hypertension in children - university of arkansas for ... docs 2/news/kidney 2012/hypertension...
TRANSCRIPT

Hypertension in ChildrenHypertension in ChildrenHypertension in ChildrenHypertension in Children
M h d Il M DMohammad Ilyas, M.D.
Associate Professor of Pediatrics
f h l fDivision of Nephrology, Department of Pediatrics. UAMS Little Rock
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

OutlineOutlineOutlineOutline
• Prevalence.Prevalence.
• AAP recommendations for BP measurement.
• Case StudyCase Study
– BP measurement.
Definition of hypertension– Definition of hypertension.
– Workup of hypertensive patient.
• Fourth Task Force treatment recommendations• Fourth Task Force treatment recommendations.
• Athletic participation.
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

HypertensionHypertension in Childrenin ChildrenHypertension Hypertension in Childrenin Children
Prevalence of Overweight in Children
16%
Prevalence of Hypertension in School Children
4.50%
5.00%
6%
8%
10%
12%
14%
eval
ence
1971-19741999-2000 2.50%
3.00%
3.50%
4.00%
4.50%
vale
nce
19892004
0%
2%
4%
6%
6 to 11 years 12 to 19 years
Pre
0.50%
1.00%
1.50%
2.00%
Prev 2004
Ogden CL et al. JAMA 2002 Sorof JM et al. Pediatrics 2004
Age Group0.00%
Year
g

PrevalencePrevalencePrevalencePrevalence
4%10%0
Children
0
Adults
10%
Htn
Pre‐htn31%
44% Htn
86% Normal
25%
Pre‐htn
Normal
5%
Sorof JM et al. Pediatrics 2004CDC Hypertension Facts
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
Significance of Pediatric HypertensionSignificance of Pediatric HypertensionSignificance of Pediatric HypertensionSignificance of Pediatric Hypertension
• For children in the upper quartile of BP on any single examination, the likelihood of remaining in the upper quartile in adulthood ranged from 41 to 52 percent for systolic BP and from 35 to 44 percent for diastolic BP (B l St d ) Shear et al Pediatrics 1986;77(6):862 9BP . (Bogalusa Study)
• Association of elevated BP and cardiovascular changes like carotid intimal medial thickness LVH
Shear et.al Pediatrics. 1986;77(6):862‐9
changes like; carotid intimal medial thickness, LVH, and arterial stiffness is reported.
Sorof JM et al. Pediatrics. 2003;111(1):
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

AAP Recommendations for Blood AAP Recommendations for Blood Pressure MeasurementPressure Measurement
• Every child 3 years or more should have, as a part of their routine continuing medical
l bl dcare, a yearly blood pressure measurement• All acutely ill children, regardless of age, h ld h bl d dishould have a blood pressure reading performed at the time of evaluation
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

Conditions Under Which Children <3 Years Conditions Under Which Children <3 Years Old Sh ld H BP M dOld Sh ld H BP M dOld Should Have BP MeasuredOld Should Have BP Measured
• History of prematurity, very low birthweight, or other neonatal complication requiring intensive carep q g
• Congenital heart disease, whether repaired or non‐repaired
• Recurrent urinary tract infections, hematuria, or proteinuria
• Known renal disease or urologic malformations
Fourth report on BP. Pediatrics August 2004
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
Fourth report on BP. Pediatrics August 2004

Role of Adult PCP in Pediatric Role of Adult PCP in Pediatric HypertensionHypertension
• 4296 adolescents4296 adolescents – 73% 11‐14 yrs
66% boys– 66% boys
– 53% Black
48% i ht– 48% overweight
– 23% received antihypertensive treatment
f f• 60 % of patients received prescriptions from adult primary care physicians.
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
Yoon EY et al. Yoon EY et al. Pediatrics Pediatrics 2012;129:12012;129:1––88

CASE STUDYCASE STUDYCASE STUDYCASE STUDY
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

14 yrs old asymptomatic WF had a blood pressure of 14 yrs old asymptomatic WF had a blood pressure of 142/82 mm Hg on a sports physical Referred to PCP142/82 mm Hg on a sports physical Referred to PCP142/82 mm Hg on a sports physical. Referred to PCP 142/82 mm Hg on a sports physical. Referred to PCP officeofficeExam: NormalExam: Normal
10
BP: 156/80 &150/79 mm HgBP: 156/80 &150/79 mm HgWeight: 58 kg (50Weight: 58 kg (50thth %)%)Height: 174 cm (50Height: 174 cm (50thth %)%)Choose ONE best answerChoose ONE best answer1 She is hypertensive
0% 0%0%0%
1. She is hypertensive
2. She has normal BP
3 I don’t know1 2 3 4
0% 0%0%0%3. I don’t know
4. Need more information
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

Definition of HypertensionDefinition of HypertensionDefinition of HypertensionDefinition of Hypertension
HTN Classification 2004 Working Group (percentiles) JNC VII (mmHg)
Children Adults
Normotensive <90th <120/80
Pre‐hypertension 90th to <95th or if BP > 120/80 even <90th 120‐139/80‐89Pre hypertension 90 to <95 or if BP > 120/80 even <90 120 139/80 89
Stage I HTN 95th‐99th +5mmHg (three separate visits) 140‐159/90‐99
hStage 2 HTN >99th+5 mmHg (three separate visits) > 160/100
Fourth report on BP. Pediatrics August 2004
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

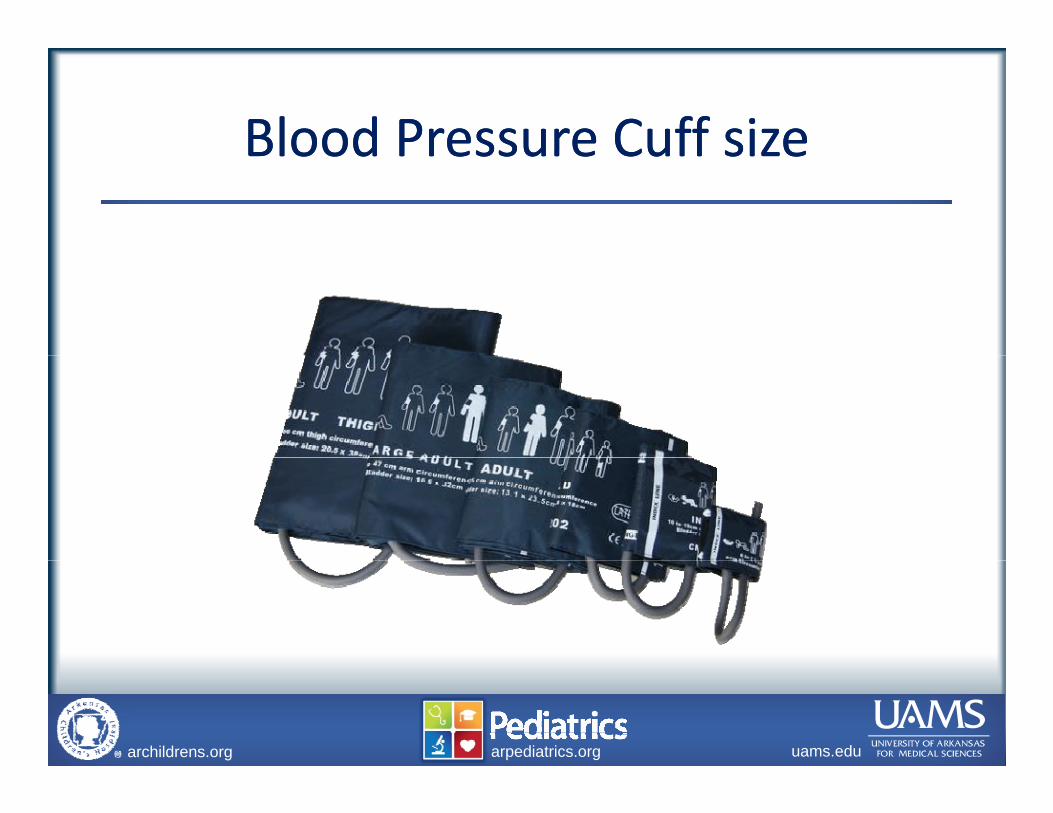
Blood Pressure Cuff sizeBlood Pressure Cuff sizeBlood Pressure Cuff sizeBlood Pressure Cuff size
Images MD
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
g

Blood Pressure Cuff SizeBlood Pressure Cuff SizeBlood Pressure Cuff SizeBlood Pressure Cuff Size
Index line Cuff length = 80% of MACIndex line
Bladder length (80%) 20%
Cuff length 80% of MAC
g ( )
Cuff width = 40% of MAC
Largest allowable mid arm circumference for bladder (100%)
Cuff width = 40% of MACMAC
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
circumference for bladder (100%)

Case HistoryCase HistoryCase HistoryCase History
• 12 years old boy
• Admitted for cellulitis of left lower leg• Admitted for cellulitis of left lower leg
• BP= 210/110 mm Hg
• Blood pressure rechecked
• Physical examination, Wt. 587 poundsy , p
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
Blood Pressure Cuff sizeBlood Pressure Cuff sizeBlood Pressure Cuff sizeBlood Pressure Cuff size
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

Definition of HypertensionDefinition of HypertensionDefinition of HypertensionDefinition of Hypertension
HTN Classification JNC VII (mmHg)
Adults
Normotensive <120/80
Pre‐hypertension 120‐139/80‐89Pre hypertension 120 139/80 89
Stage I HTN 140‐159/90‐99
Stage 2 HTN > 160/100
Fourth report on BP. Pediatrics August 2004
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
Pediatric BP StandardsPediatric BP StandardsPediatric BP StandardsPediatric BP Standards
• Blood pressure correlates with:pAge
GenderGender
Height percentile
St d d• StandardsAges 1‐12 months: 1987 task force
Ages 1‐17 years: Fourth BP report
Fourth report on BP. Pediatrics August 2004
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
p g
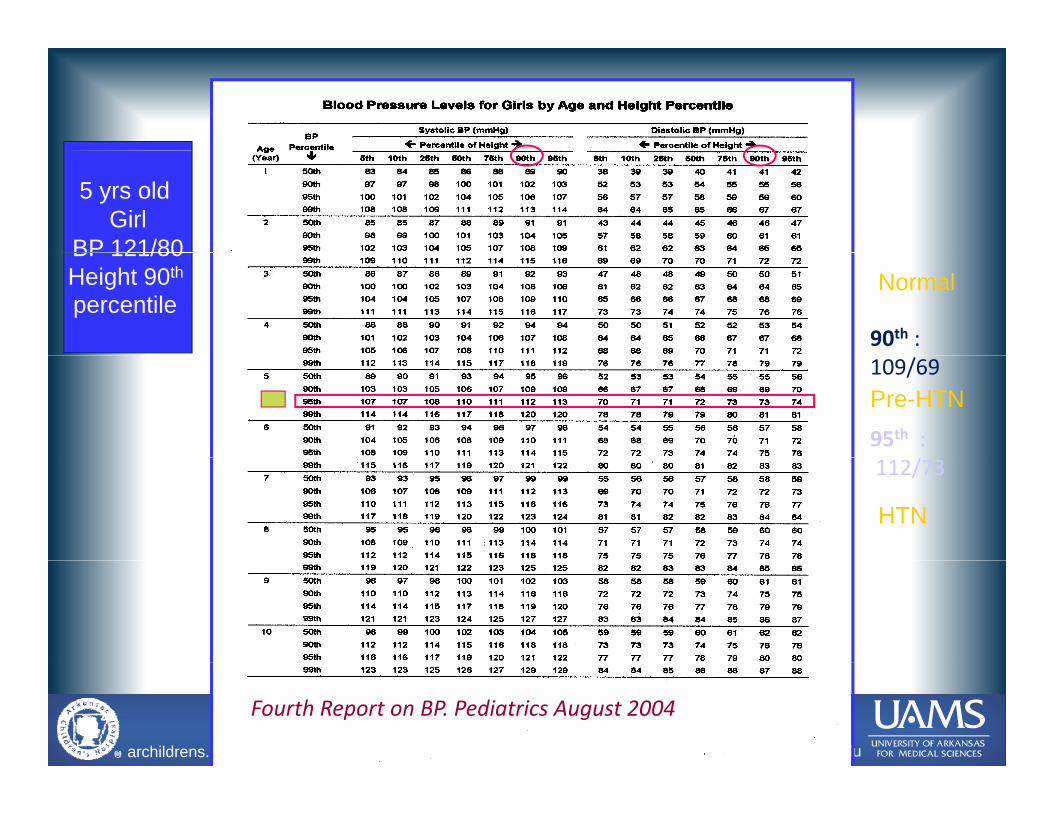
5 yrs old Girl
BP 121/80BP 121/80Height 90th
percentile90th :
Normal
95th :/
109/69Pre-HTN
112/73
HTN
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
Fourth Report on BP. Pediatrics August 2004

5 yrs old Girl
BP 121/80Height 90th
percentile 90th :percentile
95th :112/73
109/69
112/73
99th :120/81120/81
Stage I
>125/86
Stage II
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
Fourth Report on BP. Pediatrics August 2004

Definition of HypertensionDefinition of HypertensionDefinition of HypertensionDefinition of Hypertension
HTN Classification 2004 Working Group (percentiles) JNC VII (mmHg)
Children Adults
Normotensive <90th <120/80
Pre‐hypertension 90th to <95th or if BP > 120/80 even <90th 120‐139/80‐89Pre hypertension 90 to <95 or if BP > 120/80 even <90 120 139/80 89
Stage I HTN 95th‐99th +5mmHg (three separate visits) 140‐159/90‐99
hStage 2 HTN >99th+5 mmHg (three separate visits) > 160/100
Fourth report on BP. Pediatrics August 2004
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

Following study will most likely be helpful in the Following study will most likely be helpful in the 10g y y pg y y pdiagnosisdiagnosis
10
Choose ONE best answer
1. Echocardiogram
2 Chest X ray and EKG2. Chest X‐ray and EKG
3. Ambulatory BP monitoring
4. Arteriogram of renal vessels
0% 0% 0%0%0%
g
5. Chest X‐ray and echocardiogram
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
1 2 3 4 5
0% 0% 0%0%0%

Case Study Case Study
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

Case Study Case Study
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

Definition of HypertensionDefinition of HypertensionDefinition of HypertensionDefinition of Hypertension
ClassificationClinic BP
(percentiles)Mean ambulatory SBP (percentiles)
SBP Load (%)
Normal BP <95th <95th <25Normal BP 95 95th 25
White coat HTN >95th <95th <25
Masked HTN <95th >95th >25
P h i 95 95th 25 50Pre‐hypertension >95 <95th 25‐50
Ambulatory HTN >95th >95th 25‐50
Severe ambulatory >95th >95th >50HTN
Urbina et al. Hypertension. 2008
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

Clinical Evaluation of Confirmed Clinical Evaluation of Confirmed H iH i **HypertensionHypertension**
Study or Procedure PurposeStudy or Procedure Purpose
History, including sleep, family, risk Helps focus subsequent factors, diet, smoking, drinking and physical examination
evaluation
BUN creatinine electrolytes R/O renal diseaseBUN, creatinine, electrolytes, urinalysis, and urine culture CBC
R/O renal disease, pyelonephritis anemia
Renal ultrasound R/O renal scar, congenital anomaly
* * All children with persistent BP > 95All children with persistent BP > 95thth percentilepercentile
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
* * All children with persistent BP > 95All children with persistent BP > 95thth percentilepercentile

Clinical Evaluation of Confirmed Clinical Evaluation of Confirmed H iH i **HypertensionHypertension**
Study or Procedure PurposeStudy or Procedure Purpose
Fasting lipid panel, fasting glucose**
Identify hyperlipidemia and metabolic abnormalitiesglucose metabolic abnormalities
Drug screen *** Identify substances causing hypertension
Polysomnography *** Identify sleep disorder associated with HTN
thth* * All children with persistent BP > 95All children with persistent BP > 95thth percentilepercentile
** Overweight children with BP 90** Overweight children with BP 90thth --9494thth percentilepercentile*** History of drugs or snoring*** History of drugs or snoring Fourth Report on BP. Pediatrics August 2004
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
p g

Clinical Evaluation of Confirmed Clinical Evaluation of Confirmed H iH i **HypertensionHypertension**
Study or Procedure PurposeStudy or Procedure Purpose
Echocardiography** Identify LVH or other cardiac involvement
Retinal examination* Identify retinal vascular changes
ABPM *** Identify white coat hypertension
* * All children with persistent BP > 95All children with persistent BP > 95thth percentilepercentile** Children with co morbid risk factors with BP 90** Children with co morbid risk factors with BP 90thth --9494thth percentilepercentile*** When white coat hypertension suspected*** When white coat hypertension suspected
Fourth report on BP Pediatrics August 200
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
Fourth report on BP. Pediatrics August 200

Clinical Evaluation of Confirmed Clinical Evaluation of Confirmed HypertensionHypertension**HypertensionHypertension
Study or Procedure Purposey
Plasma renin level Identify low renin, suggesting mineralocoticoid related HTNmineralocoticoid related HTN
Renovascular imaging Identify renovascular disease
Plasma and urine steroid levels
Identify steroid mediated HTN
Plasma and urine Identify catecholamine mediatedPlasma and urine catecholamines
Identify catecholamine mediated hypertension
* * Young children with stage 1 and any child with stage 2 HTNYoung children with stage 1 and any child with stage 2 HTN
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
Fourth Report on BP. Pediatrics August 2004

Most Common Causes by AgeMost Common Causes by Agey gy g
< 1 th 1 th t < 6
Renal arterial thrombosis Coarctation of aorta
Renal parenchymal diseaseCoarctation of aorta
< 1 month 1 month to < 6 yr
Coarctation of aortaCongenital renal diseaseBPD
Coarctation of aortaRenal arterial stenosis
Renal parenchymal disease Essential hypertension6 to < 10 yr 10 to < 18 yr
Renal parenchymal diseaseRenal arterial stenosisEssential hypertension
Essential hypertensionEssential hypertensionRenal parenchymal disease
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

Classification of Hypertension in ChildrenClassification of Hypertension in Childrenand Adolescents With Therapy Recommendationsand Adolescents With Therapy Recommendationsand Adolescents, With Therapy Recommendationsand Adolescents, With Therapy Recommendations
Therapeutic Lifestyle ChangesTherapeutic Lifestyle Changes
N lN l E h lth di t l dNormalNormal Encourage healthy diet, sleep, and physical activity.
PrePre--hypertensionhypertension Recommend weight management counseling if overweight; introduce physical activity and diet management.
Stage 1 hypertensionStage 1 hypertension Recommend weight managementStage 1 hypertensionStage 1 hypertension Recommend weight management counseling if overweight; introduce physical activity and diet management.
Stage 2 hypertensionStage 2 hypertension Recommend weight management counseling if overweight; introduce physical activity and diet management.
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
Fourth Report on BP. Pediatrics August 2004

What is the antihypertensive group of your first What is the antihypertensive group of your first h i i 14 ld l ith fi dh i i 14 ld l ith fi dchoice in a 14 years old male with confirmed choice in a 14 years old male with confirmed hypertension?hypertension?Choose ONE BEST AnswerChoose ONE BEST AnswerChoose ONE BEST AnswerChoose ONE BEST Answer
A. Thiazide diuretic
B CCBB. CCB
C. Beta blocker
D. ACEi/ARB
E. Benzodiazepine
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org
p

Choosing an AntihypertensiveChoosing an AntihypertensiveChoosing an AntihypertensiveChoosing an AntihypertensiveNo evidence that HCTZ should be first line agent No evidence that HCTZ should be first line agent in children and adolescentsin children and adolescentsRacial differences in response to various drug Racial differences in response to various drug classes have yet to be shown in children and classes have yet to be shown in children and adolescentsadolescentsD h i t i ll b d b fit/ idD h i t i ll b d b fit/ idDrug choice typically based on benefit/side Drug choice typically based on benefit/side effect profile, availability, and ease of effect profile, availability, and ease of administrationadministrationadministrationadministrationMaximizing dose of single agent is Maximizing dose of single agent is recommended before adding an additional agentrecommended before adding an additional agentrecommended before adding an additional agentrecommended before adding an additional agent

Calcium Channel BlockersCalcium Channel BlockersCalcium Channel BlockersCalcium Channel BlockersDihydropyridine CCBsDihydropyridine CCBs
Inhibit Ca influx into vascular smooth muscle whichInhibit Ca influx into vascular smooth muscle which–– Inhibit Ca influx into vascular smooth muscle which Inhibit Ca influx into vascular smooth muscle which decreases peripheral vascular resistancedecreases peripheral vascular resistance
–– Common first line agent when etiology of HTN is unknownCommon first line agent when etiology of HTN is unknown–– Side effectsSide effects
Flushing, Headache, peripheral edema, fatigueFlushing, Headache, peripheral edema, fatigue–– ExamplesExamplesExamplesExamples
Amlodipine (0.1 Amlodipine (0.1 -- 0.6 mg/kg/day q day)0.6 mg/kg/day q day)–– Infants may need BID dosingInfants may need BID dosing–– Can be compounded in a 1 mg/mL suspensionCan be compounded in a 1 mg/mL suspensionp g pp g p
Nifedipine XR (0.25 mg/kg/day Nifedipine XR (0.25 mg/kg/day –– no max dose established q day no max dose established q day or BID)or BID)
–– Capsule must be swallowed wholeCapsule must be swallowed whole
–– The use of short acting CCBs (e.g. Nifedipine) is not The use of short acting CCBs (e.g. Nifedipine) is not recommended for chronic treatment of HTNrecommended for chronic treatment of HTN

ACE Inhibitors/ARBsACE Inhibitors/ARBsACE Inhibitors/ARBsACE Inhibitors/ARBsTypically well tolerated although concern for inducing Typically well tolerated although concern for inducing renal failure limits use prior to evaluationrenal failure limits use prior to evaluationrenal failure limits use prior to evaluationrenal failure limits use prior to evaluationFirst line agents in diabetics and patients with proteinuriaFirst line agents in diabetics and patients with proteinuriaSide effectsSide effects
Cough (ACEi) angioedema decline in renal functionCough (ACEi) angioedema decline in renal function–– Cough (ACEi), angioedema, decline in renal function, Cough (ACEi), angioedema, decline in renal function, hyperkalemiahyperkalemia
–– ACE fetopathy during 2ACE fetopathy during 2ndnd and 3and 3rdrd trimestertrimesterExamplesExamplesExamplesExamples–– Lisinopril (0.07 Lisinopril (0.07 -- 0.6 mg/kg/day q day)0.6 mg/kg/day q day)
May need BID dosing in infantsMay need BID dosing in infantsCan be compounded as a 1 mg/mL suspensionCan be compounded as a 1 mg/mL suspension20 20 –– 30 mg is typically max dose at which BP response is observed30 mg is typically max dose at which BP response is observed
–– Enalapril (0.08 Enalapril (0.08 -- 0.6 mg/kg/day q day or BID)0.6 mg/kg/day q day or BID)Can be compounded as a 1 mg/mL suspensionCan be compounded as a 1 mg/mL suspension
Losartan (0 7Losartan (0 7 1 4 mg/kg/day q day)1 4 mg/kg/day q day)–– Losartan (0.7 Losartan (0.7 -- 1.4 mg/kg/day q day)1.4 mg/kg/day q day)Can be compounded as a 2.5 mg/mLCan be compounded as a 2.5 mg/mL

Management AlgorithmManagement AlgorithmF th R t BP P di t i A t 2004
Measure BP and Height and Calculate BMIDetermine BP category for sex, age, and height
g gg gFourth Report on BP. Pediatrics August 2004
Educate on Heart Healthy
Prehypertensive
90–<95% <90%
Normotensive
TherapeuticLifestyle
Stage 2 Hypertension Stage 1 Hypertension
Repeat BPLifestyle
For the family
Diagnostic Workup Includes
>95%
LifestyleChanges
Repeat BPIn 6 months
Over 3 visits
90–<95% or 120/80 mmHg
or 120/80 mmHg
Diagnostic Workup Includes
Rx Specific
Evaluation for Target-Organ Damage
SecondaryHypertension
In 6 months
Consider Diagnostic Workup and
PrimaryHypertension
Consider Referral
Evaluation for Target-Organ Damage
Therapeutic
SecondaryHypertension
or PrimaryHypertension
Rx Specificfor Cause
>95% OverweightNormal BMI Overweight
Consider Diagnostic Workup and Evaluation for Target-Organ Damage
If overweight or comorbidity exists
Normal BMI
Consider ReferralTo provider with expertisein pediatric hypertension
Overweight Normal BMI
Therapeutic LifestyleChanges
Drug Rx‡ MonitorQ 6 Mo
BMI
Weight Reduction
BMI
Drug Rx Weight Reductionand Drug Rx
Weight Reduction
Still >95%
BMI

Athletic ParticipationAthletic ParticipationAthletic ParticipationAthletic Participation
• Regular, non‐competitive physical activity should be g p p y yencouraged because it reduces hypertension.
• Dynamic exercise– Increase SBP
– Moderate increase in MAP
– Decrease in DBP, and TPR
• Static exercise– SBP, DBP, MAP all increase significantly
– TPR unchanged
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

Athletic ParticipationAthletic ParticipationAthletic ParticipationAthletic Participation
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

IIIABobsledding/lugeField events
IIIBBody buildingDownhill skiing
IIICBoxingCanoeing/kayaking
GymnasticsMartial artsSailing, water skiingWeight liftingWindsurfing
gSnowboardingSkateboardingWrestling
g/ y gCyclingDecathlonRowingSpeed skatingTriathlonWindsurfing Triathlon
IIAArcheryAuto racingDiving
IIBAmerican football, jumpingFigure skating, RodeoRugby
IICBasketballIce hockeyCross country skiingDiving
EquestrianMotorcycling
RugbyRunning (sprint)SurfingSynchronized swimming
Cross‐country skiingLacrosseRunningTeam handball
IABilliardsBowlingCricket
IBBaseball/softballFencingTable tennis
ICBadmintonField hockey, TennisOrienteering
CurlingGolfRiflery
Volleyball Race walkingRacquetball/squashRunning (long distance)Soccer
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

RecommendationsRecommendationsRecommendationsRecommendations
• Lifestyle modification.y
• Pre‐hypertension , no restriction.
• Stage I hypertension: In absence of TOD including g yp gLVH or concomitant heart disease , no restriction. Recheck BP in 1‐2 weeks to confirm hypertension
• Stage 2 hypertension: in the absence of TOD, restrict high static sport until BP in normal range.
• HTN and other CV disease– Participation is based on type and severity of CVS disease
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

RecommendationsRecommendationsRecommendationsRecommendations
• Salt intake in athletes.
• Care should be taken to appropriately diagnose and monitor the overweight athletes and athletes with spinal cord injuries
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org

SummarySummarySummarySummary
• Prevalence of hypertension is much lower in childrenPrevalence of hypertension is much lower in children compared to adults but has increased significantly in last 15 years.
• Adult hypertension may have roots in pediatric age, so it is important to identify these children.
• Accurate BP measurement is the key for diagnosis.
• ABPM study may be helpful before initiating pharmacologic treatment.
archildrens.org uams.eduarpediatrics.orgarchildrens.org uams.eduarpediatrics.org