iaslc atlas of alk testing in lung cancer
DESCRIPTION
This guide is designed to help pathologists, laboratory scientists, and practicing physicians better understand the background, protocol, and interpretation of results of ALK testing in patients with advanced NSCLC.TRANSCRIPT

IASLC AtL AS of ALK teStIng In Lung CAnCer
international association for the study of lung cancer
edited by Ming sound tsao, Md, frcPcfred r. hirsch, Md, Phdyasushi yatabe, Md, Phd

IASLC AtL AS of ALK teStIng In Lung CAnCer

International Association for the Study of Lung Cancer, Aurora, Colorado, USA
Editors: Ming Sound Tsao, MD, FRCPC Fred R. Hirsch, MD, PhD Yasushi Yatabe, MD, PhD
An IASLC publication published by IASLC Press
Original cover and book layout design by Biographics
IASLC Press Office: IASLC, 13100 East Colfax Ave., Unit 10, Aurora, Colorado 80011, USA www.iaslc.org
First IASLC Press Printing October 2013 10 9 8 7 6 5 4 3 2 1
ISBN: 978-1-940488-00-4
Copyright ©2013 International Association for the Study of Lung Cancer All rights reserved
Without limiting the rights under copyright reserved above, no part of this publication may be reproduced, stored in or introduced into a retrieval system, or transmitted in any form, or by any means without prior written permission.
While the information in this book is believed to be true and accurate as of the publication date, neither the IASLC nor the editors nor the publisher can accept any legal responsibility for any errors or omissions that may be made. The publisher makes no warranty, express or implied, with response to the material contained therein.

Edited by Ming Sound Tsao, MD, FRCPC
Fred R. Hirsch, MD, PhD
Yasushi Yatabe, MD, PhD
INTERNATIONAL ASSOCIATION FOR THE STUDY OF LUNg CANCER
IASLC AtL AS of ALK teStIng In Lung CAnCer

Acknowledgments
IASLC acknowledges the generous funding and support provided by Pfizer Oncology for this ALK Atlas project.
The co-editors and all contributors also acknowledge the editorial assistance of Lori Alexander, MTPW, ELS, and support of Deborah A. Whippen, Editorial Rx, Inc., and Rania gaspo, PhD, Pfizer Oncology, during the preparation of this publication.

ContentS
List of Contributors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
Abbreviations . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
Manufacturers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8
Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9
Chapter 1 Candidates for ALK Testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .11
Chapter 2 Sample Acquisition, Processing, and general Diagnostic Procedures . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .13
Chapter 3 Fluorescence in situ Hybridization (FISH) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .17
Chapter 4 Immunohistochemistry (IHC) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29
Chapter 5 Reverse-Transcriptase Polymerase Chain Reaction (RT-PCR) and Multiple gene Assays . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .38
Chapter 6 Comparison of Different Assay Platforms for ALK Testing . . . . . . . . . . . . . . . . . . .44
Chapter 7 ALK Analysis in Cytology . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .53
Chapter 8 Reporting of ALK Testing . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .58
Chapter 9 guidelines and Standardization Studies . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .61
Chapter 10 Summary and Future Perspectives . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .67
References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .69
Appendix 1 Summary of Published Studies on ALK gene Rearrangement Testing in Lung Cancer. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .74
Appendix 2 CAP/IASLC/AMP Molecular Testing guideline for Selection of Patients with Lung Cancer for Treatment with EgFR and ALK Tyrosine Kinase Inhibitors . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .76

6IASLC ATLAS OF ALK TESTING IN LUNG CANCER
Ming Sound Tsao, MD, FRCPCPathologist and Senior Scientist, Princess Margaret Cancer Centre, University Health Network Professor, Department of Laboratory Medicine and Pathobiology, University of Toronto Toronto, Canada
Fred R. Hirsch, MD, PhD Professor, Department of MedicineDepartment of PathologyUniversity of Colorado at DenverDenver, Colorado, USA
Yasushi Yatabe, MD, PhD Chief, Department of Pathology and Molecular Diagnostics,Aichi Cancer CenterNagoya, Japan
List of Contributors
Elisabeth Brambilla, MD, PhDProfessor, Département d’Anatomie et Cytologie PathologiquesINSERM U823 Institut Albert Bonniot Centre Hospitalier Universitaire de grenoble, Université Joseph Fouriergrenoble, France
Lukas Bubendorf, MDProfessor and Head, Division of CytopathologyInstitute for Pathology, University Hospital BaselBasel, Switzerland
Jin-Haeng Chung, MD, PhDProfessor, Department of PathologySeoul National University Bundang HospitalSeoul, South Korea
Keith M. Kerr, FRCPathProfessor, Department of PathologyAberdeen University Medical SchoolAberdeen Royal InfirmaryAberdeen, Scotland, United Kingdom
Sylvie Lantuéjoul, MD, PhDProfessor and Chair, Départementd’Anatomie et Cytologie PathologiquesINSERM U 823 Institut Albert BonniotCentre Hospitalier Universitair A Michallon, Université Joseph Fourier grenoble, France
Kengo Takeuchi, MD, PhDPathology Project for Molecular Targets of the Cancer InstituteDivision of Pathology of the Cancer Institute HospitalJapanese Foundation for Cancer Research Tokyo, Japan
Erik Thunnissen, MD, PhDConsultant Pathologist, VU University Medical CenterAmsterdam, The Netherlands
Marileila Varella-Garcia, PhDProfessor, Department of Medicine/Medical OncologyDepartment of Pathology University of Colorado at DenverDenver, Colorado, USA
Ignacio Wistuba, MDProfessor and Chair, Jay and Lori Eisenberg Endowed ProfessorDepartment of Translational Molecular PathologyThe University of Texas MD Anderson Cancer CenterHouston, Texas, USA
Akihiko Yoshida, MD, PhDAttending Pathologist, Department of PathologyNational Cancer Center HospitalTokyo, Japan
Contributing Authors
Editors
IASLC ALK Testing Workshop attendees, Sorrento, Italy, 2013. Front row, left to right–Y. Yatabe, M. Varella-garcia, E. Brambilla, S. Lantéujoul, R. gaspo (Pfizer Oncology), J-H Chung; back row, left to right–A. Yoshida, I. Wistuba, F. R. Hirsch, M. S. Tsao, E. Thunnissen, L. Bubendorf, K. Kerr.

7AbbREvIATIONS
AEC: 3-amino-9-ethylcarbazol ALK: anaplastic lymphoma kinaseAMP: Association for Molecular Pathology ATS: American Thoracic Society CAP: College of American PathologistsCISH: chromogenic in situ hybridizationDAB: 3, 3' diaminobenzidineEBUS: endobronchial ultrasound EDTA: ethylenediaminetetraacetic acidEGFR: epidermal growth factor receptorEML4: echinoderm microtubule-associated protein-like 4ERS: European Respiratory SocietyETOP: European Thoracic Oncology PlatformEUS: transesophageal ultrasound FDA: US Food and Drug AdministrationFFPE: formalin-fixed paraffin-embeddedFISH: fluorescence in situ hybridizationFNA: fine-needle aspirationH & E: hematoxylin & eosinHER2: human epidermal growth factor receptor-2iAEP: intercalated antibody-enhanced polymerIASLC: International Association for the Study of Lung CancerIHC: immunohistochemistryISH: in situ hybridizationKIF5B: kinesin family member 5BNOS: not otherwise specifiedNSCLC: non-small cell lung cancerNgS: next-generation sequencingRET: ret proto-oncogeneROS1: c-ros oncogene 1RT-PCR: reverse-transcriptase polymerase chain reactionSCLC: small cell lung cancerTKI: tyrosine kinase inhibitorv: variant
AbbreviationsThe following abbreviations are used in the text.

8IASLC ATLAS OF ALK TESTING IN LUNG CANCER
ManufacturersThe following manufacturers and their products are noted in this Atlas. The locations given for each manufacturer is not the only location; most manufacturers have offices worldwide.
Abbott MolecularAbbott Park, Illinois, USAVysis LSI ALK Break Apart FISH Probe Kit, Spectrum Orange Probe, and Spectrum Green Probe
AbcamCambridge, UKAnti-ALK antibody (5A4)
BD (Becton, Dickinson and Company) DiagnosticsFranklin Lakes, New Jersey, USASurePath
Cell Signaling TechnologyDanvers, Massachusetts, USAD5F3 antibody (ALK [D5F3] XP Rabbit mAb)
Dakoglostrup, DenmarkCarpinteria, California, USAADVANCE, ALK1 antibody, EnVision, EnVision+, EnVision FLEX, and EnVision FLEX+, PT Link, and Target Retrieval Solution Hologic, Inc.Bedford, Massachusetts, USAThinPrep
Invitrogen, Life Technologies CorporationCarlsbad, California, USAAnti-ALK antibody
Leica BiosystemsBuffalo grove, Illinois, USAWetzlar, germanyBond-Max, Novolink Polymer Detection System
Nichirei Biosciences, Inc.Tokyo, Japan5A4 antibody (Histofine ALK Detection Kit)
NovocastraNewcastle, UK5A4 antibody
NanoString TechnologiesSeattle, Washington, USANanoString assay
Pfizer OncologyNew York, New York, USAXalkoriTM
Ventana Medical Systems, Inc. (member of the Roche group)Tucson, Arizona, USA BenchMark XT, iVIEW DAB Detection Kit, OptiView DAB IHC Detection Kit, OptiView Amplification Kit, and ultraView Universal DAB Kit, and Rabbit Monoclonal Primary Antibody assay
ZytoVision GmbHBremerhaven, germanyZytoDot 2C SPEC ALK break-apart probe

Over the past years, the diagnosis and treatment of patients with advanced lung cancer have under-gone transformational changes. The current paradigm for prescribing novel targeted therapies is based on selecting patients according to the presence of specific oncogenic abnormalities in the tumor. The first such abnormalities to be discovered in lung cancer were epidermal growth factor (EGFR) kinase domain mutations, and tumors with these mutations were found to have sensitivity to EgFR tyrosine kinase inhibitors (TKIs). Since then, the anaplastic lymphoma kinase (ALK) gene has emerged as the second driver oncogene in lung cancer for which highly effective novel therapies have been developed. The novel ALK fusion gene is formed by a rearrangement occurring on the short arm of chromosome 2 and involves the genes encoding for ALK (2p23.2) and echinoderm microtubule-associated protein-like 4 (EML4) (2p21) or, rarely, genes on other chromosomes. The protein product of this new fusion gene has a constitutively active ALK kinase because the basic domain of the EML4 gene provides a mechanism for the dimerization of the new chimeric protein. Multiple variants of a rearranged EML4-ALK fusion gene have been identified in lung cancers. The fusions involve the N-terminal portion of the EML4 gene and the C-terminal kinase domain of the ALK gene. Because this gene rearrangement involves large chromosomal inversion and translocation, fluo-rescence in situ hybridization (FISH) has become the method of choice for detecting all forms of ALK gene rearrangement, and it was the assay used to detect this genetic aberration in the first clinical trials of the ALK inhibitor crizotinib (Xalkori®, Pfizer Oncology) (Bang 2010, Kwak 2010, Camidge 2012). Thus, FISH with ALK break-apart rearrangement probes has become the criterion standard for the diagnosis of lung cancers with the ALK rearrangement, and the US Food and Drug Administration (FDA) has approved the Vysis LSI ALK Break Apart FISH Probe Kit (Abbott Molecular). This assay, along with well-defined criteria for positive and negative results, was used to identify patients with advanced non-small cell lung cancer (NSCLC) that was positive for ALK rearrangement. In a phase I/II study, crizotinib was associated with an objective response rate of 61% and a median progression-free survival of 9.7 months (Camidge 2012). In a randomized phase III study (PROFILE 1007), in which crizotinib was compared with chemotherapy in patients in whom disease had progressed during conventional chemotherapy, treatment with crizotinib was associated with an objective response rate of 65% (compared with 20% for chemotherapy) and a median progression-free survival of 7.7 months (compared with 3.0 months for chemotherapy) (Shaw 2013).
By Ming Sound Tsao, Fred R. Hirsch, and Yasushi Yatabe
IntroduCtIon

10IASLC ATLAS OF ALK TESTING IN LUNG CANCER
A new generation of ALK inhibitors has been developed, and these inhibitors are being studied in ongoing clinical trials. As the nature of various gene rearrangements become known, assays using polymerase chain reaction (PCR) and sequencing to detect the fusion genes have been developed. In addition, studies from multiple institutions have shown that ALK protein can be detected by immunohistochemistry (IHC) with signal amplification in almost all tumors that are ALK positive on FISH, and several case reports have also reported that NSCLC tumors harboring atypical ALK pat-terns on FISH (ALK FISH negative) that are ALK positive on IHC may respond to treatment with ALK inhibitors (Peled 2012). In this context, commercial IHC kits are currently under development and validation. The development of these multiple diagnostic platforms provides alternative methods for labo-ratories to detect ALK gene rearrangements or fusion proteins, depending on the local availability of technical expertise and equipment. Because clinical diagnostic testing requires assays that can be performed with robust reproducibility and reliability, standardization of these assays is needed. To address this issue, the Pathology Committee of the International Association for the Study of Lung Cancer (IASLC) convened a panel of experts to publish this guide, which can help pathologists, laboratory scientists, and practicing physicians better understand the background, protocol, and interpretation of results of ALK testing in patients with advanced NSCLC.
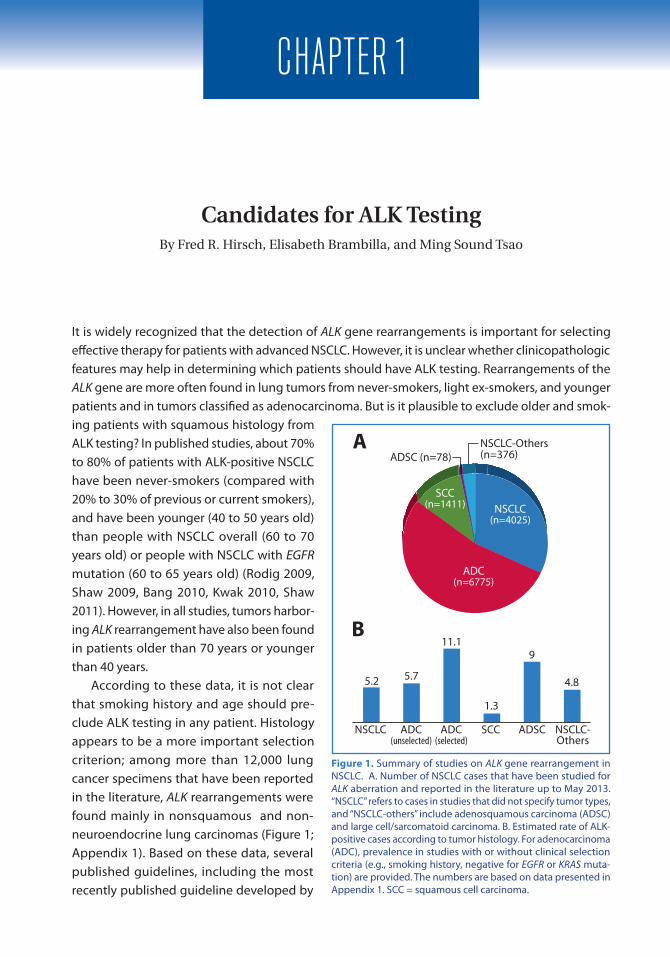
It is widely recognized that the detection of ALK gene rearrangements is important for selecting effective therapy for patients with advanced NSCLC. However, it is unclear whether clinicopathologic features may help in determining which patients should have ALK testing. Rearrangements of the ALK gene are more often found in lung tumors from never-smokers, light ex-smokers, and younger patients and in tumors classified as adenocarcinoma. But is it plausible to exclude older and smok-ing patients with squamous histology from ALK testing? In published studies, about 70% to 80% of patients with ALK-positive NSCLC have been never-smokers (compared with 20% to 30% of previous or current smokers), and have been younger (40 to 50 years old) than people with NSCLC overall (60 to 70 years old) or people with NSCLC with EGFR mutation (60 to 65 years old) (Rodig 2009, Shaw 2009, Bang 2010, Kwak 2010, Shaw 2011). However, in all studies, tumors harbor-ing ALK rearrangement have also been found in patients older than 70 years or younger than 40 years. According to these data, it is not clear that smoking history and age should pre-clude ALK testing in any patient. Histology appears to be a more important selection criterion; among more than 12,000 lung cancer specimens that have been reported in the literature, ALK rearrangements were found mainly in nonsquamous and non-neuroendocrine lung carcinomas (Figure 1; Appendix 1). Based on these data, several published guidelines, including the most recently published guideline developed by
Candidates for ALK TestingBy Fred R. Hirsch, Elisabeth Brambilla, and Ming Sound Tsao
ChApter 1
Figure 1. Summary of studies on ALK gene rearrangement in NSCLC. A. Number of NSCLC cases that have been studied for ALK aberration and reported in the literature up to May 2013. “NSCLC” refers to cases in studies that did not specify tumor types, and “NSCLC-others” include adenosquamous carcinoma (ADSC) and large cell/sarcomatoid carcinoma. B. Estimated rate of ALK-positive cases according to tumor histology. For adenocarcinoma (ADC), prevalence in studies with or without clinical selection criteria (e.g., smoking history, negative for EGFR or KRAS muta-tion) are provided. The numbers are based on data presented in Appendix 1. SCC = squamous cell carcinoma.
5.2 5.7
11.1
1.3
NSCLC ADC(unselected)
ADC(selected)
SCC ADSC NSCLC-Others
9
4.8
A
B
NSCLC-Others (n=376)ADSC (n=78)
NSCLC(n=4025)
ADC(n=6775)
SCC(n=1411)

12IASLC ATLAS OF ALK TESTING IN LUNG CANCER
the College of American Pathologists (CAP)/International Association for the Study of Lung Cancer (IASLC)/Association for Molecular Pathology (AMP), have recommended that ALK testing not be routinely performed on advanced NSCLC with squamous histology (Lindeman 2013). (See Appendix 2 and Chapter 9 for a complete discussion of guidelines for ALK testing.) However, ALK rearrangement has been detected in approximately 1.3% of more than 1,400 squamous cell lung carcinomas (Appendix 1) and in several case reports in which ALK rearrangement was verified by IHC (Alrifai 2013, An 2013, Ochi 2013). The discordance among studies of squamous cell lung carcinoma may be caused by the difficulties that still exist in diagnosing histologic subtypes of NSCLC. A lung cancer diagnosis is often made according to the examination of a small biopsy specimen or cytology samples, but histopathologic diagnoses made on small biopsy specimens are not always representative of the whole tumor. Reassessment of a squamous cell cancer diagnosis in such specimens with no evidence of EGFR and KRAS mutations demonstrated components of adenocarcinoma in 15 of 16 tumors (Rekhtman 2012). Therefore, the CAP/IASLC/AMP guideline suggests that ALK testing be done only for patients with adenocarcinomas and mixed lung cancers with an adenocarcinoma component in the setting of a fully excised lung cancer specimen. ALK testing is also recommended for limited specimens, such as biopsy and cytology specimens, where an adenocarcinoma component cannot be completely excluded. Screening for ALK with IHC may represent an ideal solution to the concerns of ALK testing in squamous cell lung carcinoma. Considering its low cost and high reproducibility, sensitivity, and specificity, IHC testing is conceivable for patients with squamous cell lung carcinoma, with FISH, which is more expensive, used to confirm positive results of IHC. For patients with localized or local-regional NSCLC, testing for ALK rearrangement is not currently associated with any immediate therapeutic consequences. However, ALK testing may be beneficial, as many of these patients will subsequently have disease recurrence, and the test results may save time and effort later on.

Testing for ALK gene rearrangements is one of several diagnostic procedures that may be required on a tissue sample containing lung cancer. In most patients, a single sampling procedure will gener-ate a relatively small amount of tissue that must then be used in the most efficient manner to allow for the most fully informed diagnosis possible. Two important points about tissue samples should be remembered: there is a possibility that a sample will not contain tumor tissue, and there is only one opportunity to fix and process the tissue. Thus, acquisition and processing are crucial steps in quality control in order to facilitate all the diagnostic procedures that may need to be done on a tissue sample.
Obtaining Tissue for DiagnosisIn most cases, ALK testing is performed on a small tissue specimen obtained by biopsy or on cytology samples taken from patients who have advanced disease. Less often, the whole tumor is avail-able from a patient who had surgical resection of early-stage disease and subsequent recurrence. Tissue sampling for diagnosis should be aimed at obtaining the largest yield of tumor in the safest and least invasive way possible (Thunnissen 2012d). Sampling may involve the primary tumor, intrathoracic metastatic disease, or extrathoracic metastases. Although discrepancies in ALK status between primary and metastatic disease have been reported (Kim 2013), data are insufficient to guide approaches to tissue acquisition. The primary tumor may be sampled at endoscopy (by endo-bronchial or transbronchial forceps biopsy, cryobiopsy, or fine-needle aspiration [FNA] ), or with a percutaneous, transthoracic approach (by core-needle biopsy or FNA. Intrathoracic metastatic disease is now routinely sampled using endobronchial ultrasound (EBUS) or transesophageal ultra-sound (EUS) guidance; pleural disease (either pleural biopsy or fluid cytology) is often a good source of diagnostic material. Distant extrathoracic metastatic disease can be sampled as appropriate to the site; in all cases, several imaging techniques are helpful in targeting the sampling to improve tumor yield (Rivera 2007). In most centers, surgical procedures may be used to obtain tissue if suf-ficient material was not obtained with image-guided procedures or when such procedures are not likely to be successful.
Tissue for ALK TestingBoth tissue biopsy and cytology samples may be used for ALK testing; the key issues are that the material must be processed and handled appropriately and the sample must contain sufficient
Sample Acquisition, Processing, and General Diagnostic Procedures By Keith M. Kerr, Ignacio Wistuba, and Yasushi Yatabe
ChApter 2
14IASLC ATLAS OF ALK TESTING IN LUNG CANCER
tumor cells (Thunnissen 2012b). The number of tumor cells required for IHC assessment of ALK protein remains undefined, but a minimum of 50 assessable tumor cells are required for FISH for the ALK gene rearrangement. Alternative approaches for cytology smear samples are available, but the most appropriate approach with cytology samples is usually the preparation of a cell block that allows sections to be prepared and treated in the same way as sections of tissue biopsy samples. In general, all of the tissue or cellular material received in the pathology laboratory should be processed. Surgical resection specimens are an exception, although, as a general rule, tumors with a diameter of 3 cm or less should be processed in toto. Large pleural effusions may also be processed in part; storage of fluid is recommended until all diagnostic procedures are complete.
Tissue ProcessingFixation by immersion, or where appropriate, by inflation, with 10% neutral buffered formalin is recommended. Pre-fixation in some alcohol-based fixatives may alter tissue antigenicity or DNA integrity. Acidic decalcifying solutions used on bone biopsy samples may interfere with IHC, frequently compromise FISH testing, and often degrade DNA, making mutation testing less reliable. Fixatives that are acidic (such as Bouin’s fluid) or based on hard-metal salts should also be avoided. In general, a period of fixation of more than 6 hours and less than 48 hours is recommended, especially when biomarker testing is to be done (for which DNA integrity is important) (Wolff 2007, Hunt 2007). Underfixation or overfixation may have deleterious effects on DNA and protein antigen epitopes (Werner 2000, Atkins 2004, Oyama 2007, Bussolati 2008, Eberhard 2008). One of the significant parts of this phase in tissue handling is the period of time beginning immediately after the sample is removed from the patient and placed in preservative. Most laboratories have neither control of nor data on how much time elapses between tissue removal and immersion in a fixative and its arrival in the laboratory. In addition, most tissue processing machines include a fixation step, which increases the fixation time. In practice, most laboratories will adjust their staining processes relevant to IHC and in situ hybridization (ISH) to allow for their own average fixation time. Determining the nature and duration of fixation is a greater challenge in laboratories that receive samples from many outside sources with widely differing fixation procedures.
Tissue Handling for Biomarker TestingMost biomarker investigations (IHC, ISH, or RNA/DNA studies) are performed during the initial diag-nostic workup. In these circumstances, freshly cut sections should be used for biomarker testing. Tissue stored on glass sections will deteriorate in a matter of days or weeks and certainly over months. Degradation depends on the storage conditions and most likely also on the specific biomarker (Atkins 2004). The stability of ALK protein on unstained cut sections has not yet been studied systematically. Therefore, similar to the case of HER2 testing in breast cancer, slides with tissue sections stored for longer than 6 weeks should not be used for IHC testing for ALK. If storage is necessary, the sections should be coated in wax or a similar medium to prevent air oxidation and the sections should be kept in cool, dry, dark conditions. Tissue in formalin-fixed paraffin-embedded (FFPE) blocks is less prone to deterioration, and recutting the tissue block as needed at a later time works well in most circumstances. Various strategies can help limit the number of times the block needs to be cut to provide material for initial morphologic assessment, IHC staining, and subsequent molecular analysis. For example, extra sections may be cut at the first cutting session, and although this strategy may

15ChApTER 2: SAmpLE ACqUISITION, pROCESSING, ANd GENERAL dIAGNOSTIC pROCEdURES
save the inevitable waste of precious material at each new cutting session, unnecessary cutting may be done and may raise issues related to the storage of cut sections (Figure 1).
The first step in the evaluation of a sample is to identify the presence or absence of malignancy. Depending on patient selection, choice of sampling technique, and operator skill, the rate of posi-tive tumor findings is generally high but may range from approximately 60% to more than 90% (Schreiber 2003). It is well recognized that, even when tumor is present in the sample, it may not be present in all tissue fragments and it generally comprises a small proportion of the tissue sub-mitted (Coghlin 2010). Once malignancy is confirmed, the next step is to exclude the possibility
Figure 1. Preparation of tissue sections during diagnostic workup. Current routine practice involves making additional sections for IHC assay and/or molecular testing after the initial sectioning and hematoxylin and eosin (H & E) staining for histologic diagnosis. Multiple sequential sectioning may deplete the tumor volume each time block trimming is necessary. In the era of molecularly targeted therapies, the preparation of additional unstained sections for possible IHC analysis and/or molecular testing may significantly reduce the amount of tissue sample lost and improve turnaround time.
Common procedure to date
The procedure in era of molecularly targeted drugs
H & E staining for histologic diagnosis
For IHC
For molecular testing
H & E staining for histologic diagnosis
For IHC
For molecular testing
Repeat sectioning
Repeat sectioning

16IASLC ATLAS OF ALK TESTING IN LUNG CANCER
of nonepithelial malignancy (such as lymphoma or sarcoma) and/or the possibility that a cancer, especially adenocarcinoma, is not lung metastasis from another organ (Kerr 2013b). Most often, this step can be done easily, based on the evaluation of adequate clinical and radiographic information accompanying the sample and the basic H & E-based morphologic assessment. A lack of clinical information, however, may lead to unnecessary ancillary IHC testing on the sample in an attempt to exclude possible extrathoracic sources for an adenocarcinoma, which may leave insufficient material for molecular testing. Assuming the tumor is primary lung cancer, the next step is to distinguish small cell lung cancer (SCLC) from other types, as advanced SCLC is treated differently from NSCLC. This discrimination can usually be made with high accuracy on the basis of morphologic characteristics (Burnett 1994), but IHC may be required. Most cases that are not SCLC can be accurately and consistently classified morphologically as squamous cell carcinoma, adenocarcinoma or, rarely, another NSCLC type. In 25% to 40% of cases, however, depending on the sample type and case mix, morphologic features are not adequate for accurate and consistent NSCLC subtype classification; such cases should be initially designated NSCLC not otherwise specified (NOS) (Chuang 1984). Diagnostic IHC can then be used to predict the likely NSCLC subtype (Loo 2010, Travis 2011, Travis 2013). This approach, using a limited IHC panel, can reduce the proportion of NSCLC-NOS cases to less than 10% and predict the NSCLC subtype in most NOS cases with an accuracy of more than 80% (Loo 2010). Cases reported in conjunction with this use of IHC should be described by the recommended terminology (e.g., NSCLC, favor adenocarcinoma) in a morphologically undifferentiated case, where IHC predicts adenocarcinoma (Travis 2011, Kerr 2013a).
ConclusionThe identification of patients with therapeutically targetable molecular drivers in their tumors is now a standard of care. The need for extra molecular testing, beyond that required for initial morphologic diagnosis and refinement of tumor classification by IHC when necessary, makes the acquisition, handling, processing, and judicious use of diagnostic tumor tissue of crucial importance. Every effort must be made to ensure that a sufficient amount of tumor tissue is available for a subsequent diagnostic step. However, lack of sufficient tissue may be inevitable in some cases and will have the greatest impact on molecular tests that follow the tumor diagnosis. When the amount of tissue is insufficient, repeat biopsy is increasingly being done.
ChApter 3
FISH with a break-apart probe set was originally developed for detecting gene fusions created by interchromosomal translocations. Break-apart FISH is a reliable diagnostic method in surgical pathol-ogy because it is easily applicable to FFPE specimens even when the exact fusion partners are not known. FISH with break-apart probes for ALK has been successfully incorporated into diagnostic practice for lymphomas and mesenchymal tumors, and the discovery of ALK rearrangement in a rare subset of NSCLCs broadened the application of break-apart FISH (Soda 2007). However, in the latter setting, FISH has been associated with unexpected challenges, primarily because the common fusion variants occur between ALK (2p23.2) and the closely situated gene EML4 (2p21) through intrachromosomal inversions; only rarely is ALK fused with other genes through intrachromosomal translocations. Thus, break-apart FISH for the diagnosis of lung cancers with ALK rearrangement must be performed with special attention to technical details and interpretation of the results.
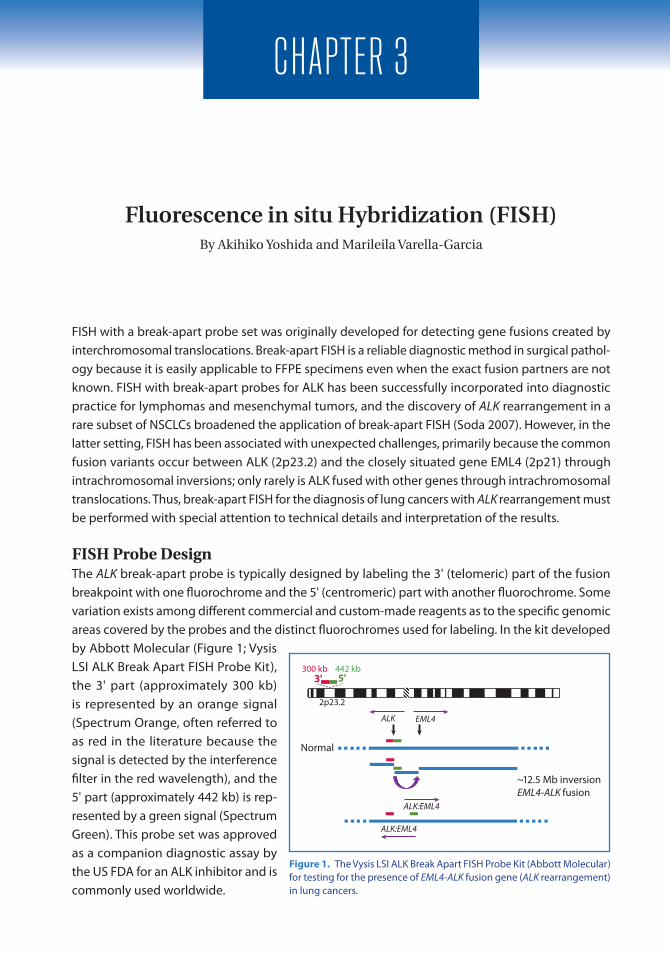
FISH Probe DesignThe ALK break-apart probe is typically designed by labeling the 3' (telomeric) part of the fusion breakpoint with one fluorochrome and the 5' (centromeric) part with another fluorochrome. Some variation exists among different commercial and custom-made reagents as to the specific genomic areas covered by the probes and the distinct fluorochromes used for labeling. In the kit developed by Abbott Molecular (Figure 1; Vysis LSI ALK Break Apart FISH Probe Kit), the 3' part (approximately 300 kb) is represented by an orange signal (Spectrum Orange, often referred to as red in the literature because the signal is detected by the interference filter in the red wavelength), and the 5' part (approximately 442 kb) is rep-resented by a green signal (Spectrum green). This probe set was approved as a companion diagnostic assay by the US FDA for an ALK inhibitor and is commonly used worldwide.
Fluorescence in situ Hybridization (FISH)By Akihiko Yoshida and Marileila Varella-Garcia
Figure 1. The Vysis LSI ALK Break Apart FISH Probe Kit (Abbott Molecular) for testing for the presence of EML4-ALK fusion gene (ALK rearrangement) in lung cancers.
2p23.2
300 kb 442 kb5'3'
ALK EML4
ALK:EML4
ALK:EML4
~12.5 Mb inversionEML4-ALK fusion
Normal
18IASLC ATLAS OF ALK TESTING IN LUNG CANCER
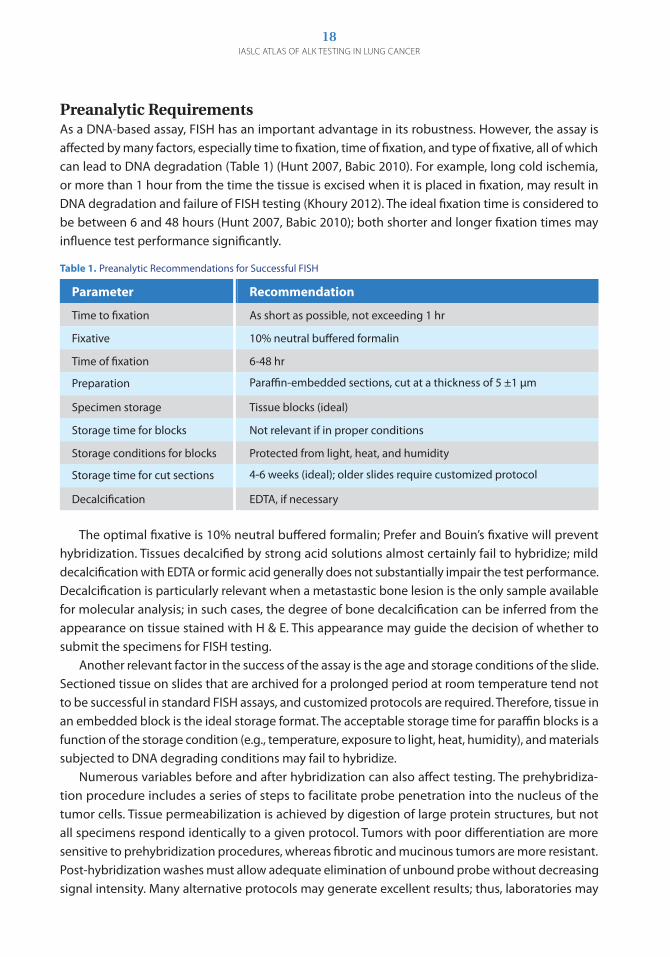
Preanalytic RequirementsAs a DNA-based assay, FISH has an important advantage in its robustness. However, the assay is affected by many factors, especially time to fixation, time of fixation, and type of fixative, all of which can lead to DNA degradation (Table 1) (Hunt 2007, Babic 2010). For example, long cold ischemia, or more than 1 hour from the time the tissue is excised when it is placed in fixation, may result in DNA degradation and failure of FISH testing (Khoury 2012). The ideal fixation time is considered to be between 6 and 48 hours (Hunt 2007, Babic 2010); both shorter and longer fixation times may influence test performance significantly.
The optimal fixative is 10% neutral buffered formalin; Prefer and Bouin’s fixative will prevent hybridization. Tissues decalcified by strong acid solutions almost certainly fail to hybridize; mild decalcification with EDTA or formic acid generally does not substantially impair the test performance. Decalcification is particularly relevant when a metastastic bone lesion is the only sample available for molecular analysis; in such cases, the degree of bone decalcification can be inferred from the appearance on tissue stained with H & E. This appearance may guide the decision of whether to submit the specimens for FISH testing. Another relevant factor in the success of the assay is the age and storage conditions of the slide. Sectioned tissue on slides that are archived for a prolonged period at room temperature tend not to be successful in standard FISH assays, and customized protocols are required. Therefore, tissue in an embedded block is the ideal storage format. The acceptable storage time for paraffin blocks is a function of the storage condition (e.g., temperature, exposure to light, heat, humidity), and materials subjected to DNA degrading conditions may fail to hybridize. Numerous variables before and after hybridization can also affect testing. The prehybridiza-tion procedure includes a series of steps to facilitate probe penetration into the nucleus of the tumor cells. Tissue permeabilization is achieved by digestion of large protein structures, but not all specimens respond identically to a given protocol. Tumors with poor differentiation are more sensitive to prehybridization procedures, whereas fibrotic and mucinous tumors are more resistant. Post-hybridization washes must allow adequate elimination of unbound probe without decreasing signal intensity. Many alternative protocols may generate excellent results; thus, laboratories may
Parameter Recommendation
Time to fixation As short as possible, not exceeding 1 hr
Fixative 10% neutral buffered formalin
Time of fixation 6-48 hr
Preparation Paraffin-embedded sections, cut at a thickness of 5 ±1 μm
Specimen storage Tissue blocks (ideal)
Storage time for blocks Not relevant if in proper conditions
Storage conditions for blocks Protected from light, heat, and humidity
Storage time for cut sections 4-6 weeks (ideal); older slides require customized protocol
Decalcification EDTA, if necessary
Table 1. Preanalytic Recommendations for Successful FISH

19ChApTER 3: FLUORESCENCE IN SITU hybRIdIzATION
choose any of these protocols, as long as conditions are properly adjusted to the characteristics of the specimen.
Quality Assessment of the Hybridized Specimen and Selection of Scorable CellsIt is essential that the quality of tissue morphology and signal intensity be rigorously assessed before a specimen is accepted for analysis. Specimens are optimal for analyses when they exhibit excel-lent morphology and signal intensity with very low background noise (Figures 2 and 3). Specimens with evidence of chromatin overdigestion or poor probe penetration are not acceptable and must be retested after troubleshoot-ing technical conditions. For example, specimens are not acceptable when the pretreatment of tissue is insufficient or excessive (Figure 4) or when technical sectioning artifacts that generate over-lapped nuclei with stringy signals make it impossible to measure the separation between red and green (Figure 5). ALK rearrangement appears homo-geneously distributed in the tumor, reflecting its critical oncogenic role (Camidge 2010). Therefore, it is not necessary to select a specific tumor area based on morphology or immuno-profile, and scoring in several different tumor areas is recommended. Scoring must be done on the well-preserved nonoverlapping tumor cells that have
Figure 2. Microscopic fields of ALK-negative lung tumors.
Figure 3. Microscopic fields of ALK-positive lung tumors, showing predominantly the split 3'-5' pattern (3A-3C) and the isolated 3' pattern (3D, 3E).
A B C
D
E
A
B C

20IASLC ATLAS OF ALK TESTING IN LUNG CANCER
at least one copy each of the 5’ and 3’ signals. Because lung cancers tend to assume a wide range of growth patterns, and because tumor cells may closely intermingle with non-tumor tissue elements (e.g., alveolar macrophages and lymphocytes), the accurate identification of tumor cells may be difficult in a dark field. It is advisable to always refer to a serially cut, H & E-stained tissue slide for appropriate morpho-logic adjustment.
Cell Classification: Signal PatternsIn concept, the genomic areas homologous to the 5' and 3' probes are molecularly very close and these signals are seen as fused, touching, or adjacent in normal cells. In contrast, when the EML4-ALK fusion gene is present, the 5' ALK green signal becomes far removed from the 3' ALK red signal (by approximately 12.5 Mb), and the signals are seen as
being split. In reality, the 3' and 5' signals may be seen as far apart from or as close to each other in normal host cells because of various degrees of condensation and three-dimensional arrangement of the chromatin. Similarly, because of the proximity of EML4 and ALK, the split can be so narrow that the signals may seem fused in ALK rearrangement (Figure 6). Furthermore, this genomic region seems to be highly unstable, and the homologous regions to one of the probes can be lost, with the corresponding signal being missing. As a result, each tumor cell may display a variety of combina-tions of co-localized 5'-3' ALK signals and isolated 5' or 3' ALK signals. Despite this diversity in signal profile, cells can be classified into one of the following four pat-terns based on each signal number and location.
Fused (normal) pattern (Figure 7A). A cell is interpreted as having a normal pattern (ALK negative) when the 5' and 3' signals are fused (Figure 2). Any separation of 5' and 3' signals by a distance of less than two signal diameters should be classified as fused. The number of fused 5'-3' signals per tumor
Figure 4. Specimens unacceptable for analyses because of tissue overdigestion (4A) or tissue underdigestion (4B).
Figure 5. Specimens unacceptable for analyses because of high background noise (5A) and stringy signals (5B).
A B
A B

21ChApTER 3: FLUORESCENCE IN SITU hybRIdIzATION
nucleus is not relevant for pattern classification.
Split (positive) pattern (Figure 7B). A cell is inter-preted as having a split pattern (ALK positive) when the 5' and 3' signals are separated, regardless of the number of actual isolated signals (Figure 3). The sepa-ration between the 5' and 3' signals must be two or more times the diameter of the largest signal (Camidge 2010). The number of iso-lated 5' and 3' signals does not need to be equal; for example, a cell with two copies of isolated 5' signal and three copies of isolated 3' signals is classified as split. The number of accompanying fused 5'-3' signals in the cell is not relevant for pattern classification. Isolated 3' (posi-tive) pattern (Figure 7C). A cell is interpreted as having an isolated 3' pattern when isolated 3' signals are present with no isolated 5' sig-nals. When a cell has both isolated 3' and 5' signals, with more 3' signals than 5' signals, the correct classification is the split pattern, not isolated 3'. The number of accompany-ing fused signals is not relevant for pattern classification.
Isolated 5' (negative) pattern (Figure 7D). A cell is interpreted as having an iso-lated 5' pattern when isolated 5' signals are present with no isolated 3' signals. When a cell has both isolated 3' and 5' signals, with more 5' signals than 3' signals, the correct classification is the split pattern, not isolated 5'. The number of accompany-ing fused signals is not relevant for pattern classification.
Note: The criteria for the split pattern are pri-marily based on testing of FFPE tumor sections
Figure 6. Signal patterns in lung tumor nuclei hybridized with ALK break-apart FISH.
Nonrearranged tumors:Rearrangement-positive cell rate<15% of cells
Rearranged tumors:Rearrangement-positive cell rate≥15% of cells
SIGNAL CLASSIFICATION
SPECIMEN CLASSIFICATION
Red and green separated by <2 signal diameters
Red and green separated by ≥2 signal diameters
Patterns observed in native ALK Patterns observed in split 3'-5' ALK
Classi�ed as positive
Classi�ed as negative
Red and green separated by ≥2 signal diametersClassi�ed as positive
Red and green separated by <2 signal diametersClassi�ed as negative
Patterns Examples
A.Fused
B.Split
C.Isolated
3' ALK
D.Isolated
5' ALK
Figure 7. Tumor cell classification based on the ALK signal pattern on FISH.

22IASLC ATLAS OF ALK TESTING IN LUNG CANCER
with the Vysis LSI ALK Break Apart FISH Probe Kit, and the criteria should be validated when a different analytic reagent or biologic specimen is used. The probe size may differ among probe designs, and a larger probe size results in both a larger signal size and a shorter distance required for the definition of a split.
ScoringA minimum of 50 tumor cells is needed when there is one scorer and a minimum of 100 tumor cells is needed when there are two scorers (see more information in the “Cutoff Value” section). Specimens with fewer assessable cells are not suitable for FISH analysis (Camidge 2010). The signal pattern for each tumor cell should be recorded on a scoring worksheet (Figure 8). Scoring is likely to be more accurate when it is done while viewing the tissue under a micro-scope with single (red and green) and dual interference filters. Image-based scoring has limitations and the image must represent all section depths in order to avoid false interpre-tation of isolated signals (Figure 9). Copy number gain of native ALK is common in NSCLC (Figure 10) and there is no indication that it is associated with protein overexpression. At this time, we do not recom-mend that ALK copy number be routinely included as part of scoring.
Note: The signal size in cap-tured images tends to be slightly larger than that seen on actual examination under fluorescent microscopy. When scoring is done on captured images, the distance between signals may be underestimated, which may compromise the results of analysis. Another pitfall of using images for scoring is that image capturing often consolidates multiple focus levels into one plane, and as a result, a vertically split signal along the z-axis of the tissue plane may be indistinguishable from a fused signal.
Figure 8. An example of a worksheet for scoring cells.
Summary of Scoring:Total # of cells scored: 50Total # of cells with fused pattern: 19Total # of cells with split pattern: 22Total # of cells with isolated 3' pattern: 5Total # of cells with isolated 5' pattern: 4Total # of cells with rearrangement-positive patterns: 22+5=27Rearrangement-positive cell rate: 27÷50 x100=54%
Cell Fusedsignal
5'signal
3’signal Pattern
Cell 1 2 0 0 Fused
Cell 2 2 1 1 Split
Cell 3 2 0 1 Isolated 3'
Cell 4 1 1 0 Isolated 5'
Cell 5 0 1 2 Split
Cell 6 1 0 0 Fused
Cell 50 2 0 0 Fused
Figure 9. Image-based analysis is difficult if z-stacking (consolidation of multiple focus levels into one plane) does not represent the whole depth of the section.
A BNo z-stacking16 planes at 0.4 µm= 6.4 µm z-stacking

23ChApTER 3: FLUORESCENCE IN SITU hybRIdIzATION
Specimen Classification: Rate of Rearrangement-Positive Cells The rate of rearrangement-positive cells is defined as follows:Rearrangement-positive cell rate (%) = [(number of cells with split pattern + number of cells with isolated 3' pattern) /Total number of cells evaluated] × 100
Note: Because the kinase domain of ALK tyrosine kinase is encoded by the 3' part of the gene, it is the unpaired 3' signal that indicates the oncologically relevant fusion gene, whereas the unpaired 5' signal represents a likely nonfunctional reciprocal fusion product. Therefore, cells with an isolated 3' pattern are categorized as rearrangement-positive cells along with those with a split pattern. Cells with an isolated 5' pattern should not be interpreted as rearrangement-positive cells. Disregarding the isolated 3' pattern and limiting the definition of rearrangement to the split pattern reduces the sensitivity of the ALK FISH assay to 60% to 70% (Yoshida 2011a, Paik 2011).
Cutoff ValueBecause the EML4-ALK fusion gene is typically created by a small intrachromosomal inversion involv-ing two genes located in close proximity, the distance between the split signals representing an ALK rearrangement is typically narrow when the break-apart FISH assay is used. Because of the degree of chromatin condensation in the cells or its physical distribution, narrow splits are sometimes technically indistinguishable from fused signals (Figure 6), which can cause the rate of rearrange-ment-positive cells in ALK-rearranged NSCLCs to be low (40% to 70%) (Perner 2008, Camidge 2010, Camidge 2012b). In addition, NSCLCs without ALK rearrangement may have rearrangement-positive patterns (i.e., split pattern or isolated 3' pattern) in a fraction of cells (Perner 2008, Camidge 2010, Yoshida 2011a), likely because of truncation artifact or perhaps a stochastic genomic alteration that does not indicate a specific fusion gene (Figure 6). As a result, the distribution of rearrange-ment-positive cell rates in NSCLC is continuous, and the difference between ALK-rearranged and ALK-wild-type NSCLCs is a statistical matter. Therefore, careful quantitative assessment is mandatory for optimal test performance. A cutoff value of 15% has been set to allow for the best separation between ALK-rearranged (ALK positive) and ALK-wild-type (ALK negative) NSCLCs (Camidge 2010, Kwak 2010, Yoshida 2011a).
Figure 10. Copy number gain of native ALK signals is commonly increased in lung cancer specimens, with levels ranging from low (10A) to very high (10C). A cluster of numerous copies suggests gene amplification (10D, 10E). Copy number gain should not be interpreted as a positive result.
A B C
D
E

24IASLC ATLAS OF ALK TESTING IN LUNG CANCER
To minimize technical bias, we recommend a two-step assessment strategy with two independent scorers (Figure 11). The first scorer scores 50 tumor cells. A rate of rearrangement-positive cells less than 10% (i.e., rearrangement in fewer than five of the 50 cells) is considered negative; a rate greater than 50% (i.e., more than 25 of 50 cells) is considered positive; and a rate of 10% to 50% (i.e., 5 to 25 of 50 cells) is considered equivocal and additional scoring should be done. In that case, a second inde-pendent scorer scores an additional 50 tumor cells, and a final rate of rearrangement-positive cells is calculated on the sum of the first and second scores. If the final rate is 15% or more, the specimen is interpreted as positive for ALK gene rearrangement; if the rate is less than 15%, the specimen is interpreted as negative for ALK gene rearrangement.
Note: The 15% cutoff is primarily based on testing with the Vysis LSI ALK Break Apart FISH Probe Kit (Abbott Molecular) and should be validated when a different reagent is used.
Laboratory ValidationThe ALK FISH assay should be properly validated in the laboratory before testing is offered in a clinical setting (Halling 2012, Saxe 2012). The accuracy of the results—that is, the degree to which the assay discriminates between normal (ALK negative) and abnormal (ALK positive) —should be compared with the accuracy at another laboratory where the validated assay is being performed properly and/or compared with the accuracy for a previously validated method in the same labo-ratory. The precision or reproducibility of results should be verified according to the degree of agreement between measurements conducted on the same specimen by different technologists and/or at different times, and the entire analytic process should be verified. Verification of accuracy and precision should be repeated periodically. Moreover, the analytic sensitivity and specificity of the assay should be verified in specimens with known genotype. ALK wild-type NSCLC and benign tissue must be evaluated to assess the distance in a true-positive split signal (a distance of at least two times the signal diameter). These tasks are simpler when commercial reagents are used and require higher level of details when laboratory-developed reagents are used.
ChallengesALK break-apart FISH has been associated with four primary challenges: false-negative and false-positive results, atypical FISH signal profiles, borderline rates of rearrangement-positive cells, and the need for repeat testing.
Figure 11. Recommended scoring algorithm for ALK FISH.
1st Reader-50 tumor cells
10%-50% Positive
Equivocal
2nd Reader-50 tumor cells
1st + 2nd Readers-100 tumor cells
<10% Positive>50% Positive
<15% Positive≥15% Positive
Specimen is positive for ALK rearrangement
Specimen is negative for ALK rearrangement

25ChApTER 3: FLUORESCENCE IN SITU hybRIdIzATION
False-Negative and False-Positive ResultsAlthough break-apart FISH has been used as the criterion standard for diagnosing ALK-positive lung cancer, it remains difficult to evaluate the true sensitivity and specificity of the test. Most discor-dance between FISH and other modalities arises because of technical reasons. However, FISH may generate true false-positive or false-negative results, which can have a significant impact on disease management. False-positive results are particularly difficult to demonstrate, mainly because of the well-acknowledged limited sensitivity of RT-PCR and IHC. Nonetheless, there is some clinical sugges-tion that a diagnosis based on FISH results predicts response to treatment with an ALK inhibitor less accurately than a combination of FISH, IHC, and RT-PCR, and clinically discordant cases may rarely include true false-positive FISH results (Chihara 2011). Novel technologies such as genome-wide massive parallel sequencing may provide opportunities to demonstrate the existence of false-pos-itive FISH results. In contrast, a few cases of false-negative FISH results are well documented in the literature (Yoshida 2011a, Murakami 2012, Peled 2012). In such cases, atypical FISH signal patterns may or may not be seen. The genomic mechanisms underlying false-negative FISH results have not been fully clarified, but it is conceivable that complex gene rearrangements and cryptic insertions may be contributing factors.
Atypical Signal ProfileThere are rare instances (approximately 6% of cases, (Camidge 2013) when FISH produces atypical signal profiles that are both recurrent and sufficiently distinct as to be recognizable. At least some such patterns are known to be associated with false-negative results. One such example is when most of the tumor cells harbor an isolated 5' predominant pattern, with only a few cells having a split or an isolated 3' pattern (“5' predominant pattern,” Figure 12). By conventional enumeration rule, the isolated 5' pattern should be classified as ALK negative and these cases tend to be overlooked as nega-tive for ALK rearrangement. Nevertheless, cases with this signal pattern have been reported to carry an EML4-ALK fusion transcript when the results were con-firmed by RT-PCR (Yoshida 2011a). Another atypical FISH signal is a so-called red-doublet pattern, in which a pair of 3' signals fuses with a 5' signal (Figure 13A) (Peled 2012). ALK-positive NSCLCs with a red-doublet pattern may be misinterpreted as negative for ALK rearrangement because such a signal cluster may mimic a conventional fused signal. Sometimes, three or more copies of 3' signals may cluster and fuse with a 5' signal (referred to as a red-triplet pattern and so on, according to the number of copies; Figure 13B, 13C). In yet other
Figure 12. An atypical pattern in lung cancer with break-apart FISH is the isolated 5' predominant pattern. Arrows indicate single green signals (5' ALK).
A B

26IASLC ATLAS OF ALK TESTING IN LUNG CANCER
rare instances, most of the tumor cells in ALK-positive NSCLCs may exhibit only isolated 3' signals without normal copies of ALK (Figure 13D). Cells with such a pattern are regarded as nonevaluable by con-ventional scoring rules because of the possi-bility of a hybridization failure of the 5' probe, and ALK-positive cancers with such a pattern may be overlooked. Although it is not yet completely clear how consistently such atypical signal patterns predict fusion status, these patterns should at least raise a high index of suspicion and prompt testing with other diagnostic modalities (e.g., RT-PCR, IHC). Future studies may identify other atypical signal profiles that are associated with false-negative FISH results.
Borderline Rates of Rearrangement-Positive Cells In approximately 8% of NSCLC cases, the rate of rearrangement-positive cells falls within the range of 10% to 20% (Camidge 2013). Although the currently accepted cutoff of 15% technically classi-fies such cases as either positive or negative for ALK rearrangement, our experience is limited as to whether such a borderline prevalence of rearrangement signals by FISH accurately represents pres-ence of the fusion gene. We recommend that cells be carefully counted again on such specimens, with particular attention paid to the morphologic differentiation between tumor and nontumor cells. Including nontumor cells in the count dilutes the rate of rearrangement-positive cells. The recommended two-step scoring algorithm should minimize these technical errors. Similar atten-tion should be paid to the vertically split signals along the z-axis of the tissue plane, which could be mistaken as a fused signal. This latter pitfall is particularly relevant in a laboratory in which the evaluation is performed on the captured digital images that consolidate multiple focus levels to produce one image (z-stacking). These borderline cases may also harbor atypical signal profiles, as described earlier. Specifically, a red-doublet pattern may initially stand out as a borderline rate of rearrangement-positive cells. Analysis using a single-color filter may facilitate the identification of closely apposed signals that may be overlooked by a dual-color (red and green) or a triple-color (blue, red, and green) filter. If the rate of rearrangement-positive cells is still borderline on careful reassessment, the final interpretation may be either positive or negative using the 15% cutoff, with the addition of a cautionary note to consider other diagnostic modalities, such as IHC or RT-PCR, for further workup.
Need for Repeat TestingThe findings of a few reports have suggested that the ALK status, including ALK copy number gain over the clinical course, can change, particularly after treatment with an ALK inhibitor (Doebele
Figure 13. Atypical patterns seen in lung tumors with break-apart FISH. 13A: 3'-5-3' (red-doublet pattern); 13B and 13C: 3'-3'-5'-3' (red-triplet pattern); 13D: Isolated 3’ signals, mostly without normal ALK signals). Arrows indicate ALK rearrangement.
A
B
C D

27ChApTER 3: FLUORESCENCE IN SITU hybRIdIzATION
2012). Although the exact incidence and mechanism of such change are not yet clear, repeat test-ing should be considered when the tumor demonstrates acquired resistance following treatment with an ALK inhibitor, and a new therapeutic regimen must be selected. However, the data are still immature, and further research and validation are needed.
Chromogenic in situ Hybridization (CISH)FISH is not without limitations, which include the need for highly specialized equipment, inevitable signal fading after long-term storage of tissue, and dark-field examination that may obscure tissue architecture and cytomorphology. The latter factor can be particularly problematic because lung cancers often show complex growth patterns intimately admixed with nontumor cells; differenti-ating tumor cells from nontumor elements may be difficult without architectural or cytoplasmic information. CISH has been developed to overcome these disadvantages of FISH. With CISH, each hybridization probe is visualized by chromogens rather than fluorochromes (Figure 14). CISH allows for detection of specific genetic alterations while preserving tumor architecture and cytomorphol-ogy under the routine bright-field microscope. The utility of ALK break-apart CISH for lung cancer diagnosis has been evaluated, and all studies have demonstrated excellent concordance with the results of FISH and/or RT-PCR (Kim 2011, Yoshida 2011a, Nitta 2013, Schildhaus 2013). CISH still must be validated for use in detecting ALK rearrangement in lung cancers, and different cutoffs (15% and 20%) and scoring criteria (1-diameter gap versus 2-diameter gap) have been used in the few reported studies.
ConclusionBreak-apart FISH is a reliable technique for the diagnosis of ALK-rearranged NSCLCs and has been accepted as the criterion standard to select patients for treatment with an ALK inhibitor. However, FISH testing heavily depends on careful preparation and interpretation with strict adherence to
Target DNA
Probe
SecondaryantibodyPrimary
antibody
Enzyme
SubstrateChromogenicreaction
Figure 14. Principles of CISH; left. Individual probes are labeled with different haptens that are visualized by antibody reac-tions similar to that in IHC. ALK break-apart CISH is applied to ALK-positive tumors (right). Black dots represents normal ALK gene, and rearranged ALK genes are seen as split single red or blue signals.

28IASLC ATLAS OF ALK TESTING IN LUNG CANCER
guidelines. Furthermore, FISH may rarely produce equivocal or even erroneous results. As any other clinical test, ALK break-apart FISH has unique strengths and limitations and should be used within an appropriate diagnostic context. It is also strongly recommended that each laboratory perform internal validation studies using known controls before this method is introduced as a routine test. In addition, laboratories should participate in periodic slide exchange programs with other accredited clinical laboratories or in proficiency testing surveys provided by approved vendors.
ChApter 4
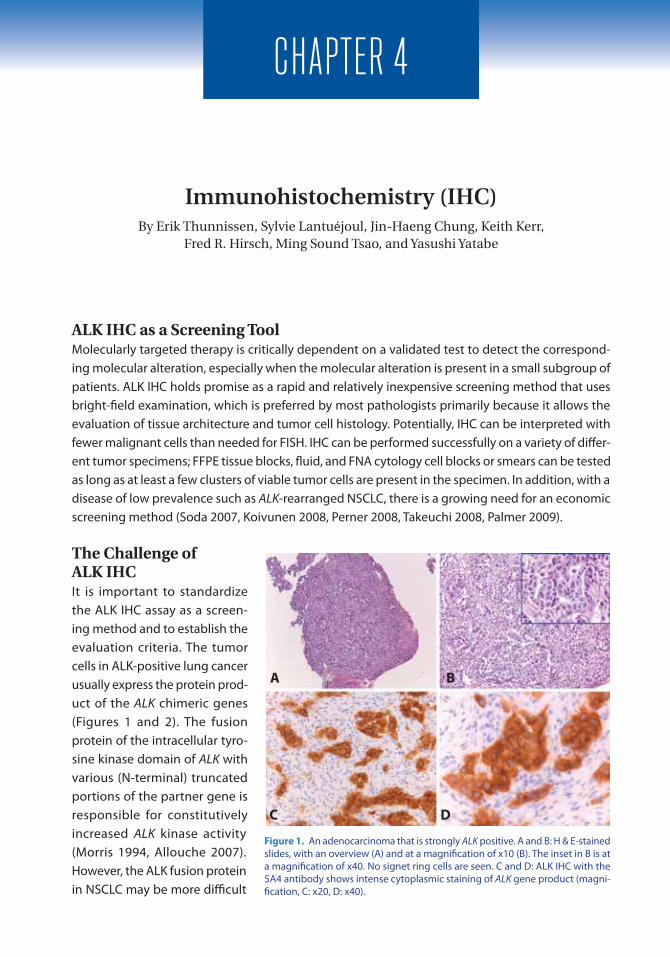
ALK IHC as a Screening ToolMolecularly targeted therapy is critically dependent on a validated test to detect the correspond-ing molecular alteration, especially when the molecular alteration is present in a small subgroup of patients. ALK IHC holds promise as a rapid and relatively inexpensive screening method that uses bright-field examination, which is preferred by most pathologists primarily because it allows the evaluation of tissue architecture and tumor cell histology. Potentially, IHC can be interpreted with fewer malignant cells than needed for FISH. IHC can be performed successfully on a variety of differ-ent tumor specimens; FFPE tissue blocks, fluid, and FNA cytology cell blocks or smears can be tested as long as at least a few clusters of viable tumor cells are present in the specimen. In addition, with a disease of low prevalence such as ALK-rearranged NSCLC, there is a growing need for an economic screening method (Soda 2007, Koivunen 2008, Perner 2008, Takeuchi 2008, Palmer 2009).
The Challenge of ALK IHCIt is important to standardize the ALK IHC assay as a screen-ing method and to establish the evaluation criteria. The tumor cells in ALK-positive lung cancer usually express the protein prod-uct of the ALK chimeric genes (Figures 1 and 2). The fusion protein of the intracellular tyro-sine kinase domain of ALK with various (N-terminal) truncated portions of the partner gene is responsible for constitutively increased ALK kinase activity (Morris 1994, Allouche 2007). However, the ALK fusion protein in NSCLC may be more difficult
Immunohistochemistry (IHC) By Erik Thunnissen, Sylvie Lantuéjoul, Jin-Haeng Chung, Keith Kerr,
Fred R. Hirsch, Ming Sound Tsao, and Yasushi Yatabe
Figure 1. An adenocarcinoma that is strongly ALK positive. A and B: H & E-stained slides, with an overview (A) and at a magnification of x10 (B). The inset in B is at a magnification of x40. No signet ring cells are seen. C and D: ALK IHC with the 5A4 antibody shows intense cytoplasmic staining of ALK gene product (magni-fication, C: x20, D: x40).
A B
C D

30IASLC ATLAS OF ALK TESTING IN LUNG CANCER
to detect with the ALK1 antibody, which is used to diagnose anaplastic large cell lymphoma (ALCL), as the protein expression is generally lower in NSCLC (Mino-Kenudson 2010). To overcome this issue, several technical steps have been introduced, including antigen retrieval, use of a primary antibody with higher affinity and at a sufficiently high concentration, strong signal amplification steps (e.g., with a tyramide cascade and intercalation of an antibody-enhanced polymer), and the development of novel antibodies (Table 1).
Another important aspect of ALK IHC testing of lung cancer specimens is the lack of an internal positive control for immunostaining, which makes it difficult to judge whether a negative IHC result is truly negative for expression of the ALK fusion protein. However, because the normal lung tissue does not express ALK, diffuse expression of ALK protein in lung cancer cells is always associated with expression of the aberrant ALK fusion protein (Takamochi 2013, Takeuchi 2013). FFPE cell blocks with ALK-rearranged cell lines (H3122-variant 1 and H2228-variant 3) may be used to control the optimal staining condition, but differences between tissue sections and cell line-cell blocks should be considered, particularly with a lower epitope concentration of ALK IHC (Figure 3).
Fixation and Sectioning The preanalytic steps for ALK IHC are the same as those for other IHC procedures. Regardless of origin, diagnostic biopsies or surgical specimens should immediately be fixed in an adequate amount (ratio
Table 1. Commercially Available Antibodies for IHC to Detect ALK Protein Expression
Clone Clone Type Isotype Immunogen
ALK1 Mouse monoclonal Igg3, kappa Amino acids 1359–1460 of the full length human ALK protein, corresponding to amino acids 419–520 of the chimeric NPM-ALK protein
5A4 Mouse monoclonal Igg1 C-terminus of the NPM-ALK transcript (419-520 amino acids)
D5F3 Rabbit monoclonal Not available Carboxyl terminus of human ALK
Anti-ALK Rabbit monoclonal Igg Recombinant protein representing amino acids 426-528 of human ALK
Figure 2. An adenocarcinoma that is strongly ALK positive. A: H & E-stained slide. B: ALK IHC with the D5F3 antibody and tyramide amplification shows intense cytoplasmic staining of ALK gene product (magnification, x40).
A B

31 ChApTER 4: ImmUNOhISTOChEmISTRy
of 10 times more than the volume of the specimen) of 10% neutral buffered formalin and embed-ded in paraffin ( FFPE). Fixation must be done as soon as possi-ble to avoid cold ischemia effects. Fixation times of less than 6 hours are not recommended because conventional staining as well as IHC can be adversely affected. Antigen preservation for IHC is epitope dependent, and some epitopes may not be hampered by fixation times of as long as 120 hours. For practical purposes, a fixation interval of 6 to 48 hours is recommended for all specimens. After paraffin embedding, the tumor tissue is stable and pre-served against oxidative damages or other degenerative effects. However, once 3 to 4-µm thick slides are cut from the FFPE block, the storage time of these sections mounted on glass microscope slides at room temperature is limited to a maximum of 6 weeks. For storage at colder temperatures, the slides remain adequate for a longer period of time. However, slides of tissue sections that were prepared more than 6 weeks earlier should be interpreted very carefully, as they may present false-negative results.
Immunostaining For the analytic procedure, i.e., the actual ALK IHC testing, several issues need to be controlled and optimized: epitope retrieval, type and concentration of the antibody, incubation time, incubation temperature, and amplification. A single uniform technique, or comparator, has not been evaluated in the studies on ALK IHC in NSCLC. Instead, the type or source of antibodies, the process of antigen retrieval and antibody detection, and the amplification techniques have varied substantially (Table 2). When different antibodies were compared head-to-head, D5F3 (Cell Signaling Technology) and 5A4 (Novocastra) with the ADVANCE system (Dako) appeared to be both more sensitive and more specific than the ALK1 antibody (Dako) (Figure 4) (Conklin 2013). (See Chapter 6 for a discussion of various platforms.) Commercial ALK IHC kits are currently in development and validation. The sensitivity for detecting the ALK fusion protein has been enhanced by using several signal amplification steps (Figure 5) (Rodig 2009, Sakairi 2010, McLeer-Florin 2012). Standardization may also be obtained with automation of IHC using a commercially available IHC kit. Standardization with automated stainers may lead to more consistent staining, occasionally at the expense of a higher concentration of the primary antibody. Recently, a highly sensitive detection method that combined
Figure 3. The effect of a low (blue circles) and a high (red triangles) signal enhancement system in IHC. Note that a low epitope concentration may become positive with a high signal enhancement system, (thin arrow), but negative with a low signal enhancement system. In addition, a higher intensity plateau is reached; once positive, a higher epitope concentration will not lead to darker staining. With ALK IHC, the epitope concentration is higher (thick arrow) in lymphomas than in NSCLC (thin arrow), and a low signal enhancement system may suffice. In NSCLC, a high-affinity antibody with high concentration and high enhancement is necessary. Epitope concentration has a logarithmic scale and a linear scale for intensity (A.U. = arbitrary units). Adapted from Prinsen CF, Klaassen CH, Thunnissen FB. Microarray as a model for quantitative visualization chemistry. Appl Immunohistochem Mol Morphol. 2003;11:168-173.
801010
20
10
Inte
nsity
(A.U
.)
Epitope Concentration

32IASLC ATLAS OF ALK TESTING IN LUNG CANCER
Table 2. Immunostaining Conditions Using Commercially Available ALK Antibodies in Selected Published Studies in which Commercially Available Kits Were Not Used
Study Antibody Antigen Retrieval
Dilution Incubation Detection System
Yi et al., 2011 ALK1 EDTA, pH 8.0, 30 min in PT Link
1:100 30 min at room temperature
ADVANCE
Mino-Kenudson et al., 2010
ALK1EDTA, pH 8.0, in pressure cooker
1:2
Overnight EnVision+ D5F3 1:100
Minca et al., 2013a D5F3 Heat mediated with BenchMark XT
1:100 Not specified OptiView
Martinez et al., 2013 D5F3 Standard on BenchMark XT
1:50 16 min at 37ºC ultraView
Paik et al., 2011 5A4 CC1 solution, 100ºC, 20 min
1:30 2 hr at 42°C iVIEW
Hofman et al., 2011 5A4 Target Retrieval Solution, pH 9.0, 97°C, 40 min
1:50 30 min at room temperature
EnVision FLEX
McLeer-Florin et al., 2012
5A4 CC1 solution with EDTA, pH 8.4, 1 hr
1:50 2 hr at 37°C Amplification Kit
Kim et al., 2011 5A4 CC1 solution, 100°C, 20 min
1:30 2 hr at 42°C iVIEW
Sholl et al., 2013 5A4 Citrate buffer, pH 6.0, in pressure cooker, 122ºC,
30-45 min
1:50 40 min at room temperature
EnVision FLEX+
Wong et al., 2009 Anti-ALK Citrate buffer, pH 6.0, in microwave, 95ºC, 30 min
1:1000 Overnight at 4ºC Streptavidin-biotinylated horseradish peroxidase
complex
Chen et al., 2012 Anti-ALK CC1 solution, 95ºC, 30 min 1:500 Overnight at room temperature
ultraView
Clone ALK1 Clone D5F3Figure 4. ALK IHC with ALK1 and D5F3 antibodies show significantly different positive intensities on identical tissue sections.
Antibodies: ALK1 is a product of Dako; D5F3 is a product of Cell Signaling Technology; 5A4 is a product of Novocastra in the studies by Paik et al., Kim et al., and Sholl et al. and is a product of Abcam in the studies by Hofman et al. and McLeer-Florin et al; and anti-ALK is a product of Invitrogen, Life Technologies Corporation. Antigen Retrieval: PT Link and Target Retrieval Solution are products of Dako, and BenchMark XT is a product of Ventana Medical Systems, Inc. Detection systems: ADVANCE, EnVision+, and EnVision FLEX+ are products of Dako; OptiView (DAB Kit), ultraView (DAB Kit), iVIEW (DAB Kit), and Amplification Kit are products of Ventana Medical Systems, Inc.

33 ChApTER 4: ImmUNOhISTOChEmISTRy
a novel hapten (3-hydroxy-2-quinoxaline; HQ) with tyramide amplification, was developed (Nitta 2013). With this HQ-tyramide IHC detection system, all tumor cells were positive, despite variations of intensity, suggesting that heterogeneous staining with some methods is a matter of a detec-tion threshold. Furthermore, the hypothesis was confirmed using the gene-protein assay that combined the highly sensitive IHC with a bright-field break-apart ISH.
Evaluation of StainingThe postanalytic phase starts with microscopic evaluation of the stained slide. In NSCLC, ALK staining is cytoplasmic; it may have a granular character and, in some cases, there may be membrane accentuation. The assessment of staining intensity is subjective, but the use of successive microscope objective lenses with inherent related spatial resolution is a physical aid in establishing the intensity level, as first applied to HER2 testing (Ruschoff 2012). The use of this approach may lead to more uniformity in intensity scoring. Strong staining (3+) is clearly visible with use of a x2 or x4 microscope objective lens; moderate staining (2+) requires a x10 or x20 objective lens to be seen clearly; and weak staining (1+) can be seen only with a x40 objective lens. The classic H-score is derived by multiplying the percentage of tumors that stain posi-tively by the intensity (0, 1, 2, or 3), giving a range of 0 to 300. This approach takes greater account of the heterogeneity of the staining. Different criteria for ALK-positive and ALK-negative results on IHC have been applied in different studies. Some authors have scored the intensity from 1+ to 3+ (Figure 6), with an ambigu-ous threshold around 1+ or 2+ ; this scoring approach seems to be mainly related to the amplification system used and the background observed with some anti-bodies (Mino-Kenudson
Regular Polymer Method Linker-Polymer Method
Figure 5. Schemes of regular polymer and linker-polymer methods.
!"#$%"&'%()*+,&'
Primary antibody
Antigens
Polymer with secondary antibodies
Linker
01+
2+3+
Figure 6. An example of ALK IHC scores ranging from 0 to 3+.

34IASLC ATLAS OF ALK TESTING IN LUNG CANCER
2010, Conklin 2013). Others have applied a simple evaluation of the positivity, defining ALK-positive expression as more than 10% of tumor cells being positive, regardless of the intensity (Rodig 2009, Mino-Kenudson 2010, McLeer-Florin 2012, Martinez 2013, Sholl 2013). More recently, however, Takeuchi found that almost all cancer cells were stained in more than 300 ALK-rearranged lung can-cers that were tested by IHC with the 5A4 antibody and the intercalated antibody-enhanced polymer (iAEP) method (Takeuchi 2013). This staining homogeneity suggests that, in ALK-rearranged lung cancers, all tumor cells harbor the ALK gene rearrangement. Until further data are available regarding false-positive IHC results, for high-throughput screening with ALK IHC, which is currently proposed in most publications, pathologists should confirm any positive signal by the reference technique, fluorescence FISH. However, an increasing number of patients who have tumors that test positively on IHC and negatively on FISH (according to strictly defined criteria) have had a good response to crizotinib therapy (Peled 2012). Another consideration is the reproducibility of ALK IHC results among different laboratories and pathologists. At the time of writing, two IHC protocols seem to be validated. In one study, using the Ventana ALK IHC kit (Ventana Medical Systems, Inc.), the reproducibility among seven international pathologists was evaluated; in a binary classification using the defined Ventana standard operating procedure, the reproducibility among the observers was 95% and 97% for both positive and negative results (Hirsch 2013). The other is the European Thoracic Oncology Platform (ETOP) protocol using the 5A4 antibody (Novocastra) (Thunnissen 2012c), in which 12 laboratories stained, either manually or with use of an automated procedure, the same tumors in a consistent manner. (See Chapter 9 for more detailed information on standardization.)
Practical Implementation of ALK IHCPathologists should be familiar with various artifacts that may lead to false-positive staining: light cytoplasmic stippling in alveolar macrophages (Figure 7), cells of neural origin (nerve and ganglion cells), glandular epithelial staining, extracellular mucin, and necrotic tumor areas. Background stain-ing is rarely observed within normal lung parenchyma, but several staining pitfalls have been noted (Table 3).
A B
C D
Figure 7. Nonspecific staining with IHC with the D5F3 antibody. A: Alveolar macrophages at the margin of an ALK-negative tumor. B: Cytology cell block of a needle aspirate from a lung nodule, showing NSCLC. Light cytoplasmic stip-pling in alveolar macrophages is an artifact that may lead to a false-positive interpretation. Cell block (C) and biopsy (D) of adenocarcinoma with stippling, which was negative for ALK rearrange-ment on FISH.

35 ChApTER 4: ImmUNOhISTOChEmISTRy
ALK protein expression may be increased in some situations without ALK rearrangement, and the IHC results may be positive with a negative (or atypical) pattern on ALK FISH (Figure 8) (also see Chapter 3). In addition, lack of ALK protein expression despite gene amplifica-tion has been reported (Pelosi 2012, Salido 2011). For example, Pelosi et al. reported that a subset of sarco-matoid carcinoma had amplification of the ALK gene, but ALK protein expression was not detected using two different antibodies. The clini-cal implications of ALK gene copy number gain associated with protein expression needs to be elucidated further (Salido 2011, Kim 2013). Histologically, mucin-containing cells such as signet ring cells require careful interpretation of ALK immu-noreactivity. A thin membranous positive pattern on ALK IHC may be masked by intracellular mucin vacuole (Figure 9), and the positive pattern may then be difficult to detect in the signet ring cells (Rodig 2009, Yoshida 2011b, Popat 2012). Some researchers have noted membranous staining, particu-larly in the apical portion, in FISH-negative cancer (Murakami 2012, Mino-Kenudson [personal communication]). This finding was not specific to cancer cells and was also seen in some nontu-mor cells, such as reactive type II pneumocytes. In addition, some neuroendocrine carcinomas have also been associated with posi-tive reactions (Murakami 2012, Nakamura 2013).
Figure 8. An example of ALK protein expression (left) with atypical pattern on FISH (diffuse single green signals; right).
Table 3. Potential Pitfalls in Interpreting the Results of IHC
Mucin- producing cells
Cytoplasm is masked by intracellular mucin, with absence of ALK protein, leading to negative staining or marginally membranous-like staining, and a false-negative interpretation.
Membranous staining
Nonspecific membranous staining, particularly prominent in the apical portion, is seen occasionally. This finding is not specific to tumor cells and is also seen in normal pneumocytes.
Neuroendocrine cells
Some squamous cell carcinomas, large cell neuroendocrine carcinomas, and normal ganglion cells show positive reactions.
Nonspecific mucin staining
Depending on the amplification system used, some background can be found on extracellular mucin and within the cytoplasm of alveolar macrophages and bronchial cells.
A B
Figure 9. A tumor with variation in morphology and staining. H & E staining shows (A) an area with many signet ring cells, and (B) area with solid pattern with few signet ring cells. ALK 5A4 immunohistochemistry shows (C) small cytoplas-mic rim low (+1) and (D) high (+2/+3) staining intensities (magnification, x40).

36IASLC ATLAS OF ALK TESTING IN LUNG CANCER
The staining may appear heterogeneous in some tumors, particularly in surgical specimens (Figure 10); however, if preanalytic conditions are controlled for, the vast majority of tumor cells are stained, paralleling the homogeneous distribution of the ALK gene rearrangement in FISH analysis. The heterogeneity is likely related to heterogeneity of the fixation and does not seem to be related to the presence of a different histologic pattern. The sensitivity of ALK protein to delay of fixation is not an issue for biopsy specimens, but may be an issue when using tissue microarrays for screening of ALK in archived specimens. The paranuclear dot-like pattern reported as typical of the KIF5B-ALK rearrangement may require further confirmation (Figure 11) (Takeuchi 2009).
Figure 11. Unusual positive reactions on IHC of a KIF5B-ALK-positive adenocarcinoma, showing a strong golgi area-highlighted staining pattern (A: H & E staining, B: ALK staining) and a perinuclear halo pattern (C: H & E staining, D: ALK staining). The bars = 100 μm. Reprinted from Takeuchi K, et al. KIF5B-ALK, a novel fusion oncokinase identified by an IHC-based diagnostic system for ALK-positive lung cancer. Clin Cancer Res. 2009;15:3143-3149.
Figure 10. An example of heterogeneous positive staining in an ALK-positive tumor. The boxes in the left panel correspond to the images on the right. Signet ring cell carcinoma component is a potential pitfall for negative staining.
A B
C D

37 ChApTER 4: ImmUNOhISTOChEmISTRy
ConclusionALK IHC assays are currently being validated and standardized and appear to be a promising clinical tool for cost-effective screening for the presence of ALK-rearrangement in NSCLC. The procedure is already recommended by organizations in Europe, Japan, and Asia. In the United States, where treatment of NSCLC with an ALK inhibitor is currently dependent on positive results on ALK FISH, positive results on ALK IHC still require verification by ALK FISH for eligibility for ALK inhibitor therapy. However, in the near future, the IHC test may be approved by the US FDA, and patients with positive results on ALK IHC would also be eligible for treatment with an ALK inhibitor. In Europe, ALK-positive lung cancer is not restricted to testing by ALK FISH.
ChApter 5
Reverse-Transcriptase Polymerase Chain Reaction (RT-PCR) and Multiple Gene Assays
By Yasushi Yatabe, Kengo Takeuchi, and Ignacio Wistuba
PCR is clinically feasible, as this technique is used in most assays to detect EGFR mutations in NSCLC. However, assays with reverse transcriptase (RT)-PCR are used primarily for hematologic malignancies, as high-quality RNA is required, which is difficult to obtain in clinical practice. Indeed, in the CAP/IASLC/AMP guideline, RT-PCR is not recommended for testing to select patients for ALK inhibitor therapy for lung cancer because of the risk of false-negative results and a high failure rate for RNA-based assays on FFPE samples. However, RT-PCR provides the most robust and detailed information about ALK fusion patterns. Furthermore, some recently developed techniques can be applied to clinical samples with a high success rate.
RT-PCREML4-ALK shows many fusion variants. The breakpoint of ALK is constantly located before the 5'-end of exon 20 (ENST00000389048) where the kinase domain starts, and this constant retention is seen in other cancers with ALK translocation, such as lymphoma and sarcoma. In contrast, the breakpoint of EML4 may distribute various exons. Following the discovery of the first two fusion variants (Soda 2007), more than 13 variants and three fusion partners have been found (Figure 1). In the six most common EML4-ALK variants, the exons of EML4 and ALK are directly fused in an in-frame fashion without any insertion or deletion. The three major variants (v1: E13;A20, v2: E20;A20, and v3: E6;A20) account for more than 90% of lung cancers associated with EML4-ALK. Among the minor variants, E2;A20 (v5) and E18;A20 (v5') are found in 1% to 2% of lung cancers with EML4-ALK (Takeuchi 2008, Wong 2009). E21;A20 has been identified in colorectal cancer (Lin 2009), but not yet in lung cancer. RT-PCR on fresh or snap-frozen tumor samples may be more sensitive than other methods in terms of the number of cancer cells required. However, high sensitivity is achieved only when the fusion pattern is within a detectable range of primer pairs. To detect all the possible EML4-ALK variants, primer sets should be designed in a comprehensive way (Table 1), and even a comprehensive design may not detect irregular variants with deletions in the annealing site of the primers. Furthermore, RT-PCR systems designed for detecting EML4-ALK cannot detect ALK fusions with other partner sets such as kinesin family member 5B (KIF5B) and kinesin light chain 1 (KLC1) (Takeuchi 2009, Togashi 2012). To overcome this limitation, primers for other fusion partners have been designed, enabling simultaneous one-tube RT-PCR detection of EML4-ALK, KIF5B-ALK (Figure 2), and ret proto-oncogene (RET) fusions (Takeuchi 2012). Despite these efforts, fusions with unknown partners have remained undetectable. Therefore, RT-PCR is not recommended for screening of patients for treatment with
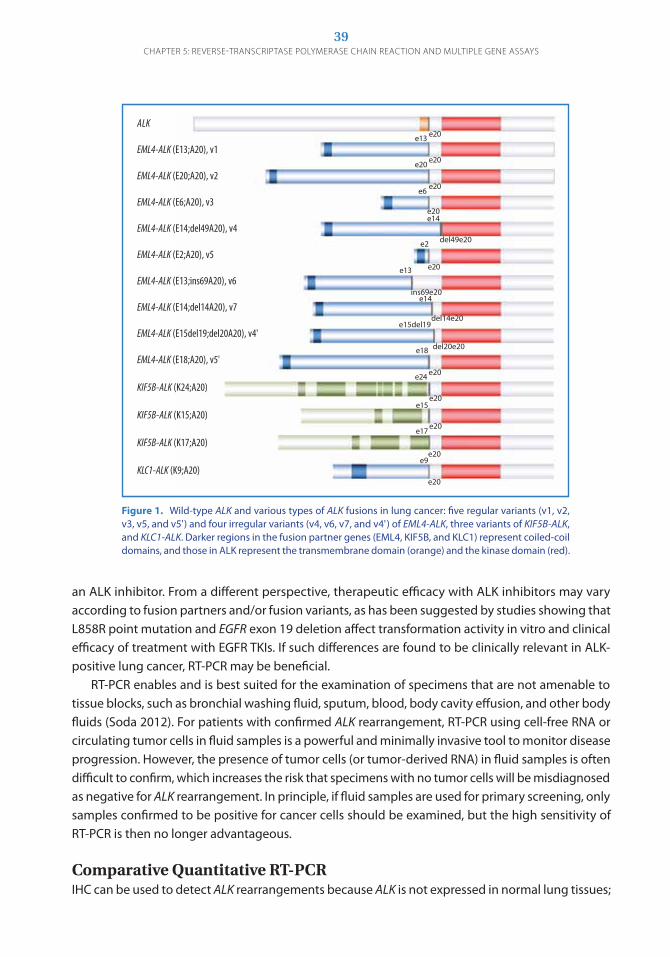
39ChApTER 5: REvERSE-TRANSCRIpTASE pOLymERASE ChAIN REACTION ANd mULTIpLE GENE ASSAyS
ALK
EML4-ALK (E13;A20), v1
EML4-ALK (E20;A20), v2
EML4-ALK (E6;A20), v3
EML4-ALK (E14;del49A20), v4
EML4-ALK (E2;A20), v5
EML4-ALK (E13;ins69A20), v6
EML4-ALK (E14;del14A20), v7
EML4-ALK (E15del19;del20A20), v4'
EML4-ALK (E18;A20), v5'
KIF5B-ALK (K24;A20)
KIF5B-ALK (K15;A20)
KIF5B-ALK (K17;A20)
KLC1-ALK (K9;A20)
e20
e20
e13
e20
e20e6
e20e14
e20
e2 del49e20
e13
ins69e20e14
del14e20
e18
e15del19
del20e20
e20
e20
e20
e20
e20
e9
e17
e15
e24
Figure 1. Wild-type ALK and various types of ALK fusions in lung cancer: five regular variants (v1, v2, v3, v5, and v5') and four irregular variants (v4, v6, v7, and v4') of EML4-ALK, three variants of KIF5B-ALK, and KLC1-ALK. Darker regions in the fusion partner genes (EML4, KIF5B, and KLC1) represent coiled-coil domains, and those in ALK represent the transmembrane domain (orange) and the kinase domain (red).
an ALK inhibitor. From a different perspective, therapeutic efficacy with ALK inhibitors may vary according to fusion partners and/or fusion variants, as has been suggested by studies showing that L858R point mutation and EGFR exon 19 deletion affect transformation activity in vitro and clinical efficacy of treatment with EgFR TKIs. If such differences are found to be clinically relevant in ALK-positive lung cancer, RT-PCR may be beneficial. RT-PCR enables and is best suited for the examination of specimens that are not amenable to tissue blocks, such as bronchial washing fluid, sputum, blood, body cavity effusion, and other body fluids (Soda 2012). For patients with confirmed ALK rearrangement, RT-PCR using cell-free RNA or circulating tumor cells in fluid samples is a powerful and minimally invasive tool to monitor disease progression. However, the presence of tumor cells (or tumor-derived RNA) in fluid samples is often difficult to confirm, which increases the risk that specimens with no tumor cells will be misdiagnosed as negative for ALK rearrangement. In principle, if fluid samples are used for primary screening, only samples confirmed to be positive for cancer cells should be examined, but the high sensitivity of RT-PCR is then no longer advantageous. Comparative Quantitative RT-PCRIHC can be used to detect ALK rearrangements because ALK is not expressed in normal lung tissues;

40IASLC ATLAS OF ALK TESTING IN LUNG CANCER
Study Applicability to Regular Variants of EML4-ALK Specimen Type No. of Primers
Major Variants* Minor Variants*
E13;A20 E20;A20 E6;A20 E2;A20 E18;A20 E21;A20
Soda et al., 2007
Yes Yes No No Yes Yes Frozen 2
Inamura et al., 2008
Yes Yes No No Yes Yes Frozen 2
Shinmura et al., 2008
Yes Yes No No Yes Yes Frozen 3
Takeuchi et al., 2008
Yes Yes Yes Yes Yes Yes Frozen 3
Martelli et al., 2009
Yes Yes Yes No Yes Yes Frozen 3
Takeuchi et al., 2009
Yes Yes Yes Yes Yes Yes Frozen5
(including 2 primers for KIF5B-ALK)
Wong et al., 2009
Yes Yes Yes No Yes Yes Frozen 4
Takahashi et al., 2010
Yes Yes Yes Yes Yes Yes Frozen 3
Sun Y et al., 2010
Yes Yes Yes Yes Yes Yes Frozen 4
Sanders et al., 2011
Yes Yes Yes Yes Yes Yes FFPE 23
Takeuchi et al., 2012
Yes Yes Yes Yes Yes Yes Frozen
6 (including 3 primers
for KIF5B-ALK and RET fusions)
Shaozhang et al., 2012
Yes Yes Yes Yes Yes Yes Frozen 4
Soda et al., 2012
Yes Yes Yes Yes Yes Yes Frozen9
(including 4 primers for KIF5B-ALK)
*Major variants are found in more than 90% of lung cancers with EML4-ALK; minor variants are found in 1% to 2% of lung cancers with EML4-ALK.
Table 1. RT-PCR Settings for EML4-ALK Screening
as such, a positive reaction of ALK on IHC always suggests aberrant ALK expression that is most fre-quently caused by rearrangement in lung cancer. This principle can be applied to expression of the ALK transcript. The breakpoint in ALK occurs before the oncogenic kinase domain (exon 20) that the chimeric transcript consistently retains. Therefore, when ALK is fused with EML4 or other partners, the 3' and 5' regions of the ALK transcript are expressed differently (Figure 3). On the basis of this principle, exon array has been used to detect the fusion gene, with identifica-tion of novel variants of EML4-ALK in addition to common fusion patterns (Lin 2009). Real-time PCR has also been used (Wang R 2012a, Wang R 2012b). NanoString assay (NanoString Technologies) was recently introduced to detect ALK fusion genes (Lira 2013), as well as ROS1 and RET (Suehara 2012).
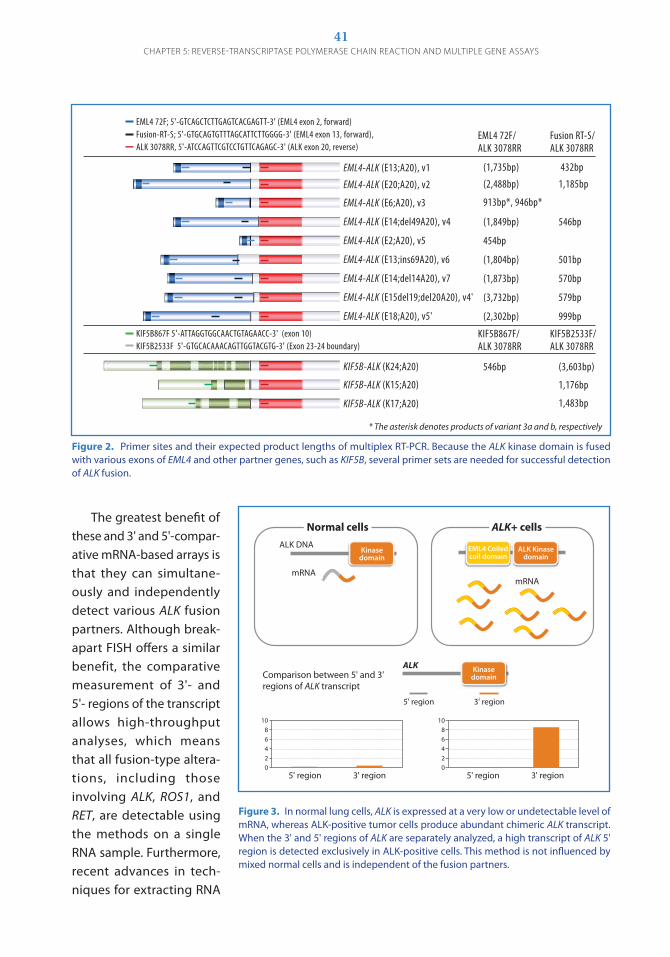
41ChApTER 5: REvERSE-TRANSCRIpTASE pOLymERASE ChAIN REACTION ANd mULTIpLE GENE ASSAyS
The greatest benefit of these and 3' and 5'-compar-ative mRNA-based arrays is that they can simultane-ously and independently detect various ALK fusion partners. Although break-apart FISH offers a similar benefit, the comparative measurement of 3'- and 5'- regions of the transcript allows high-throughput analyses, which means that all fusion-type altera-tions, including those involving ALK, ROS1, and RET, are detectable using the methods on a single RNA sample. Furthermore, recent advances in tech-niques for extracting RNA
Figure 2. Primer sites and their expected product lengths of multiplex RT-PCR. Because the ALK kinase domain is fused with various exons of EML4 and other partner genes, such as KIF5B, several primer sets are needed for successful detection of ALK fusion.
EML4-ALK (E13;A20), v1
EML4-ALK (E20;A20), v2
EML4-ALK (E6;A20), v3
EML4-ALK (E14;del49A20), v4
EML4-ALK (E2;A20), v5
EML4-ALK (E13;ins69A20), v6
EML4-ALK (E14;del14A20), v7
EML4-ALK (E15del19;del20A20), v4'
EML4-ALK (E18;A20), v5'
KIF5B-ALK (K24;A20)
KIF5B-ALK (K15;A20)
KIF5B-ALK (K17;A20)
(1,735bp)
(2,488bp)
913bp*, 946bp*
(1,849bp)
454bp
(1,804bp)
(1,873bp)
(3,732bp)
(2,302bp)
546bp
432bp
1,185bp
546bp
501bp
570bp
579bp
999bp
(3,603bp)
1,176bp
1,483bp
EML4 72F; 5'-GTCAGCTCTTGAGTCACGAGTT-3' (EML4 exon 2, forward)Fusion-RT-S; 5'-GTGCAGTGTTTAGCATTCTTGGGG-3' (EML4 exon 13, forward), ALK 3078RR, 5'-ATCCAGTTCGTCCTGTTCAGAGC-3' (ALK exon 20, reverse)
KIF5B867F 5'-ATTAGGTGGCAACTGTAGAACC-3' (exon 10)KIF5B2533F 5'-GTGCACAAACAGTTGGTACGTG-3' (Exon 23-24 boundary)
EML4 72F/ALK 3078RR
Fusion RT-S/ALK 3078RR
KIF5B867F/ALK 3078RR
KIF5B2533F/ALK 3078RR
!"#$%&#'()!*+,&-./0(1* ()*02+345/ (($+-45(
!"#$%&#'()!-.,&-./0(1- ()-0$6645/ (*0*6345(
!"#$%&#'()!7,&-./0(1+ (8*+4590(8$7459(
!"#$%&#'()!*$,:;<$8&-./0(1$ ()*06$845/ (3$745(
!"#$%&#'()!-,&-./0(13 ($3$45(
!"#$%&#'()!*+,=>?78&-./0(17 ()*06.$45/ (3.*45(
!"#$%&#'()!*$,:;<*$&-./0(12 ()*062+45/ (32.45(
!"#$%&#'()!*3:;<*8,:;<-.&-./0(1$@( ()+02+-45/ (32845(
!"#$%&#'()!*6,&-./0(13@ ()-0+.-45/ (88845(
&#'(+.26AA0(3 %&BCC&DBBCDBCCBDBBC&D&DC%+ ()&#'(;EF>(-.0(G;1;G?;/(HI?=F>%AB%J,(3 %DBDC&DBDBBB&DC&BBCBBDDDD%+ ()!"#$(;EF>(*+0(KFGLMG:/0((!"#$(2-H,(3 %DBC&DCBCBBD&DBC&CD&DBB%+ ()!"#$(;EF>(-0(KFGLMG:/(
!"#$(2-HN(&#'(+.26AA(
HI?=F>(AB%JN(&#'(+.26AA(
'OH3P%&#'()'-$,&-./ (3$745 ()+07.+45/((
'OH3P%&#'()'*3,&-./ ( (*0*2745((
'OH3P%&#'()'*2,&-./ ( (*0$6+45(
'OH3P672H(3@%&BB&DDBDDC&&CBDB&D&&CC%+@(();EF>(*./('OH3P-3++H((3@%DBDC&C&&&C&DBBDDB&CDBD%+@()!EF>(-+%-$(4FI>:MGQ/(
'OH3P672HN(&#'(+.26AA(
'OH3P-3++HN(&#'(+.26AA(
9(BR;(M?S;G=?T(:;>FS;?((5GF:IUS?(FK(1MG=M>S(+M(M>:(40(G;?5;UV1;<Q(
!"#$%&#'()!*+,&-./0(1* ()*02+345/ (($+-45(
!"#$%&#'()!-.,&-./0(1- ()-0$6645/ (*0*6345(
!"#$%&#'()!7,&-./0(1+ (8*+4590(8$7459(
!"#$%&#'()!*$,:;<$8&-./0(1$ ()*06$845/ (3$745(
!"#$%&#'()!-,&-./0(13 ($3$45(
!"#$%&#'()!*+,=>?78&-./0(17 ()*06.$45/ (3.*45(
!"#$%&#'()!*$,:;<*$&-./0(12 ()*062+45/ (32.45(
!"#$%&#'()!*3:;<*8,:;<-.&-./0(1$@( ()+02+-45/ (32845(
!"#$%&#'()!*6,&-./0(13@ ()-0+.-45/ (88845(
&#'(+.26AA0(3 %&BCC&DBBCDBCCBDBBC&D&DC%+ ()&#'(;EF>(-.0(G;1;G?;/(HI?=F>%AB%J,(3 %DBDC&DBDBBB&DC&BBCBBDDDD%+ ()!"#$(;EF>(*+0(KFGLMG:/0((!"#$(2-H,(3 %DBC&DCBCBBD&DBC&CD&DBB%+ ()!"#$(;EF>(-0(KFGLMG:/(
!"#$(2-HN(&#'(+.26AA(
HI?=F>(AB%JN(&#'(+.26AA(
'OH3P%&#'()'-$,&-./ (3$745 ()+07.+45/((
'OH3P%&#'()'*3,&-./ ( (*0*2745((
'OH3P%&#'()'*2,&-./ ( (*0$6+45(
'OH3P672H(3@%&BB&DDBDDC&&CBDB&D&&CC%+@(();EF>(*./('OH3P-3++H((3@%DBDC&C&&&C&DBBDDB&CDBD%+@()!EF>(-+%-$(4FI>:MGQ/(
'OH3P672HN(&#'(+.26AA(
'OH3P-3++HN(&#'(+.26AA(
9(BR;(M?S;G=?T(:;>FS;?((5GF:IUS?(FK(1MG=M>S(+M(M>:(40(G;?5;UV1;<Q(* The asterisk denotes products of variant 3a and b, respectively
Figure 3. In normal lung cells, ALK is expressed at a very low or undetectable level of mRNA, whereas ALK-positive tumor cells produce abundant chimeric ALK transcript. When the 3' and 5' regions of ALK are separately analyzed, a high transcript of ALK 5' region is detected exclusively in ALK-positive cells. This method is not influenced by mixed normal cells and is independent of the fusion partners.
Normal cells ALK+ cells
Kinase domain
EML4 Coiled coil domain
ALK Kinase domain
ALK DNA
mRNA
mRNA
Kinase domain
ALK
5’ region 3’ region
!"#$%&'(")*+,-.,,)*/0*%)1*20*&,3'")(*"4*567*-&%)(8&'$-*
9*
:*
;*
<*
=*
>9*
5' region 3' region
9*
:*
;*
<*
=*
>9*
5' region 3' region
ALK+ cellsNormal cells
ALK DNA
mRNAmRNA
Comparison between 5' and 3'regions of ALK transcript
5' region 3' region
ALK
1086420
5' region 3' region
1086420
5' region 3' region
ALK+ cellsNormal cellsALK DNA
mRNAmRNA
Comparison between 5' and 3'regions of ALK transcript
5' region 3' region
ALK
1086420
5' region 3' region
1086420
5' region 3' region
Kinasedomain
ALK Kinasedomain
EML4 Coiledcoil domain
Kinasedomain
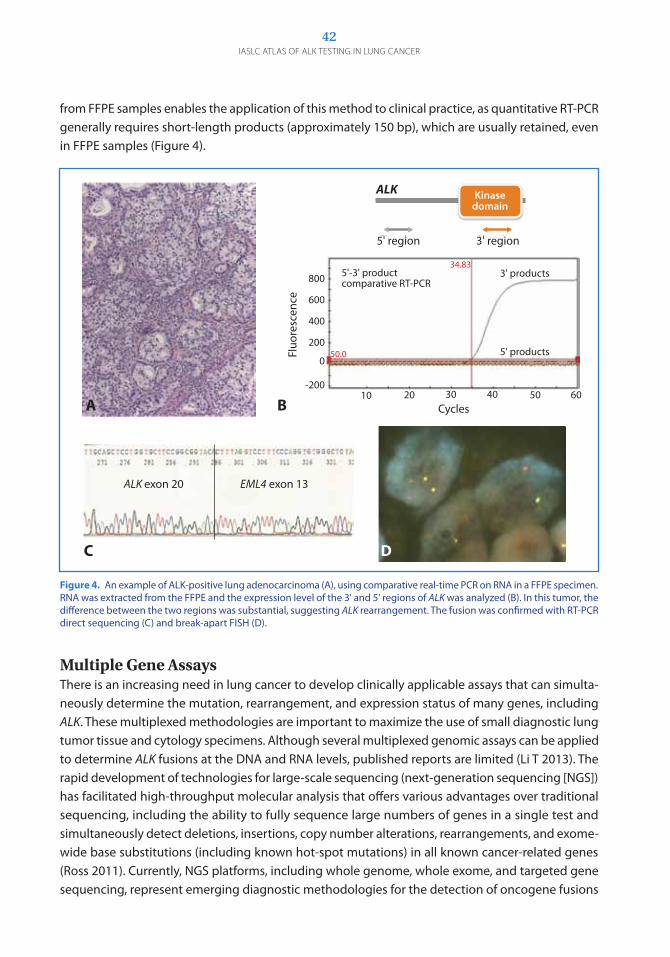
42IASLC ATLAS OF ALK TESTING IN LUNG CANCER
Figure 4. An example of ALK-positive lung adenocarcinoma (A), using comparative real-time PCR on RNA in a FFPE specimen. RNA was extracted from the FFPE and the expression level of the 3' and 5' regions of ALK was analyzed (B). In this tumor, the difference between the two regions was substantial, suggesting ALK rearrangement. The fusion was confirmed with RT-PCR direct sequencing (C) and break-apart FISH (D).
Normal cells ALK+ cells
Kinase domain
EML4 Coiled coil domain
ALK Kinase domain
ALK DNA
mRNA
mRNA
Kinase domain
ALK
5’ region 3’ region
!"#$%&'(")*+,-.,,)*/0*%)1*20*&,3'")(*"4*567*-&%)(8&'$-*
9*
:*
;*
<*
=*
>9*
5' region 3' region
9*
:*
;*
<*
=*
>9*
5' region 3' region
ALK+ cellsNormal cells
ALK DNA
mRNAmRNA
Comparison between 5' and 3'regions of ALK transcript
5' region 3' region
ALK
1086420
5' region 3' region
1086420
5' region 3' region
ALK+ cellsNormal cellsALK DNA
mRNAmRNA
Comparison between 5' and 3'regions of ALK transcript
5' region 3' region
ALK
1086420
5' region 3' region
1086420
5' region 3' region
Kinasedomain
ALK Kinasedomain
EML4 Coiledcoil domain
Kinasedomain
800
600
400
200
0
-20010 20 30 40 50 60
Cycles
Fluo
resc
ence
34.83
50.0
5'-3' product comparative RT-PCR
3' products
5' products
ALK exon 20 EML4 exon 13
A B
C D
from FFPE samples enables the application of this method to clinical practice, as quantitative RT-PCR generally requires short-length products (approximately 150 bp), which are usually retained, even in FFPE samples (Figure 4).
Multiple Gene AssaysThere is an increasing need in lung cancer to develop clinically applicable assays that can simulta-neously determine the mutation, rearrangement, and expression status of many genes, including ALK. These multiplexed methodologies are important to maximize the use of small diagnostic lung tumor tissue and cytology specimens. Although several multiplexed genomic assays can be applied to determine ALK fusions at the DNA and RNA levels, published reports are limited (Li T 2013). The rapid development of technologies for large-scale sequencing (next-generation sequencing [NgS]) has facilitated high-throughput molecular analysis that offers various advantages over traditional sequencing, including the ability to fully sequence large numbers of genes in a single test and simultaneously detect deletions, insertions, copy number alterations, rearrangements, and exome-wide base substitutions (including known hot-spot mutations) in all known cancer-related genes (Ross 2011). Currently, NgS platforms, including whole genome, whole exome, and targeted gene sequencing, represent emerging diagnostic methodologies for the detection of oncogene fusions

43
and mutations in tumor tissue specimens, including FFPE samples (Lipson 2012, Takeuchi 2012). In one study, NgS of genomic DNA, involving breakpoints in at least five different genomic loci, detected a complex ALK rearrangement in a sample that was ALK-negative on break-apart FISH (Peled 2012). Experience is limited with determining ALK mutations and gene copy number varia-tions in clinical lung tumor tissue specimens. With use of DNA extracted from FFPE samples of lung tumor tissues, a multiplexed NgS assay detected ALK gene mutations associated with resistance to crizotinib treatment in three of 13 patients with lung cancer (Huang 2013). ConclusionRT-PCR to detect EML4-ALK should be designed as comprehensively as possible, with the targets narrowed to the three major variants that account for more than 90% of lung cancers with EML4-ALK. RT-PCR may be an adequate tool for confirming the results of IHC and FISH analyses, but is less appropriate for primary screening for ALK rearrangment, especially when the amount of tissue sample is adequate. Novel multiplexed genomic assays, particularly NgS, represent promising clini-cally applicable methodologies for the detection of ALK fusions, as well as other gene abnormalities, including mutations, copy number gains, and gene expression. However, published data on these assays are limited.
ChApTER 5: REvERSE-TRANSCRIpTASE pOLymERASE ChAIN REACTION ANd mULTIpLE GENE ASSAyS

ChApter 6
As noted earlier, FISH has been universally accepted as a reference standard in the assessment of ALK rearrangement, and it has been clinically validated and approved for testing to select patients for treatment with an ALK inhibitor (crizotinib). FISH can detect ALK rearrangement regardless of the gene partner and variant and can be performed on archived FFPE specimens. However, FISH requires a minimum of 50 tumor cells, and this requirement may be the reason FISH cannot be used in as many as 20% of lung cancer biopsies (Camidge 2010, McLeer-Florin 2012). FISH has many other limitations; it is time-consuming, has a high cost, requires a fluorescent microscope, and necessitates specialized training for interpretation of results. Because of its limitations, FISH is not available in all routine pathology laboratories, and other assay platforms have been evaluated for their usefulness in detecting ALK in NSCLC. Studies have focused on comparing FISH with IHC with use of various antibodies, multiplex and quantitative RT-PCR, and CISH. IHC may, in theory, detect all ALK fusion proteins, but some variants and fusion partners may generate low protein levels that may be difficult to detect. Therefore, many IHC assays now include an amplification process to enhance the protein signal. IHC remains the most popular and cost-effective platform because it • Isusedinpathologylaboratoriesworldwide• CanbeusedonroutinelypreparedFFPEspecimens• Isrelativelyinexpensive• Requireslimitedequipment• Offersrapidtrainingandoptimization• Usuallyrequiresasmallnumberoftumorcellstodetectthepresenceofthefusionprotein
Although correlation of results of ALK IHC and ALK FISH is excellent, IHC as a predictive marker for response to ALK inhibitor therapy has not been validated in large patient cohorts. IHC also does not directly demonstrate the ALK rearrangement, and some false-negative and false-positive results (compared with FISH results) have been reported. Some specimens that have tested as ALK positive on IHC and ALK negative on FISH have been associated with a good response to crizotinib (Peled 2012). Standardization of the IHC assay for ALK testing is currently ongoing. However, many guidelines, such as those developed in Europe and Japan, already recommend ALK IHC for screening, with verifi-cation of positive results by FISH for eligibility for crizotinib therapy. Also, the US guideline notes that
Comparison of Different Assay Platformsfor ALK Testing
By Sylvie Lantuéjoul, Marileila Varella-Garcia, Erik Thunnissen, and Yasushi Yatabe

45ChApTER 6: COmpARISON OF dIFFERENT ASSAy pLATFORmS FOR ALK TESTING
ALK IHC, if carefully validated, may be considered for screening patients with lung adenocarcinoma (Lindeman 2013). RT-PCR is a highly specific and reliable technique, as it allows for the precise identification of the 5’ partners and breakpoint variants. But atypical ALK variants or fusion partners (such as an irregular variant with insertion or deletion) may be undetected. RT-PCR of EML4-ALK is highly sensitive because the primers will not amplify a product in normal cells, but intact mRNA is poorly preserved in an archived FFPE specimen. The cost of RT-PCR is still being evaluated and depends on the laboratory and the test used. CISH is a new method for detection of ALK rearrangement, with the aim of overcoming some of the disadvantages of FISH (Kim 2011). CISH is a fully automated ISH assay, which provides stable staining and allows detection of ALK gene rearrangement using conventional bright-field light microscopy.
IHC versus FISHSeveral studies have compared IHC with FISH. A variety of antibodies have been used for IHC, including two mouse monoclonal antibodies clones, ALK1 (Dako) and 5A4 (Novocastra); a rabbit monoclonal antibody clone D5F3 (Cell Signaling Technology); and a rabbit polyclonal antibody (Invitrogen, Life Technologies). In most studies, FISH has been performed with an ALK break-apart rearrangement probe kit (Abbott Molecular), which has been approved by the US FDA as the com-panion diagnostic for ALK testing to determine patient eligibility for treatment with crizotinib.
ALK1 IHC versus FISH Initially used for diagnosing anaplastic large cell lymphoma, the ALK1 antibody has also been evalu-ated for the detection of ALK rearrangement in NSCLC. ALK1 IHC and FISH were compared in three large series of adenocarcinoma of the lung or NSCLC (Table 1) (Rodig 2009, Mino-Kenudson 2010, Yi 2011). Compared with FISH, ALK1 IHC seems less sensitive for detecting ALK-rearranged lung cancer than for detecting anaplastic large cell lymphoma, possibly because the ALK fusion protein is expressed at lower levels in NSCLC. ALK1 offers good specificity, but sensitivity has ranged from 67% to 100%. Some specimens have tested positively for ALK on FISH but negatively for ALK on IHC, but no specimens have tested positively on IHC and negatively on FISH (Rodig 2009, Mino-Kenudson
StudyNo. of
Specimens ALK1
DilutionAntigen Retrieval
Detection and Amplification
SystemScoring
IHC Positive
Threshold
IHC Sensitivity (vs. FISH)
IHC Specificity (vs. FISH)
Rodig et al., 2009
358 1:2 EDTA (pH 8.0) inpressure cooker
Tyramideamplification and EnVision
0 vs. + >10% positive
tumor cells
80% with amplification (40% without)
100%
Mino- Kenudson et al., 2010
153 1:2 EDTA (pH 8.0) inpressure cooker
EnVision 0, 1+, 2+, or 3+ and % of tumor cells
stained
>10% positive
tumor cells
67% 97%
Yi et al., 2011
101 1:100 EDTA (pH 8.0) in PT Link
ADVANCE 0, 1+, 2+, or 3+
>0 90% 97.8%
Table 1. Staining Features of IHC with ALK1 Antibody
PT Link, EnVision, and ADVANCE are products of Dako.

46IASLC ATLAS OF ALK TESTING IN LUNG CANCER
2010). In one study, 1+ and 3+ IHC scores defined ALK negative and ALK positive, respectively, with a 2+ score considered to be an equivocal result (Yi 2011). This classification is similar to that for HER2 testing in breast cancer. The use of tyramide amplification was recommended to increase the sensitivity of detection, but nonspecific staining of tumor and nontumor cells was reported at a high concentration of ALK1 antibody (Mino-Kenudson 2010).
D5F3 IHC versus FISHIHC with the D5F3 clone has been compared with FISH in three studies (Table 2) (Mino-Kenudson 2010, Martinez 2013, Minca 2013). The sensitivity was 83% to 100%, and the specificity was 99% and 100%. Among six specimens that were ALK positive by FISH in one study, one specimen was ALK negative by IHC, but none of the specimens that were ALK negative by FISH were ALK positive by IHC (Martinez 2013). In addition to these studies, an international panel of pathologists evaluated D5F3 IHC in a series of lung adenocarcinoma with known ALK genotype. Overall, the sensitivity was 90% and the specificity was 95% for IHC compared with FISH, and the interobserver concordance in scoring was high (Hirsch 2013).
5A4 IHC versus FISH At least six studies have compared IHC with the 5A4 clone and FISH in a large series (Table 3) (Jokoji 2010, Kim 2011, Paik 2011, Lopes 2012, McLeer-Florin 2012, Sholl 2013). Across all studies, the sen-sitivity and specificity ranged from 93% to 100% and 96% to 100%, respectively. However, in one study, false-positive or false-negative results were reported; in one case, the malignant cells were missed on FISH, and the result was ALK positive by IHC, and in another case, asymmetric split signals with weak green probe signals were misinterpreted as ALK positive on FISH (Sholl 2013). Overall, in that study, the specificity of FISH compared with IHC was 98.5%.
Table 2. Staining Features of IHC with D5F3 Antibody
StudyNo. of
Specimens D5F3
DilutionAntigen Retrieval
Detection and Amplification
SystemScoring
IHC Positive
Threshold
IHC Sensitivity (vs. FISH)
IHC Specificity (vs. FISH)
Mino- Kenudson et al., 2010
153 1:100 EDTA (pH 8.0) inpressure cooker
EnVision+ 0, 1+, 2+, or 3+ and % of tumor cells
>10% positive
tumor cells
100% 99%
Martinez et al., 2013
79 1:50 Standard on BenchMark XT
ultraView 0 vs. + ≥10% positive
tumor cells
83% 100%
Minca et al., 2013a
231 1:100 Heat mediated with
BenchMark XT
OptiView 0 vs. + Positive 94%** 100%
Hirsch et al., 2013b*
98 Pre-diluted
Standard on BenchMark XT
OptiView and OptiView
Amplification
0 vs. + Any strong cytoplasmic
staining
90% 95%
aTwo false-negative results on IHC testing of FFPE specimens were subsequently corrected by testing with a ThinPrep processor (positive results). bCases selected for the study included 43 specimens that were ALK positive by FISH and 55 that were ALK negative by FISH.
BenchMark XT, ultraView (Universal DAB Detection Kit), OptiView (DAB IHC Detection Kit), and OptiView Amplification Kit are products of Ventana Medical Systems, Inc. EnVision+ is a product of Dako.

47ChApTER 6: COmpARISON OF dIFFERENT ASSAy pLATFORmS FOR ALK TESTING
Rabbit Polyclonal Antibody IHC versus RT-PCRAt least two studies have involved the use of IHC with a rabbit polyclonal antibody (Table 4) (Wong 2009, Chen 2012). In one study, the results were compared with those obtained by EML4-ALK RT-PCR, and concordance was high (Chen 2012). In the other study, 11 adenocarcinomas and one adeno-squamous carcinoma that were ALK positive on RT-PCR were also positive on IHC (Wong et al 2009).
Comparison of Antibody Clones Some authors have directly addressed concordance among antibody clones using the same sample sets, and concordance has been antibody dependent (Table 5) (Rodig 2009, Takeuchi 2009, Mino-Kenudson 2010, Murakami 2011, Conklin 2013, Selinger 2013). Takeuchi et al. reported comparable
Table 3. Staining Features of IHC with 5A4 Antibody
Study No. of Specimens
5A4 Dilutiona
Antigen Retrieval
Detection and Amplification
SystemScoring
IHC Positive
Threshold
IHC Sensitivity (vs. FISH)
IHC Specificity (vs. FISH)
Jokoji et al., 2010
254 1:100 Target Retrieval Solution, high pH
EnVision FLEX+ and
iAEP
0 vs. + No score 100%(FISH done on
IHC+ specimens only)
100%
Paik et al. 2011
640 1:30 CC1 solution i-VIEW 0, 1+, 2+, or 3+
0, or 1+: negative
2+: equivocal3+: positive
100% 96%
Kim et al., 2011
465 1:30 CC1 solution i-VIEW 0, 1+, 2+, or 3+
0, or 1+: negative
2+: equivocal3+: positive
100%when score of 2+ considered
positive
98%
McLeer-Florin et al., 2012
441 1:50 CC1 solution ultraView 0, 1+, 2+, or 3+ and % of positive tumor cells
>10% positive
tumor cells
95% 100%
Lopes et al., 2012
62 1:200 Microwave Novolink
No score >10% positive
tumor cells
100% 100%
Sholl et al., 2013
186 1:50 Citrate buffer, (pH 6) in
pressure cooker
EnVision FLEX+
0, 1+, or 2+ 1+, 2+ 93% 100%
aThe 5A4 antibody used in the studies by McLeer-Florin et al., Jokoji et al., and Lopes et al. were from Abcam ; the antibody used in the other studies were from Novocastra.
iView (DAB Detection Kit) and OptiView (DAB IHC Detection Kit) are products of Ventana Medical Systems. Novolink (Polymer Detection System) is a product of Leica Biosystems.
Table 4. Staining Features of IHC with ALK Rabbit Polyclonal Antibody
StudyNo. of
Specimens (% of ALK+)
ALK1 Dilution
Antigen Retrieval
Detection/ Amplification
SystemScoring
IHC Positive
Threshold
IHC Sensitivity
(vs. RT-PCR)
IHC Specificity
(vs. RT-PCR)
Wong et al., 2009
266 (4.9%) 1:1000 Citrate buffer (pH 6.0) in microwave
HRPcomplex
None Not specified
100% Not specified
Chen et al., 2012
64 (4.7%) 1:500 CC1 solution ultraView 0, 1+, 2+, or 3+
≥2+ 100% 90%
CC1 (Tris/borate/ EDTA) is a product of Roche (Basel, Switzerland). ultraView (Universal DAB Detection Kit) is a product of Ventana Medical Systems, Inc. , and HRP (horseradish peroxidase) complex is a product of Dako.

48IASLC ATLAS OF ALK TESTING IN LUNG CANCER
Table 5. Comparison of Antibody Clones Used with IHC
StudyNo. of
Specimens (% of ALK+)
AntibodyClone
Antigen Retrieval
Detection/ Amplification
SystemScoring Standard
IHC Sensitivity
(vs. Standard)
IHC Specificity
(vs. Standard)
Takeuchi et al., 2009
21 (52%) 5A4 Target Retrieval Solution (pH 9.0)
(for all)
iAEP
0 vs. + (for all)
RT-PCR 100% 100%
5A4 EnVision+ 27% 100%
ALK1 iAEP 100% 100%
ALK1 EnVision+ 9% 100%
SP8 iAEP 20% 100%
SP8 EnVision+ 100% 18%
Rodig et al., 2009
239 (4%) ALK1 EDTA in pressure cooker (for both)
EnVision+ 0 vs. + (for both)
FISH 40% 100%
ALK1 Tyramide amplification
80% 100%
Mino- Kenudson et al., 2010
37 (59%) ALK1 EDTA in pressure cooker (for both)
EnVision+(for both)
Score >2.7 on image analysis is positive
FISH 67% 97%
D5F3 100% 99%
Murakami et al., 2011
361a (5%) ALK1 Target Retrieval Solution (pH 9.0)
(for all)
ABC (no enhancement)
0 vs. + (for all)
RT-PCR/FISH
81% 100%
5A4 EnVision FLEX+
100% 100%
EnVision FLEX+
100% 99.7%
Conklin et al., 2013
377 (3%) 5A4 According to manufacturer’s
instructions (for all)
iAEP 0, 1+, 2+, or 3+
(for all)
FISH 100% 62.5%
ALK1 EnVision FLEX 66% 100%
ALK1 ADVANCE 66% 87.5%
5A4 ADVANCE 100% 87.5%
D5F3 ADVANCE 100% 75%
Selinger et al., 2013
594 (11%) ALK1 Buffer (pH 9.0) in pressure cooker
EnVision FLEX+
0, 1+, 2+, or 3+
(for all)
FISH 100% 99%
5A4 According to manufacturer’s
instructions
ultraView and ultraView
Amplification
100% 98%
D5F3 According to manufacturer’s
instructions
OptiView and OptiView
Amplification
100% 99%
aThe number of specimens for testing with the D5F3 antibody was 356.
SP8 is a product of Abcam. Target Retrieval Solution, buffer, EnVision, EnVision FLEX+, and ADVANCE are products of Dako.. ultraView (Universal DAB Detection Kit), OptiView (DAB IHC Detection Kit), and ultraView and OptiView Amplification kits are products of Ventana Medical Systems, Inc.
ABC = avidin biotin complex.

49ChApTER 6: COmpARISON OF dIFFERENT ASSAy pLATFORmS FOR ALK TESTING
results with the ALK1 and 5A4 antibodies using an intercalated antibody-enhanced polymer (iAEP) method to amplify signals (Takeuchi 2009). However, discordance has been found in other studies. For example, Murakami et al. reported one discordant case among 12 specimens with ALK rearrange-ment; the result was negative with 5A4 IHC but positive with D5F3 IHC (Murakami 2012). Conklin et al. compared five combinations of antibody clones and detection systems, and the concordance was highest with 5A4 and D5F3 with the ADVANCE system (Dako), but a heterogeneous positive reaction was detected in a specimen that was ALK negative on FISH (Conklin 2013).
Multiplex or Quantitative RT-PCR versus FISH (with or without IHC)Although EML4-ALK transcripts were found in the tumor cells of nine NSCLCs but also in the normal lung in only one study (Martelli 2008); the presence of such transcripts in normal lung tissue has not been confirmed by others, which has led to the questioning of those data (Mano 2010, Sasaki 2010). RT-PCR is a highly sensitive method associated with high specificity and no false-positive results; however, there is a risk of false-negative results because of the difficulty in obtaining high-quality RNA from FFPE specimens. Although the false-negative rate of RT-PCR has not been addressed in detail, successful detection of ALK transcripts in a prospective manner has been reported (Soda 2012). In that study, 108 (12%) of 916 specimens were excluded because RNA was of poor qual-ity. EML4-ALK transcripts were detected in 36 specimens, 15 of which were available for IHC; all 15 specimens were ALK positive by IHC. Overall, the sensitivity and specificity of RT-PCR for detection of ALK transcripts, compared with IHC and FISH, are good, ranging from 94% to 100% (Table 6) (Takeuchi 2008, Inamura 2008, Takeuchi 2009, Soda 2013).
Table 6. Comparison of Results of RT-PCR with the Results of Other Methods of ALK Testing
StudyType of RT-PCR
IHC Antibody
FISHRT-PCR Sensitivity
(vs. FISH and/or IHC)RT-PCR Specificity
(vs. FISH and/or IHC)
Inamura et al., 2008
Multiplex RT- PCR ALK1 None 100% (vs. IHC) 100% (vs. IHC)
Takeuchi et al., 2008
Multiplex RT-PCR – FISH-based fusion assay 100% (vs. FISH) 100% (vs. FISH)
Takeuchi et al., 2009
Inverse andmultiplex RT-PCR
5A4 ALK1
EML4 and KIF5B fusion assay
100% (vs. IHC) 100% (vs. IHC)
Soda et al., 2012
Multiplex RT-PCR 5A4 ALK break-apart probe kit
100% (vs. IHC)94% (vs. FISH)
100% (vs. IHC)100% (vs. FISH)
The ALK1 antibody in the studies by Inamura et al. and Takeuchi et al. (2009) is a product of Dako. The 5A4 antibody in the study by Takeuchi et al. (2009) is a product of Abcam and, in the study by Soda et al., is a product of Nichirei Biosciences, Inc. In the study by Soda et al., the break-apart probe kit is a product of Abbott Molecular.
CISH versus Other MethodsCISH has some advantages over FISH, and studies have shown that the results of CISH are comparable with those of other methods of detecting ALK rearrangement (Table 7) (Kim 2011, Yoshida 2011a, Schildhaus 2013). In one study, the ALK-positive criteria for CISH were the same as those for FISH, but in another study, the researchers found that a different cutoff value for CISH led to better separation of ALK-positive and ALK-negative tumors (Schildhaus 2013, Yoshida 2011a). A new dual technology

50IASLC ATLAS OF ALK TESTING IN LUNG CANCER
has been developed in which ALK copy number and ALK protein expression are evaluated in the same cells (Ventana Medical Systems, Inc.) (Nitta 2013), and the method has demonstrated greater sensitivity than conventional IHC, providing more accurate assessment of ALK status. However, the assay is technically difficult. Further validation of this technology is ongoing.
Table 7. Comparison of CISH with with Other Methods of ALK Testing
CISH FISH IHC RT-PCR
Study Assay KitNo. of
Specimens (% of ALK+)
Criteria for
PositivitySensitivity Specificity Sensitivity Specificity Sensitivity Specificity
Kim et al., 2011
ALK dual-color break-apart
CISH
431 (4%) Not stated 94% 100% 66.7% 100% NA NA
Yoshida et al., 2011a
ALK dual-color break-apart
CISH
45 (31%) ≥20% cells with split
signals
100% 100% 93% 100% 93% 100%
Schildhaus et al., 2013
ZytoDot 2C SPEC ALK break-apart
probe
100 (16%) ≥15% cells with split
signals
100% 100% NA NA NA NA
The assay kit used in the studies by Kim et al. and Yoshida et al. is a product of Ventana Medical Systems, Inc. The kit used in the study by Schildhaus et al. is a product of ZytoVision GmbH.
NA = not available.
Figure 1. Algorithm proposed by the Japanese Lung Cancer Society, with screen-ing by IHC and confirmation by FISH; RT-PCR is used for cytology specimens. Dotted lines represent possible duplicate examination according to clinicopathologic features. Dotted lines indicate possible duplicated examination according to clinicopathologic features. Modified, with permission from, Biomarker Committee, Japanese Lung Cancer Society. guidance for ALK gene Testing in Lung Cancer Patients. Version 1.0 August 1, 2011. Available at http://www.haigan.gr.jp/uploads/photos/641.pdf. FISH
Negative
(rare)
Positive
ALK inhibitor
PositiveNegative
Lung CancerSamples
Negative Positive
Cytology samples, frozen
RT-PCR
IHC
Examples of Diagnostic Algorithms for ALK Testing Based on the advantages and characteristics of individual methods for detecting ALK, several investi-gator groups have proposed diagnostic algorithms for conducting ALK testing (Figures 1-6) (Japanese Lung Cancer Society 2011, Kim 2011, Paik 2011, Thunnissen 2012b, Conklin 2013, Marchetti 2013).
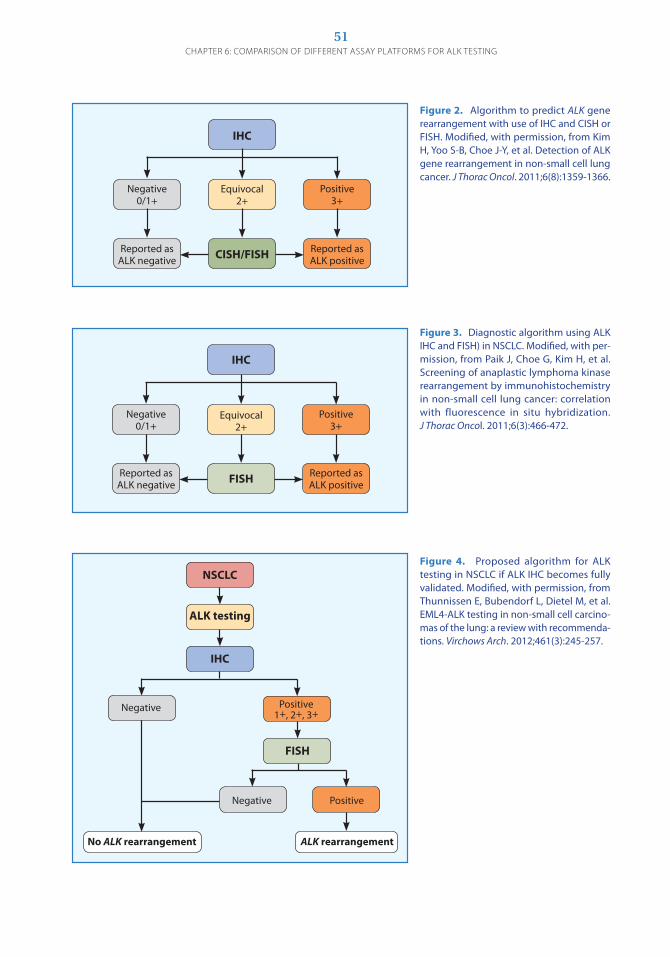
51ChApTER 6: COmpARISON OF dIFFERENT ASSAy pLATFORmS FOR ALK TESTING
Negative0/1+
Reported as ALK negative
IHC
Equivocal2+
FISH
Positive3+
Reported as ALK positive
Figure 3. Diagnostic algorithm using ALK IHC and FISH) in NSCLC. Modified, with per-mission, from Paik J, Choe g, Kim H, et al. Screening of anaplastic lymphoma kinase rearrangement by immunohistochemistry in non-small cell lung cancer: correlation with fluorescence in situ hybridization. J Thorac Oncol. 2011;6(3):466-472.
Negative0/1+
Reported as ALK negative
IHC
Equivocal2+
CISH/FISH
Positive3+
Reported as ALK positive
Figure 2. Algorithm to predict ALK gene rearrangement with use of IHC and CISH or FISH. Modified, with permission, from Kim H, Yoo S-B, Choe J-Y, et al. Detection of ALK gene rearrangement in non-small cell lung cancer. J Thorac Oncol. 2011;6(8):1359-1366.
NSCLC
ALK testing
IHC
ALK rearrangementNo ALK rearrangement
Negative Positive1+, 2+, 3+
FISH
Negative Positive
Figure 4. Proposed algorithm for ALK testing in NSCLC if ALK IHC becomes fully validated. Modified, with permission, from Thunnissen E, Bubendorf L, Dietel M, et al. EML4-ALK testing in non-small cell carcino-mas of the lung: a review with recommenda-tions. Virchows Arch. 2012;461(3):245-257.
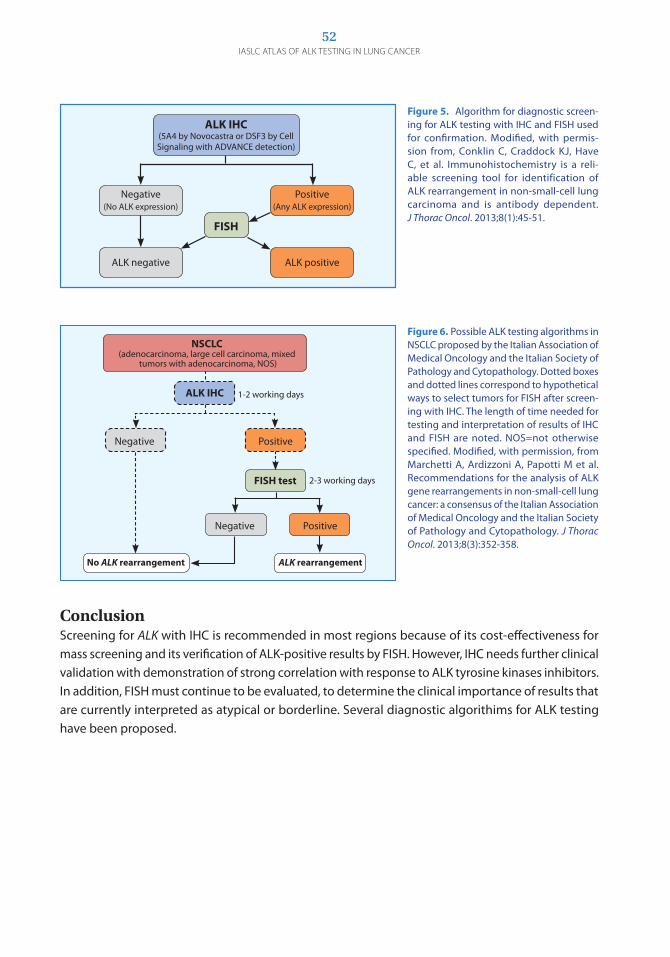
52IASLC ATLAS OF ALK TESTING IN LUNG CANCER
ALK IHC(5A4 by Novocastra or DSF3 by Cell Signaling with ADVANCE detection)
FISH
Negative(No ALK expression)
ALK negative
Positive(Any ALK expression)
ALK positive
Figure 5. Algorithm for diagnostic screen-ing for ALK testing with IHC and FISH used for confirmation. Modified, with permis-sion from, Conklin C, Craddock KJ, Have C, et al. Immunohistochemistry is a reli-able screening tool for identification of ALK rearrangement in non-small-cell lung carcinoma and is antibody dependent. J Thorac Oncol. 2013;8(1):45-51.
ALK rearrangementNo ALK rearrangement
FISH test
Negative Positive
2-3 working days
PositiveNegative
ALK IHC 1-2 working days
NSCLC(adenocarcinoma, large cell carcinoma, mixed
tumors with adenocarcinoma, NOS)
Figure 6. Possible ALK testing algorithms in NSCLC proposed by the Italian Association of Medical Oncology and the Italian Society of Pathology and Cytopathology. Dotted boxes and dotted lines correspond to hypothetical ways to select tumors for FISH after screen-ing with IHC. The length of time needed for testing and interpretation of results of IHC and FISH are noted. NOS=not otherwise specified. Modified, with permission, from Marchetti A, Ardizzoni A, Papotti M et al. Recommendations for the analysis of ALK gene rearrangements in non-small-cell lung cancer: a consensus of the Italian Association of Medical Oncology and the Italian Society of Pathology and Cytopathology. J Thorac Oncol. 2013;8(3):352-358.
ConclusionScreening for ALK with IHC is recommended in most regions because of its cost-effectiveness for mass screening and its verification of ALK-positive results by FISH. However, IHC needs further clinical validation with demonstration of strong correlation with response to ALK tyrosine kinases inhibitors. In addition, FISH must continue to be evaluated, to determine the clinical importance of results that are currently interpreted as atypical or borderline. Several diagnostic algorithims for ALK testing have been proposed.

Role of Cytology in NSCLCFISH testing for detection of ALK rearrangement as a predictive marker in NSCLC was initially approved for testing of biopsy material (Kwak 2010). Biopsy material is often preferred for translational studies in clinical trials because paraffin blocks are routinely processed in pathology laboratories and these blocks provide multiple sections for various analyses. However, as many as 40% of all advanced NSCLC are diagnosed by cytologic evaluation alone, with no concurrent histologic examination of biopsy material. Thus, reliance on histology as the only source for ALK testing would require repeat biopsy in a large proportion of patients, emphasizing the necessity to expand ALK analysis to cytologic specimens. FISH analysis of cytologic specimens has a long tradition, and FISH technology was used to evaluate cell lines or disaggregated intact nuclei from histologic tumor specimens before it became applicable to tissue sections. FISH is also an established method in several fields of diagnostic cytol-ogy. From an analytic point of view, there is no rationale against applying ALK FISH to cytologic specimens. In fact, cytologic specimens have several advantages; for example, in contrast to histo-logic sections, the nuclei on cytology smears are not truncated, which allows for the detection of the true number of FISH signals in a nucleus. Cytology is an attractive, minimally invasive method to collect tumor material for repetitive bio-marker analysis on recurrent or metastatic disease. Cytologic diagnosis of NSCLC is typically based on EBUS-FNA, transthoracic FNA, bronchial secretions or brushes, bronchoalveolar lavages, and pleural effusions or FNA from other metastatic sites. Processing such specimens for FFPE cell blocks has become the preferred method in many laboratories, as cell blocks can be handled in the same way as histologic specimens, and the same protocols for biomarker analysis can be applied (Figure 1) (Alici 2013, Kalhor 2013). Aside from the ability to generate more material with repeated sec-tioning, cell blocks also have the advantage of long-term preservation of protein or
ALK Analysis in CytologyBy Lukas Bubendorf
ChApter 7
Figure 1. Pleural effusion of a pulmonary adenocarcinoma. 1A: Papanicolaou-stained conventional smear. 1B: H & E-stained section of a cell block (x 400).
50 µm 50 µmA B
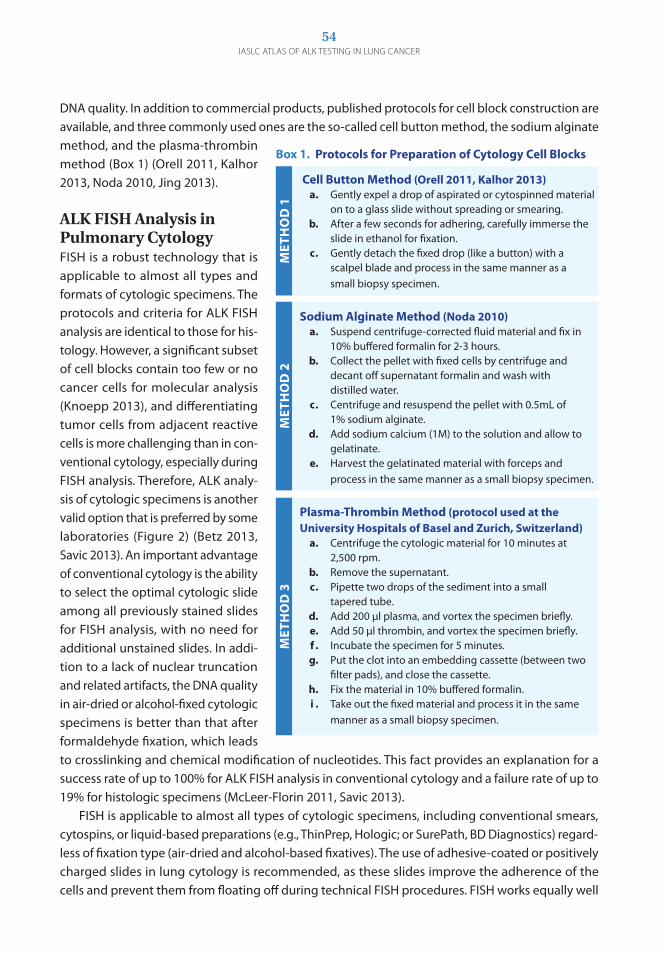
54IASLC ATLAS OF ALK TESTING IN LUNG CANCER
DNA quality. In addition to commercial products, published protocols for cell block construction are available, and three commonly used ones are the so-called cell button method, the sodium alginate method, and the plasma-thrombin method (Box 1) (Orell 2011, Kalhor 2013, Noda 2010, Jing 2013).
ALK FISH Analysis in Pulmonary CytologyFISH is a robust technology that is applicable to almost all types and formats of cytologic specimens. The protocols and criteria for ALK FISH analysis are identical to those for his-tology. However, a significant subset of cell blocks contain too few or no cancer cells for molecular analysis (Knoepp 2013), and differentiating tumor cells from adjacent reactive cells is more challenging than in con-ventional cytology, especially during FISH analysis. Therefore, ALK analy-sis of cytologic specimens is another valid option that is preferred by some laboratories (Figure 2) (Betz 2013, Savic 2013). An important advantage of conventional cytology is the ability to select the optimal cytologic slide among all previously stained slides for FISH analysis, with no need for additional unstained slides. In addi-tion to a lack of nuclear truncation and related artifacts, the DNA quality in air-dried or alcohol-fixed cytologic specimens is better than that after formaldehyde fixation, which leads to crosslinking and chemical modification of nucleotides. This fact provides an explanation for a success rate of up to 100% for ALK FISH analysis in conventional cytology and a failure rate of up to 19% for histologic specimens (McLeer-Florin 2011, Savic 2013). FISH is applicable to almost all types of cytologic specimens, including conventional smears, cytospins, or liquid-based preparations (e.g., ThinPrep, Hologic; or SurePath, BD Diagnostics) regard-less of fixation type (air-dried and alcohol-based fixatives). The use of adhesive-coated or positively charged slides in lung cytology is recommended, as these slides improve the adherence of the cells and prevent them from floating off during technical FISH procedures. FISH works equally well
MET
HO
D 3
MET
HO
D 2
Cell Button Method (Orell 2011, Kalhor 2013) a. gently expel a drop of aspirated or cytospinned material on to a glass slide without spreading or smearing. b. After a few seconds for adhering, carefully immerse the slide in ethanol for fixation. c. gently detach the fixed drop (like a button) with a scalpel blade and process in the same manner as a small biopsy specimen.
Sodium Alginate Method (Noda 2010) a. Suspend centrifuge-corrected fluid material and fix in 10% buffered formalin for 2-3 hours. b. Collect the pellet with fixed cells by centrifuge and decant off supernatant formalin and wash with distilled water. c. Centrifuge and resuspend the pellet with 0.5mL of 1% sodium alginate. d. Add sodium calcium (1M) to the solution and allow to gelatinate. e. Harvest the gelatinated material with forceps and process in the same manner as a small biopsy specimen.
Plasma-Thrombin Method (protocol used at the University Hospitals of Basel and Zurich, Switzerland) a. Centrifuge the cytologic material for 10 minutes at 2,500 rpm. b. Remove the supernatant. c. Pipette two drops of the sediment into a small tapered tube. d. Add 200 μl plasma, and vortex the specimen briefly. e. Add 50 μl thrombin, and vortex the specimen briefly. f . Incubate the specimen for 5 minutes. g. Put the clot into an embedding cassette (between two filter pads), and close the cassette. h. Fix the material in 10% buffered formalin. i . Take out the fixed material and process it in the same manner as a small biopsy specimen.
Box 1. Protocols for Preparation of Cytology Cell Blocks
MET
HO
D 1

55ChApTER 7: ALK ANALySIS IN CyTOLOGy
on unstained specimens as well as those processed with Papanicolaou, hematoxylin, or a modi-fied giemsa stain, and a separate procedure is not usually required, except for when a modified giemsa stain is used and de-staining with an acid-alcohol technique is recommended before FISH analysis (Betz 2013). Notably, FISH also applies well to immunocytochemically stained specimens if 3-amino-9-ethylcarbazol (AEC) is used as a chromogen; use of 3, 3' diaminobenzidine (DAB) can interfere with the FISH signals because of autofluorescence. A protocol for FISH on stained cytologic specimens has been published (Thunnissen 2012b). There may be concerns about using diagnostic cytologic slides for FISH analysis because of a legal requirement that cytology laboratories archive diagnostic slides for several years and the potential need to review slides related to rare cases even years after diagnosis. These concerns can be addressed by capturing representative images or by scanning the whole slide before analysis. It is also possible to re-stain slides after FISH analysis (Betz 2013).
Figure 2. Representative findings on ALK FISH testing of on conventional cytologic slides or previously Papanicolaou-stained tissue (compressed z-stacked images showing the projection of all FISH signals in the intact cell nuclei). 2A and 2B: Two ALK-negative cancers with three normal (fused) ALK signals (2A), and with higher numbers of normal ALK signals per tumor cell nucleus (2B). 2C and 2D: Two ALK-positive cancers with one or two break-apart signals (a distance between green and red signals of at least two times the diameter of the signal) (2C) or a single red signal with no corresponding green signal in addition to several normal signals per tumor cell nucleus (2D).
A B
C D

56IASLC ATLAS OF ALK TESTING IN LUNG CANCER
The threshold for a positive ALK FISH result was established on the basis of analysis of histologic samples (a signal pattern typical for ALK rearrangement in at least 15% of cancer cells), but each individual laboratory needs to determine its own threshold for ALK-negative cytologic specimens until consensus recommendations become available. (See Chapter 3 for more information on cutoff values.) Nonoverlapping tumor cells should be selected for ALK FISH, but most three-dimensional clusters remain amenable to ALK analysis, as the detection of rearrangement signals is not hampered by three-dimensionality. For specimens with a low proportion of tumor cells, use of an automated stage guided by appropriate software to reposition the cancer cells increases the precision of analysis and facilitates review of the FISH result.
ALK IHC in CytologyImmunohistochemistry to detect overexpression of the ALK protein has recently emerged as a valu-able method to screen NSCLC for subsequent FISH analysis and for further evaluation of uncertain FISH findings (as described in detail in Chapter 4 ). As with histologic specimens, ALK IHC is equally promising with cytologic specimens, including cell blocks and conventional or liquid-based cyto-logic preparations (Moreira 2012, Martinez 2013, Savic 2013, Tanaka 2013). The accuracy of ALK IHC on Papanicolaou-stained cytologic slides has been high, with a sensitivity and specificity of almost 100% compared with ALK FISH (Savic 2013, Tanaka 2013). This accuracy was achieved with the 5A4 antibody (Novocastra, See Chapter 6 ) and an automated immunostainer (Bond-Max; Leica Biosystems) (Figures 3 and 4). Additional studies are needed to validate this antibody on other platforms and to test the performance of a new standardized ALK IHC assay using the D5F3 antibody (Ventana Medical Systems, Inc.) in cytology.
Figure 3. IHC on conventional cytologic slides from malignant pleural effusions of pulmonary adenocarcinoma (x 200), showing ALK-negative (3A) and ALK-positive (3B, 3C) tumors, with an ALK-rearranged H2228 cell line used as a positive control (3D). The 5A4 antibody (Novocastra) and an automated immunostainer (Bond-Max; Leica Biosystems) were used, and all results were confirmed by FISH.
A B
C D

57ChApTER 7: ALK ANALySIS IN CyTOLOGy
Because IHC is broadly available, the number of pathology laboratories using IHC as a first means of ALK testing may increase and limit FISH analysis to equivocal or positive findings on IHC, provided that standardized assays and appropriate external quality-control programs are in place both for histologic and cytologic specimens. RT-PCRRT-PCR may be used to analyze cytologic specimens (Betz 2013, Mitiushkina 2013). As discussed in chapter 6, RT-PCR may be adequate for confirming the results of ALK IHC or FISH, but is less appropriate for primary screening for ALK rearrangement.
ConclusionCytologic preparations, including conventional slides and cell blocks can be used as a useful alternative to biopsy specimens for predictive ALK analysis.
Figure 4. ALK IHC of an ALK-positive pulmonary adenocarcinoma (x 200), with testing done with the 5A4 antibody (Novocastra) on a slide with previously Papanicolaou-stained tissue (4A) and corresponding cell block sections stained with the 5A4 antibody (4B), and the D5F3 antibody (Ventana Medical Systems, Inc.) (4D).
A
B
C
Consistent with the standard reporting of the molecular pathologic diagnosis of tumors, ALK testing reports should include four sections: preanalytic, analytic, results, and interpretation/conclusion, regardless of the diagnostic method used FISH, IHC, or RT-PCR].
Preanalytic Section In addition to patient identifiers, this section of a standard report should include a summary of the specimen type and diagnosis, if the molecular diagnosis is not part of the pathologic report being issued at the same time. The following details should be reported.
Specimen features •Specimensizeandtype:surgicalresection(lobectomy,pneumonectomy,segmentectomy,
wedge), biopsy (bronchial/transbronchial biopsy, core-needle biopsy), FNA for cytology, fluid (pleural, cerebral spinal fluid)
•Tissuepreservation:snap-frozen(storagetemperature)orFFPE•Tissuefixation:thefixationtimeanddurationandthefixativeused(onlybufferedformalinis
recommended for FFPE); if tissue has been processed with decalcification solution, this should be documented, as well as the reagent used
Tumor histologic diagnosisFor adenocarcinoma, the type and subtype should follow the 2011 IASLC/American Thoracic Society/European Respiratory Society lung adenocarcinoma classification (Travis 2011). Tumors with more than one type should be described as such: adenosquamous carcinoma, combined small cell lung cancer with adenocarcinoma, and large cell neuroendocrine carcinoma (pure or combined with adenocarcinoma). If more than one pattern or histologic type is present in the same tumor, the predominant histologic type in the testing sample should be stated, and if not, the type tested should be documented.
Tumor assessment • Estimateoftumorcellularity(percentageoftumorcellnucleicomparedwithallnucleipresent
on the section) of the whole section, to obtain an impression of whether the sample has suf-ficient tumor cells for IHC, FISH, and/or RT-PCR
Reporting of ALK Testing By Elisabeth Brambilla, Erik Thunnissen, Marileila Varella-Garcia, and Yasushi Yatabe
ChApter 8
59ChApTER 8: REpORTING OF ALK TESTING
• Percentageoftumorcellsoninitialsection/blockandoptionallyaftercancer-cellenrichment,such as macrodissection, to reflect the tumor cellularity of the sample part used for DNA/RNA isolation
• Extentofnecrosis,inflammatorycellinfiltrates,anthracosis,andtissueartifacts• Testresultsofadditionaldiagnosticimmunohistochemicalmarkers,suchasthyroidtranscrip-
tion factor-1 (TTF-1), p63/p40, and mucin stains, if available (Thunnissen 2012a)
Overall specimen adequacy• Documentedas“adequatefortesting”(relativetothefindingsnotedhere,aswellasforALK
testing) or as “suboptimal” (with notation of the reason or reasons)
Other information• Pastdrugtreatment,ifavailable(optional)
Analytic SectionThis section should include the basic methodology for each assay used, along with the assay sensitiv-ity and threshold. The information should be sufficient enough for another laboratory to understand what was done, in the event of a discrepancy between laboratories, or if asked to repeat testing.•ALKFISH:probeset(manufacturer,type)andthresholdusedtodefineapositiveresult•ALKIHC:antibodytype(source),antibodyconcentration,incubationtimeandtemperature,and
secondary signal enhancement system•ALKRT-PCR:methodused,primers,probesandtheirreferences,andassaysensitivity
Results SectionThis section should report the outcome of the test, including incidental findings and variants of uncertain significance. Inconclusive results should be clearly reported as such. The results should be reported as positive or negative for ALK rearrangement so that oncologists and nonspecialist pathologists can readily understand the results. In addition, specific elements should be reported according to the testing method used.
ALK FISH: the number of cells analyzed and the number and percentage of cells displaying positive patterns; if an atypical pattern was seen, it should be noted (for example, “negative for ALK rearrangement, see Interpretation”); if International Systems for Human Cytogenetic Nomenclature (ISCN) is used, it should be accompanied by an easily understandable discrete result
ALK IHC: The result should be reported as positive, negative, or indeterminate; when the result is indeterminate, an explanation should be provided (e.g., tumor tissue exhaustion, insufficient number of tumor cells); other optional results are the modified H-score (the percentage of stained nuclei, the intensity of staining, and the staining pattern [cytoplasmic and/or membra-nous]) and the homogeneity of staining. To ensure the validity of the technique, an external positive control is required for all tests. This positive control can be a cell block with an ALK-rearranged cell line or an ALK-positive tumor specimen.
60IASLC ATLAS OF ALK TESTING IN LUNG CANCER
ALK RT-PCR: the names of any clinically significant mutations that have been identified; the fusion pattern, such as “variant 1,” has been used, but it is recommended to use descriptions (Soda 2012) such as “EML4-ALK (E13;A20)” for variant 1 and “EML4-ALK (E14;A20 E14;ins11del49A20)” for variant 4. (Additional information is available at http://atlasgeneticsoncology.org/Tumors/inv2p21p23NSCCLungID5667.html.)
Interpretation/Conclusion SectionThis section should include the following.•Specimentypeanddiagnosis(primaryoraftertreatmentwithanALKinhibitor)•Easilyunderstandableclinicalinterpretation,includingoutcomeofthemoleculartestandan
overall statement of the likelihood that the cancer will respond to or resist ALK inhibitor therapy (considering also the clinical evidence)
•Explanation(asbestasisknown)foraninconclusiveresultordiscrepantresultswithmultipletesting, whether due to assay failure, insufficient specimen, or another reason (e.g., atypical FISH patterns) and suggestion of requirements for testing a different specimen that would be more likely to yield a successful result
ConclusionReports on the results of ALK testing should include sufficient details for both laboratory physicians and clinicians to understand the origin and features of the sample tested, the nature of the test performed, and the accuracy and potential clinical utility of the results.

ChApter 9
With the development of ALK targeted therapy for NSCLC, several oncology and pathology organi-zations around the world have established recommendations for ALK testing, either as stand-alone documents or as part of broader guidelines on molecular testing. In addition, several regional or international multicenter studies have been conducted to standardize ALK testing protocols across laboratories.
Guidelinesguidelines for molecular testing on lung cancer specimens may include clinical and methodologic recommendations. In 2011, the European Society for Medical Oncology (ESMO) noted that routine ALK testing could not be recommended at that time, but acknowledged that emerging data may lead to a clinical indication for such testing (Felip 2011). Since then, several expert groups have published consensus opinion and recommendations for molecular testing in lung cancer, including testing for ALK gene rearrangement (Table 1). The most comprehensive guideline is the result of a collaborative effort by experts representing CAP, IASLC, and AMP. This effort was based on a systematic review of studies published before February 2012. (See Appendix 2 for a summary of the recommendations in this guideline.) The guideline recommends that all patients with advanced NSCLC be tested for ALK gene rearrangement if the tumor is of adenocarcinoma subtype or has an adenocarcinoma com-ponent. Testing for ALK gene rearrarrangement should also be performed if the specimen is small and an adenocarcinoma component cannot be excluded. (Lindeman 2013). Similar to testing for the EGFR mutation, it is necessary for a pathologist to be involved in the selection of tissue samples to determine the adequacy of specimens. The current testing methodology of choice is the ALK FISH break-apart assay (Vysis LSI Break Apart FISH Probe Kit, Abbott Molecular), which is currently the only US FDA-approved test to determine eligibility for treatment with an ALK inhibitor. However, the guideline states that ALK IHC can be used for ALK screening if a validated IHC assay is used. Standardization StudiesIn the United States, the label for crizotinib notes the requirement for ALK testing with a US FDA-approved assay. Currently, the ALK FISH break-apart assay (Abbott Molecular) is the only such approved ALK FISH assay. In other parts of the world, regulatory agencies do not mandate the use of a specific method but they do require the use of a validated assay. In these countries, other methods or assays may be used if they have been standardized to detect ALK gene rearrangement. The expert
Guidelines and Standardization StudiesBy Yasushi Yatabe, Sylvie Lantuéjoul, Erik Thunnissen, Keith Kerr, and Ming Sound Tsao
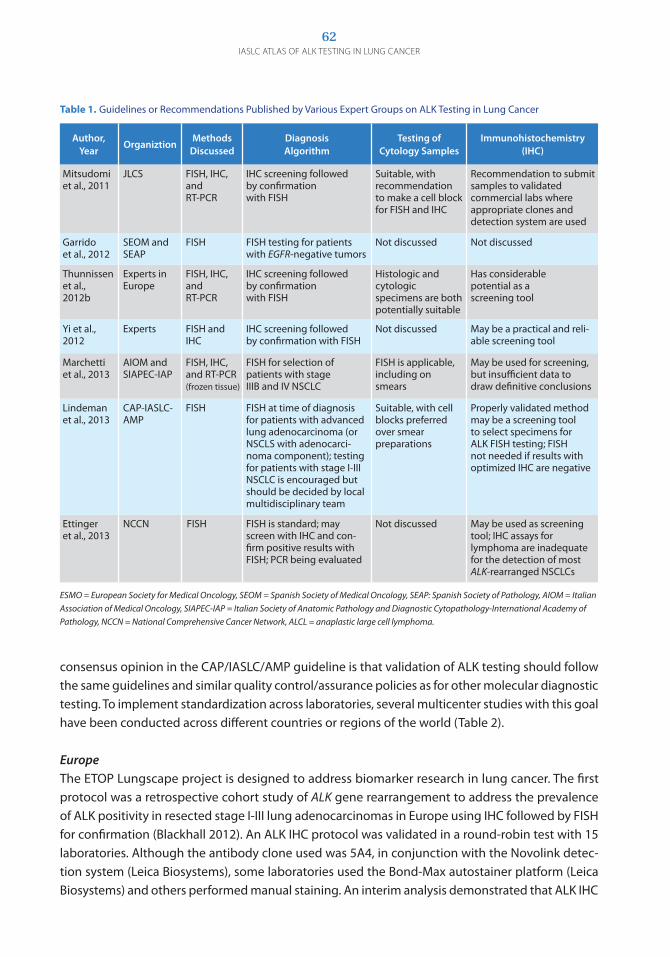
62IASLC ATLAS OF ALK TESTING IN LUNG CANCER
consensus opinion in the CAP/IASLC/AMP guideline is that validation of ALK testing should follow the same guidelines and similar quality control/assurance policies as for other molecular diagnostic testing. To implement standardization across laboratories, several multicenter studies with this goal have been conducted across different countries or regions of the world (Table 2).
Europe The ETOP Lungscape project is designed to address biomarker research in lung cancer. The first protocol was a retrospective cohort study of ALK gene rearrangement to address the prevalence of ALK positivity in resected stage I-III lung adenocarcinomas in Europe using IHC followed by FISH for confirmation (Blackhall 2012). An ALK IHC protocol was validated in a round-robin test with 15 laboratories. Although the antibody clone used was 5A4, in conjunction with the Novolink detec-tion system (Leica Biosystems), some laboratories used the Bond-Max autostainer platform (Leica Biosystems) and others performed manual staining. An interim analysis demonstrated that ALK IHC
Table 1. guidelines or Recommendations Published by Various Expert groups on ALK Testing in Lung Cancer
Author, Year
OrganiztionMethods
DiscussedDiagnosis Algorithm
Testing of Cytology Samples
Immunohistochemistry (IHC)
Mitsudomi et al., 2011
JLCS FISH, IHC, and RT-PCR
IHC screening followed by confirmation with FISH
Suitable, with recommendation to make a cell block for FISH and IHC
Recommendation to submit samples to validated commercial labs where appropriate clones and detection system are used
garrido et al., 2012
SEOM and SEAP
FISH FISH testing for patients with EGFR-negative tumors
Not discussed Not discussed
Thunnissen et al., 2012b
Experts in Europe
FISH, IHC, and RT-PCR
IHC screening followed by confirmation with FISH
Histologic and cytologic specimens are both potentially suitable
Has considerable potential as a screening tool
Yi et al., 2012
Experts FISH and IHC
IHC screening followed by confirmation with FISH
Not discussed May be a practical and reli-able screening tool
Marchetti et al., 2013
AIOM and SIAPEC-IAP
FISH, IHC, and RT-PCR (frozen tissue)
FISH for selection of patients with stage IIIB and IV NSCLC
FISH is applicable, including on smears
May be used for screening, but insufficient data to draw definitive conclusions
Lindeman et al., 2013
CAP-IASLC- AMP
FISH FISH at time of diagnosis for patients with advanced lung adenocarcinoma (or NSCLS with adenocarci-noma component); testing for patients with stage I-III NSCLC is encouraged but should be decided by local multidisciplinary team
Suitable, with cell blocks preferred over smear preparations
Properly validated method may be a screening tool to select specimens for ALK FISH testing; FISH not needed if results with optimized IHC are negative
Ettinger et al., 2013
NCCN FISH FISH is standard; may screen with IHC and con-firm positive results with FISH; PCR being evaluated
Not discussed May be used as screening tool; IHC assays for lymphoma are inadequate for the detection of most ALK-rearranged NSCLCs
ESMO = European Society for Medical Oncology, SEOM = Spanish Society of Medical Oncology, SEAP: Spanish Society of Pathology, AIOM = Italian Association of Medical Oncology, SIAPEC-IAP = Italian Society of Anatomic Pathology and Diagnostic Cytopathology-International Academy of Pathology, NCCN = National Comprehensive Cancer Network, ALCL = anaplastic large cell lymphoma.

63ChApTER 9: GUIdELINES ANd STANdARdIzATION STUdIES
Table 2. Multicenter Standardization Studies for ALK Testing Methods
Country Methods
EvaluatedParticipants No. of Specimens Study Type
Europe (ETOP)
IHC and FISH 15 laboratories 1,099 (69 ALK-positive) Round-robin test; retrospective analysis
Canada IHC and FISH 12 Canadian pathology laboratories
28 (22 ALK positive) Testing by individual laboratory protocols , followed by protocol adjustment after consensus meeting and further validation by repeat testing
Japan IHC, FISH, and quantitative RT-PCR
Nationwide screening for 3 months
2,884 (213 ALK positive) Prospective screening
France IHC, FISH, and RT-PCR
15 French thoracic pathology departments
459 (85 ALK positive) Addressing concordance among testing methods in the central laboratories
germany IHC and FISH Experts at 8 german institutes of pathology
10 (5 ALK positive) Round-robin test of known ALK status
Europe (European Society of Pathology)
IHC, FISH, and digital FISH images
80 and 150 laboratories for first and second rounds, respectively
6 resected specimens (2 ALK positive), 6 cell lines (2 ALK positive) and 4 digital images (2 ALK positive)
Round-robin test of known ALK status
was positive in 69 (6.3%) of 1,099 specimens of adenocarcinoma; the score was 3+ in 23 specimens (33.3%), 2+ in eight specimens (11%) and 1+ in 38 specimens (55%). To access concordance, an ALK IHC positive/negative 1:2 matched cohort (n = 207) was evaluated with use of FISH. FISH results were concordant in 22 (37%) of 60 ALK IHC-positive tumors and in 137 (99%) of 138 ALK IHC-negative tumors (Figure 1). This study demonstrates the importance of a clear definition of IHC positivity and what level of IHC positivity may be predictive of ALK gene rearrangement. Using these assay condi-tions applied to the 5A4 antibody, specimens with a score of 1+ or 2+ have a low probability of ALK rearrangement. Similarly, a negative IHC test carries a very high probability of no ALK rearrangement.
Canada The Canadian Anaplastic Lymphoma Kinase (CALK) study was a multicenter study conducted throughout the country to optimize and standardize ALK IHC and FISH, using FISH-confirmed tumors (22 ALK-positive tumors and six ALK-negative tumors) (Tsao 2013). The ALK-positive samples were derived from specimens that had been screened with both IHC and FISH on tissue microarrays con-structed from nearly 2,000 resected lung adenocarcinomas. Anonymized replicate sections were sent to participating laboratories for IHC and FISH testing using the ALK FISH break-apart assay (Abbott Molecular) for FISH; the antibodies ALK1 (Dako; one center), clone 5A4 (Novocastra; 12 centers), and clone D5F3 (Cell Signaling Technology; one center); and the locally available existing autostainer (Dako, Leica Biosystems, or Ventana Medical Systems, Inc.). Independent IHC scores from 12 centers that evaluated the 5A4 antibody and FISH scores from 11 centers were collected and analyzed. The intraclass correlation coefficient (ICC) between centers for IHC was 0.84. After the initial analysis of IHC results and a meeting of participating pathologists to review the slides, protocol adjustments were implemented by individual laboratories. A second-round study was done with the same set
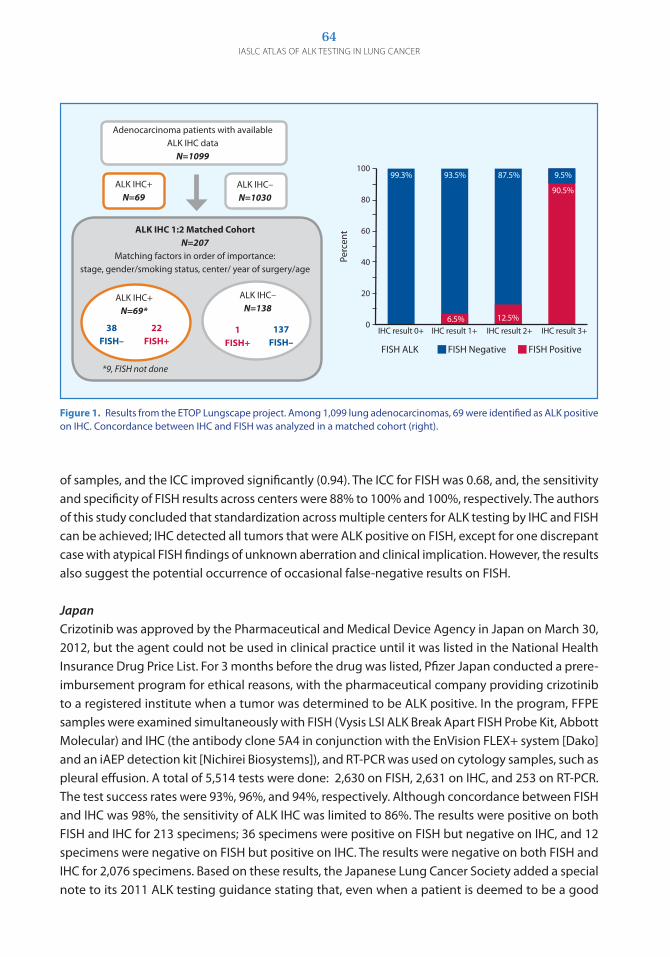
64IASLC ATLAS OF ALK TESTING IN LUNG CANCER
of samples, and the ICC improved significantly (0.94). The ICC for FISH was 0.68, and, the sensitivity and specificity of FISH results across centers were 88% to 100% and 100%, respectively. The authors of this study concluded that standardization across multiple centers for ALK testing by IHC and FISH can be achieved; IHC detected all tumors that were ALK positive on FISH, except for one discrepant case with atypical FISH findings of unknown aberration and clinical implication. However, the results also suggest the potential occurrence of occasional false-negative results on FISH.
JapanCrizotinib was approved by the Pharmaceutical and Medical Device Agency in Japan on March 30, 2012, but the agent could not be used in clinical practice until it was listed in the National Health Insurance Drug Price List. For 3 months before the drug was listed, Pfizer Japan conducted a prere-imbursement program for ethical reasons, with the pharmaceutical company providing crizotinib to a registered institute when a tumor was determined to be ALK positive. In the program, FFPE samples were examined simultaneously with FISH (Vysis LSI ALK Break Apart FISH Probe Kit, Abbott Molecular) and IHC (the antibody clone 5A4 in conjunction with the EnVision FLEX+ system [Dako] and an iAEP detection kit [Nichirei Biosystems]), and RT-PCR was used on cytology samples, such as pleural effusion. A total of 5,514 tests were done: 2,630 on FISH, 2,631 on IHC, and 253 on RT-PCR. The test success rates were 93%, 96%, and 94%, respectively. Although concordance between FISH and IHC was 98%, the sensitivity of ALK IHC was limited to 86%. The results were positive on both FISH and IHC for 213 specimens; 36 specimens were positive on FISH but negative on IHC, and 12 specimens were negative on FISH but positive on IHC. The results were negative on both FISH and IHC for 2,076 specimens. Based on these results, the Japanese Lung Cancer Society added a special note to its 2011 ALK testing guidance stating that, even when a patient is deemed to be a good
Figure 1. Results from the ETOP Lungscape project. Among 1,099 lung adenocarcinomas, 69 were identified as ALK positive on IHC. Concordance between IHC and FISH was analyzed in a matched cohort (right).
Adenocarcinoma patients with available ALK IHC data
N=1099
ALK IHC+ N=69
ALK IHC– N=1030
ALK IHC 1:2 Matched CohortN=207
Matching factors in order of importance: stage, gender/smoking status, center/ year of surgery/age
ALK IHC+ N=69*
38FISH–
22FISH+
*9, FISH not done
ALK IHC– N=138
1FISH+
137FISH–
FISH PositiveFISH NegativeFISH ALK
100
80
60
40
20
0
Perc
ent
IHC result 0+ IHC result 1+ IHC result 3+IHC result 2+
9.5%
90.5%
87.5%99.3% 93.5%
6.5% 12.5%

65ChApTER 9: GUIdELINES ANd STANdARdIzATION STUdIES
candidate for treatment with an ALK inhibitor based on the results of both IHC and FISH, there may be discrepancy between the results of the two tests, and treatment should be determined with careful consideration of the benefit-risk profile (Mitsudomi 2011).
France The French National Cancer Institute (INCa) program, started in 2007, is devoted to the prospective detection of emerging biomarkers in lung cancer, colorectal cancer, and melanoma in 28 hospital-based molecular genetics platforms for cancers. As a part of this program, the French multicenter ALK validation study is being conducted to compare IHC, using 5A4 and D5F3 antibodies (Novocastra, and Cell Signaling Technology, respectively), with FISH and quantitative RT-PCR in a series of 500 FFPE surgical specimens (Lantuéjoul 2013). Among the 459 specimens included to date, 340 were ALK negative on both FISH and IHC and 85 were ALK positive on both FISH and IHC. Among the discordant cases, 15 were negative on FISH and positive on IHC (but with low staining scores); 12 were positive on FISH and negative on IHC. Seven specimens were noninterpretable by FISH, but five of them were ALK positive on IHC. Overall, the sensitivity of IHC versus FISH was 87%, and the specificity was 96%. On quantitative RT-PCR, almost 50% of ALK-positive specimens had variant 1, 30% had variant 3a/b, and less than 5% had variant 2 or 7; 20% were negative or noninterpretable. The authors concluded that IHC with 5A4 is a reliable and easy technique for routine diagnosis of ALK abnormalities, whereas FISH and quantitative RT-PCR still depend on preanalytic conditions and technical expertise. However, no method is absolutely accurate, and when the clinical presentation is suggestive of ALK positivity, despite a negative test result, repeat testing with another method prevents missing a patient who has an ALK-positive tumor.
Germany The german Society of Pathology (Deutsche gesellschaft für Pathologie; DgP) and the Professional Association of german Pathologists (Berufsverband Deutscher Pathologie; BDP) are conducting round-robin tests for the detection of ALK fusion to certifiy the technique in individual institutes. In the pretesting phase of the study, specimens from 10 lung cancer cases were evaluated by experts at eight institutes of pathology to confirm the ALK status with use of FISH and IHC testing (V Laffert 2013). Then, the confirmed lung cancer samples were distributed as a tissue microarray section. The participating institutes used different FISH probes (from either Abbott Molecular or Zytovision gmbH), antibody clones (ALK1, 5A4, and D5F3), dilutions (1:20 to 1:200), and detection system (manual or automated stainer from Ventana Medical Systems, Leica Biosystems, or Dako). ALK-negative tumors were correctly diagnosed with either method (FISH and IHC), whereas diverse results were found for ALK-positive tumors, especially with IHC. The study clearly showed that it is crucial to establish standardized protocols to detect the ALK fusion gene.
Europe A guideline on the requirements of external quality assessment programs for molecular pathology was recently published (van Krieken 2013).The European Society of Pathology conducts a European external quality assessment program for testing biomarker mutations in NSCLC, to ensure optimal accuracy and proficiency in biomarker testing. The program accounts for two external quality assess-ment rounds for ALK testing, in which 80 and 150 laboratories participated. A tissue microarray slide

66IASLC ATLAS OF ALK TESTING IN LUNG CANCER
with cores from FFPE material and digital images of FISH were provided. The data from both rounds will be available at the end of 2013.
International Reproducibility Study of Ventana ALK IHC KitTo study the correlation between IHC and FISH, as well as the reproducibility of the Ventana ALK IHC with the D5F3 antibody (Ventana Medical Systems, Inc.), seven international observers stud-ied 100 evaluable cases. When the results of ALK IHC were correlated with those of ALK FISH, the sensitivity was 90% and the specificity was 95%, with a 93% accuracy relative to FISH. For the IHC interpretation, there was agreement of the IHC interpretation among all seven readers on 95% of the cases and among six of seven readers in 97% of the cases (Hirsch 2013). The authors concluded that there was an excellent intraobserver and interobserver agreement with the Ventana IHC Kit as well as excellent correlation with ALK FISH.
ConclusionAlthough testing for ALK gene rearrangement using break-apart ALK FISH probes is generally recog-nized as a standard diagnostic criterion for ALK TKI therapy, the screening algorithm for detection of ALK-rearranged lung cancer is still under development. groups in all parts of the world are conducting studies to develop national or regional guidelines; most of these studies focus on the standardiza-tion of both IHC and FISH tests, as well as evaluation of the sensitivity and specificity of IHC as a screening tool. As results from these studies are published, it is likely that a global consensus on an ALK screening algorithm may evolve within the next few years.

Treatment results for patients with advanced NSCLC harboring ALK gene rearrangement continues to be encouraging, and the diagnosis of these rearrangements remains challenging. It is now well-established that molecular testing for ALK gene rearrangement is crucial for the optimal choice of therapy for patients with advanced NSCLC, particularly tumors that are an adenocarcinoma or have an adenocarcinoma component. However, several questions still await definite answers.
1. Which patients should be screened for ALK gene rearrangement?2. What is the most cost-effective screening method?3. What is the most optimal screening-diagnosis paradigm for selecting patients for treatment
with ALK inhibitors in order to capture all the patients who may potentially benefit from this therapy?
4. What is the most optimal treatment paradigm based on the current clinical evidence?
Although the last question is beyond the scope of this Atlas, the first three questions have been addressed.
Which Patients Should Be Screened for ALK Gene Rearrangement?There seems to be consensus that, at minimum, screening for ALK gene rearrangement should be done for all patients with advanced NSCLC that is an adenocarcinoma or has an adenocarcinoma component. Depending on resources and academic interest, screening of patients with advanced NSCLC of other histologies should be considered, especially patients with one or more of these fea-tures: younger patient age, never/light smoking history, or negative results on testing for EGFR and KRAS mutations. Occasionally, ALK gene rearrangement is found in tumors with nonadenocarcinoma histologies, although this finding is rare. If the diagnostic specimen is small and an adenocarcinoma component cannot be excluded, ALK testing is recommended. Even though treatment with an ALK inhibitor is not currently recommended for patients with early-stage NSCLC (I-IIIA), molecular testing, including ALK testing, on the surgical specimen is rec-ommended to provide information if disease relapse or advanced disease subsequently occurs.
What Is the Most Cost-effective Screening Method? In the United States, eligibility for crizotinib therapy requires the diagnosis of ALK gene rearrange-ment on an ALK assay that is approved by the US FDA. Currently, only one assay is US FDA approved:
Summary and Future PerspectivesBy Fred R. Hirsch, Yasushi Yatabe, and Ming Sound Tsao
ChApter 10
68IASLC ATLAS OF ALK TESTING IN LUNG CANCER
the ALK FISH break-apart assay (Abbott Molecular). However, no requirement for a specific test for ALK screening has been established. Many studies have confirmed a high diagnostic specificity and sensitivity for ALK IHC compared with ALK FISH, and many guidelines already include recommenda-tions for using ALK IHC to screen for ALK gene rearrangement in large populations of people with NSCLC and verifying positive results on IHC with ALK FISH for treatment eligibility. RT-PCR is not currently recommended for ALK screening.
What Is the Most Optimal Screening-Diagnosis Paradigm for Treatment with an ALK Inhibitor?Although ALK IHC screening has been adopted in many countries, it remains unclear which test results should be verified with ALK FISH. Some guidelines recommend that all tumors that test positively on ALK IHC should be tested on ALK FISH, whereas others suggest that FISH be used to verify IHC results of 1+ and 2+. More detailed clinical-diagnostic associations in terms of response and outcome related to ALK inhibitor therapy is required before the optimal screening-diagnosis paradigm can be determined. Until such additional detailed correlative analysis results are available, the authors recommend that all IHC-positive tumors be verified with ALK FISH. However, there is an increasing number of reports of patients with tumors that are ALK FISH negative but IHC positive who have a good response to crizotinib therapy. In such cases, these negative results on ALK FISH may be true-negative or may be false-negative results because of a borderline or atypical FISH pat-tern. More in-depth analysis of these cases is ongoing and will help answer important questions.
Where Are We Going in the Future?From a therapeutic point of view, several second-generation ALK inhibitors are currently in clinical development, as are dual ALK/EgFR inhibitors, with very encouraging results. Only future studies can tell what diagnostic assay will be associated with the best clinical outcomes. The ALK FISH assay is today the criterion standard for eligibility for treatment with crizotinib and is also being used in clinical studies with next-generation ALK inhibitors. However, treatment correlations with other assays, such as IHC and PCR are under investigation, and the screening-diagnosis paradigm may change in the future. Also, the introduction of new multiplex assays, particularly NgS technologies, needs to be validated both for screening and treatment eligibility of patients with NSCLC for ALK targeted therapy.
ConclusionAs illustrated throughout this Atlas, the diagnostics of ALK gene rearrangement are still developing. In the next couple of years, the diagnostic schema may change, and emergence of new targeted drugs may facilitate that transition. However, we are confident that we can now properly treat the few patients who have NSCLC with this gene alteration. All professionals in this field should ensure that all patients who may potentially benefit from ALK-targeted therapy receive optimal treatment.

69REFERENCES
Alici I, Demirci NY, Yilmaz A, et al. The combination of cytological smears and cell blocks on endobronchial ultrasound-guided transbronchial needle aspirates allows a higher diagnostic yield. Virchows Arch. 2013;462(3):323-327.
Allouche M. ALK is a novel dependence receptor: potential implications in development and cancer. Cell Cycle. 2007;6:1533-1538.
Alrifai D, Popat S, Ahmed M, et al. A rare case of squamous cell carcinoma of the lung harbouring ALK and BRAF activating mutations. Lung Cancer. 2013;80(3):339-340.
An S, Chen ZH, Su J, et al. Identification of enriched driver gene alterations in subgroups of non-small cell lung cancer patients based on histology and smoking status. PLoS One. 2012;7(6):e40109.
Atkins D, Reiffen K-A, Tegtmeier CL, et al. Immunohistochemical detection of EgFR in paraffin-embedded tumor tissues: variation in staining intensity due to choice of fixative and storage time of tissue sections. J Histochem Cytochem. 2004;52(7):893-901.
Babic A, Loftin IR, Stanislaw S, et al. The impact of pre-analytical processing on staining quality for H&E, dual hapten, dual color in situ hybridization and fluorescent in situ hybridization assays. Methods. 2010;52(4):287-300.
Bang Y, Kwak EL, Shaw AT, et al. Clinical activity of the oral ALK inhibitor PF-02341066 in ALK-positive patients with non-small cell lung cancer (NSCLC) J Clin Oncol. 2010;28(18s):(suppl; abstr 3).
Betz B, Dixon CA, Weigelin HC, et al. The use of stained cytologic direct smears for ALK gene rearrangement analysis of lung adenocarcinoma. Cancer Cytopathol. 2013 Mar 27 [Epub ahead of print].
Biomarker Committee, Japanese Lung Cancer Society. Guidance for ALK Gene Testing in Lung Cancer Patients. Version 1.0 August 1, 2011. Available at http://www.haigan.gr.jp/uploads/photos/641.pdf.
Blackhall F, Peters S, Kerr KM, et al. Prevalence and clinical outcomes for patients with ALK gene rearrangement in Europe: preliminary results from the European Thoracic Oncology Platform Lungscape project. Ann Oncol. 2013;23(Suppl 9):ix73.
Boland J, Erdogan S, Vasmatzis g, et al. Anaplastic lymphoma kinase immunoreactivity correlates with ALK gene rearrangement and transcriptional up-regulation in non-small cell lung carcinomas. Hum Pathol. 2009;40(8):1152-1158.
Burnett R, Swanson Beck J, Howatson SR, et al. Observer variability in histopathological reporting of malignant bronchial biopsy specimens. J Clin Pathol. 1994;47(8):711-713.
Bussolati g, Leonardo E. Technical pitfalls potentially affecting diagnoses in immunohistochemistry. J Clin Pathol. 2008;61(11):1184-1192.
Camidge D, Bang YJ, Kwak EL, et al. Activity and safety of crizotinib in patients with ALK-positive non-small-cell lung
cancer: updated results from a phase 1 study. Lancet Oncol. 2012;13(10):1011-1019. (a)
Camidge D, Kono SA, Flacco A, et al. Optimizing the detection of lung cancer patients harboring anaplastic lymphoma kinase (ALK) gene rearrangements potentially suitable for ALK inhibitor treatment. Clin Cancer Res. 2010;16(22):5581-5590.
Camidge DR, Skokan M, Kiatsimkul P, et al. Native and rearranged ALK copy number and rearranged cell count in non-small cell lung cancer. Implications for ALK inhibitor therapy. Cancer. 2013 Sept 10 [Epub ahead of print].
Camidge D, Theodoro M, Maxson DA, et al. Correlations between the percentage of tumor cells showing an anaplastic lymphoma kinase (ALK) gene rearrangement, ALK signal copy number, and response to crizotinib therapy in ALK fluorescence in situ hybridization-positive nonsmall cell lung cancer. Cancer. 2012;118(18):4486-4494. (b)
Chen T, Chang IC, Liu HP, et al. Correlation of anaplastic lymphoma kinase overexpression and the EML4-ALK fusion gene in non-small cell lung cancer by immunohistochemical study. Chang Gung Med J. 2012;35(4):309-317.
Chihara D, Suzuki R. More on crizotinib [letter]. N Engl J Med. 2011;364(8):776-778.
Chuang M, Marchevsky A, Teirstein AS, et al. Diagnosis of lung cancer by fibreoptic bronchoscopy: problems in the histological classification of non-small cell carcinomas. Thorax. 1984;39(3):175-178.
Coghlin C, Smith LJ, Bakar S, et al. Quantitative analysis of tumour in bronchial biopsy specimens. J Thorac Oncol. 2010;5(4):448-452.
Conklin C, Craddock KJ, Have C, et al. Immunohistochemistry is a reliable screening tool for identification of ALK rearrange-ment in non-small-cell lung carcinoma and is antibody dependent. J Thorac Oncol. 2013;8(1):45-51.
Dai Z, Kelly JC, Meloni-Ehrig A, et al. Incidence and patterns of ALK FISH abnormalities seen in a large unselected series of lung carcinomas. Molec Cytogenetics. 2012;5(1):44.
DiVito K, Charette LA, Rimm DL, Camp RL. Long-term preservation of antigenicity in tissue microarrays. Lab Invest. 2004;84(8):1071-1078.
Doebele R, Pilling AB, Aisner DL, et al. Mechanisms of resistance to crizotinib in patients with ALK gene rearranged non-small cell lung cancer. Clin Cancer Res. 2012;18(5):1472-1482.
Eberhard D, giaccone g, Johnson BE; Non-Small-Cell Lung Cancer Working group. Biomarkers of response to epidermal growth factor receptor inhibitors in Non-Small-Cell Lung Cancer Working group: standardization for use in the clinical trial setting. J Clin Oncol. 2008;26(6):983-994.
Edwards S, Roberts C, McKean ME, et al. Preoperative histological classification of primary lung cancer: accuracy of diagnosis and use of the non-small cell category. J Clin Pathol. 2000;53(7):537-540.
References

70IASLC ATLAS OF ALK TESTING IN LUNG CANCER
Felip E, gridelli C, Baas P, et al. Metastatic non-small-cell lung cancer: consensus on pathology and molecular tests, first-line, second-line, and third-line therapy: 1st ESMO Consensus Conference in Lung Cancer; Lugano 2010. Ann Oncol. 2011;22:1507-1519.
gainor J, Varghese AM, Ou SH, et al. ALK rearrangements are mutually exclusive with mutations in EgFR or KRAS: an analysis of 1,683 patients with non-small cell lung cancer. Clin Cancer Res. 2013;19(15):4273-4281.
garrido P, de Castro J, Concha Á et al. guidelines for biomarker testing in advanced non-small-cell lung cancer. A national consensus of the Spanish Society of Medical Oncology (SEOM) and the Spanish Society of Pathology (SEAP). Clin Transl Oncol. 2012;14(5):338-339.
Halling K, Schrijver I, Persons DL. Test verification and validation for molecular diagnostic assays. Arch Pathol Lab Med. 2012;136(1):11-13.
Hirsch F, Yatabe Y, Dietel M, et al. ALK-immunohistochemistry (IHC) standardization with D5F3 antibody in non-small cell lung carcinoma (NSCLC): an international consensus study. J Clin Oncol. 2013;31(May 20 Supplement):e22042.
Huang D KD, Kotsakis A, et al. Multiplexed deep sequencing analysis of ALK kinase domain identifies resistance mutations in relapsed patients following crizotinib treatment. Genomics. 2013 Feb 20 [Epub ahead of print].
Hunt J. Molecular pathology in anatomic pathology practice: a review of basic principles. Arch Pathol Lab Med. 2007; 132(2):248-260.
Inamura K, Takeuchi K, Togashi Y, et al. EML4-ALK fusion is linked to histological characteristics in a subset of lung cancers. J Thorac Oncol. 2008;3:13-17.
Jin g, Jeon HS, Lee EB, et al. EML4-ALK fusion gene in Korean non-small cell lung cancer. J Korean Med Sci. 2012; 27(2):228-230.
Jing X, Li QK, Bedrossian U, Michael CW. Morphologic and immunocytochemical performances of effusion cell blocks prepared using 3 different methods Am J Clin Pathol. 2013; 139(2):177-182.
Jokoji R, Yamasaki T, Minami S, et al. Combination of morpho-logical feature analysis and immunohistochemistry is useful for screening of EML4-ALK-positive lung adenocarcinoma. J Clin Pathol. 2010;63(12):1066-1070.
Kalhor N, Wistuba, II. Perfecting the fine-needle aspirate cell block. Cancer Cytopathol. 2013;121(3):109-110.
Kerr K. Clinical relevance of the new IASLC/ERS/ATS adenocarcinoma classification. J Clin Pathol. 2013 Apr 6 [Epub ahead of print]. (a)
Kerr K, Loo PS, Nicolson MC. Pathology and personalized medicine in lung cancer. Lung Cancer Mange. 2013;2(1):35-46. (b)
Khoury T. Delay to formalin fixation alters morphology and immunohistochemistry for breast carcinoma. Appl Immunohistochem Mol Morphol. 2012;20(6):531-542.
Kim H, Xu X, Yoo SB, et al. Discordance between anaplastic lymphoma kinase status in primary non-small-cell lung cancers and their corresponding metastases. Histopathology. 2013;62(2):305-314.
Kim H, Yoo S-B, Choe J-Y, et al. Detection of ALK gene rearrangement in non-small cell lung cancer. J Thorac Oncol. 2011;6(8):1359-1366.
Knoepp S, Roh MH. Ancillary techniques on direct-smear aspirate slides: a significant evolution for cytopathology techniques. Cancer Cytopathol. 2013;121(3):120-128.
Koivunen J, Mermel C, Zejnullahu K, et al. EML4-ALK fusion gene and efficacy of an ALK kinase inhibitor in lung cancer. Clin Cancer Res. 2008;14(13):4275-4283.
Kwak E, Bang YJ, Camidge DR, et al. Anaplastic lymphoma kinase inhibition in non-small-cell lung cancer. N Engl J Med. 2010;363(18):1693-1703.
Lantuéjoul S, Rouquette I, Begueret H, et al. A French multi-centric and prospective validation study for ALK translocation diagnosis in lung adenocarcinomas J Clin Oncol. 2013;31 (May 20 Supplement):8100.
Li T, Kung HJ, Mack PC, gandara DR. genotyping and genomic profiling of non-small-cell lung cancer: implications for current and future therapies. J Clin Oncol. 2013;31:1039-1049.
Li Y, Li Y, Yang T, et al. Clinical significance of EML4-ALK fusion gene and association with EgFR and KRAS gene mutations in 208 Chinese patients with non-small cell lung cancer. PLoS One. 2013;8(1):e52093.
Lin E, Li L, guan Y, et al. Exon array profiling detects EML4-ALK fusion in breast, colorectal, and non-small cell lung cancers. Mol Cancer Res. 2009;7:1466-1476.
Lindeman N, Cagle PT, Beasley MB, et al. Molecular testing guideline for selection of lung cancer patients for EgFR and ALK tyrosine kinase inhibitors: guideline from the College of American Pathologists, International Association for the Study of Lung Cancer, and Association for Molecular Pathology. J Thorac Oncol. 2013;8(7):823-859.
Lipson D, Capelletti M, Yelensky R, et al. Identification of new ALK and RET gene fusions from colorectal and lung cancer biopsies. Nature Med. 2012;18:382-384.
Lira M, Kim TM, Huang D, et al. Multiplexed gene expression and fusion transcript analysis to detect ALK fusions in lung cancer. J Molec Diag. 2013;15:51-61.
Loo P, Thomas SC, Nicolson MC, et al. Subtyping of undif-ferentiated non-small cell carcinomas in bronchial biopsy specimens. J Thorac Oncol. 2010;5(4):442-447.
Lopes L, Bacchi CE. Anaplastic lymphoma kinase gene rearrangement in non-small-cell lung cancer in a Brazilian population. Clinics (Sao Paulo). 2012;67:845-847.
Mano H, Takeuchi K. EML4-ALK fusion in lung [letter]. Am J Pathol. 2010;176(3):1552-1553.
Marchetti A, Ardizzoni A, Papotti M, et al. Recommendations for the analysis of ALK gene rearrangements in non-small-cell lung cancer: a consensus of the Italian Association of Medical Oncology and the Italian Society of Pathology and Cytopathology. J Thorac Oncol. 2013;8(3):352-358.
Martelli M, Sozzi g, Hernandez L, et al. EML4-ALK rearrangement in non-small cell lung cancer and non-tumor lung tissues. Am J Pathol. 2009;174(2):661-670.

71REFERENCES
Martinez P, Hernandez-Losa J, Montero MA, et al. Fluorescence in situ hybridization and immunohistochemistry as diagnostic methods for ALK positive non-small cell lung cancer patients. PLoS One. 2013;8(2):e52261.
McLeer-Florin A, Moro-Sibilot D, Melis A, et al. Dual IHC and FISH testing for ALK gene rearrangement in lung adenocarcinomas in a routine practice: a French study. J Thorac Oncol. 2012;7(2):348-354.
Minca E, Portier BP, Wang Z, et al. ALK status testing in non-small cell lung carcinoma: correlation between ultrasensitive IHC and FISH. J Mol Diagn. 2013;15(3):341-346.
Mino-Kenudson M, Chirieac LR, Law K, et al. A novel, highly sensitive antibody allows for the routine detection of ALK-rearranged lung adenocarcinomas by standard immu-nohistochemistry. Clin Cancer Res. 2010;16(5):1561-1571.
Mitiushkina N, Iyevleva Ag, Poltoratskiy AN, et al. Detection of EgFR mutations and EML4-ALK rearrangements in lung adenocarcinomas using archived cytological slides. Cancer Cytopathol. 2013;121(7):370-376.
Moreira A, Hasanovic A. Molecular characterization by immunocytochemistry of lung adenocarcinoma on cytol-ogy specimens. Acta Cytol. 2012;56(6):603-610.
Morris S, Kirstein MN, Valentine MB, et al. Fusion of a kinase gene, ALK, to a nucleolar protein gene, NPM, in non-Hodgkin’s lymphoma. Science. 1994;263:1281-1284.
Murakami Y, Mitsudomi T, Yatabe Y. A screening method for the ALK fusion gene in NSCLC. Front Oncol. 2012;2:24.
Nakamura H, Tsuta K, Yoshida A, et al. Aberrant anaplastic lymphoma kinase expression in high-grade pulmonary neuroendocrine carcinoma. J Clin Pathol. 2013;66:705-707.
National Comprehensive Cancer Network. Non-small cell lung cancer. Version 2.2013. Available at www.nccn.org.
Nitta H, Tsuta K, Yoshida A, et al. New methods for ALK status diagnosis in non-small-cell lung cancer: an improved ALK immunohistochemical assay and a new, brightfield, dual ALK IHC-in situ hybridization assay. J Thorac Oncol. 2013; 8(8):1019-1031.
Noda Y, Fujita N, Kobayashi g, et al. Diagnostic efficacy of the cell block method in comparison with smear cytology of tissue samples obtained by endoscopic ultrasound-guided fine-needle aspiration. J Gastroenterol. 2010;45(8):868-875.
Ochi N, Yamane H, Yamagishi T, et al. Can we eliminate squamous cell carcinoma of the lung from testing of EML4-ALK fusion gene? Lung Cancer. 2013;79(1):94-95.
Orell S, Sterrett gF (eds). Orell and Sterrett’s Fine Needle Aspiration Cytology, 5th ed. New York: Churchill Livingstone; 2011.
Oyama T, Ishikawa Y, Hayashi Y, et al. The effects of fixation, processing and evaluation criteria of immunohistochemical detection of hormone receptors in breast cancer. Breast Cancer. 2007;12(2):182-188.
Paik J, Choe g, Kim H, et al. Screening of anaplastic lymphoma kinase rearrangement by immunohistochemistry in non-small cell lung cancer: correlation with fluorescence in situ hybridization. J Thorac Oncol. 2011;6(3):466-472.
Paik J, Choi CM, Kim H, et al. Clinicopathologic implication of ALK rearrangement in surgically resected lung cancer: a proposal of diagnostic algorithm for ALK-rearranged adenocarcinoma. Lung Cancer. 2012;76:403-409.
Palmer R, Vernersson E, grabbe C, Hallberg B. Anaplastic lymphoma kinase: signalling in development and disease. Biochem J. 2009;420:345-361.
Park H, Lee JK, Kim DW, et al. Immunohistochemical screening for anaplastic lymphoma kinase (ALK) rearrangement in advanced non-small cell lung cancer patients. Lung Cancer. 2012;77:288-292.
Peled N, Palmer g, Hirsch FR, et al. Next-generation sequenc-ing identifies and immunohistochemistry confirms a novel crizotinib-sensitive ALK rearrangement in a patient with metastatic non-small-cell lung cancer. J Thorac Oncol. 2012;7(9):e14-16.
Pelosi g, gasparini P, Cavazza A, et al. Multiparametric molecular characterization of pulmonary sarcomatoid carcinoma reveals a nonrandom amplification of anaplastic lymphoma kinase (ALK) gene. Lung Cancer. 2012;77:507-514.
Perner S, Wagner PL, Demichelis F, et al. EML4-ALK fusion lung cancer: a rare acquired event. Neoplasia. 2008;10(3):298-302.
Popat S, gonzalez D, Min T, et al. ALK translocation is associated with ALK immunoreactivity and extensive signet-ring morphology in primary lung adenocarcinoma. Lung Cancer. 2012;75:300-305.
Prinsen C, Klaassen CH, Thunnissen FB. Microarray as a model for quantitative visualization chemistry. Appl Immunohistochem Mol Morphol. 2003;11:168-173.
Rekhtman N, Paik PK, Arcila ME, et al. Clarifying the spectrum of driver oncogene mutations in biomarker-verified squamous carcinoma of lung: lack of EgFR/KRAS and presence of PIK3CA/AKT1 mutations. Clin Cancer Res. 2012; 18(4):1167-1176.
Rikova K, guo A, Zeng Q, et al. global survey of phosphoty-rosine signaling identifies oncogenic kinases in lung cancer. Cell. 2007;131:1190-1203.
Rivera M, Mehta AC, American College of Chest Physicians. Initial diagnosis of lung cancer: ACCP evidence-based clinical practice guidelines (2nd edition). Chest. 2007;132(3 Supple):131S-148S.
Rodig S, Mino-Kenudson M, Dacic S, et al. Unique clini-copathologic features characterize ALK-rearranged lung adenocarcinoma in the western population. Clin Cancer Res. 2009;15(16):5216-5223.
Ross J, Cronin M. Whole cancer genome sequencing by next-generation methods. Am J Clin Pathol. 2011;136:527-539.
Rothschild S, Zippelius A, Betticher DC, et al. Neue Therapiekonzepte beim Bronchuskarzinom. Schweiz Med Forum. 2011;11:7.
Ruschoff J, Kerr KM, grote HJ, et al. Reproducibility of immunohistochemical scoring for epidermal growth factor receptor expression in non-small cell lung cancer. Arch Pathol Lab Med. 2012 Dec 27 [Epub ahead of print].

72IASLC ATLAS OF ALK TESTING IN LUNG CANCER
Sakairi Y, Nakajima T, Yasufuku K, et al. EML4-ALK fusion gene assessment using metastatic lymph node samples obtained by endobronchial ultrasound-guided transbronchial needle aspiration. Clin Cancer Res. 2010;16(20):4938-4945.
Salido M, Pijuan L, Martinez-Aviles L, et al. Increased ALK gene copy number and amplification are frequent in non-small cell lung cancer. J Thorac Oncol. 2011;6(1):21-27.
Sanders H, Li HR, Bruey JM, et al. Exon scanning by reverse transcriptase-polymerase chain reaction for detection of known and novel EML4-ALK fusion variants in non-small cell lung cancer. Cancer Genet. 2011;204:45-52.
Sasaki T, Rodig SJ, Chirieac LR, et al. The biology and treatment of EML4-ALK non-small cell lung cancer. Eur J Cancer. 2010;46:1773-1780.
Savic S, Bode B, Diebold J, et al. Detection of ALK-positive non-small-cell lung cancers on cytological specimens: high accuracy of immunocytochemistry with the 5A4 clone. J Thorac Oncol. 2013;8(8):1004-1011.
Saxe D, Persons DL, Wolff DJ, et al. Validation of fluorescence in situ hybridization using an analyte-specific reagent for detection of abnormalities involving the mixed lineage leukemia gene. Arch Pathol Lab Med. 2012;136(1):47-52.
Schildhaus H, Deml KF, Schmitz K, et al. Chromogenic in situ hybridization is a reliable assay for detection of ALK rearrangements in adenocarcinomas of the lung. Mod Pathol. 2013 Jun 7 [Epub ahead of print].
Schreiber g, McCrory DC. Performance characteristics of different modalities for diagnosis of suspected lung cancer: summary of published evidence. Chest. 2003;123(1 Suppl):115S-128S.
Selinger C, Rogers TM, Russell PA, et al. Testing for ALK rearrangement in lung adenocarcinoma: a multicenter comparison of immunohistochemistry and fluorescent in situ hybridization. Mol Pathol. 2013 Jun 7 [Epub ahead of print].
Shaozhang Z, Xiaomei L, Aiping Z, et al. Detection of EML4-ALK fusion genes in non-small cell lung cancer patients with clinical features associated with EgFR mutations. Genes Chromsomes Cancer. 2012;51(10):925-932.
Shaw A, Kim DW, Nakagawa K, et al. Crizotinib versus chemo-therapy in advanced ALK-positive lung cancer. N Engl J Med. 2013;368(25):2385-2394.
Shaw A, Yeap BY, Mino-Kenudson M, et al. Clinical features and outcome of patients with non-small-cell lung cancer who harbor EML4-ALK. J Clin Oncol. 2009;27(26):4247-4253.
Shaw A, Yeap BY, Solomon BJ, et al. Effect of crizotinib on overall survival in patients with advanced non-small-cell lung cancer harbouring ALK gene rearrangement: a retrospective analysis. Lancet Oncol. 2011;12(11):1004-1012.
Shinmura K, Kageyama S, Tao H, et al. EML4-ALK fusion tran-scripts, but no NPM-, TPM3-, CLTC-, ATIC-, or TFg-ALK fusion transcripts, in non-small cell lung carcinomas. Lung Cancer. 2008;61(2):163-169.
Sholl L, Weremowicz S, gray SW, et al. Combined use of ALK immunohistochemistry and FISH for optimal detection of ALK-rearranged lung adenocarcinomas. J Thorac Oncol. 2013;8(3):322-328.
Soda M, Choi YL, Enomoto M, et al. Identification of the transforming EML4-ALK fusion gene in non-small-cell lung cancer. Nature. 2007;448(7153):561-566.
Soda M, Isobe K, Inoue A, et al. A prospective PCR-based screening for the EML4-ALK oncogene in non-small cell lung cancer. Clin Cancer Res. 2012;18(20):5682-5689.
Sun J, Choi YL, Won JK, et al. A dramatic response to crizotinib in a non-small-cell lung cancer patient with IHC-positive and FISH-negative ALK. J Thorac Oncol. 2012;7:e36-e38.
Sun Y, Ren Y, Fang Z, et al. Lung adenocarcinoma from East Asian never-smokers is a disease largely defined by targetable oncogenic mutant kinases. J Clin Oncol. 2010;28(30):4616-4620.
Takahashi T, Sonobe M, Kobayashi M, et al. Clinicopathologic features of non-small-cell lung cancer with EML4-ALK fusion gene. Ann Surg Oncol. 2010;17(3):889-897.
Takamochi K, Takeuchi K, Hayashi T, et al. A rational diagnostic algorithm for the identification of ALK rearrangement in lung cancer: a comprehensive study of surgically treated Japanese patients. PLoS One. 2013;8(8):e69794.
Takeuchi K. Interpretation of anti-ALK immunohistochemistry results [letter]. J Thorac Oncol. 2013;8(7):e67-e68.
Takeuchi K, Choi YL, Soda M, et al. Multiplex reverse transcription-PCR screening for EML4-ALK fusion transcripts. Clin Cancer Res. 2008;14(20):6618-6624.
Takeuchi K, Choi YL, Togashi Y, et al. KIF5B-ALK, a novel fusion oncokinase identified by an immunohistochemistry-based diagnostic system for ALK-positive lung cancer. Clin Cancer Res. 2009;15(9):3143-3149.
Takeuchi K, Soda M, Togashi Y, et al. RET, ROS1 and ALK fusions in lung cancer. Nature Med. 2012;18:378-381.
Tanaka H, Tone K, Hayashi A, et al. Clinical application of immunocytochemical detection of ALK rearrangement on cytology slides for detection or screening of lung adenocarcinoma. Lung Cancer. 2013;80(3):289-292.
Thomas J, Lamb D, Ashcroft T, et al. How reliable is the diagnosis of lung cancer using small biopsy specimens? Report of a UKCCCR Lung Cancer Working Party. Thorax. 1993; 48(11):1135-1139.
Thunnissen E, Boers E, Heideman DA, et al. Correlation of immunohistochemical staining p63 and TTF-1 with EgFR and K-ras mutational spectrum and diagnostic reproducibility in non small cell lung carcinoma. Virchows Arch. 2012;461(6):629-638. (a)
Thunnissen E, Bubendorf L, Dietel M, et al. EML4-ALK testing in non-small cell carcinomas of the lung: a review with recommendations. Virchows Arch 2012;461(3):245-257. (b)
Thunnissen E, Kerr KM, Bubendorf L, et al. External quality assessment for ALK immunohistochemistry testing in lung adenocarcinoma within the European Thoracic Oncology Platform Lungscape Project. Ann Oncol. 2012;23(suppl 9):2932. (c)
Thunnissen E, Kerr KM, Herth FJ, et al. The challenge of NSCLC diagnosis and predictive analysis on small samples. Practical approach of a working group. Lung Cancer. 2012;76(1):1-18. (d)

73REFERENCES
To KF, Tong JH, Yeung KS, et al. Detection of ALK rearrangement by immunohistochemistry in lung adenocarcinoma and the identification of a novel EML4-ALK variant. J Thorac Oncol. 2013;8(7):883-891.
Togashi Y, Soda M, Sakata S, et al. KLC1-ALK: a novel fusion in lung cancer identified using a formalin-fixed paraffin-embedded tissue only. PLoS One. 2012;7:e31323.
Travis W, Brambilla E, Noguchi M, et al. International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society international multidisciplinary classification of lung adenocarcinoma. J Thorac Oncol. 2011; 6(2):244-285.
Travis W, Brambilla E, Noguchi M, et al. Diagnosis of lung cancer in small biopsies and cytology: implications of the 2011 International Association for the Study of Lung Cancer/American Thoracic Society/European Respiratory Society classification. Arch Pathol Lab Med. 2013;137(5):668-684.
Tsao M, Craddock K, Brandao g, et al. Canadian ALK (CALK): A pan-Canadian multicenter study to optimize and standardize ALK immunohistochemistry (IHC) and fluorescence in situ hybridization (FISH) for ALK gene rearrangements. J Clin Oncol. 2013;31(May 20 Supplement):8096.
V Laffert M, Warth A, Penzel R, et al. Anaplastic lymphoma kinase (ALK) gene rearrangement in non-small cell lung cancer (NSCLC): results of a multi-centre ALK-testing. Lung Cancer. 2013;81:200-206.
van Krieken J, Normanno N, Blackhall F, et al. guideline on the requirements of external quality assessment programs in molecular pathology. Virchows Arch. 2013;462:27-37.
Wang R, Hu H, Pan Y, et al. RET fusions define a unique molecular and clinicopathologic subtype of non-small-cell lung cancer. J Clin Oncol. 2012;30:4352-4359. (a)
Wang R, Pan Y, Li C, et al. The use of quantitative real-time reverse transcriptase PCR for 5’ and 3’ portions of ALK transcripts to detect ALK rearrangements in lung cancers. Clin Cancer Res. 2012;18(4725-4732. (b)
Wang Z, Zhang X, Bai H, et al. EML4-ALK rearrangement and its clinical significance in Chinese patients with advanced non-small cell lung cancer. Oncology. 2012;83(5):248-256.
Werner M, Chott A, Fabiano A, Battifora H. Effect of formalin tissue fixation and processing on immunohistochemistry. Am J Surg Pathol. 2000;24(7):1016-1019.
Wolff A, Hammond ME, Schwartz JN, et al. American Society of Clinical Oncology/College of American Pathologists guideline recommendations for human epidermal growth factor receptor 2 testing in breast cancer. Arch Pathol Lab Med. 2007;131(1):18-43.
Wong D, Leung EL, So KK, et al. The EML4-ALK fusion gene is involved in various histologic types of lung cancers from nonsmokers with wild-type EgFR and KRAS. Cancer. 2009;115(8):1723-1733.
Wu S, Kuo YY, Chang YL, et al. EML4-ALK translocation predicts better outcome in lung adenocarcinoma patients with wild-type EgFR. J Thorac Oncol. 2012;7(1):98-104.
Yang P, Kulig K, Boland JM, et al. Worse disease-free survival in never-smokers with ALK+ lung adenocarcinoma. J Thorac Oncol. 2012;7(1):90-97.
Yi E, Boland JM, Maleszewski JJ, et al. Correlation of IHC and FISH for ALK gene rearrangement in non-small cell lung carcinoma: IHC score algorithm for FISH. J Thorac Oncol 2011;6:459-465.
Yi E, Chung JH, Kulig K, Kerr KM. Detection of anaplastic lymphoma kinase (ALK) gene rearrangement in non-small cell lung cancer and related issues in ALK inhibitor therapy: a literature review. Mol Diagn Ther. 2012;16:143-150.
Yoshida A, Tsuta K, Nitta H, et al. Bright-field dual-color chromogenic in situ hybridization for diagnosing echinoderm microtubule-associated protein-like 4-anaplastic lymphoma kinase-positive lung adenocarcinomas. J Thorac Oncol. 2011;6(10):1677-1686. (a)
Yoshida A, Tsuta K, Watanabe S, et al. Frequent ALK rearrange-ment and TTF-1/p63 co-expression in lung adenocarcinoma with signet-ring cell component. Lung Cancer. 2011;72:309-315. (b)
Zhang X, Zhang S, Yang X, et al. Fusion of EML4 and ALK is associated with development of lung adenocarcinomas lacking EgFR and KRAS mutations and is correlated with ALK expression. Mol Cancer. 2010;9:188.
Zhang Y-g, Jin M-L, Li L, et al. Evaluation of ALK rearrangement in Chinese non-small cell lung cancer using FISH, immunohistochemistry, and real-time quantitative RT-PCR on paraffin-embedded tissues. PLOS One. 2013;8(5):e64821.
Zhang Y, Sun Y, Pan Y, et al. Frequency of driver mutations in lung adenocarcinoma from female never-smokers varies with histologic subtypes and age at diagnosis. Clin Cancer Res. 2012;18(7):1947-1953.
Zhou J, Yang H, Deng Q, et al. Oncogenic driver mutations in patients with non-small-cell lung cancer at various clinical stages. Ann Oncol. 2013;24(5):1319-1325.

74IASLC ATLAS OF ALK TESTING IN LUNG CANCER
Ap
pen
dix
1Su
mm
ary
of P
ub
lish
ed S
tud
ies
on
AL
K G
ene
Rea
rran
gem
ent T
esti
ng
in L
un
g C
ance
r
Stud
yCo
untr
yTe
st P
latf
orm
No.
of
NSC
LC*
No.
(%)
ALK
+ N
o. o
f A
DC
No.
(%)
ALK
+N
o. o
f SC
CN
o. (%
) A
LK+
No.
A
DSC
No
(%)
ALK
+
No.
N
SCLC
, ot
hers
No.
(%)
ALK
+N
o.
NE C
aN
o (%
) A
LK+
Patie
nt
Sele
ctio
n
Riko
va e
t al.,
200
7Ch
ina
RT-P
CR10
34
(4%
)-
--
--
--
--
Soda
et a
l., 2
007
Japa
nRT
-PCR
755
(6.7
%)
202
(10.
0%)
111
(9.1
%)
20
420
00
Koiv
unen
et a
l.,
2008
US/
Kore
aRT
-PCR
305
8 (2
.6%
)20
88
(3.8
%)
880
90
00
00
Pern
er e
t al.,
200
8U
S/Sw
itzer
land
FISH
/RT-
PCR
603
16 (2
.7%
)-
--
--
--
--
-
Shin
mur
a et
al.,
20
08Ja
pan
RT-P
CR/g
en S
eq77
2 (2
.6%
)50
2 (4
.0%
)20
03
04
00
0
Take
uchi
et a
l.,
2008
Japa
nRT
-PCR
/FIS
H/g
en S
eq34
011
(3.2
%)
253
11 (4
.3%
)71
07
09
024
0N
E Ca
incl
uded
SC
LC +
LCN
EC
Bola
nd e
t al.,
200
9U
SIH
C/FI
SH/R
T-PC
R33
56
(1.8
%)
185
5 (2
.7%
)15
01
(0.7
%)
00
00
00
Mar
telli
et a
l., 2
009
Italy
/Spa
inRT
-PCR
/FIS
H/IH
C12
09
(7.5
%)
633
(4.8
%)
484
(8.3
%)
22
(100
%)
70
00
Rodi
g e
t al.,
200
9U
SIH
C/FI
SH35
820
(5.6
%)
358
20 (5
.6%
)0
00
00
00
0
Shaw
et a
l., 2
009
US
FISH
141
19 (1
3.5%
)13
018
(12.
8%)
20
41
(25%
)5
00
0N
on/li
ght
smok
ers,
Asi
an,
wom
en
Take
uchi
et a
l.,
2009
Japa
nIH
C/RT
-PCR
& F
ISH
130
4 (3
.1%
)13
04
(3.1
%)
00
00
00
00
Won
g et
al.,
200
9Ch
ina
(HK)
RT-P
CR26
613
(4.9
%)
209
11 (5
.3%
)34
00
023
2 (8
.7%
)0
0
Joko
ji et
al.,
201
0Ja
pan
IHC
254
8 (3
.1%
)25
48
(3.1
%)
00
00
00
00
Saka
iri e
t al.,
201
0Ja
pan
IHC/
FISH
& R
T-PC
R10
97
(6.4
%)
827
(8.5
%)
180
00
90
00
Salid
o et
al.,
201
0Sp
ain
FISH
/IHC
107
3 (2
.8%
)69
3 (4
.3%
)30
00
08
00
0
Sun
Y et
al.,
201
0Ch
ina
RT-P
CR52
3 (5
.8%
)52
3 (5
.8%
)0
00
00
00
0N
ever
-sm
oker
s
Taka
hash
i et a
l.,
2010
Japa
nRT
-PCR
/Dire
ct S
eq31
35
(1.6
%)
211
5 (2
.4%
)75
00
027
00
0
Zhan
g X
et a
l., 2
010
Chin
aRA
CE/ R
T-PC
R10
312
(11.
7%)
6210
(16.
1%)
292
(6.9
%)
00
120
00
Paik
et a
l., 2
011
Kore
aIH
C/FI
SH73
528
(3.8
%)
395
27(6
.8%
)29
20
00
481
(2.1
%)
00
Yi e
t al.,
201
1U
SFI
SH/IH
C10
110
(9.9
%)
101
10 (9
.9%
)0
00
00
00
0N
ever
-sm
oker
s w
ith a
deno
car-
cino
ma

75AppENdIx1
An
et a
l., 2
012
Chin
aRA
CE-P
CR23
915
(6.3
%)
130
10 (7
.7%
)97
4 (4
.1%
)-
-12
1 (8
.3%
)0
0
Dai
et a
l., 2
012
US
FISH
1387
49 (3
.7%
)-
--
--
--
--
-
Jin
et a
l., 2
012
Kore
aRT
-PCR
167
10 (6
.0%
)12
19
(7.4
%)
461
(0.2
%)
00
00
00
McL
eer-
Flor
in e
t al
., 20
12Fr
ance
IHC/
FISH
441
29 (6
.6%
)44
129
(6.6
%)
00
00
00
00
Mur
akam
i et a
l.,
2012
Japa
nRT
-PCR
/IHC/
FISH
811
31 (3
.8%
)71
330
(4.2
%)
521
(1.9
%)
80
380
00
Park
et a
l., 2
012
Kore
aIH
C/FI
SH25
825
(9.7
%)
182
17 (9
.3%
)0
00
076
8 (1
0.5%
)4
0
EGFR
wild
-typ
e or
non
resp
onse
to
pre
viou
s Eg
FR T
KIs
Shao
zhan
g et
al.,
20
12Ch
ina
RT-P
CR10
28(
7.8%
)73
5 (6
.2%
)14
1 (7
.1%
)14
2 (1
4.3%
)1
00
0
Wom
en, n
on/
light
sm
oker
s, an
d/or
ade
no-
carc
inom
a
Wan
g Z
et a
l., 2
012
Chin
aFI
SH/IH
C11
311
(9.7
%)
9510
(10.
5%)
181
(5.6
%)
00
00
00
Wu
et a
l., 2
012
Taiw
anRT
-PCR
/FIS
H11
639
(34%
)11
639
(34%
)0
00
00
00
0EG
FR w
ild-t
ype,
pl
eura
l effu
sion
Yang
et a
l., 2
012
US
IHC/
FISH
300
34 (1
1.3%
)30
034
(11.
3%)
00
00
00
00
Nev
er-s
mok
ers
Zhan
g Y
et a
l., 2
012
Chin
aRA
CE-P
CR34
915
(4.3
%)
349
15 (4
.3%
)0
00
00
00
0Fe
mal
e ne
ver-
smok
ers
gai
nor e
t al.,
201
3U
SFI
SH16
8375
(4.4
%)
--
--
--
--
--
Li Y
et a
l., 2
013
Chin
aRT
-PCR
/IHC
208
7 (3
.4%
)95
6 (6
.3%
)96
07
1 (1
4.3%
)10
00
0
Mar
tinez
et a
l.,
2013
Spai
nFI
SH/IH
C99
7 (7
.1%
)79
5 (6
.3%
)7
00
013
2 (1
5.4%
)0
0
Min
ca e
t al.,
201
3U
SIH
C/FI
SH24
932
(12.
8%)
--
--
--
--
--
Shol
l et a
l., 2
013
US
IHC/
FISH
186
12 (6
.5%
)18
612
(6.5
%)
To e
t al.,
201
3Ch
ina
(HK)
IHC/
FISH
/RT-
PCR
373
22 (5
.9%
)37
322
(5.9
%)
00
00
00
00
Zhan
g Y-
g e
t al.,
20
13Ch
ina
RT-P
CR/IH
C/FI
SH46
920
(4.2
%)
341
19 (2
.6%
)11
20
40
121
(8.3
%)
00
Zhou
et a
l., 2
013
Chin
aA
RMS
RT-P
CR48
828
(5.7
%)
349
25 (7
.2%
)10
12
(2.0
%)
181
(5.6
%)
200
00
Tota
l12
665
662
(5.2
%)
6775
444
(6.6
%)
1411
18 (1
.3%
)78
7 (9
.0%
)37
617
(4.5
%)
280
*Exc
lude
s neu
roen
docr
ine
canc
ers (
NE
Ca);
NSC
LC =
non
-sm
all c
ell l
ung
carc
inom
a, A
DC
= ad
enoc
arci
nom
a, S
CC =
squa
mou
s cel
l car
cino
ma,
AD
SC =
mix
ed a
deno
carc
inom
a/sq
uam
ous c
ell c
arci
nom
a, S
CLC
= sm
all c
ell l
ung
carc
inom
a LC
NEC
= la
rge
cell
neur
oend
ocrin
e ca
rcin
oma,
EG
FR =
epi
derm
al g
row
th fa
ctor
rece
ptor
, TKI
s = ty
rosi
ne k
inas
e in
hibi
tors
, RT-
PCR
= re
vers
e tr
ansc
ripta
se p
olym
eras
e ch
ain
reac
tion,
FI
SH =
fluo
resc
ence
in si
tu h
ybrid
izat
ion,
Gen
seq
= ge
netic
sequ
enci
ng, I
HC
= im
mun
ohis
toch
emis
try,
RAC
E =
rapi
d am
plifi
catio
n of
cD
NA
ends
, and
ARM
S am
plifi
catio
n-re
fract
ory
mut
atio
n sy
stem
.

76IASLC ATLAS OF ALK TESTING IN LUNG CANCER
Appendix 2CAP/IASLC/AMP Molecular Testing Guideline for Selection of Patients with Lung Cancer for Treatment with EGFR and ALK Tyrosine Kinase Inhibitors
Summary of Recommendations
Section I. When Should Molecular Testing of Lung Cancers Be Performed?
Question 1. Which Patients Should Be Tested for EGFR Mutations and ALK Rearrangements? 1.1a: Recommendation: EGFR molecular testing should be used to select patients for EgFR targeted tyrosine kinase inhibitor therapy, and patients with lung adenocarcinoma should not be excluded from testing on the basis of clinical characteristics. 1.1b: Recommendation: ALK molecular testing should be used to select patients for ALK targeted tyrosine kinase inhibitor therapy, and patients with lung adenocarcinoma should not be excluded from testing on the basis of clinical characteristics. 1.2: Recommendation: In the setting of lung cancer resection specimens, EGFR and ALK testing is recommended for adenocarcinomas and mixed lung cancers with an adenocarcinoma component, regardless of histologic grade. In the setting of fully excised lung cancer specimens, EGFR and ALK testing is not recommended in lung cancers that lack any adenocarcinoma component, such as “pure” squamous cell carcinomas, “pure” small cell carcinomas, or large cell carcinomas lacking any immunohistochemistry (IHC) evidence of adenocarcinoma differentiation. 1.3: Recommendation: In the setting of more limited lung cancer specimens (biopsies, cytology) where an adenocarcinoma component cannot be completely excluded, EGFR and ALK testing may be performed in cases showing squamous or small cell histology but clinical criteria (eg, young age, lack of smoking history) may be useful in selecting a subset of these samples for testing. 1.4: Recommendation: To determine EGFR and ALK status for initial treatment selection, primary tumors or metastatic lesions are equally suitable for testing. 1.5: Expert consensus opinion: For patients with multiple, apparently separate, primary lung adenocarcinomas, each tumor may be tested but testing of multiple different areas within a single tumor is not necessary.
Question 2. When Should a Patient Specimen Be Tested for EGFR Mutation or ALK Rearrangement? 2.1a: Recommendation: EGFR mutation testing should be ordered at the time of diagnosis for patients presenting with advanced-stage disease (stage IV according to the 7th edition TNM staging system) who are suitable for therapy or at time of recurrence or progression in patients who originally presented with lower-stage disease but were not previously tested. 2.1b: Suggestion: ALK rearrangement testing should be ordered at the time of diagnosis for patients presenting with advanced-stage disease (stage IV according to the 7th edition TNM staging system) who are suitable for therapy or at time of recurrence or progression in patients who originally presented with lower-stage disease but were not previously tested. 2.2a: Expert consensus opinion: EGFR testing of tumors at diagnosis from patients presenting with stage I, II, or III disease is encouraged but the decision to do so should be made locally by each laboratory, in collaboration with its oncology team. 2.2b: Expert consensus opinion: ALK testing of tumors at diagnosis from patients presenting with stage I, II, or III disease is encouraged, but the decision to do so should be made locally by each laboratory, in collaboration with its oncology team. 2.3: Recommendation: Tissue should be prioritized for EGFR and ALK testing.
Question 3. How Rapidly Should Test Results Be Available? 3.1: Expert consensus opinion: EGFR and ALK results should be available within 2 weeks (10 working days) of receiving the specimen in the testing laboratory.
77AppENdIx 2
3.2: Expert consensus opinion: Laboratories with average turnaround times beyond 2 weeks need to make available a more rapid test—either in-house or through a reference laboratory—in instances of clinical urgency. 3.3: Expert consensus opinion: Laboratory departments should establish processes to ensure that specimens that have a final histopathologic diagnosis are sent to outside molecular pathology laboratories within 3 working days of receiving requests and to intramural molecular pathology laboratories within 24 hours.
Section II. How Should EGFR Testing Be Performed?
Question 4. How Should Specimens Be Processed for EGFR Mutation Testing? 4.1: Expert consensus opinion: Pathologists should use formalin-fixed, paraffin-embedded (FFPE) specimens or fresh, frozen, or alcohol-fixed specimens for PCR-based EGFR mutation tests. Other tissue treatments (eg, acidic or heavy metal fixatives, or decalcifying solutions) should be avoided in specimens destined for EGFR testing. 4.2: Expert consensus opinion: Cytologic samples are also suitable for EGFR and ALK testing, with cell blocks being preferred over smear preparations.
Question 5. What Are the Specimen Requirements for EGFR Testing? 5.1: Expert consensus opinion: Pathologists should determine the adequacy of specimens for EGFR testing by assessing cancer cell content and DNA quantity and quality. 5.2: Expert consensus opinion: Each laboratory should establish the minimum proportion and number of cancer cells needed for mutation detection during validation. 5.3: Expert consensus opinion: A pathologist should assess the tumor content of each specimen and either perform, or guide a trained technologist to perform, microdissection for tumor cell enrichment as needed.
Question 6. How Should EGFR Testing Be Performed? 6.1: Recommendation: Laboratories may use any validated EGFR testing method with sufficient performance characteristics. 6.2: Expert consensus opinion: Laboratories should use EGFR test methods that are able to detect mutations in specimens with at least 50% cancer cell content, although laboratories are strongly encouraged to use (or have available at an external reference laboratory) more sensitive tests that are able to detect mutations in specimens with as little as 10% cancer cells. 6.3: Expert consensus opinion: Clinical EGFR mutation testing should be able to detect all individual mutations that have been reported with a frequency of at least 1% of EGFR-mutated lung adenocarcinomas. 6.4: Recommendation: Immunohistochemistry for total EgFR is not recommended for selection of EgFR TKI therapy. 6.5: Recommendation: EGFR copy number analysis (ie, FISH or CISH) is not recommended for selection of EgFR TKI therapy.
Question 7. What Is the Role of KRAS Analysis in Selecting Patients for Targeted Therapy With EGFR TKI? 7.1: Recommendation: KRAS mutation testing is not recommended as a sole determinant of EgFR TKI therapy.
Question 8. What Additional Testing Considerations Are Important in the Setting of Secondary or Acquired EGFR TKI Resistance? 8.1: Recommendation: If a laboratory performs testing on specimens from patients with acquired resistance to EgFR kinase inhibitors, such tests should be able to detect the secondary EGFR T790M mutation in as few as 5% of cells.

78IASLC ATLAS OF ALK TESTING IN LUNG CANCER
Section III. How Should ALK Testing Be Performed?
Question 9. What Methods Should Be Used for ALK testing? 9.1: Recommendation: Laboratories should use an ALK FISH assay using dual-labeled break-apart probes for selecting patients for ALK TKI therapy; ALK immunohistochemistry, if carefully validated, may be considered as a screening methodology to select specimens for ALK FISH testing. 9.2: Recommendation: RT-PCR is not recommended as an alternative to FISH for selecting patients for ALK inhibitor therapy. 9.3: Expert consensus opinion: A pathologist should be involved in the selection of sections for ALK FISH testing, by assessing tumor architecture, cytology, and specimen quality. 9.4: Expert consensus opinion: A pathologist should participate in the interpretation of ALK FISH slides, either by performing the analysis directly or by reviewing the interpretations of cytogeneticists or technologists with specialized training in solid tumor FISH analysis. 9.5: Expert consensus opinion: Testing for secondary mutations in ALK associated with acquired resistance to ALK inhibitors is not currently required for clinical management.
Section IV. Should Other Genes Be Routinely Tested in Lung Adenocarcinoma?
Question 10. Are Other Molecular Markers Suitable for Testing in Lung Cancer? 10.1a: Recommendation: Testing for EGFR should be prioritized over other molecular markers in lung adenocarcinoma. 10.1b: Suggestion: After EGFR testing, testing for ALK should be prioritized over other proposed molecular markers in lung adenocarcinoma, for which published evidence is insufficient to support testing guideline development at the present time.
Section V. How Should Molecular Testing of Lung Adenocarcinomas Be Implemented and Operationalized?
Question 11. Must All Adenocarcinomas Be Tested for Both EGFR and ALK? 11.1: Expert consensus opinion: Laboratories may implement testing algorithms to enhance the efficiency of molecular testing of lung adenocarcinomas, provided the overall turnaround time requirements are met.
Question 12. How Should EGFR and ALK Results Be Reported? 12.1: Expert consensus opinion: EGFR mutation testing reports and ALK FISH reports should include a results and interpretation section readily understandable by oncologists and by nonspecialist pathologists.
Question 13. How Should EGFR and ALK Testing Be Validated? 13.1: Expert consensus opinion: EGFR and ALK testing validation should follow the same guidelines as for other molecular diagnostics and FISH tests.
Question 14. How Should Quality Assurance Be Maintained? 13.1: Expert consensus opinion: Laboratories should follow similar quality control and quality assurance policies and procedures for EGFR and ALK testing in lung cancers as for other clinical laboratory assays. In particular, laboratories performing EGFR and ALK testing for TKI therapy should enroll in proficiency testing, if available.
Abbreviations: CISH, chromogenic in situ hybridization; EGFR, epidermal growth factor receptor; FISH, fluorescence in situ hybridization; PCR, polymerase chain reaction; RT-PCR, reverse transcription-polymerase chain reaction; TKI, tyrosine kinase inhibitor; TNM, tumor node metastasis.
Reprinted, with permission from, Lindeman NI, Cagle PT, Beasley MB, et al. Molecular testing guideline for selection of lung cancer patients for EgFR and ALK tyrosine kinase inhibitors: guideline from the College of American Pathologists (CAP), International Association for the Study of Lung Cancer (IASLC), Association for Molecular Pathology (AMP). J Thorac Oncol 2013;8:823-859.



The IASLC Atlas of ALK Testing in Lung Cancer is designed to help patholo-gists, laboratory scientists, and practicing physicians better understand various methods of ALK testing and the interpretation of test results. In the United States, FISH is the approved method for detecting ALK rearrangement to select patients with advanced NSCLC for treatment with an ALK inhibitor, but other assay platforms are also available. Molecular testing for ALK gene rearrange-ment is crucial for the optimal choice of therapy for patients with advanced NSCLC. This Atlas defines the appropriate candidates for ALK testing, describes and compares several assay platforms for ALK testing, and discusses proposed screening-diagnosis paradigms for treatment with ALK inhibitors.
IASLC acknowledges the generous funding and support provided
by Pfizer Oncology for this ALK Atlas project.
www.iaslc.org