identifying people who are likely to be in the last year of...
TRANSCRIPT

www.england.nhs.uk
Programme Board deep dive
session
Identifying people who are likely to
be in the last year of life
9th August 2017
Chaired by:
Professor Bee Wee,
National Clinical Director for End of Life Care
NHS England

www.england.nhs.uk
Purpose of the session:
• To provide an overview on why identification is important; what the current situation is and some of the tools available
• To hear different perspectives from across the system on identification including: people with lived experience; clinicians/providers and commissioners
• To inform the scope of a project NHS England will lead in this area to improve identification of those in the last year of life and agree actions and next steps across system

www.england.nhs.uk
Throughout the presentation - consider the
following questions, which we’ll come back to at
the end:
• What mechanism should we use for supporting better identification?
• Should we be using prognostication tools? If so, how do we encourage /enable use of the tools?
• Are there any barriers or opportunities not already raised?
• Is there any other national work we need to be aware of which may have an impact on this project?
• What leverage options do we have?
• What else do we need to consider?
• What are the agreed actions and next steps?

www.england.nhs.uk
Scene setting: context

www.england.nhs.uk
Why?
For the person
• Opportunity to initiate conversations about important
decisions – now, for future and in parallel
• Optimise symptom management and quality of life
• Encourage person to consider and discuss views and
preferences with family and those close to them

www.england.nhs.uk
Why?
For clinicians and ‘system’
• Triggers proactive approach and MDT involvement
• Documentation:
• Facilitates information sharing across organisational boundaries
• Data monitoring for inequalities
• Pitfalls with over-identification
• Aiming for the right outcomes

www.england.nhs.uk
Current situation
• Identification – patchy, often not timely
• GP – specialist: who triggers?
• Cancer vs non-cancer difference in GP registers:
• 48-66% of people with cancer on register vs <20%
non-cancer

www.england.nhs.uk
Tools to assist identification
CLINICAL JUDGEMENT, supported by:
• Surprise question
• Gold Standards Framework Proactive Identification
Guidance (ex-Prognostic Indicator Guidance)
• Supportive and Palliative Care Indicators Tool (SPICT)
• Palliative Performance Scale
• Palliative Prognostic Index
• Prognosis in Palliative Care
• …….

www.england.nhs.uk
Accuracy of Surprise Question
• Systematic review: 22 papers
• 25,718 estimates: clinician intuition correct in 82%
• Meta-analysis:
• Correct prediction of outcome: 74.8%
• Slightly higher as more imminent: 76.4%
• Doctors slightly more accurate than nurses:
• C-statistic: 0.735 (docs) vs 0.632 (nurses)
• Accuracy better in cancer:
• 78.6% (cancer) vs 76.1% (renal) vs others (72.3%)
• But low proportion of deaths in each study (16% overall) and low numbers of high quality studies included
Ref: White et al, 2017

www.england.nhs.uk
Discussion today….
• How can we improve identification or recognition of people
with advanced conditions who are at risk of deteriorating
and dying, such that they could benefit from holistic needs
assessment and proactive care planning?
• Whilst avoiding:
• inherent inaccuracies in prognostication, and
• pitfalls of over-identification?

www.england.nhs.uk
A Service user perspective
Tony Bonser
Patient & Public Voice representative
Diana Robinson
Patient & Public Voice representative

www.england.nhs.uk
Clinicians/service
providers perspective
Catherine Millington-Saunders
RCGP and Marie Curie National EoLC Clinical Champion
David Warriner & Dr Lucy Flanders
National Medical Director’s Clinical Fellows
NHS England

General Practice
Deep Dive Identification
Dr Catherine Millington-Sanders
RCGP and Marie Curie National EOLC Clinical
Champion
9th August 2017
1
3

Main Funding Sources
• GMS and PMS contracts
• QOF and Clinical Disease Registers
• National or Locally Enhanced Services

GMS and PMS contracts
General Medical Services
The contract provides a ‘global sum’, which is
determined by linking the amount paid to a
practice to the needs of its registered patients.
Personal Medical Services
rather than a ‘global sum’, PMS providers are
paid a fixed annual rate for the provision of
services. This is another way of allowing them to
tailor their services to meet local needs.

QOF – PC Clinical Disease Register
The value of a QOF point for 2016/18 is £165.18.

Rise in multi-morbidity

And complexity
Systems on the left, the population is on the right

Why is this Important to General
Practice

Traditional bio-medical model
History
Examine
Physical or
mental
state
What is the
problem
and how
does it
affect you
Investigations
Blood tests x-
rays, scans etc.
Diagnosis
Differential
or absolute
diagnosis of
the
presenting
problem
Treat
Medication
advice,
surgery
and/or
referral
Review
Reassess
diagnosis
and/or
impact of
treatment
Of course, life is not so easy and
anyway medicine is rarely a simple
straight forward linear process!!!
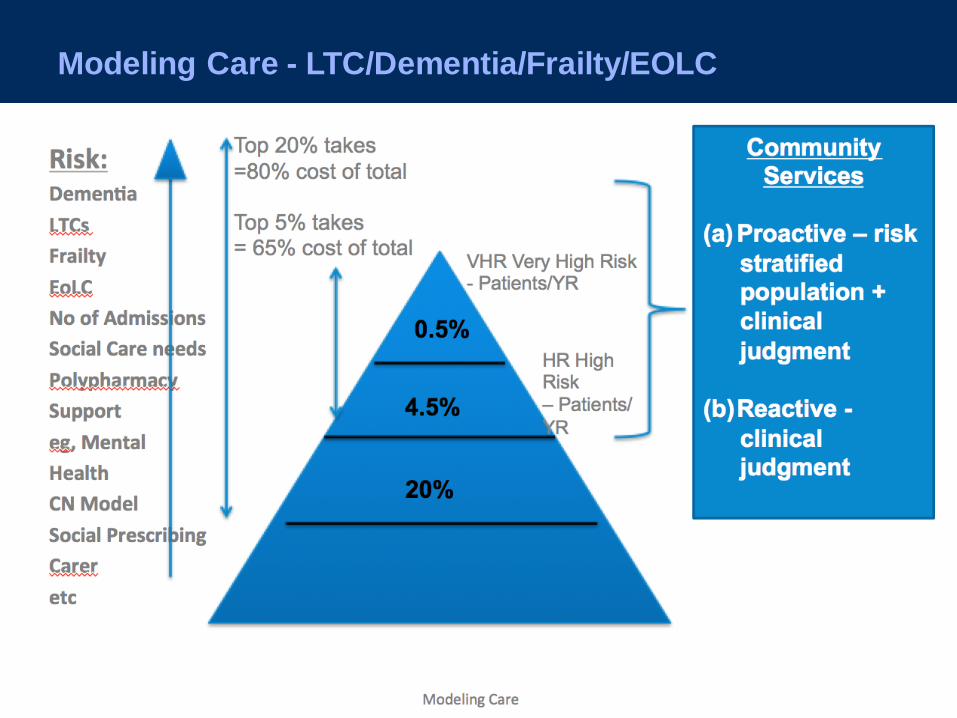
Modeling Care - LTC/Dementia/Frailty/EOLC
Top 20% takes
=80% cost of total
Top 5% takes
= 65% cost of total VHR Very High Risk - Patients/YR
0.5
% 4.5
% 20%
HR High Risk – Patients/YR
Community
Services
(a)Proactive
– risk
stratified
populatio
n +
clinical
judgment
(b)Reactive
- clinical Modeling Care

Impact on the System
3 59 14 21
3447
64
85100
151
20
31
51
74
115
151
200
242
318
342
479
0
100
200
300
400
500
600
0 1 2 3 4 5 6 7 8 9 10+
An
nu
al a
dm
issi
on
rat
e p
er
10
00
pat
ien
ts
No of conditions
Potentially preventable admission
Other emergency admissions
And on us!
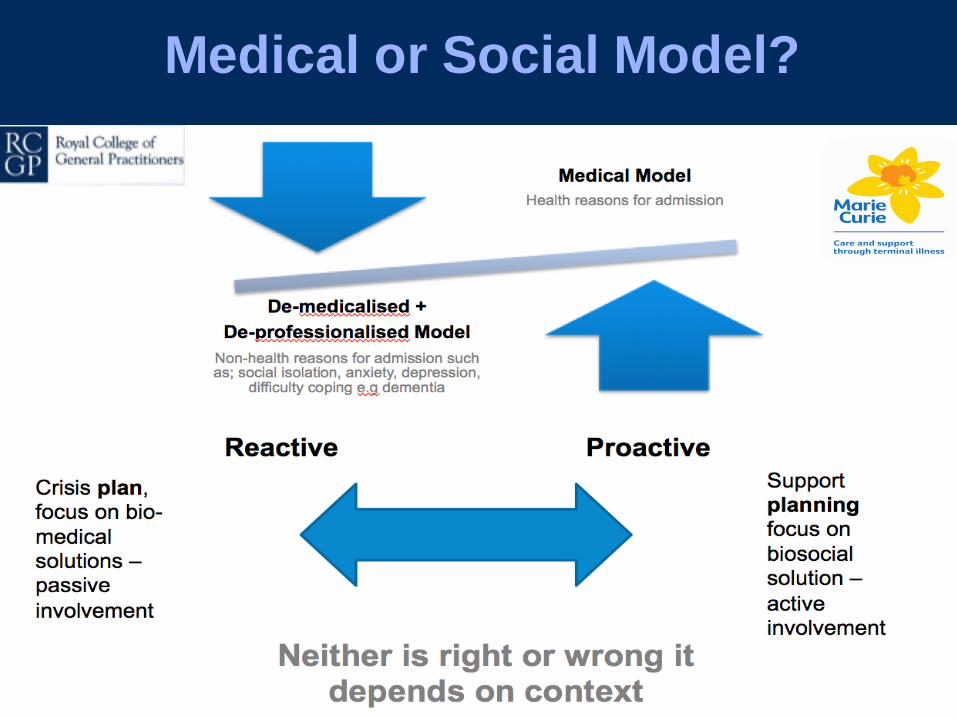
Medical or Social Model?
Crisis plan,
focus on bio-
medical
solutions –
passive
involvement
Support
planning
focus on
biosocial
solution –
active
involvement
Neither is right or wrong it
depends on context
Reactive Proactive

MDT

A proactive social model
Care and Support planning: a consultation model for
Long Term Conditions – Page 11
Think Local Act Personal, Personalised care and support planning tool. Available at: http:// www.thinklocalactpersonal. org.uk/personalised-care-and-support-planning-tool
http://www.rcgp.org.uk/clinical-and-research/our-programmes/~/media/Files/CIRC/Care%20Planning/stepping-forward-web-061015a.ashx

Purpose
UK General Practice:
Quality Improvement Standards
For Advanced Serious Illness + EOLC
Free, self-directed resource for practices
Robust, evidence-based quality
improvement step-by-step guidance
To inspire, support and enable general
practice to improve EOLC quality and
outcomes, at scale.

The 8 Standards
Standard 1: Professional and competent staff
Standard 2: Early identification
Standard 3: Carer Support - pre and post death
Standard 4: Seamless, planned, coordinated care
Standard 5: assess unique needs of the patient
Standard 6: Quality care during the last days of life
Standard 7: Care after death
Standard 8: General Practice being hubs within
Compassionate Communities

Next steps?
RCGP Quality Improvement team review
Working Group of practicing
clinicians/commissioners/legal/ PPI for independent
review and challenge – June 2017
Pilot practices/ CCGs to commence–Sept/Oct 2017
Pilot evaluation and model evolution–Feb-Mar 2018
Wider implementation and evaluation to
start April 2018

Dr Catherine Millington-Sanders
RCGP and Marie Curie National End of
Life Care Clinical Champion
For more information:
Acknowledgement: CCSP slides from Dr. David Paynton
Clinical Lead for RCGP Centre for Commissioning

IDENTIFICATION OF PATIENTS AT THE END OF
THEIR LIFE C ON D I T I ON S PE C I F I C G U I D E
Dr David Warriner and Dr Lucy Flanders
National Medical Director’s Clinical
Fellows
NHS ENGLAND

BACKGROUND
• The Ambitions for Palliative and End of Life Care focuses on 6 key
ambitions.
• This is further supported by the foundation of ‘Personalised Care
Planning.’
“everyone approaching the end of life must be offered the chance to
create a personalised care plan.”

BACKGROUND
• The focus of end of life care is often on managing patients with a
cancer diagnosis
• We identified that there is a less unified approach to those with non-
cancer diagnosis, despite the numbers of elderly patients with
multiple co-morbidities and chronic disease
• The numbers of patients approaching the end of life with multiple
morbidities is increasing and it was felt necessary to think about how
guidance could be developed to help in the management of this cohort
• Decision to hold a scoping workshop with a multidisciplinary group
of generalists and specialists with an interest in end of life care

SPECIALIST INTERVIEWS
• Conducted with a range of senior healthcare professionals e.g. commissioners,
NCD’s, specialist nurses, GP’s and specialists.
• Designed to feed into the workshop and help shape the input and output
• Common themes :
• multi-morbidity, community,
• identification
• transfer of patients
• everyone's responsibility
• prognostic uncertainty


NON-CANCER WORKSHOP KEY THEMES
When is the right
time to have the
conversation?
Who should be having
the discussion?
primary/secondary/palliat
ive care?
Interface between primary and
secondary care- documentation,
conversations, discharge summaries
Every transition between care setting,
should be an opportunity for a discussion
Unpredictable disease
trajectories
Complex patients,
therefore seen by
multiple
specialties…who takes
the lead?
Poor evidence base around
prognostic indicators
Importance of using
the right language

CONCLUSIONS FROM THE WORKSHOP
• A group of clinical fellows met to discuss the key
themes raised from the workshop and to
determine what they felt should be the outputs of
the meeting
• A number of different options were considered
• What does good look like for end of life care in
patients with a non-cancer diagnosis?
• Need to be solution not problem focused
• These were presented to the EOLC team
• Conclusion was to produce condition specific
guidance for recognition and care of patients at the
end of their life for the generalist

OUR PLAN
• Each fellow to compose a
guidance document for their
area of interest
• For there to be a common
format for the guidance
• Introduction of a new toolkit
named REACT
• Request input from experts,
patients and specialist
organisations

OBJECTIVES OF THE DOCUMENT
• To include key symptoms which allow identification of patients at
end of life
• To include a patient perspective
• Condition specific top tips for managing the patient
• Encourage the involvement of other healthcare professionals early
on
• Focus on the importance of communication involvement of the
MDT team and shared decision making, in keeping with the
Ambitions.
• Highlight available resources that may be less well known to
healthcare professionals

OUR VISION
• Creation of a suite of documents
• Available to all healthcare professionals, but aimed at the
generalist
• NHS England document, but supported by specialist organisations
• Dissemination through patient organisations, specialist societies, royal
colleges

WHAT WE HAVE ACHIEVED SO FAR
• Two mature draft documents for respiratory and cardiovascular disease,
with a third for liver disease in development
• Input received from NCDs
• Input received from British Lung Foundation, British Society for Heart
Failure, British Thoracic Society
• Contact made with the RCGP

WHAT WE STILL NEED TO DO
• Consult expert patient groups
• Request a review of the document from the generalists
• Consider whether there needs to be a patient translated document
• Who is going to own this document?
• How do we measure impact?
• Requirement to keep document up to date- who is going to sustain this?

HOW CAN YOU HELP US?
• What do you think of the documents?
• Can you point us in the direction of expert patients?
• Where do you think the documents would be best placed?
• Any ideas for dissemination?

www.england.nhs.uk
A commissioner
perspective
Jacqueline Lansley
Director of Strategy, Commissioning &
Procurement
Integrated Commissioning Team
NHS Southend CCG and Southend-on-Sea
Borough Council

End of Life
A South East Essex approach to identification

• Identification happens via health and care professionals asking the simple question …. • ‘would I be surprised if the patient died within the next 12
months?’
• Health and care professionals range from GPs, Care Homes, Community Health, Hospice, Hospital, ambulance service etc
• Referrals are made to South East Essex Palliative Care Support Register (PCSR)
• PCSR maintained on SystmOne and managed by Community Health provider
• The benefits of being on the PCSR are better / more bespoke care, reduced admissions and a higher rate of achieving preferred place of death
Identification (1)

• SEE total population is circa 360K. National figures suggest that 1% of population will die per year of which 25% will be sudden / accidental
• We therefore expect for 2,700 people be in classed as EoL
• As at June 2017 the PCSR has 1307 patients registered as EoL
• Capacity to deliver enhanced services aside, there are circa 1400 patients in SEE who should be on the register
• This represents a challenge for SEE health and care providers to identify patients for the register
Identification (2)

• Other ways of identifying patients for the PCSR include;
• Serious Illness Conversation training;
• EoL champion within the Ambulance service;
• Treatment & Escalation planning;
• Macmillan GPs
Identification (3)

Increasing identification (1) … to increase confidence and raise profile of register
• Audit of Out of Hours (OOH) data for EoL patients; – Making sure that we understand the types of service
EoL patients require OOHs to ensure there is a benefit of being referred to the register
• Making sure the register is effective; – Time of referral (i.e. early enough to make a difference
to quality of life and not just referring in last days of life)
– Ensuring that there is enough staff to provide a high quality of care

• Treatment & Escalation planning;
– Hospital working in partnership with community health and primary care to provide high quality care for EoL register patients
• One care record across the system;
– Access to care records from health and care providers from different organisations
Increasing identification (2) … to increase confidence and raise profile of register

• Treatment & Escalation planning;
– Hospital working in partnership with community health and primary care to provide high quality care for EoL register patients
• One care record across the system;
– Access to care records from health and care providers from different organisations. Challenge is for the hospital to provide access to staff to SystmOne
Increasing identification (3) … to increase confidence and raise profile of register

• GP training;
– Vast majority of interaction with potential EoL patients is with primary care
– Resource and efforts being made to encourage primary care to refer patients to register, eg serious illness conversation, Mac GP, Governing Body lead by examples etc
Increasing identification (4) … to increase confidence and raise profile of register

Key Challenges
• Ownership of referrals to the register;
• Timeliness of referrals to the register;
• Current capacity of register team and keyworkers to undertake advanced care plans;
• Resource required for SystmOne rollout at hospital;
• Engagement with wider system professionals for Treatment & Escalation plans
• Data

www.england.nhs.uk
Questions for board discussion:
• What mechanism should we use for supporting better identification?
• Should we be using prognostication tools? If so, how do we
encourage /enable use of the tools?
• Are there any barriers or opportunities not already raised?
• Is there any other national work we need to be aware of which may have an impact on this project?
• What leverage options do we have?
• What else do we need to consider?
• What are the agreed actions and next steps?