ibrutinib treatment of mantle cell lymphoma relapsing at
TRANSCRIPT

Case ReportIbrutinib Treatment of Mantle Cell Lymphoma Relapsing atCentral Nervous System A Case Report and Literature Review
Donato Mannina and Barbara Loteta
Hematology Unit Papardo Hospital cda Papardo 98158 Messina Italy
Correspondence should be addressed to Donato Mannina donamannigmailcom
Received 15 December 2016 Accepted 12 June 2017 Published 16 July 2017
Academic Editor Sudhir Tauro
Copyright copy 2017 Donato Mannina and Barbara Loteta This is an open access article distributed under the Creative CommonsAttribution License which permits unrestricted use distribution and reproduction in any medium provided the original work isproperly cited
Mantle cell lymphoma (MCL) accounts for about 5 of all lymphomas Its clinical and histological features are heterogeneous Aftera frequently good initial response the disease generally and repeatedly relapses and finally the outcome is poor Particularly severe isthe prognosis of the rare occurrence of CNSi (Central Nervous System involvement) Ibrutinib an oral inhibitor of Bruton tyrosinekinase (BTK) has shown strong activity in relapsing patients with Chronic Lymphocytic Leukemia (CLL) and MCL Few reportsare available about treatment with ibrutinib of patients presenting CNSi by lymphoproliferative diseases (LPD) In all of themibrutinib at the dosage between 420 and 560mgday showed an impressive effectiveness Here we describe a case of MCL withCNS relapse showing an excellent response to ibrutinib administered at the unusual dose of 280mgday because of concomitanttreatment of cardiological disease
1 Introduction
Mantle cell lymphoma (MCL) is a subtype of B-cell non-Hodgkinrsquos lymphoma (NHL) accounting for about 5 of alllymphomas [1] Lymph node or extranodal biopsy is essentialfor diagnosis Positivity of CD5 and CD19 and negativity ofCD23 are the immunohistochemical markers Cytogeneticand molecular findings are the translocation t(1114)(q13q32)and the overexpression of Cyclin D1
The clinical presentation is heterogeneousThe majority of the patients is in advanced stage at
presentation and may have extranodal involvement Theresponse at first-line therapy is generally goodUnfortunatelymost of the patients eventually relapse and the outcome aftersalvage treatment is very disappointing with a median overallsurvival of about three years
First-line therapy consists generally of ARA-C containingregimens followed by autologous hemopoietic stem cellstransplantation (HSCT)
The central nervous system (CNS) involvement is arelatively rare event in advancedrelapsed MCL [2 3] Thisis a very severe condition with a very poor prognosis
Ibrutinib is an oral inhibitor of Bruton tyrosine kinase(BTK) recently approved for relapsingrefractory (RR)patients with Chronic Lymphocytic Leukemia (CLL) andMCL [4 5]
We report a case of MCL with CNS relapse that showedan excellent response to ibrutinib
2 Case Report
A 59-year-old man was diagnosed with classical MCL atanother institution in April 2012
At diagnosis ECOG performance status was one AnnArbor stage was IV for bone marrow and gastric andintestinal involvement Axillary laterocervical supraclavearmediastinal celiac crural iliac inguinal paralumboaorticand perigastric lymph nodes were enlarged The diseasepresented with leukemic expression No B symptoms werepresent MIPI score was five
The patient was treated according to MCL0208 protocoldesigned by the Fondazione Italiana Linfomi (FIL) con-sisting in an induction phase (3 cycles of R-CHOP givenevery 21 days) followed by a consolidation phase (high-dose
HindawiCase Reports in HematologyVolume 2017 Article ID 9583257 4 pageshttpsdoiorg10115520179583257
2 Case Reports in Hematology
105
104
103
102
105
104
103
102
CD19PerC
P-A
CD5 FITC-A
105
104
103
102
105
104
103
102
CD23PE
-A
CD20 FITC-A
Figure 1 Flow cytometry on CSF reveals a positive expression of CD19 CD20 and CD5 and negativity of CD23
cyclophosphamide 2 cycles of high-dose Ara-C BEAM andHSCT) After completion of first-line high-dose chemother-apy patients achieving complete or partial response went torandomization between maintenance with lenalidomide orobservation
Our patient randomized for maintenance came to ourobservation in complete remission (CR) on December 2013after 6 cycles of themaintenance phase At our institution themaintenance program was continued and finally completedon Jun 2015
During the follow-up the patientwas continuously inCRIn March 2016 the admission at an Orthopedic Unit
was necessary due to severe back pain resulting from a fallthat had caused a spinal fracture and a fracture of the leftwrist A few days after the discharge a new hospitalizationat a Neurological Department occurred urgently because ofaphasia andmental obnubilation Brain CT scan was negativefor focal lesions however the lumbar puncture (LB) showedthe presence of 300 mononucleated cells (MNC)120583l in thecerebrospinal fluid (CSF)The patient came to our institutionwith the suspected recurrence of lymphoma at CNS
At admission the patientrsquos general conditions were poorHe was bedridden His mental state was compromised anderratically shiny Arterial pressure was 14080mmHg heartrate 72m1015840 SpO2 96 and 119879 367∘C Peripheral blood countand biochemistry tests were normal except for light increaseof sALT Whole-body CT scan and trephine biopsy werenegative so systemic relapse was excluded
We performed a first LP withmethotrexate (MTX) 12mgIt showed the presence of 800MNCmm3 The immunophe-notype showed the typical pattern of mantle cell lymphoma(CD519+ CD23 neg) (Figure 1)
We performed further LP with MTX (12mg) and ARA-C(50mg) two times a week for six times until the cell count in
the CSF fell to 5 cells120583l The clinical condition of the patientgradually improved We discharged the patient on April 19after 20 days from hospitalization
We started ibrutinib at the dose of 280mgday We usedthis dosage because of a history of repeated episodes ofatrial fibrillation and ongoing prophylactic treatment withoral amiodarone The patient was not on anticoagulationtherapy No other LPs were performed nor any systemicchemotherapy was administrated
In December 2016 the patient came to clinical controlcomplaining of back pain without other symptoms Westopped ibrutinib administration because of the potentialbleeding risk related to invasive procedures and 2 daysafter we performed a LP No cells were present in CSF thusexcluding the suspicion of a new relapse The back pain wasvery likely due to concomitant discopathy Then we restartedibrutinib administration
Currently 13 months after starting ibrutinib the patientcontinues to be in CR
3 Discussion
The involvement of CNS by a relapsing MCL is a very seriouscondition with high mortality rate and a median overallsurvival of approximately 37 months [2]
Very few reports are available in literature but theincidence of CNS involvement in MCL might be higher thanpreviously recognized
In a study of 1994 of 22 patients with MCL 6 developedCNS involvement at a median of 18 months from diagno-sis All of them had poor MCL histological subtypes andadvanced disease In most of the cases CNS infiltration waspart of resistant disease or generalized relapse and had anominous significance [6]
Case Reports in Hematology 3
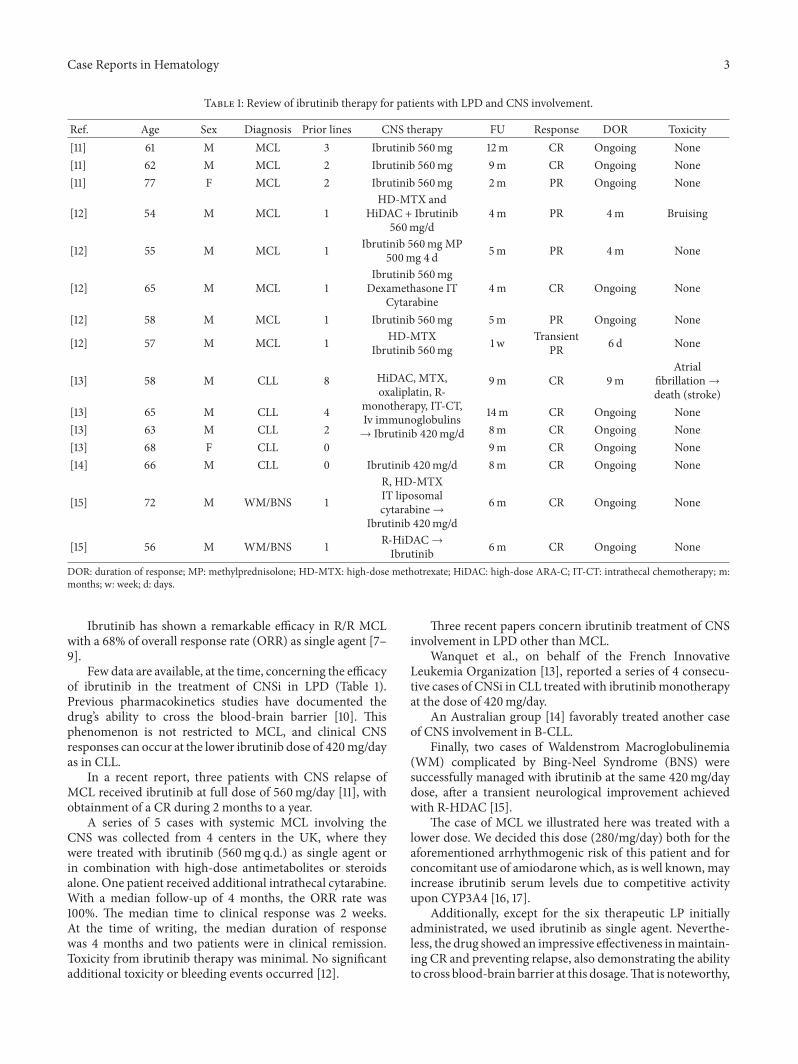
Table 1 Review of ibrutinib therapy for patients with LPD and CNS involvement
Ref Age Sex Diagnosis Prior lines CNS therapy FU Response DOR Toxicity[11] 61 M MCL 3 Ibrutinib 560mg 12m CR Ongoing None[11] 62 M MCL 2 Ibrutinib 560mg 9m CR Ongoing None[11] 77 F MCL 2 Ibrutinib 560mg 2m PR Ongoing None
[12] 54 M MCL 1HD-MTX and
HiDAC + Ibrutinib560mgd
4m PR 4m Bruising
[12] 55 M MCL 1 Ibrutinib 560mg MP500mg 4 d 5m PR 4m None
[12] 65 M MCL 1Ibrutinib 560mgDexamethasone IT
Cytarabine4m CR Ongoing None
[12] 58 M MCL 1 Ibrutinib 560mg 5m PR Ongoing None
[12] 57 M MCL 1 HD-MTXIbrutinib 560mg 1w Transient
PR 6 d None
[13] 58 M CLL 8 HiDAC MTXoxaliplatin R-
monotherapy IT-CTIv immunoglobulinsrarr Ibrutinib 420mgd
9m CR 9mAtrial
fibrillationrarrdeath (stroke)
[13] 65 M CLL 4 14m CR Ongoing None[13] 63 M CLL 2 8m CR Ongoing None[13] 68 F CLL 0 9m CR Ongoing None[14] 66 M CLL 0 Ibrutinib 420mgd 8m CR Ongoing None
[15] 72 M WMBNS 1
R HD-MTXIT liposomalcytarabinerarr
Ibrutinib 420mgd
6m CR Ongoing None
[15] 56 M WMBNS 1 R-HiDACrarrIbrutinib 6m CR Ongoing None
DOR duration of response MP methylprednisolone HD-MTX high-dose methotrexate HiDAC high-dose ARA-C IT-CT intrathecal chemotherapy mmonths w week d days
Ibrutinib has shown a remarkable efficacy in RR MCLwith a 68 of overall response rate (ORR) as single agent [7ndash9]
Few data are available at the time concerning the efficacyof ibrutinib in the treatment of CNSi in LPD (Table 1)Previous pharmacokinetics studies have documented thedrugrsquos ability to cross the blood-brain barrier [10] Thisphenomenon is not restricted to MCL and clinical CNSresponses can occur at the lower ibrutinib dose of 420mgdayas in CLL
In a recent report three patients with CNS relapse ofMCL received ibrutinib at full dose of 560mgday [11] withobtainment of a CR during 2 months to a year
A series of 5 cases with systemic MCL involving theCNS was collected from 4 centers in the UK where theywere treated with ibrutinib (560mg qd) as single agent orin combination with high-dose antimetabolites or steroidsalone One patient received additional intrathecal cytarabineWith a median follow-up of 4 months the ORR rate was100 The median time to clinical response was 2 weeksAt the time of writing the median duration of responsewas 4 months and two patients were in clinical remissionToxicity from ibrutinib therapy was minimal No significantadditional toxicity or bleeding events occurred [12]
Three recent papers concern ibrutinib treatment of CNSinvolvement in LPD other than MCL
Wanquet et al on behalf of the French InnovativeLeukemia Organization [13] reported a series of 4 consecu-tive cases of CNSi in CLL treated with ibrutinibmonotherapyat the dose of 420mgday
An Australian group [14] favorably treated another caseof CNS involvement in B-CLL
Finally two cases of Waldenstrom Macroglobulinemia(WM) complicated by Bing-Neel Syndrome (BNS) weresuccessfully managed with ibrutinib at the same 420mgdaydose after a transient neurological improvement achievedwith R-HDAC [15]
The case of MCL we illustrated here was treated with alower dose We decided this dose (280mgday) both for theaforementioned arrhythmogenic risk of this patient and forconcomitant use of amiodarone which as is well known mayincrease ibrutinib serum levels due to competitive activityupon CYP3A4 [16 17]
Additionally except for the six therapeutic LP initiallyadministrated we used ibrutinib as single agent Neverthe-less the drug showed an impressive effectiveness inmaintain-ing CR and preventing relapse also demonstrating the abilityto cross blood-brain barrier at this dosageThat is noteworthy
4 Case Reports in Hematology
especially in a very serious and prognostically unfavorablecondition lacking efficacious therapeutic alternatives for thelong-term control of the disease
This result could suggest modulating the standard dosein some cases reducing both off-target effects and drug-related complications and allowing treating a larger numberof patients
Conflicts of Interest
The authors declare no competing financial interests
Authorsrsquo Contributions
Donato Mannina and Barbara Loteta collected the dataDonato Mannina wrote the paper Donato Mannina andBarbara Loteta conducted diagnostic and therapeutic man-agement of the patient
References
[1] S Swerdlow E Campo N Harris et al WHO classificationof tumors of hematopoietic and lymphoid tissues InternationalAgency for Research and Cancer Lyon France 4th edition2008
[2] C Y Cheah A George E Gine et al ldquoCentral nervoussystem involvement in mantle cell lymphoma Clinical featuresprognostic factors and outcomes from the Europeanmantle celllymphomanetworkrdquoAnnals of Oncology vol 24 no 8 pp 2119ndash2123 2013
[3] A Ferrer F Bosch N Villamor et al ldquoCentral nervous systeminvolvement inmantle cell lymphomardquoAnnals of Oncology vol19 no 1 pp 135ndash141 2008
[4] L A Honigberg A M Smith M Sirisawad et al ldquoThe Brutontyrosine kinase inhibitor PCI-32765 blocks B-cell activationand is efficacious in models of autoimmune disease and B-cellmalignancyrdquo Proceedings of the National Academy of Sciences ofthe United States of America vol 107 no 29 pp 13075ndash130802010
[5] R W Hendriks S Yuvaraj and L P Kil ldquoTargeting Brutonrsquostyrosine kinase in B cell malignanciesrdquo Nature Reviews Cancervol 14 no 4 pp 219ndash232 2014
[6] E Montserrat F Bosch A Lopez-Guillermo et al ldquoCNSinvolvement in mantle-cell lymphomardquo Journal of ClinicalOncology vol 14 no 3 pp 941ndash944 1996
[7] M L Wang S Rule and P Martin ldquoTargeting BTK withibrutinib in relapsed or refractory mantle-cell lymphomardquo TheNew England Journal of Medecine vol 369 no 6 pp 507ndash5162013
[8] M L Wang K A Blum P Martin et al ldquoLong-term follow-up ofMCL patients treated with single-agent ibrutinib updatedsafety and efficacy resultsrdquo Blood vol 126 no 6 pp 739ndash7452015
[9] R H Advani J J Buggy and J P Sharman ldquoBruton tyrosinekinase inhibitor ibrutinib (PCI-32765) has significant activity inpatients with relapsedrefractory B-cell malignanciesrdquo Journalof Clinical Oncology vol 31 no 1 pp 88ndash94 2013
[10] FDA ldquoClinical Pharmacology Reviews Ibrutinib205552Orig1s000rdquo 2013
[11] S Bernard L Goldwirt S Amorim et al ldquoActivity of ibrutinibin mantle cell lymphoma patients with central nervous systemrelapserdquo Blood vol 126 no 14 pp 1695ndash1698 2015
[12] D L Tucker G Naylor A Kruger M S Hamilton G Followsand S A Rule ldquoIbrutinib is a safe and effective therapy forsystemic mantle cell lymphoma with central nervous systeminvolvementmdasha multi-centre case series from the United King-domrdquo British Journal of Haematology 2016
[13] AWanquet R Birsen R LemalMHunault V Leblond andTAurran-Schleinitz ldquoTo the editor Ibrutinib responsive centralnervous system involvement in chronic lymphocytic leukemiardquoBlood vol 127 no 19 pp 2356ndash2358 2016
[14] C S Tam T Kimber and J F Seymour ldquoIbrutinibmonotherapyas effective treatment of central nervous system involvement bychronic lymphocytic leukaemiardquo British Journal of Haematol-ogy vol 176 no 5 pp 829ndash831 2016
[15] A Cabannes-Hamy R Lemal L Goldwirt et al ldquoEfficacy ofibrutinib in the treatment of Bing-Neel syndromerdquo AmericanJournal of Hematology vol 91 no 3 pp E17ndashE19 2016
[16] J-Y Lee S Y Lee S J Oh K H Lee Y S Jung and S K KimldquoAssessment of drug-drug interactions caused by metabolism-dependent cytochrome P450 inhibitionrdquo Chemico-BiologicalInteractions vol 198 no 1-3 pp 49ndash56 2012
[17] KOhyamaMNakajimaM Suzuki N ShimadaH Yamazakiand T Yokoi ldquoInhibitory effects of amiodarone and its N-deethylated metabolite on human cytochrome P450 activitiesprediction of in vivo drug interactionsrdquo British Journal ofClinical Pharmacology vol 49 no 3 pp 244ndash253 2000
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Case Reports in Hematology
105
104
103
102
105
104
103
102
CD19PerC
P-A
CD5 FITC-A
105
104
103
102
105
104
103
102
CD23PE
-A
CD20 FITC-A
Figure 1 Flow cytometry on CSF reveals a positive expression of CD19 CD20 and CD5 and negativity of CD23
cyclophosphamide 2 cycles of high-dose Ara-C BEAM andHSCT) After completion of first-line high-dose chemother-apy patients achieving complete or partial response went torandomization between maintenance with lenalidomide orobservation
Our patient randomized for maintenance came to ourobservation in complete remission (CR) on December 2013after 6 cycles of themaintenance phase At our institution themaintenance program was continued and finally completedon Jun 2015
During the follow-up the patientwas continuously inCRIn March 2016 the admission at an Orthopedic Unit
was necessary due to severe back pain resulting from a fallthat had caused a spinal fracture and a fracture of the leftwrist A few days after the discharge a new hospitalizationat a Neurological Department occurred urgently because ofaphasia andmental obnubilation Brain CT scan was negativefor focal lesions however the lumbar puncture (LB) showedthe presence of 300 mononucleated cells (MNC)120583l in thecerebrospinal fluid (CSF)The patient came to our institutionwith the suspected recurrence of lymphoma at CNS
At admission the patientrsquos general conditions were poorHe was bedridden His mental state was compromised anderratically shiny Arterial pressure was 14080mmHg heartrate 72m1015840 SpO2 96 and 119879 367∘C Peripheral blood countand biochemistry tests were normal except for light increaseof sALT Whole-body CT scan and trephine biopsy werenegative so systemic relapse was excluded
We performed a first LP withmethotrexate (MTX) 12mgIt showed the presence of 800MNCmm3 The immunophe-notype showed the typical pattern of mantle cell lymphoma(CD519+ CD23 neg) (Figure 1)
We performed further LP with MTX (12mg) and ARA-C(50mg) two times a week for six times until the cell count in
the CSF fell to 5 cells120583l The clinical condition of the patientgradually improved We discharged the patient on April 19after 20 days from hospitalization
We started ibrutinib at the dose of 280mgday We usedthis dosage because of a history of repeated episodes ofatrial fibrillation and ongoing prophylactic treatment withoral amiodarone The patient was not on anticoagulationtherapy No other LPs were performed nor any systemicchemotherapy was administrated
In December 2016 the patient came to clinical controlcomplaining of back pain without other symptoms Westopped ibrutinib administration because of the potentialbleeding risk related to invasive procedures and 2 daysafter we performed a LP No cells were present in CSF thusexcluding the suspicion of a new relapse The back pain wasvery likely due to concomitant discopathy Then we restartedibrutinib administration
Currently 13 months after starting ibrutinib the patientcontinues to be in CR
3 Discussion
The involvement of CNS by a relapsing MCL is a very seriouscondition with high mortality rate and a median overallsurvival of approximately 37 months [2]
Very few reports are available in literature but theincidence of CNS involvement in MCL might be higher thanpreviously recognized
In a study of 1994 of 22 patients with MCL 6 developedCNS involvement at a median of 18 months from diagno-sis All of them had poor MCL histological subtypes andadvanced disease In most of the cases CNS infiltration waspart of resistant disease or generalized relapse and had anominous significance [6]
Case Reports in Hematology 3
Table 1 Review of ibrutinib therapy for patients with LPD and CNS involvement
Ref Age Sex Diagnosis Prior lines CNS therapy FU Response DOR Toxicity[11] 61 M MCL 3 Ibrutinib 560mg 12m CR Ongoing None[11] 62 M MCL 2 Ibrutinib 560mg 9m CR Ongoing None[11] 77 F MCL 2 Ibrutinib 560mg 2m PR Ongoing None
[12] 54 M MCL 1HD-MTX and
HiDAC + Ibrutinib560mgd
4m PR 4m Bruising
[12] 55 M MCL 1 Ibrutinib 560mg MP500mg 4 d 5m PR 4m None
[12] 65 M MCL 1Ibrutinib 560mgDexamethasone IT
Cytarabine4m CR Ongoing None
[12] 58 M MCL 1 Ibrutinib 560mg 5m PR Ongoing None
[12] 57 M MCL 1 HD-MTXIbrutinib 560mg 1w Transient
PR 6 d None
[13] 58 M CLL 8 HiDAC MTXoxaliplatin R-
monotherapy IT-CTIv immunoglobulinsrarr Ibrutinib 420mgd
9m CR 9mAtrial
fibrillationrarrdeath (stroke)
[13] 65 M CLL 4 14m CR Ongoing None[13] 63 M CLL 2 8m CR Ongoing None[13] 68 F CLL 0 9m CR Ongoing None[14] 66 M CLL 0 Ibrutinib 420mgd 8m CR Ongoing None
[15] 72 M WMBNS 1
R HD-MTXIT liposomalcytarabinerarr
Ibrutinib 420mgd
6m CR Ongoing None
[15] 56 M WMBNS 1 R-HiDACrarrIbrutinib 6m CR Ongoing None
DOR duration of response MP methylprednisolone HD-MTX high-dose methotrexate HiDAC high-dose ARA-C IT-CT intrathecal chemotherapy mmonths w week d days
Ibrutinib has shown a remarkable efficacy in RR MCLwith a 68 of overall response rate (ORR) as single agent [7ndash9]
Few data are available at the time concerning the efficacyof ibrutinib in the treatment of CNSi in LPD (Table 1)Previous pharmacokinetics studies have documented thedrugrsquos ability to cross the blood-brain barrier [10] Thisphenomenon is not restricted to MCL and clinical CNSresponses can occur at the lower ibrutinib dose of 420mgdayas in CLL
In a recent report three patients with CNS relapse ofMCL received ibrutinib at full dose of 560mgday [11] withobtainment of a CR during 2 months to a year
A series of 5 cases with systemic MCL involving theCNS was collected from 4 centers in the UK where theywere treated with ibrutinib (560mg qd) as single agent orin combination with high-dose antimetabolites or steroidsalone One patient received additional intrathecal cytarabineWith a median follow-up of 4 months the ORR rate was100 The median time to clinical response was 2 weeksAt the time of writing the median duration of responsewas 4 months and two patients were in clinical remissionToxicity from ibrutinib therapy was minimal No significantadditional toxicity or bleeding events occurred [12]
Three recent papers concern ibrutinib treatment of CNSinvolvement in LPD other than MCL
Wanquet et al on behalf of the French InnovativeLeukemia Organization [13] reported a series of 4 consecu-tive cases of CNSi in CLL treated with ibrutinibmonotherapyat the dose of 420mgday
An Australian group [14] favorably treated another caseof CNS involvement in B-CLL
Finally two cases of Waldenstrom Macroglobulinemia(WM) complicated by Bing-Neel Syndrome (BNS) weresuccessfully managed with ibrutinib at the same 420mgdaydose after a transient neurological improvement achievedwith R-HDAC [15]
The case of MCL we illustrated here was treated with alower dose We decided this dose (280mgday) both for theaforementioned arrhythmogenic risk of this patient and forconcomitant use of amiodarone which as is well known mayincrease ibrutinib serum levels due to competitive activityupon CYP3A4 [16 17]
Additionally except for the six therapeutic LP initiallyadministrated we used ibrutinib as single agent Neverthe-less the drug showed an impressive effectiveness inmaintain-ing CR and preventing relapse also demonstrating the abilityto cross blood-brain barrier at this dosageThat is noteworthy
4 Case Reports in Hematology
especially in a very serious and prognostically unfavorablecondition lacking efficacious therapeutic alternatives for thelong-term control of the disease
This result could suggest modulating the standard dosein some cases reducing both off-target effects and drug-related complications and allowing treating a larger numberof patients
Conflicts of Interest
The authors declare no competing financial interests
Authorsrsquo Contributions
Donato Mannina and Barbara Loteta collected the dataDonato Mannina wrote the paper Donato Mannina andBarbara Loteta conducted diagnostic and therapeutic man-agement of the patient
References
[1] S Swerdlow E Campo N Harris et al WHO classificationof tumors of hematopoietic and lymphoid tissues InternationalAgency for Research and Cancer Lyon France 4th edition2008
[2] C Y Cheah A George E Gine et al ldquoCentral nervoussystem involvement in mantle cell lymphoma Clinical featuresprognostic factors and outcomes from the Europeanmantle celllymphomanetworkrdquoAnnals of Oncology vol 24 no 8 pp 2119ndash2123 2013
[3] A Ferrer F Bosch N Villamor et al ldquoCentral nervous systeminvolvement inmantle cell lymphomardquoAnnals of Oncology vol19 no 1 pp 135ndash141 2008
[4] L A Honigberg A M Smith M Sirisawad et al ldquoThe Brutontyrosine kinase inhibitor PCI-32765 blocks B-cell activationand is efficacious in models of autoimmune disease and B-cellmalignancyrdquo Proceedings of the National Academy of Sciences ofthe United States of America vol 107 no 29 pp 13075ndash130802010
[5] R W Hendriks S Yuvaraj and L P Kil ldquoTargeting Brutonrsquostyrosine kinase in B cell malignanciesrdquo Nature Reviews Cancervol 14 no 4 pp 219ndash232 2014
[6] E Montserrat F Bosch A Lopez-Guillermo et al ldquoCNSinvolvement in mantle-cell lymphomardquo Journal of ClinicalOncology vol 14 no 3 pp 941ndash944 1996
[7] M L Wang S Rule and P Martin ldquoTargeting BTK withibrutinib in relapsed or refractory mantle-cell lymphomardquo TheNew England Journal of Medecine vol 369 no 6 pp 507ndash5162013
[8] M L Wang K A Blum P Martin et al ldquoLong-term follow-up ofMCL patients treated with single-agent ibrutinib updatedsafety and efficacy resultsrdquo Blood vol 126 no 6 pp 739ndash7452015
[9] R H Advani J J Buggy and J P Sharman ldquoBruton tyrosinekinase inhibitor ibrutinib (PCI-32765) has significant activity inpatients with relapsedrefractory B-cell malignanciesrdquo Journalof Clinical Oncology vol 31 no 1 pp 88ndash94 2013
[10] FDA ldquoClinical Pharmacology Reviews Ibrutinib205552Orig1s000rdquo 2013
[11] S Bernard L Goldwirt S Amorim et al ldquoActivity of ibrutinibin mantle cell lymphoma patients with central nervous systemrelapserdquo Blood vol 126 no 14 pp 1695ndash1698 2015
[12] D L Tucker G Naylor A Kruger M S Hamilton G Followsand S A Rule ldquoIbrutinib is a safe and effective therapy forsystemic mantle cell lymphoma with central nervous systeminvolvementmdasha multi-centre case series from the United King-domrdquo British Journal of Haematology 2016
[13] AWanquet R Birsen R LemalMHunault V Leblond andTAurran-Schleinitz ldquoTo the editor Ibrutinib responsive centralnervous system involvement in chronic lymphocytic leukemiardquoBlood vol 127 no 19 pp 2356ndash2358 2016
[14] C S Tam T Kimber and J F Seymour ldquoIbrutinibmonotherapyas effective treatment of central nervous system involvement bychronic lymphocytic leukaemiardquo British Journal of Haematol-ogy vol 176 no 5 pp 829ndash831 2016
[15] A Cabannes-Hamy R Lemal L Goldwirt et al ldquoEfficacy ofibrutinib in the treatment of Bing-Neel syndromerdquo AmericanJournal of Hematology vol 91 no 3 pp E17ndashE19 2016
[16] J-Y Lee S Y Lee S J Oh K H Lee Y S Jung and S K KimldquoAssessment of drug-drug interactions caused by metabolism-dependent cytochrome P450 inhibitionrdquo Chemico-BiologicalInteractions vol 198 no 1-3 pp 49ndash56 2012
[17] KOhyamaMNakajimaM Suzuki N ShimadaH Yamazakiand T Yokoi ldquoInhibitory effects of amiodarone and its N-deethylated metabolite on human cytochrome P450 activitiesprediction of in vivo drug interactionsrdquo British Journal ofClinical Pharmacology vol 49 no 3 pp 244ndash253 2000
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
Case Reports in Hematology 3
Table 1 Review of ibrutinib therapy for patients with LPD and CNS involvement
Ref Age Sex Diagnosis Prior lines CNS therapy FU Response DOR Toxicity[11] 61 M MCL 3 Ibrutinib 560mg 12m CR Ongoing None[11] 62 M MCL 2 Ibrutinib 560mg 9m CR Ongoing None[11] 77 F MCL 2 Ibrutinib 560mg 2m PR Ongoing None
[12] 54 M MCL 1HD-MTX and
HiDAC + Ibrutinib560mgd
4m PR 4m Bruising
[12] 55 M MCL 1 Ibrutinib 560mg MP500mg 4 d 5m PR 4m None
[12] 65 M MCL 1Ibrutinib 560mgDexamethasone IT
Cytarabine4m CR Ongoing None
[12] 58 M MCL 1 Ibrutinib 560mg 5m PR Ongoing None
[12] 57 M MCL 1 HD-MTXIbrutinib 560mg 1w Transient
PR 6 d None
[13] 58 M CLL 8 HiDAC MTXoxaliplatin R-
monotherapy IT-CTIv immunoglobulinsrarr Ibrutinib 420mgd
9m CR 9mAtrial
fibrillationrarrdeath (stroke)
[13] 65 M CLL 4 14m CR Ongoing None[13] 63 M CLL 2 8m CR Ongoing None[13] 68 F CLL 0 9m CR Ongoing None[14] 66 M CLL 0 Ibrutinib 420mgd 8m CR Ongoing None
[15] 72 M WMBNS 1
R HD-MTXIT liposomalcytarabinerarr
Ibrutinib 420mgd
6m CR Ongoing None
[15] 56 M WMBNS 1 R-HiDACrarrIbrutinib 6m CR Ongoing None
DOR duration of response MP methylprednisolone HD-MTX high-dose methotrexate HiDAC high-dose ARA-C IT-CT intrathecal chemotherapy mmonths w week d days
Ibrutinib has shown a remarkable efficacy in RR MCLwith a 68 of overall response rate (ORR) as single agent [7ndash9]
Few data are available at the time concerning the efficacyof ibrutinib in the treatment of CNSi in LPD (Table 1)Previous pharmacokinetics studies have documented thedrugrsquos ability to cross the blood-brain barrier [10] Thisphenomenon is not restricted to MCL and clinical CNSresponses can occur at the lower ibrutinib dose of 420mgdayas in CLL
In a recent report three patients with CNS relapse ofMCL received ibrutinib at full dose of 560mgday [11] withobtainment of a CR during 2 months to a year
A series of 5 cases with systemic MCL involving theCNS was collected from 4 centers in the UK where theywere treated with ibrutinib (560mg qd) as single agent orin combination with high-dose antimetabolites or steroidsalone One patient received additional intrathecal cytarabineWith a median follow-up of 4 months the ORR rate was100 The median time to clinical response was 2 weeksAt the time of writing the median duration of responsewas 4 months and two patients were in clinical remissionToxicity from ibrutinib therapy was minimal No significantadditional toxicity or bleeding events occurred [12]
Three recent papers concern ibrutinib treatment of CNSinvolvement in LPD other than MCL
Wanquet et al on behalf of the French InnovativeLeukemia Organization [13] reported a series of 4 consecu-tive cases of CNSi in CLL treated with ibrutinibmonotherapyat the dose of 420mgday
An Australian group [14] favorably treated another caseof CNS involvement in B-CLL
Finally two cases of Waldenstrom Macroglobulinemia(WM) complicated by Bing-Neel Syndrome (BNS) weresuccessfully managed with ibrutinib at the same 420mgdaydose after a transient neurological improvement achievedwith R-HDAC [15]
The case of MCL we illustrated here was treated with alower dose We decided this dose (280mgday) both for theaforementioned arrhythmogenic risk of this patient and forconcomitant use of amiodarone which as is well known mayincrease ibrutinib serum levels due to competitive activityupon CYP3A4 [16 17]
Additionally except for the six therapeutic LP initiallyadministrated we used ibrutinib as single agent Neverthe-less the drug showed an impressive effectiveness inmaintain-ing CR and preventing relapse also demonstrating the abilityto cross blood-brain barrier at this dosageThat is noteworthy
4 Case Reports in Hematology
especially in a very serious and prognostically unfavorablecondition lacking efficacious therapeutic alternatives for thelong-term control of the disease
This result could suggest modulating the standard dosein some cases reducing both off-target effects and drug-related complications and allowing treating a larger numberof patients
Conflicts of Interest
The authors declare no competing financial interests
Authorsrsquo Contributions
Donato Mannina and Barbara Loteta collected the dataDonato Mannina wrote the paper Donato Mannina andBarbara Loteta conducted diagnostic and therapeutic man-agement of the patient
References
[1] S Swerdlow E Campo N Harris et al WHO classificationof tumors of hematopoietic and lymphoid tissues InternationalAgency for Research and Cancer Lyon France 4th edition2008
[2] C Y Cheah A George E Gine et al ldquoCentral nervoussystem involvement in mantle cell lymphoma Clinical featuresprognostic factors and outcomes from the Europeanmantle celllymphomanetworkrdquoAnnals of Oncology vol 24 no 8 pp 2119ndash2123 2013
[3] A Ferrer F Bosch N Villamor et al ldquoCentral nervous systeminvolvement inmantle cell lymphomardquoAnnals of Oncology vol19 no 1 pp 135ndash141 2008
[4] L A Honigberg A M Smith M Sirisawad et al ldquoThe Brutontyrosine kinase inhibitor PCI-32765 blocks B-cell activationand is efficacious in models of autoimmune disease and B-cellmalignancyrdquo Proceedings of the National Academy of Sciences ofthe United States of America vol 107 no 29 pp 13075ndash130802010
[5] R W Hendriks S Yuvaraj and L P Kil ldquoTargeting Brutonrsquostyrosine kinase in B cell malignanciesrdquo Nature Reviews Cancervol 14 no 4 pp 219ndash232 2014
[6] E Montserrat F Bosch A Lopez-Guillermo et al ldquoCNSinvolvement in mantle-cell lymphomardquo Journal of ClinicalOncology vol 14 no 3 pp 941ndash944 1996
[7] M L Wang S Rule and P Martin ldquoTargeting BTK withibrutinib in relapsed or refractory mantle-cell lymphomardquo TheNew England Journal of Medecine vol 369 no 6 pp 507ndash5162013
[8] M L Wang K A Blum P Martin et al ldquoLong-term follow-up ofMCL patients treated with single-agent ibrutinib updatedsafety and efficacy resultsrdquo Blood vol 126 no 6 pp 739ndash7452015
[9] R H Advani J J Buggy and J P Sharman ldquoBruton tyrosinekinase inhibitor ibrutinib (PCI-32765) has significant activity inpatients with relapsedrefractory B-cell malignanciesrdquo Journalof Clinical Oncology vol 31 no 1 pp 88ndash94 2013
[10] FDA ldquoClinical Pharmacology Reviews Ibrutinib205552Orig1s000rdquo 2013
[11] S Bernard L Goldwirt S Amorim et al ldquoActivity of ibrutinibin mantle cell lymphoma patients with central nervous systemrelapserdquo Blood vol 126 no 14 pp 1695ndash1698 2015
[12] D L Tucker G Naylor A Kruger M S Hamilton G Followsand S A Rule ldquoIbrutinib is a safe and effective therapy forsystemic mantle cell lymphoma with central nervous systeminvolvementmdasha multi-centre case series from the United King-domrdquo British Journal of Haematology 2016
[13] AWanquet R Birsen R LemalMHunault V Leblond andTAurran-Schleinitz ldquoTo the editor Ibrutinib responsive centralnervous system involvement in chronic lymphocytic leukemiardquoBlood vol 127 no 19 pp 2356ndash2358 2016
[14] C S Tam T Kimber and J F Seymour ldquoIbrutinibmonotherapyas effective treatment of central nervous system involvement bychronic lymphocytic leukaemiardquo British Journal of Haematol-ogy vol 176 no 5 pp 829ndash831 2016
[15] A Cabannes-Hamy R Lemal L Goldwirt et al ldquoEfficacy ofibrutinib in the treatment of Bing-Neel syndromerdquo AmericanJournal of Hematology vol 91 no 3 pp E17ndashE19 2016
[16] J-Y Lee S Y Lee S J Oh K H Lee Y S Jung and S K KimldquoAssessment of drug-drug interactions caused by metabolism-dependent cytochrome P450 inhibitionrdquo Chemico-BiologicalInteractions vol 198 no 1-3 pp 49ndash56 2012
[17] KOhyamaMNakajimaM Suzuki N ShimadaH Yamazakiand T Yokoi ldquoInhibitory effects of amiodarone and its N-deethylated metabolite on human cytochrome P450 activitiesprediction of in vivo drug interactionsrdquo British Journal ofClinical Pharmacology vol 49 no 3 pp 244ndash253 2000
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Case Reports in Hematology
especially in a very serious and prognostically unfavorablecondition lacking efficacious therapeutic alternatives for thelong-term control of the disease
This result could suggest modulating the standard dosein some cases reducing both off-target effects and drug-related complications and allowing treating a larger numberof patients
Conflicts of Interest
The authors declare no competing financial interests
Authorsrsquo Contributions
Donato Mannina and Barbara Loteta collected the dataDonato Mannina wrote the paper Donato Mannina andBarbara Loteta conducted diagnostic and therapeutic man-agement of the patient
References
[1] S Swerdlow E Campo N Harris et al WHO classificationof tumors of hematopoietic and lymphoid tissues InternationalAgency for Research and Cancer Lyon France 4th edition2008
[2] C Y Cheah A George E Gine et al ldquoCentral nervoussystem involvement in mantle cell lymphoma Clinical featuresprognostic factors and outcomes from the Europeanmantle celllymphomanetworkrdquoAnnals of Oncology vol 24 no 8 pp 2119ndash2123 2013
[3] A Ferrer F Bosch N Villamor et al ldquoCentral nervous systeminvolvement inmantle cell lymphomardquoAnnals of Oncology vol19 no 1 pp 135ndash141 2008
[4] L A Honigberg A M Smith M Sirisawad et al ldquoThe Brutontyrosine kinase inhibitor PCI-32765 blocks B-cell activationand is efficacious in models of autoimmune disease and B-cellmalignancyrdquo Proceedings of the National Academy of Sciences ofthe United States of America vol 107 no 29 pp 13075ndash130802010
[5] R W Hendriks S Yuvaraj and L P Kil ldquoTargeting Brutonrsquostyrosine kinase in B cell malignanciesrdquo Nature Reviews Cancervol 14 no 4 pp 219ndash232 2014
[6] E Montserrat F Bosch A Lopez-Guillermo et al ldquoCNSinvolvement in mantle-cell lymphomardquo Journal of ClinicalOncology vol 14 no 3 pp 941ndash944 1996
[7] M L Wang S Rule and P Martin ldquoTargeting BTK withibrutinib in relapsed or refractory mantle-cell lymphomardquo TheNew England Journal of Medecine vol 369 no 6 pp 507ndash5162013
[8] M L Wang K A Blum P Martin et al ldquoLong-term follow-up ofMCL patients treated with single-agent ibrutinib updatedsafety and efficacy resultsrdquo Blood vol 126 no 6 pp 739ndash7452015
[9] R H Advani J J Buggy and J P Sharman ldquoBruton tyrosinekinase inhibitor ibrutinib (PCI-32765) has significant activity inpatients with relapsedrefractory B-cell malignanciesrdquo Journalof Clinical Oncology vol 31 no 1 pp 88ndash94 2013
[10] FDA ldquoClinical Pharmacology Reviews Ibrutinib205552Orig1s000rdquo 2013
[11] S Bernard L Goldwirt S Amorim et al ldquoActivity of ibrutinibin mantle cell lymphoma patients with central nervous systemrelapserdquo Blood vol 126 no 14 pp 1695ndash1698 2015
[12] D L Tucker G Naylor A Kruger M S Hamilton G Followsand S A Rule ldquoIbrutinib is a safe and effective therapy forsystemic mantle cell lymphoma with central nervous systeminvolvementmdasha multi-centre case series from the United King-domrdquo British Journal of Haematology 2016
[13] AWanquet R Birsen R LemalMHunault V Leblond andTAurran-Schleinitz ldquoTo the editor Ibrutinib responsive centralnervous system involvement in chronic lymphocytic leukemiardquoBlood vol 127 no 19 pp 2356ndash2358 2016
[14] C S Tam T Kimber and J F Seymour ldquoIbrutinibmonotherapyas effective treatment of central nervous system involvement bychronic lymphocytic leukaemiardquo British Journal of Haematol-ogy vol 176 no 5 pp 829ndash831 2016
[15] A Cabannes-Hamy R Lemal L Goldwirt et al ldquoEfficacy ofibrutinib in the treatment of Bing-Neel syndromerdquo AmericanJournal of Hematology vol 91 no 3 pp E17ndashE19 2016
[16] J-Y Lee S Y Lee S J Oh K H Lee Y S Jung and S K KimldquoAssessment of drug-drug interactions caused by metabolism-dependent cytochrome P450 inhibitionrdquo Chemico-BiologicalInteractions vol 198 no 1-3 pp 49ndash56 2012
[17] KOhyamaMNakajimaM Suzuki N ShimadaH Yamazakiand T Yokoi ldquoInhibitory effects of amiodarone and its N-deethylated metabolite on human cytochrome P450 activitiesprediction of in vivo drug interactionsrdquo British Journal ofClinical Pharmacology vol 49 no 3 pp 244ndash253 2000
Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpswwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom