imaging for coronary atherosclerosis - dr raghu · at mail business centre, ... young doctors who...
TRANSCRIPT

RNI Number: TELENG/2015/65122 th th Posted on 15 & 16 of every month
at Mail Business Centre, Plat Form No. 10, Secunderabad Railway Station, Secunderabad
thPublished on 10 of every month
Postal Registration No.: HCD-5001-2016-2018
Volume-2 Issue-9 September - 2016
Notional Cost: Rs. 20/-Pages: 12
A Physician with No Boundaries
New drug therapies for
Pulmonary Hypertension
Imaging for Coronary
Atherosclerosis
Quiz
Prime News
How low should the BP be in
a Diabetic Hypertensive Patient?
DASH Diet (Eating Right) to Lower Blood Pressure

Dear Colleagues,
When should a doctor retire?
“Doctors die but never retire” is a quote commonly used. Prime Minister Narendra Modi's announcement to bring parity on the retirement age for doctors to 65 years is a welcome move. This is an important step by the government considering the rapid improvement in the life expectancy to 68 years over the past five years. Certain state governments have also pursued a similar strategy. The MCI has increased the retirement age to medical teachers up to 70 and propose to increase further to 75 years. Last month a group of doctors from Army Medical Corps have approached the Supreme Court requesting it to intervene and increase the retirement age from the current 60 or 62 years (depending on the rank) to 65 years or else transfer to the central government services. This question is still under the consideration of the tribunal for Armed Forces.
Personally I feel that this move is an apt move considering the scarcity of medical professionals especially in the public hospitals. In addition professionals such as doctors become better with accumulation of experience both clinical and administrative. But young doctors who plan to pursue career in the government sector and as medical teachers will get frustrated owing to the stagnation of career. So government needs to find solutions for career enrichment and enhancement for the younger doctors too. Time bound promotions instead of vacancy determined, incentives for the younger doctors based on outcomes as well as volumes of patients treated, promotion of research and publication as a measure for promotions and most importantly a feed back from the patients could be certain parameters by which younger doctors could be motivated to perform better and contribute to the society.
Unfortunately, many retirees haven't saved enough or planned carefully enough to finance their usual lifestyle after they retire from a career in medicine. The amount of funds needed at the time of retirement varies and is dependent on four factors: longevity, tax rate, investment returns and spending level. Doctors in private practice should plan a transition structure, as the value of patient volume accumulated over decades cannot be allowed to wither away. A good idea (akin to the West) is to sell the practice when the practice is in good shape. Leasing out the existing building to a younger colleague with an escalation clause (should match inflation) when the practice is in good shape and gradually reduce the number of working days and hours is a good strategy to add value to the hard work over many decades. A common mistake is to look for a person to purchase the building and infrastructure without the practicing doctor. We need to understand that retirement for doctors happens only after attaining financial security, availability of pursuits for a happy retirement (you need to be engaged otherwise boredom sets in) and patients with whom you have been associated for decades are handed over to a responsible colleague.
I am sure these strategies help you in planning a retirement which is as important as planning a career.
Warm regards, Raghu Cherukupalli
For appointments: text or call +91 95420 81999 or
+91 98481 55650
www.drraghu.com
drraghu-cardiologist
www.youtube.com/c/Drraghucardio
www.facebook.com/drraghucardiologist
twitter.com/cardioraghu
google.com/+Drraghucardio
Dr C RaghuMD, DMInterventional - Cardiologist & Vascular specialist
practo.com/hyderabad/doctor/raghu-c-cardiologist

Myocardial infarction is the leading
cause of death and a major health-care
burden. Treatments have evolved rapidly
over the past 50 years, but myocardial
infarction remains an unpredictable
event and one that is frequently the first
clinical manifestation of the underlying
atherosclerotic disease process.
Cardiovascular risk scores based on
traditional risk factors are widely
employed, but they remain imprecise in
estimating the risk of myocardial
infarction on an individual basis.
Advances have occurred in a variety of
both invasive and noninvasive imaging
modalities. Invasive coronary imaging
relies on gaining access to the arterial
system and administering contrast
media and specifically designed
catheters into the coronary vessels.
Advances in catheter
design and technology
now allow for an array
of additional invasive
approaches, beyond
t h e s t a n d a r d
assessments of luminal
stenosis.
Coronary physiology
c a n b e r o u t i n e l y
a s s e s s e d u s i n g
fractional flow reserve
(FFR), whereas coronary
plaque imaging has
become possible using
intravascular ultrasonography (IVUS),
and, more recently, optical coherence
tomography (OCT), near-infrared
spectroscopy (NIRS), and near-infrared
fluorescence (NIRF). Each approach
provides different capacities and
potentially complementary information
Noninvasive imaging has undergone
similar developments. In assessing
physiology, absolute quantification of
myocardial blood flow has become
Imaging for Coronary Atherosclerosis
maximal hyperemia. The use of FFR
m e a s u r e m e n t s t o g u i d e
revascularization decisions seems to
improve outcomes after intervention
compared with standard visual
estimations of stenosis
Technological advances in CT now allow
for noninvasive imaging of the coronary
arteries with high spatial resolution.
Coronary CT angiography (CCTA) is
performed during a breath-hold using
scanners with fast detector rotation
times. As with invasive coronary
angiography, a step-
wise deterioration in
prognosis associated
with one-vessel, two-
vessel, and three-vessel
d i s e a s e h a s b e e n
established in multiple
studies using CCTA. The
major current strength
of CCTA is its negative
predictive value: as high
as 95% to 99% in several
studies. Coupled with
the excellent prognosis
of patients found to
have normal coronary arteries, CCTA is
perhaps most useful in ruling out
coronary artery disease in those
considered to be at low or intermediate
risk.
The use of coronary magnetic resonance
angiography for the assessment of
coronary stenosis is attractive in principle
Coronary CT angiography.
C o r o n a r y m a g n e t i c
resonance angiography.
possible, and detailed coronary plaque
imaging is now feasible through
developments in computed tomography
(CT), cardiovascular magnetic resonance
imaging (MRI), and positron emission
tomography (PET).
Invasive coronary angiography involves
the intracoronary administration of
radio-opaque contrast to opacify the
lumen and delineates any existing
stenoses. The presence of luminal
stenoses in one, two, or three vessels is
associated with a step-wise increase in
adverse outcomes. However, the visual
assessment of luminal stenosis correlates
poorly with hemodynamic significance,
particularly for coronary stenosis
between 30% and 80%.
Pressure-wire-derived FFR has become
the favored technique, providing a
lesion-specific surrogate measure of flow
limitation derived from the difference in
arterial pressure proximal and distal to a
coronary lesion of interest during
Assessment of Stenosis,
Obstruction, and Ischemia
I n v a s i v e c o r o n a r y
angiography:
Fractional Flow Reserve (FFR):
3

Coronary artery calcium
scoring
Virtual histology IVUS
Optical Coherence
Tomography (OCT)
Coronary artery calcium (CAC) scoring
using electrocardiogram-gated CT
provides an accurate and simple measure
of the overall atherosclerotic burden in
the coronary arteries. Without the need
for contrast, CAC scoring quantifies
macroscopic calcium within these
vessels, which is pathognomonic of
atherosclerosis.
Virtual histology (VH)-IVUS is an invasive
technique that uses spectral analysis of
the ultrasound backscatter signal to
categorize plaque constituents into
fibrous, fibro-lipidic, calcific, and
necrotic tissue in real time
OCT incorporates an intracoronary fiber-
optic wire, which emits light in the near-
inf rared spect rum (wave length
1,250–1,350 nm) and measures the
backscatter from tissues during a
Imaging for adverse plaque
characteristics
given the avoidance of ionizing
radiation. However, in practice, major
challenges persist in correcting for
coronary artery motion while delivering
the necessary spatial resolution.
Therefore, although its diagnostic
accuracy is improving, coronary
magnetic resonance angiography
remains inferior to CCTA, and is rarely
used in clinical practice.
In myocardial perfusion imaging
(MPI), radioactive tracers are
used that distribute to the
myocardium according to blood
flow. In particular, single-photon
e m i s s i o n c o m p u t e d
tomography (SPECT) and PET
could be used to measure
myocardial perfusion at rest and
during stress, identifying regions
of reversible ischemia associated
with obstruct ive luminal
stenoses.
IVUS involves a miniaturized ultrasound
transducer to record the reflection of
h i g h - f r e q u e n c y s o u n d w a v e s ,
generating grey-scale cross-sectional
images of the arterial wall. This process
provides accurate assessments of
luminal dimensions and plaque volume
that can aid in the evaluation of luminal
stenoses, particularly in the left main
coronary artery. In addition IVUS can
provide accurate quantification of
plaque burden, acting as a powerful
predictor of disease progression and
adverse clinical outcomes.
Myocardial perfusion
imaging
Intravascular
Ultrasonography (IVUS)
Imaging of
Atherosclerotic Plaque
Burden
4
rotational pullback along the artery.
Image acquis i t ion requires the
generation of a blood-free field, using
small flushes of saline or contrast media.
A particular advantage of OCT is its
excellent axial resolution (12–18 μm
versus 150–200 μm for IVUS), which
allows detailed microstructural analysis
of the superficial plaque layers. In
particular, OCT allows imaging of
thrombus, plaque rupture, and
superficial plaque erosion with
improved sensitivity compared with
alternative modalities. OCT is also
increasingly being used clinically to
assess stent deployment and for
post-intervention complications.
NIRS relies on the phenomenon that
organic molecules absorb and reflect
l ight d i f ferent ly at spec i f ic
wavelengths. When near-infrared
light is emitted into a tissue, the
spectrum of absorbance, therefore,
reflects its chemical composition.
This technique can be tuned to
detect lipid within atherosclerotic
plaque creating a 'chemogram' that can
be used to identify lipid-rich lesions and
quantify the lipid core burden index.
Imaging markers of luminal stenosis,
myocardial ischemia, plaque burden,
adverse plaque characteristics, and
disease activity provide complementary
i n f o r m a t i o n a b o u t c o r o n a r y
atherosclerosis — itself a complex,
multifaceted condition. Novel imaging
approaches combining these different
factors might del iver not only
pathological insight, but also major
improvements in cardiovascular risk
prediction.
Near-Infrared
Spectroscopy (NIRS)
Multi-parametric imaging
Current protocol based on Imaging foratherosclerosis

Dr. Bernard Lown, a Nobel Peace
Laureate,is currently the Professor
Emeritus at the Harvard School of Public
Health and Senior Physician at the
Brigham and Women's Hospital in
Boston. He is also the founder of the
Lown Cardiovascular Group and the
Chairman Emeritus of the Lown Institute
that aims to reform both the health care
system and the society.
During his research career spanning
more than 50 years, Dr. Lown's
achievements changed the practice of
cardiology. He was the original developer
of the DC defibrillator and the
cardioverter. He developed the
cardioverter for correcting rapid
disordered heart rhythms and the direct
current defibril lator for cardiac
resuscitation – now the standard of care
for cardiac resuscitation.
Dr. Lown kept his focus on and
relentlessly pursued the arduous
problem of sudden cardiac death, a
leading cause of death in most of the
developed countries. He has been an
ideal clinical educator and lecturer who
inspired hundreds of students pursuing
medicine and more than 200 research
fellows in the Lown Training Program.
Dr. Lown also introduced the new use for
the drug l idoca ine to contro l
disturbances in the heartbeat. All
through his medical career, he focused
on two major medical challenges:
= The problem of sudden cardiac death
= The role of psychological stress on
the cardiovascular system
Dr. Lown's investigations led to many
medical breakthroughs. Among those
were the coronary care unit. In addition,
apart from host of other innovations, his
meticulous work made possible and also
made much of modern cardiac surgery
safe.
Dr. Lown has been instrumentals in
involving physicians worldwide in raising
awareness of the catastrophic
consequences of a Nuclear War and the
urgent need to stop these weapons of
mass destruction. He co-founded the
organization, International Physicians for
the Prevention of Nuclear War, along with
Soviet Cardiologist Dr. Yevgeny Chazov
who later was Minister of Health of the
then USSR. He accepted the Nobel Peace
Prize in 1985, on behalf of the
International Physicians for the Prevention
of Nuclear War.
Dr. Lown is the author and co-author of
four books and over 400 articles that had
been published in leading global medical
journals. His book, 'The Lost Art of
Healing' is worth a special mention here.
Drawing on his 50-plus years of practice
as a cardiologist with vast knowledge of
literature and medical history, Dr. Lown
probes the heart and soul of the doctor-
patient relationship in this book. While
his wisdom stimulate reflection, the
dramatic accounts of real-life characters
and problems throughout his 50-plus-
year career will surely move you. Don't
miss this significant conversation with a
profound individual.
A graduate from Summa Cum Laude
from the University of Maine, Dr. Lown
received his MD from the Johns Hopkins
University of Medicine.
A Physician with No Boundaries
5
"Now the doctor, by virtue of
accepting science so totally,
creates a total imbalance,
forgetting the art of healing,
fo rge t t ing the a r t o f
engagement, forgetting the
art of listening, forgetting the
art of caring and ceasing to
invest time with the patient.
So I believe medicine has lost
its human face. "
– Dr. Bernard Lown, Physician and Nobel prize winner

Clopidogrel Approval by US FDA
Endothelin Receptor
Antagonists
Nitric Oxide pathway
Prostacyclin pathway
Tyrosine kinase inhibitor
Ambrisentan
Bosentan Macitentan
Sildenafil Tadalafil
Vardenafil Riociguat
Beraprost Epoprostenol
Iloprost Treprostinil
Selexipag
Imatinib
Yes
Vardenafil
not approved yet
Beraprost approved in
Japan Trepostinil in
subcutaneous and
inhaled forms only
Selexipag not approved
Unapproved
Examples
Drug therapy for Pulmonary Hypertension
Therapy for Pulmonary Hypertension (PH)
has evolved rapidly over the past 2
decades from the era where only
Nifedipine was the only approved
therapy to the current era where we have
four different groups of drugs (Table 1).
= Acute vasoreactivity testing should
be performed in all patients with
Idiopathic PAH (group 1).
= Vasoreactive patients should be
treated with high and optimally
tolerated doses of CCBs adequate
response should be confirmed after
3 to 4 months of treatment.
= N o n - r e s p o n d e r s t o a c u t e
vasoreactivity testing who are in
WHO-FC II should be treated with
a n o r a l c o m p o u n d .
= N o n - r e s p o n d e r s t o a c u t e
vasoreactivity testing should be
cons idered cand idates fo r
treatment with any of the approved
PAH drugs.
10 steps in management of
Pulmonary Hypertension
The suggested initial approach after the
diagnosis of PAH is the adoption of the
general measures, the initiation of the
supportive therapy, and referral to an
expert center.
New drug therapies for
Pulmonary HypertensionDrug Review
= As head-to-head comparisons
among different compounds are
not available, no evidence-based
first- line treatment can be
proposed (see previous) for either
WHO-FC II or III patients.
= Continuous IV Epoprostenol is
recommended as first- line therapy
for WHO-FC IV PAH patients
because of the survival benefit in
this subset. In absence of IV
Epoprostenol all other compounds
may be utilized.
= Although Ambrisentan, Bosentan,
and sildenafil are approved in
WHO-FC IV patients in the United
States, most experts consider these
treatments as a second line in
severely ill patients.
= In case of inadequate clinical
response, sequential combination
therapy should be considered. In
case of inadequate clinical response
with double combination therapy,
triple combination therapy should
be attempted.
= It seems reasonable to consider
eligibility for lung transplantation
after an inadequate clinical
response to the initial monotherapy
and to refer the patient for lung
transplantation soon after the
inadequate clinical response is
c o n f i r m e d o n m a x i m a l
combination therapy.
= Balloon atrial septostomy should
be regarded as a palliative or
bridging procedure in patients
deteriorating despite maximal
medical therapy.
6

A 45-year male had MI 10 days prior to admission and
referred for coronary angiography and possible
revascularization. His admission ECG is shown in Figure 1.
Coronary angiography revealed two-vessel disease critical
stenosis of Left Anterior Descending and Left circumflex
coronary arteries. He underwent adhoc angioplasty and
stenting for both.
Post angioplasty on day 2 had a broad QRS tachycardia
(Figure 2). He was hemodynamically stable.
7
Q & A in the next page

8
Questions:
1. The baseline ECG (Figure 1) reveals:
2. The broad QRS tachycardia ECG (Figure 2) shows:
3. How do you treat this patient initially?
A.
B.
C.
D.
A.
B.
C.
D.
A.
B.
C.
D.
Infero-Posterior MI
Atrio-ventricular dissociation
Complete RBBB
Complete LBBB.
Ventricular tachycardia
Supravent r i cu la r tachycard ia withaberrancy
Rate dependent broadening of the QRS complex
SVT with bundle branch block
iv Adenosine
iv Amiodarone
Cardioversion
iv Metoprolol
Key to ECG Quiz: E. Concordant pattern in precordial
leads suggests VT, but positive 1. QRS duration more than 120 msec
concordancy may occur during SVT indicates complete bundle branch
with AV conduction over a left block. QRS duration in this ECG is about
posterior AP 80 msec. Presence of prominent R in
F. R nadir S>100ms in one or more lead V1 is suggestive of RBBB if the QRS precordial leads suggests VT, but duration is prolonged. The differential may be found in: diagnosis for a prominent R in lead V1
include: right bundle branch block, left SVT on drugs slowing intra-ventricular ectopy, right ventricular ventricular conduction hypertrophy, acute right ventricular
SVT with AV conduction over an AP dilation (acute right heart strain), type a
Pre-existent BBB (especially LBBB) Wolff-Parkinson-White syndrome,
posterior myocardial infarction,
h ype r t roph i c ca rd iomyopa thy, G. QR complexes during VT suggest
progressive muscular dystrophy, previous myocardial infarction as
dextrocardia, misplaced precordial aetiology
leads, and normal variant1.
The correct answer is APresence of prominent R in V2 (R/S >1)
is indicative of posterior MI and 3. Correct answer is B as the presence of QS in inferior leads
patient is hemodynamically suggestive of inferior MI.stable . But i f unstable ,
Answer for question 1 is Option A.cardioversion is the appropriate
treatment.
2. Broad QRS tachycardia of RBBB Take Home Messages
morphology is seen here. Do not panic when confronted with a
Approach to broad QRS tachycardia is broad QRS tachycardia. Look for clinical
based on these features2: signs of AV dissociation and evaluate the
A. AV dissociation suggests VT, but VA 12 lead ECG systematically. Also, when
conduction may be present during available, look at the 12 lead ECG during
VT sinus rhythm. This approach usually gives
the correct diagnosis of VT versus SVT. B. A QRS width of > 160 ms suggests
Keep in mind that statistically VT is much VT, but need to rule out:
more common than SVT in the broad C. Left axis deviation (to the left of −30) QRS tachycardia. Never make the
suggests VT, but is not helpful in: mistake of rejecting VT because the
b r o a d Q R S t a c h y c a r d i a i s LBBB shaped QRS haemodynamically well tolerated. When
SVT with conduction over a right in doubt, do not give verapamil or
sided or postero-septal AP adenosine; procainamide should be used
SVT during use of class 1 C drugs instead.
D. Right axis deviation (to the right of
+90) suggests VT in LBBB shaped
QRS.
=
=
=
=
=
=
References:
=
=
Prominent R wave in lead V1: Electrocardiographic differential diagnosis. Am J Emerg Med 2001:19; 504-13
Ventricular tachycardia: diagnosis of broad QRS complex tachycardia: Heart 2001;86: 579–585

How low should the BP be in a Diabetic Hypertensive Patient?
The relationship between blood pressure and blood including 49 randomized, controlled trials comprising
glucose has been known for >40 years, when Leren 73,738 participants mainly with type 2 diabetes (Table
et al. reported positive correlations between blood 1). The meta-analysis included only trials with >100
glucose levels and systolic and diastolic blood patients with diabetes who were treated for >12
pressure in a healthy population of white men. months. The included trials involved comparison of an
However, the association between blood pressure antihypertensive agent versus placebo, two agents
and glucose received little or no attention until versus one agent, or any blood-pressure target with
1998. In this year, the findings from the another blood-pressure target. Comparative trials
Hypertension Optimal Treatment trial and the UK between antihypertensive agents or combined
Prospective Diabetes Study addressing the interventions were excluded.
treatment of hypertension in patients with diabetes The systematic review and meta-analysis confirmed were published, and the interest in and awareness that, if the systolic blood pressure before treatment was of hypertension in patients with diabetes escalated. <140 mmHg, no benefit was obtained with the Large outcome trials have been performed in antihypertensive treatment, but was instead associated patients with diabetes and hypertension, and other with an increased risk of cardiovascular death. If systolic hypertension outcome trials have been enriched blood pressure at baseline was >150 mmHg, with large subgroups of patients with diabetes. antihypertensive treatment reduced the risk of all-cause
Today, the question is mostly how low should blood death, cardiovascular death, myocardial infarction,
pressure be lowered in patients with diabetes in stroke, and end-stage renal disease. When the systolic
order to protect against cardiovascular and renal blood pressure was 140–150 mmHg, the risk of all-
disease, because the recommended blood-pressure cause death, myocardial infarction, and heart failure
target of <130/80 mmHg has been questioned. A was reduced. The meta-regression analyses, which
well-designed, single mega-trial with appropriate included a large amount of previously unpublished
statistical power is yet to be conducted. However, data, revealed that the beneficial effect of
Brunström and Carlberg have assessed the effect of antihypertensive treatment on cardiovascular mortality
antihypertensive treatment on mortality and and myocardial infarction decreased with each unit
cardiovascular morbidity in patients with diabetes, decrease in baseline systolic blood pressure, and was
at different blood-pressure levels, in a meta-analysis harmful below certain levels.
9
BaselineSystolic BP
>150mmHg
140-150mmHg
<140mmHg
Effects
â
â Cardiovascular mortality
â Myocardial infarction
â End-stage renal disease
All-cause mortality
â
â Myocardial infarction
â Heart failure
All-cause mortality
á Cardiovascular mortality
á All-cause mortality
Table-1 | BP-lowering therapy & diabetes
DASH Diet (Eating Right) to Lower Blood Pressure
10
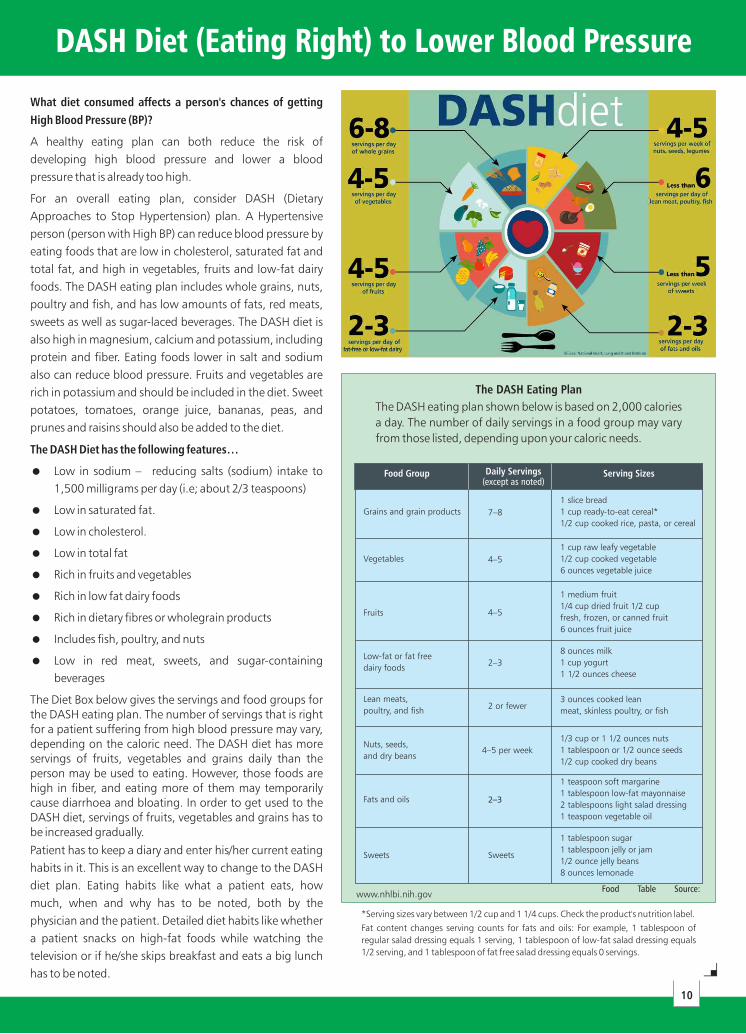
What diet consumed affects a person's chances of getting
High Blood Pressure (BP)?
A healthy eating plan can both reduce the risk of
developing high blood pressure and lower a blood
pressure that is already too high.
For an overall eating plan, consider DASH (Dietary
Approaches to Stop Hypertension) plan. A Hypertensive
person (person with High BP) can reduce blood pressure by
eating foods that are low in cholesterol, saturated fat and
total fat, and high in vegetables, fruits and low-fat dairy
foods. The DASH eating plan includes whole grains, nuts,
poultry and fish, and has low amounts of fats, red meats,
sweets as well as sugar-laced beverages. The DASH diet is
also high in magnesium, calcium and potassium, including
protein and fiber. Eating foods lower in salt and sodium
also can reduce blood pressure. Fruits and vegetables are
rich in potassium and should be included in the diet. Sweet
potatoes, tomatoes, orange juice, bananas, peas, and
prunes and raisins should also be added to the diet.
The DASH Diet has the following features…
The Diet Box below gives the servings and food groups for the DASH eating plan. The number of servings that is right for a patient suffering from high blood pressure may vary, depending on the caloric need. The DASH diet has more servings of fruits, vegetables and grains daily than the person may be used to eating. However, those foods are high in fiber, and eating more of them may temporarily cause diarrhoea and bloating. In order to get used to the DASH diet, servings of fruits, vegetables and grains has to be increased gradually.
Patient has to keep a diary and enter his/her current eating
habits in it. This is an excellent way to change to the DASH
diet plan. Eating habits like what a patient eats, how
much, when and why has to be noted, both by the
physician and the patient. Detailed diet habits like whether
a patient snacks on high-fat foods while watching the
television or if he/she skips breakfast and eats a big lunch
has to be noted.
=
=
=
=
=
=
=
=
=
Low in sodium – reducing salts (sodium) intake to
1,500 milligrams per day (i.e; about 2/3 teaspoons)
Low in saturated fat.
Low in cholesterol.
Low in total fat
Rich in fruits and vegetables
Rich in low fat dairy foods
Rich in dietary fibres or wholegrain products
Includes fish, poultry, and nuts
Low in red meat, sweets, and sugar-containing
beverages
Grains and grain products
Vegetables
Fruits
Low-fat or fat free
dairy foods
Lean meats,
poultry, and fish2 or fewer
Nuts, seeds,
and dry beans4–5 per week
Fats and oils
Sweets Sweets
2–3
7–8
4–5
4–5
2–3
The DASH Eating Plan
The DASH eating plan shown below is based on 2,000 calories
a day. The number of daily servings in a food group may vary
from those listed, depending upon your caloric needs.
Food Table Source:
*Serving sizes vary between 1/2 cup and 1 1/4 cups. Check the product's nutrition label.
Fat content changes serving counts for fats and oils: For example, 1 tablespoon of
regular salad dressing equals 1 serving, 1 tablespoon of low-fat salad dressing equals
1/2 serving, and 1 tablespoon of fat free salad dressing equals 0 servings.
www.nhlbi.nih.gov

Dr. C. Raghu was at Wipro office located at
Gachibowli, Hyderabad on 4 August and 11
August 2016 to deliver a wellness talk on
"Boosting Energy – Tips from a Cardiologist".
11
Dr C Raghu was Guest faculty at the
Telangana state Cardiological Society of
India held at Hotel Avasa on the 28
August 2016. He delivered a lecture on
"Primary Angioplasty – Radial/Femoral".
Dr. Raghu at Wipro Office, Hyderabad
Dr. C. Raghu talking as faculty for the first batch of CCMH
(Certificate Course in Management of Hypertension) Cycle -
I course for Hyderabad Centre at Aster Prime Hospitals.
Initiated in association with Public Health Foundation of
India, Center for Chronic Disease Control, International
Society of Hypertension and British Hypertension Society,
CCMH is an evidence-based learning, up-to-date curriculum
and on-the-job training for general physicians in India.
stDr. Raghu Taking Class for 1 Cycle of CCMH
Dr. Raghu as Guest Faculty at TS CSI

RNI Number: TELENG/2015/65122 th th Posted on 15 & 16 of every month at Mail Business Centre, Plat Form No. 10,
thSecunderabad Railway Station, Secunderabad, Published on 10 of every month,
Notional Cost: Rs. 20/-Printed at New Classic Printers, H.No. 6-3-840/A, Near MCH Market, Ameerpet, Hyderabad - 16, Telangana
Postal Registration No.: HCD-5001-2016-2018,
Printed and Published by Smt. Uma Sreedevi,
Owned by Smt. Uma Sreedevi
Registered Address: G2, Krishna Apartments, Ameerpet Cross Roads, Yellareddyguda, Hyderabad - 73, Telangana
Editor: Dr. C. Raghu
If undelivered please return to
Flot No. 201, 2nd Floor, Manjeera Square, Plot No. 6 & 7, Ameerpet, Hyderabad - 500 038
Ph: 8096398789
Dr C Raghu along with Dr Wataru Nagamatsu from Hokusetsu General Hospital, Osaka,
Japan and Dr Srinivas Movva from Aster Prime Hyderabad, have performed a complex thangioplasty of Chronic Total Occlusion of right coronary artery on 24 August 2016.