hypnotics opa march 3, 2007 jonathan emens, m.d. sleep medicine clinic sleep and mood disorders...
TRANSCRIPT

Hypnotics
OPAMarch 3, 2007
Jonathan Emens, M.D.Sleep Medicine Clinic
Sleep and Mood Disorders LaboratoryOregon Health & Science University Portland, OR

Disclosure
None of my slides, abstracts and/or handouts contain any advertising, trade names or product–group messages. Any treatment recommendations I make will be based on best clinical evidence or guidelines.

Outline
• Review of Sleep Physiology• Epidemiology of Insomnia• Morbidity in Insomnia• Diagnoses in Insomnia• Hypnotics

Brief review of Sleep
• Reversible, unresponsive state

Brief review of Sleep
• Reversible, unresponsive state• Divided into two states: NREM and REM
Brief review of Sleep
• Reversible, unresponsive state• Divided into two states: NREM and REM• NREM: Divided into 4 stages based on
EEG patterns

EEG in NREM Sleep
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

EEG in NREM Sleep
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000

EEG in NREM Sleep
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

EEG in NREM Sleep
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

Brief review of Sleep
• Reversible, unresponsive state• Divided into two states: NREM and REM• NREM: Divided into 4 stages based on EEG
patterns• REM: distinct EEG, muscle atonia, rapid
eye movements, dreams, PGO waves (measured in animals)

EEG, EOG, and EMG in REM Sleep

Sleep Staging
• Stage 1: 2-5%
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000

Sleep Staging
• Stage 1: 2-5%
• Stage 2: 45-55%
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000

Sleep Staging
• Stage 1: 2-5%
• Stage 2: 45-55%
• Stage 3: 3-8%
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000

Sleep Staging
• Stage 1: 2-5%
• Stage 2: 45-55%
• Stage 3: 3-8%
• Stage 4: 10-15%
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000

Sleep Staging
• Stage 1: 2-5%
• Stage 2: 45-55%
• Stage 3: 3-8%
• Stage 4: 10-15%
• REM: 20-25%
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000

REM and NREM patterns
• First third of the night mostly NREM, especially stage 3 and 4 (slow wave) sleep

REM and NREM patterns
• First third of the night mostly NREM, especially stage 3 and 4 (slow wave sleep)
• Last third of the night mostly REM sleep

REM and NREM patterns
• First third of the night mostly NREM, especially stage 3 and 4 (slow wave sleep
• Last third of the night mostly REM sleep
• Cycles of NREM and REM sleep occur every 90-110 minutes

REM and NREM patterns
• First third of the night mostly NREM, especially stage 3 and 4 (slow wave sleep)
• Last third of the night mostly REM sleep• Cycles of NREM and REM sleep occur
every 90-110 minutes• Amount of slow wave sleep (SWS)
decreases with age (greater decreases in men)

Changes in Sleep with Age
Ohayon M, et al. Sleep. 2004;27:1255-1273.

Memory impairment surrounding sleep onset
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000

Insomnia Definitions
• “difficulty in initiating and/or maintaining sleep.” – International Classification of Sleep Disorders (ICSD)
• Difficulty Falling Asleep• Difficulty maintaining sleep• Early morning awakening• Daytime fatigue, poor concentration, and
irritability

Epidemiology of Insomnia
• Depends on Definition: 4.4-48% prevalence in general population
Ohayon M, Sleep Med Rev. 2002;6: 97-111.

Epidemiology of Insomnia
• Depends on Definition: 4.4-48% prevalence in general population
• Insomnia Symptoms: 30-48%
Ohayon M, Sleep Med Rev. 2002;6: 97-111.

Epidemiology of Insomnia
• Depends on Definition: 4.4-48% prevalence in general population
• Insomnia Symptoms: 30-48%• Insomnia Symptoms > 3 times/week or “often” or
“always”: 16-21%
Ohayon M, Sleep Med Rev. 2002;6: 97-111.

Epidemiology of Insomnia
• Depends on Definition: 4.4-48% prevalence in general population
• Insomnia Symptoms: 30-48%• Insomnia Symptoms > 3 times/week or “often” or
“always”: 16-21%• Insomnia Symptoms that are “moderate” or “severe”:
10-28%
Ohayon M, Sleep Med Rev. 2002;6: 97-111.

Epidemiology of Insomnia
• Depends on Definition: 4.4-48% prevalence in general population
• Insomnia Symptoms: 30-48%• Insomnia Symptoms > 3 times/week or “often” or
“always”: 16-21%• Insomnia Symptoms that are “moderate” or “severe”:
10-28%• Insomnia Symptoms with Daytime sequelae: 9-15%
Ohayon M, Sleep Med Rev. 2002;6: 97-111.

Epidemiology of Insomnia
• Depends on Definition: 4.4-48% prevalence in general population
• Insomnia Symptoms: 30-48%• Insomnia Symptoms > 3 times/week or “often” or
“always”: 16-21%• Insomnia Symptoms that are “moderate” or “severe”:
10-28%• Insomnia Symptoms with Daytime sequelae: 9-15%• Dissatisfaction with amount or quality of sleep: 8-18%
Ohayon M, Sleep Med Rev. 2002;6: 97-111.

Epidemiology of Insomnia
• Depends on Definition: 4.4- 48% prevalence in general population
• Insomnia Symptoms: 30-48%• Insomnia Symptoms > 3 times/week or “often” or
“always”: 16-21%• Insomnia Symptoms that are “moderate” or “severe”:
10-28%• Insomnia Symptoms with Daytime sequelae: 9-15%• Dissatisfaction with amount or quality of sleep: 8-18%• Insomnia Diagnosis (DSM-IV): 4.4-11.7% (many with
symptoms don’t meet DSM criteria)
Ohayon M, Sleep Med Rev. 2002;6: 97-111.

Epidemiology of Insomnia
• 5,622 subjects
Ohayon M, J Psychiatr Res. 1997;31:333-346.

Epidemiology of Insomnia
• 5,622 subjects• 18.7% had complaints of difficulty initiating or
maintaining sleep or of non-restorative sleep
Ohayon M, J Psychiatr Res. 1997;31:333-346.

Epidemiology of Insomnia
• 5,622 subjects• 18.7% had complaints of difficulty initiating or
maintaining sleep or of non-restorative sleep• 12.7% had sleep complaints for > 1 month that
caused “clinically significant distress or impairment”
Ohayon M, J Psychiatr Res. 1997;31:333-346.

Epidemiology of Insomnia
• 5,622 subjects• 18.7% had complaints of difficulty initiating or
maintaining sleep or of non-restorative sleep• 12.7% had sleep complaints for > 1 month that
caused “clinically significant distress or impairment”• 10.3% with Axis I or II disorder
Ohayon M, J Psychiatr Res. 1997;31:333-346.

Epidemiology of Insomnia
• 5,622 subjects• 18.7% had complaints of difficulty initiating or
maintaining sleep or of non-restorative sleep• 12.7% had sleep complaints for > 1 month that
caused “clinically significant distress or impairment”• 10.3% with Axis I or II disorder• 1.3% primary insomnia
Ohayon M, J Psychiatr Res. 1997;31:333-346.

Epidemiology of Insomnia
• 5,622 subjects• 18.7% had complaints of difficulty initiating or
maintaining sleep or of non-restorative sleep• 12.7% had sleep complaints for > 1 month that
caused “clinically significant distress or impairment”• 10.3% with Axis I or II disorder• 1.3% primary insomnia• 0.5% general medical condition
Ohayon M, J Psychiatr Res. 1997;31:333-346.

Epidemiology of Insomnia
• 5,622 subjects• 18.7% had complaints of difficulty initiating or
maintaining sleep or of non-restorative sleep• 12.7% had sleep complaints for > 1 month that
caused “clinically significant distress or impairment”• 10.3% with Axis I or II disorder• 1.3% primary insomnia• 0.5% general medical condition• 0.3% circadian disorder
Ohayon M, J Psychiatr Res. 1997;31:333-346.

Morbidity/Co-Morbidity• Objective cognitive/performance deficits?
Ford DE and Kamerow DB, JAMA. 1989;262:1479-1484.Mellinger GD et al., Arch Gen Psych. 1985;42:225-232.Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

Morbidity/Co-Morbidity• Objective cognitive/performance deficits?• Quality of life: subjective deficits in memory,
concentration, & work performance
Ford DE and Kamerow DB, JAMA. 1989;262:1479-1484.Mellinger GD et al., Arch Gen Psych. 1985;42:225-232.Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

Morbidity/Co-Morbidity• Objective cognitive/performance deficits?• Quality of life: subjective deficits in memory,
concentration, & work performance• Psychiatric: prevalence of any psychiatric
disorder is 2-3x greater in insomniacs, depression prevalence is 4x greater
Ford DE and Kamerow DB, JAMA. 1989;262:1479-1484.Mellinger GD et al., Arch Gen Psych. 1985;42:225-232.Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

Morbidity/Co-Morbidity• Objective cognitive/performance deficits?• Quality of life: subjective deficits in memory,
concentration, & work performance• Psychiatric: prevalence of any psychiatric
disorder is 2-3x greater in insomniacs, depression prevalence is 4x greater
• Medical: insomnia associated with multiple medical conditions; increased HD risk & impaired immune function? Increased mortality rates? –confounding factors.
Ford DE and Kamerow DB, JAMA. 1989;262:1479-1484.Mellinger GD et al., Arch Gen Psych. 1985;42:225-232.Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

Morbidity/Co-Morbidity
Chang PP, Am J Epidemiol. 1997;146:105-114.

Morbidity/Co-Morbidity
Weissman MM, Gen Hosp Psych. 1997;19:245-250.

Differential Diagnosis
• Psychiatric• Medical• Neurological• Environmental• Circadian Rhythm Disorder• Primary Sleep Disorder: sleep apnea, PLMs & restless legs
syndrome, & parasomnias• “Behavioral”: inadequate sleep hygiene • Stress related transient Insomnia • “Primary Insomnias”: psychophysiological insomnia, sleep state
misperception, & idiopathic insomnia (no primary insomnia in ICSD vs. DSM)
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000

Treatment
• Treat underlying Medical Condition• Treat underlying Psychiatric Condition • Improve sleep Hygiene• Change environment• CBT: “primary insomnias”, transient insomnia• Pharmacological• Light, melatonin, or “chronotherapy” for
Circadian disorders

Treatment
• Treat underlying Medical Condition• Treat underlying Psychiatric Condition • Improve sleep Hygiene• Change environment• CBT: “primary insomnias”, transient insomnia• Pharmacological• Light, melatonin, or “chronotherapy” for
Circadian disorders

“Hypnotics”
• Benzodiazepine Receptor Agonists (BzRAs)– Benzodiazepines– Non-Benzodiazepines GABAA agonists
• Sedating Antidepressants• Sedating Antipsychotics • Antihistamines• Gamma-Hydroxybutyrate (GHB)• Melatonin and Melatonin agonists,
Gabapentin, Valerian

BzRAs
• Benzodiazepines, zaleplon, zolpidem, zopiclone, & eszopiclone
• All act on gamma-aminobutyric acidA (GABAA) benzodiazepine receptor complex
• Preoptic area of anterior hypothalamus?
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005
GABAA benzodiazepine receptor complex
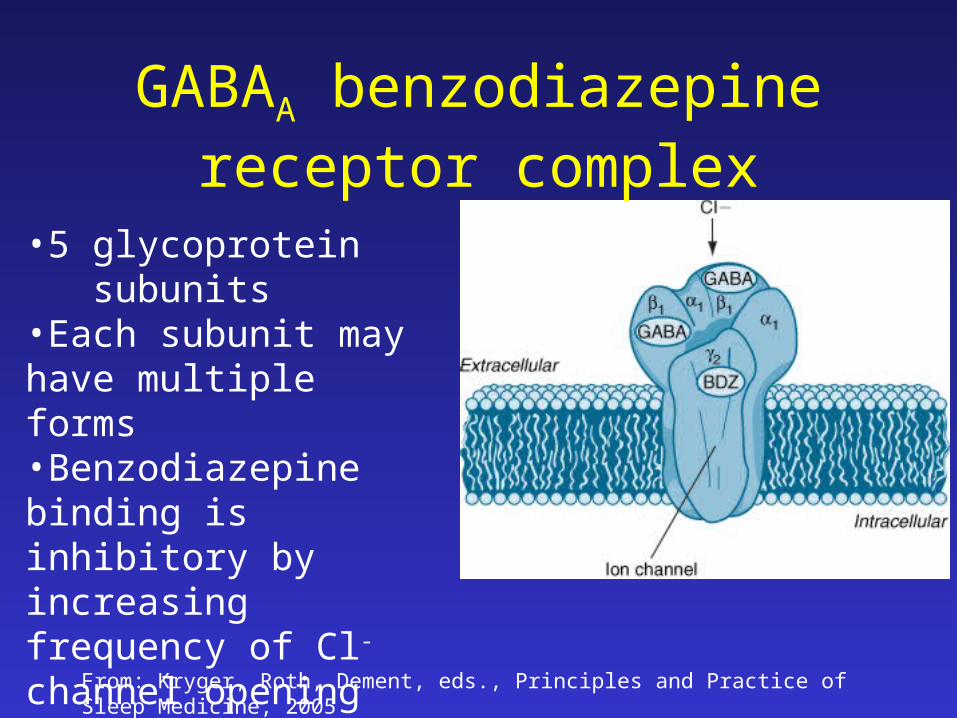
•5 glycoprotein subunits•Each subunit may have multiple forms•Benzodiazepine binding is inhibitory by increasing frequency of Cl- channel opening

From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005
GABAA benzodiazepine receptor complex
•Two common types of GABAA receptors: - Type I (1, 2, 2), 40%
- Type II (3, 2,2), 20%
•Newer non-benzo. hypnotics preferentially bind to Type I receptors

Hypnotic Drugs*Half-life (hr) Onset of Action (min)† Pharmacologically Active Metabolites Dose (mg)
Benzodiazepine hypnotics
Quazepam 48-120 30 N-desalkyl (flurazepam) 7.5-15
Flurazepam 48-120 15-45 N-desalkyl (flurazepam) 15-30
Triazolam 2-6 2-30 None 0.125-0.25
Estazolam 8-24 Intermediate None 1-2
Temazepam 8-20 45-50 None 15-30
Loprazolam 4.6-11.4 - None 1-2
Flunitrazepam 10.7-20.3 Short N-desmethyl (flunitrazepam) 0.5-1
Lormetazepam 7.9-11.4 - None 1-2
Nitrazepam 25-35 Intermediate None 5-10
Nonbenzodiazepine hypnotics
Eszopiclone 5-7 Intermediate None 2-3 adult, 1 elderly
Zolpidem 1.5-2.4 Rapid None 5-10 (age >65 yr)
10-20 (age <65 yr)
Zopiclone 5-6 Intermediate None 3.75 (age >65 yr)
7.5 (age <65 yr)
Zaleplon 1 Rapid None 5-10
Nonhypnotics sometimes used to aid sleep
Clonazepam 30-40 - 4-Amino derivative 0.5-3¶
Diazepam 30-100 Rapid N-desmethyl 2-10¶
Chlordiazepoxide 24-28 Intermediate N-desmethyl (chlordiazepoxide, demoxepam, oxazepam ) 10-25¶
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005
BzRAs: Pharmacokinetics

BzRAs: Effects
• Anterograde amnesia.
Scharf MB et al., J Clin Psych. 1994;55:182-199.Walsh JK et al., Sleep Med. 2000;1:41-49.Krystal AD et al., Sleep. 2003;26:793-799.Perlis M et al., J Clin Psych. 2004;65:1128-1137.Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

BzRAs: Effects
• Anterograde amnesia. • PSG studies show decreased sleep latency and wake
after sleep onset (WASO) and increased total sleep time (not zaleplon)
Scharf MB et al., J Clin Psych. 1994;55:182-199.Walsh JK et al., Sleep Med. 2000;1:41-49.Krystal AD et al., Sleep. 2003;26:793-799.Perlis M et al., J Clin Psych. 2004;65:1128-1137.Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

BzRAs: Effects
• Anterograde amnesia. • PSG studies show decreased sleep latency and wake
after sleep onset (WASO) and increased total sleep time (not zaleplon)
• Slight decrease in REM sleep
Scharf MB et al., J Clin Psych. 1994;55:182-199.Walsh JK et al., Sleep Med. 2000;1:41-49.Krystal AD et al., Sleep. 2003;26:793-799.Perlis M et al., J Clin Psych. 2004;65:1128-1137.Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

BzRAs: Effects
• Anterograde amnesia. • PSG studies show decreased sleep latency and wake
after sleep onset (WASO) and increased total sleep time (not zaleplon)
• Slight decrease in REM sleep• Suppress slow wave sleep (not zolpidem)
Scharf MB et al., J Clin Psych. 1994;55:182-199.Walsh JK et al., Sleep Med. 2000;1:41-49.Krystal AD et al., Sleep. 2003;26:793-799.Perlis M et al., J Clin Psych. 2004;65:1128-1137.Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

BzRAs: Effects
• Anterograde amnesia. • PSG studies show decreased sleep latency and wake
after sleep onset (WASO) and increased total sleep time (not zaleplon)
• Slight decrease in REM sleep• Suppress slow wave sleep (not zolpidem)• Tolerance? Studies:
– zolpidem and zaleplon nightly for 5 weeks– eszopiclone nightly for 6 months– Zolpidem (3-5x/week) for 12 weeks
Scharf MB et al., J Clin Psych. 1994;55:182-199.Walsh JK et al., Sleep Med. 2000;1:41-49.Krystal AD et al., Sleep. 2003;26:793-799.Perlis M et al., J Clin Psych. 2004;65:1128-1137.Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

BzRAs: Effects
Walsh JK et al., Sleep. 2000;23:1087-1096.
• Zolpidem, 10mg vs. Placebo
• 3-5x/week for 8 weeks

BzRAs: Effects
Krystal AD et al., Sleep. 2003;26:793-799.
• Eszopiclone, 3mg vs. Placebo
• Nightly for 6 months
• Sleep Latency

BzRAs: Effects
Krystal AD et al., Sleep. 2003;26:793-799.
• Eszopiclone, 3mg vs. Placebo
• Nightly for 6 months
• Time awake after sleep onset

BzRAs: Side effects & Safety
• Anterograde amnesia• Residual sedation – longer acting BzRAs • Rebound Insomnia? • Abuse and Dependence?
– Mostly used short term (2 weeks)– When used as a sleeping aid dose escalation rare – No studies of physical dependence with nighttime use– Low psychological dependence with nighttime use
• Increased fall risk in the elderly• Cognitive effects in the elderly• Increased mortality with sleep aids?
From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005

Smith MT et al., Am J Psych. 2002;159:5-11.
Treatment: Comparisons

Smith MT et al., Am J Psych. 2002;159:5-11.
Treatment: Comparisons

The End