosal Hyperplasia of the Gallbladder . . . . . . . . . . 3Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Papillary Hyperplasia of the Gallbladder . . . . . . . . . . . . . 3Pathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Histopathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Differential Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Glandular Hyperplasia of the Gallbladder . . . . . . . . . . . . 4
Adenomyomatous Hyperplasia . . . . . . . . . . . . . . . . . . . . . 4Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Classification . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4Epidemiology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Clinical and Imaging Features . . . . . . . . . . . . . . . . . . . . . . . . 5Pathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Histopathology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6Differential Diagnosis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Is Adenomyomatosis a Precancerous Lesion? . . . . . . . . 7Pathogenic Pathways . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Rokitansky-Aschoff Sinuses . . . . . . . . . . . . . . . . . . . . . . . . . 7
Metaplastic Changes of the Gallbladder . . . . . . . . . . . 8Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Gastric Metaplasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Pyloric Gland Metaplasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8Antral Gland Metaplasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9Gastric Heterotopia Versus Gastric Metaplasia . . . . . . . 9Intestinal Metaplasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Squamous Cell Metaplasia . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11Other Forms of Epithelial Gallbladder Metaplasia . . . 11Mesenchymal Metaplastic Changes of the Gallbladder 11Pathogenesis . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
AbstractVarious types of hyperplastic lesions and meta-plastic changes can develop in the gallbladder.Adenomatous hyperplasia of the gallbladder isa condition characterized by a hyperplasia ofmetaplastic pyloric-type glands and of deep-seated glands in the absence of cellular atypia.Macroscopically, this alteration presents in theform of a thick and nodular gallbladdermucosa, particularly in its diffuse form, but itcan also produce polypoid lesions. The epithe-lial surface of the gallbladder and glandularepithelial can undergo focal to diffuse hyper-plastic changes. In one rare form, papillaryhyperplasia is present, usually in a diffuse pat-tern. Adenomyomatous hyperplasia is a reac-tive alteration characterized by hyperplasticand cystic changes in deep parts of the gall-bladder mucosa associated with smooth mus-cle hypertrophy. This distinct hyperplasiaexists in diffuse, segmental or annular, andlocalized or focal patterns. The gallbladderepithelium can be subject to various metaplas-tic changes, including pyloric gland metapla-sia, antral gland metaplasia, intestinalmetaplasia, and squamous cell metaplasia.
# Springer International Publishing Switzerland 2016A. Zimmermann, Tumors and Tumor-Like Lesions of the Hepatobiliary Tract,DOI 10.1007/978-3-319-26587-2_154-1
1

Adenomatous Hyperplasiaof the Gallbladder
Introduction
Adenomatous hyperplasia of the gallbladder(AHGB) is a condition characterized by a hyper-plasia of metaplastic pyloric-type glands and ofdeep-seated glands in the absence of cellularatypia. AHGB is sometimes interpreted as apseudotumor of the gallbladder and has noknown malignant potential so far (Christensenand Ishak 1970; Lee et al. 2004). The lesion hasbeen included in the spectrum of cholecystitisglandularis proliferans, but AHGB can clearlydevelop in the absence of inflammatory changeof the gallbladder (Kikiros et al. 2003).
Epidemiology
AHGB is often considered to be a rare lesion, butthe incidence is difficult to assess owing to thelack of a consensus regarding diagnostic criteria(Piegza et al. 1978; Farinon et al. 1991; Tyagiet al. 1992; Baig et al. 2002; Kikiros et al. 2003;Stokes et al. 2007). Christensen and Ishak (1970)reviewed 180 tumors and pseudotumors of thegallbladder and identified AHGB in 18 cases/10 %. Elfving et al. (1969) reported the gallblad-der mucosal hyperplasia was present in 22 % oftheir 104 patients who had presented with calcu-lous cholecystitis. In a morphologic investigationof 415 cholecystectomy specimens, AHGB wasdetected in 10.1 % of the gallbladders (Tyagiet al. 1992). In a series of 40 patients from Indiawith cholelithiasis undergoing cholecystectomy, adetailed histologic examination with numeroussections revealed five cases of AHGB. In a retro-spective study evaluating gallbladder wall thick-ening in 342 patients who had undergone MRcholangiography prior to cholecystectomy,144 patients revealed wall thickening defined asa wall thickness of 3 mm or more, and amongthese, no case of AHGB was found (Junget al. 2005). The lesion is much rare in men thanin females, with an estimated male to female ratio
of 1:13 (Tyagi et al. 1992). Interestingly, AHGBwas not seen in gallbladders containing pigmentstones, but found in gallbladders containingmixed or cholesterol stones (Baig et al. 2002).AHGB has been observed in the pediatric agegroup (Kikiros et al. 2003).
Pathology
MacroscopyMacroscopically, AHGB has been described aslesion with a thick and nodular gallbladdermucosa, at least in the diffuse form (Stokeset al. 2007). It can present as polypoid lesions(Farinon et al. 1991; Kikiros et al. 2003), thepolyps being usually small but sometimes clus-tered to small groups of exophytic lesions.
Histopathology
AHGB is a focal or diffuse lesion (Tyagiet al. 1992). Histologically, the mucosa revealselongated papillary folds with a fibrotic core anda mild lymphocytic infiltrate. The surface showshyperplasia of metaplastic pyloric-type glands,while branching mucous glands are found indeeper layers, focally filling the lamina propria.Numerous deep-seated Rokitansky-Aschoffsinuses are common (Stokes et al. 2007). In con-trast to adenomyomatosis, hypertrophy of themuscularis is not a feature in AHGB. Cellularatypia is consistently lacking. Tyagi andcoworkers (1992) distinguished two types ofAHGB: (1) spongious type described asprolonged but coalesced villi and (2) villoustype, characterized by abnormally long and ram-ifying villi. In their material of 415 cholecystec-tomy specimens, 33.3 %were type 1, 52.4 %weretype 2, and 14.3 % were mixed types.
Differential Diagnosis
Adenomyomatosis of the gallbladder resembles inseveral aspects AHGB, but shows hypertrophy of
2 Hyperplastic Lesions and Metaplastic Changes of the Gallbladder
the muscle layer and extensive Rokitansky-Aschoff sinuses.
Mucosal Hyperplasiaof the Gallbladder
Introduction
The surface epithelium and glandular epithelia ofthe gallbladder mucosa can undergo focal to dif-fuse hyperplastic changes that may be confoundedwith precursor lesion of cancer.
Papillary Hyperplasiaof the Gallbladder
IntroductionPapillary hyperplasia of the gallbladder (PHGB)is a rare mucosal change characterized by a usu-ally diffuse benign papillary proliferation of gall-bladder epithelia (Albores-Saavedra et al. 1990).PHGB comes in two forms, i.e., primary PHGBand secondary PHGB often associated withpancreaticobiliary maljunction. As, in addition tothe gallbladder, other parts of the biliary tract canbe involved, PHGB may represent an organ-specific manifestation of a systemic biliary disor-der. PHGB is usually not found incholecystolithiasis.
Primary PHGB is a disorder that develops inthe entire gallbladder mucosa in the absence ofrelevant background chronic inflammation-related gallbladder or bile duct disease. It hasfirst been reported in 1990 based on the observa-tion of a young female patient with a papillaryhyperplastic lesion involving the mucosa of theentire gallbladder and the cystic and common bileducts (Albores-Saavedra et al. 1990). Few otherdescriptions of this condition have since appeared(Celoria et al. 1994; Huang et al. 2001; Stringer etal. 2001; Umudum et al. 2006; Baba et al. 2014).The etiology of primary PHGB is not yet known.
Secondary PHGB is well known to develop inpatients with pancreaticobiliary maljunction(PBMJ) (Yamato et al. 1999; Yamaguchi
et al. 2009). PHGB in PBMJ exhibits senescentfeatures including expression of p16(INK4A) andsenescent-associated beta-galactosidase, lowexpression of the polycomb group proteinEZH2, and low or increased proliferative activity.In contrast, secondary PHGB in PBMJ showingtransformation into cancer showed upregulationof EZH2 (Yamaguchi et al. 2009).
Pathology
MacroscopyMacroscopically, the gallbladder mucosa may bethickened and exhibits an increased granularity ofits surface or a diffuse velvety structure, some-times with tiny frond-like excrescences. In theinvestigation of Albores-Saavedra et al. (1990),the gallbladder mucosa was pink-yellow and borenumerous small papillary projections rangingfrom 0.2 to 0.8 cm in height.
Histopathology
Histologically, mucosal folds of the gallbladderare close to one another and taller than normal(Albores-Saavedra et al. 1990). The folds presenta villous or papillary pattern with abnormalbranching. The hyperplastic-hypertrophic foldsare lined by normal-looking-well-differentiatedcolumnar epithelial cells, usually without atypiain primary PHGB. The nuclei are basally or cen-trally placed. Part of cells exhibit subnuclear vac-uoles, and an increased number of pencil-like cellsare admixed with the columnar cells. Paneth cells,goblet cells, or argyrophilic cells are not present.In secondary PHGB, focal cellular and nuclearatypia/dysplasia can be found, precursor lesionsof papillary gallbladder carcinoma associatedwith PBMJ (Kinoshita et al. 2002). In the vicinityof papillary to papillary-tubular carcinoma inPBMJ, atypical epithelial hyperplasia wasdescribed (Ohta et al. 1990). The nonneoplasticepithelium of secondary PHGB in PBMJ canexpress mucin core protein MUC1, similar togallbladder carcinoma (Yamato et al. 1999). It
Mucosal Hyperplasia of the Gallbladder 3

has been proposed that reflux of pancreatic juicecaused by maljunction may induce a distinct formof chronic inflammatory change in the gallbladderfavoring the development of hyperplasic, dysplas-tic, and finally neoplastic alterations.
Differential Diagnosis
Differential diagnosis of PHGB includespapillomatosis of the gallbladder, multiple villousadenomas, and highly differentiated papillarycarcinoma.
Glandular Hyperplasiaof the Gallbladder
Glandular hyperplasia is a rare form of mucosalhyperplasia. It was observed in a small child withcholedochal cyst, where the gallbladder mucosadisplayed cribriform proliferation of the glandbase of the mucosa, associated with the presenceof hyperplastic glandular structures within lymphvessels, but in the absence of malignant change(Hirayama et al. 2009).
Adenomyomatous Hyperplasia
Introduction
Adenomyomatous hyperplasia/adenomyomatosisof the gallbladder (synonyms: diverticular diseaseof the gallbladder, adenomyosis of the gallblad-der, cholecystitis glandularis proliferans, intramu-ral diverticulosis of the gallbladder) is a well-recognized reactive alteration of the gallbladder,characterized by hyperplastic and cystic changesof deep parts of the mucosal epithelium associatedwith muscle hypertrophy. Together withcholesterolosis, adenomyomatosis has been allo-cated to a group of disorders termed hyperplasticcholecystoses, a term denoting reactive, benignalterations sharing a hyperplastic reaction ofmucosal cells (Jutras 1960; Halin 1964; Feltner1966; Jelaso et al. 1967; Lubera et al. 1967;
Govoni 1981; Berk et al. 1983). It seems thatmost of the cases previously described as chole-cystitis cystica in fact representadenomyomatosis.
Selected References Eiserth 1938; Akerlundand Rudhe 1950; Caroli et al. 1951; King 1952,1953; Zinober 1952; Burt and Masel 1955; Rosset al. 1955; Le Quesne and Ranger 1957; Rushet al. 1957; Goldberg and Dodgson 1958; Ludin1960; Halpert 1961; Verhage and Van der Werff1964; Brown et al. 1966; reviews: Owen andBilhartz 2003.
Classification
Based on the distribution pattern and the exten-sion of the lesions, adenomyomatosis is dividedinto three major types (Table 1).
Mass-forming lesions in localized or segmen-tal adenomyomatosis are sometimes termedadenomyoma (Eiserth 1938; Maderna and Tritto1959; Young 1959; Andrei and Nobile 1960;Caldone Firrao 1960; Ochsner 1962; Bricker andHalpert 1963; Jutras et al. 1964; Levesqueet al. 1964; Tompkins 1967; Inoue and Matsuda1978; Herrmann and Saul 1986). Anadenomyoma is defined as a nodular mural lesioncomposed of fascicles of smooth muscle cells andclusters of dilated, hyperplastic biliary-typeglands. The term is misleading insofar as“adenomyomas” developing in the setting ofadenomyomatosis are not true benign neoplasms,but reactive nodular lesions. Focal/isolatedadenomyomas mostly occur in the gallbladderfundus (Eiserth 1938).
Table 1 Types of adenomyomatosis
Diffuse (generalized) adenomyomatosis, in which theentire gallbladder mucosa is involved
Segmental (annular) adenomyomatosis, whereby onlyone gallbladder segment is involved, with a ringlikeinvolvement of one gallbladder part
Localized (focal) adenomyomatosis, whereby only acircumscribed part is involved, most often in thegallbladder fundus
4 Hyperplastic Lesions and Metaplastic Changes of the Gallbladder

Epidemiology
Lesions of the adenomyomatosis spectrum werefirst described by Sutherland (1898) and Eiserth(1938) under the term adenomyoma of the gall-bladder. Since then, this entity has been furthercharacterized in numerous reports. It seems thatadenomyomatosis is detectable in 2–5 % of allcholecystectomies. In a study of 4,704 consecu-tive cholecystectomies, adenomyomatosis wasdetected in 2.4 % (Kim et al. 2010). In a furtheranalysis of 30 patients, age at diagnosis rangedfrom 22 to 77 years (mean, 52.3 years), andthe male to female ratio was 8:7. Twelve caseswere segmental, ten were diffuse/generalized,and eight were fundal lesions. In 20 patients, thelesions were associated with gallstones (Kasaharaet al. 1992). Gallbladder adenomyomatosisalso occurs in the pediatric age group(Alberti et al. 1998; Zani et al. 2005; Akçamet al. 2008).
Selected References Colquhoun 1961; Katz andRickard 1963; Fotopoulos and Crampton 1964;Seyss 1966; Bevan 1970; Heald 1970; Davies1971; Frommhold and Lagemann 1971; McCor-mick and Lang 1971; Skapinker 1971; Ram andMidha 1975; Muto et al. 1978; Hidalgo andLewicki 1980; Meguid et al. 1984; Kidneyet al. 1986; Williams et al. 1986; Costa-Greco1987; Halpert et al. 1989; Kasahara et al. 1992;Yang et al. 1996; Chang et al. 1998; Secilet al. 2005; Boscak et al. 2006; Dirks et al. 2006;Lin et al. 2011; Ray et al. 2012.
Clinical and Imaging Features
In most patients, adenomyomatosis is clinicallysilent. Some patients report vague abdominalpain or occasional colics, but these may becaused by accompanying gallstone disease. Infact, adenomyomatosis is often associated withcholecystolithiasis. Specifically, the segmentalvariant of adenomyomatosis seems to predis-pose to cholecystolithiasis (Nishimuraet al. 2004). Among 64 cases of
adenomyomatosis, 38 had black pigment stones,alone (N = 22) or in association with singe(N = 12) or multiple (N = 4) cholesterol gall-stones. At least in initial phases of stone forma-tion, Rokitansky-Aschoff sinuses were foundclose to small intraparietal vessels, and some-times they contained black pigment microstones(Cariati and Cetta 2003). A subset of gallbladderadenomyomatosis is associated with anomalouspancreatobiliary ductal union (Wu et al. 1995;Chang et al. 1998). The fundal (localized) typeof adenomyomatosis seems to differ from theother types in several respects. It has a lowerfrequency of gallstones and a lower inflamma-tory grade (Kim et al. 2010).
Sonographically, the main feature is a localizedor generalized thickening of the gallbladder wallwith a generally smooth outer contour. Smallintramural cysts are identifiable in part of thecases, and gallbladder contractility is preserved,in contrast to malignancy (Rice et al. 1981;Raghavendra et al. 1983; Sagar and Naik 1984;Izumi et al. 1985; Fowler and Reid 1988; Brambset al. 1990; Gerard et al. 1990; Hwang et al. 1998).The intramural foci may show “comet tail” rever-beration artifacts, indicative of cholesterol crys-tals within Rokitansky-Aschoff sinuses. These“comet tails” extend from the near wall into theanechoic lumen (Boscak et al. 2006; Mariani andHsue 2011). Postcontrast CT images demonstratethe characteristic rosary sign or necklace sign,formed by the enhanced epithelial structures inthe intramural diverticula surrounded by thenon-enhancing hypertrophied muscle tissue(Chao et al. 1992; Zissin et al. 2003; Chinget al. 2007; Poonam et al. 2008; Stunellet al. 2008). The rosary or necklace signs aremostly found in the diffuse form ofadenomyomatosis, while the segmental formoften presents as a dumbbell-shaped gallbladder,and the localized form either presents as a polyp-oid structure or a nodular mass lesion(“adenomyoma”). The so-called pearl necklacesign is a typical feature of adenomyomatosis andis also well visualized at magnetic resonancecholangiopancreatography (MRCP; Haradomeet al. 2003). The pocket-like wall lesions are best
Adenomyomatous Hyperplasia 5
seen on CT in the fundal type ofadenomyomatosis (Klose et al. 1991). In markedadenomyomatosis, CT imaging may result in find-ings mimicking gallbladder carcinoma (Agrawalet al. 2012). OnMR, T1-weighted images reveal adiffusely thickened gallbladder wall and intramu-ral cavities, which are hyperintense onT2-weighted images. The cavities representRokitansky-Aschoff sinuses (Yoshimitsuet al. 1999; Boscak et al. 2006). The phenotypeof nonneoplastic and neoplastic gallbladder dis-ease as displayed on MR images has been dividedinto four layered patterns, viz., type 1 shows twolayers with a thin hypointense inner layer andthick hyperintense outer layer; type 2 has twolayers of ill-defined margin; type 3 reveals multi-ple hyperintense cystic spaces in the gallbladderwall; and type 4 shows a diffuse nodular thicken-ing without layering. Adenomyomatosis was cor-related with type 3, while types 1 and 2 weretypical for chronic and acute cholecystitis, respec-tively, and type 4 was a characteristic for gallblad-der carcinoma (Jung et al. 2005).
Pathology
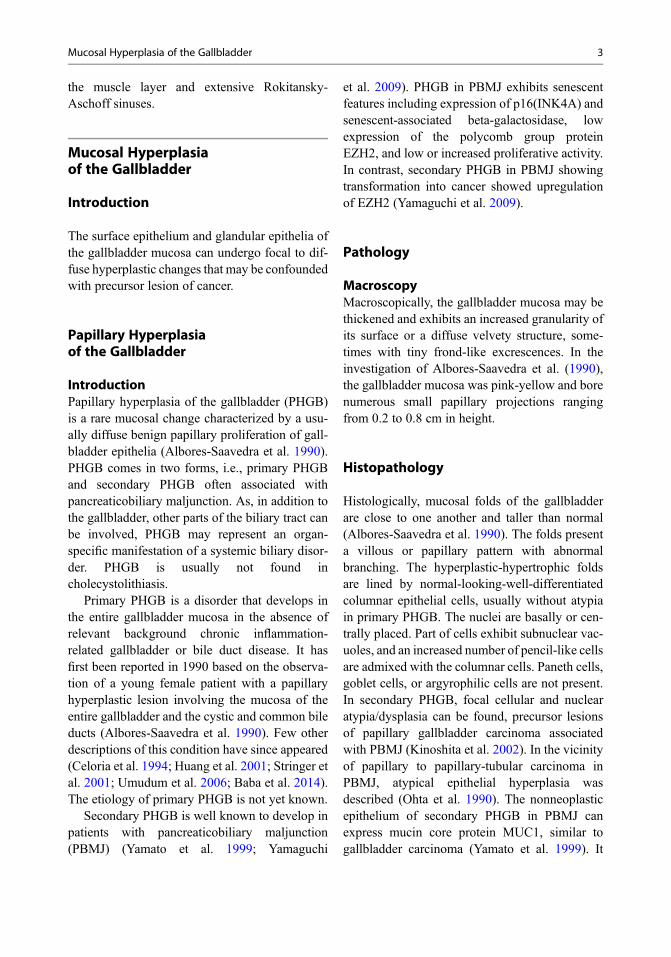
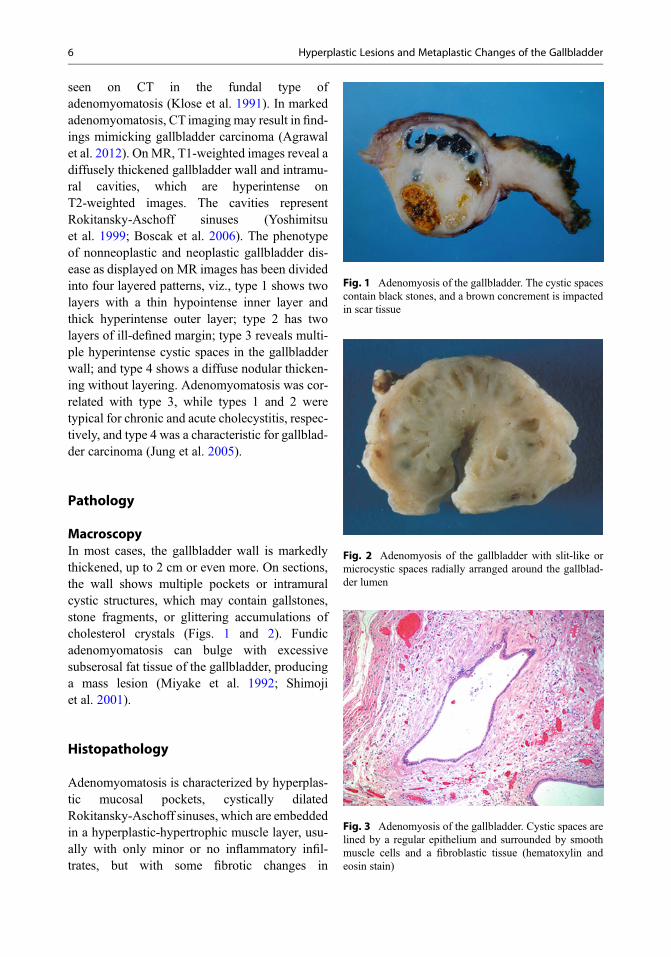
MacroscopyIn most cases, the gallbladder wall is markedlythickened, up to 2 cm or even more. On sections,the wall shows multiple pockets or intramuralcystic structures, which may contain gallstones,stone fragments, or glittering accumulations ofcholesterol crystals (Figs. 1 and 2). Fundicadenomyomatosis can bulge with excessivesubserosal fat tissue of the gallbladder, producinga mass lesion (Miyake et al. 1992; Shimojiet al. 2001).
Histopathology
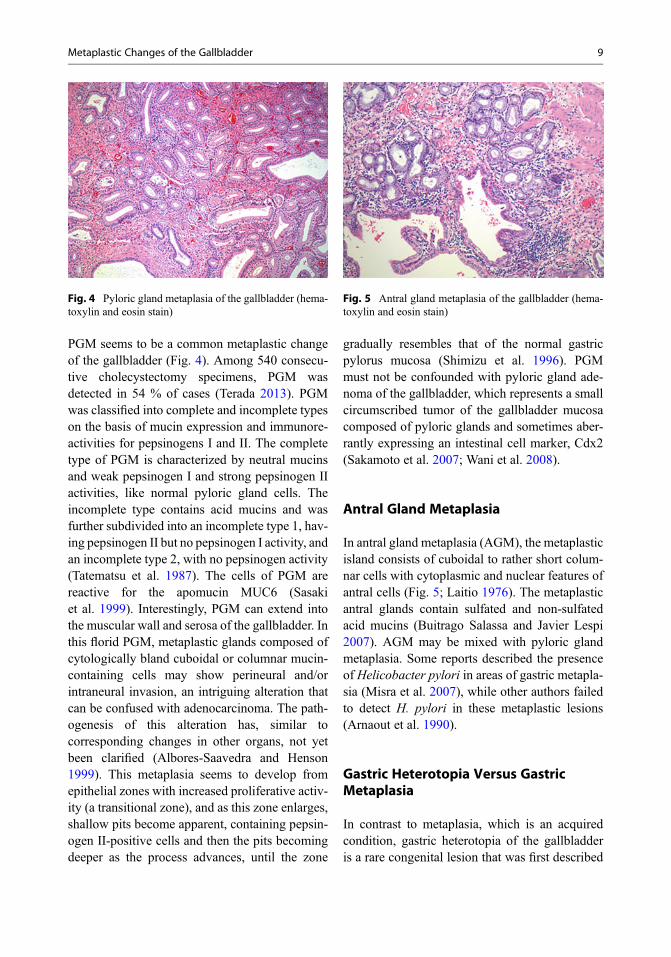
Adenomyomatosis is characterized by hyperplas-tic mucosal pockets, cystically dilatedRokitansky-Aschoff sinuses, which are embeddedin a hyperplastic-hypertrophic muscle layer, usu-ally with only minor or no inflammatory infil-trates, but with some fibrotic changes in
Fig. 1 Adenomyosis of the gallbladder. The cystic spacescontain black stones, and a brown concrement is impactedin scar tissue
Fig. 2 Adenomyosis of the gallbladder with slit-like ormicrocystic spaces radially arranged around the gallblad-der lumen
Fig. 3 Adenomyosis of the gallbladder. Cystic spaces arelined by a regular epithelium and surrounded by smoothmuscle cells and a fibroblastic tissue (hematoxylin andeosin stain)
6 Hyperplastic Lesions and Metaplastic Changes of the Gallbladder

advanced stages of the disease (Fig. 3). In part ofthe cases, Rokitansky-Aschoff sinuses are veryprominent and appear as elongated and dilated,sometimes cystic epithelial pockets resemblingdiverticula. Hyperplastic changes may also benoted in more superficial epithelia of the mucosa.The mucosal pockets (Rokitansky-Aschoffsinuses) often contain inspissated bile, in part ofthe cases intermingled with stones, stone frag-ments, and/or cholesterol crystals. Adenomyoma,mostly seen in the fundal variant ofadenomyomatosis (Ozgonul et al. 2010), is char-acterized by a nodule, predominantly fundic, ofhypertrophic smooth muscle cells, containingdistorted and in part cystically dilated glandularstructures.
Differential Diagnosis
Radiologically, gallbladder cancer withintratumoral anechoic foci can be a mimic ofadenomyomatosis (Ishizuka et al. 1998). Well-differentiated gallbladder adenocarcinoma withintratumoral cystic components and abundantmucin production may mimic adenomyomatosis(Yoshimitsu et al. 2005).
Is Adenomyomatosis a PrecancerousLesion?
So far, it is not known whether adenomyomatosishas any clinical significance and whether it willtruly lead to inflammation or even cancer (Chan-Wilde et al. 1990). Based on the observation ofdysplastic changes and the association of gall-bladder carcinoma with adenomyomatosis, it hasbeen suggested that adenomyomatosis mightrepresent a premalignant condition (Bevan1970; Aldridge et al. 1991; Funabikiet al. 1993; Kurihara et al. 1993; Imaiet al. 2011). Diffuse adenomyomatosis wasfound to be associated with dysplastic gallblad-der adenoma (Di Carlo et al. 2010). There is onereported case of papillary mucinous adenomaarising in adenomyomatous hyperplasia of thegallbladder (Lauwers et al. 1995). Early
gallbladder adenocarcinoma has been found inassociation with adenomyomatosis (Fujitaet al. 1988). A causal relationship betweenadenomyomatosis and carcinoma has beensuggested based on a close spatial relationshipof the two lesions (Paraf and Potet 1988). In onecase, noninvasive carcinoma of the gallbladderwas found in the mucosa overlying localized typeof adenomyomatosis with a papillary adenoma inone of the cystic structures (Katoh et al. 1988).There is some evidence that the segmental formof adenomyomatosis predisposes to gallbladdercarcinoma (Ootani et al. 1992; Kai et al. 2011). Ina study of 4,560 consecutive patients undergoingcholecystectomies, 60 clinically noncancerousgallbladders with segmental adenomyomatosiswere examined for epithelial alterations. Histol-ogy revealed previously unrecognized carcinomain 6.6 % of cases, while the other types ofadenomyomatosis did not show any significantincrease in the incidence of gallbladder cancer,suggesting that segmental adenomyomatosismay represent a high-risk condition for carci-noma, especially in elderly patients (Nabatameet al. 2004).
Pathogenic Pathways
Etiology and pathogenesis of adenomyomatosisare not known. A pathogenic role of an increasedintra-gallbladder pressure has been suggested,with a pressure-induced dilatation and prolifera-tion of Rokitansky-Aschoff sinuses, but thismechanistically oriented hypothesis fails to haveany support.
Rokitansky-Aschoff Sinuses
Rokitansky-Aschoff sinuses (RAS or crypts),already discussed in the previous paragraph asa component of adenomyomatosis, are intramu-ral diverticulum-like invaginations of gallblad-der epithelium with an associated sheath offibroblastoid cells with extracellular matrix.RAS extend down the gallbladder wallthrough smooth muscle gaps. The deep-most
Rokitansky-Aschoff Sinuses 7

reaching RAS reach the peri-/extra-muscularconnective tissue (Zinober 1952; Rosset al. 1955; Rush et al. 1957; Halpert 1961;reviews: Albores-Saavedra and Henson 1984;Albores-Saavedra et al. 1998). In addition totheir role in adenomyomatous hyperplasia,RAS are commonly found in gallbladderresection specimens irrespective of the presenceof bona fide adenomyomatosis. In a Japaneseseries of 540 consecutive cholecystectomies,RAS were detected in 65 % of cases (Terada2013).
Histologically, RAS are pocket-like, long, andoften tortuous invaginations lined by a singlelayer of biliary-type columnar cells. At the bot-tom, RAS may show considerable branching,mainly at the gallbladder outlet and the first partof the cystic duct, causing crowded epithelialtubular clusters that may be confounded withwell-differentiated adenocarcinoma. However,in contrast to carcinoma, epithelia of RAS lackany relevant atypia, reveal no increased mitoticactivity, are in continuation with the mucosalsurface, show an organoid/lobular texture, andlack the cellular stroma characterizing carci-noma. In addition, cells of RAS are not reactivefor p53 protein and exhibit a very low prolifera-tive activity based on MIB1 immunostaining(Dorantes-Heredia et al. 2013). RAS may accu-mulate mucin in their lumina which sometimesescapes into the extracellular space, simulatingmucinous carcinoma of the gallbladder, but againthe participating cells are p53 negative and lowproliferative (Albores-Saavedra et al. 2009). Inthe course of chronic fibrosing cholecystitis, thenecks of RAS may be stenosed or even obliter-ated, causing fluid stasis followed by cystic dila-tation, sometimes with trapping of thickenedbile, cholesterol crystals, or stones in the lumina.The etiology and pathogenesis of RAS are notyet known, although factors such as increasedluminal pressure and weakness of the musclelayer have been discussed. It has also been pro-posed that chronic cholecystitis may weakenmural muscle bundles and hence reduce theircapability to resist to outpouchings (Stalkeret al. 1955).
Metaplastic Changesof the Gallbladder
Introduction
Similar to other organs of the gastrointestinaltract, the mucosa of the gallbladder can undergoseveral types of epithelial metaplasia, gastricmetaplasia and intestinal metaplasia being themost common forms (Pessel et al. 1950). Apartfrom its differential diagnostic importance, meta-plasia plays a role as a potential precursor lesionfor carcinogenic pathways (Yamagiwa andTomiyama 1986; Inada et al. 1989; Duarteet al. 1993; Lewis et al. 2007; Meirelles-Costaet al. 2010), an issue further discussed in thechapter on gallbladder carcinoma.
Gastric Metaplasia
General FeaturesGastric gland metaplasia of the gallbladder isdefined as the presence of gastric-type glands,either single or in groups, within the mucosa(lamina propria) or, less commonly, in themuscularis of the gallbladder. The areas of gastricmetaplasia can contain pyloric, antral or mucousglands, or mixtures thereof. Neuroendocrine cellsmay also occur (Yamamoto et al. 1986). The fre-quency of gastric metaplasia of the gallbladdervaries considerably among reports, ranging from66 % to more than 80 %. The metaplastic changesare often associated with chronic cholecystitis,and formation of lymph follicles (cholecystitisfollicularis) has been found in association withmetaplasia, but mainly in cases with H. pyloriinfection (Misra et al. 2007). Gastric metaplasiamay also occur within adenocarcinomas of thegallbladder (Azadeh and Parai 1980).
Pyloric Gland Metaplasia
Pyloric gland metaplasia (pseudopyloric glandmetaplasia) is identified in several parts of thegastrointestinal tract, including the gallbladder.
8 Hyperplastic Lesions and Metaplastic Changes of the Gallbladder
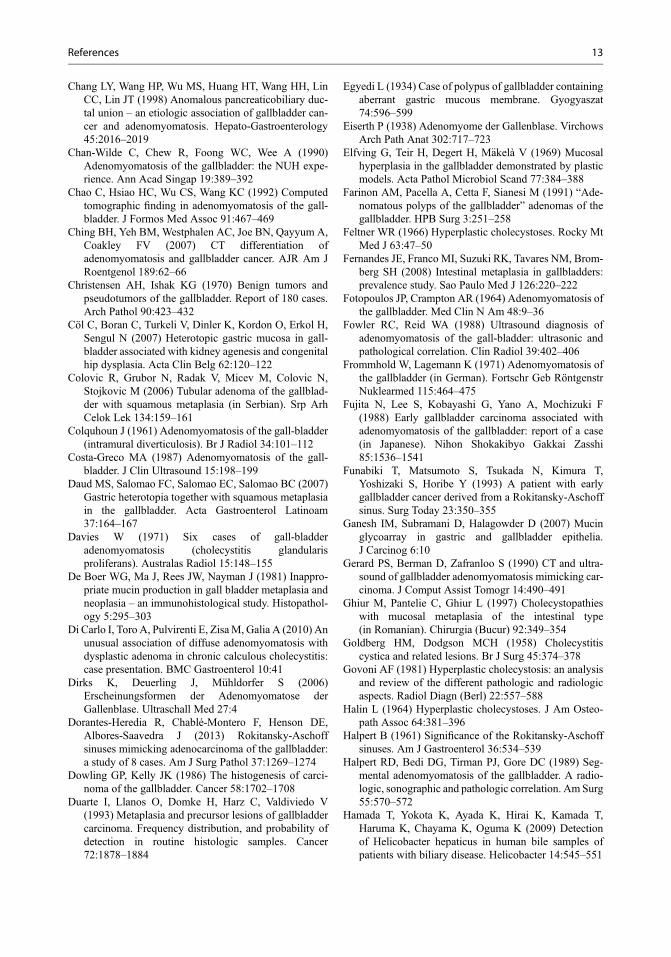
PGM seems to be a common metaplastic changeof the gallbladder (Fig. 4). Among 540 consecu-tive cholecystectomy specimens, PGM wasdetected in 54 % of cases (Terada 2013). PGMwas classified into complete and incomplete typeson the basis of mucin expression and immunore-activities for pepsinogens I and II. The completetype of PGM is characterized by neutral mucinsand weak pepsinogen I and strong pepsinogen IIactivities, like normal pyloric gland cells. Theincomplete type contains acid mucins and wasfurther subdivided into an incomplete type 1, hav-ing pepsinogen II but no pepsinogen I activity, andan incomplete type 2, with no pepsinogen activity(Tatematsu et al. 1987). The cells of PGM arereactive for the apomucin MUC6 (Sasakiet al. 1999). Interestingly, PGM can extend intothe muscular wall and serosa of the gallbladder. Inthis florid PGM, metaplastic glands composed ofcytologically bland cuboidal or columnar mucin-containing cells may show perineural and/orintraneural invasion, an intriguing alteration thatcan be confused with adenocarcinoma. The path-ogenesis of this alteration has, similar tocorresponding changes in other organs, not yetbeen clarified (Albores-Saavedra and Henson1999). This metaplasia seems to develop fromepithelial zones with increased proliferative activ-ity (a transitional zone), and as this zone enlarges,shallow pits become apparent, containing pepsin-ogen II-positive cells and then the pits becomingdeeper as the process advances, until the zone
gradually resembles that of the normal gastricpylorus mucosa (Shimizu et al. 1996). PGMmust not be confounded with pyloric gland ade-noma of the gallbladder, which represents a smallcircumscribed tumor of the gallbladder mucosacomposed of pyloric glands and sometimes aber-rantly expressing an intestinal cell marker, Cdx2(Sakamoto et al. 2007; Wani et al. 2008).
Antral Gland Metaplasia
In antral gland metaplasia (AGM), the metaplasticisland consists of cuboidal to rather short colum-nar cells with cytoplasmic and nuclear features ofantral cells (Fig. 5; Laitio 1976). The metaplasticantral glands contain sulfated and non-sulfatedacid mucins (Buitrago Salassa and Javier Lespi2007). AGM may be mixed with pyloric glandmetaplasia. Some reports described the presenceof Helicobacter pylori in areas of gastric metapla-sia (Misra et al. 2007), while other authors failedto detect H. pylori in these metaplastic lesions(Arnaout et al. 1990).
Gastric Heterotopia Versus GastricMetaplasia
In contrast to metaplasia, which is an acquiredcondition, gastric heterotopia of the gallbladderis a rare congenital lesion that was first described
Fig. 4 Pyloric gland metaplasia of the gallbladder (hema-toxylin and eosin stain)
Fig. 5 Antral gland metaplasia of the gallbladder (hema-toxylin and eosin stain)
Metaplastic Changes of the Gallbladder 9

in 1934 (Egyedi 1934). The lesion is discussed inmore detail in a separate paragraph and may beconfounded with gastric metaplasia of the gall-bladder (Yamamoto et al. 1989). The diagnosisrequires the identification of a focus composedof an entire (full-thickness) gastric-type mucosa,usually fundic, with PAS-positive foveolar cells,chief and parietal cells, and sometimes abundantpyloric glands (Isik et al. 2002; Ben Brahimet al. 2011). Gastric heterotopia often forms abulged mucosal area or a polypoid lesion andless commonly an intramural nodular mass(Boyle et al. 1992; Vallera and Dawson 1992;Uchiyama et al. 1995; Leyman et al. 1996;Hamazaki and Fujiwara 2000; Sciumèet al. 2005; Cöl et al. 2007), whereas metaplasticlesions are commonly flat. Furthermore, gastricheterotopia is detected more frequently in youn-ger adults and is mostly found in the gallbladderneck or even in the cystic duct (Isik et al. 2002),whereas metaplasia shows a more extended dis-tribution. Gastric heterotopia may be associatedwith focal intestinal metaplasia with goblet cellsin the surrounding gallbladder mucosa(Xeropotamos et al. 2001; Isik et al. 2002; Tavliet al. 2005).
Intestinal Metaplasia
Intestinal metaplasia (IM) of the gallbladder ischaracterized by the presence of areas composedof intestinal columnar cells, goblet cells, neuroen-docrine cells and Paneth cells, and a distinctmucin expression mode (Ganesh et al. 2007).Complete IM was found in 9.8–85.7 % of gall-bladders with gallstone disease, mainly in patientsless than 40 years of age (J€arvi and Laurén 1967;Kozuka and Hachisuka 1984; Dowling and Kelly1986; Yamagiwa and Tomiyama 1986; Yamagiwa1989; Jukemura 1996; Ghiur et al. 1997;Mukhopadhyay and Landas 2005; Fernandeset al. 2008; Sakamoto et al. 2009; Khanet al. 2011), but there are also reports withmarkedly lower frequencies of IM in cholelithia-sis, e.g., 5.4 % (Jukemura 1996). Apart fromgeographical and genetic differences, variationsin criteria used to identify IM may play a role for
these marked differences. It was claimed that thefrequency of IM increases as a function of increas-ing age, but this was not confirmed in all reports.Specifically, one study found a peak in incidencein individuals younger than 40 years (Fernandeset al. 2008). Histologic features consistent withIM were also identified in the pediatric age group,where the presence of intestinal gallbladder fea-tures seems to be a physiological trait (Zenet al. 2011). On the other hand, IM of the gall-bladder in children has also been observed in thesetting of pancreaticobiliary maljunction (Onoet al. 2011). Goblet cells are a feature of IM, buttheir mere presence as such does not suffice for adiagnosis of IM. Goblet cells were detected inmore than half of gallbladder specimens in onestudy (Laitio 1980). Sporadic goblet cells com-monly occurred in so-called goblet cell areaswhich, as small lesions, are usually located inthe tops of gallbladder mucosal folds. IMdevelops when goblet cells also involve deeperparts of folds, associated with a change fromsulfated mucins to non-sulfated mucins and theemergence of intestinal-type columnar cells andeventually enterochromaffin cells (Laitio 1975;Laitio and Nevalainen 1975a). Less commonly,IM can also contain Paneth cells (Laitio andNevalainen 1975b). Ultrastructurally, interveningcolumnar cells (enterocyte-like cells) containcytoplasmic mucin granules (Laitio andNevalainen 1975b). IM cells express large intes-tinal mucin antigen/LIMA and small intestinalmucin antigen/SIMA (De Boer et al. 1981).Cells of IM are reactive for the transcription fac-tor, Cdx2 (Sakamoto et al. 2007, 2009). Based onthe absence of the presence of endocrine cells,Albores-Saavedra and coworkers (1986) dividedIM into two groups. The gallbladder with IMlacking endocrine cells contained isolated orsmall clusters of mature goblet cells, while thosewith endocrine cells, in addition to goblet cells,contained argyrophil and argentaffin cells and,less frequently, Paneth cells and gland-like struc-tures resembling colonic crypts. Both groupsshowed pyloric gland and superficial gastric-typeepithelium. The most common endocrine cellswere serotonin-positive elements. Based on thesefindings, the involvement of an endodermal stem
10 Hyperplastic Lesions and Metaplastic Changes of the Gallbladder

cell was suggested (Albores-Saavedraet al. 1986).
Squamous Cell Metaplasia
This is, in comparison with other forms of meta-plasia, one of the least common variants. It ischaracterized by the replacement of a glandulargallbladder epithelium by a stratified squamouscell epithelium (keratinocytes) with or withoutkeratinization (Fig. 6). Massive and diffuse squa-mous cell metaplasia with keratinization canresult in a pseudoepidermoid cyst of the gallblad-der, mimicking a gallbladder tumor (Teoet al. 2005). Extended squamous cell metaplasiaof the gallbladder with dysplastic changescan occur in association with squamous cellcarcinoma (Hanada et al. 1986). A component ofsquamous cell metaplasia was found ingastric heterotopia of the gallbladder (Daudet al. 2007) and in a tubular adenoma (Colovicet al. 2006).
Other Forms of Epithelial GallbladderMetaplasia
Ciliated gallbladder epithelium has been observedin a patient with duplication of the gallbladder(Raeburn 1969).
Mesenchymal Metaplastic Changesof the Gallbladder
Osseous metaplasia (or heterotopic bone) is a veryrare alteration of the gallbladder, sometimes asso-ciated with chronic cholecystitis (II’chenkoet al. 2011; Rege and Vargas 2011). This type ofmetaplasia can present as a focal hyperdenselesion that may be confounded with a gallstone(Nelson and Kahn 2009). Osseous gallbladdermetaplasia was observed in association with pol-ypoid cholesterolosis (Ortiz-Hidalgo andBaquera-Heredia 2000). A similar type of meta-plasia rarely develops in the stroma of gallbladdercarcinomas (stromal osseous metaplasia; Cavazzaet al. 1999).
Pathogenesis
Similar to other organs having a glandularmucosa, metaplastic changes in the gallbladderare thought to be caused, or their developmentfavored, by chronic inflammatory disease, butthe exact pathogenic pathways are not yet eluci-dated. There is recent evidence that severalenterohepatic Helicobacter (H.) species canoccur in inflammatory disorders and gallstonedisease of the gallbladder and may play a patho-genic role, including H. hepaticus, H. bilis,H. pullorum, and H. pylori (Apostolovet al. 2005; Kobayashi et al. 2005; Hamadaet al. 2009; Karagin et al. 2010; Lee et al. 2010;Boonyanugomol et al. 2012; Attaallah et al. 2013;Javed et al. 2013). Helicobacter infection of gall-bladder mucosa in patients with chronic cholecys-titis was associated with metaplasia (Zhouet al. 2013). In one study, H. pullorum was onlyfound in gallbladders with metaplasia (Karaginet al. 2010).
References
Agrawal S, Khurana J, Daruwala C (2012) Gallbladderadenomyomatosis: a malignant masquerader. DigLiver Dis 44:e23
Fig. 6 Squamous cell metaplasia of the gallbladder(hematoxylin and eosin stain)
References 11

Akçam M, Buyukyavuz I, Ciris M, Eris N (2008)Adenomyomatosis of the gallbladder resembling hon-eycomb in a child. Eur J Pediatr 167:1079–1081
Akerlund A, Rudhe U (1950) Intramural small-cysticdiverticulosis of the gallbladder. Acta Radiol33:147–164
Alberti D, Callea F, Camoni G, Falchetti D, Rigamonti W,Caccia G (1998) Adenomyomatosis of the gallbladderin childhood. J Pediatr Surg 33:1411–1412
Albores-Saavedra J, Henson DE (1984) Tumors of thegallbladder and extrahepatic bile ducts, Atlas of tumorpathology, second series, fascicle 22. Armed ForcesInstitut of Pathology, Washington, DC
Albores-Saavedra J, Henson DE (1999) Pyloric glandmetaplasia with perineural invasion of the gallbladder:a lesion that can be confused with adenocarcinoma.Cancer 86:2625–2631
Albores-Saavedra J, Nadji M, Henson DE, Ziegels-Weissman J, Mones JM (1986) Intestinal metaplasiaof the gallbladder: a morphologic and immunocyto-chemical study. Hum Pathol 17:614–620
Albores-Saavedra J, Defortuna SM, Smothermon WE(1990) Primary papillary hyperplasia of the gallbladderand cystic and common bile ducts. Hum Pathol21:228–231
Albores-Saavedra J, Henson DE, Klimstra DS (1998)Tumors of the gallbladder, extrahepatic bile ducts, andampulla of Vater, Atlas of tumo pathology, third series,fascicle 27. Armed Forces Institute of Pathology,Washington, DC
Albores-Saavedra J, Galliani C, Chable-Montero F,Batich K, Hensen DE (2009) Mucin-containingRokitansky-Aschoff sinuses with extracellular mucindeposits simulating mucinous carcinoma of the gall-bladder. Am J Surg Pathol 33:1633–1638
Aldridge MC, Gruffaz F, Castaing D, Bismuth H (1991)Adenomyomatosis of the gallbladder. A premalignantlesion? Surgery 109:107–110
Andrei A, Nobile F (1960) A characteristic benign tumor ofthe gallbladder: adenomyoma (in Italian). Atti AccadFisiocrit Siena Med Fis 8:874–882
Apostolov E, Al-Soud WA, Nilsson I, Kornilovska I,Usenko V, Lyzogubov V, Gaydar Y et al (2005)Helicobacter pylori and other Helicobacter species ingallbladder and liver of patients with chronic cholecys-titis detected by immunological and molecularmethods. Scand J Gastroenterol 40:96–102
Arnaout AH, Abbas SH, Shousha S (1990) Helicobacterpylori is not identified in areas of gastric metaplasia ofgall bladder. J Pathol 160:333–334
Attaallah W, Yener N, Ugurlu MU, Manukyan M,Asmaz E, Aktan AO (2013) Gallstones and concomi-tant gastric Helicobacter pylori infection. GastroenterolRes Pract 2013:643109
Azadeh B, Parai SK (1980) Argentaffin cells, intestinalmetaplasia and antral metaplasia in carcinoma of thegall bladder. Histopathology 4:653–659
Baba H, Wakabayashi M, Oba A, Tsubomoto T,Nakamura H, Sanada T, Kuwabara H et al (2014)
Primary papillary hyperplasia of the gallbladder mim-icking gallbladder cancer. Int Surg 99:247–251
Baig SJ, Biswas S, Das S, Basu K, Chattopadhyay G(2002) Histopathological changes in gallbladdermucosa in cholelithiasis: correlation with chemicalcomposition of gallstones. Trop Gastroenterol23:25–27
Ben Brahim E, Jouini R, Aboulkacem S, Jaouadi F,Labbene N, Cherif R, Helal Y, Sayed S et al (2011)Gastric heterotopia: clinical and histological study of12 cases (in French). Tunis Med 89:935–939
Berk RN, van der Vegt JH, Lichtenstein JE (1983) Thehyperplastic cholecystoses: cholesterolosis andadenomyomatosis. Radiology 146:593–601
Bevan G (1970) A calculous adenomyomatosis of thegallbladder. Gut 11:1029–1034
Bonnyanugomol W, Chomvarin C, Sripa B,Bhudhisawasdi V, Khuntikeo N, Hahnvajanawong Cet al (2012) Helicobacter pylori in Thai patients withcholangiocarcinoma and its association with biliaryinflammation and proliferation. HPB (Oxford)14:177–184
Boscak AR, Al-Hawary M, Ramsburgh SR (2006) Bestcases from the AFIP: adenomyomatosis of the gallblad-der. Radiographics 26:941–946
Boyle L, Gallivan MV, Chun B, Lack EE (1992)Heterotopia of gastric mucosa and liver involving thegallbladder. Report of two cases with literature review.Arch Pathol Lab Med 116:138–142
Brambs HJ, Wrazidlo W, Schilling H (1990) The sono-graphic image of gallbladder adenomyomatosis(in German). Röfo 153:633–636
Bricker DL, Halpert B (1963) Adenomyoma of the gall-bladder. Surgery 53:615–620
Brown HW, Goodsitt E, Snearly R (1966) Cholecystitisglandularis proliferans. Int Surg 45:650–654
Buitrago Salassa C, Javier Lespi P (2007) Detection of acidmucins in gastric metaplasia of the gallbladder(in Spanish). Acta Gastroenterol Latinoam 37:11–14
Burt LI, Masel H (1955) Cholecystitis glandularisproliferans; (diverticula of the gall-bladder). Med JAust 42:270–272
Caldone Firrao G (1960) Adenomyoma of the gallbladder(in Italian). Policlinico Prat 67:1483–1488
Cariati A, Cetta F (2003) Rokitansky-Aschoff sinuses ofthe gallbladder are associated with black pigment gall-stone formation: a scanning electron microscopy study.Ultrastruct Pathol 27:265–270
Caroli J, Paraf A, Beaugrand G (1951) Contribution to thestudy of multilobular gallbladders; radiological studyof the Rokitansky-Aschoff sinuses; nature of this for-mation (in French). Arch Mal Appar Dig Mal Nutr40:886–887
Cavazza A, De Marco L, Asioli S, Pastore L, Gardini G(1999) Stromal osseous metaplasia in metastatic ade-nocarcinoma of the gallbladder. Tumori 85:133–134
Celoria GC, Rodriguez Otero JC, Proske SA, Vallilengua C(1994) Papillary hyperplasia and cholesterolosis of thegallbladder. Medicine (B Aires) 54:31–34
12 Hyperplastic Lesions and Metaplastic Changes of the Gallbladder
Chang LY, Wang HP, Wu MS, Huang HT, Wang HH, LinCC, Lin JT (1998) Anomalous pancreaticobiliary duc-tal union – an etiologic association of gallbladder can-cer and adenomyomatosis. Hepato-Gastroenterology45:2016–2019
Chan-Wilde C, Chew R, Foong WC, Wee A (1990)Adenomyomatosis of the gallbladder: the NUH expe-rience. Ann Acad Singap 19:389–392
Chao C, Hsiao HC, Wu CS, Wang KC (1992) Computedtomographic finding in adenomyomatosis of the gall-bladder. J Formos Med Assoc 91:467–469
Ching BH, Yeh BM, Westphalen AC, Joe BN, Qayyum A,Coakley FV (2007) CT differentiation ofadenomyomatosis and gallbladder cancer. AJR Am JRoentgenol 189:62–66
Christensen AH, Ishak KG (1970) Benign tumors andpseudotumors of the gallbladder. Report of 180 cases.Arch Pathol 90:423–432
Cöl C, Boran C, Turkeli V, Dinler K, Kordon O, Erkol H,Sengul N (2007) Heterotopic gastric mucosa in gall-bladder associated with kidney agenesis and congenitalhip dysplasia. Acta Clin Belg 62:120–122
Colovic R, Grubor N, Radak V, Micev M, Colovic N,Stojkovic M (2006) Tubular adenoma of the gallblad-der with squamous metaplasia (in Serbian). Srp ArhCelok Lek 134:159–161
Colquhoun J (1961) Adenomyomatosis of the gall-bladder(intramural diverticulosis). Br J Radiol 34:101–112
Costa-Greco MA (1987) Adenomyomatosis of the gall-bladder. J Clin Ultrasound 15:198–199
Daud MS, Salomao FC, Salomao EC, Salomao BC (2007)Gastric heterotopia together with squamous metaplasiain the gallbladder. Acta Gastroenterol Latinoam37:164–167
Davies W (1971) Six cases of gall-bladderadenomyomatosis (cholecystitis glandularisproliferans). Australas Radiol 15:148–155
De Boer WG, Ma J, Rees JW, Nayman J (1981) Inappro-priate mucin production in gall bladder metaplasia andneoplasia – an immunohistological study. Histopathol-ogy 5:295–303
Di Carlo I, Toro A, Pulvirenti E, ZisaM, Galia A (2010) Anunusual association of diffuse adenomyomatosis withdysplastic adenoma in chronic calculous cholecystitis:case presentation. BMC Gastroenterol 10:41
Dirks K, Deuerling J, M€uhldorfer S (2006)Erscheinungsformen der Adenomyomatose derGallenblase. Ultraschall Med 27:4
Dorantes-Heredia R, Chablé-Montero F, Henson DE,Albores-Saavedra J (2013) Rokitansky-Aschoffsinuses mimicking adenocarcinoma of the gallbladder:a study of 8 cases. Am J Surg Pathol 37:1269–1274
Dowling GP, Kelly JK (1986) The histogenesis of carci-noma of the gallbladder. Cancer 58:1702–1708
Duarte I, Llanos O, Domke H, Harz C, Valdiviedo V(1993) Metaplasia and precursor lesions of gallbladdercarcinoma. Frequency distribution, and probability ofdetection in routine histologic samples. Cancer72:1878–1884
Egyedi L (1934) Case of polypus of gallbladder containingaberrant gastric mucous membrane. Gyogyaszat74:596–599
Eiserth P (1938) Adenomyome der Gallenblase. VirchowsArch Path Anat 302:717–723
Elfving G, Teir H, Degert H, M€akelà V (1969) Mucosalhyperplasia in the gallbladder demonstrated by plasticmodels. Acta Pathol Microbiol Scand 77:384–388
Farinon AM, Pacella A, Cetta F, Sianesi M (1991) “Ade-nomatous polyps of the gallbladder” adenomas of thegallbladder. HPB Surg 3:251–258
Feltner WR (1966) Hyperplastic cholecystoses. Rocky MtMed J 63:47–50
Fernandes JE, Franco MI, Suzuki RK, Tavares NM, Brom-berg SH (2008) Intestinal metaplasia in gallbladders:prevalence study. Sao Paulo Med J 126:220–222
Fotopoulos JP, Crampton AR (1964) Adenomyomatosis ofthe gallbladder. Med Clin N Am 48:9–36
Fowler RC, Reid WA (1988) Ultrasound diagnosis ofadenomyomatosis of the gall-bladder: ultrasonic andpathological correlation. Clin Radiol 39:402–406
Frommhold W, Lagemann K (1971) Adenomyomatosis ofthe gallbladder (in German). Fortschr Geb RöntgenstrNuklearmed 115:464–475
Fujita N, Lee S, Kobayashi G, Yano A, Mochizuki F(1988) Early gallbladder carcinoma associated withadenomyomatosis of the gallbladder: report of a case(in Japanese). Nihon Shokakibyo Gakkai Zasshi85:1536–1541
Funabiki T, Matsumoto S, Tsukada N, Kimura T,Yoshizaki S, Horibe Y (1993) A patient with earlygallbladder cancer derived from a Rokitansky-Aschoffsinus. Surg Today 23:350–355
Ganesh IM, Subramani D, Halagowder D (2007) Mucinglycoarray in gastric and gallbladder epithelia.J Carcinog 6:10
Gerard PS, Berman D, Zafranloo S (1990) CT and ultra-sound of gallbladder adenomyomatosis mimicking car-cinoma. J Comput Assist Tomogr 14:490–491
Ghiur M, Pantelie C, Ghiur L (1997) Cholecystopathieswith mucosal metaplasia of the intestinal type(in Romanian). Chirurgia (Bucur) 92:349–354
Goldberg HM, Dodgson MCH (1958) Cholecystitiscystica and related lesions. Br J Surg 45:374–378
Govoni AF (1981) Hyperplastic cholecystosis: an analysisand review of the different pathologic and radiologicaspects. Radiol Diagn (Berl) 22:557–588
Halin L (1964) Hyperplastic cholecystoses. J Am Osteo-path Assoc 64:381–396
Halpert B (1961) Significance of the Rokitansky-Aschoffsinuses. Am J Gastroenterol 36:534–539
Halpert RD, Bedi DG, Tirman PJ, Gore DC (1989) Seg-mental adenomyomatosis of the gallbladder. A radio-logic, sonographic and pathologic correlation. AmSurg55:570–572
Hamada T, Yokota K, Ayada K, Hirai K, Kamada T,Haruma K, Chayama K, Oguma K (2009) Detectionof Helicobacter hepaticus in human bile samples ofpatients with biliary disease. Helicobacter 14:545–551
References 13

Hamazaki K, Fujiwara T (2000) Heterotopic gastricmucosa in the gallbladder. J Gastroenterol 35:376–381
Hanada M, Shimizu H, Talami M (1986) Squamous cellcarcinoma of the gallbladder associated with squamousmetaplasia and adenocarcinoma in situ of the mucosalcolumnar epithelium. Acta Pathol Jpn 36:1879–1886
Haradome H, Ichikawa T, Sou H, Yoshikawa T,Nakamura A, Araki T, Hachiya J (2003) The pearlnecklace sign: an imaging sign of adenomyomatosisof the gallbladder at MR cholangiopancreatography.Radiology 227:80–88
Heald RJ (1970) Adenomyomatosis as a source of error inthe diagnosis of gall-bladder disease. Br J Surg57:353–356
Herrmann PK, Saul WM (1986) Clinical pathology ofadenomyoma of the gallbladder (in German). ZentralblAllg Pathol 131:379–382
Hidalgo HJ, Lewicki AM (1980) Adenomyomatosis of thegallbladder. Am J Gastroenterol 73:81–84
Hirayama Y, Kubota M, Hasegawa G, Okuyama N,Ohtaki M, Kobayashi K, TsukadaM, Sato K, NishikuraK et al (2009) A case of a choledochal cyst associatedwith a lymphatic infiltration of a hyperplastic gallblad-der epithelium. J Pediatr Surg 44:831–835
Huang CS, Lien HH, Jeng JY, Huang SH (2001) Role oflaparoscopic cholecystectomy in the management ofpolypoid lesions of the gallbladder. Surg LaparoscEndosc Percutan Tech 11:242–247
Hwang JI, Chou YH, Tsay SH, Chiang JH, Chang CY,Boland GW, Mueller PR (1998) Radiologic and patho-logic correlation of adenomyomatosis of the gallblad-der. Abdom Imaging 23:73–77
II’chenko AA, Orlova IuN, Khomeriki SG (2011) Bonemetaplasia in the gallbladder wall (in Russian). EkspKlin Gastroenterol 8:86–90
Imai H, Osada S, Sasaki Y, Ikawa A, Takahashi T,Yamaguchi K, Hirose Y, Yoshida K (2011) Gallbladderadenocarcinoma with extended intramural spread inadenomyomatosis of the gallbladder with the pearlnecklace sign. Am Surg 77:E57–E58
Inada A, Konishi F, Yamamichi N, Ito H (1989) Histogen-esis of gallbladder cancer with special reference tometaplastic changes and distribution of various mucinsand CEA (in Japanese). Nihon Geka Gakkai Zasshi90:894–906
Inoue S, Matsuda H (1978) A case of adenomyoma of thegallbladder with gastric polyps (in Japanese). NihonShokakibyo Gakkai Zasshi 75:366–373
Ishizuka D, Shirai Y, Tsukada K, Hatakeyama K (1998)Gallbladder cancer with intratumoral anechoic foci: amimic of adenomyomatosis. Hepato-Gastroenterology45:927–929
Isik I, Sezer C, Dursun A (2002) Gastric heterotopia in thegallbladder: a case report. Turk J Gastroenterol13:172–174
Izumi N, Koyama W, Irie T, Miyakawa H, Ito Y,Kanayama M, Hasumura Y, Takeuchi J (1985) Ultra-sonography and computed tomography in
adenomyomatosis of the gallbladder. Acta RadiolDiagn (Stockh) 26:689–692
J€arvi O, Laurén P (1967) Intestinal metaplasia in themucosa of the gallbladder and common bile duct withadditional observations on pancreas heterotopy. AnnMed Exp Biol Fenn 45:213–223
Javed S, Mejias-Luque R, Kalali B, Bolz C, Gerhard M(2013) Helicobacter bilis gamma-glutamyltranspeptidase enhances inflammatory stressresponse via oxidative stress in colon epithelial cells.PLoS ONE 8:e73160
Jelaso D, Burdick CO, Brown RK (1967) Hyperplasticcholecystosis – segmental adenomyomatosis type.Report of two cases. Arch Surg 95:70–73
Jukemura J (1996) Colelitiase e risco de cancer de vesiculabiliar, Thesis, Facultade de Medicina da Universitadede Sao Paulo, Brazil
Jung SE, Lee JM, Lee K, Rha SE, Choi BG, Kim EK, HahnST (2005) Gallbladder wall thickening: MR imagingand pathologic correlation with emphasis on layeredpattern. Eur Radiol 15:694–701
Jutras JA (1960) Hyperplastic cholecystoses; Hickey lec-ture, 1960. Am J Roenetgenol Radium Ther Nucl Med83:795–827
Jutras A, Levesque HP, Larini GP (1964) Adenomyomaand adenomyomatosis of the gallbladder (in Italian).Nunt Radiol 30:1223–1245
Kai K, Ide T, Masuda M, Kitahara K, Miyoshi A,Miyazaki K, Noshiro H, Tokunaga O (2011) Clinico-pathologic features of advanced gallbladder cancerassociated with adenomyomatosis. Virchows Arch459:573–580
Karagin PH, Stenram U, Wadström T, Ljungh A (2010)Helicobacter species and common gut bacterial DNA ingallbladder with cholecystitis. World J Gastroenterol16:4817–4822
Kasahara Y, Sonobe N, Tomiyoshi H, Imano M,Nakatani M, Urata T, Morishita A et al (1992)Adenomyomatosis of the gallbladder: a clinical surveyof 30 surgically treated patients. Nihon Geka Hokan61:190–198
Katoh T, Nakai T, Hayashi S, Satake T (1988) Noninvasivecarcinoma of the gallbladder arising in localized typeadenomyomatosis. Am J Gastroenterol 83:670–674
Katz JS, Rickard EH (1963) Adenomyosis of the gallblad-der. S Afr Med J 37:1011–1014
Khan MR, Raza SA, Ahmad Z, Naeem S, Pervez S,Siddiqui AA, Ahmed M, Azami R (2011) Gallbladderintestinal metaplasia in Pakistani patients with gall-stones. Int J Surg 9:482–485
Kidney M, Goiney R, Cooperberg PL (1986)Adenomyomatosis of the gallbladder: a pictorialexhibit. J Ultrasound Med 5:331–333
Kikiros C, Arunachalam P, LamMH (2003) Adenomatoushyperplastic polyp of the gall bladder associated withcholelithiasis in a child. Pediatr Surg Int 19:118–199
Kim JH, Jeong IH, Han JH, Kim JH, Hwang JC, Yoo BM,Kim JH, Kim MW, Kim WH (2010) Clinical/
14 Hyperplastic Lesions and Metaplastic Changes of the Gallbladder

pathological analysis of gallbladder adenomyomatosis;type and pathogenesis. Hepato-Gastroenterology57:420–425
King ES (1952) Cholecystitis glandularis (Rokitansky-Luschka-Aschoff sinuses) and related conditions.Aust NZ J Surg 22:100–110
King ES (1953) Cholecystitis glandularis and diverticulaof the gall-bladder. Br J Surg 41:156–161
Kinoshita H, Hara M, Hashino M, Nishimura K,Kodama T, Hamada S, Matsuo H, Yasunaga Met al (2002) A case of gallbladder cancer associatedwith pancreaticobiliary maljunction. Kurume Med J49:61–65
Klose KC, Persigehl M, Biesterfeld S, G€unther RW (1991)Adenomyomatosis of the gallbladder in CT(in German). Radiologie 31:73–81
Kobayashi T, Harada K, Miwa K, Nakanuma Y (2005)Helicobacter genus DNA fragments are commonlydetectable in bile from patients with extrahepatic biliarydiseases and associated with their pathogenesis. DigDis Sci 50:862–867
Kozuka S, Hachisuka K (1984) Incidence by age and sex ofintestinal metaplasia in the gallbladder. Hum Pathol15:779–784
Kurihara K, Mizuseki K, Ninomiya T, Shoji I, Kajiwara S(1993) Carcinoma of the gall-bladder arising inadenomyomatosis. Acta Pathol Jpn 43:82–85
Laitio M (1975) Goblet cells, enterochromaffin cells,superficial gastric-type epithelium and antral-typeglands in the gallbladder. Beitr Pathol 156:343–358
Laitio M (1976) Intestinal, gastric body- and antral-typemucosal metaplasia in the gallbladder. Beitr Pathol159:271–279
Laitio M (1980) Morphology and histochemistry ofnon-tumorous gallbladder epithelium. A series of103 cases. Pathol Res Pract 167:335–345
Laitio M, Nevalainen T (1975a) Ultrastructure of endo-crine cells in metaplastic epithelium of human gallbladder. J Anat 120:219–225
Laitio M, Nevalainen J (1975b) An electron microscopicstudy of intestinal metaplasia in human gallbladder.Beitr Pathol 155:297–308
Lauwers GY, Wahl SJ, Scott GV, DeRoux SJ (1995) Pap-illary mucinous adenoma arising in adenomyomatoushyperplasia of the gall bladder. J Clin Pathol48:965–967
Le Quesne LP, Ranger I (1957) Cholecystitis glandularisproliferans. Br J Surg 44:447–458
Lee KF, Wong J, Li JC, Lai PB (2004) Polypoid lesions ofthe gallbladder. Am J Surg 188:186–190
Lee JW, Lee DH, Lee JI, Jeong S, KwonKS, KimHG, ShinYW, Kim YS, Choi MS et al (2010) Identification ofHelicobacter pylori in gallstone, bile, and otherhepatobiliary tissues of patients with cholecystitis.Gut Liver 4:60–67
Levesque HP, LongtinM, Jutras A (1964) Adenomyoma ofthe gallbladder. Anatomic and radiological findings(in French). Union Med Can 93:1487–1506
Lewis JT, Talwalkar JA, Rosen CB, Smyrk TC, AbrahamSC (2007) Prevalence and risk factors for gallbladderneoplasia in patients with primary sclerosingcholangitis: evidence for a metaplasia-dysplasia-carci-noma sequence. Am J Surg Pathol 31:907–913
Leyman P, Saint-Marc O, Hannoun L, Parc R (1996) Het-erotopic gastric mucosa presenting as gallbladderpolyps. Acta Chir Belg 96:128–129
Lin SH, Chang FY, Yang YS, Jin JS, Chen TW (2011) Raregallbladder adenomyomatosis presenting as atypicalcholecystitis: case report. BMC Gastroenterol 11:106
Lubera RJ, Climie AR, Kling GE (1967) Cholecystitis andthe hyperplastic cholecystoses: a clinical, radiologic,and pathology study. Am J Dig Dis 12:696–704
Ludin H (1960) Pseudopolypous cholecystitis (cholecysti-tis glandularis proliferans) with lymphatic cysts of theadjacent parietal peritoneum (in German). Fortschr GebRöntgenstr Nuklearmed 93:133–135
Maderna N, Tritto VA (1959) Adenomyoma of the gall-bladder (in Italian). Riforma Med 73:1026–1030
Mariani PJ, Hsue A (2011) Adenomyomatosis of the gall-bladder: the “good omen” comet. J Emerg Med40:415–418
McCormick DL, Lang EK (1971) Adenomyomatosis andprominent Aschoff-Rokitansky sinuses of the gallblad-der. J La State Med Soc 123:322–323
Meguid MM, Aun F, Bradford ML (1984)Adenomyomatosis of the gallbladder. Am J Surg147:260–262
Meirelles-Costa AL, Bresciani CJ, Perez RO, BrescianiBH, Siqueria SA, Cocconello I (2010) Are histologicalalterations observed in the gallbladder precancerouslesions ? Clinics (Sao Paulo) 65:143–150
Misra V, Misra SP, Dwivedi M, Shouche Y, Dharne M,Singh PA (2007) Helicobacter pylori in areas of gastricmetaplasia in the gallbladder and isolation of H. pyloriDNA from gallstones. Pathology 39:419–424
Miyake H, Aikawa H, Hori Y, Mori H, Sakamoto I,Matsuoka Y, Himeno K, Yamashita H (1992)Adenomyomatosis of the gallbladder with subserosalfatty proliferation: CT findings in two cases.Gastrointest Radiol 17:21–23
Mukhopadhyay S, Landas SK (2005) Putative precursorsof gallbladder dysplasia: a review of 400 routinelyresected specimens. Arch Pathol Lab Med129:386–390
Muto Y, Uchimura M, Waki S, Sameshima Y, Lin T,Matsumoto T, Kadono H, Tsugane Yet al (1978) Clin-icopathological study of 37 cases of adenomyomatosis(localized type) of the gallbladder (in Japanese). NihonShokakibyo Gakkai Zasshi 75:1756–1767
Nabatame N, Shirai Y, Nishimura A, Yokoyama N,Wakai T, Hatakeyama K (2004) High risk of gallblad-der carcinoma in elderly patients with segmentaladenomyomatosis of the gallbladder. J Exp Clin CancerRes 23:593–598
Nelson JJ, Kahn AG (2009) A case of bone metaplasia ofthe gallbladder epithelium. South Med J 102:322–324
References 15

Nishimura A, Shirai Y, Hatakeyama K (2004) Segmentaladenomyomatosis of the gallbladder predisposes tocholecystolithiasis. J Hepatobiliary Pancreat Surg11:342–347
Ochsner SE (1962) Adenomyoma of the gallbladder. Am JRoentgenol Radium Ther Nucl Med 88:778–782
Ohta T, Nagakawa T, Ueno K, Maeda K, Ueda N,Kayahara M, Akiyama T, Kanno M et al (1990) Clin-ical experience of biliary tract carcinoma associatedwith anomalous union of the pancreaticobiliary ductalsystem. Jpn J Surg 20:36–43
Ono S, Fumino S, Iwai N (2011) Implications of intestinalmetaplasia of the gallbladder in children with pancreati-cobiliary maljunction. Pediatr Surg Int 27:237–240
Ootani T, Shirai Y, Tsukada K, Muto T (1992) Relationshipbetween gallbladder carcinoma and the segmental typeof adenomyomatosis of the gallbladder. Cancer69:2647–2652
Ortiz-Hidalgo C, Baquera-Heredia J (2000) Osseous meta-plasia in polypoid cholesterolosis. Am J Surg Pathol24:895
Owen CC, Bilhartz LE (2003) Gallbladder polyps,cholesterolosis, adenomyomatosis, and acuteacalculous cholecystitis. Semin Gastrointest Dis14:178–188
Ozgonul A, Bitiren M, Guldur ME, Sogut O, Yilmaz LE(2010) Fundal variant adenomyomatosis of the gall-bladder: report of three cases and review of the litera-ture. J Clin Med Res 2:150–153
Paraf F, Potet F (1988) Gallbladder carcinoma arising inadenomyomatosis. Am J Gastroenterol 83:1439
Pessel JF, Beairsto EB, Wise JB, Greeley JP, Rathmell TK(1950) Gastro-intestinal mucosa in the wall of thehuman gall-bladder. Gastroenterology 15:533–540
Piegza S, Tyszkiewicz S, Turczynski J, Szklarz Z (1978)Adenomatous hyperplasia in chronic cholecystitis andits significance in carcinogenesis (in Polish). Wiad Lek31:1667–1670
Poonam Y, Ashu S, Rohini G (2008) Clinics in diagnosticimaging (121). Gallbladder adenomyomatosis. SingapMed J 49:262–264
Raeburn C (1969) Ciliated epithelium occurring in dupli-cation of the gall bladder. J Pathol 97:402–403
Raghavednra BN, Subramanyam BR, Blathazar EJ, HoriiSC, Megibow AJ, Hilton S (1983) Sonography ofadenomyomatosis of the gallbladder: radiologic-pathologic correlation. Radiology 146:747–752
Ram MD, Midha D (1975) Adenomyomatosis of the gall-bladder. Surgery 78:224–229
Ray R, Dey R, Chatterjee S, Guha P (2012) Gallbladderadenomyomatosis with tubercular portal lymphade-nopathy masquerading as gallbladder carcinoma.Arab J Gastroenterol 13:150–152
Rege TA, Vargas SO (2011) Cholecystitis and cholelithia-sis associated with an intramural fasciitis-like prolifer-ation and osseous metaplasia. Pediatr Dev Pathol14:80–83
Rice J, Sauerbrei EE, Semogas P, Cooperberg PL,Burhenne HJ (1981) Sonographic appearance of
adenomyomatosis of the gallbladder. J Clin Ultrasound9:336–337
Ross WD, Finby N, Evans JA (1955) Intramural divertic-ulosis of the gallbladder; Rokitansky-Aschoff sinuses.Radiology 64:366–372
Rush DK, Figiel LS, Figiel SJ (1957) Rokitansky-Aschoffsinuses; historical review and presentation of threecases. Grace Hosp Bull 35:53–61
Sagar G, Naik DR (1984) Ultrasound diagnosis ofadenomyomatosis of the gall bladder. Br J Radiol57:432–435
Sakamoto H, Mutoh H, Ido K, Satoh K, Hayakawa H,Sugano K (2007) A close relationship between intesti-nal metaplasia and Cdx2 expression in human gallblad-ders with cholelithiasis. Hum Pathol 38:66–71
Sakamoto H, Mutoh H, Ido K, Satoh S, Kumagai M,Hayakawa H, Tamada K, Sugano K (2009) Intestinalmetaplasia in gallbladder correlates with high amylaselevels in bile in patients with a morphologically normalpancreaticobiliary duct. Hum Pathol 40:1762–1767
Sasaki M, Yamato T, Nakanuma Y, Ho SB, Kim YS (1999)Expression of MUC2, MUC5AC and MUC6apomucins in carcinoma, dysplasia and non-dysplasticepithelia of the gallbladder. Pathol Int 49:38–44
Sciumè C, Geraci G, Pisello E, Li VE, Facella T, Modica G(2005) Heterotopic gastric mucosa in the gallbladder:case report and literature review. Ann Ital Chir76:93–97
Secil M, Karasu S, Sagol O, Coker A (2005) Combinedsegmental and focal adenomyomatosis involving thebody of the gallbladder. J Clin Ultrasound 33:248–250
Seyss R (1966) Schizotonia of the gallbladder (segmentaladenomyosis). Zentralbl Chir 91:1364–1366
Shimizu M, Kitoh K, Fujimitsu Y, Inada K, Ichinose M,Miki K, Yamao K, Nakazawa S et al (1996) Cellulardifferentiation and development of pyloric mucosalmetaplasia in the human gall-bladder. Pathol Int46:261–266
Shimoji H, Nakachi A, Matsubara H, Miyazato H, Isa T,Hiroyasu S, Shiraishi M, Muto Y (2001) Fundicadenomyomatosis bulged with the subserosal excessivefat of the gallbladder mimicking polypoid carcinoma: acase report with unusual imaging and morphologicalfeatures. Clin Imaging 25:187–191
Skapinker S (1971) Adenomyomatosis of the gallbladder.S Afr J Surg 9:143–146
Stalker LK, Davies B, Guest TP (1955) Rokitansky-Aschoff sinuses as related to chronic cholecystitis.AMA Arch Surg 71:124–127
Stokes MC, Burnette R, Ballard B, Ross C, Beech DJ(2007) Adenomatous hyperplasia of the gallbladder.J Natl Med Assoc 99:959–961
Stringer MD, Abbott C, Arthur RJ, Lealman G (2001)Primary papillary hyperplasia of the gallbladder: arare cause of biliary colic. J Pediatr Surg 36:1584–1586
Stunell H, Buckley O, Geoghegan T, O’Brien J, Ward E,Torreggiani W (2008) Imaging of adenomyomatosisof the gall bladder. J Med Imag Radiat Oncol52:109–117
16 Hyperplastic Lesions and Metaplastic Changes of the Gallbladder

Sutherland LR (1898) Small adeno-myoma of the gall-bladder. Glasg Med J 50:216–217
Tatematsu M, Furihata C, Miki K, Ichinose M, Shirai T,Tatematsu K, Ito N (1987) Complete and incompletepyloric gland metaplasia of human gallbladder. ActaPathol Jpn 37:39–46
Tavli L, Belviranli M, Erikoglu M, Esen H, Toy H (2005)Gastric heterotopia together with intestinal metaplasiain the gallbladder: case report and review of literature.Turk J Gastroenterol 16:160–162
Teo CH, Leow CK, Chang SA (2005) A pseudoepidermoidcyst arising from exuberant squamous metaplasia of thegallbladder. Arch Pathol Lab Med 129:e138–e140
Terada T (2013) Histopathologic features and frequency ofgall bladder lesions in consecutive 540 cholecystecto-mies. Int J Clin Exp Pathol 6:91–96
Tompkins RK (1967) Surgical management of solitaryadenomyoma of the gallbladder. Am Surg 33:415–418
Tyagi SP, Tyagi N, Maheshwari V, Ashraf SM, Sahoo P(1992)Morphological changes in diseased gall bladder:a study of 415 cholecystectomies at Aligarh. J IndianMed Assoc 90:178–181
Uchiyama S, Imai S, Suzuki T, Anita A, Takeda K,Sujino H, Kameda H (1995) Heterotopic gastricmucosa of the gallbladder. J Gastroenterol 30:543–546
Umudum H, Gunbatili E, Sanal M, Ceyhan K (2006)Primary diffuse papillary hyperplasia of the gallblad-der. Pathology 38:591–592
Vallera DU, Dawson PJ (1992) Gastric heterotopia in thegallbladder. Path Res Pract 188:49–52
Verhage F, Van der Werff JJ (1964) Intramural diverticulo-sis (Rokitansky-Aschoff sinuses) in septate gallbladder.NY State J Med 64:3006–3009
Wani Y, Notohara K, Fujisawa M (2008) Aberrant expres-sion of an “intestinal marker” Cdx2 in pyloric glandadenoma of the gallbladder. Virchows Arch453:521–527
Williams I, Slavin G, Cox A, Simpson P, de Lacey G(1986) Diverticular disease (adenomyomatosis) of thegallbladder: a radiological-pathological survey. Br JRadiol 59:29–34
Wu MS, Wang HP, Shun CT, Yu SC, Wang TH, Lin JT(1995) Coexistence of anomalous pancreaticobiliaryductal union with adenomyomatosis of the gallbladder.Gastrointest Endosc 42:265–269
Xeropotamos N, Skopelitou AS, Batsis C, Kappas AM(2001) Heterotopic gastric mucosa together with intes-tinal metaplasia and moderate dysplasia in the gallbladder: report of two clinically unusual cases withliterature review. Gut 48:719–723
Yamagiwa H (1989) Mucosal dysplasia of gallbladder:isolated and adjacent lesions to carcinoma. Jpn J Can-cer Res 80:238–243
Yamagiwa H, Tomiyama H (1986) Intestinal metaplasia-dysplasia-carcinoma sequence of the gallbladder. ActaPathol Jpn 36:989–997
Yamaguchi J, Sasaki M, Harada K, Zen Y, Sato Y, Ikeda H,Itatsu K, YokoyamaYet al (2009) Papillary hyperplasiaof the gallbladder in pancreaticobiliary maljunctionrepresents a senescence-related lesion induced by lyso-lecithin. Lab Invest 89:1018–1031
Yamamoto M, Nakajo S, Tahara E (1986) Endocrine cellsand lysozyme immunoreactivity in the gallbladder.Arch Pathol Lab Med 110:920–927
Yamamoto M, Murakami H, Ito M, Nakajo S, Tahara E(1989) Ectopic gastric mucosa of the gallbladder: com-parison with metaplastic polyp of the gallbladder. Am JGastroenterol 84:1423–1426
Yamato T, Kurumaya H, Ohama K, Yamamichi N,Watanabe Y, Harada K, Sasaki M et al (1999)Frequent expression of mucin core protein MUC1 innon-neoplastic gallbladder mucosa from patients withpancreaticobiliary maljunction. Liver 19:281–287
YangWG,Wang SS,WengYJ, Tsay SH, Chen CC, ChiangJH, Su CH, Lee FY, Lee SD (1996) Adenomyomatosisof the gallbladder. Zhonghua Yi Xue Za Zhi (Taipei)58:12–17
Yoshimitsu K, Honda H, Jimi M, Kuroiwa T, Hanada K,Irie H, Tajima T, Takashima M et al (1999) MR diag-nosis of adenomyomatosis of the gallbladder and dif-ferentiation from gallbladder carcinoma: importance ofshowing Rokitansky-Aschoff sinuses. AJR Am JRoentgenol 172:1535–1540
Yoshimitsu K, Irie H, Aibe H, Tajima T, Nishie A,Asayama Y, Matake K, Yamaguchi K et al (2005)Well-differentiated adenocarcinoma of the gallbladderwith intratumoral cystic components due to abundantmucin production: a mimicker of adenomyomatosis.Eur Radiol 15:229–233
Young TE (1959) So-called adenomyoma of the gallblad-der. Am J Clin Pathol 31:423–427
Zani A, Pacilli M, Conforti A, Casati A, Bosco S, CozziDA (2005) Adenomyomatosis of the gallbladder inchildhood: report of a case and review of the literature.Pediatr Dev Pathol 8:577–580
Zen Y, Zen C, Quaglia A, Davenport M, Heaton N,Portmann B (2011) Intestinal phenotypes inpediatric gallbladder epithelium. Hum Pathol 42:1454–1458
Zhou D, Guan WB, Wang JD, Zhang Y, Gong W, QuanZW (2013) A comparative study of clinicopathologicalfeatures between chronic cholecystitis patients with andwithout Helicobacter pylori infection in gallbladdermucosa. PLoS ONE 8:e70265
Zinober M (1952) Rokitansky-Aschoff sinuses of the gallbladder; their demonstration during cholecystography.S Afr Med J 26:35
Zissin R, Osadchy A, Shapiro-FeinbergM, Gayer G (2003)CT of a thickened-wall gall bladder. Br J Radiol76:137–143
References 17