hypertension: specific aspects in women najat joubran fares m.d st george hospital university of...
TRANSCRIPT
Hypertension: Specific Aspects in women
Najat Joubran Fares M.DSt George Hospital
University of Balamand

Prevalence of high blood pressure by age and race/ethnicity for men and women, US population 18 years of age and older. *Estimate based on sample size not meeting minimum requirements of the National Health and Nutrition Examination Survey III design or relative SEM greater than
30%.
Vicki L. Burt et al. Hypertension. 1995;25:305-313
Copyright © American Heart Association, Inc. All rights reserved.

Physiological Effects of Sex Hormones on Blood Pressure
Role of Testosterone:- In adolescence and puberty, blood pressure is higher in boys than in
girls (Androgen level is increasing)- The blood pressure in postpubescent boys does not dip as low at
night as in girls.- Women with polycystic ovary syndrome or adrenal virilizing tumors,
which are characterized by elevated testosterone levels, experience hypertension.
Hypertension 2001; 37: 1199-1208 Recklhoff et al

Androgen receptor antagonism in intact male SHR reduced mean arterial blood pressure at 14 to 16 weeks of age to the same level as found in castrated males and intact female SHR of similar
ages.
Jane F. Reckelhoff Hypertension. 2001;37:1199-1208
Copyright © American Heart Association, Inc. All rights reserved.

Effect of Androgen on Blood pressure• Plasma renin activity (PRA) is positively modulated by androgens,
maybe by increasing pro angiotensinogen level• Prorenin and PRA levels are greater in men than in women.• James et al reported that PRA was 27% higher in men than in women
in all age groups.• Reckelhoff et al demonstrated that Enalapril decreased BP by 65% in
male SHRs which was greater than in female rats (40%)

Beelen et al japplphysiol.00548.2001

Physiological Effects of Sex Hormones on Blood Pressure
Role of Estrogen• It has been reported that AT2R (Angiotensine Receptor type 2)
expression is higher in female than male rats (Sampson et al Hypertension 2008; 52: 666-71)
• Estrogen Deficit: low AT2R mRNA level in vascular smooth muscle cells
• Stimulation of AT1R will lead to Na absorption and Hypertension• Stimulation of AT2R will lead to natriuresis: Antihypertensive effect

Figure 1. The effect of chronic Ang II infusion on MAP in male and female rats.
Amanda K. Sampson et al. Hypertension. 2008;52:666-671
Copyright © American Heart Association, Inc. All rights reserved.
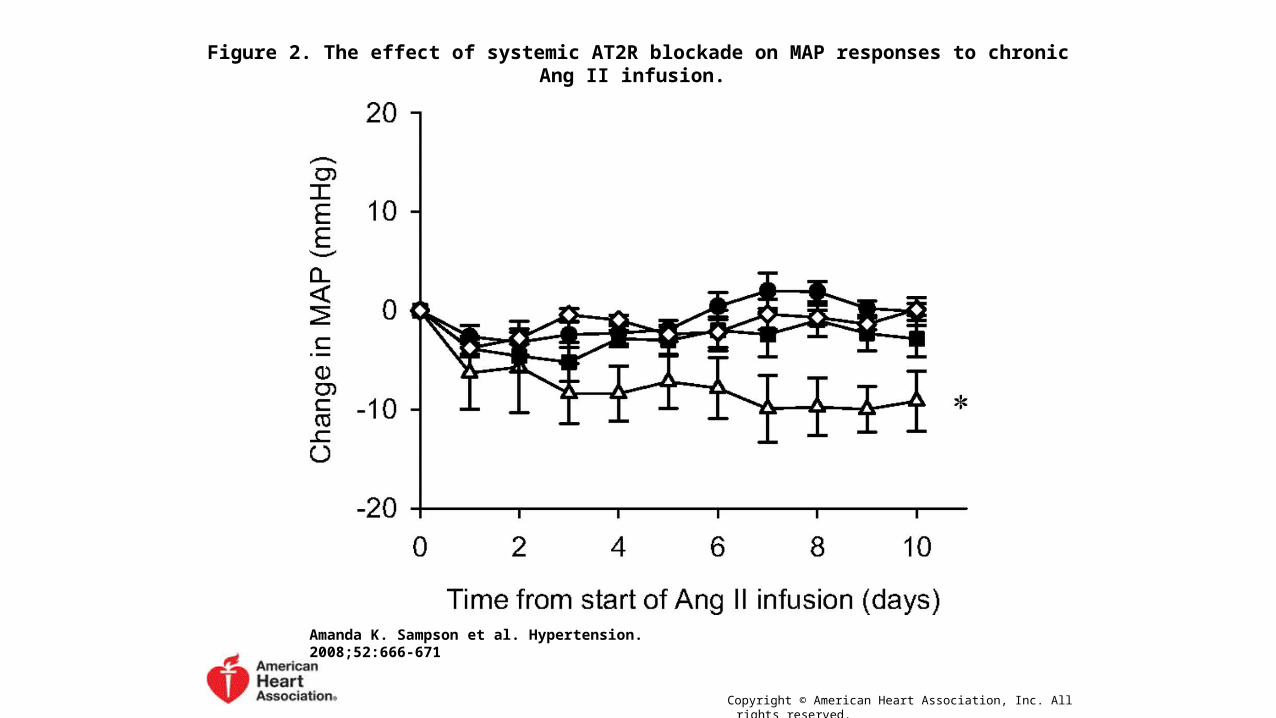
Figure 2. The effect of systemic AT2R blockade on MAP responses to chronic Ang II infusion.
Amanda K. Sampson et al. Hypertension. 2008;52:666-671
Copyright © American Heart Association, Inc. All rights reserved.

Physiological Effects of Sex Hormones on Blood Pressure
Role of Estrogen• The estradiol metabolites 2-hydroxyestradiol and 2-methoxyestradiol
inhibit endothelin-1 synthesis, this will lower PRA• Increase in NO synthesis which will decrease renin secretion• Decrease the effect of Angiotensin II on Aldosterone secretion:
Angiotensin II increases peak plasma aldosterone levels in dependence of the estrogen status with highest levels observed in male or ovariectomised rats
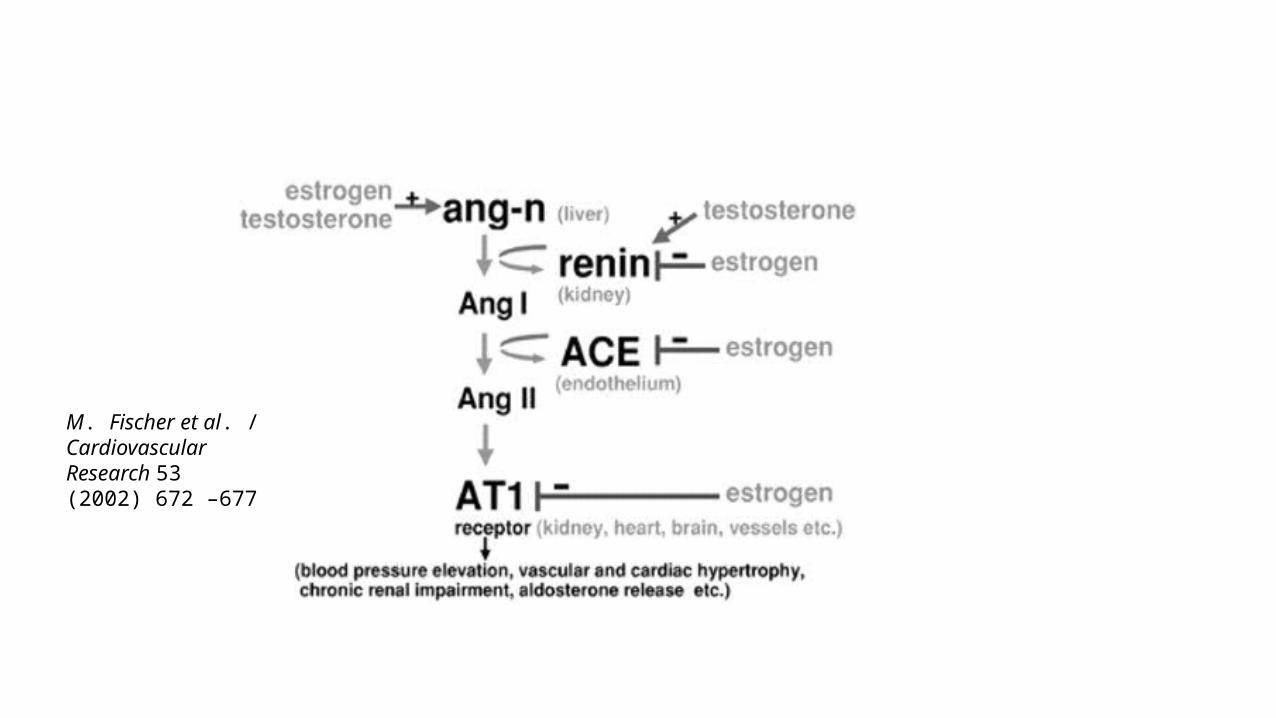
M. Fischer et al. / Cardiovascular Research 53 (2002) 672 –677

Menopause and Hypertension
• HTN is less prevalent in premenopausal women than men, the prevalence increases after menopause to become similar or even more important than that of men

Mean systolic and diastolic blood pressures by age and race/ethnicity for men and women, US population 18 years of age and older.
Vicki L. Burt et al. Hypertension. 1995;25:305-313
Copyright © American Heart Association, Inc. All rights reserved.

Menopause and Salt Sensitivity
• Loss of female hormones and increase in Androgen after Menopause will shift the curve of salt excretion to the Right, so this will increase salt sensitivity and predispose to HTN


Menopause and Salt Sensitivity
• The percentage of uncontrolled hypertension seems to be more in women ( 50.8±2.1% in men and 55.9±1.5% in women) (J Women’s Health 2006; 15:734–746)
• Nondipping is associated with greater end organ damage in female than male (Can J Cardiol. 2009; 25:e157–e163)

Menopause and Salt Sensitivity: Pathophysiology• Activation of RAS, by the effect of Androgen on liver pro
angiotensinogen synthesis• Increase in Endothelin synthesis, and possible increase in ETA
receptors By the loss of Estrogen• Increased Number of AT1 Receptors due to loss of Estrogen• Decreased NO production due to loss of Estrogen• Beyond Hormonal Effect: Menopause is associated with weight gain,
the associated increase in plasma leptin levels has been shown to cause sympathetic activation. Increased Insulin and Insuline Resistance, and Volume Retention
Hormonal Replacement Therapy in Post Menopausal Women
• Conjugated Estrogen with Medroxyprogesterone, or conjugated estrogen alone in hysterectomized patients, Mainly used and effective on hot flushes
• Many studies showed negligible effect of estrogen alone or in combination with progesterone on arterial blood pressure in non hypertensive postmenopausal women (HERS, WHI, PEPI trials). Possible effect on lowering nocturnal blood pressure
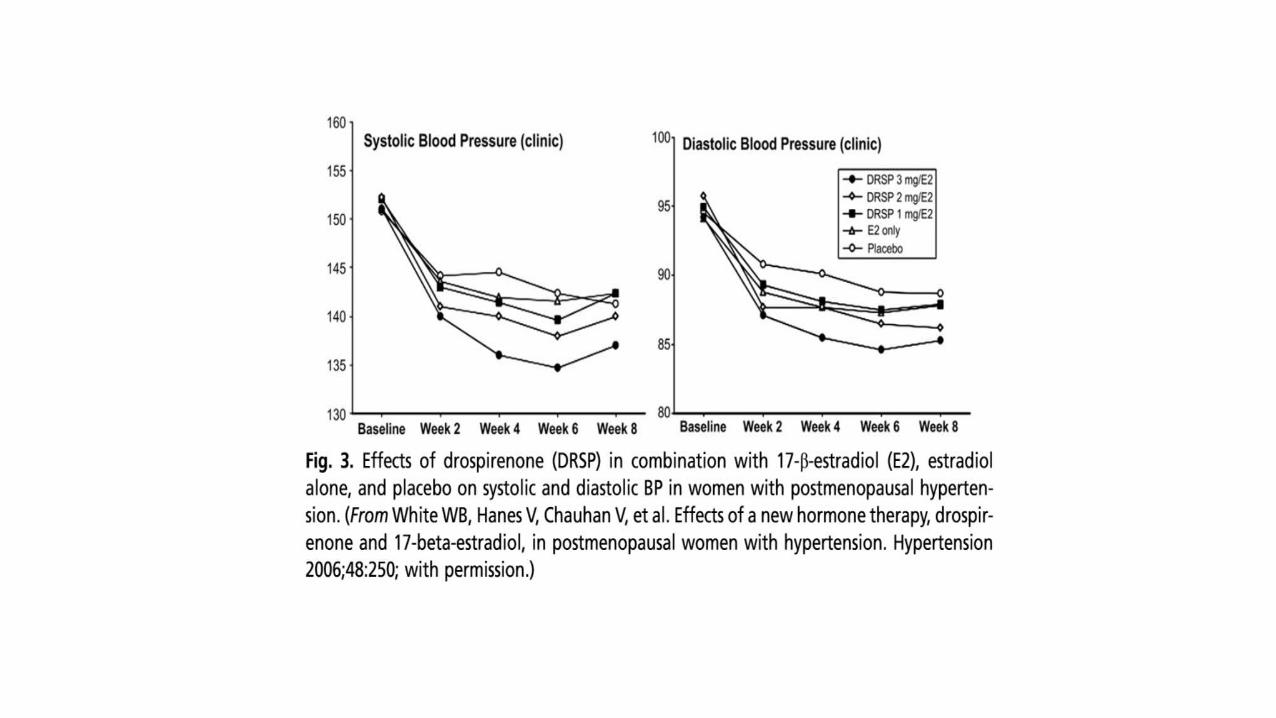
• Estrogen may have beneficial effect on blood pressure in hypertensive postmenopausal patients

Int J women Health 2014;6: 747

Int J Women Health 2014;6: 747

Hypertension. 2009;54:11-18.

Hormonal Replacement Therapy in Post Menopausal Women
• The introduction of the new progestin, the drospirenone, that will antagonize the effect of Estrogen showed safety in hypertensive postmenopausal women.

Postmenopausal Hypertension: Treatment• Because of increased salt sensitivity, diuretics have a specific role in
hypertension treatment in postmenopausal patients• Selective ER modulators, eg, raloxifene, which are agonists for the
novel vasodilating estrogen receptor GPER32 could possibly be used in the treatment of postmenopausal hypertension
Oral Contraceptives: Effect on Blood Pressure
• Oral Contraception is the most common contraceptive modality used.• The association between oral contraceptive use and hypertension was
first reported by Laragh and colleagues in 1967 (JAMA. 1967; 201(12):918-922)
• Hypertension is 2-3 times more common in women taking oral contraceptives than in age-matched women not taking these medications (Contraception. 1989;40(2):147-156.)
• It may induce mild increase in Blood pressure in the general population, however it may cause significant increase in BP in 5% of female subjects
• The Effect on BP is dependent on the type, the dose of Estrogen, the duration of treatment, the body mass and the age. (Advances in Chronic Kidney Disease, Vol 20, No 5 (September), 2013: pp 396-401396)
Types of Oral Contraceptive Agents
• Classified in Generations according to the date of introduction in the Market and the dose of Estrogen and type of progestin used
• 4 Generations• Third and 4th Generations: 20-35 Micg of ethynil estradiol or other
form of estrogen vs 150 in the first generation• Third and 4th Generations: Progestin with less andogenic and fewer
metabolic effect than first and second generations• Drospirenone: Fourth generation progestin with spirinolactone like
effect.

Oral Contraceptives: Effect on Blood Pressure
• Combined oral contraceptive preparations containing Ethinyl-Estradiol (EE) may increase blood pressure by 15 mmHg
• The effect is due to stimulation of liver synthesis of protein/ Angiotensinogen I, and secondary increase in Aldosterone
• Progestin will increase Na retention• New agents containing Estradiol instead of EE, showed neutral effect
on BP, and this because of less effect on liver protein synthesis• New combinations with drospirenone, a synthetic progestin,
structurally similar to spironolactone, has an anti mineralocorticoid effect and will counteract the hypertensive effect of EE
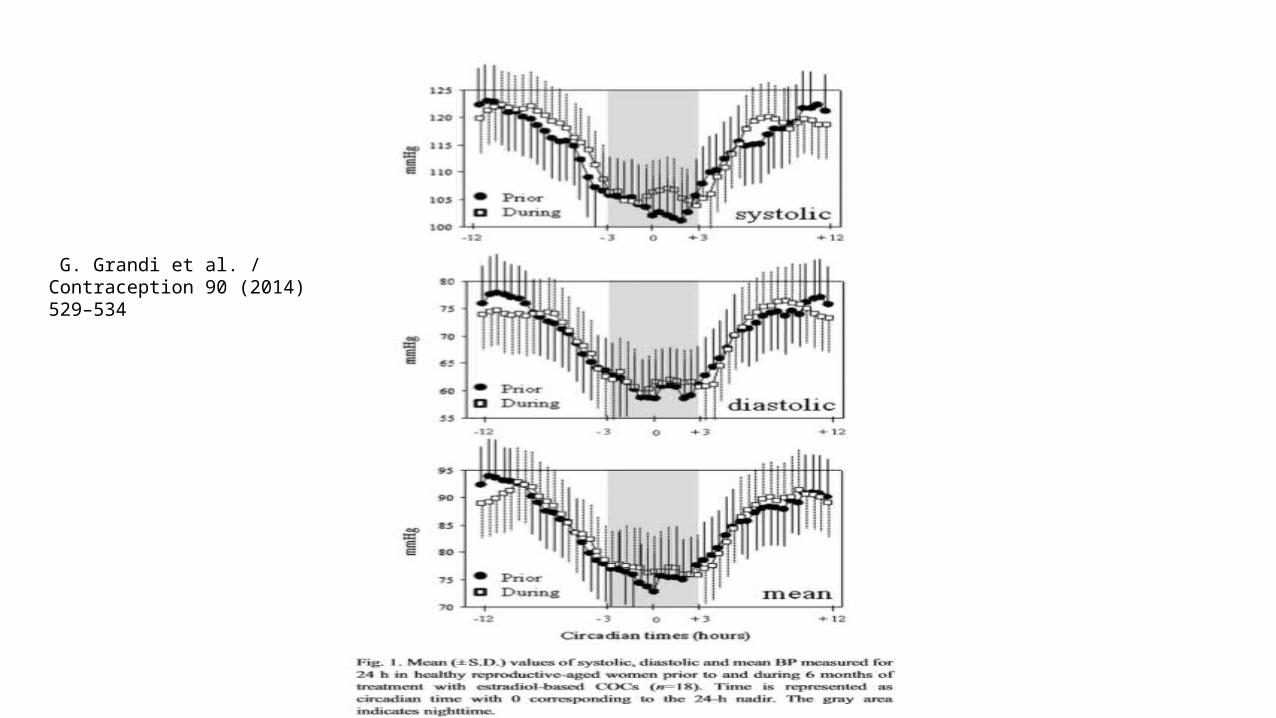
G. Grandi et al. / Contraception 90 (2014) 529–534

Effect of Oral contraceptive formulation with Drospirenone
Boldo et al, Endocrinol Metab Clin N Am 40 (2011) 419–432
Summary
• The prevalence of hypertension in low in premenopausal women, it will increase post menopause, due in part to the effect of sexe hormones on regulation of blood pressure
• Hormone replacement therapy has no major effect on blood pressure of Normotensive Postmenopausal Women, and may decrease blood pressure in Hypertensive Postmenopausal patients
• Oral contraception is associated with increased risk of hypertension• The effect of contraception depends on the type of estrogen and
progestin used. • Prospirenone, a new generation progestin has an antihypertensive effect.

THANK YOU!