idiopathic club foot
TRANSCRIPT

Done by\ malika hameedGroup D
Talipes Equinovarus
Talipes Equinovarus
* Talipes: derived from talus ( L = ankle bone ) and pes ( L = foot ).
* Equinovarus: one of the several different deformities of talipes and means that the entire hindfoot is in varus and the mid & forefoot are adducted and supinated.
* Others: Talipes calcaneus & Talipes valgus.


Incidence
* 1-2 every 1000 live births.
* Boys : Girls → 2 : 1 .
* Sporadic but may be autosomaldominant trait.
* Bilateral in 50% of patients or in one third of cases.

Causes / Mechanisms
1- Genetic defect : primary germ plasm defect in the talus causes continued planter flexion and inversion of this bone and soft tissue changes.
2- Form of arrested development.
3- Neuromuscular disorder : primary soft tissue abnormalities within neuromuscular units cause secondary bony changes , e.g : neural tube defect.




What part of the foot is affected?
Clubfoot primarily affects three bones: calcaneus, talus and navicular.
The deformity can affect the growth of the entire foot to some degree so other bones may be involved as well.
Pathological Anatomy
①Talus :
- Neck : downwards , deviated medially.
- Body : rotated slightly outwards in relation to calcaneus and ankle mortise.
②Calcaneus :
- Posterior part is held close to fibula by a tight calcaneo-fibular ligament and tilted into equinus and medially rotated beneath the ankle.

③Navicular & the entire forefoot :
- Shifted medially and rotated into supination.
④Metatarsals : adducted & deviated at tarsometatarsal joints.


Clinical Picture
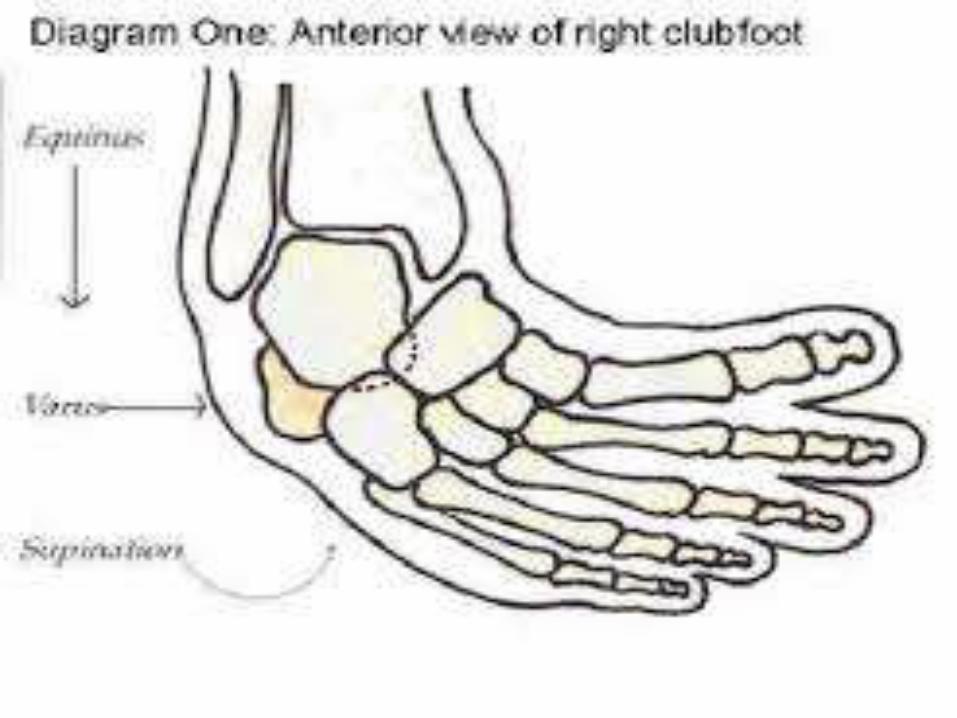
1- Foot is turned & twisted inwards , so the sole faces posteromedially with high medial arch ( cavus ) & smaller than the other normal foot.
2- Ankle is in equinus.
3- Forefoot is adducted & supinated.
4- Skin & soft tissues of the calf &medial side of the foot are short & underdeveloped.
5- The heel is small & high.
6- Deep creases appear posteriorly & medially.


Examination
* In infants :
examine associated disorders as congenital hip dislocation & spina bifida.
* 3 Basic components of club foot :
equinus , varus , adduction , & may be cavus.


Roentgenographic Evaluation
* Before , during & after treatment.
* To assess progress after treatment.
* 3 views:
- AP with foot 30° planter flexion & tube angled 30°.
- Stress dorsiflexion lateral view of both heels.
- Lateral standing view : in older children.
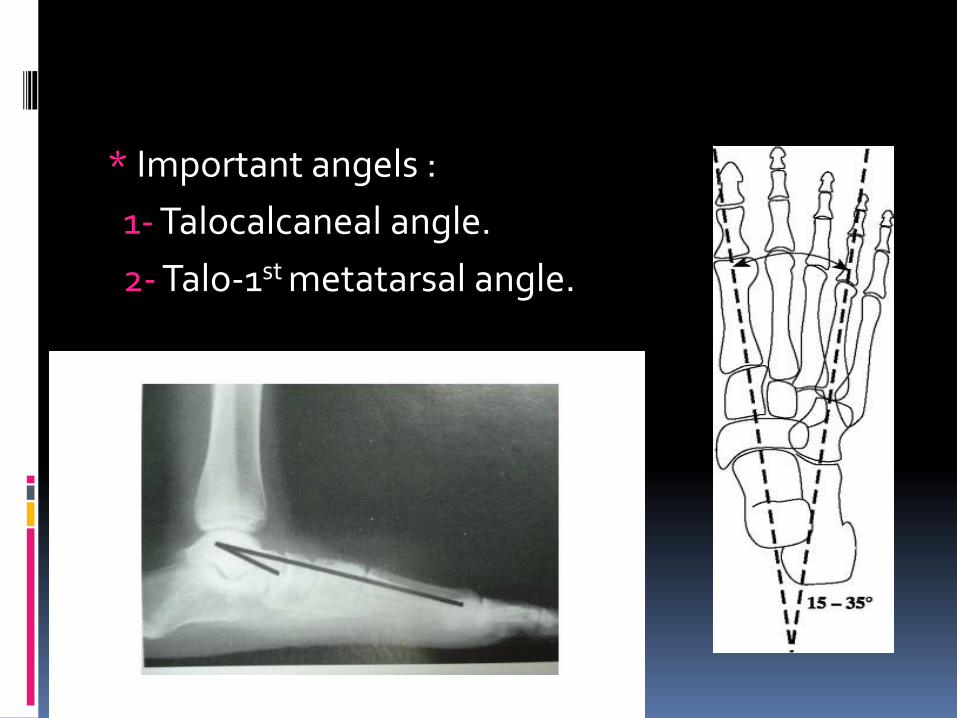
* Important angels :
1- Talocalcaneal angle.
2- Talo-1st metatarsal angle.
AP film
- Line is drawn through the long axis of talus parallel to its medial border & through the calcaneus parallel to its lateral border , normally cross at angle 20°- 40° “ Kite’s angle
“, in club foot , the two lines may be parallel.

Lateral Film
* Foot is forced dorsiflexion.
* Line is drawn through the mid-longitudinal axis of talus & lower border of calcaneus , normally the angle is 40°.
* If the angle is less than 20° >>> club foot.
* Angles normally changes with age.
* Club foot can’t be dorsiflexed , but if so , it will be broken at the midtarsal level producing “Rocker – Bottom deformity”.


Treatment
- Aim : to produce & maintain a plantigrade , replase may occur in neuromuscular disorders babies.
① Non-operative : the initial treatment.
- Repeated manipulation & adhesive strapping.
- Weekly serial manipulation & light plaster cast during the first 6 weeks of life followed by manipulation & casting every the other week untill the foot clinically & roentgenohraphiccorrected.

* With experience , predict which feet will respond to non-surgical treatment.
* The more the rigid the initial deformity , more likely surgical treatment.
* The order of correction :
1- Correction of forefoot adduction : rotational alignment with hindfoot , by ↑ supination deformity.
2- Correction of hindfoot & forefoot for varus & supination by keeping fulcrum on the lateral side of head of talus.
3- Correction of hindfoot equinus by bringing the heel down & dorsiflexing the ankle & percutaneous tendo Achillislengthening.

* The aim of the order is to prevent “Rocker Bottom Deformity”by dorsiflexing the foot from the hindfoot rather than midfoot , but if occurs, forefoot placed back in planter flexion , casting & surgery is important here.
* Casting by Kite , modified by Lovell & Hancock.
* Manipulation & casting success rate is 15-80%.
* Resistant cases declare after 8-12 weeks of serial manipulation & strapping , so early surgery or continued conservative treatment is indicated.
* Delaying surgery untill child walking >>> surgery is easier & maintenance of the correction. It is suitable for severe ,
rigid deformities.
* Less severe cases >>> operation at 6 months.







Operative Treatment ②

Operative Treatment
* Indication :
1- No response to conservative treatment often in children with significant rigid deformity.
2- Deformity has recurred.
3- The forefoot has been corrected by conservative treatment but hindfoot remains fixed in both varus & equinus.
* Surgical treatment is according to the age of child & deformity to be corrected.

* Objectives :
1- Complete release of joint tethers.
2- Lengthening of tendons.

Incisions
1- Posteromedial incision >>> Turco.
2- Posterior curved transverse , extended anteriorly on both sides medial & lateral >>>Cincinatti – Crawford.
3- Posterolateral with separate curved medial incision >>> Caroll.



* To correct equinus :
1- Achillis tendon & tibialis posterior tendon are lengthened through Z-divisions.
2- Posterior capsules of ankle & subtalar joints are divided.
* To correct cavus :
1- Release contractures around talonavicular & calcanocuboid joints.
2- Origin of intrinsic muscles & planter fascia from calcaneum are divided.


* The foot , in its corrected position , is immobilized in a plaster cast.
* Kirshner wires >>> across talonavicular & subtalar joint.
* Wires & cast are removed at 6-8 weeks.

* After immobilization , hobble boots “Dennis
Browne “.
* Stretching exercises are continued.

Dennis Browne “

DAFOs for Clubfoot:designed for soft, comfortable repositioning of
clubfoot or maintaining post-surgical positions

Late or relapsed club foot
* Late >>> comes with secondary bony changes.
* Relapsed >>> scarring of previous surgery.
*Youngs ( 4-7 ) years >>> calcaneo-cuboid fusion or cuboid enucleation ( Dilwyn Evans ).
* Calcaneal osteotomies >>> for varus.
* Tendon transfer.
* Circular external fixator ( Ilizarov method ) >>> gradual correction.



Metatarsus adductus

* Varies from slightly curved forefoot to mild club foot.* Management :
- 90% improve spontaneously.- corrective casts followed by straight last shoes.- Extensive capsulectomy of tarsometatarsal
joints. No splintage to avoid early degenerative arthritis.
- Dilwyn Evans procedure + Basal metatarsal osteotomy.
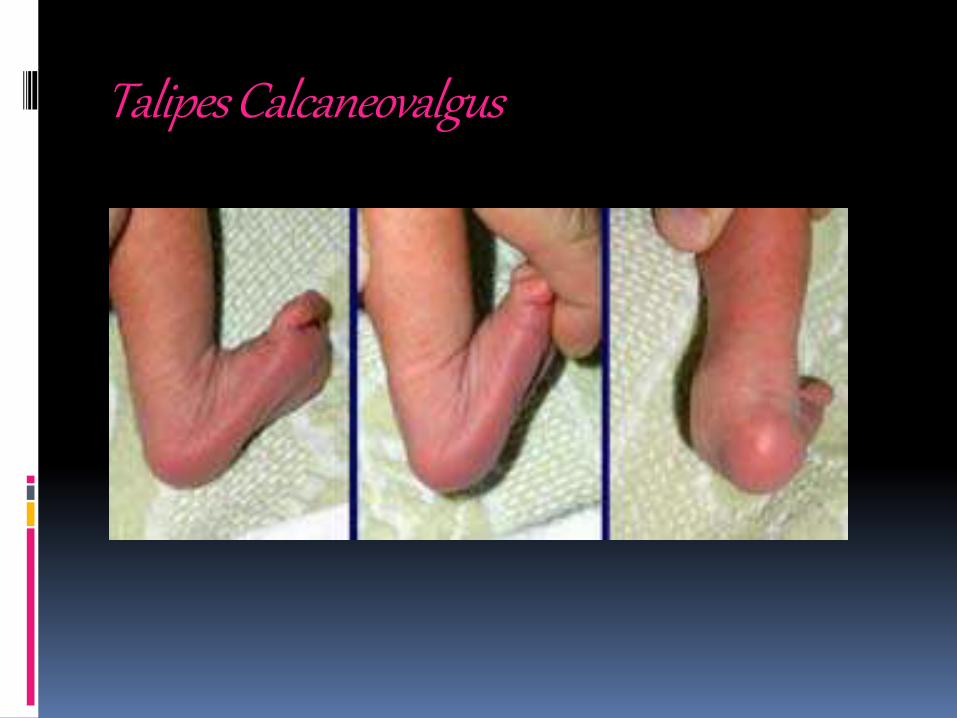
Talipes Calcaneovalgus
