hypoxaemiaafter and anaesthesia - bmj
TRANSCRIPT

POSTGRAD. MED. J., (1966) 42, 341
HYPOXAEMIA AFTER SURGERY ANDANAESTHESIA
J. P. PAYNE, M.B., F.F.A.R.IC.S., D.A. C. M. CONWAY, M.B., F.F.A.R.C.S., D.A.
Research Department of Anaesthetics, Royal College of Surgeonsof England, Lincoln's Inn Fields, London, W.C.12
THE significance of even transien't anoxia duringanaesthesia has been w'idely recognised formany years but until recently the frequentoccurrence and potendtiaJ danger of minor deg-rees of prolonged oxygen desaturation duringthe immediate post-operatlive period had notbeen appreciated. In 1962 however Nunn andPayne making use of the newer techniques ofblood gas analysis demonstralted that somedegree of arterial desaturation comimonly oc-curred after even 'the most trivial surgicalprocedures under general anaesthesia. S'incethen post-operative hypoxaemia has been in-tensively investigated and though the problemis not solved some of the relevant factors havebeen more clearly iden«tified.
I't has of course been widely known sincethe work of Maier and Cournand in 1943that lung surgery is associated with a substanytialreduction in arterial saturation which persistsfor severall dlays and even weeks after surgery,an observation later confirmed by Bjork andHilty (1954) who drew attention to the sig-nificance of post-operative hypoxaemia inrelation to the management of patients afteropen-chest surgery. Three years earl'ier Troell(195 1) had observed that 'major abdominal sur-gery was often followed by arterial desaturationboth in patients who had breatlhed spontane-ously and in those who had been artificiallyventilated. In 1958 Gordh, Linderholm andNorlander who were the first workers in thisfield to use an oxygen electrode to determineoxygen tensions in blood obtained a mean fallin arterill oxygen tension of albout 16 mm.Hg.after major non-thoracic surgery in patientsfree from card'iovascular and respiratorydisease.Diagnosis of Postoperative HypoxaemiaOne of the problems of post-operative hyp-
oxaemia is the difficulty of diagnosis. For manyyears it was widely believed that the colourof the patient's skin would give the first indica-tion of oxygen lack but even with an adequateskin blood flow the arterial oxygen tensioncan fall to as low as 40 mm.Hg. withoutevidence of cyanosis (Nunn, 1966). In fact
obvious clinical signs are absent with minordegrees of post-operative hypoxaemia and art-erial oxygen saturation values show only aslight fall below normal. But this observationis less re-assuring than is sometimes supposed.Because of the characteristic shape of thehaemoglobin oxygen dissocialtion curve slighhtreductions in oxygen saturation at the upper endof the curve correspond to much larger reduc-tions in arteridal oxygen tension; (Fig. 1). Thusan oxygen saturation of 90% has anequivalent tension of no more than 60 mm.Hg.in otherwise normal arterial blood. This ex-plains why the measurement of arterial oxygentension prov-ides a much more sensitive indexof minor degrees of arterial hypoxaemia thandoes the measurement of saturation.Oxygen tension measurements are usually
made by a pollarographic technique which is achemical method of analysis based on the factthat When an inert metal such as gold, mercuryor platinum is negatively charged and immersedin an electrolyte it will give up el&trons tod'issolved oxygen. The transfer of electrons isproportional to the current flowing which inturn is dependent on the amount of oxygenpresent. The resulltanrt current change ismeasured and expressed in terms of oxygentension.The first measurements of oxygen tension in
blood by polarography were carried out with adropping mercury electrode such as that usedby Gordh and his colleagues (1958) but' thisproved both ted(ious and difficult to use. Inparticular the deposition of plasma proteinson the surface of the electrodes was a majorsource of trouble. However by 1956 Clark haddemonstrated that it was possible to separatetihe entire electric celil from the blood or tissueby means of a thin polyethylene membranewhich prevented the passage of electrolytes butremained permeable to oxygen. This discoverycomfpletely revdkitionfised the design of oxygenelectrodes so that today virtually all commer-cially produced electrodes are based on Clark'soriginal description.To the improved methods of analysis must
be added the more sophisticated techniques
by copyright. on D
ecember 21, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.488.341 on 1 June 1966. Dow
nloaded from

342 POSTGRADUATE MEDICAL JOURNAL June, 1966
100
90
s0
*70
0 s
60a6
,,,o4-,~~~~~~~~
404
tm
0~~~~~~~~2
0 10 20 30 40 50 60 70 80 90 100 110 120 130 140
P02 mm. Hq.FIG. 1 -The relationship between oxygen tension and saturation showing the influence of tem-
perature and carbon dioxide on the slope of the dissociatilon curve (modified fromSamson Wright's Applied Phys,iology. p. 168. 11th Edi.).
for collecting arterial blood. In particular thedevelopmenlt within recent years of a percutane-ous technique for catheterising small arteriessuch as the radial has made possible serialstudies of blood gas ohanges during surgeryand anaesthesia. The fact that both the elect-rode design and the techhnique of arterialcatheterisation are recent developments explainswhy the detailed study of changes in arterialoxygen tension under different clinical con-ditions has only just begun.Mechanism of Postoperative Hypoxaemia
In the original series of Nunn and Payne(1962) 24 patients who had breathed spontane-ously during anaesthesia for a variety ofrelatively minor surgical procedures were foundto be hypoxic for up to 48 hours after theend of the anaesthetic. In these patients themean arterial oxygen saturation was 89% whichcorresponds to a mean oxygen tension of slightlyless than 60 m,m.Hg. In contrast the meancarbon dioxide tension was viftually normalwithin 20 minutes of the anaesthetic beingdiscontinued. This suggested that under-ventila-tion was not a factor in the development of
post-operative hypoxaemia and the belief tihatdepression of respiration did not contribute toarteriai oxygen desaturation was supported byConway and Payne (1963) who found noevidence of under-ventilation while observingthe effect of adm'inistering oxygen-enrichedmixtures to hypoxaemic patients in the im-mediate post-operative period. Twelve patientsWho vere studied while breathing room airbetween one and two hours after the end ofoperation showed an immediate improvement inarterial saturation when exposed to an inspiredmixture congtaining 30% oxygen. Increasing theinspired mixture to 50% oxygen did nolt mat-erially affect the improvement which was notsustained when the oxygen-enriched mixtureswere withdrawn. Throughout the study thearterial carbon dioxide tensions remained with-in normal limits but the extent of the desatura-tion varied over a faieldy wide range and was notobviously related to the anaesthetic technique,the duration of the anaesthetic nor to thenature of the surgery.
Since, on the evidence, under-ventilation hadnot contributed to the arterial desaturation,consideration had to be given to other factors
by copyright. on D
ecember 21, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.488.341 on 1 June 1966. Dow
nloaded from

PAYNE and CONWAY: Hypoxaemia
capable of interfering with oxygen transfer inthe lungs of relatively normal individuals. Ofthese reduced oxygen diffusing capaci-ty,though important in heavy exercise at altitude(West, Lahiri, Gill, Milledge, Pugh, and Ward,1962), does not cause a fall in oxygen saturationat rest and therefore could be disregarded.This left only two major possibilities, pulmo-nary shunts and maldistribution within thelungs. Tihe calculated shunt in the study ofNunn and Payne (1962) was approximately25% of the pulmonary blood flow. The onlyknown cause for such a large symptomlessshunt is pulmonary collapse but no rad'iolo-gical evidence of frank atelectasis was obtainedin any of these patients. Fuetthermore the factthat in such patients arterial oxygen saturationreturned allmogt to normal on exposure to onlymoderately enriched mixtures virtually excludedshunting as the cause of the desaturation. Thusmaldistribution or relative under-ventilation ina large proportion of the alveoli was left asthe most likely explanation for the observedhypoxaemia.The fact that patients on controlled respira-
tion had not been included in these studies ledto speculation that artificial ventilation mightprevent the development of post-operatlive hyp-
oxaemia but work by Bendixen, Hedley-Whiteand Laver (1963) and Conway and Payne(1964) demonstrated that impaired oxygenationoccurred in surgical patients just as readilyafter control'led ventilation under general anaes-
thesia as after spontaneous breathing duringthe anaesthetic.
In the series of Bendixen and his colleagues18 patients free from known pulmonary dis-ease were studied while undergoing operationswhich required profound muscular relaxationand oontro'lled venti;ation. A mean fall inoxygen tension of 22% and a decrease in lung
compliance of 15% were demonstrated over
a period of study averaging 76 minutes duringwhich ventilation was maintained at a constantlevel. At the end of the period of constantventilation three successive hyperinflations ofthe lungs restored both arterial oxygen ten-sion and lung compliance to control values.
Bendixen and his colleagues indicated thatthe progressive fall in lung compliance couldbe caused partly by changes in surface tensionin the lungs but suggested that most of thedecrease in compliance was due to the collapseof air spaces. The faet thaat the trend towardsimpaired oxygenation and reduced lung com-
pliance was reversed by periodic hyperinfia-
tion was used to support the argument thatthe arterial desaturation was due to pulmonarycollapse since it is well known that higherpressures are needed to open completely col-lapsed air spaces than to further inflate partiallyventilated alveoli.The impaired oxygenation of the arteri^wal
blood was attributed to capillary blood flowbeing maintained through collapsed and there-fore unventillated segments of lung. This per-fusion of underventi;lated alveoli was thoughtto divert part of the pulmonary blood flowin'to the systemic circulation without participa-tion in tihe normal ventilation processes of thelung. Normally less than 5% of the total cardiacoutput is shunted in this way but t-he develop-ment of atelectasis can lead to a variable butoften significant increase in the total shunt asreflected in a substantial fall in arterial oxygentension.On the basis of their observations Bendixen
and his group postuilated that progressive pul-monary atelectas'is associated witih impairedoxygenation of the arterial blood regularlyaccompanies anaesthesia if period"ic hyperinfla-tion of the lungs does not occur even whenventilation is normal by the usual criteria.The validity of this interpretation is doubt-
ful however. It does not explain the observationsof Conway and Payne (1964) who also invest-igated the relationship between artificialventilation duting surgery and post-operativeoxygen desaturation in a group of 15 patientsanaesthetised for routine elective surgery. Inthis study the patients were anaesthetised witha nitrous oxide-relaxaant tedhnique and ventillatedmanually so that the ventilation althoughadequate, was unlikely to be uniform, a factwhich was confirmed by the variations in thecarbon dioxide tensions of the arterial blood(Fig. 2.)
Despite the irregular hyperventillation Conwayand Payne observed a mean arterial oxygensaturattion after surgery of only 91.2%, equiva-lent to an oxygen tension of 68 mm.Hg. Butnot only was hypoxaemia present post-operatively, it was also in evidence duringsurgery even When hyperventilation was em-ployed and in spite of an inspired oxygenconcentraltion in the anaesthetic mixture, whichwas never reduced below 25%. Most surprisingof all however was the observation that somedegree of desaturation was present in fivepremedicated patients studied before the in-duction of anaesthesia.
This unexpected observa:tion gave supportto the view that neither the anaesthetic agent
June, 1966 343by copyright.
on Decem
ber 21, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.488.341 on 1 June 1966. D
ownloaded from

344 POSTGRADUATE MEDICAL JOURNAL June, 1966
INDUCTION END OF120 OPERATION
190100
70 g d
605050
~40
30
2021
20
-5 0 15 30 60 120 240 0 20 40 80 160 320MINUTES
DURING OPERATION POSTOPERATIVEFIG. 2.-Changes in arterial oxygen tension, arterial carbon dioxide tension
and standard bicarbonate be-fore, during and after anaesthesia withcontrolled respiration. Horizontal l-ines denote mean values and ver-ttical bars indicate standard devi!ations. Time scale is logarithmic.:(By courtesy of the Editor of the Lancet).
nor the technique was solely responsible forthe hypoxaemia and focused attention on pre-medication. Thus a more careful scrutiny ofearlier papers revealed that oxygen desatura-tion after premedication was not uncommon,although in most instances the observation hadbeen repor,ted without comment (Tomlin, Con-way and Payne, 1964).Effect of PremedicationThe first evidence of impaired arterial oxy-
genation after premedication was puiblished in1951 by Johnson who descrilbed a fall in oxygensaturation from 95 to 92% in nine patients
given morphine and hyoscine before surgery.A-bout the same time Troell (1951) reporteda mean oxygen saturation value of 92.8% in 28patients prepared for surgery; unfortunately thepremedication was not stated. A further studyin which the premedication was unspecifiedwas that of Holiday, Ma and Papper (1957)who found a mean oxygen satu-ration of 83%in a group of 25 patients before surgery.Although these authors themselves expresseddoubt about the accuracy of their method ofdetermining oxygen saturation, the 10% errorwhich they were willing to concede still implied
by copyright. on D
ecember 21, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.488.341 on 1 June 1966. Dow
nloaded from

PAYNE and CONWAY: Hypoxaentia
a significant degree of hypoxaemia in theirpatients.
Further evidence of impaired arteriail oxy-genation after premed'ication is to be foundin the work of Gord'h, 'Lindejholm and Nor-lander (1958) whose patients showed asignificant 'fall in arterial oxygen tension afterthe injection of morphine and hyoscine. In t'hecourse of 'their investigations Gordh and his'colleagues administered pure oxygen to pre-medicated patients and demonstrated a sulbstan-tia'l increase in the alveolar-arterial oxygengradient. This 'increased venous-admixturefollowing premedication was attributed to bed-rest and possilbly to pre-existen't pulmonarydisease.
Other evidence of arterial oxygen desatura-tion in premedicated patienits before surgerywas obtained from a series of palpers puiblishedbetween 1959 and 1962 'by Dobkin and hisgroup who measured the arterial oxygen satura-tion in a 'total of 161 premedicated patientsbefore ithe induction of anaeSthesia (Dobkin,1959; Dobkin, Drummond and Perkin, 1959;Dobbk'in, Jdhnston and Skinner, 1959; Dobkinand Byles, 1962a, 1962b; Dobkin and Song,1962). The mean arterial oxygen saturation of90.7% derived from these determinationsimplied a significant degree of impaired oxy-genation ascribed 'by Dobkin and 'his colleaguesto 'the centtral depressanrt effect of the narcoticdrugs included in the premedication.
But the post-operative hypoxaemria observedby Conway and Payne (1964) occurred inpatien'ts given atropine only and 'therefore couldnot be attributed to narcotic drugs. The possgilbi-lity that atropine could influence the oxygenconten't of arterial blood had then to be con-sidered. Accordingly Tomlin, Conway andPayne (1964) compared the'mean 'arterial oxy-gen saturation of 24 patients given atropinewith Ithat of a similar unpremedicated group.The mean arterial oxygen saturation in theatropirised group was 93.4%, a value sig-nificanttly lower than Ithe vailue of 96% obtainedfrom the control 'grou'p. Wlhen the saturationvalues were interpolated 'to obtain the cor-responding oxygen 'tensions the atropinisedpa'tients were 'shown to 'have a mean arterialoxygen 'tension 15 m'm.Hg. lower than that inthe contrdl group.Other investigators however have failed to
confirm this observation. Daly, Ross andBehnke (1963) found no dhange in arterialoxygen saturation 'ten m'inutes after intravenousatropine and Nunn and Bergmnan (1964) wereunable to find a significant change in arterial
oxygen tension twenty minutes after the drughad been given intravenously; but 'bolth thesegroups demonstrated a'marked increase'in phy-siological and anatomical dead space in the'irhealthy vo'lunteers after 'the administration ofatropine. Simi'larly in a limited study of sixhealthy young women admitted to lhospital foruterine curettage Taylor, Scott and Donald(1964) showed 'that 'the arterial oxygen tensionwas not significantly altered by tihe adlmintistra-tion of atropine given intramuscularly. Becauseof the apparent discrepancies Conway andhis colleagues planned to ex'tend their work toascertain firstly whe'ther 'the action o-f atropinewas dependent upon the route of administra-tion of 'the drug and secondly whether theomission of atropine premedication would subs-tan,tially modify the course of post-operativehypoxaemia'(Conway, 1966).Arterial Oxygen Tension in Normal PatientsOne difficullty that 'had 'to be overcome
before such an 'investigation could be carried ou'twas the lack of agreement among cliniciansalbout the normal arterial oxygen tension inhospitallised patients awailting surgery. 'indeedit was 'argued by Stephen and Talton (1964)that the real values were unknown. Theseworkers in a study of 14 surgical patientsobtained 'the low mean value of 80.4 'mm.Hg.,and Hamilton and 'his colleagues (1964) derivedan even lower value of 76.5 mm.Hg. from27 patients awaiting elective surgery.To estalblish normal values 'for th'is parameter
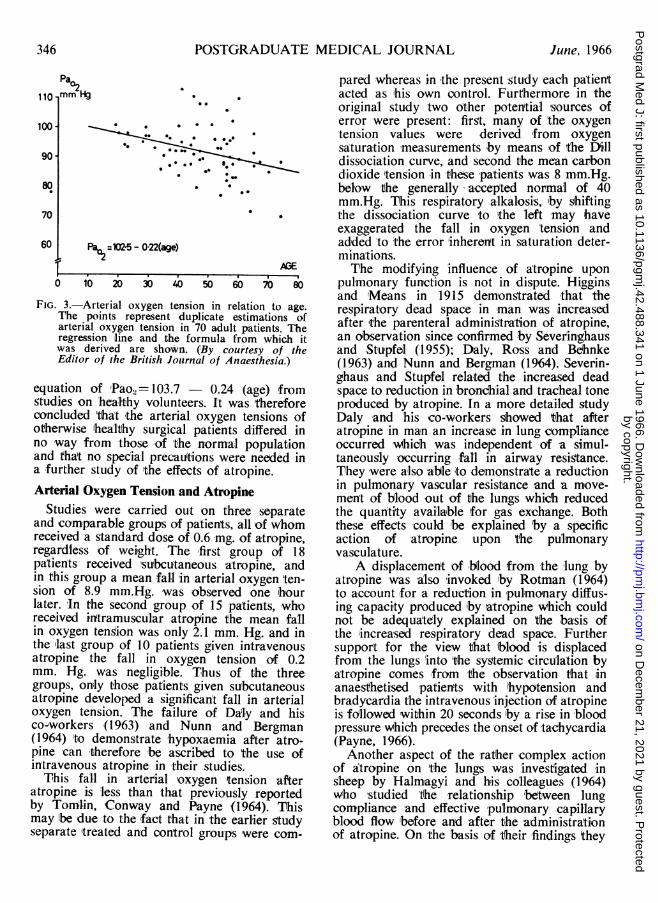
arterial iblood gas 'tensions were determined ina series of patients admitted 'to hospital forelective surgery. For the 'purpose 'of 'this studypatients suffering from any form of cardiovasc-lar or respiratory disease were excluded sincethe presence of sudh disease woutld almostcertain'ly 'impair the oxygenation of arterialblood. Apart from 'this assessment of 'physica;lstatus patients were selected for the trial atrandom. Du!plicate determinations of arterialoxygen and carbon dioxide tensions were madein 70 adult pa'tients of both sexes. No differ-ence in arterial ioxygen tension was notedbetween the sexes, bu't 'there was a markedinverse correlation between arterial oxygentension and age. Sta'ti5tical evaluation of thisrelation-ship gave a regression equation of theform Pao2=102.5-0.22 (age), (Fig. 3) with astandard deviation of 4.7 'mm.Hg., and a cor-relaltion coefficient, r= -0.61 '(Conway, Payneand Tomlin, 1965). This relationship 'is su,bs-tantially 'the same as 'that described by Ra'ineand Bishop '(1963) who derived a regression
June, 1966 345by copyright.
on Decem
ber 21, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.488.341 on 1 June 1966. D
ownloaded from
POSTGRADUATE MEDICAL JOURNAL
Pa
110- mm H
100 -
90-
80
70
60
* 0 a
0.'
0**~~~~~ -~* esa
*
Pa02=102-5- 0-22(age)
O 10 20 30 40 50 60 7b 80
FIG. 3.-Arterial oxygen tension in relation to age.The points represent duplicate estimations ofarterial oxygen tension in 70 adult patients. Theregression line and the formula from which itwas derived are shown. (,By courtesy of theEditor of the British Journal of Anaesthesia.)
equation of 'Pao2= 103.7 - 0.24 (age) fromgtudies on healthy volunteers. It was thereforeconcluded 'thait the arterial oxygen tensions ofotherwise 'healthy surgical patients diiffered inno way from those of tihe normal populationand that no special precautions were needed ina further study of the effects of atropine.Arterial Oxygen Tension and Atropine
Studies were carried out on three separateand comparable groups of patients, all of whomreceived a standard dose of 0.6 mg. of atropine,regardless of weight. The 'first group of 18patients received 'subcutaneous -atropine, andin this group a mean fall in arterial oxygen 'ten-sion of 8.9 mm.Hg. was observed one hourlater. 1In the second group of 15 patients, whoreceived initramuscular atrooine the mean falilin oxygen tensiion was only 2.1 mm. Hg. and inthe last group of 10 patients given intravenousatropine the fall in oxygen tension of 0.2mm. Hg. was negligtible. Thus of the threegroups, only those patients given subcutaneousatropine developed a significan't fall in arterialoxygen tension. TIhe failure of Daly and hisco-workers (l963) and Nunn and Bergman(1964) to demonstrate hypoxaemia after atro-pine -can therefore 'be ascribed to the use ofintravenous atropine in their studies.
This fall in arterial oxygen tension afteratropine is less than that previously reportedby Tomlin, Conway and Payne (1964). Thismay Ibe due to the fact that in the earlier sftudyseparate treated and control groups were com-
pared whereas in the present study each pa'tien'tacted as 'his own control. Furthermore in theoriginal study two other potential sources oferror were present: first, many of the oxygentension values were derived 'from oxygensaturation 'measurements by means of the Dilldissociation curve, and second the mean carbondioxide 'tension in these pa9tients was 8 mm.Hg.below the generally accepted normal of 40mm.Hg. This respiratory alkalosis, by shiftingthe dissociation curve to 'the left may haveexaggerated the fall in oxygen tension andad'ded 'to 'the error inherent in saturation deter-minations.The modifying influence of atropine upon
pulmonary function is not in dispute. Higginsand 'Means in 1915 demongtrated that therespiratory dead space in man was increasedafter ithe parenteral adimini5tration of atropine,an observation since confirmed by Severinghausand Stu'pfel (1955); Daly, Ross and Beshnke(1963) and Nunn and Bergman (1964). Severin-ghaus and Stupfel related the increased deadspace to reduction in brondhial and tracheal toneproduced by atropine. In a more detailed studyDaly and ihis co-workers showed that afteratropine in man an increase in lung complianceoccurred w1hich was independent of a simul-taneously occurring fall in airway resigtance.They'were also able to demonstrate a reductionin pulmonary vascular resistance and a move-ment of blood out of the lungs which reducedthe quantity availlable for gas exchange. Boththese effects could 'be explained by a specificaction of atropine upon the pulmonaryvasculature.
A displacemen't of blood from the lung byatropine was also invoked 'by Rotman (1964)to account for a reduction in pulmonary diffus-ing capacity produced iby atropine which couldnot be adequa'tely explained on the basis ofthe 'increased respiratory dead space. Furthersupport for the view that blood is displacedfrom the lungs 'into 'the sysotemic circulation byatropine comes from the o'bservation that inanaesthetised 'patients with hypotension andbradycardia the intravenous injection of atropineis fdllowed within 20 seconds by a rise in bloodpressure which precedes the onset of tachycardia(Payne, 1966).Another aspect of the rather complex action
of atropine on 'tihe lungs was investigated insheep by Halmagyi and h'is colleagues (1964)who studied 'She relationship between lungcompliance and effective pulmonary capillaryblood flow 'before and after the administrationof atropine. On 'the basis of 'their ifindings they
346 June, 1966
0
ig
by copyright. on D
ecember 21, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.488.341 on 1 June 1966. Dow
nloaded from

PAYNE and CONWAY: Hypoxaemia
postulated the existence of a local pulmonaryalveolar vascular reflex by which perfusion 'isregulated in response to ventilation. Theyfurtther postula:ted that atropine 'blocks thislocal reflex and renders the pulmonary bloodflow passive.Thus the fall iin arterial oxygen tension
following the suibcutaneous adm!inistration ofatropine could ibe due to its action on thenervous or local reflex regulation of the cir-culation 'through the 'lung; 'but it could alsoresult from impaired ventilation due to in-creased tenacity of secretions following atropine.The fact that the fall in oxygen tension appearsto be a ifunction of the route of administrationsupports 'the latter explanation. This pheno-menon could n6t be demonstrated when atropinewas given by intravenous injection which favoursrapid albsorption, a high initia:l (blood 'level, anda re'latively short duration of action. Sub-cutaneous adminigtration allows slow absorp-tion and the possibility of prdlongedmain'tenance of effective (blood levels. In thisconnection it has long been recognised thatthe subjective effects of atropine are minimalwhen given intravenously and most pronouncedafter subcutaneous administration.The circulatory and venrtilatory effects of
atropine on the 'lung are difficult to reconcileparticularly in relation to the effects on arterialoxygen tension. Nevertheless -there is sufficientevidence that the drug is 'implicated in thedevelopment of poSt-operative 'hypoxaemia tojustify 'the recommendation that it should nolonger be used routinely for premedication.
Postoperative Hypoxaemia and AgeRecently N'unn (1965) 'has demonstrated a
sign'ificant correlation between the severity ofof post-opera-tive 'hypoxaemia and age, and hasdrawn atten'tion 'to the existence of a s'imilarrelationship in 'previous 'published series byother authors. Such a relaltionship between ageand arterial oxygen tension during -the post-operative period might of course have been anti-cipated from 'the -work of ,Raine and Bis'hop(1963) which related arterial oxygen tension toage 'in normal subjects. Of considerable im-portance is 'the fact that 'the slope of thearterial oxygen 'tension-age regression line ismu,h steeper in 'pa!tien'ts after 'surgery than innormal volunteers (Ra'ine and Bishop, 1963)or in 'healthy patients awaiting surgery (Con-way, Payne and Tomlin, 1965). The increasedslope of 'this line 'in the post-operative periodimplies that a greater fa:'ll in arterial oxygentension is ito be expected in elderly patients
Pa02 L NmmHg
70N
60 -NFE
0 20 40 60 80 yrsAGE
FIG. 4.-A. Conway, Payne and Tomlin
(1965) conscious surgicalpatients 102.5-0.22 (age)
B. Raine and Bishop (1963)healthy volunteers 103.7-0.24 (age)
C. Gordh, Linderholm andNorlander (1958) 92.1-0.327 (aFge)
E. Nunn (1965) 1 'hour afteroperation 84.8-0.343 (age)
D. Palmer and Gardiner (1964)day after operation 97.7-0.429 (age)
F. Nunn (1965) pooled data 94.3-0.455 (age)Regression lines A and B represent the fall inoxygen tension with age in healthy subjects. 'Re-gression lines C, D, E and F represent the fallin oxygen tension with age in patients afteranaesthesia and surgery and indicate that notonly is the oxygen tension lower after anaesthesiaand surgery but also !that the fall is greater withincreasing age.
(Fig. 4) Whose arterial oxygen tension is alreadylow and 'who are 'therefore least able 'to toleratefurther impairment (Payne and Conway, 1965).
Other FactorsAlthough there is now considerable agree-
ment t-hatt the fundamental disorder in 'post-operative hypoxaemtia is a disturbance in theventilaltion-perfusion ratio, other explanationsfor 'tihis 'phenomenon Ihave Ibeen advanced.
In a review of the factors influencing post-operative hypoxaemia 'Marshall and Millar(1965) claimed that the hypoxaemia Whlich 'theyobserved could 'be explained almost entirelyby a combination of under-ventilation and'diffusion hypoxia' but their evidence is notconvincing. The 'higthest 'mean carbon dioxidetension recorded in their studies was 43
347June, 1966by copyright.
on Decem
ber 21, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.488.341 on 1 June 1966. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
mm.Hg., a level scarcoly compatible with sig-nificant under-ventilation. The occurrence of'diffusion hypoxia' following tihe return to air-breathing after inha'ling nitrous oxide is ofcourse welil known (Fink, 1955). It is due tothe rapid passage of large vlu'mes of nitrousoxide 'from the pulmonary capillary blood intothe alveoli. Such a transfer of ni'trous oxidedi'lutes the alveolar air and 'produces inspiratoryhypoventilation with a tendency to expiratoryhyperventilation. The phenomenon however isessenitiadlly transient and is unlikeily to give riseto post-operative hypoxaemia lasting severalhours.
In support of their contention Marshall andMi'l'lar pointed out 'that they had 'been u,nableto demonstrate'post-operative hypoxaemia aftershort operations 'but that it was common aftermore prollonged procedures. They argued thatduring long operaltions more nitrous oxide istaken up and as a result a greater amount ofthe gas is available to cause diffusi,on lhypoxiawhen the anaesthetic is withdrawn. But nitrousoxide is a re'latively 'insoluible anaesthetic gaswith a 'high rate of uptake only during theinduction sgtage; thereafter the uptake falls offvery rapidly so -that the amount dissolved inthe body when anaesthesia is prolonged is notsulbstantially increased. This, together with thefact thalt impaired oxygenation is commonlyfound post-operatively in ipatients who havenot been exposed to 'nitrous oxide, virtuallyexcludes diffus'ion 'hypoxia as a'major factor inthe development of 'post-operative hypoxaemia.Nunn and ihis colleagues '(1965) have
descrilbed andther possible factor in the genesisof post-operative 'hypoxaemia. They showed thatWhen volunteers breathed 'within their functionalresidual capacity 'by deliberately contracting thealbdominal muscles during expira'tion increasedghunting of blood occurred 'in the lungs. Nunnand 'his col'leagues also showed that the shuntingeffect was 'increased 'by 'breathing -pure oxygenand -that on return 'to a!ir-breathing the oxygentens'ion fell sharply to below normal levelsand was associated with a varying degree oflung cIllapse 'Which persisted for up to 48'hours.
This cobservation may explain Why patientsstraining on an endotracheal 'tube are oftencyanosed even wuhen the tida:l volume isaoparently normal. Presumably patients witthchronic chest diisease are particularly sus-ceptilble to this type of col'lalpse and -this pro-bably accounlts for Hobsley's observations(1963) that if a reduced arterial oxygen tensionwas foun'd immediately after operation in
patien'ts with chronic bronehlitis frank collapsealmost invariably followed.
In addition to chronic chest disease a varietyof other conditions such as obesity, abdominalsurgery and relaxant drugs can reduce t-hefunctional residual capacity, and it is wellwithin the 'bounds of possibility ithat *this re-duction can exaggerate or even provoke post-operative hypoxaemia. It is difficult howeverto see how 'such 'hypoxaemia could be symptom-less; almost certainly in these circumstances thefrank atelectasis descri(bed iby Hobsley woulddevelop and diagnosis would be relatively easy.It is worth remembering thatthe hypoxaetmiadescriibed 'by Nunn and Payne ('1962) was notassociated with demonstrable atelectasis or in-deed with any signs and symptoms other thanthe reduced oxygen 'tension in 'the blood, where-in ilies the danger.Significance of Postoperative HypoxaemiaThe clinical significance of post-operative
hypoxaemia is not easy 'to assess. A reductionof arterial oxygen tension of 20 or even 30mm.Hg. from the normal level is 'unlikely toresult 'in dangerous tissue hypoxia in 'healthyindividuals at rest but such a reduction occur-ring in patients whose arterial oxygen tensionis a(lready low might easily lead 'to serioushypoxia and even death. The danger is greatestin the im'mediate post-operative iperiod whenthe restlessness of hypoxia is of'ten misinter-preted as evidence of pain and treated withmorphine. Patients with limited cardiac orrespiratory reserves are particularly vulnerableas also are 'patients whose metabolism 'is in-creased or otherwise deranged, and the administ-ration of oxygen 'should be a rou'tine part oftheir post-operative management. Elderlypatients who are liable to a greater degree ofpost-operative 'hypoxaemia superimposed uponpre-existing normally low arterial oxygen ten-sions should also rece'ive such routine oxygentherapy.The administration of oxygen does not solve
the prdblem of post-operative oxygen deficiencybut at least it relieves the hypoxia and inindividual cases it may even prevent the onsetof irreversible bra'in damage. Recently howeverRavin (1966) has daimed that 'the impairedoxvgenation seen after surgery and anaesthesiawill irespond to deep breathing in nearly everyinstance. In ihis series 20 'healthy patients werestuidied following surgery. One hour afteroperation arterial blood samples were with-drawn for the determination of oxygen satura-tion values, Ithereafter ten patien'ts selected at
348 June, 1966by copyright.
on Decem
ber 21, 2021 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.42.488.341 on 1 June 1966. D
ownloaded from

June, 1966 PAYNE and CONWAY: Hypoxaemia 349
random were asked ito take five consecutivedeep breaths. The effect of this was to pro-duce a mean arterial oxygen saturation thatwas significantly greater than in the controlgroup; this difference remained significant aftereight to ten hours. If Ravin's observa:tions canbe substantiated the management of post-operative hypoxaemia wil'l be considerablysimplified and perhaps a ilarge element of therisk involved eliminated.
REFERENCESBENDIXEN, H. H., HEDLEY-WHYTE, J., and LAVER,M. B. (1963): Impaired Oxygenation in SurgicalPatients during General Anesthesia with ControlledVentilation. A Concept of Atelectasis, New Engl. J.Med., 269, 991.
BioRK, 0. V., and HILTY, H. J. (1954): The ArterialOxygen and Carbon Dioxide Tensions during thePost-operative Period in Cases of Pulmonary Re-sections and Thoracoplasties, J. thorac. Surg., 27,455.
CLARK, L. C. (1956): Monitor and Control of Bloodand Tissue Oxygen Tension, Trans. Soc. for art. Int.Organs, 2, 41.
CONWAY, C. M. (1966): Arterial Oxygen Tensions inSurgical Patients. In: 'Oxygen Measurements inBlood and Tissues and their Significance. p.173.Ed. J. P. Payne and D. W. Hill. London: J. A.Churchill.
CONWAY, C. M., and PAYNE, J. P. (1963): Post-operative Hypoxaemia and Oxygen Therapy, Brit.med. J., i, 844.
CONWAY, C. M., and PAYNE, J. P. (1964): HypoxaemiaAssociated with Anaesthesia and Controlled Res-piration, Lancet, i, 12.
CONWAY, C. M., PAYNE, J. P., and TOMLIN, P. J.(1965): Arterial Oxygel Tensions of Patients await-ing Surgery, Brit. J. Anaesth., 37, 405.
DALY, W. J., Ross, J. C., and BEHNKE, R. H. (1963):The Effect of Changes in the Pulmonary VascularBed produced by Atropine, Pulmonary Engorge-ment and Positive-pressure Breathing on Diffusingand Mechanical Properties of the Lung, J. clin.Invest., 42, 1083.
DOBKIN, A. B. (1959): The Effect of Fluothane onAti&base 'Balance, Anesthesiology, 20, 10.
DOBKIN, A. 'B., DRUMMOND, K., and PURKIN, N.(1959): Anaesthesia with the Azeotropic Mixtureof Halothane and Diethyl Ether, Brit. J. Anaesth.,31, 53.
DOBKIN, A. B., JOHNSTON, H. J., and 'SKINNER, L. C.(1960): A Study of Chloroform Anaesthesia in aPrecisio'n System: I. The Effect on Anion-cationBalance in Man, Canad. Anaesth. Soc. J., 7, 257.
DOBKIN, A. B., and BYLES, P. H. (1962): Effect ofFluroxene (Fluoromar) on Acid-base'Balance inMan, Acta anaesth. Scand., 6, 115.
DOBKIN, A. B., and BYLES, P. H. (1962): TheEffect of Tridhloroethylene-Nitrous Oxide Anaes-thesia on Acid-base Balance in Man, Brit. J.Anaesth., 34, 797.
DOBKIN, A. B., and SONG, Y. (1962): The Effect ofMethoxyflurane-ANitrous Oxide Anesthesia on Ar-terial :H, Oxygen Saturation, Paco., and PlasmaBicarbonate in Man, Anesthesiology, 23, 601.
FiNK, B. R. (1955): Diffusion Anoxia, Anesthesiology,16, 511.
GORDH, T., LINDERHOLM, H., and NORLANDER, 0.(1958): Pulmonary Function in Relation to Anes-thesia and Surgery Evaluated by Analysis of Oxy-gen Tension of Arterial Blood, Acta. Anaesih.Scand., 2, 15.
HALMAGYI, D. F., COLEBATCH. H. J. H., STARZECHI,B., and HORNER, G. J. (1964): Pulmonary Alveolar-Vascular Reflex, J. appl. Physiol., 19, 105.
HAMILTON, W. K., McDONALD, J. S., FISCHER, H. W.,and BETHARDS, R. (1964): Post-operative Respira-tory Complications: a Comparison of Arterial GasTensions, Radiographg and Physical Examination,Anesthesiology, 25, 607.
HIGGINS, H. L., and MEANS, J. H. (1915): The Effectof Certain Drugs on the Respiration and GaseousMetabolism in Normal Human Subjects, J.Pharmacol. exp. Ther., 7, 1.
HOBSLEY, M. (1963): Respiratory DisturlbancesCaused by General Surgical Operations, Ann. roy.Coll. Surg. EngI., 33, 105.
HOLADAY, D. A., MA, D., and PAPPER, E. M. (1957):The Immediate Effects of Respiratory Depressionon Acid-base Balance in Anaesthetised Man, J.clin. Invest, 36, 1121.
JOHNSON, S. R. (1951): The Effect of Some Anaes-thetic Agents on the Circulation in M,an. WithSpecial Reference to the Significance of PulmonaryBlood Volume for the Circuilatory Regulation, Acta.chir. Scand. Suppl., 158.
MAIER, H. C., and COURNAND, A. (1943): Studies ofArterial Oxygen Saturation in the Post-operativePeriod after Pulmonary Resection, Surgery, 13, 199.
MARSHALL, B. E., and MILLER, R. A. (1965): SomeFactors Influencing Post-operative Hypoxaemia,Anaesthesia, 20, 408.
NUNN, J. F. (1965): Influence of Age and OtherFactors on Hypoxaemia in the Post-operativePeriod, Lancet, ii, 466.
NUNN, J. F. (1966): Alveolar-Arterial Po2 Differencein Anaesthesia. In: Oxygen Measurements in Bloodand Tissues and their Significance. Ed. Payne, J. P.,and Hill, D. W. p. 187. London: J. and A.Churchill.
NUNN, J. P., and BERGMAN, N. A. (1964): The Effectof Atropine on Pulmonary Gas Exc1hange, Brit. J.Anaesth., 36, 68.
NUNN, J. F., COLEMAN, A. J., SACHITHANANDAN, T.,BERGMAN, N. A., and LAWS, J. W. (1965): Hypox-aemia and Atelectasis Produced by Forced Expira-tion, Brit. J. Anaesth., 37, 3.
PALMER, K. N., and GARDINER, A. J. (1964): Effectof Partial Gastrectomy on Pulmonary Physiology,Brit. med. J., i, 347.
PAYNE, J. P., and CONWAY, C. iM. (1965): Hypoxaemiaafter General Anaesthesia, Lancet, ii, 631.
PAYNE, J. P. (1966): In: Oxygen Measurements inBlood and Tissues and their Significance. Ed. Payne,J. P., and Hill, D. W. p.182. London: J. and A.Churchill.
PAYNE, J. P., and CONWAY, C. M. (1965): Hypoxaemiiain the Post-operative Period, Lancet, ii, 638.
RAINE, JUNE, and BISHOP, J. M. (1963): A Differencein 09 Tension and Physiological Dead Space inNormal Man, J. appl. Physiol., 18, 284.
RAVIN, M. B. (1966): Value of Deep Breaths inReversing Post-operative Hypoxaemia, N.Y. StateJ. Med., 66, 244.
ROTMAN, H. H. (1964): Effect of Atropine on Pul-monary Diffusing Capacity in Man, Brit. J.Anaesth., 36, 74.
by copyright. on D
ecember 21, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.488.341 on 1 June 1966. Dow
nloaded from

350 POSTGRADUATE MEDICAL JOURNAL June, 1966
SEVERINGHAUS, J. W., and S2$6915, M. A. (1955):Respiratory Dead Space Increase Following Atro-pine in Man and Atropine, Vagal or GanglionicBlockade and Hypothermia in Dogs, J. appl.Physiol., 8, 81.
STEPHEN, C. B., and TALTON, I. (1964): ImmediatePost-operative Care, with Particular Reference toBlood-gas Studies, Canad. Anaesth. Soc. J., 11, 586.
TAYLOR, S. H., Scorr, D. B., and DONALD, K. W.(1964): Respiratory Effects of General Anaesthesia,Lancet, i, 841.
TOMLIN, P. J., CONWAY, C. M., and PAYNE, J. P.(1964): Hypoxaemia Due to Atropine, Lancet, i,14.
TROELL, L. (1951): Post-operative Changes in Cir-culation and the Effects of Oxygen Therapy, Acta.chir. Scand., 102, 203.
WEST, J. B., LAHIRI, S., GILL, M. B., MILLEDGE, J. S.,PUGH, L. G. C. E., and WARD, M. P. (1962):Arterial Oxygen Saturation During Exercise at HighAltitude, J. appl. Physiol., 17, 617.
by copyright. on D
ecember 21, 2021 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.42.488.341 on 1 June 1966. Dow
nloaded from