iii – workshop resources - cwchealthcarecoalitions.org · iii – workshop resources 1. project...
TRANSCRIPT

Minnesota Healthcare System Business Continuity Planning Workshop
III – Workshop Resources 1. Project Map and Timeline Template
2. Business Continuity Action Plan
3. EM BCP Framework Master
4. CEO Letter Template
5. EM BCP Policy Template
6. EM BCP SBAR Template
7. Healthcare Core Services and Operations
8. Governance BCP Structure PowerPoint Slide
9. Steps for Leadership and Physician Engagement
10. Sample email to department head requesting function representative
11. Sample email to function representative assigned to be interviewed
12. Governance - Committees
13. BCP Demo – Questionnaire
14. 10 tips for interviews
15. Questionnaire Scores Analytics Demo
16. BCP Demo 2
17. EOP – BCP Plan Content

Nov - Dec
Jan
Nov
Oct
Recommendations to leadersAdditional department surveys (Only 2-3 done in 1st round)Planning and Management (ongoing)
- 96 hour plan- Business Impact Analysis (BIA)- Hazmat Vulnerability Analysis (HVA)Jan - Dec
Jan - Feb
Jan - Dec
Jul - Dec
Your Healthcare Facility
Regional Management Team (RMT) endorsementKick-off meeting with Pilot SiteAgenda: Overview, Work Plan, Governance, Identify Critical Departments, Prioritize Departments, Schedules, QuestionsPilot Site Survey (Essential services)
Departmental BCP template, Integration and Recovery Strategies, Testing & Exercising, Monitoring & Evaluation
Train with COOP Project Team members (individual facilities determine members)
Begin additional healthcare facility kick-off meetings and essential services surveys. Prioritize and select 2-3 departments.
Regional touch point meetingReview pilot sites and determine next steps
Review results with regional EMC, COOP workgroup, governance, etc.
Plan DevelopmentReport out to EMC/RMT, COOP workgroup, governance, etc.
2014
2016-2017
2015

Business Continuity Development Action Plan
©2014 Wakefield Brunswick, Inc. 1 | P a g e
Project Initiation and Governance 1. Scope the effort • Determine who owns responsibility for
developing and managing plans • Determine current level of executive buy-
in/support for business continuity • Determine level of continuity awareness within
the organization • Identify total number of operational
departments that need to be developed
2. Plan the effort • Establish plan development goals and time frames
• Schedule and conduct executive briefing(s) to get buy-in/support to proceed
• Identify the operational departments and unit representatives to be assigned to participate in plan development efforts
3. Establish your program policy
• Download the business continuity program policy template
• Tailor the policy template to your organization
4. Identify your program sponsor
• Coordinate with your supervisor to identify a leader to serve as your executive sponsor
• Work with your executive sponsor and supervisor to form your committees
5. Educate and engage leadership
• Download the CEO letter and SBAR • Tailor the materials to your organization. • Send executive letter with SBAR • Conduct an executive briefing / presentation
and reinforce key principles in SBAR • Present the policy, organization chart and
leadership briefing to your steering committee • Gain approval from steering committee on
policy and organizational chart

Business Continuity Development Action Plan
©2014 Wakefield Brunswick, Inc. 2 | P a g e
Data Gathering 6. Develop interview
questions • Create questions - include impact categories
with definitions • Create pre-populated tables for drop down
menus
7. Setup interviews • Review/verify operational departments identified in plan development goals
• Communicate with departmental management to identify representative to participate in interviews
• Communicate with departmental representatives to schedule interviews
8. Conduct interviews • Ask questions to identify: o Essential functions and services o IT applications and services o Vital records, equipment and supplies o Interdependencies o Impact of service interruptions
9. Analyze the data • Review all the data for completeness and integrity
• Add impact scores by function and application - rank according to priority
10. Report on findings • Provide a summary of findings to include rankings of functions, applications and impact ratings
• Identify any gaps in capabilities and requirements for recovery
Strategies and Action Plans 11. Review data • Review BIA and Hazard Vulnerability Analysis
(HVA) findings to understand what risks pose the greatest threat to essential functions
• Use data to make decisions to reduce risks that will have the greatest adverse impacts
12. Examine current capabilities
• Examine 96-hour capabilities finalize strategies for ensuring continuity of essential services.
• Meet with facilities, supply chain and IT to understand capabilities and integration points.

Business Continuity Development Action Plan
©2014 Wakefield Brunswick, Inc. 3 | P a g e
13. Evaluate strategies • Identify strategies for continuity of operations o Alternate locations o Mobile capabilities
14. Establish recovery strategies
• Develop cost estimates for strategies • Present strategies/costs to governance group
or steering committee for approval. • Establish agreements with vendors and
suppliers required to implement recovery strategies
15. Develop recovery actions • Use information from interviews to identify high level actions for recovery of functions and services
16. Create departmental plan • Use Departmental BCP Template to document o Essential functions o Essential applications o Vital records o Vital equipment and supplies
• Document strategies approved for recovery of functions and services
• Document recovery actions
Integration 17. Develop integrated plan
framework • Conduct review meetings with all management
and staff involved in your facility’s emergency management program to ensure plan integration and alignment with: o IT Disaster Recovery o EOPs o HICS
Plan Testing and Maintenance 18. Develop plan testing
program • Identify types of tests to be conducted • Establish annual testing goals and objectives • Establish annual testing schedule
19. Establish plan maintenance program
• Establish plan maintenance objectives • Develop plan review and update schedules • Monitor departments adherence to plan review
and update schedules

Business Continuity Development Action Plan
©2014 Wakefield Brunswick, Inc. 4 | P a g e
20. Establish monitoring and evaluation process
• Track and monitor continuity metrics (e.g. # BIA’s completed, # plans, completed).
• Identify gaps that exist • Assign gaps resolution tasks and monitor
resolution progress • Conduct periodic gaps and metrics review with
governance group or steering committee

Healthcare Emergency Management & Business Continuity Framework Continuity l Response l Recovery
An integrated, multi-disciplinary program focused on supporting and strengthening the organization’s core mission
Emergency Operations
Incident Specific Plans
Safety/Fire
Safety Procedures
Fire Procedures
Utility Interruptions
Emergency Codes
Human, Natural, Technological Hazard Response
Patient Clinical & Support Activities
HICS, Crisis Comm, Triage, Surge, Public Health, Evacuation
Management of Staff, Resources and Assets
Organizational/Departmental
Operations for Clinical, Business & Research
Downtime Procedures
Business Continuity Branch Director (Service Continuity, Records Preservation and Business Relocation Units)
Network Systems and Applications Telecom
Vital Records, Equipment
and Supplies
Essential Services
Governance & Crisis Management
A resource provided by The Minnesota Department of Health – Office of Emergency
Preparedness (in partnership with Wakefield
Brunswick)
Emergency Operations Planning (EOP)
Plans, procedures and resources for all four emergency phases (mitigation, preparedness, response, and recovery), for all types of emergencies and disasters.
Business Continuity Planning
(BCP) Plans, procedures and resources to maintain and/or recover essential services and functions impacted by an event causing an interruption of normal operations.
Disaster Recovery Planning (DRP)
Plans, procedures and resources to maintain and/or recovery the information technology systems, network, and telecommunications services.

Dear <insert name>, The Office of the Assistant Secretary for Preparedness and Response provides leadership and funding to our facilities through grants and cooperative agreements to support healthcare preparedness. We have assessed our planning efforts to date against the national funding priorities and identified business continuity, also called continuity of operations (COOP), as a key initiative throughout our current 5-year grant cycle. To provide further background I am enclosing a SBAR Report that summarizes healthcare business continuity. On <insert date>, you will receive an e-mail that provides further information and links for our organization. Please share these materials with our leadership team <insert name> to ensure our organization benefits from upcoming resources and training. I can be reached at ___________ with any requests or questions you may have about this initiative. Kind regards, <name>

<insert header/logo & policy template format>
POLICY #:
Emergency Management (EM) and Business Continuity Program (BCP) PURPOSE Company XYZ is a patient-centered health system concentrating on the provision and coordination of health services. The purpose of the program is to provide the guidance and framework to ensure continuation of essential operations at XYZ in the event of a disruption to normal operations or emergency event. A disruption to normal operations is defined as an event resulting in the unavailability of raw materials, information technologies, skilled labor, facilities or other resources that threaten the organization’s capacity to continue operations or impacting one or more of the following:
• Colleagues, property, facilities, assets, critical infrastructure and/or supply chain • Continuity of operations and/or or delivery of services, including the cascading effects of local,
regional, national or international events • Reputation of, or confidence in the entity • Economic and financial condition • Regulatory and contractual obligations
An emergency event is any event that may pose an immediate danger to the safety and well being of patients, staff or visitors; or a natural, technological, man-made or public health emergency affecting the community we serve. The program is a comprehensive approach to responding to emergencies and to ensure the continuity of essential services during an event that has an adverse impact on our community, hospital operations or facilities. GUIDING PRINCIPLES Consistent with this strategy, the Board of Trustees, the medical staff and the health system administration have established and provided support for an Emergency Management (EM) and Business Continuity Program (BCP) that will do the following: 1. Provide a framework for the management of internal or external emergencies, whether actual events
or exercises, encompassing the six critical areas of emergency management. These are: Communication, Resources and Assets, Safety and Security, Staff Responsibilities, Utilities Management and Patient Clinical and Support Activities.

2. Evaluate potential emergency scenarios using an “all hazards” concept with consideration for mitigation, preparedness, response and recovery.
3. Provide training to health system staff that identifies their roles in the Emergency Operations and Business Continuity Plan.
4. Work cooperatively with the City of XYZ, County, State and Emergency Medical Services Region to ensure integration of community emergency management with the health system and with the state tier level rules.
5. Provide a mechanism for program documentation and evaluation. Results shall be used to identify opportunities for improvement in the planning process, the plans, staff training and/or the resources available during operational interruptions or emergencies.
6. Record, analyze and act on opportunities for improvement observed during implementation of the plan. The findings shall be forwarded to the Environment of Care (EOC) committee for inclusion in an action plan for the ongoing development of the program.
7. Collect appropriate performance data during implementation of the plan and during routine safety evaluations. The data shall be used to improve performance, mitigation, preparedness, response, recovery and staff training.
8. Conduct an annual evaluation of the objectives, scope, performance and effectiveness of the program and report the findings of that evaluation to the EM/BCP Committee and leadership.
ASSUMPTIONS 1. Effective assessment and planning reduce the impact of emergencies on the quality of patient care. 2. Many types of emergencies are identified from past organizational or community experiences. The
experiences provide a baseline of likely potential threats and an opportunity to learn from actual events.
3. Hospital facilities, clinic buildings, operational space, personnel, supplies, communications and other resources are considered part of the planning efforts.
4. On duty staff may be unable to maintain essential services. Emergency conditions may require modification of normal patient care routines. These conditions may require the health system to discontinue services, divert regional patient transfers, initiate facility evacuation, discharge patients or initiate surge capacity programs.
5. Periodic exercises are an essential element in maintaining health system staff awareness of emergency procedures and for evaluating the effectiveness of plans. Scheduled exercises and/or actual implementation of the Emergency Operations Plan (EOP) provide opportunities to observe staff performance and to identify potential areas of improvement.
6. The health system’s return to normal operations after an emergency occurs may take days, weeks or months depending on the type of emergency. Business and clinical BCP recovery plans are essential components of the EOP.
7. Consideration is given to the fact that the lives of staff, patients and/or visitors may be lost due to associated injury or disease.
8. Remaining workers may be psychologically affected by disaster, disease, family concerns, economic loss or fear.
9. Staff may be reduced by the need for some workers to attend to family illness or to children remaining at home or due to school closures.
10. An emergency condition may require the transfer of essential functions to other personnel or possibly relocation site(s).
11. Some of the information and communications systems supporting operations during normal non-emergency periods may not be available.
DEFINITIONS

Company XYZ: All facilities associated with Company XYZ including XYZ Hospital, XYZ Specialty Clinic, XYZ Family Clinic and the XYZ Outreach Clinic. Continuity of Operations (COO): Internal organization efforts to ensure that a viable capability exists to continue essential functions through plans and procedures that delineate essential functions; specify succession to office and the emergency delegation of authority; provide for the safekeeping of vital records and databases; identify alternate operating facilities; provide for interoperable communications; develop alternative scheduling to offset staff losses; provide staff support during emergencies and validate the capability through tests, training and exercises. Business Continuity Plan/Continuity of Operations Plan (BCP/COOP): Plan that provides for the continuity of essential functions of XYZ in the event an emergency prevents occupancy of its primary buildings, or an event that limits operations through extensive staff losses or other resource limitations. Devolution: The transfer of essential functions, as the result of a COO event, to another organizational element (i.e., person, office or organization, etc.) geographically located outside of the threat area. Alternate Care Site (ACS): The physical location of treatment areas to which XYZ moves all or part of its operations to continue essential functions in the event the main facility is threatened or incapacitated. Essential Functions: Essential functions are those functions that enable XYZ to provide vital services, maintain safe and quality operations, maintain the safety of employees and associates and sustain an industrial/economic base during an emergency. Administrator On Call (AOC): The operational head of XYZ during off duty hours. The AOC serves as the CEO/NHA designee when the CEO/NHA is unavailable. If the AOC is unable to respond to the facility, the AOC’s responsibility may be delegated to any administrative officer on the AOC roster or as defined in section 3-7 (Orders of Succession and Delegation of Authority) in this document. Centers for Disease Control (CDC): Federal level disease reporting and information agency located in Atlanta, Georgia. World Health Organization (WHO): Reporting agency for worldwide disease and pandemic outbreak information and tracking. Office of Emergency Management (OEM): XYZ County Office of Emergency Management that is responsible for coordinating emergency response and recovery activities within XYZ County during an emergency or disaster event. This office coordinates local response as well as requests assistance from the XYZ State OEM. Hospital Command Center (HCC): HCC will be the place from which all activities will be directed during an interruption or emergency event. At minimum, the following staff will be located at the HCC:
a) The Incident Commander b) The Safety Officer c) Public Information Officer d) Operations, Planning, Logistics and Finance Section Chiefs
The Plan: The Emergency Operations and Business Continuity Plan which will be used in the event of a disaster (or threat of a disaster). The Plan consists of emergency plans addressing command and control, safety and security, crisis communications, operations, public health emergencies, evacuation, hazmat response, logistics and finance planning.

SCOPE Procedures, activities of or responses to potential events specific only to the sites identified above are detailed Facility and/or Unit-specific Plans. Each of these plans is an extension of the XYZ Emergency Operations and Business Continuity Plan. The Emergency and Business Continuity Plan is managed by the Emergency Operations Manager (EM)/Business Continuity Planner (BCP). The EOP/BCP is reviewed and approved by the EM/BCP Committee (see Organization and Responsibility). The EOP/BCP will be reviewed, tested, and updated in accordance to the Performance Management standards, the Hazard Vulnerability and Business Impact Analysis outcomes, and as necessary to mitigate risks or meet regulatory changes. THE EMERGENCY OPERATIONS PLAN AND BUSINESS CONTINUITY PLAN EOP/BCP consists of emergency plans addressing the following:
• Command and Control • Safety and Security • Crisis Communications • Operations – Emergency Clinical Operations and BCP • Public Health Emergencies • Evacuation – Full Building and Departmental Procedures • Hazmat Response • Logistics • HICS Planning and Finance Sections
Operations Plan The Operations Section will be responsible for managing the tactical objectives outlined by the Incident Commander. This section is typically the largest in terms of resources to marshal and coordinate. To maintain a manageable span of control and streamline the organizational management, branches, divisions and units are implemented as needed. The degree to which command positions are activated depends on the situational needs and the availability of qualified command officers. The Operations Section Chief is responsible for overseeing the operations including:
Evacuation/Staging Procedures
HAZMAT Branch
Business Continuity Branch
o Vital Records
o Alternative Work Site Procedures
o Departmental Business Continuity Plans
Infrastructure Branch
o Management of loss of Utilities

Medical Care Branch
o Management of Patients/Surge
o Alternate Care Site Procedures
o Public Health Emergencies and Biohazards
o Inpatient/Outpatient Unit
o Casualty Care Unit
o Mental Health Unit
o Clinical Support Services Unit
o Patient Registration Unit
o Morgue/Fatality Management
The Medical Care Branch is made up of the clinical operations of the hospital. The Operations Plan details the overarching procedures for response and Business Continuity including alternate site relocation and operations for the overarching response. However, each unit has an individual plan detailing their department’s specific Emergency and Business Continuity procedures. These plans are found online under the Operations, Medical Branch folder and on site in the unit’s Orange Binders. In addition, each unit has a Red Emergency Response Manual highlighting key actions in the event of various incidents impacting the hospital which reflect the more detailed information in the EOP/BCP. However, all staff:
o Will return to their department unless involved in the immediate care of a patient o Are deemed essential and are not to leave without authorization from their
manager or designee. This includes shift changes.
o Are not to report to or call the ED (other than ED staff) until requested.
o Are to ensure communication about the event is provided under the direction of
the department leader.
Logistics Section The Logistics Section will be responsible for managing the infrastructure, service and support functions to support the tactical objectives outlined by the Incident Commander. To maintain a manageable span of control and streamline the organizational management, branches, divisions, and units are implemented as needed. The degree to which command positions are activated depends on the situational needs and the availability of qualified command officers. The Logistics Section Chief is responsible for overseeing the operations including:
• Service Branch
o Communications Unit
o IT Unit/Disaster Recovery
• Support Branch
o Family Care Unit
o Supply Unit and Emergency Acquisition of Resources
o Transportation Unit

o Labor Pool & Credentialing Unit
RECOVERY Based on damage assessments and evaluation of operational needs, incident recovery plans will be developed and implemented. Each individual department and/or unit shall be responsible for initiating this activity. The Incident Command System will remain operational during this period but may gradually de-escalate as warranted. Meetings shall be scheduled as deemed appropriate by the Incident Commander. Criteria that shall be considered as part of the recovery process include, but are not limited to:
• Facility repair/restoration • Utility system restoration • Equipment replacement • Supply inventory restoration • Patient care support • Staff support • Financial reimbursement and recovery • Traumatized staff
ORGANIZATION AND RESPONSIBILITY Environment of Care (EOC) Committee: Led by the EOC Chairman, all EOC Chapters are represented and report progress in their respective areas to ensure the Joint Commission Elements of Performance are met. The EOC Committee receives regular reports of the activities of the Emergency Management (EM) and Business Continuity Program (BCP) and communicates recommendations or concerns to the Emergency Manager/Business Continuity Planner. The Emergency Manager/Business Continuity Planner submits quarterly reports on relevant issues to the (EOC) Committee. The Joint Commission (TJC) steering committee receives periodic reports of performance improvement and other activities of the EOC Committee. The EOC Chairman presents summary report and recommendations are presented to the Quality Patient EOC committee. Emergency Management and Business Continuity Committee: Led by the Committee Chairman, with support from the EM/BCP. The Executive Vice-President and Chief Operating Officer (or designee) has administrative oversight for the Emergency and Business Continuity Plan. The Chief Operating Officer (or designee) in collaboration with the EOC Chairman, BCP Committee Chairman and EM is responsible for the maintenance of the Emergency and Business Continuity Plan. The development and maintenance is conducted in coordination with the EM/BCP Committee. Leadership: The Board of Directors and Health System Administration represent leadership.
Leadership provides an annual operating budget for the EM/BCP program. The authority to implement the plan is the ultimate responsibility of the CEO/COO or designated administrator on-call per the Command and Control Section of the EOP. Department Management: Each System Unit/ Area Manager shall be responsible for:
• Maintaining the applicable unit-specific plan • Orientating new or temporary personnel to task-specific responsibilities for Emergency
Management Program Plan response • Annual department staff training/education
General Staff: Individual system staff members, ancillary staff members, physician members and temporary staff members are responsible for learning and following job specific procedures for Emergency and Business Continuity planning, response, recovery and resumption. PROGRAM ELEMENTS OF PERFORMANCE HAZARD VULNERABILITY ANALYSIS A hazard vulnerability analysis of the operations and environment of shall be used and maintained by the Safety Officer and the EM/BCP. The hazard vulnerability analysis shall be used to determine what conditions or events may be likely to have a significant adverse impact on the health and safety of patients, staff and visitors. In addition, the analysis shall be used to determine the potential impact of the events on the ability of health system to conduct normal patient care and activities. The Safety Officer and the EM/BCP use an “all hazards” approach to planning for emergencies. Potential emergencies (natural or man-made) shall be evaluated annually (or as needed) to determine the probability of occurrence as well as the potential for damage or risk to the organization. The hazard vulnerability analysis shall use a quantitative scoring process to assist in setting mitigation and preparedness priorities. It shall be implemented by the Safety Officer in conjunction with the EM/BCP and are reviewed annually or as situations develop. COMMUNITY INTEGRATION XYZ is part of the XYZ County medical care community. XYZ cooperates with the County Disaster Committee and Public Health Department in an effort to define the role each provider shall fulfill during an emergency and/or disaster response. XYZ shall be represented on City, County, Regional and State Disaster Committees to coordinate medical response to emergencies. XYZ shall participate in at least one community-wide emergency preparedness exercise per year. The EM/BCP should attempt to meet at least once per year with the city’s police and fire departments to compare emergency management plans to insure compatibility.
Remote sites of XYZ are not, as a rule, included in activation of the county, city and regional emergency management plans. If additional staff is needed, the Incident Command Center at XYZ shall contact the appropriate administrative personnel from the remote sites and request support. For emergencies that occur at remote sites, 911 and the health system security department shall be called. In weather emergencies, remote sites shall cancel appointments and close as needed. COOPERATIVE PLANNING AMONG HOSPITALS

XYZ Hospital is a participating member of the integrated emergency management committee comprised of city/county emergency management representatives, along with other hospitals in the city. Information is shared on a monthly basis for cooperative emergency management planning. Essential information such as names and roles of individuals in their command structure and command telephone numbers is shared with this committee. Resources and assets are shared in an emergency response situation with all hospitals in the region and the State Hospital. XYZ Hospital is designated as the lead hospital in this region and is the state designated disaster XYZ hospital as identified in the state medical disaster plan. PLAN DEVELOPMENT The Emergency Operations and Business Continuity Plan is developed by a multi-disciplinary disaster committee that consists of management from each of following disciplines/departments: physicians, EMS, disaster, facilities, safety, nursing, administration, security, communications, VNA, surgery, critical care, XYZ Health Physicians, emergency department, trauma, central supply, human resources and epidemiology. The membership may expand to include ad-hoc representation as needed. The Board of Directors, the medical staff and the health system administration have established and provided support for an Emergency Operations Program. Operational Concept Objective The objective of this plan is to ensure the execution of XYZ’s essential functions, during any crisis, that are critical to the wellbeing of our patients, residents, employees and communities. The objective is also to provide for the safety of the patients, residents and employees during any emergency or crisis when a sudden or ongoing and severe reduction in staff/human resources and/or the physical structures of XYZ are unsafe to occupy. Specific objectives of this plan include:
• Ensuring the continuous performance of essential functions during an emergency to the greatest extent possible.
• Communication with all staff of XYZ. • Communication with key community government agencies. • Communication with key first responding agencies. • Protecting the safety and productivity of staff, patients, residents and visitors. • Reducing or mitigating disruptions to operations. • Addressing behavioral health issues that may affect the organization. • Pre-planning for potentially critical losses of staff through scheduling, identification of alternate
resources and temporary business reduction efforts. • Reducing loss of life and minimizing damage and losses. • Achieving a timely and orderly recovery from an emergency and resumption of full service to
customers. Concept of Execution Emergencies, or threatened emergencies, may adversely affect the ability of XYZ to continue to carry out essential functions and operations. Infectious diseases, terrorist agents and natural disasters may cause:
• Severe damage to the physical structures of XYZ • Loss of utilities and communications • Severe staffing shortages • Full or partial evacuation and relocation of patients, residents and essential functions of XYZ
Any event that would compromise the safety and services provided to patients, residents and our communities would warrant execution of the Plan. This may be due to manmade or natural disasters, infectious disease outbreak, civil unrest or riots or any number of events both planned for and unforeseen. These events may also lead to a partial or full evacuation of patients and residents. They may also include a partial or full closure of the physical structures of XYZ. Relocation of essential functions to ACS may be indicated and should be coordinated with the Huerfano County OEM. While some emergency events, such as disease outbreaks or severe winter weather, will in most cases come with some advanced warning, other events such as tornado, utility disruption, fire, terrorist attack, etc. may happen with little or no notice. Advance preparation for these events is the key to a successful implementation of the Plan. XYZ may direct full or partial activation of the Plan. Activation of the Plan may initiate the transfer of essential functions and the deployment of pre-identified personnel and equipment/supplies to an ACS. Activation of the plan may also involve significant alteration of work plans and assignments of staff to critical work areas, use of contractors, extension of overtime for well workers and similar alternatives in order to offset staff reduction. The Plan may be activated if adequate staff is not available for work in order to keep critical business interests operational. It should be kept in mind that the Plan is NOT an evacuation plan, rather it is a deliberate and planned deployment of pre-identified and trained personnel and/or the transfer of essential functions to an ACS. Should activation of the plan be necessary, the Incident Commander will disseminate notification of the Plan activation with appropriate instructions by any and all available means including radios, pagers, telephone, runners or e-mail. Pre-identified personnel should follow the instructions given in accordance with the instructions contained in the Plan. If the event results in senior administrative staff becoming unavailable to respond to the HICC, a major consideration becomes reconstitution of key leadership positions in accordance with the Order of Succession. Following the event, the primary effort will be the regeneration of XYZ’s Emergency Department with adequate personnel and equipment to restore complete Emergency Department business operations. Reconstitution activities are oriented towards the determination of physical structure safety, identification of any ACS that may be needed to perform essential functions and alternate human resources to offset staff losses for limited or extended periods of time. When sufficient functions have been restored at XYZ and all other occupied space or reconstituted facility(s), the Incident Commander or his/her designated successor can order the termination of contingent operations. PHASES/METHODOLOGIES The Emergency and Business Continuity Plan considers the four phases of emergency management: MITIGATION: Activities designed to reduce the impact or severity of potential emergencies. They include but are not limited to:
• Compliance with the Life Safety Code to reduce the risk of fire.

• Appropriately sized emergency power systems where required. • Inspecting, testing and maintenance of utilities systems and medical equipment. • Consideration of potential emergency issues in planning for construction and/or
renovation. PREPAREDNESS: These activities identify resources needed in the event of an emergency. Business Continuity plans are in place to initiate resource searches through vendors after the first or second operational period greater than 16 hours. Consideration of the asset and resource inventory needed on site or that would be needed during an emergency. The 96 hour grid illustrating this is evaluated annually. (Appendix A) Considerations include, but are not limited to:
• Staff call lists and call back systems • Minimum 36 hours fuel supply for the emergency generator • Minimum 72 hours food and water on hand • Preparations for snow removal • Preparations for support of staff and their families • Preparations for management of the media • Identification of alternate care sites • Identification of alternate sources of essential utilities • Identification of back-up communications systems • Maintenance of a decontamination facility • Identification of additional supplies for nuclear, Bioterrorism and chemical response. • Preparations for needs with regards to pharmaceutical, surgical and medical resources
RESPONSE: These activities are related to management of the actual emergency. They include, but are not limited to:
• Incident command system • Treatment of victims • Community coordination • Assignment of personnel • Personnel identification • Management of patient activities • Emergency supply carts • Food service • Evacuation • Decontamination • Business Continuity
RECOVERY: These activities are related to the post response and to reestablish normal business operations following an emergency situation. Based on damage assessments and evaluation of operational needs, incident recovery plans will be developed and implemented. Each individual department and/or unit shall be responsible for initiating this activity. The Incident Command System will remain operational during this period but may gradually de-escalate as warranted. Meetings shall be scheduled as deemed appropriate by the Incident Commander. Criteria that shall be considered as part of the recovery process include, but are not limited to:
• Facility repair/restoration • Utility system restoration • Equipment replacement

• Supply inventory restoration • Patient care support • Staff support • Financial issues • Traumatized staff
Devolution of Essential Functions The devolution of essential functions identifies how the organization will identify and conduct essential operations during periods of severe staff reduction. The plan for devolution of essential functions includes the identification of mission critical systems; capabilities to perform essential functions given specific losses of staff and expertise; reliable logistical support, services and infrastructure alternatives; communications between staff, and related computer/software issues. Each department has documented this information in their plans. Order of Succession and Delegation of Authority The Chief Executive Officer of Hospital (CEO) and Nursing Home Administrator (NHA) are equal partners in the operations of XYZ. The following is an order of succession for the CEO or NHA if he/she is no longer able to carry out their functions:
1) Hospital CEO 2) Nursing Home Administrator (NHA) 3) Director of Human Resources 4) Chief Financial Officer 5) Director of Support Services and Safety 6) Hospital Chief Nursing Officer 7) Nursing Home Director of Nursing
Delegation of Authority creates continuity in the flow of authority from the CEO/NHA/AOC cascading to successors. The persons named in the order of succession will have full, unlimited authority to operate XYZ to the fullest extent possible until such person is relieved by the next highest ranking officer. Delegation to successors other than CEO/NHA, extending more than seven days, will need approval by the XYZ County Hospital District Board of Directors. A delegation of authority includes:
• Name and title of the successor being delegated the authority • Date and event that trigger delegation (i.e., COOP implementation) • Authorities delegated, together with any limitations on or exceptions to their use • Date of termination or the point at which delegation is automatically revoked (i.e. 7 days) • Date authority extended if applicable • Name, title and signature authorizing extension • Name and title of person assuming authority upon termination of delegation • Date of authority assumption
The form to be completed is contained in the Plan. DRILLS AND EXERCISES Exercises to test our response to emergency situations are conducted regularly. A response to an actual emergency may be substituted for a planned exercise. All facilities designated as healthcare occupancies

receive two exercises per year. All other patient care areas in facilities designated as business occupancies receive one exercise per year. The hospital conducts at least one exercise per year that includes an influx of volunteers or simulated patients. The hospital shall conduct at least one exercise per year that is escalated to evaluate how effectively the organization performs when it cannot be supported by the local community. The hospital shall participate in at least one community-wide emergency preparedness exercise per year. Each exercise must be realistic and relevant to the priority emergencies identified in the hazard vulnerability analysis. The exercise design team should include a multi-disciplinary approach with a dedicated individual whose sole responsibility is to evaluate performance and is knowledgeable about the goals and objectives of the exercise. This person is responsible for documentation of opportunities for improvement. The After Action Report (AAR) shall include areas of improvement identified and evaluate the effectiveness of improvement that was made in response to critiques of the previous exercise. The exercises will be designed to evaluate performance in at least one of the six critical areas of emergency management:
1. Communication: The organization must be evaluated on the ability to maintain communication pathways within the organization and to external community resources.
2. Resources and assets: The organization must be evaluated on the ability to access materials, supplies, vendor and community services as well as State and Federal resources to ensure patient safety and sustain care, treatment and services.
3. Safety and security: The organization must be evaluated on the ability to provide a safe and secure environment for of its patients and staff.
4. Staff responsibilities: The organization must be evaluated on the ability to enable staff to adapt to their roles to meet new demands and on their ability to care for patients in the presence of new risks and changing conditions.
5. Utilities management: The organization must be evaluated on the ability to maintain the uninterrupted function of key utilities such as power, water, ventilation and fuel.
6. Patient clinical and support activities: The organization must be evaluated on the ability to implement plans to address the needs of patients during extreme conditions when the organization’s infrastructure and resources are taxed.
All exercises are critiqued to identify deficiencies and opportunities for improvement based on the evaluation of the individual performance monitor. The exercise must be critiqued through a multi-disciplinary process that includes administration, clinical (including physicians) and support staff. Based on the outcome of the critique of the emergency management plan(s), processes and related training shall be modified. The EM/BCP is responsible for communicating the strengths and weaknesses identified during the exercise to the disaster committee. PERFORMANCE MONITORS The Chief Operating Officer (or designee), in collaboration with the EOC Chairman, Disaster Committee Chairman and Emergency Manager/Business Continuity Planner shall oversee, implement, establish processes and monitor performance of the EM/BCP and its implementation during an actual or potential emergency event. The Emergency Manager/Business Continuity Planner shall obtain relevant data and information gathered through work orders, surveillance, incidents, exercises and other means. This information shall be reported to the Chairman of the Disaster Committee, the Safety Officer and the EOC Committee.

ANNUAL EVALUATION The Chief Operating Officer (or designee) in collaboration with the EOC Chairman, Disaster Committee Chairman and Emergency Manager/Business Continuity Planner, in conjunction with the Disaster Committee, shall be responsible for providing an annual evaluation of the Emergency Management Program. The annual review shall examine the objectives, scope, performance, effectiveness, performance improvement project and applicability of the Emergency Operations Plan. The annual review shall be presented by the Emergency Manager/Business Continuity Planner to the EOC Committee each year during the first quarter in a narrative summary report. This report will be supported by relevant data and appropriate project improvement processes will be initiated. Strengths and weaknesses shall be identified and goals for process improvement shall be established for the next year. The EOC Committee shall review the report and make recommendations and/or approve the plan. The action of the EOC committees shall be documented in the meeting minutes.

Approved by: ________________________________________ ___________________________ Date Executive Vice-President and Chief Operating Officer ________________________________________ ___________________________ Date Chairman, EM/BCP Committee ________________________________________ ___________________________ Date Chairman, Environment of Care Committee ________________________________________ ___________________________ Date Emergency Manager/Business Continuity Planner

S Situation
Recent events have pointed to remaining gaps in healthcare preparedness – mainly the capacity of our clinics, hospitals and long-term care to continue to deliver essential services when impacted by a service interruption or disaster. Healthcare Business Continuity Planning improves the capacity of our provider organizations to maintain essential services in the event normal operations are adversely affected. We are working to identify requirements and deliver training and tools that align with the specified needs of healthcare organizations.
Business Continuity for Healthcare Organizations
B Background
A Assessment
R Recommendation
In January 2012 the Office of the Assistant Secretary for Preparedness and Response (ASPR) released eight (8) capabilities they identified as the basis for healthcare preparedness. Several healthcare organizations have assessed planning efforts to date against these capabilities and identified the development of a business continuity program; also called continuity of operations plans (COOP), as a key initiative throughout the current 5-year grant cycle.
The cross-section of requirements by ASPR, CMS, HIPAA, and Meaningful Use increasingly stress the need for business continuity planning. To address this, healthcare leaders aim to integrate planning efforts with operations in order to maintain the capacity to operate during emergency events. An unprecedented number of healthcare facilities have closed temporarily or permanently following events due in part to facilities lacking continuity strategies. Aligning these strategies with executive priorities and organizational strategy is essential.
It is recommended that organizations develop an integrated, multi-disciplinary program focused on supporting and strengthening healthcare capabilities and resiliency through the development of a business continuity program.
Shore Health System's Dorchester General Hospital, Cambridge, Md., evacuated patients early Sunday morning because of wind and water damage from Irene and closed for several days. The decision was made after severe damage to the laboratory room warranted the lab's closure. The hospital also saw damage to its operating rooms, central supply, some patient rooms and chemotherapy unit.

Sample Departments Listing for Business Continuity
ActivitiesCare/Case ManagementCommunicationsEnvironmental ServicesFacilities ManagementFinanceFood ServicesHealth Information Management/Medical RecordsHuman ResourcesInfection ControlInformation Services/TechnologyMaterials Management/Supply Chain/Resource ManagementNursing (Patient Care Services, Administration, Education)Palliative CarePsychiatry/Mental HealthRehabilitation Medicine/ServicesSocial WorkSpiritual CareTelecommunications

Sample Departments Listing for Business Continuity
AnesthesiologyAudiologyBariatricsBed ManagementBehavioral HealthCardiovascular/Vascular ServicesCare ManagementChronic Disease ManagementClinical InformaticsClinical ResearchClinical/Service/Operations ExcellenceCommunicationsCommunity Affairs and AdvocacyCorporate Decision SupportCritical Care Services (ICUs)Diagnostic ImagingDialysisEmergency DepartmentEmployee HealthEndoscopyEngineeringEnvironmental ServicesEpidemiologyFacilities ManagementFamily MedicineFinanceFood ServicesFoundationGastroenterologyGeneral MedicineHealth Information Management/Medical RecordsHome Health ServicesHuman ResourcesInfection ControlInformation Services/TechnologyInfusion ServicesIntegrative Medicine
Common Mission Critical Departments are in BOLD

Interpreter ServicesLaboratory ServicesLaundryLegal/General CounselMaterials Management/Supply Chain/Resource ManagementNeonatal Services/NICUNephrologyNeurophysiologyNeuroscienceNuclear Medicine
Nursing (Patient Care Services, Administration, Education)
Obstetrics ServicesOncology OrthopedicsPain ManagementPalliative CarePastoral CarePathology - Morgue PediatricsPeri-operative ManagementPharmacyPre-Admission TestingPsychiatry/Mental HealthPurchasingQuality Mgmt & Patient SafetyRadiation OncologyRadiation SafetyRegistration/Patient AccessRehabilitation Medicine/ServicesCardiopulmonarySecurityShipping/ReceivingSleep EvaluationSocial WorkSpeech PathologySpiritual CareSurgerical Services( Pre-Op/PACU, OR, Clinics/Ambulatory Surgery)

TelecommunicationsTransplantTransportation-Patient/Equip Volunteer ServicesWomen's HealthWound Care

Sample Services/Functions Listing for Business Continuity
Bed managementCash managementCharge captureChart archive managementChart assembly and analysisClean equipment / instrumentsClinical trialsCodingComplete / review preoperative assessmentComplete preoperative checklistDecontaminate equipment / instrumentsDelivery of food ordersDiagnostic testingDictationDishwashingDispensing medicationDistribute equipment / instrumentsDocumentationEmergency treatmentEnter physician ordersFood deliveryGeneral ledger and A/PInterpreting and reviewing imagesInterpreting and reviewing test resultsMaintaining sanitationManage code cartsManage float poolManage traveling nursesMaternal labor & delivery managementMedical staff credentiallingMedication administrationMedication reconciliationMenu planningNursing supervisionOrdering medicationOrdering TestsPackage equipment / instruments

PagingPatient admissionsPatient assessmentPatient dischargePatient monitoringPatient registrationPatient trackingPatient transferPerform imaging proceduresPerform surgeryPreparing foodProcess imageProcessing bill paymentsProcessing claimsProcessing medication ordersProcessing of meal ordersProcessing of payrollProcessing reimbursements & patient paymentsRe-evaluationReceive Diet Orders Receive equipment / instrumentsReceive orderRelease of information Room rurnoverScheduling proceduresScheduling staffSend imagesSpecimen collectionSpecimen testingSterilize equipment / instrumentsStore equipment / instrumentsSubmission of requistionsSupply & equipment managementTelemtryTranscriptionTransfusion servicesTreatmentViewing patient recordsVoice operations

Sample Equipment Listing for Business Continuity
Ambu BagsAnesthesia CartBair Hugger BlanketBedding - Sheets (in sets)Bedding - Sheets / BlanketsBedsBlanket WarmerBlanketsCardiac Monitors with defibrillator capabilitiesCell SaverClippersComputersCopierCrash Cart Cardiac Monitors with defibrillator capabilitiesFaxFlash SterilizerGownsHEPA FilterIce MachineLift equipmentMed refrigeratorOR lightOR tablePhonesPortable suctionPPEPrinterPrintersPt RefrigeratorPyxisSurgicountTourniquetTransport MonitorVentilatorsVideo EquipmentWater / Normal SalineWheelchairWireless phones X-ray aprons

1
1
Steering Committee Chairperson
Members
A committee responsible for program governance who meet at least quarterly to review progress reports and make decisions. Members include executive sponsor (e.g. COO), and key leaders (e.g. CNO, VP Facilities, CMO, VP Human Resources, Emergency Manager and CIO).
Continuity Committee Chairperson
Members
A committee responsible for executing projects/activities led by the Continuity Coordinator/Chairperson. Members include key operational leaders (e.g. supply chain, support services, finance, risk/compliance, emergency management, IT disaster recovery, security, emergency dept., human resources, nursing)
Governance Structure

Establish Governance Model Define the role and responsibilities
of an executive sponsor and
committee representation and
participation requirements
consistent with new standards and
regulations. !Develop or Modify Policy Define EM and BC competencies and
responsibilities of EP Coordinators,
executives, department leaders and
physicians. !
Engaging Leadership & Physicians in EM/BCP
WAK
EFIELD
BRUN
SWIC
K
emergency management l business continuity l information technology l healthcare management
Distribute a One-Page SBAR
Send a report that details “situation,
background, assessment and
recommendation” information to key
executive and physician leadership. !Conduct a 10-Minute Presentation
Explain EM and BCP in the context of
leadership priorities to Executive
Leadership, Medical Executive
Committee, etc. on an annual basis. !Distribute an EM/BCP Annual Activity Calendar
Set up the current years tasks and
activity requirements that move the
System closer to strategic goals !Align with Financial Priorities Ensure detailed strategies for
reducing response costs and improve
outcomes during recovery. !Improve Access to Information Distribute posters and fliers at
strategic locations throughout the
hospital and create a link for easy
web access to plans (e.g. place on an
existing intranet and physician
portal).
7 Actions for strengthening leadership engagement and physician participation in Emergency Operations and Business Continuity Planning through education and alignment with financial and strategic priorities.

Sample email to Department Head requesting that they assign a function representative for the department’s plan development interviews
Dept. head name,
As part of the business continuity planning process at our facility, the plan development team is seeking to identify a representative from your department to participate in a plan development interview. The person selected should be somewhat knowledgeable or be able to obtain information about the department’s mission critical services and processes and the key services that support them.
The in-person interviews will take approximately 60 - 90 minutes. If needed, we may need to conduct follow up phone interviews to clarify or verify data gathered during the interview.
Our team will capture all the information from the interviews to assist in the development of the business continuity plan. During the interview we will have 3 of our team members participate to facilitate the interview as well as document the information from our meeting.
In preparation for the interview, we will ask the departmental representative to take a few minutes to consider the following:
1. If your primary workspace (offices, patient care area, research area, etc.) were unavailable for 5 days, what services and processes would need to be resumed at an alternate location? In 4 hours? In 24 hours?
2. What IT applications, supplies and equipment you would need to resume those services and processes at an alternative location?
3. Does your department have any pre-existing policies, procedures or other documents that should be incorporated into your plan (e.g. downtime procedures, supply par level lists, department-specific emergency procedures)
Although one person should be chosen to represent the department, that person can, if desired, bring other department personnel to the interview to support them in providing information to the plan development team.
Please provide us with the name of the individual you have selected, by date
For questions regarding our project or the interview, please contact me anytime at phone number

Sample email to Department Representative assigned to participate in the plan development interviews
Department Representative name Thank you for agreeing to participate in our pilot business continuity project. We are scheduling in-person interviews Date to conduct the first step in this process – a business impact analysis. The purpose of the interviews is to identify your department’s mission critical services and processes and the key services that support them. The in-person interviews will take approximately 60 - 90 minutes. If needed, we will follow up with you or conduct phone interviews for those who were unable to attend the session. Our team will capture all the information from the interviews to assist in the development of your business continuity plan. During the interview we will have 3 of our team members participate to facilitate the interview as well as document the information from our meeting.
In preparation for the interview, please take a few minutes to consider the following:
1. If your primary workspace (offices, patient care area, research area, etc.) were unavailable for 5 days, what services and processes would need to be resumed at an alternate location? In 4 hours? In 24 hours?
2. What IT applications, supplies and equipment you would need to resume those services and processes at an alternative location?
3. Does your department have any pre-existing policies, procedures or other documents that should be incorporated into your plan (e.g. downtime procedures, supply par level lists, department-specific emergency procedures)
If you believe it is necessary, please feel free to invite other departmental personnel present to assist in providing the plan development information we will need.
For questions regarding our project or the interview, please contact me anytime at phone number

2
FAQ’S
WHAT IS A BUSINESS IMPACT ANALYSIS?
A business impact analysis assists in identifying your department’s mission critical services and processes and the key services that support them. As part of the analysis we assess the impacts that an interruption of these services would cause to our patients, staff and community. Examples of he impacts we are measuring include Patient Safety, Operational (Research, School of Medicine and Hospital), and Financial.
WHAT IS A MISSION CRITICAL SERVICE/PROCESS?
It is not your department name or title.
It includes the activities your department carries out that when non-operational would have a significant adverse impact to our organization. Consider what the three most important things that your department does each day. Think about what processes or IT software applications are needed to carry out those services and processes. Consider applications such as EPIC, or direct process dependencies (e.g. lab results, student registration or physician orders) rather than enterprise services that apply to all departments. (e.g. internet access or power)
HOW DO I PREPARE?
Please review the three considerations provided. Invite all key department staff (Manager, Admin Director, Chair) that would help round out the information needed for your plan.
HOW LONG DO I HAVE?
In order for the team to conduct the data analysis and submit our report, we will need to complete the data gathering, follow ups, and adjustments by the middle of November.

3
FOLLOW UPS
After the in-person interviews, we will follow up with you or conduct phone interviews for those who were unable to attend the session if needed.
There may be some research involved in answering a few of the questions. If you do not have access to that information, we ask that you provide us with the appropriate person to follow up with and attain that answer.

Steering Committee !A committee responsible for program governance who meet at least quarterly to review progress reports and make decisions. !Members include executive sponsor (e.g. COO), and key leaders (e.g. CNO, VP Facilities, CMO, VP Human Resources, Emergency Manager and CIO).
Continuity Committee !A committee responsible for executing projects/activities led by the Continuity Coordinator/Chairperson. !Members include key operational leaders (e.g. supply chain, support services, finance, risk/compliance, emergency management, IT disaster recovery, security, emergency dept., human resources, nursing)
GOVERNANCE
emergency management l business continuity l information technology l healthcare management
Illustration 1
�1
The steering committee meets quarterly to review progress reports and make decisions. Depending on the needs and size of the organization, this can be part of the responsibilities of an existing leadership committee or the establishment of a new committee. (see steering committee responsibilities) The leader responsible for the activities of the program can be a separate position or the responsibility of another leader. (see business continuity director responsibilities) If the selected leader is the emergency manager, continuity committee activities may be carried out under the existing emergency management (EM) committee structure. However, it is recommended that this only be considered in cases where the emergency manager is a dedicated full-time employee.

GOVERNANCEWAK
EFIELD
BRUN
SWICK
emergency management l business continuity l information technology l healthcare management
�2
Steering Committee Responsibilities !• Attend the plan development kickoff meetings
• Attend meetings quarterly to review data for decision support regarding recovery solutions, risk mitigation strategies and any investments regarding the program
• Make decisions regarding project timelines and resources when required by the Project Manager
• Establish a EM/BCP policy
• Allocate knowledgeable personnel and sufficient financial resources to properly implement the BCP
• Ensure that the BCP is reviewed and approved at least annually
• Ensure employees are trained and aware of their roles in the implementation of the BCP
• Review the BCP testing program and test results
• Ensure the BCP is continually updated to reflect the current operating environment
!Business Continuity Director/Committee Chairperson Responsibilities !• Identify plan development participants and manage their availability
• Schedule and coordinate resources necessary to complete the project tasks
• Coordinate efforts to identify, obtain, and deliver the information required to complete the deliverables in the required time frames
• Oversee and ensure completion of any data gathering and other tasks assigned to project participants
• Review and approve deliverables in a timely manner
• Attend and participate in key interviews and program development activities
• Act as the resource responsible for coordinating future plan development efforts and ongoing plan maintenance and testing activities
• Provide education to department leaders

Healthcare Business Continuity Data Collection Questionnaire
Angela [email protected]
whitelight blue areas are populated with your data from previously completed portions of the survey.grey
Step 1: Save File
Save this file directly to your computer as BIA_<name of your department> e.g. BIA_Pharmacy.
When you receive this questionnaire via e-mail attachment, be sure you detach (save) the file to your computer so you do not lose any changes you make and allows you to work on the questionnaire at your convenience.
Thank you for taking the time to complete this survey. The questions in this survey are for your department and will assist you in the development of your business continuity plan. Please follow the step by step process below. This is a very simple Business Impact Analysis (BIA) sample to illustrate some of the content you my wish to capture as part of the BIA. It is not intended to be a complete or comprehensive tool. It is meant to provide a starting point for healthcare organizations to customize to their needs. Please direct any questions to:
Please complete the questionnaire below. You may use the "Tab" key on your keyboard to maneuver through user input fields. Cells in the survey are categorized as follows:
areas are for user input
areas prepopulated and/or include reference information
The questionnaire includes an "Additional Comments" area at the bottom of the questionnaire to capture additional information which you think would be helpful understanding the answers you have provided.

Healthcare Business Continuity Data Collection Questionnaire
Essential number of staff required
Step 2: Fill out your department profile on the BCP Tab
Step 3: Document your essential functions in the table below
Which functions and services must be resumed after an event disrupts normal operations? Consider the minimum essential functions that will allow you to resume department/unit operations if you needed to relocate your department/unit.
Essential Function

Healthcare Business Continuity Data Collection Questionnaire
How would you rate the risk to patients when this function is not available?What is the operational impact to the organization if this function is not available?What is the impact to the family and/or patient experience if this function is not available?
Essential Function or Service
Patient Safety Impact
Operational Impact
Patient Experience
ImpactScoring Legend
0
0
0
0
0
0
Please list essential IT applications for each essential function.
Essential Function or Service
0
0
0
0
0
For each essential application:
Step 4: For each essential function or service, assess the impact when essential functions are not available
5 = Immediately needed, presents life threatening or catastrophic impact if interrupted4 = Needed in less than 4 hrs or it may present threat to life safety3 = Needed in same shift or < 12 hrs or likely to impact operations and/or patient satisfaction
3 = Minimal impact or risk, needed within 1 to 3 days
1 = Need in long term, beyond 3 days
0 = NA
Step 5: Identify essential applications
Application(s) Required to Perform Function

Healthcare Business Continuity Data Collection Questionnaire
Essential Function or Service
Patient Safety Impact
Operational Impact
Downtime Tolerance
0
0
0
0
0
Step 7: List vital records needed to perform essential functions
Step 6: Assess the impact when essential applications are not available
Patient Safety Impact: How would you rate the risk to patients when this application is not available?
Operational Impact: What is the operational impact to the organization if this application is not available?
Downtime Tolerance: How long can you continue to perform this essential function using downtime procedures?
Application(s) Required to Perform Function
0
0
0
0
0

Healthcare Business Continuity Data Collection Questionnaire
Step 9: Document Strategy for Recovery and Interruption Impact
Document the steps for closing down the department and procedures for setting up operations at an alternate location. The procedures should include steps for reopening/recovering operations and returning to normal operations. Use bulleted steps, starting each sentence with action words/verbs.
Step 8: List vital equipment and supplies needed to perform essential functions

10 Quick Tips for Successful Interviews
www.wakefieldbrunswick.com
1. Send out introductory e-mail at least 3-4 weeks before kick-off with follow-up e-mail one week prior
2. Send out selected materials in advance of interviews
3. Conduct interviews immediately following kick-off
4. Schedule 1-1/2 hour first round interviews for selected business, clinical and research units
5. Schedule 2 hour first round interviews for IT staff
6. Hold the interviews in a neutral site (i.e. conference room) so they come to you – where distractions are limited
7. Schedule the interviews back-to-back (with 15 minute break for notes review)
8. Limit the interviews to one functional area and no more than around 5- 6 people beside yourself – err on the side of less people
9. You take all of the notes!!! Interviewees will love you for it and you will end up with better control of the project deliverables
10. Conclude by reflecting back to interviewees any actions, to-do items, or issues you have identified
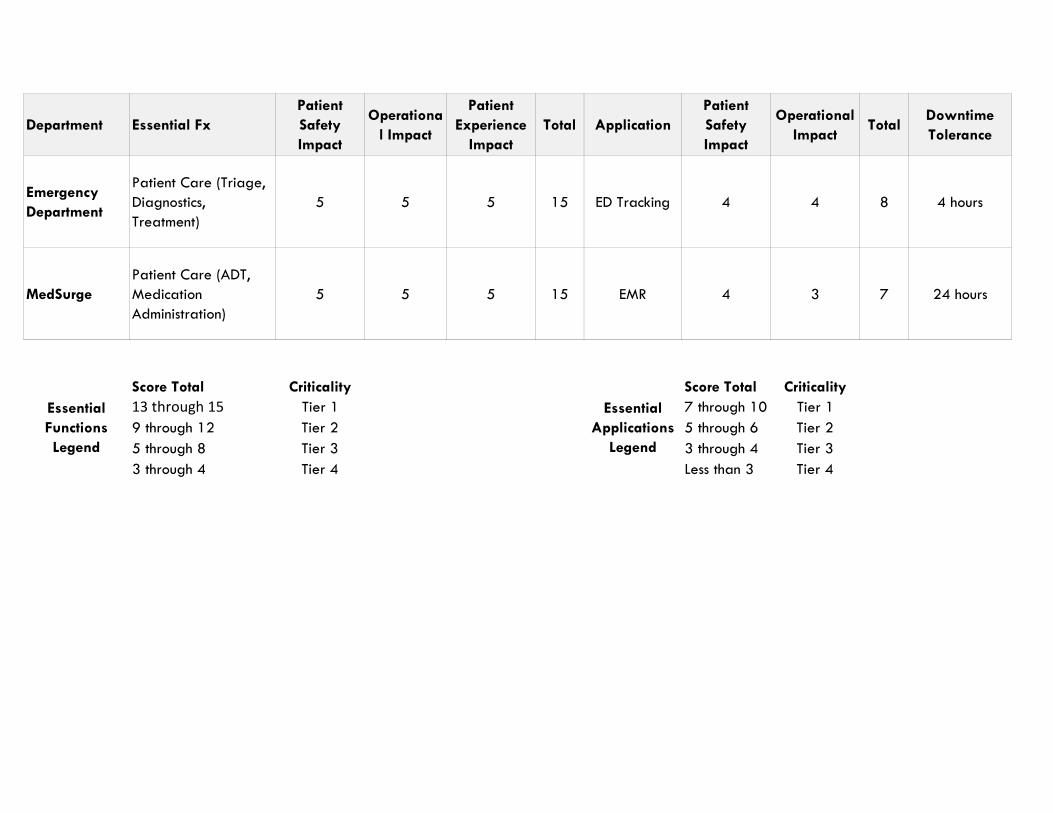
Department Essential FxPatient Safety Impact
Operational Impact
Patient Experience
ImpactTotal Application
Patient Safety Impact
Operational Impact
TotalDowntime Tolerance
Emergency Department
Patient Care (Triage, Diagnostics, Treatment)
5 5 5 15 ED Tracking 4 4 8 4 hours
MedSurgePatient Care (ADT, Medication Administration)
5 5 5 15 EMR 4 3 7 24 hours
Score Total Criticality Score Total Criticality13 through 15 Tier 1 7 through 10 Tier 19 through 12 Tier 2 5 through 6 Tier 25 through 8 Tier 3 3 through 4 Tier 33 through 4 Tier 4 Less than 3 Tier 4
Essential Functions Legend
Essential Applications
Legend

Essential Function or Service
Maximum Interruption Tolerance (hrs)
Functional
Application(s) Required to Perform Function or Service
FunctionalEssential number of staff required
Can Work Be Performed At Home?
12345
Record Name Record Type (Electronic/Paper)12345
Equipment/Supplies DetailsNormal/Par Level
Post-Incident
Gap
12345
Division Name BCP ContactDivision Vice-President/Director Work Phone
Phone Number Emergency/Cell PhoneEmail Address Email Address
Functions, Criticality and Recovery Priority
Department
Vital RecordsBack up or Alternate Record Location
Vital Equipment and Supplies
Relocate to

Strategy for Recovery and Interruption Impact

8875 Hidden River Parkway, Suite 300, Tampa, FL 33637 l www.wakefieldbrunswick.com
EMERGENCY MANAGEMENT AND BUSINESS CONTINUITY PLAN CONTENT SUMMARY Category Joint
Commission ASPR HPP Guidance EOP – BCP Description
Plan Overview
Describes the EM/BCP program
Incident Command
Orders of successions and delegations of authorities
Addresses plan activation and command center operations.
Safety and Security
Safety & Security
Addresses the role of the Safety and Security Officer.
Crisis Management
Communications Continuity communications plan
Addresses Crisis Communications procedures and the role of the Public Information Officer.
Operations Patient Clinical & Support Activities
A means to recognize and understand healthcare organizations shelter-in-place operations and alternate care site operations plans
Location of continuity facilities
Addresses Medical Care & Public Health Emergencies, Hazmat and Evacuation Procedures. It also includes business continuity plans that include Alternate Care Site procedures for relocation and continuity of critical clinical functions.
Patient Clinical & Support Activities
Reduced/altered operations for in-facility movement of service (devolution plan)
Plan for management of vital services
Addresses Departmental Plans including emergency operations and business continuity procedures for Inpatient Units and Clinical Support Services such as Pharmacy and Clinical Labs.
• Integration with HICS, the Business Continuity Branch and the IT Disaster Recovery Plan.
• Continuity Assessment Form • Criteria and steps for closing
and relocating a dept/unit • Resumption of operations of
critical clinical functions • Downtime procedures for an
extended IT outage

8875 Hidden River Parkway, Suite 300, Tampa, FL 33637 l www.wakefieldbrunswick.com
Category Joint Commission
ASPR HPP Guidance EOP – BCP Description
Logistics Utilities Management
Communications
Resources and Assets
Staff Responsibilities
Guidance to assist healthcare organizations with the process for resupply for the transition from COOP to normal operations
Continuity staffing plan (Human capital)
Addresses Infrastructure (this can also be under Operations), Support Branch and Services Branch activities including Communications, Personnel Pool, Supply Chain Management and Family Care.
Planning Addresses the role of the Planning Chief in the command center during activation. Includes templates for Incident Action Plans and associated job action sheets.
Finance Guidance to assist healthcare organizations with the process for reimbursement, reconstitution, or resupply for the transition from COOP to normal operations
Addresses the role of the Finance Chief in the command center during activation. Includes details on Insurance, Local, State and FEMA reporting and/or reimbursement (e.g. forms for claims)
Additionally the finance department template includes the following:
• Continuity Assessment Form • Resumption of operations of critical
business functions • Downtime procedures for an
extended IT outage
Recovery & Resumption
Identification of healthcare organizations healthcare recovery needs to move from COOP to normal operations
Provides overarching strategic guidance for recovery and resumption of operations in a large-scale event that augments the departmental business continuity and recovery strategies.
Appendices 96 Hour Requirement
Hazard Specific Response, 96 hour grid and MOUs