hypertension lin show pdf -...
TRANSCRIPT

Masked HypertensionWhy Should We Care?
Dr. Peter J. Lin Director Primary Care Initiatives - Canadian Heart Research Centre
PRESENTER DISCLOSUREFaculty: Dr. Peter Lin•Relationships with commercial interests:
•Grants/Research Support: None
•Speakers Bureau/Honoraria: Astrazeneca, BMS, Takeda, Purdue BoeringherIngelheim, Bayer, Eli Lilly, Amgen, Janssen, Forest Laboratories, J&J, Merck, Novartis, Pfizer, Servier, Sanofi, Abbott, Mylan
•Consulting Fees: Astrazeneca, Boeringher Ingelheim, Bayer, Eli Lilly, Merck, Sanofi, Amgen, MdBriefCase•Other: None
MITIGATING POTENTIAL BIAS
Potential bias was mitigated through the use of current Hypertension Canada guidelines as the primary literature source for recommendations in the slide deck.
1931 - Key Opinion Leaders :
Please do not measure the blood pressure because you
might want to treat it.


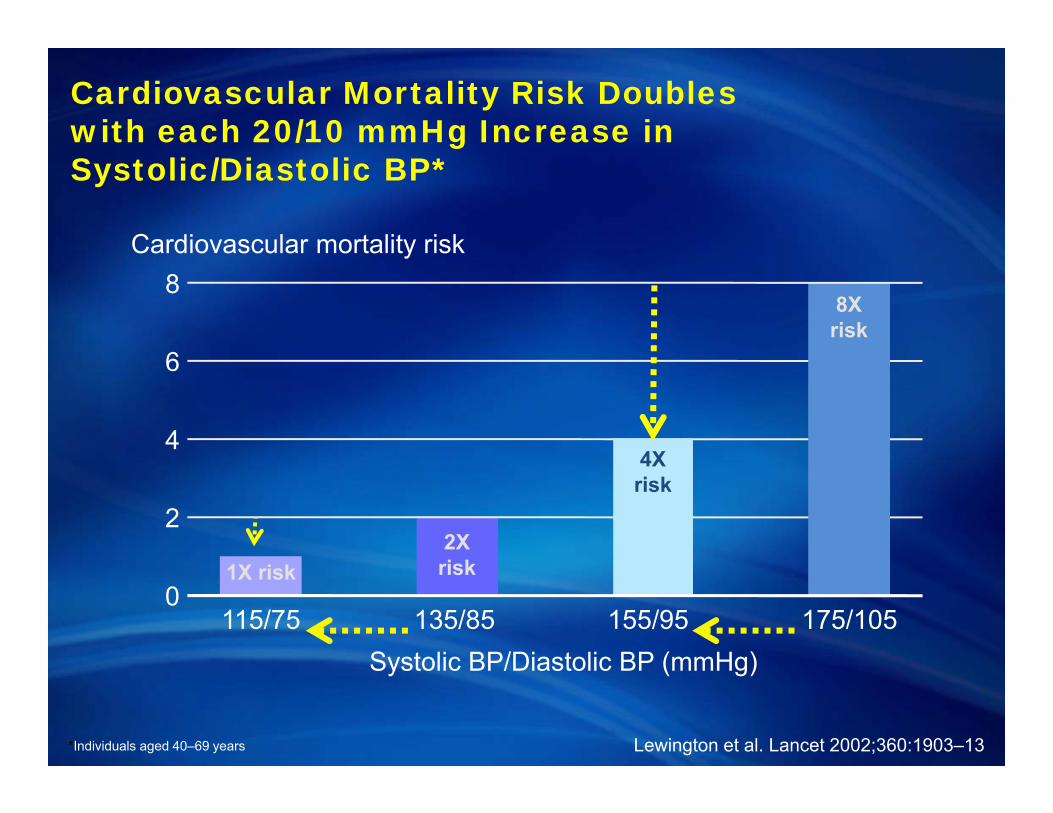
1X risk2X risk
Cardiovascular mortality risk
0
2
4
8
115/75 135/85 155/95 175/105
6
Systolic BP/Diastolic BP (mmHg)
*Individuals aged 40–69 years
4X risk
8X risk
Cardiovascular Mortality Risk Doubles with each 20/10 mmHg Increase in Systolic/Diastolic BP*
Lewington et al. Lancet 2002;360:1903–13
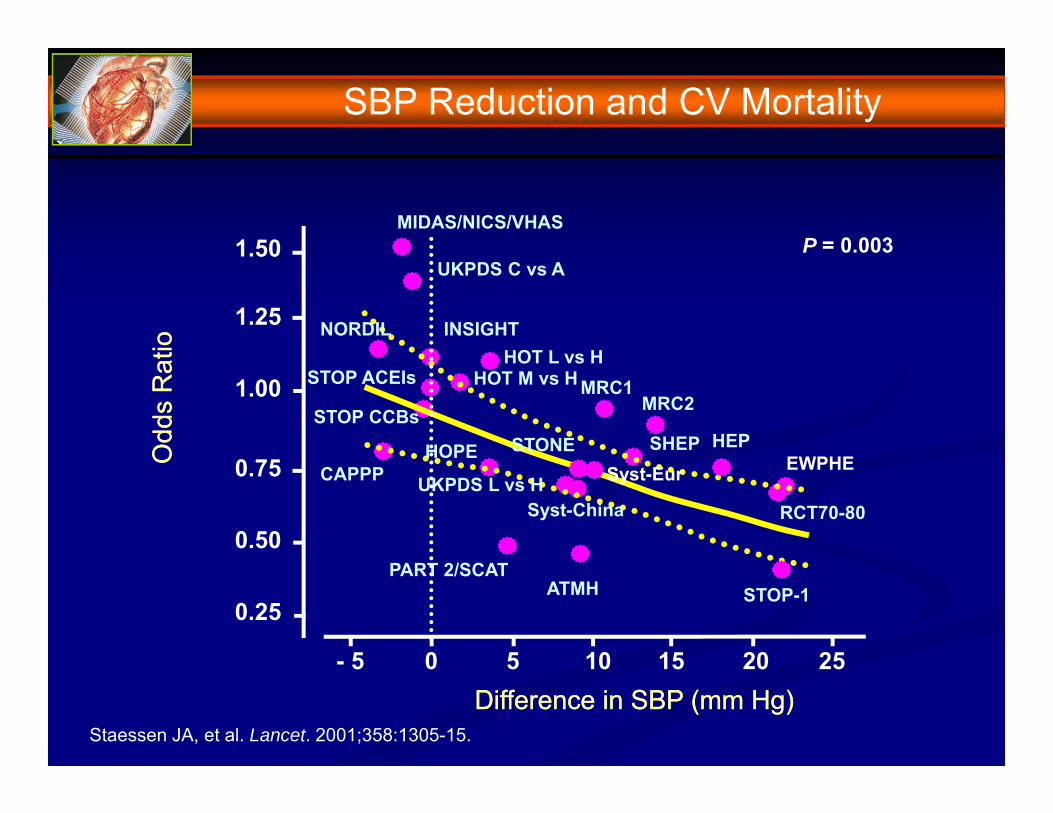
Staessen JA, et al. Lancet. 2001;358:1305-15.
Difference in SBP (mm Hg)Difference in SBP (mm Hg)
Odd
s R
atio
Odd
s R
atio
P = 0.003
0 5 10 15 20 25- 5
HOPE
MIDAS/NICS/VHAS
UKPDS C vs A
NORDIL INSIGHTHOT L vs H
HOT M vs HSTOP ACEIs
STOP CCBs
CAPPP UKPDS L vs HSyst-China
STONESyst-Eur
MRC1MRC2
SHEP HEPEWPHE
RCT70-80
STOP-1PART 2/SCAT
ATMH
1.50
1.25
1.00
0.75
0.50
0.25
SBP Reduction and CV Mortality

Staessen JA, et al. Lancet. 2001;358:1305-15.
Difference in SBP (mm Hg)Difference in SBP (mm Hg)
Odd
s R
atio
Odd
s R
atio
P = 0.003
0 5 10 15 20 25- 5
1.50
1.25
1.00
0.75
0.50
0.25
SBP Reduction and CV Mortality

102009 Canadian Hypertension Education Program Recommendations2009 Canadian Hypertension Education Program Recommendations
Office SBP mmHg
Hom
e or
Day
tim
e A
BP
MS
BP
mm
Hg
135 135
140
140
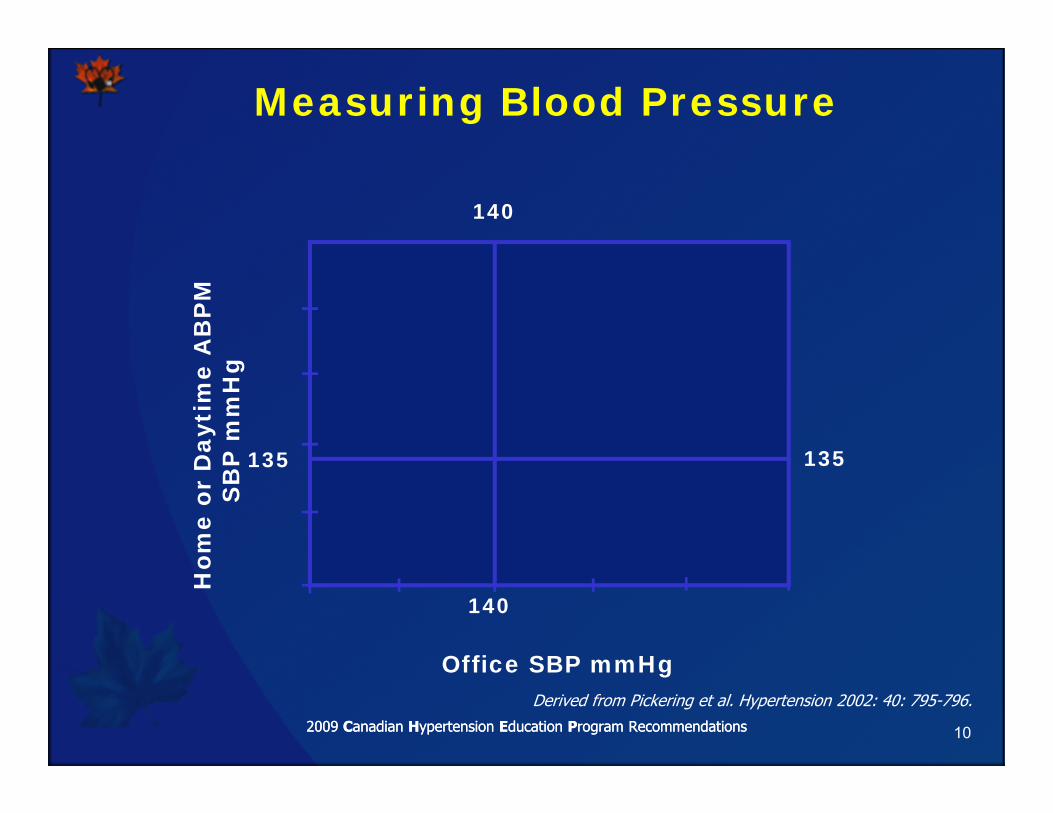
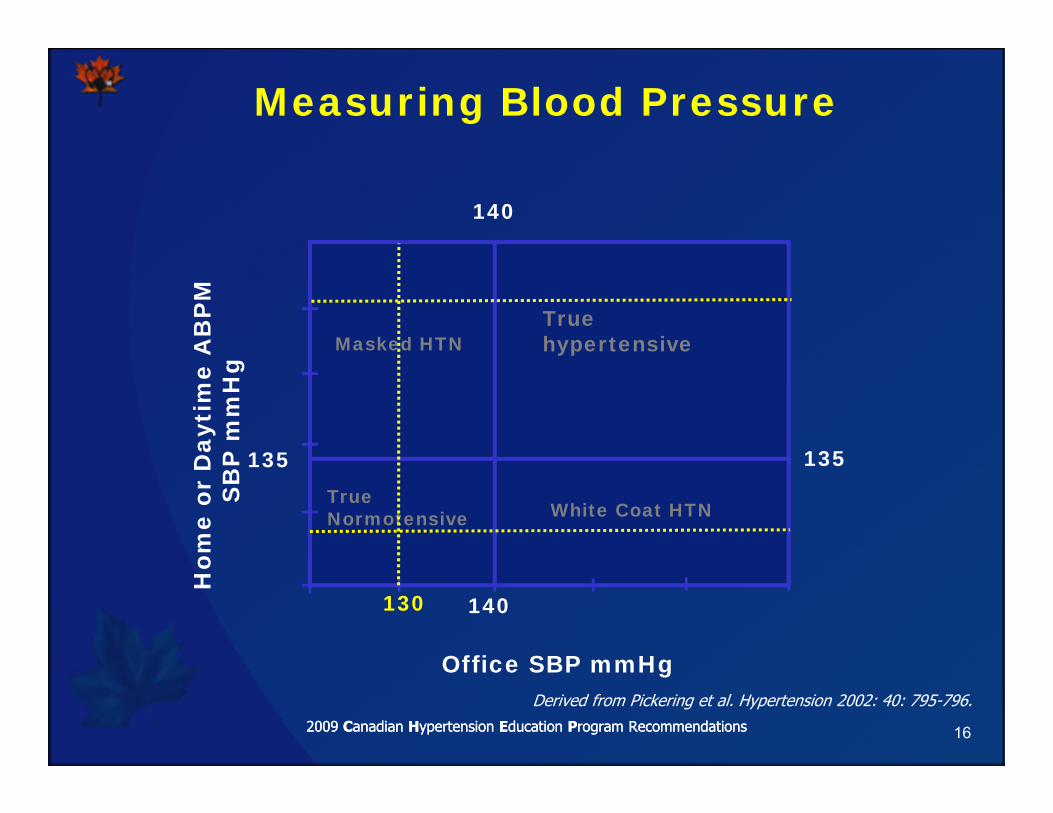
Derived from Pickering et al. Hypertension 2002: 40: 795-796.
Measuring Blood Pressure

112009 Canadian Hypertension Education Program Recommendations2009 Canadian Hypertension Education Program Recommendations
Office SBP mmHg
Hom
e or
Day
tim
e A
BP
MS
BP
mm
Hg
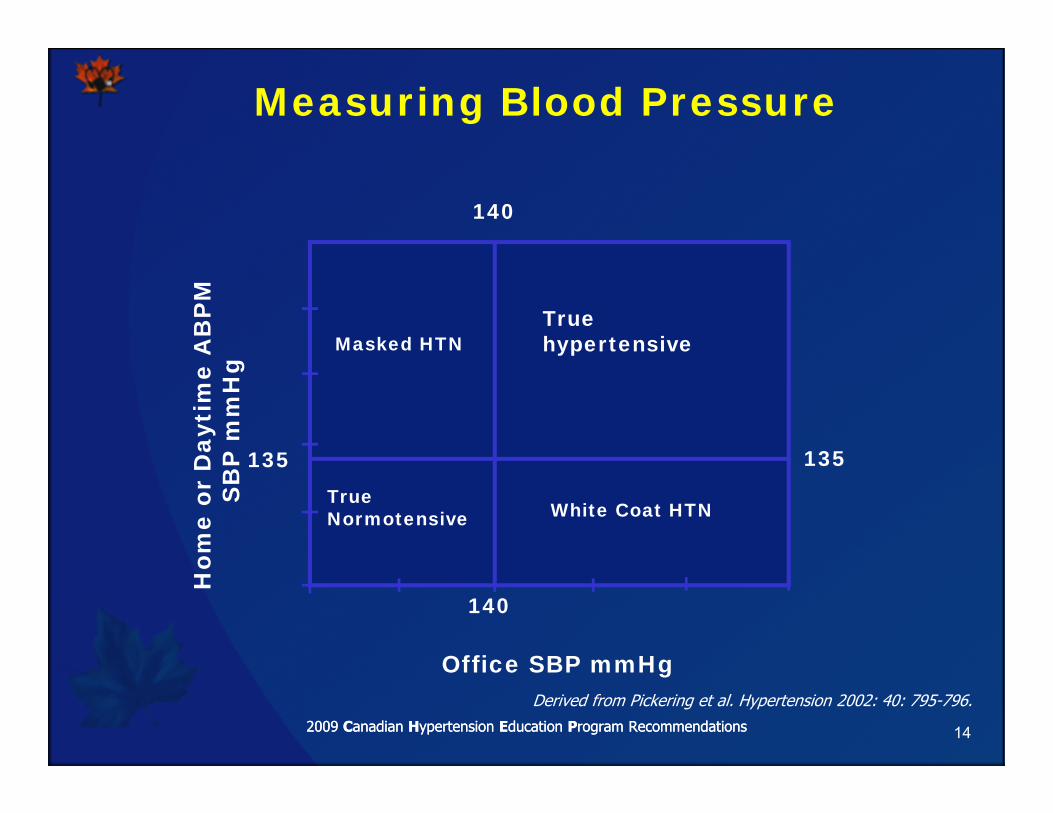
Truehypertensive
TrueNormotensive White Coat HTN
135
140
135
140
Derived from Pickering et al. Hypertension 2002: 40: 795-796.
Measuring Blood Pressure
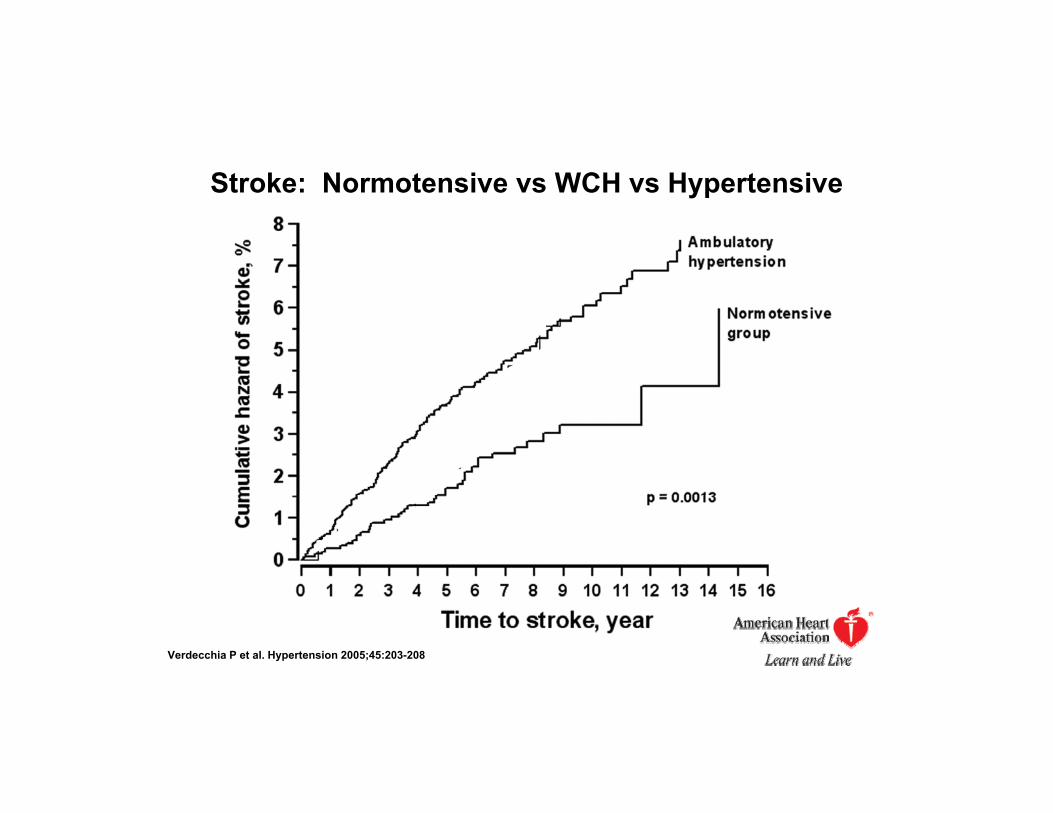
Stroke: Normotensive vs WCH vs Hypertensive
Verdecchia P et al. Hypertension 2005;45:203-208

Stroke: Normotensive vs WCH vs Hypertensive
Verdecchia P et al. Hypertension 2005;45:203-208
142009 Canadian Hypertension Education Program Recommendations2009 Canadian Hypertension Education Program Recommendations
Office SBP mmHg
Hom
e or
Day
tim
e A
BP
MS
BP
mm
Hg
Truehypertensive
TrueNormotensive White Coat HTN
Masked HTN
135
140
135
140
Derived from Pickering et al. Hypertension 2002: 40: 795-796.
Measuring Blood Pressure

152009 Canadian Hypertension Education Program Recommendations2009 Canadian Hypertension Education Program Recommendations
Office SBP mmHg
Hom
e or
Day
tim
e A
BP
MS
BP
mm
Hg
Truehypertensive
TrueNormotensive White Coat HTN
Masked HTN
135
140
135
140
Derived from Pickering et al. Hypertension 2002: 40: 795-796.
Measuring Blood Pressure
150
162009 Canadian Hypertension Education Program Recommendations2009 Canadian Hypertension Education Program Recommendations
Office SBP mmHg
Hom
e or
Day
tim
e A
BP
MS
BP
mm
Hg
Truehypertensive
TrueNormotensive White Coat HTN
Masked HTN
135
140
135
140
Derived from Pickering et al. Hypertension 2002: 40: 795-796.
Measuring Blood Pressure
130
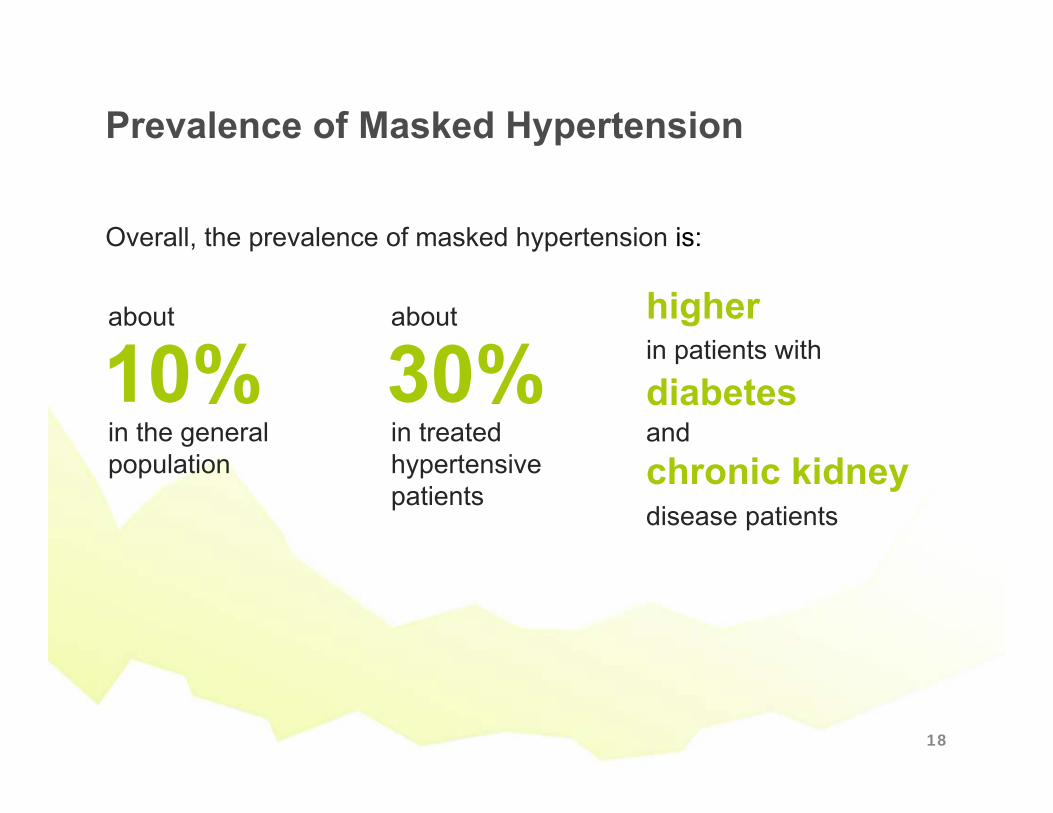
Prevalence of Masked Hypertension
Overall, the prevalence of masked hypertension is:
10%about
in the general population
30%about
in treated hypertensive patients
diabetesin patients with
and
higher
chronic kidney disease patients
18

19
20
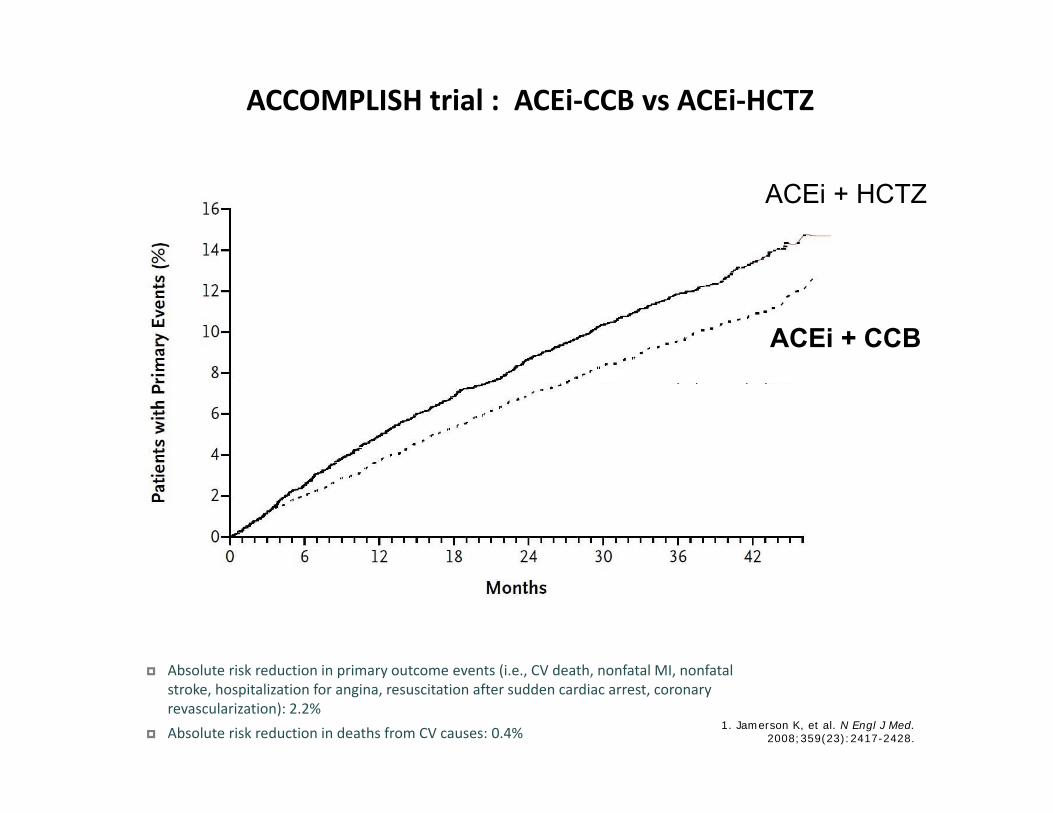
ACCOMPLISH trial : ACEi‐CCB vs ACEi‐HCTZ
Absolute risk reduction in primary outcome events (i.e., CV death, nonfatal MI, nonfatal stroke, hospitalization for angina, resuscitation after sudden cardiac arrest, coronary revascularization): 2.2%
Absolute risk reduction in deaths from CV causes: 0.4% 1. Jamerson K, et al. N Engl J Med. 2008;359(23):2417-2428.
ACEi + HCTZ
ACEi + CCB
21
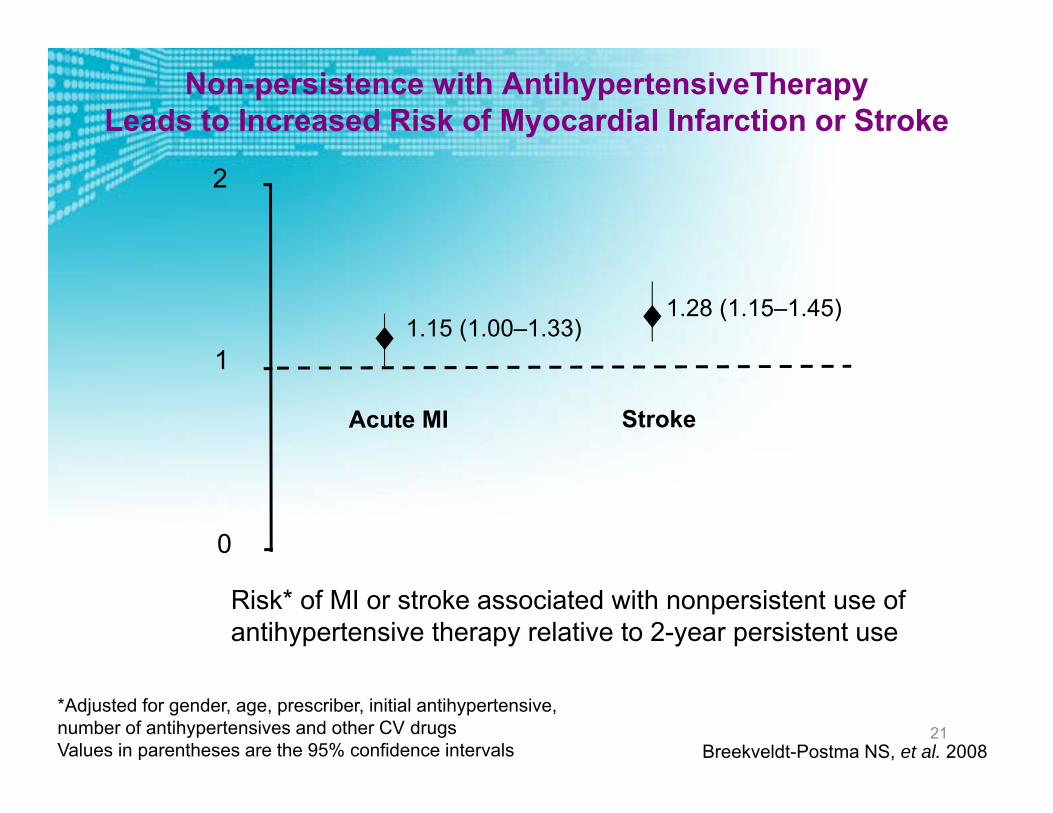
Non-persistence with AntihypertensiveTherapy Leads to Increased Risk of Myocardial Infarction or Stroke
Risk* of MI or stroke associated with nonpersistent use of antihypertensive therapy relative to 2-year persistent use
*Adjusted for gender, age, prescriber, initial antihypertensive,number of antihypertensives and other CV drugsValues in parentheses are the 95% confidence intervals Breekveldt-Postma NS, et al. 2008
1
Acute MI Stroke
1.15 (1.00–1.33)1.28 (1.15–1.45)
0
2

22
Poor Compliance is Linked to Hospitalization Risk
Level of compliance (%)
All-cause hospitalization risk† (%)
†The probability of one or more hospitalizations during a 12-month period*p<0.05 vs 80–100% compliant group
(n=350) (n=344) (n=562) (n=921) (n=5804)
Sokol MC, et al. 2005
**
*
*
4439
36
3027
0
10
20
30
40
50
1–19 20–39 40–59 60–79 80–100

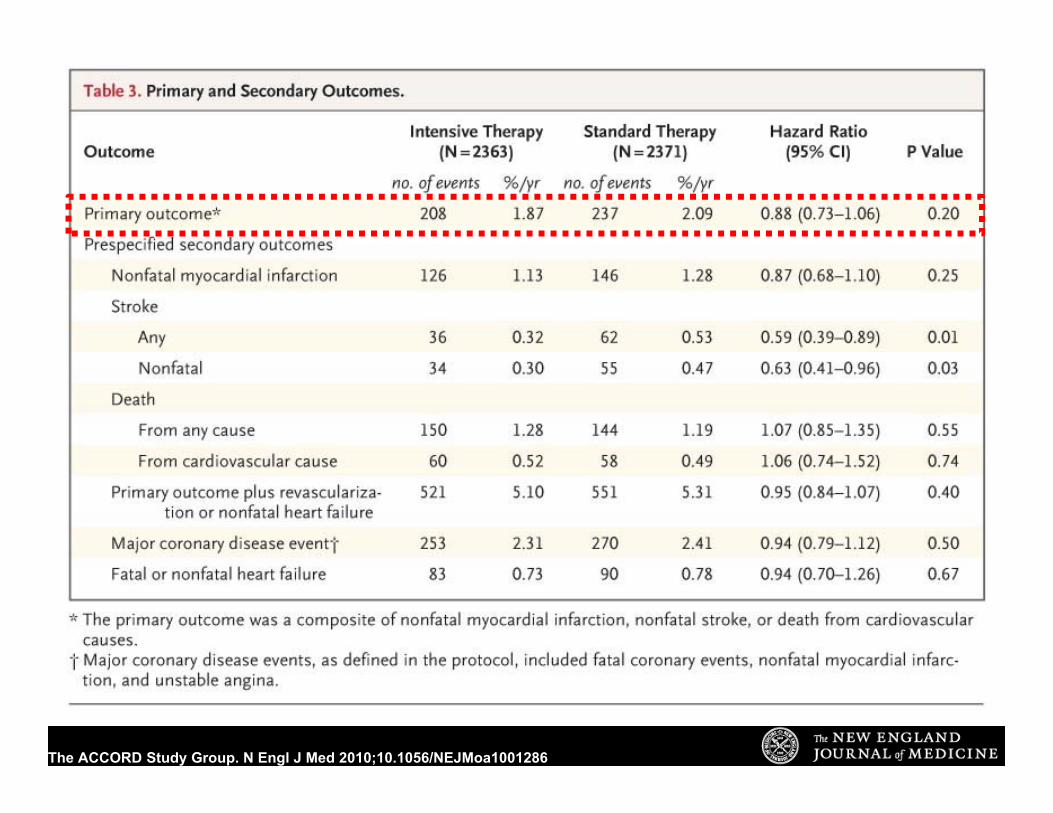
The ACCORD Study Group. N Engl J Med 2010;10.1056/NEJMoa1001286
ACCORD – Blood Pressure
135 mmHg
120 mmHg
The ACCORD Study Group. N Engl J Med 2010;10.1056/NEJMoa1001286
1X risk2X risk
Cardiovascular mortality risk
0
2
4
8
115/75 135/85 155/95 175/105
6
Systolic BP/Diastolic BP (mmHg)
*Individuals aged 40–69 years
4X risk
8X risk
Cardiovascular Mortality Risk Doubles with each 20/10 mmHg Increase in Systolic/Diastolic BP*
Lewington et al. Lancet 2002;360:1903–13

mmHg
ALLHAT 1
HOPE
PROGRESS
CAPPP
INSIGHT
NORDIL
HOT
STONE
STOP-2
LIFE
ALLHAT 2
ANBP2
INVEST
SCOPE
ASCOTVALUE
BP reductions achieved in recent trials
Mancia and Grassi J.Hypertension 2002 updated
130
140
150
160
170
180
190
200
SBP
Recommendations: Hypertension/ Blood Pressure Control (2)
Systolic Targets:• People with diabetes and hypertension should be
treated to a systolic blood pressure goal of <140 mmHg. A
American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87

The ACCORD Study Group. N Engl J Med 2010;10.1056/NEJMoa1001286
Stroke benefit

Recommendations: Hypertension/ Blood Pressure Control (2)
Systolic Targets:• People with diabetes and hypertension should be
treated to a systolic blood pressure goal of <140 mmHg. A
• Lower systolic targets, such as <130 mmHg, may be appropriate for certain individuals at high risk of CVD, if they can be achieved without undue treatment burden. C
American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87

mmHgmmHg
ALLHAT 1
HOPE
PROGRESS
CAPPP
INSIGHT
NORDIL
HOT
STONE
STOP-2
LIFE
ALLHAT 2
ANBP2
INVEST
SCOPE
ASCOTVALUE
BP reductions achieved in recent trials
Mancia and Grassi J.Hypertension 2002 updated
130
140
150
160
170
180
190
200
SBP
70
80
90
100
110
120
DBP

BP Control Reduces CV Events: HOT Trial
Hansson et al. Lancet. 1998;351:1755.
P<0.005
MI,
stro
ke, C
V m
orta
lity/
1000
pt-y
Diabetes SubgroupDiabetes Subgroup
90 mm Hg (n=501)85 mm Hg (n=501)80 mm Hg (n=499)
Goal of therapy: target diastolic BP24.4
18.8
11.9
30
25
20
15
10
5
0
< 80 mmHg
< 85 mmHg

Source: Hansson L et al. Lancet 1998;351:1755-1762
Hypertension Optimal Treatment (HOT) Study
Diastolic BP goal
Patients without Diabetes
Maj
or C
V ev
ents
per
1000
pat
ient
-yea
rs
Patients with Diabetes
Diastolic BP goal
18,790 patients with a baseline diastolic BP of 100-115 mm Hg randomized to a target diastolic BP of <90 mm Hg, <85 mm Hg, or <80 mm Hg
More intensive blood pressure control provides greater benefit in patients with diabetes
Blood Pressure Lowering Therapy Evidence: Effect of Intensive Blood Pressure Control
BP=Blood pressure, CV=Cardiovascular
Recommendations: Hypertension/ Blood Pressure Control (3)
Diastolic Targets:• Patients with diabetes should be treated to a
diastolic blood pressure <90 mmHg. A• Lower diastolic targets, such as <80 mmHg,
may be appropriate for certain individuals at high risk for CVD if they can be achieved without undue treatment burden. C
American Diabetes Association Standards of Medical Care in Diabetes. Cardiovascular disease and risk management. Diabetes Care 2017; 40 (Suppl. 1): S75-S87

Pre SPRINT Targets
Population SBP DBPHigh Risk (SPRINT) ≤120 NADiabetes < 130 < 80All others* < 140 < 90
*Target BP with Automated Office Blood Pressure (AOBP) threshold < 135/85
Leung AA. 2016 CHEP Guidelines. Hypertension Canada’s 2016 Canadian Hypertension Education Program Guidelines for Blood PressureMeasurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Can Cardio Soc 2016;32:569-588.

SPRINT Trial ACCORD Trial
• Patients (n=9361)• age ≥50 years• SBP ≥130 mm Hg• ↑CV risk (but without diabetes) • assigned to:
o SBP target <120 mm Hg (intensive treatment), oro SBP target <140 mm Hg (standard treatment)
• Primary composite outcome: MI, other acute coronary syndromes, stroke, HF, or death from CV causes
1. SPRINT Research Group. N Engl J Med 2015.

Mean SBP136.2 mm Hg
Mean SBP121.4 mm Hg
Standard
Intensive
Year 1

Number ofParticipants
Hazard Ratio = 0.75 (95% CI: 0.64 to 0.89) Standard
Intensive(243 events)
Mean Follow up = 3.26 yearsNNT=61
SPRINT Primary Outcome
(319 events)

Adapt from Figure 2B in the N Engl J Med manuscript
Include NNT
All‐cause Mortality
Standard(210 deaths)
Intensive(155 deaths)
Hazard Ratio = 0.73 (95% CI: 0.60 to 0.90)NNT = 90Median = 3.26 years

Primary Outcome Experience in the Six Pre‐specified Subgroups of Interest
*Treatment by subgroup interaction
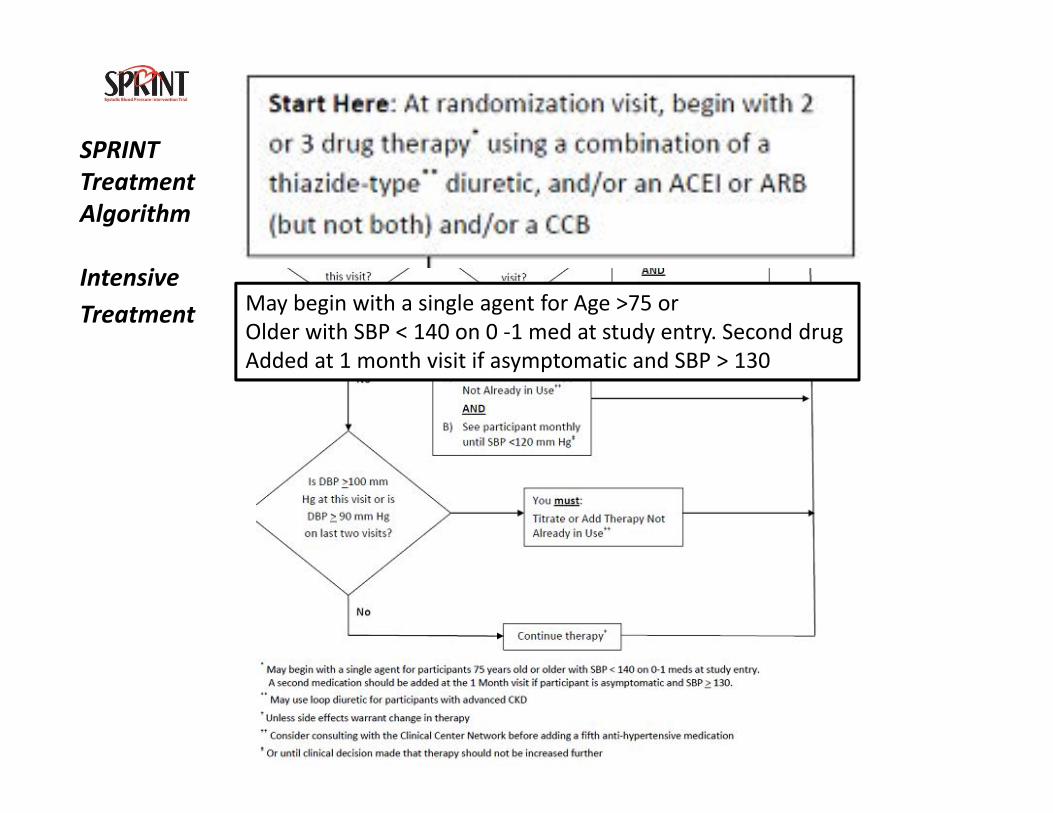
SPRINTTreatmentAlgorithm
IntensiveTreatment May begin with a single agent for Age >75 or
Older with SBP < 140 on 0 ‐1 med at study entry. Second drugAdded at 1 month visit if asymptomatic and SBP > 130

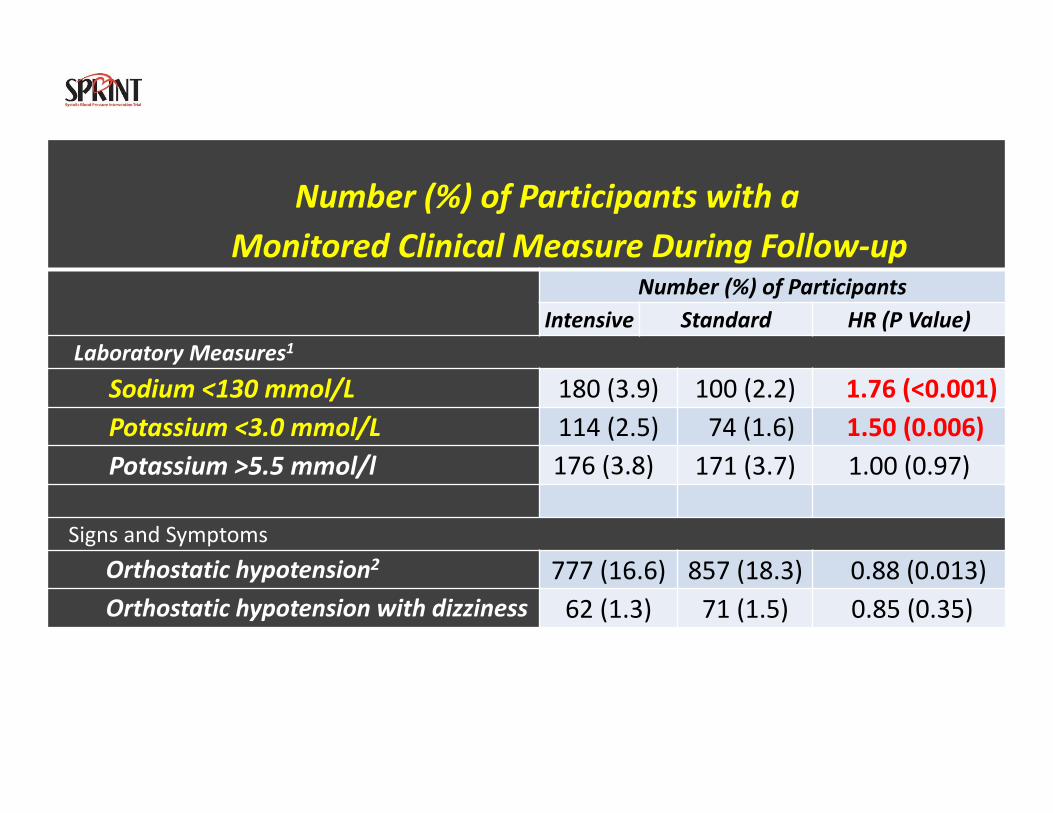
Number (%) of Participants with aMonitored Clinical Measure During Follow‐up
Number (%) of ParticipantsIntensive Standard HR (P Value)
Laboratory Measures1
Sodium <130 mmol/L 180 (3.9) 100 (2.2) 1.76 (<0.001)Potassium <3.0 mmol/L 114 (2.5) 74 (1.6) 1.50 (0.006)Potassium >5.5 mmol/l 176 (3.8) 171 (3.7) 1.00 (0.97)
Signs and SymptomsOrthostatic hypotension2 777 (16.6) 857 (18.3) 0.88 (0.013)Orthostatic hypotension with dizziness 62 (1.3) 71 (1.5) 0.85 (0.35)
1. Detected on routine or PRN labs; routine labs drawn quarterly for first year, then q 6 months2. Drop in SBP ≥20 mmHg or DBP ≥10 mmHg 1 minute after standing (measured at 1, 6, and 12 months and yearly thereafter)
Number (%) of Participants with aMonitored Clinical Measure During Follow‐up
Number (%) of ParticipantsIntensive Standard HR (P Value)
Laboratory Measures1
Sodium <130 mmol/L 180 (3.9) 100 (2.2) 1.76 (<0.001)Potassium <3.0 mmol/L 114 (2.5) 74 (1.6) 1.50 (0.006)Potassium >5.5 mmol/l 176 (3.8) 171 (3.7) 1.00 (0.97)
Signs and SymptomsOrthostatic hypotension2 777 (16.6) 857 (18.3) 0.88 (0.013)Orthostatic hypotension with dizziness 62 (1.3) 71 (1.5) 0.85 (0.35)
1. Detected on routine or PRN labs; routine labs drawn quarterly for first year, then q 6 months2. Drop in SBP ≥20 mmHg or DBP ≥10 mmHg 1 minute after standing (measured at 1, 6, and 12 months and yearly thereafter)

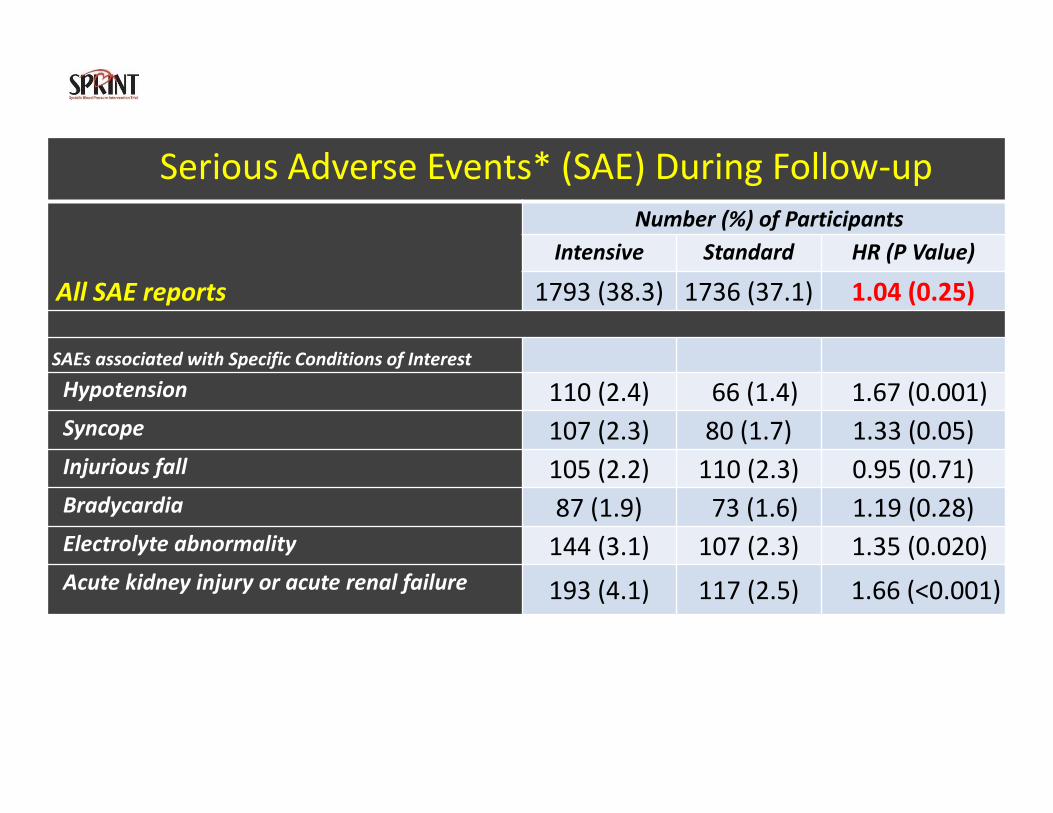
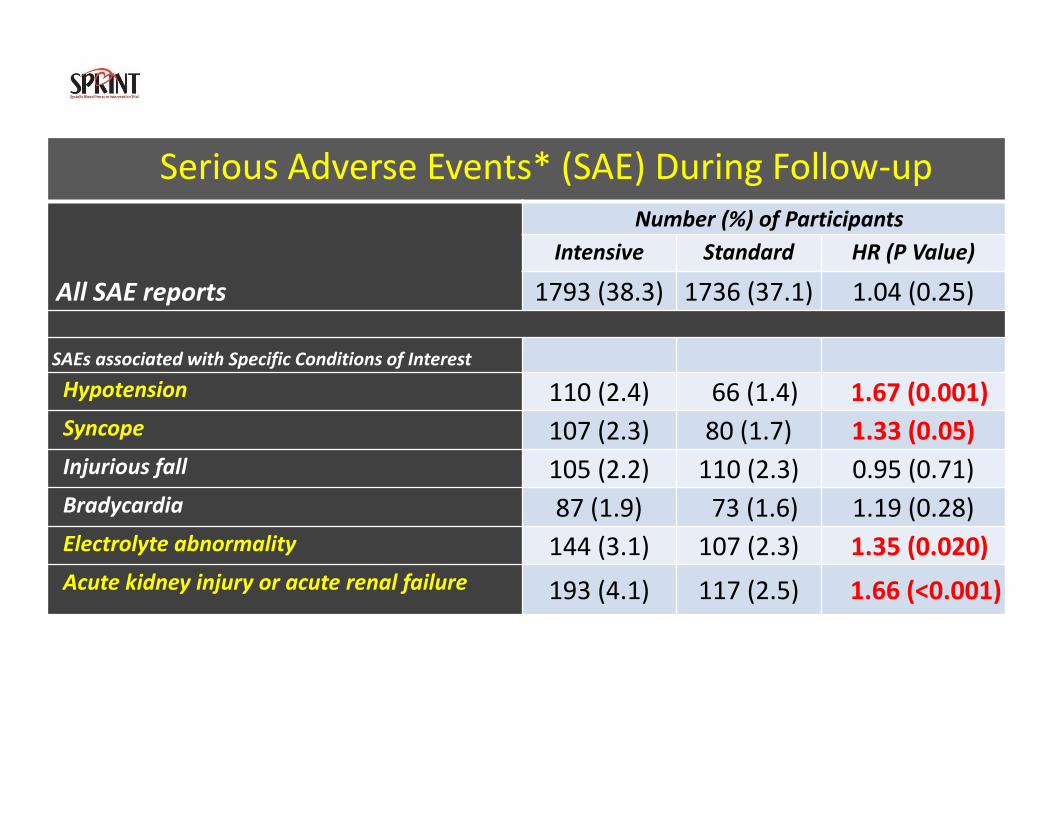
Serious Adverse Events* (SAE) During Follow‐up
All SAE reports
Number (%) of ParticipantsIntensive Standard HR (P Value)
1793 (38.3) 1736 (37.1) 1.04 (0.25)
SAEs associated with Specific Conditions of Interest
Hypotension 110 (2.4) 66 (1.4) 1.67 (0.001)Syncope 107 (2.3) 80 (1.7) 1.33 (0.05)Injurious fall 105 (2.2) 110 (2.3) 0.95 (0.71)Bradycardia 87 (1.9) 73 (1.6) 1.19 (0.28)Electrolyte abnormality 144 (3.1) 107 (2.3) 1.35 (0.020)Acute kidney injury or acute renal failure 193 (4.1) 117 (2.5) 1.66 (<0.001)
*Fatal or life threatening event, resulting in significant or persistent disability,requiring or prolonging hospitalization, or judged important medical event.
Serious Adverse Events* (SAE) During Follow‐up
All SAE reports
Number (%) of ParticipantsIntensive Standard HR (P Value)
1793 (38.3) 1736 (37.1) 1.04 (0.25)
SAEs associated with Specific Conditions of Interest
Hypotension 110 (2.4) 66 (1.4) 1.67 (0.001)Syncope 107 (2.3) 80 (1.7) 1.33 (0.05)Injurious fall 105 (2.2) 110 (2.3) 0.95 (0.71)Bradycardia 87 (1.9) 73 (1.6) 1.19 (0.28)Electrolyte abnormality 144 (3.1) 107 (2.3) 1.35 (0.020)Acute kidney injury or acute renal failure 193 (4.1) 117 (2.5) 1.66 (<0.001)
*Fatal or life threatening event, resulting in significant or persistent disability,requiring or prolonging hospitalization, or judged important medical event.
Serious Adverse Events* (SAE) During Follow‐up
All SAE reports
Number (%) of ParticipantsIntensive Standard HR (P Value)
1793 (38.3) 1736 (37.1) 1.04 (0.25)
SAEs associated with Specific Conditions of Interest
Hypotension 110 (2.4) 66 (1.4) 1.67 (0.001)Syncope 107 (2.3) 80 (1.7) 1.33 (0.05)Injurious fall 105 (2.2) 110 (2.3) 0.95 (0.71)Bradycardia 87 (1.9) 73 (1.6) 1.19 (0.28)Electrolyte abnormality 144 (3.1) 107 (2.3) 1.35 (0.020)Acute kidney injury or acute renal failure 193 (4.1) 117 (2.5) 1.66 (<0.001)
*Fatal or life threatening event, resulting in significant or persistent disability,requiring or prolonging hospitalization, or judged important medical event.
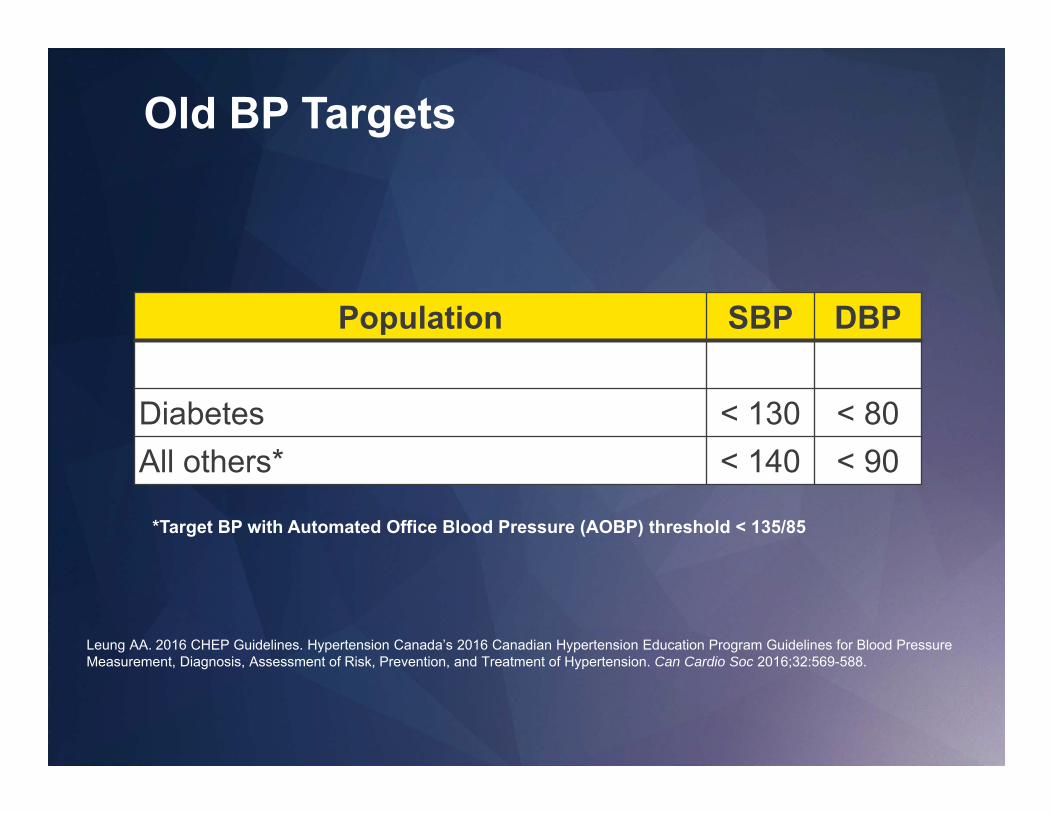
Old BP Targets
Population SBP DBPHigh Risk (SPRINT) ≤120 NADiabetes < 130 < 80All others* < 140 < 90
*Target BP with Automated Office Blood Pressure (AOBP) threshold < 135/85
Leung AA. 2016 CHEP Guidelines. Hypertension Canada’s 2016 Canadian Hypertension Education Program Guidelines for Blood PressureMeasurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Can Cardio Soc 2016;32:569-588.
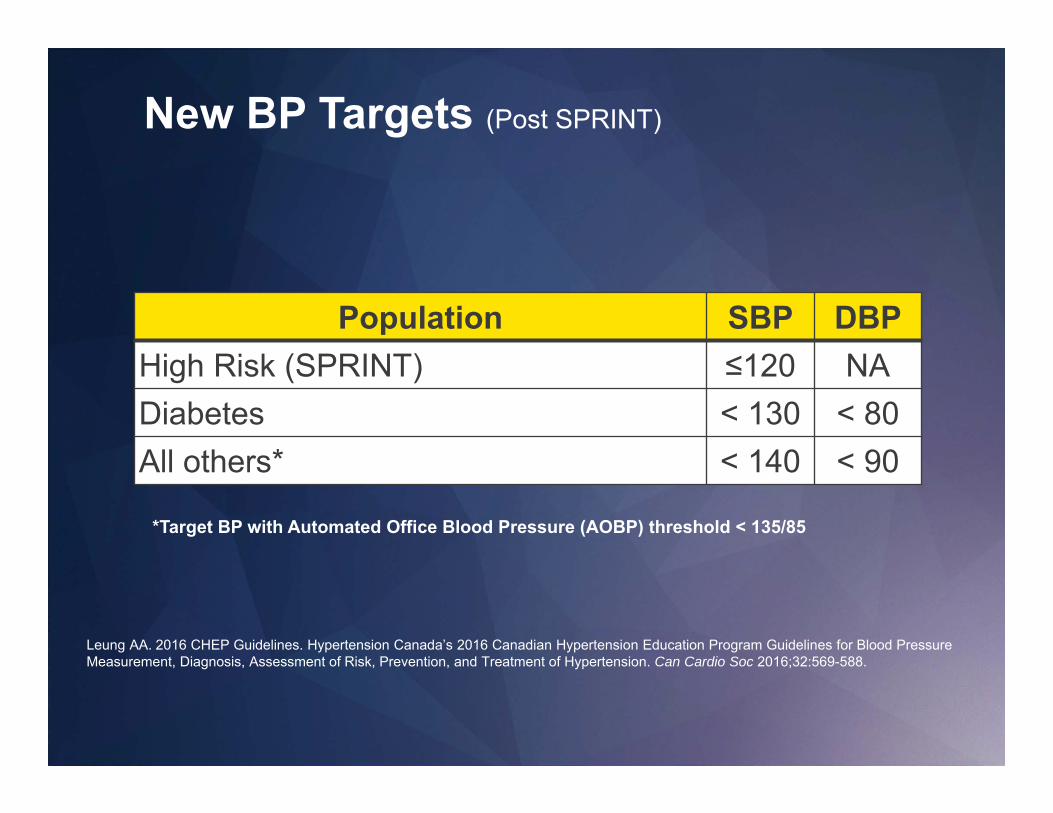
New BP Targets (Post SPRINT)
Population SBP DBPHigh Risk (SPRINT) ≤120 NADiabetes < 130 < 80All others* < 140 < 90
*Target BP with Automated Office Blood Pressure (AOBP) threshold < 135/85
Leung AA. 2016 CHEP Guidelines. Hypertension Canada’s 2016 Canadian Hypertension Education Program Guidelines for Blood PressureMeasurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Can Cardio Soc 2016;32:569-588.
Who is a High Risk (SPRINT) Patient? Someone with any of the following:
Leung AA. 2016 CHEP Guidelines. Hypertension Canada’s 2016 Canadian Hypertension Education Program Guidelines for Blood PressureMeasurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Can Cardio Soc 2016;32:569-588.
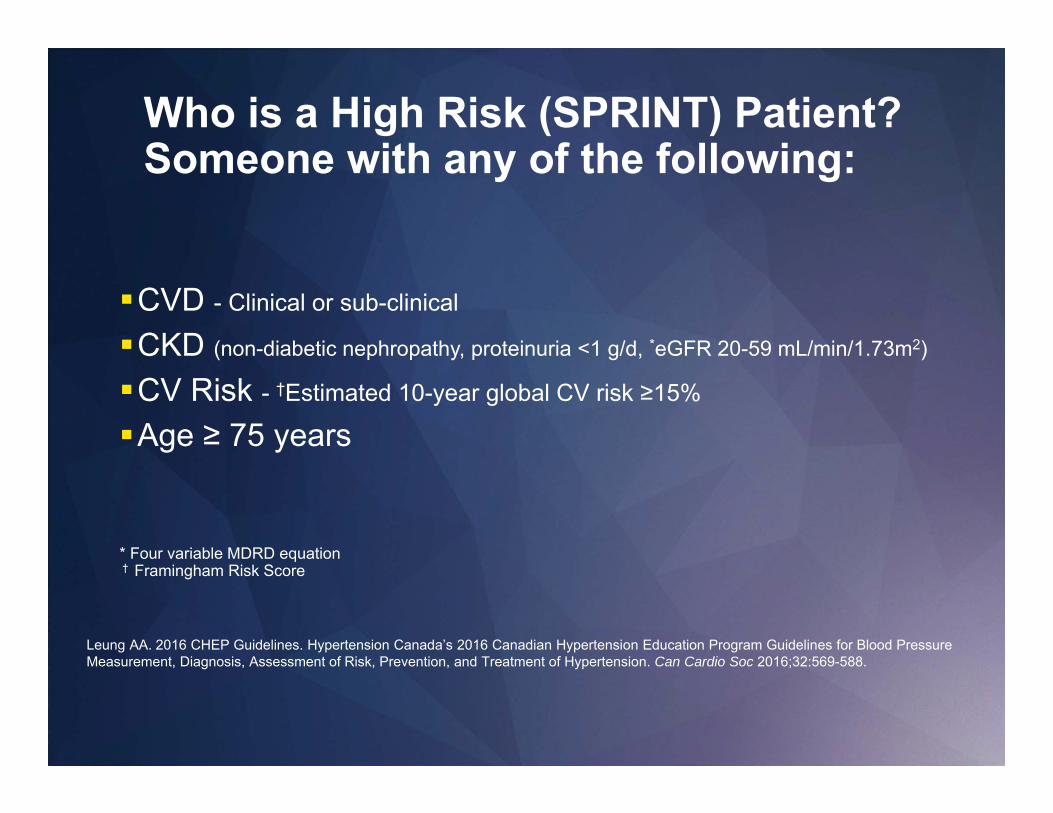
Who is a High Risk (SPRINT) Patient? Someone with any of the following:
CVD - Clinical or sub-clinical
CKD (non-diabetic nephropathy, proteinuria <1 g/d, *eGFR 20-59 mL/min/1.73m2)
CV Risk - †Estimated 10-year global CV risk ≥15%
Age ≥ 75 years
* Four variable MDRD equation† Framingham Risk Score
Leung AA. 2016 CHEP Guidelines. Hypertension Canada’s 2016 Canadian Hypertension Education Program Guidelines for Blood PressureMeasurement, Diagnosis, Assessment of Risk, Prevention, and Treatment of Hypertension. Can Cardio Soc 2016;32:569-588.

How do you make it easy?Systolic ≤ 120 < 130/80 <140/90
Diabetes □CVD □CKD (eGFR 20-59) □CV Risk > 15% □Age > 75 □Nothing from list □
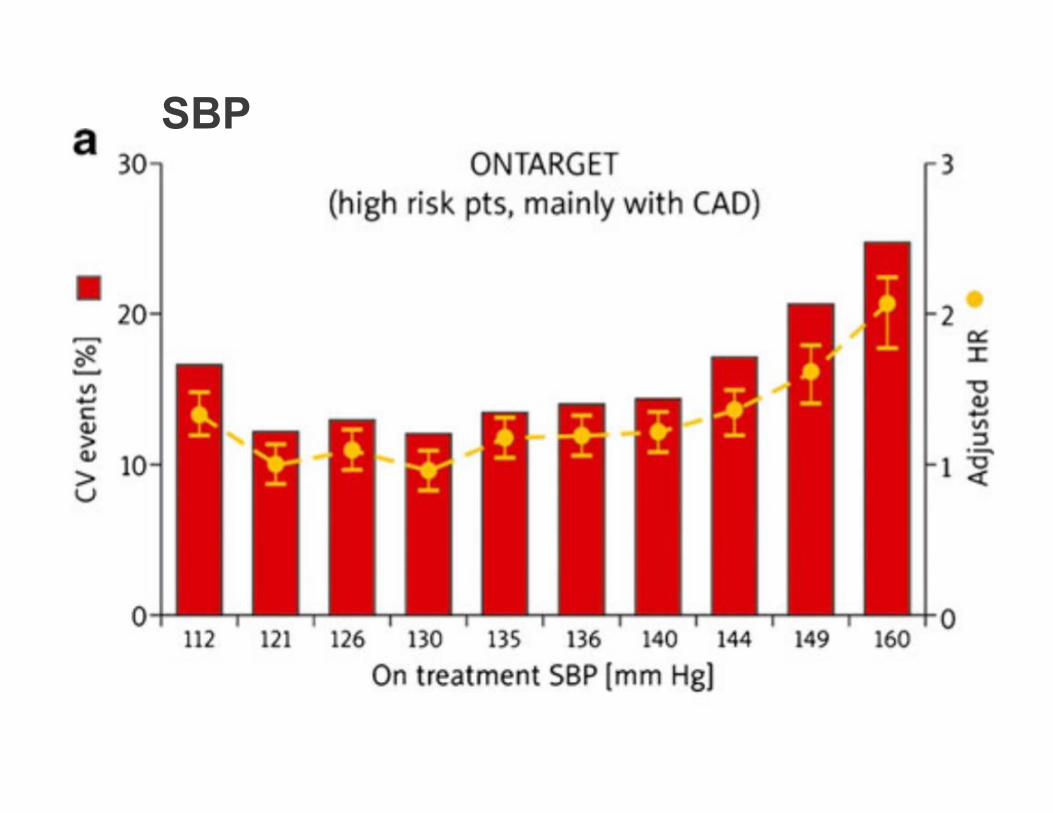
SBP

DBP
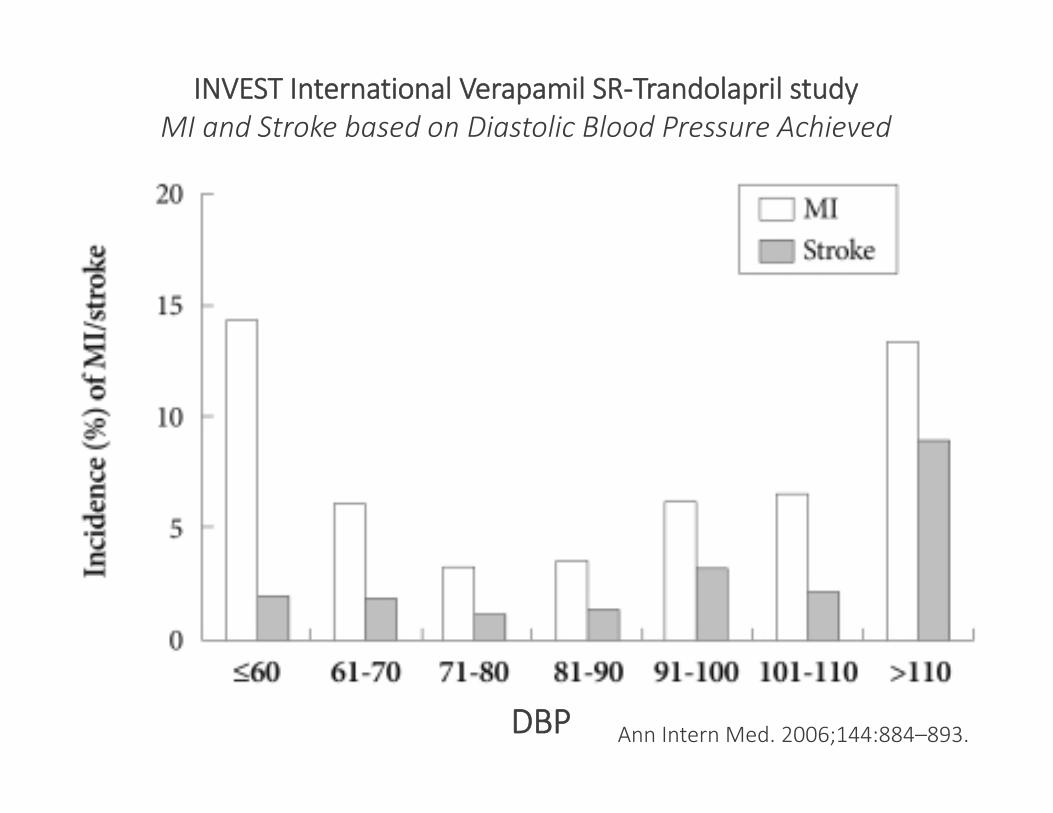
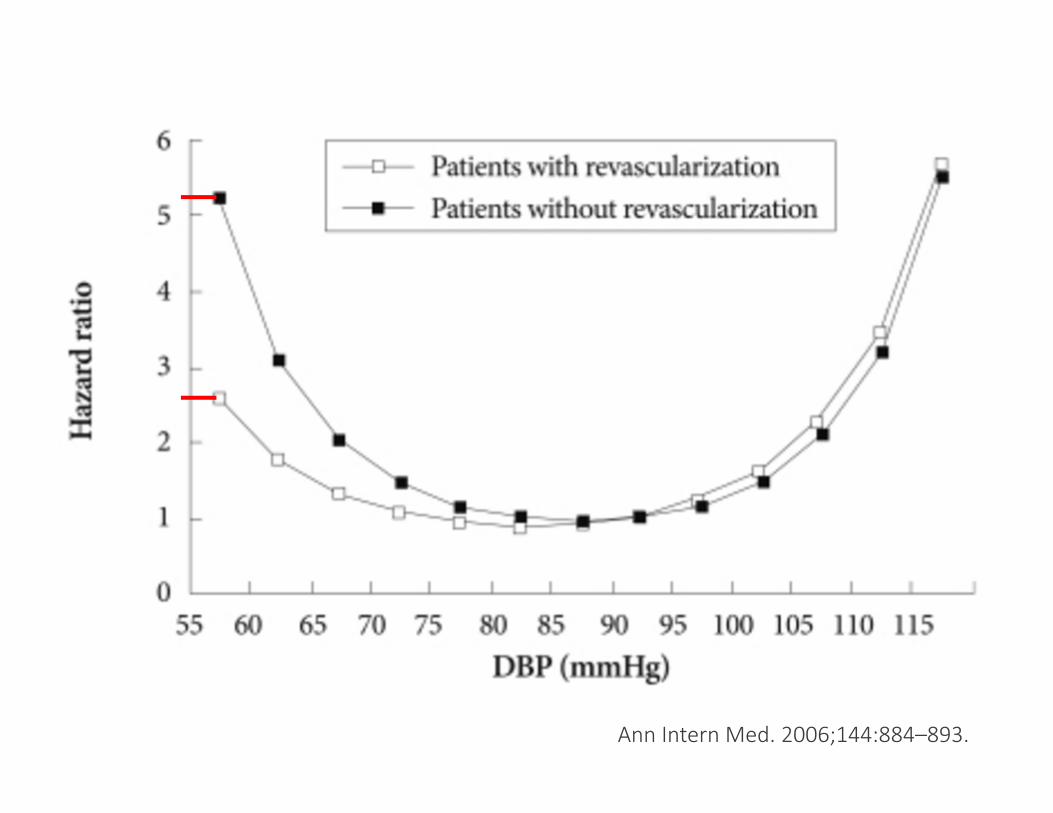
INVEST International Verapamil SR‐Trandolapril studyMI and Stroke based on Diastolic Blood Pressure Achieved
Ann Intern Med. 2006;144:884–893.DBP
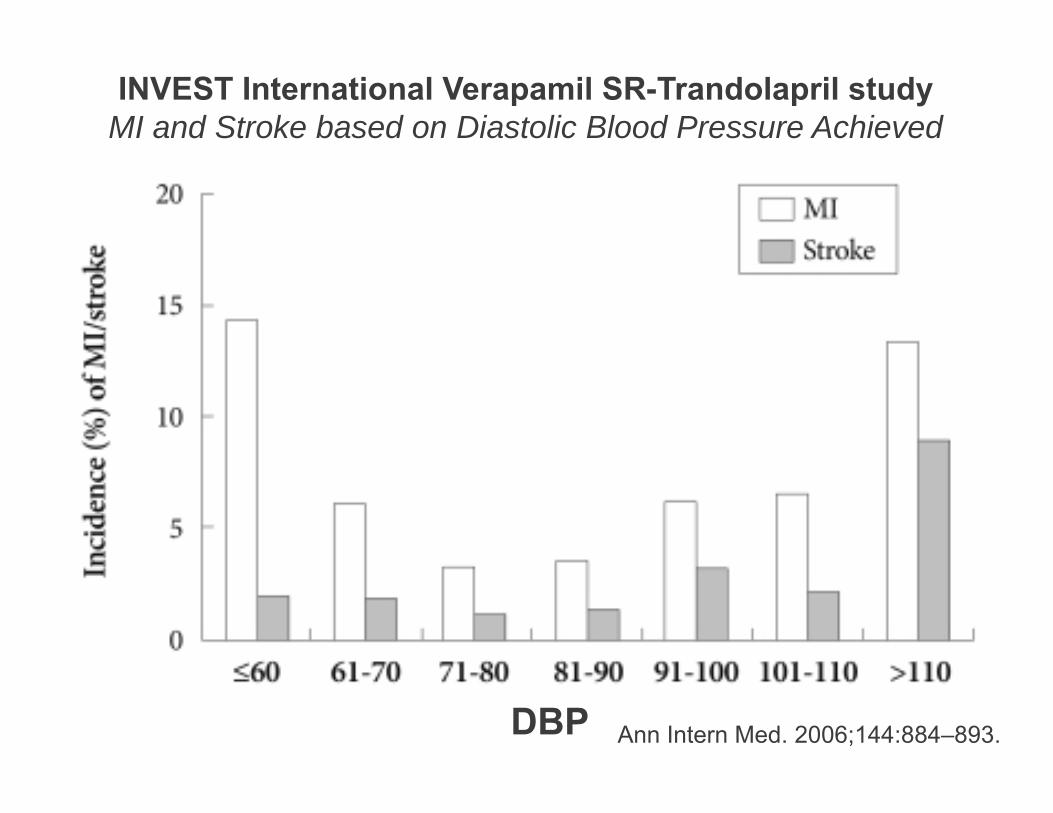
INVEST International Verapamil SR-Trandolapril studyMI and Stroke based on Diastolic Blood Pressure Achieved
Ann Intern Med. 2006;144:884–893.DBP

Baumüller S et al. Radiology 2009;253:56-64
©2009 by Radiological Society of North America
Ann Intern Med. 2006;144:884–893.
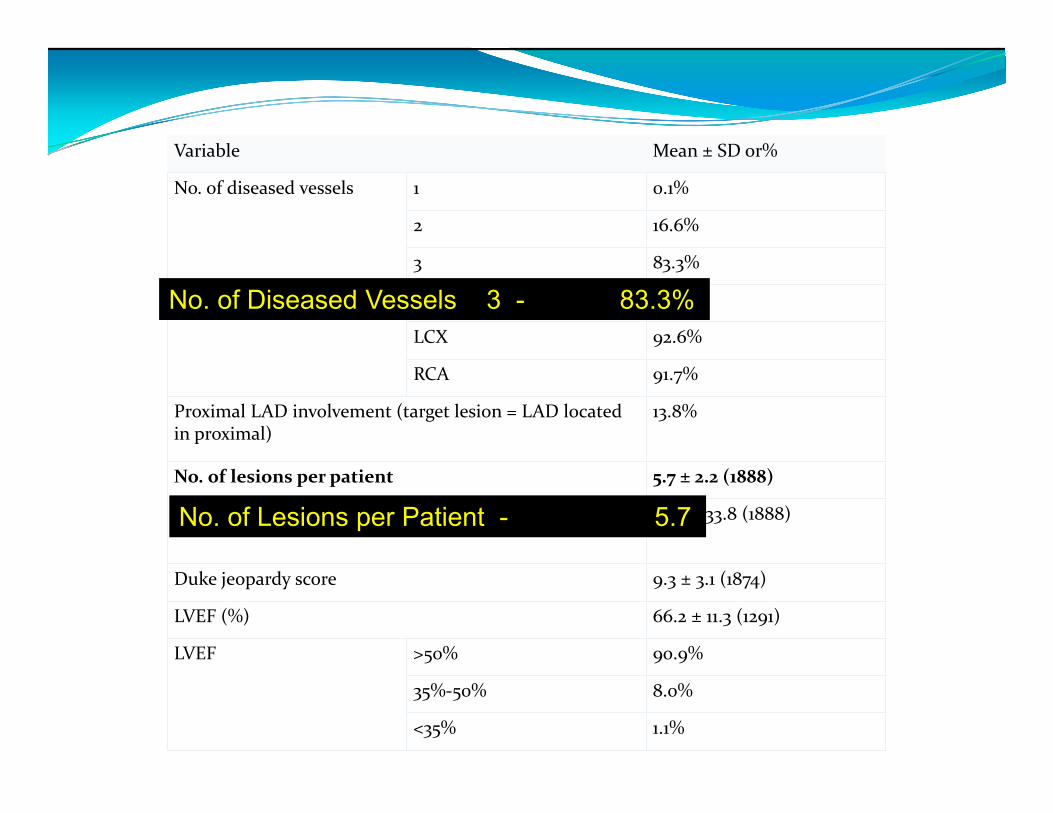
Variable Mean ± SD or%
No. of diseased vessels 1 0.1%
2 16.6%
3 83.3%
Location of disease LAD 98.9%
LCX 92.6%
RCA 91.7%
Proximal LAD involvement (target lesion = LAD located in proximal)
13.8%
No. of lesions per patient 5.7 ± 2.2 (1888)
Extent of disease per patient (total length of lesions, mm) 77.6 ± 33.8 (1888)
Duke jeopardy score 9.3 ± 3.1 (1874)
LVEF (%) 66.2 ± 11.3 (1291)
LVEF >50% 90.9%
35%‐50% 8.0%
<35% 1.1%
No. of Diseased Vessels 3 - 83.3%
No. of Lesions per Patient - 5.7
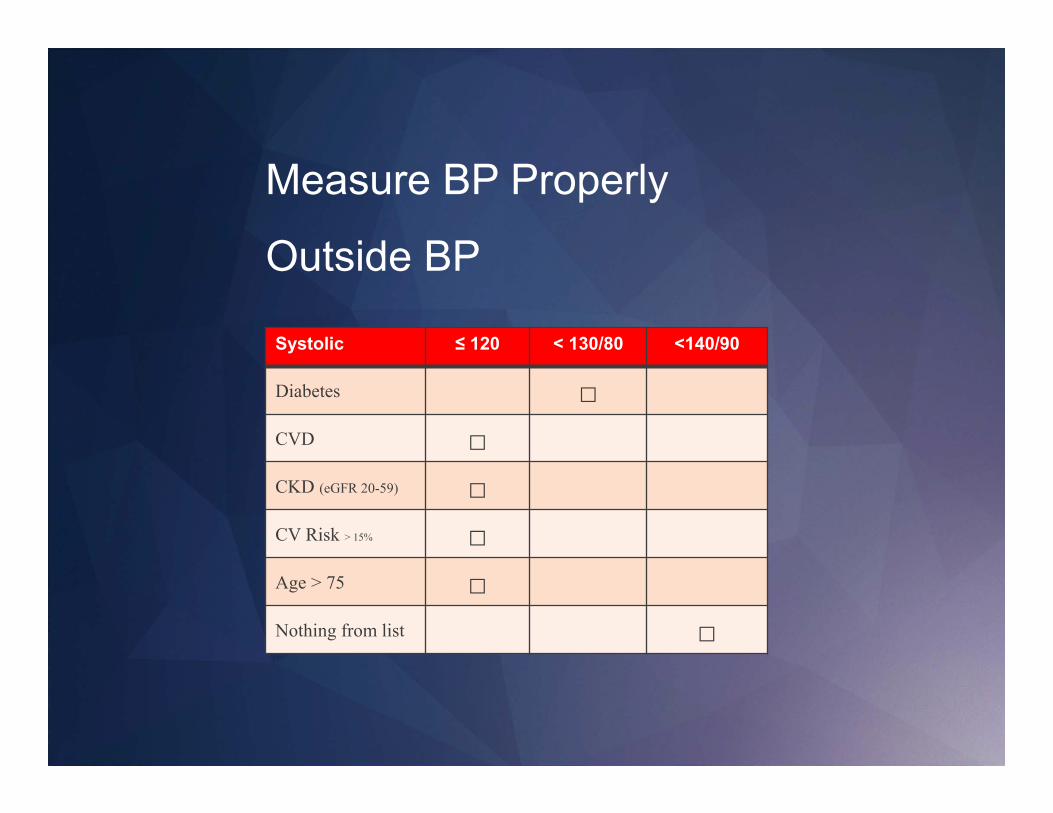
Systolic ≤ 120 < 130/80 <140/90
Diabetes □CVD □CKD (eGFR 20-59) □CV Risk > 15% □Age > 75 □Nothing from list □
Measure BP Properly
Outside BP

0
20
40
60
80
100
0
0.4
0.8
1.2
1.6
2
ALLHAT Number of Pills Needed
6 mos 1 yr 3 yr 5 yr
1 Drug 2 Drugs 3 Drugs
Pat
ien
ts (
%)
Cushman WC, et al. J Clin Hypertens. 2002;4:393-405. www.hypertensiononline.org
Averag
e # of d
rug
s
Blood pressure controlled <140/90 mmHg
49.8% 55.2% 62.3% 65.6%
1.4
1.7
2.0
1.3

Single Pill Combo and adherence
1. Sherrill B, et al. J Clin Hypertens. 2011;13(12):898‐909.
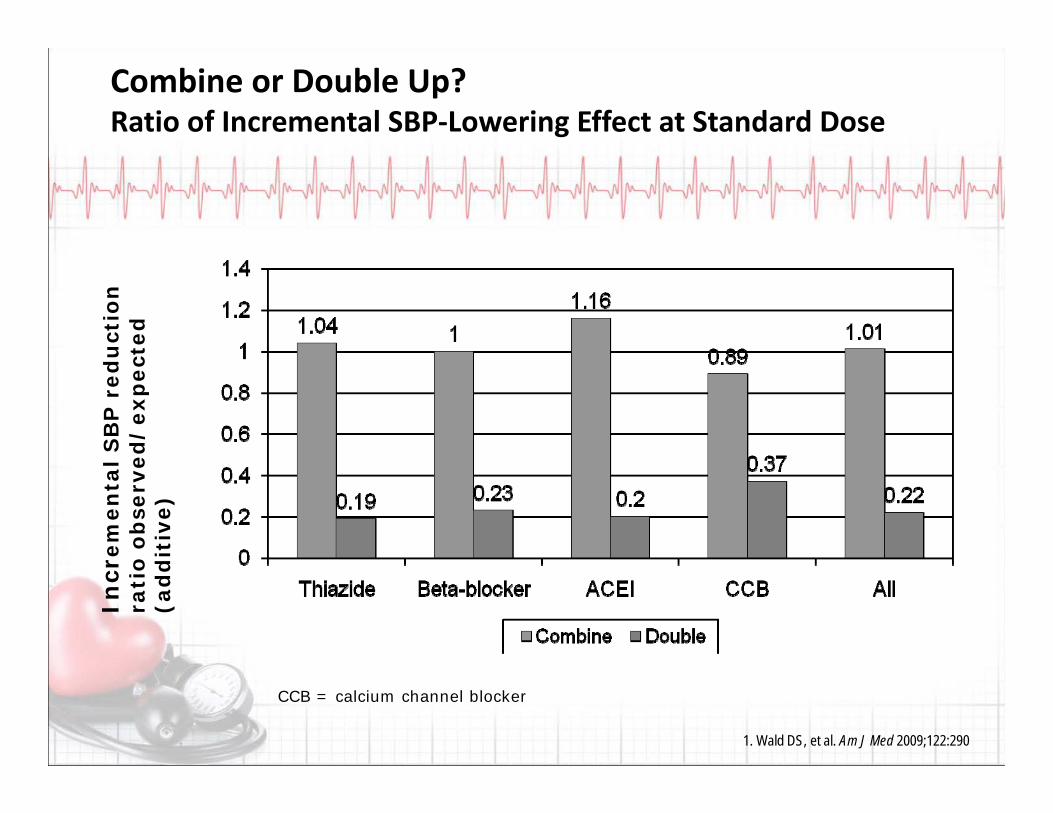
Combine or Double Up?Ratio of Incremental SBP‐Lowering Effect at Standard Dose
Incr
emen
tal
SB
P r
edu
ctio
n
rati
o ob
serv
ed/
exp
ecte
d
(ad
dit
ive)
1. Wald DS, et al. Am J Med 2009;122:290
CCB = calcium channel blocker

CV risk ‐ Initial combination therapy
1. Corrao G, et al. Hypertension. 2011;58(4):566‐572.
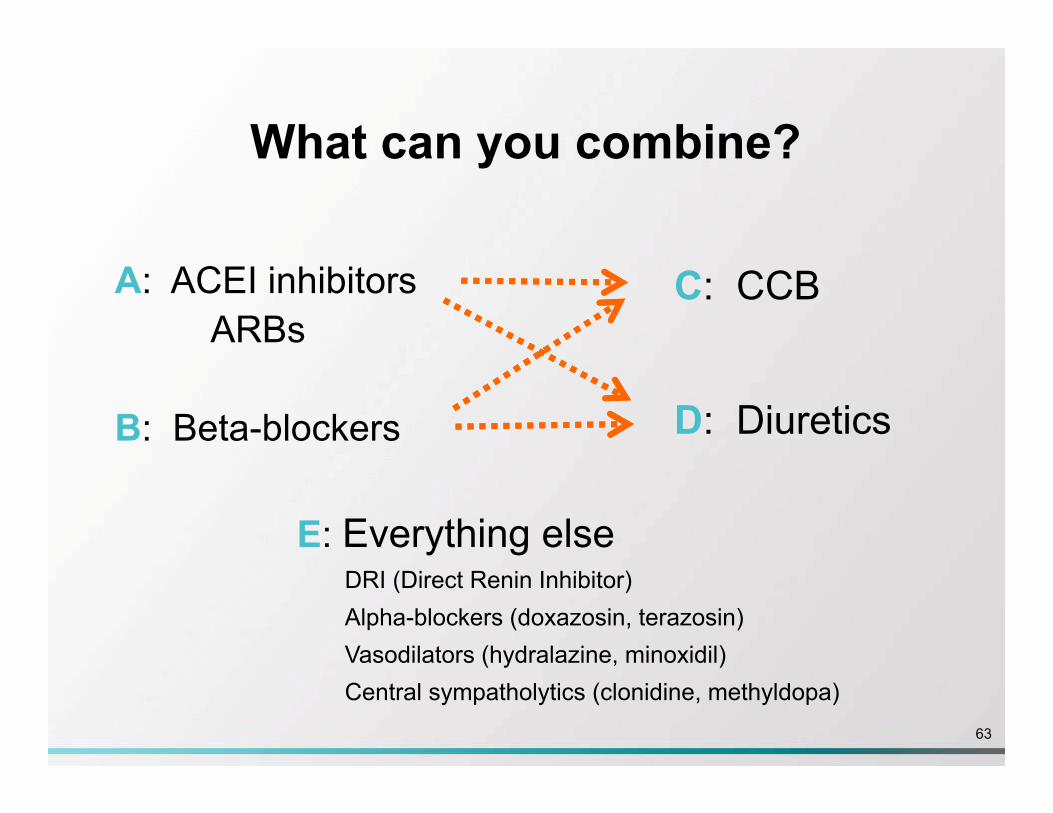
What can you combine?
A: ACEI inhibitorsARBs
B: Beta-blockers
C: CCB
D: Diuretics
E: Everything elseDRI (Direct Renin Inhibitor)Alpha-blockers (doxazosin, terazosin)Vasodilators (hydralazine, minoxidil)Central sympatholytics (clonidine, methyldopa)
63
64
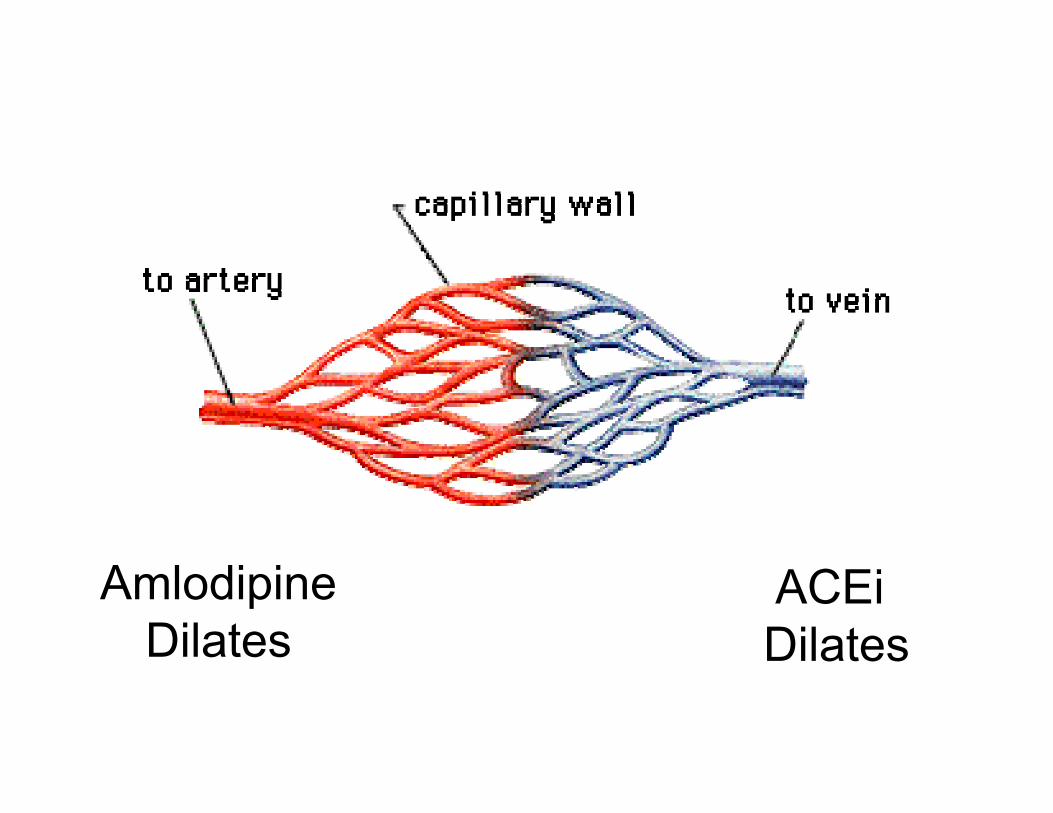
AmlodipineDilates
ACEi Dilates

AmlodipineDilates
ACEiDilates

STITCH algorithm
1. Feldman RD, et al. Hypertension. 2009;53(4):646-653.

STITCH study: Results
1. Feldman RD, et al. Hypertension. 2009;53(4):646-653.
Absolute difference: 12.0% 95% CI 1.5-22.4%P = 0.026
68

Thiazide/thiazide‐like* ACEI§ Long‐acting
CCB
TARGET <135/85 mmHg (automated measurement method)
ARB § Beta‐blocker†
First Line Treatment of Adults with Systolic/DiastolicHypertension Without Other Compelling Indications
Health behaviour management
Single pill combination**
† BBs are not indicated as first line therapy for age 60 and above§Renin angiotensin system (RAS) inhibitors are contraindicated in pregnancy and
caution is required in prescribing to women of child bearing potential
* Longer‐acting (thiazide‐like) diuretics are preferred over shorter‐acting (thiazide) diuretics
INITIAL TREATMENT
**Recommended SPC choices are those in which an ACE‐I is combined with a CCB,an ARB with a CCB, or an ACE‐I or ARB with a diuretic