if fifty is the new forty…then 1 st trimester screening is the new thirty five james keller md
Post on 21-Dec-2015
214 views
TRANSCRIPT
IF FIFTY IS THE NEW FORTY…THEN 1ST TRIMESTER SCREENING IS THE
NEW THIRTY FIVE
James Keller MD

BACKGROUND

Down Syndrome Risk AssessmentDown Syndrome Risk Assessment
• Maternal age was the original “screening test” used in determining which women would undergo invasive testing for fetal Down syndrome.
• Since most children with Down syndrome are born to women younger than 35, most affected pregnancies will not be detected using age as a screening test.
• In the early 1980s it was discovered that MSAFP was significantly lower in mothers carrying a fetus affected with trisomy 21 (0.74 MoM).
• Other analytes added to refine screening to increase detection rate and to decrease false positives

QUAD SCREEN
• Intact HCG is 2.06 MoM in DS compared to euploid • Unconjugated estriol is is 0.75MoM compared to
euploid• Inhibin A 1.77 MoM in DS compared to euploid• The detection rate of the quad screen was 80% with
a 5% false positive rate• This is a good test..remember why we wanted better
Timing of Aneuploidy Risk Assessment
• Data from patient questionnaires demonstrated a clear preference for earlier risk assessment, even at the risk of slightly higher FPR and/or slightly lower detection rates
Spencer et al. Ultrasound Obstet Gynecol 2004;24:735.Sharma et al. Am J Obstet Gynecol 2005; 193: 1429.

Nuchal Translucency
“…The skin…is deficient in elasticity, giving the appearance of being too large for the body.”
Down L. Observations on an ethnic classification of idiots. Clin Lectures and Reports 1866;3:259-62.
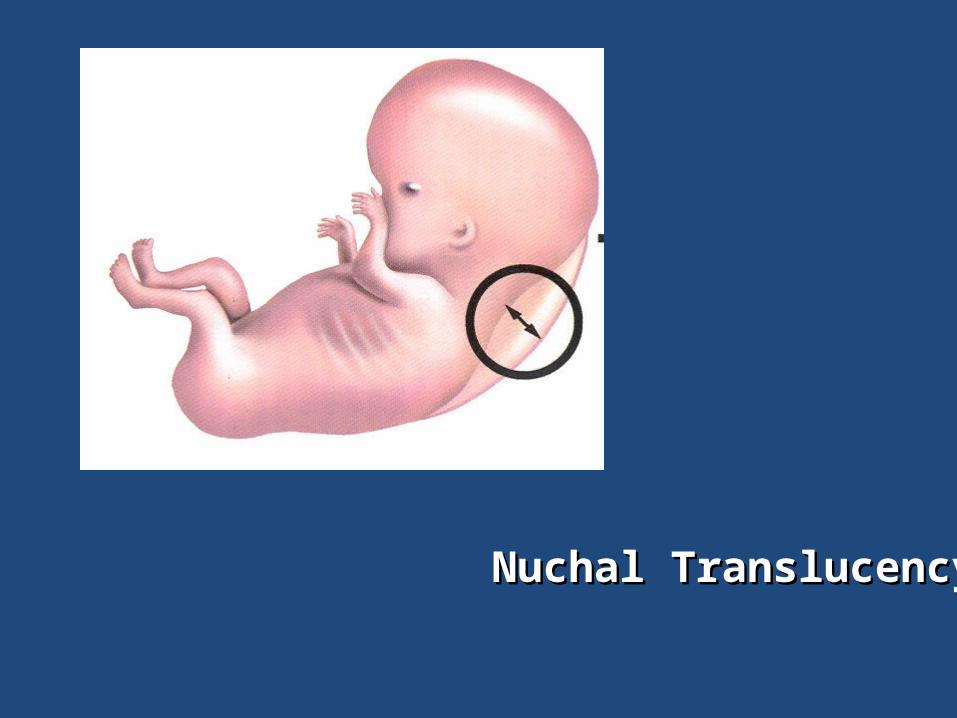
Nuchal TranslucencyNuchal Translucency

Nuchal TranslucencyNuchal Translucency
• Gestation 11w1d-13w6dGestation 11w1d-13w6d• CRL 45-84 mmCRL 45-84 mm• Mid-sagittal viewMid-sagittal view• Image size: callipers 0.1mmImage size: callipers 0.1mm• Neutral positionNeutral position• Away from amnionAway from amnion• Maximum lucencyMaximum lucency• Callipers on-to-onCallipers on-to-on
Down Syndrome Risk AssessmentDown Syndrome Risk Assessment
• The Fetal Medicine Foundation screened approximately 100,000 pregnancies in 22 centers in the United Kingdom.
• Standardized techniques were used. • At a risk cutoff of 1 in 300, the sensitivity was 82.2%
for Down syndrome and 77.9% for other chromosomal abnormalities, with a false-positive rate of 8.3%.
Snijders et al. Lancet 1998;351:343.
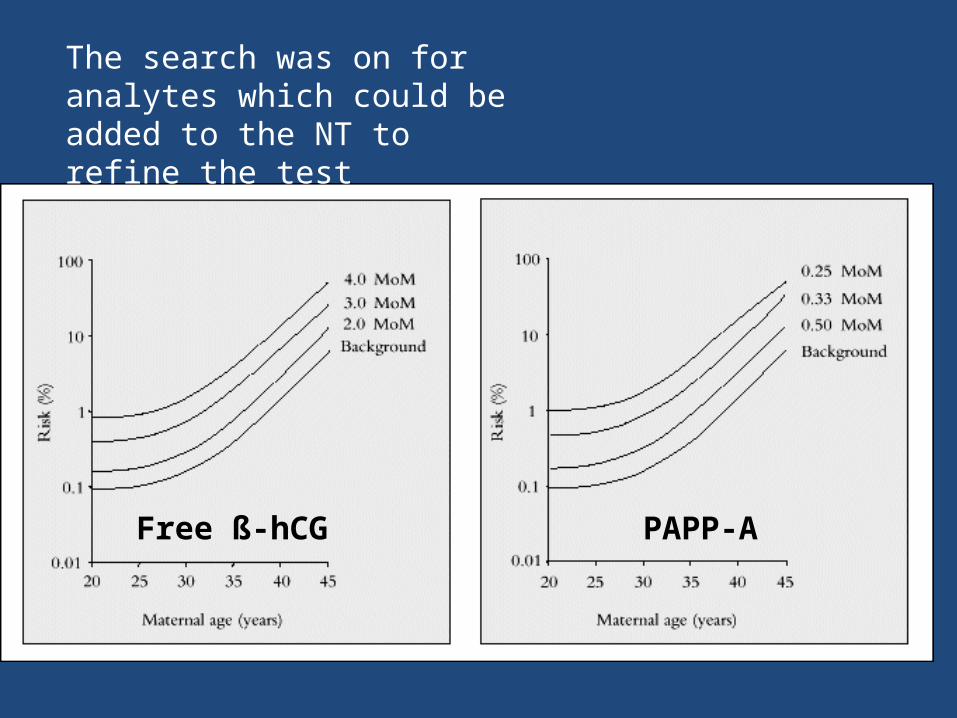
Free ß-hCG PAPP-A
The search was on for analytes which could be added to the NT to refine the test

First Trimester Screening for Trisomies 21 and 18
Wapner et al, NEJM 2003
• Known as the BUN study• Used screening positive parameters still in use• 1/270, for trisomy 21, 1/150 for trisomy 18• 12 participating institutions• 8816 patients

BUN STUDYPATIENT DETECTION RATE
(%) (1/270)FALSE POSITIVE (%)
MATERNAL AGE 80 48AGE + BIOCHEM 85 23AGE + NT 82 12AGE + NT + BIOCHEM
85 9
AGE<35 67 4 AGE>/= 35 90 15
Proved effective screening possible in the 1st trimester
It was to be expected that a trial be performed to look at all screening
tests to date

First-Trimester or Second-Trimester Screening, or Both, for Down's Syndrome
Fergal D. Malone, M.D., Jacob A. Canick, Ph.D., Robert H. Ball, M.D., David A. Nyberg, M.D., Christine H. Comstock, M.D., Radek Bukowski, M.D., Richard L. Berkowitz, M.D., Susan J. Gross,
M.D., Lorraine Dugoff, M.D., Sabrina D. Craigo, M.D., Ilan E. Timor-Tritsch, M.D., Stephen R. Carr, M.D., Honor M. Wolfe, M.D., Kimberly Dukes, Ph.D., Diana W. Bianchi, M.D., Alicja R. Rudnicka, Ph.D., Allan K. Hackshaw, M.Sc., Geralyn Lambert-Messerlian, Ph.D., Nicholas J.
Wald, F.R.C.P. and Mary E. D'Alton, M.D.
N Engl J MedVolume 353;19:2001-2011
November 10, 2005

WHAT WAS TESTED• 1ST trimester serum screening• 1st trimester combined combined screening (serum+NT)• 2nd trimester quad screen• Independent sequential screening-pt provided results of 1st
and 2nd trimester testing• Stepwise sequential screening, like independent, but overall
2nd trimester risk calculated, using all data• Serum integrated screening-PAPPA+quad screen• Fully integrated uses NT in addition to serum integrated
screening• All tests take into account maternal age
RELEVANT TESTS
• 1ST TRIMESTER COMBINED SCREENING “NT”• QUAD SCREEN• INTEGRATED TEST
– Fully integrated– Serum integrated
• SEQUENTIAL– Independent– Stepwise– Contingent

DETECTION RATE (%)5% FALSE POSITIVE
WEEKS 11 12 13 2ND TRI
TEST
NT 70 68 64
serum 70 67 65
Combined (nt+serum)
87 85 82
Serum integrated 88 86 85
Fully integrated 96 95 94
Triple 69
Quad 81
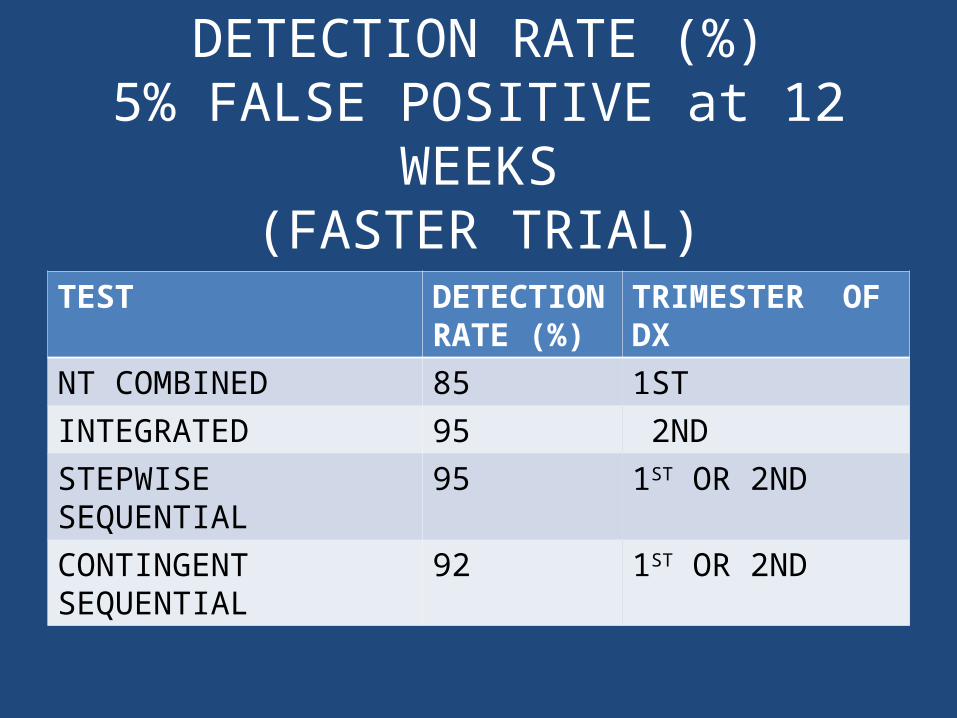
DETECTION RATE (%)5% FALSE POSITIVE at 12 WEEKS
(FASTER TRIAL)
TEST DETECTION RATE (%)
TRIMESTER OF DX
NT COMBINED 85 1STINTEGRATED 95 2NDSTEPWISE SEQUENTIAL 95 1ST OR 2NDCONTINGENT SEQUENTIAL 92 1ST OR 2ND
EXPERT OPINIONACOG
• A strategy that incorporates both first and second trimester screening should be offered to woman who seek prenatal care in the first trimester
• Woman found to have an increased risk of aneuploidy with first-trimester screening should be offered genetic counseling and diagnostic testing
• These are conflicting statements leading to confusion about aneuploidy screening
WOMAN WANT EARLY SCREENING

PATIENT PREFERENCES FOR SCREENING IN THE FIRST TRIMESTER
Werner at al Prenatal Diagnosis 2008
• Formal genetic counseling offering integrated screening or first trimester screening
• 60% chose 1st trimester screening vs. 40% choosing integrated
• As expected the motivation for the choice was early results versus most information

HOW RELEVANT ARE THE DATA TO THE REAL WORLD?
• Almost all studies are based upon modeling rather than a true clinical trial
• There are relatively few clinical trials where these models have been tested
• A case cannot be detected with a screening test alone
• Reluctance to undergo a diagnostic test will lead to an undiagnosed case, even in a screen positive patient
SEQUENTIAL SCREENING IN PRACTICE
STEPWISE SEQUENTIAL SCREENING FOR FETAL ANEUPLOIDYBenn, et al AJOG 2007

Sequential Screening• 1528 woman, average age 36.2 years• 133 woman, positive 1st trimester
– 30 chose cvs – 88 sequenced– 15 stopped
• 88 sequenced– 30 positive
• 25 declined amniocentesis in spite of two positive tests• 5 had amniocentesis
– 58 negative• Of 35 woman who chose invasive testing, 30 chose after 1st
trimester testing

Sequential Screening• 1395 screened negative 1st trimester
– 0 had invasive testing• 1085 sequenced (300 stopped testing)• 30 positive,
– 13 amnios, 17 no testing• ThreeTrisomy 21’s in the 1528patients, two
detected in 1st trimester and one after positive 1st and 2nd trimester tests
Sequential Screening• 1283 patients having 1st trimester elsewhere then
included, due to small numbers• 2456 women, 6 cases of trisomy 21, 5 of six
detected in the 1st trimester• One of six, would have been missed by 1st trimester
screening• One of six, would have been missed by sequential or
certainly integrated screening (1:91, 1:574)• In this study both tests performed equally, with NT
combined yielding an earlier diagnosis
Sequential ScreeningOther Lessons
• The majority of people who screened positive, do not have a diagnostic test-especially those who screen positive twice (25/30), 17 of 30 who screen positive only by their integrated result, also do not test.
• Of the 48 patients who had an indicated diagnostic test with sequential screening-30 chose after the 1st trimester test

CONTINGENT SEQUENTIAL
• Patients undergo 1st trimester screening• If very high risk (>1:30-1:50) are offered
diagnostic testing• If very low risk (<1:1500-1:2000) are finished
with testing• If intermediate, go on to integrated testing
scheme

Contingent Sequential
• Withholding of abnormal test results– Model only works if 1st trimester diagnostic test only
offered to risks much greater than standard accepted (1/30)
• 20-25% of people, will be flagged for further testing– Some with classically low risks (1/500-1000), may
consider an invasive test when they cannot be reassured by 1st trimester results
– This will eliminate any advantage in false positive rate
STEPWISE SEQUENTIAL
• Over 90% of patients will need to proceed to 2nd trimester testing
• Patients with high risk results may be falsely reassured by second test
• Clinical experience shows that those with a positive 1st trimester screen who choose further testing unlikely to have a diagnostic test, thus increasing expense with little contribution to detection rate
Pitfalls of Integrated Testing
• Theoretically this is the best test– Highest detection rate– Lowest false positives
• Is it ethical to withhold a positive screening results in the hopes it will be corrected– And what if it is incorrectly corrected– In true integrated testing you wont know
• What if the test isn’t completed

INTEGRATED TEST
• No shows for second test– Whose liability?
• Withholding abnormal results which could result in significant clinical advantage
• Extra cost• May be an advantage to this test when NT
cannot be performed

COMBINED NT USING FREE BETA hCG
CLINICAL USE OF 1ST TRIMESTER ANEUPLOIDY SCREENING IN A U.S. POPULATION CAN REPLICATE DATA FROM CLINICAL
TRIALSPERNI et al AJOG 2006
CLINICAL USE OF 1ST TRIMESTER ANEUPLOIDY SCREENING IN A U.S. POPULATION CAN REPLICATE DATA FROM CLINICAL TRIALS
PERNI et al AJOG 2006
• 4883 patients, Cornell University, median maternal age 33 years old
• 22 cases of trisomy 21• Detection rate 91%, false positive rate 5% for
trisomy 21• All cases of trisomy 18 detected• Used Free Beta-hCG, NTD labs
Is it a Myth or a FactBy Larry Platt, OB/GYN NTOC Member Prof. Ob-Gyn, Geffen School of Medicine at UCLA, Director, Center for Fetal Medicine and Women's Ultrasound
MYTH: ACOG Practice bulletin mandates integrated testing as the method of choice for prenatal diagnosis.
FACT: The ACOG PB provides a variety of ways to achieve the most desirable outcome including combined First Trimester risk assessment with NT and biochemistry alone, second trimester alone or a combination of testing schemes etc. Quality monitoring of NT performance is emphasized as essential.
NASAL BONE
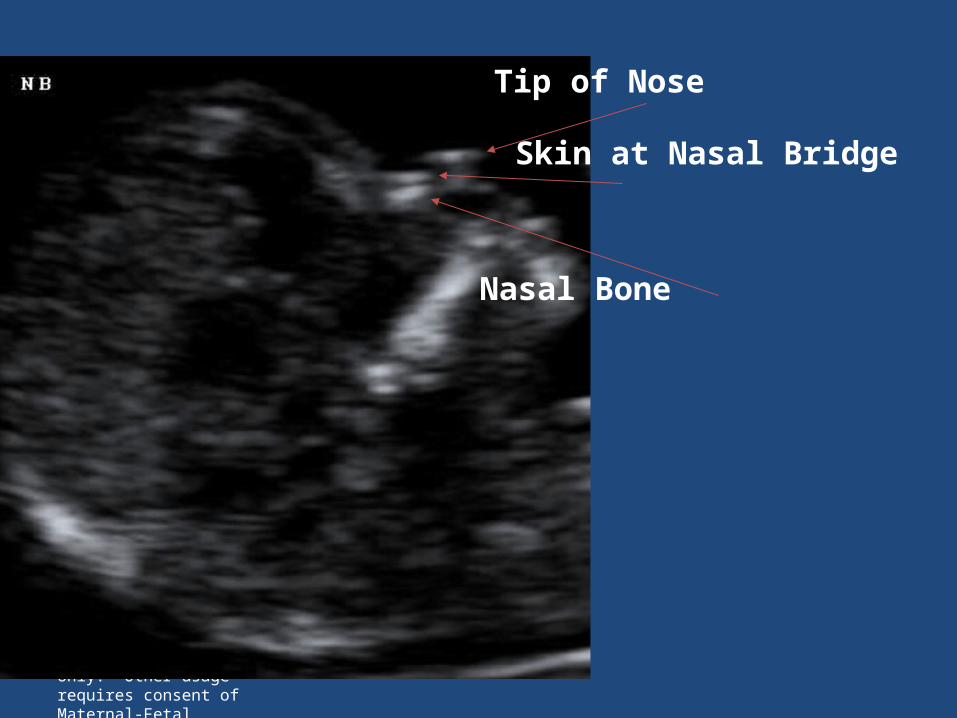
© 2007 Nuchal Translucency Quality Review. Reproduction permitted for personal educational use only. Other usage requires consent of Maternal-Fetal Medicine Foundation. Content may not be modified in any way without permission.
Tip of Nose
Skin at Nasal Bridge
Nasal Bone

© 2007 Nuchal Translucency Quality Review. Reproduction permitted for personal educational use only. Other usage requires consent of Maternal-Fetal Medicine Foundation. Content may not be modified in any way without permission.
Tip of Nose
4th
AS
3rd

Cicero S, Avgidou K, Rembouskos G, Kagan KO, Nicolaides KH. Nasal bone in first-trimester screening
for trisomy 21. Am J Obstet Gynecol 2006
• Study of a high-risk population with a median maternal age of 35 years assessed by nuchal translucency, nasal bone, and biochemistry
• Estimated that 93.6% of Down syndrome cases would be detected at a false-positive rate of 5%.
• For a false-positive rate of 2.5%, the detection rate would be 90.0%
• The experience of highly specialized and high-risk centers and are not generalizable to less experienced centers.
INSTANT SCREENING

00 22 44 66 88 1010 1414
LMPLMP PregnancyTest
PregnancyTest
1212 1616
free-Beta / PAPP-Afree-Beta / PAPP-A
DiagnosisDiagnosis
ConceptionConception
Weeks
Instant Risk AssessmentInstant Risk Assessment
CVSCVS
NTNT

SUMMARY• Most models show an advantage in integrated or
sequential screening programs as compared to combined NT screening alone
• This has not been shown in large clinical trials where decisions about accepting invasive testing has been included.
• When those decisions are included, the largest trial available showed a 90% detection rate using combined NT alone
• Combined NT using free beta hCG is an appropriate screen for Down Syndrome