hypertension and pregnancy: before, during, and after
TRANSCRIPT
Hypertension and Pregnancy: Before, During, and After
Jourdie Triebwasser, MD, MA Fellow, Maternal-Fetal Medicine
December 15, 2017

Disclosures
• I have no relevant financial disclosures or conflicts of interest.
2
Case 1
• 35 yo G2P0111 presents for preconception counseling after having a cesarean delivery at 33 weeks for intractable headache and elevated blood pressure. Her BP is 135/85. She would like to know what she should do in a future pregnancy.
• You offer which of following (more than 1 may be correct)? – A) Prescribe a calcium channel blocker
– B) Start a prenatal vitamin with folic acid
– C) Recommend starting low dose aspirin by 16 weeks in a future pregnancy
– D) Recommend checking renal and liver function with initial prenatal labs
3

Case 2
• 32 yo G2P0010 at 36w5d presents for routine OB appt. Her BP is 145/91. Her BP last week was 142/85. She is asymptomatic. An NST is reactive. You plan to send CBC, Cr, AST/ALT, and UPC.
• When do you recommend delivery if all labs return normal? – A) Now
– B) 37 weeks
– C) 38 weeks
– D) 39 weeks
4
Case 3
• 27 yo G1P1001 is PPD#2 from a vaginal delivery at 38 weeks. She was diagnosed with pre-eclampsia on admission after presenting with contractions. Her last BP was 140/90.
• What do you tell her about her future cardiovascular risk? – A) Nothing, she is only PPD#2
– B) There is no association between pregnancy complications and lifelong cardiovascular risk
– C) As long as her BP is normal by her PP visit, she has no increased risk
– D) She has an increased life-long risk of cardiac disease
5
Objectives
• To review classification of hypertensive disorders of pregnancy
• To outline preconception planning related to hypertension
• To determine when women with hypertensive disorders of pregnancy require antihypertensive medications antepartum
• To discuss timing of delivery with hypertensive disorders in pregnancy
• To consider lifelong risk associated with hypertensive disorders of pregnancy
6

7
Hypertensive Disorders of Pregnancy (HDP)
8
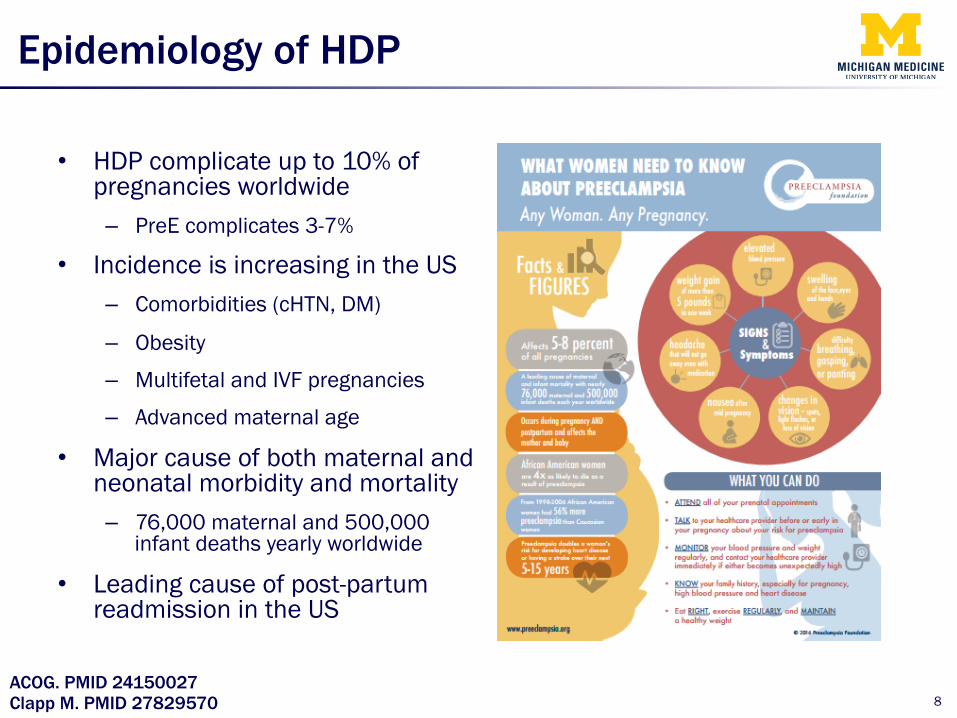
Epidemiology of HDP
• HDP complicate up to 10% of pregnancies worldwide – PreE complicates 3-7%
• Incidence is increasing in the US – Comorbidities (cHTN, DM)
– Obesity
– Multifetal and IVF pregnancies
– Advanced maternal age
• Major cause of both maternal and neonatal morbidity and mortality – 76,000 maternal and 500,000
infant deaths yearly worldwide
• Leading cause of post-partum readmission in the US
Clapp M. PMID 27829570 ACOG. PMID 24150027

• Pre-eclampsia (preE)/Eclampsia
• Chronic hypertension (cHTN)
• Chronic hypertension with superimposed preE
• Gestational hypertension (gHTN)
9
Classification of HDP
ACOG. PMID 24150027

Classification of HDP
10
BP ≥ 140/90 x 2* After 20 weeks
Proteinuria - UPC ≥ 0.3 - 24 h > 300 mg
*If mild range at least 4 hr apart *If ≥160/110, confirm within minutes
+
-
PreE
gHTN
Severe Features
BP ≥ 140/90 x 2 Before 20 weeks cHTN Ex
acer
batio
n of
HTN
, new
/inc
reas
ing
prot
einu
ria

Classification of HDP (Severe Features)
• Blood pressure – Systolic ≥ 160 – Diastolic ≥ 110
• Thrombocytopenia (<100K) • Impaired liver function
– AST/ALT > 2x upper limit of normal
– Or RUQ/epigastric pain unresponsive to meds and not explained by other Dx
• Renal insufficiency – Cr > 1.1 mg/dL or doubling of serum creatinine
• Pulmonary edema • New-onset cerebral or visual disturbances
11
12
Preconception Counseling

Assess risk factors for preE/HDP
• Primiparity
• Multifetal gestation
• IVF
• Personal or family history of preE
• cHTN or chronic renal disease or both
• History of thrombophilia
• Pregestational diabetes
• SLE
• Obesity
• Advanced maternal age (>40 yo)
13 ACOG. PMID 24150027
Pregnancy Factors
Medical Factors
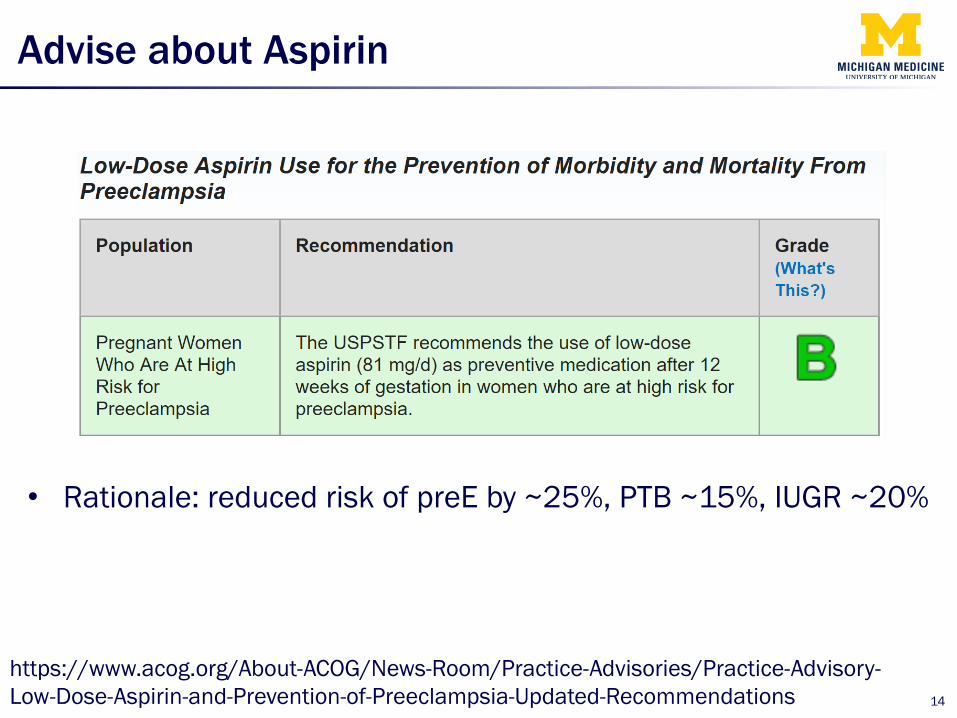
Advise about Aspirin
• Rationale: reduced risk of preE by ~25%, PTB ~15%, IUGR ~20%
14
https://www.acog.org/About-ACOG/News-Room/Practice-Advisories/Practice-Advisory-Low-Dose-Aspirin-and-Prevention-of-Preeclampsia-Updated-Recommendations
Advise about Aspirin
• ACOG updated its “high risk” factors to correlate with USPSTF in 2016 – History of preE, especially if associated with adverse outcome
– Multifetal gestation
– cHTN
– Pregestational diabetes
– Renal disease
– Autoimmune disease (SLE, APLS)
15
Assess Baseline Labs
• Can be done at preconception visit if no documentation of normal creatinine, LFTs after affected pregnancy
• Otherwise discuss baseline evaluation of renal function, liver function, and proteinuria with initial prenatal labs – CBC from prenatal panel to assess platelets
– Consider 24 hour urine collection in women with baseline proteinuria (SLE, poorly controlled DM or HTN, CKD, severe range proteinuria in prior pregnancy)
16

17
Antepartum HTN Management
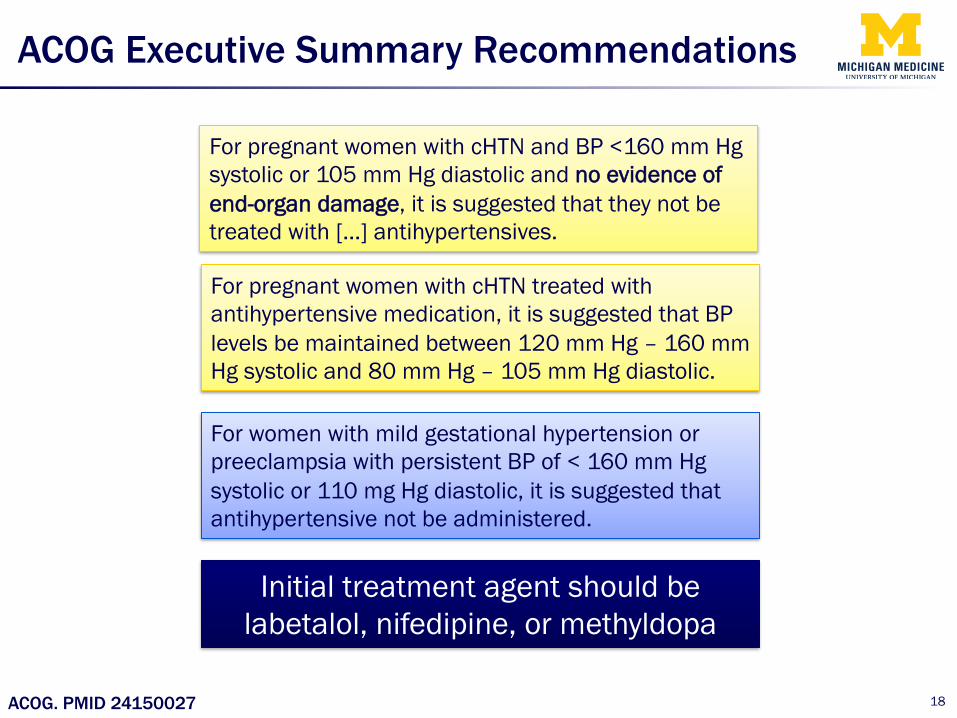
ACOG Executive Summary Recommendations
18 ACOG. PMID 24150027
For pregnant women with cHTN and BP <160 mm Hg systolic or 105 mm Hg diastolic and no evidence of end-organ damage, it is suggested that they not be treated with […] antihypertensives.
For pregnant women with cHTN treated with antihypertensive medication, it is suggested that BP levels be maintained between 120 mm Hg – 160 mm Hg systolic and 80 mm Hg – 105 mm Hg diastolic.
For women with mild gestational hypertension or preeclampsia with persistent BP of < 160 mm Hg systolic or 110 mg Hg diastolic, it is suggested that antihypertensive not be administered.
Initial treatment agent should be labetalol, nifedipine, or methyldopa

CHIPS study
19 Magee. PMID 26061848

20
Timing of Delivery with HDP
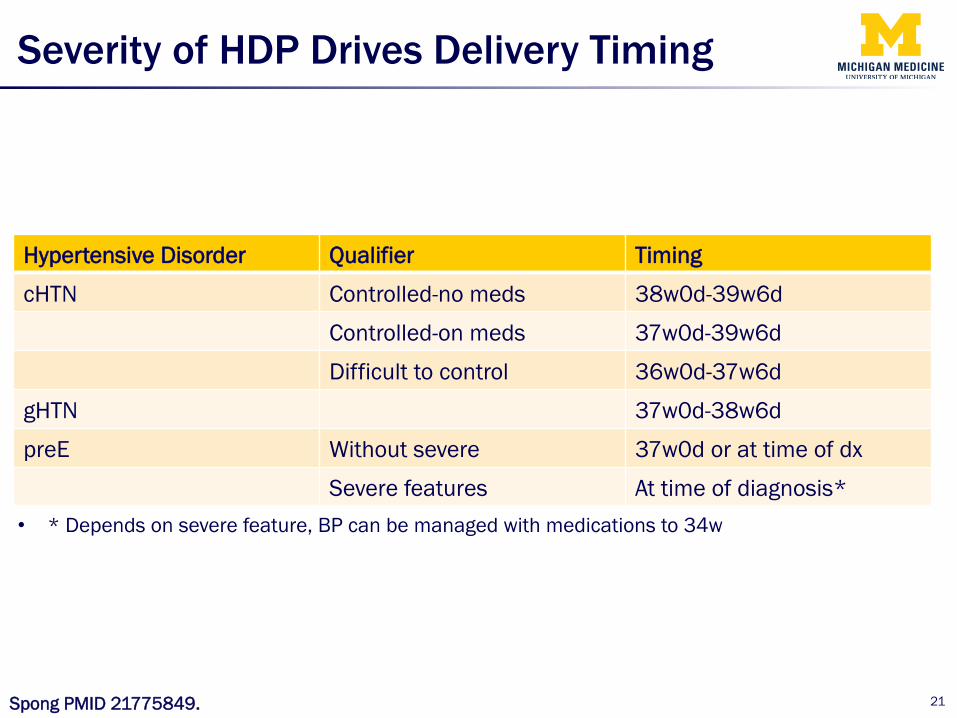
Severity of HDP Drives Delivery Timing
21
Hypertensive Disorder Qualifier Timing
cHTN Controlled-no meds 38w0d-39w6d
Controlled-on meds 37w0d-39w6d
Difficult to control 36w0d-37w6d
gHTN 37w0d-38w6d
preE Without severe 37w0d or at time of dx
Severe features At time of diagnosis* • * Depends on severe feature, BP can be managed with medications to 34w
Spong PMID 21775849.
22
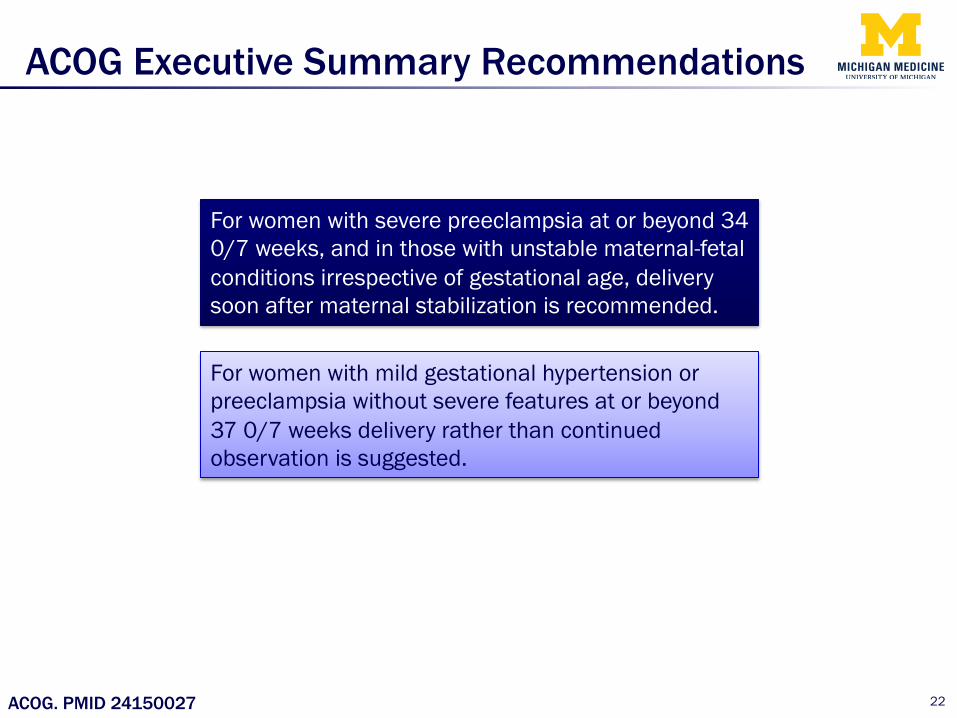
ACOG Executive Summary Recommendations
For women with severe preeclampsia at or beyond 34 0/7 weeks, and in those with unstable maternal-fetal conditions irrespective of gestational age, delivery soon after maternal stabilization is recommended.
For women with mild gestational hypertension or preeclampsia without severe features at or beyond 37 0/7 weeks delivery rather than continued observation is suggested.
ACOG. PMID 24150027
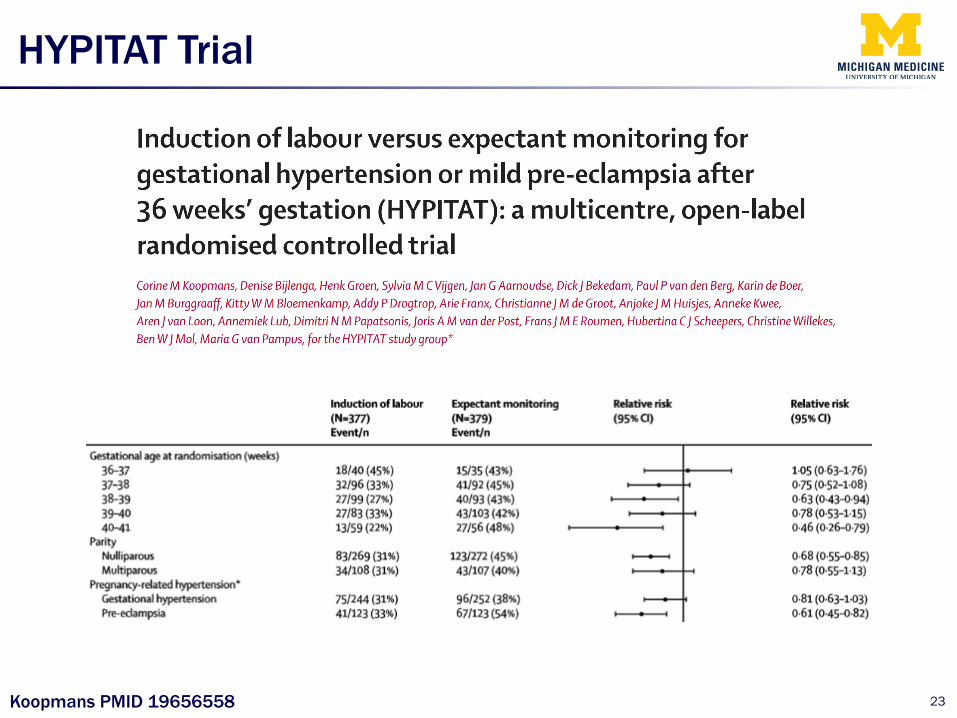
HYPITAT Trial
23 Koopmans PMID 19656558

24
Long-term Sequelae

Long-Term Sequelae of HDP
25 McDonald PMID 19061708
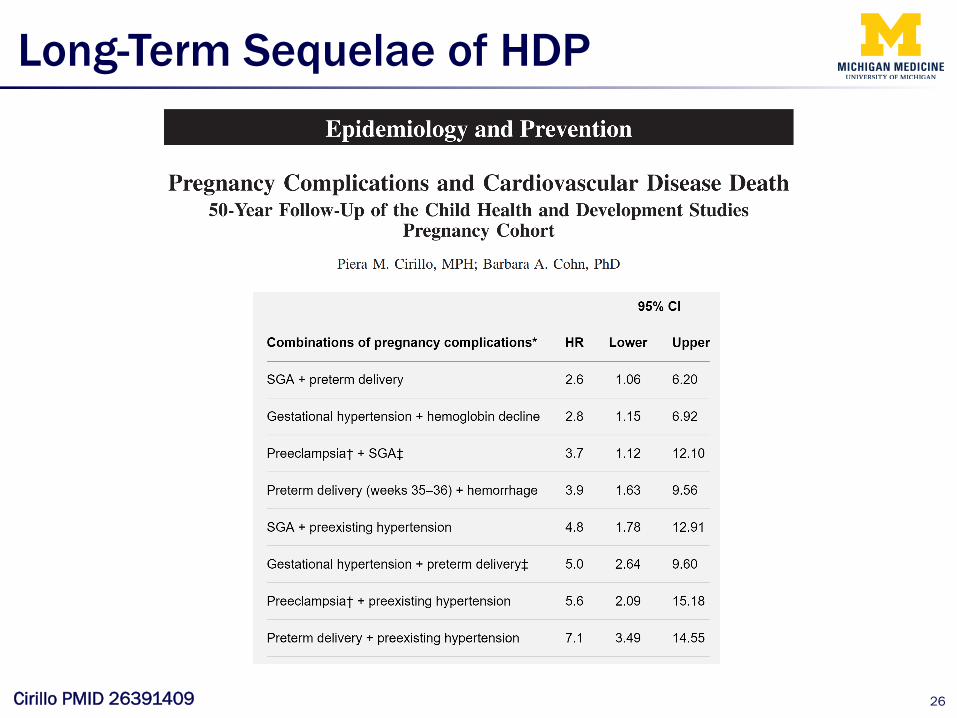
Long-Term Sequelae of HDP
26 Cirillo PMID 26391409
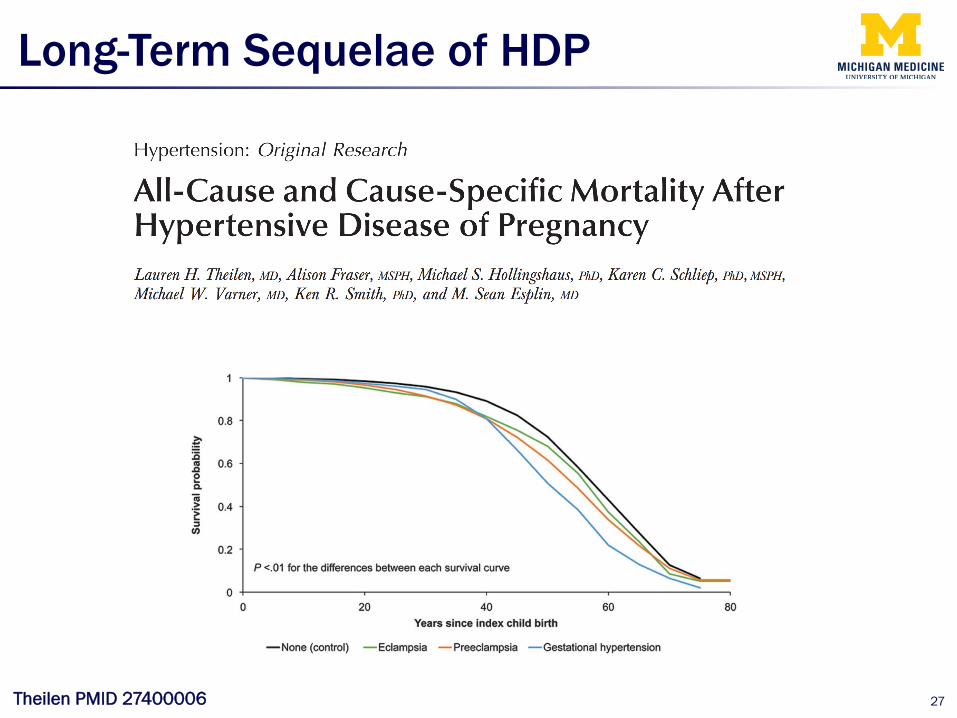
Long-Term Sequelae of HDP
27 Theilen PMID 27400006
28
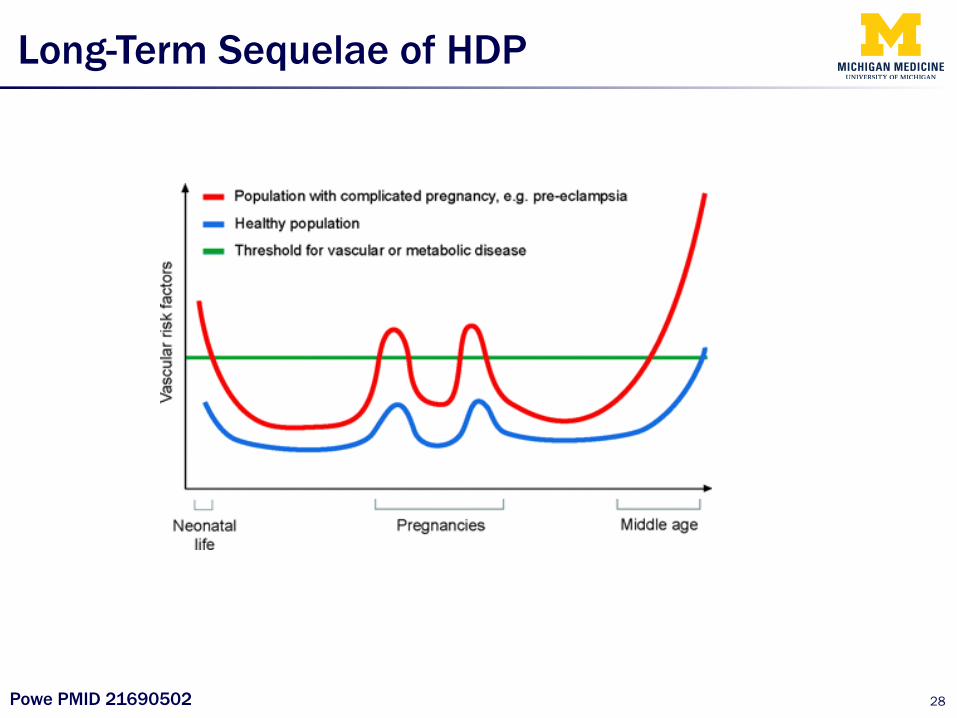
Long-Term Sequelae of HDP
Powe PMID 21690502
29
Long-Term Sequelae of HDP

30
Cases
Case 1
• 35 yo G2P0111 presents for preconception counseling after having a cesarean delivery at 33 weeks for intractable headache and elevated blood pressure. Her BP is 135/85. She would like to know what she should do in a future pregnancy.
• You offer which of following (more than 1 may be correct)? – A) Prescribe a calcium channel blocker
– B) Start a prenatal vitamin with folic acid
– C) Recommend starting low dose aspirin by 16 weeks in a future pregnancy
– D) Recommend checking renal and liver function with initial prenatal labs
31
Case 2
• 32 yo G2P0010 at 36w5d presents for routine OB appt. Her BP is 145/91. Her BP last week was 142/85. She is asymptomatic. An NST is reactive. You plan to send CBC, Cr, AST/ALT, and UPC.
• When do you recommend delivery if all labs return normal? – A) Now
– B) 37 weeks
– C) 38 weeks
– D) 39 weeks
32

Case 3
• 27 yo G1P1001 is PPD#2 from a vaginal delivery at 38 weeks. She was diagnosed with pre-eclampsia on admission after presenting with contractions. Her last BP was 140/90.
• What do you tell her about her future cardiovascular risk? – A) Nothing, she is only PPD#2
– B) There is no association between pregnancy complications and lifelong cardiovascular risk
– C) As long as her BP is normal by her PP visit, she has no increased risk
– D) She has an increased life-long risk of cardiac disease
33

34
Final Thoughts
Conclusions
• Clarify diagnosis of HTN early in pregnancy – It may alter decision making later in pregnancy
• Low dose aspirin is recommended to reduce the risk of preE
• Women with gHTN or preE generally should not be treated with antihypertensives (on an outpatient basis)
• Women with gHTN and preE should be delivered at 37 weeks
• Be an advocate for you patient – Talk about lifelong risk
– Advise her on PCP follow-up after HDP
35

36
Thank you! Questions?