ihe / rsna image sharing project - ihe colombia workshop (12/2014) module 5c
TRANSCRIPT

IMAGING INFORMATICS: IHE RADIOLOGY ORDER ENTRY
CLINICAL DECISION SUPPORT
Based on the RSNA 2014 presentation, December 2014
Written by: David S. Mendelson, M.D.
Professor of Radiology
Senior Associate- Clinical Informatics
The Mount Sinai Medical Center
Co-chair IHE International Board
Adapted and presented for the IHE Colombia IHE
Workshop by:
Elliot B. Sloane, PhD, CCE, FHIMSS
Co-chair IHE International Board
President, Center for Healthcare Information
Research and Policy (CHIRP)
Radiology Orders
The right order The right reason for
exam and background information
Automated scheduling
Pre-defined Procedure steps at the modality
Uniformity of exam
Radiology Order Entry Clinical Decision Support
Standard Exam dictionary RADLEX Playbook
Modality Worklist Standard Protocols
mapped to a modality RADLEX Playbook Series pre-defined
What do we need? Enablers

Radiology Orders
Appropriateness Cost Control

Radiology Order Entry Clinical Decision Support Ensure the correct order based upon
standardized rule sets Utilization control
Inappropriate Utilization Redundant Imaging
Replacement for Radiology Benefit Managers
Education for the clinician Compare their ordering metrics to their
peers
Inappropriate Utilization
Defensive Medicine – Liability concern Tort Reform
Patient Demand Financial Incentives
Self referral Pressures to minimize overall cost of an episode of
care Physician lack of knowledge Duplicate exams
Results not easily available Patient lack of understanding of exams already
performed Fragmented care – no coordination of care
Up to 20% of imaging exams may be inappropriate


Iglehart JK. Health Insurers and Medical-Imaging Policy — A Work in Progress. N Engl J Med 2009;360:1030-1037
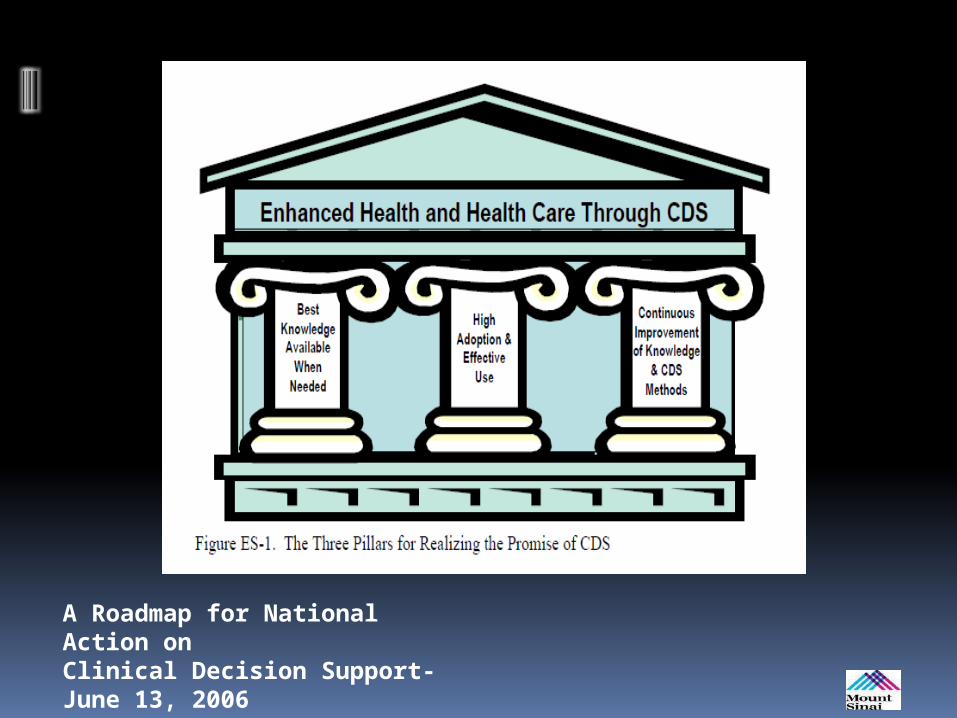
A Roadmap for National Action onClinical Decision Support-June 13, 2006

Decision Support
Collegial advice Text references Web sites Computer systems
Passive Active
Alerts Reminders Corollary Orders Guidelines

Clinical Decision Support Systems (CDSS or CDS)
Incorporates Patient data (EHR) Rules Engine Medical Knowledge
Produces a patient specific recommendation
Clinical Decision Support - CDS CDS is a technology that may help to
significantly improve the appropriateness of orders through dissemination of Comparative Effectiveness Research (CER) to clinicians at the point of order-entry.

American College of Radiology Appropriateness Criteria (ACR AC) A formal mechanism to determine the
utility of imaging exams to diagnose disease
Evaluate existing evidence comparing candidate modalitites
Synthesize a utility index Rand/UCLA Appropriateness method
Evidence Consensus
Limitation – evidence is generally not on double blinded randomized studies
Radiology Benefit Managers RBM services to obtain pre-clearance
for high cost procedures Effectively Diminish Utilization
Issues Burden of a frustrating time consuming
solution with a significant cost in manpower
Implementation Is this done rationally?
CDS- some data
Pilot study in Minnesota with members of Institute for Clinical Systems Improvement (ICSI)
Imaging growth was curbed while simultaneously improving the rate of indicated examinations (ambulatory environment
Added benefit was that while RBM pre-certification required an average of 10 minutes of interaction, the CDSS only required 10 seconds Efficient workflow and scheduling, with a
diminished need to reschedule patients


Decision Support
Clinician Radiologist
ACR – National Decision Support Clearinghouse

EMRCPOE
Radiology CDS
Radiology RIS
High Appropriateness
score

EMRCPOE
Radiology CDS
Radiology RIS
High Appropriateness
score
Low Appropriateness Score- Try
Again!

Radiology Order Entry Clinical Decision Support
Imaging 3.0: A Framework for Radiologists’ Future

Utilization Management 3.0
• Drive towards appropriate utilization of imaging– Ensure value of proper
imaging (and the Radiologists role) is defined as valuable
– Right test, right time, properly performed and interpreted
– Create a platform and tools to promote the value of imaging
Utilization Management and Value based Radiology
Bob Cooke

23
Decision Support System
• The ACR Appropriateness Criteria ® must become a “digitally consumable” DSS to be used as part of a Clinical Decision Support System
• The ACR has formed a commercial entity so that the AC® can be used to integrate this “knowledge base” into CDS systems
24
National Decision Support Company
• The ACR manages the content of the knowledge base. NDSC is the exclusive agent of the ACR for delivery of the content into the market
• NDSC is the commercial entity to manage the delivery and integration of this knowledge base into CDS systems

ACR’s Role
• Curates the clinical content based on market feedback obtained by NDSC, development of new imaging procedures, and member feedback.
Aggregate user experience
Content Updates Market Feedback
New Releases

CDS- Challenges
Issue Definition Approach to Resolution
Alert Fatigue users begins to ignore (white noise) or override alerts due to a high frequency of alerts
Content domains and triggers for the selected Imaging CDSS
Overriding CDSS interventions that appear all too frequently,
Assess local practice and correct if necessary; re-assess AC
Delivery to the wrong population
Delivery of CDS to the correct user population also impacts adherence and success
Selectively turn off CDSS for certain category of clinicians.
Appropriateness Criteria is incorrect
Accuracy of CDSS is a critical factor in CDSS success
Review and correct in system. Feedback to clinical staff
Game the system Enter inaccurate information merely to obtain approval for desired examination
Look for disproportionate utilization even if seemingly justified. Check if rules never trigger. Counsel offenders (?Penalize- last resort)
Close the loop
Measure each clinicians performance Communication Compare anonymously to peers
Mount Sinai Experience
Data Collection Phase System is in place with discrete orders No feedback Determine Baseline performance
Presentation state is important Change management Utility scores of 1-3
Consistently 8% Educate
Plan – turn on feedback