imaging of aortic dissection
TRANSCRIPT
DR.SAKHER-ALKHADERI CONSULTANT RADIOLOGIST AMC
18/8/2015
Imaging Of Imaging of aortic
dissection
INTRODUCTION

OBJECTIVES
2-Early diagnosis of Aortic dissection based on the imaging criteria
3-Differentiate between true & false lumen
4-Recognize the imaging features which help in management decision
1-Differentiate the 3 types of acute aortic syndrome
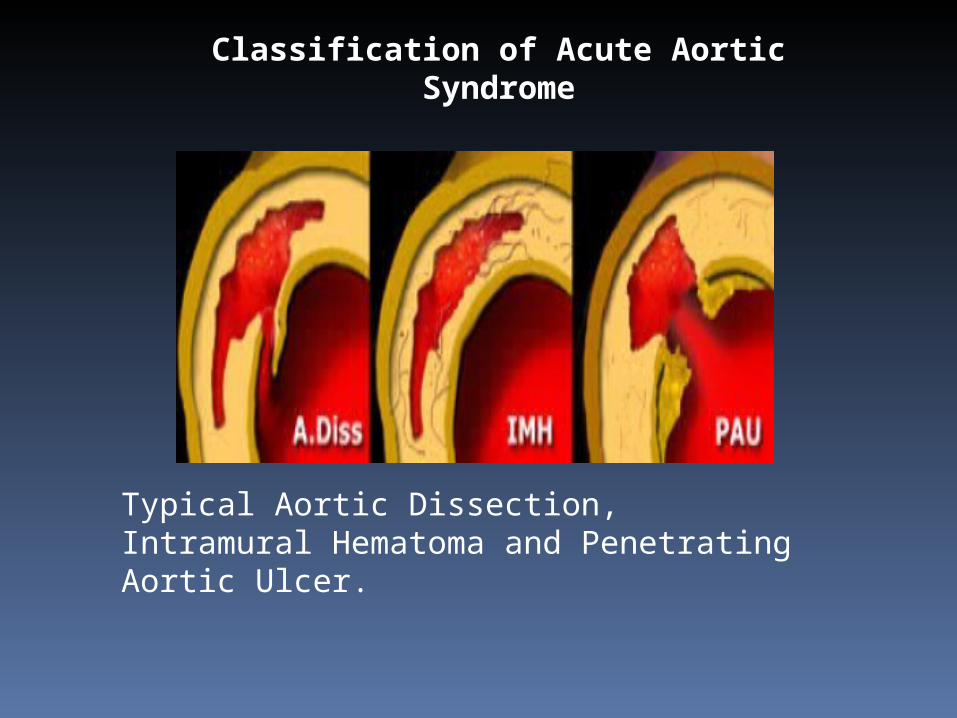
Classification of Acute Aortic Syndrome
Typical Aortic Dissection, Intramural Hematoma and Penetrating Aortic Ulcer.

Aortic Dissection (AD) definition
Classic aortic dissection is a longitudinal split or partition in the media of the aorta. An intimal tear connects the media with the aortic lumen, and an exit tear creates a true and a false lumen. The smaller true lumen is lined by intima, and the false lumen is lined by media. Typically, flow in the false lumen is slower than in the true lumen, and the false lumen often becomes aneurysmal when subjected to systemic pressure. An acute aortic dissection is considered chronic at 2 weeks. The dissection usually stops at an aortic branch vessel or at the level of an atherosclerotic plaque.[1, 2]
Diagram illustrates events leading to aortic dissection from formation of entrance tear and exit tear of intima to splitting of aortic media and formation of intimomedial flap. Blood under pressure dissects media longitudinally, and double-channel aorta is formed with blood filling both true and false lumens.
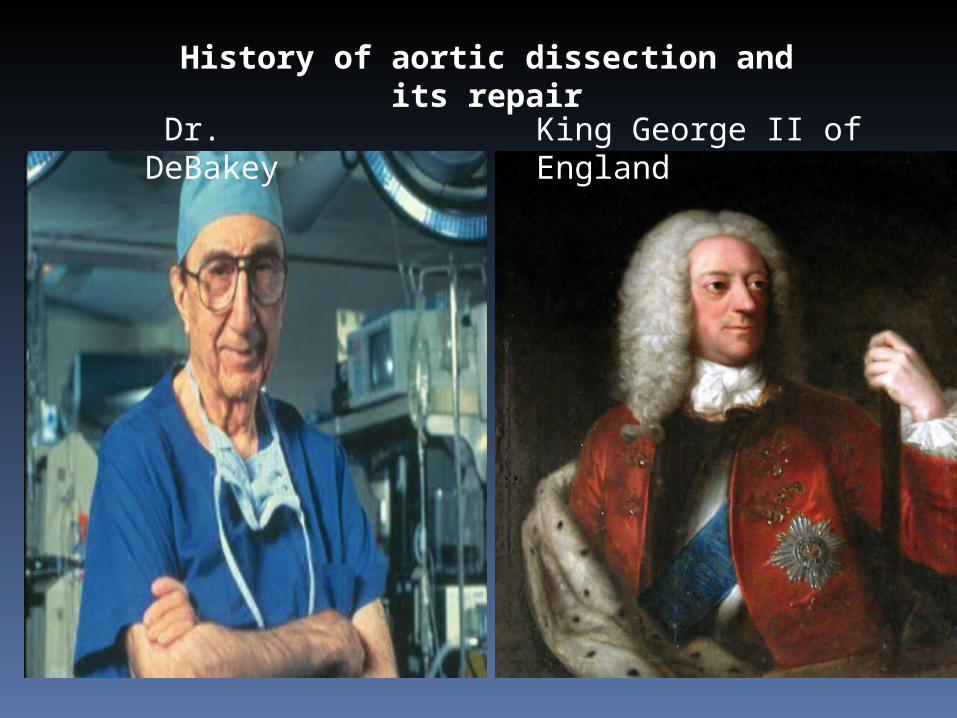
History of aortic dissection and its repair
King George II of England Dr. DeBakey

History of aortic dissection and its repair
The first well-documented case of aortic dissection occurred in 1760, when King George II of England died while straining on the commode. In 1761, the celebrated Italian anatomist Giovanni Battista Morgagni provided the first detailed pathologic description of aortic dissection.Aortic dissection was associated with a high mortality rate before the introduction of the cardiopulmonary bypass in the 1950s, which led to aortic arch repair and construction. DeBakey performed the first successful operative repair in 1955.Modern techniques of diagnosing and repairing thoracic aortic dissections transformed the condition from a death sentence to a treatable disorder—as shown by the experience of Dr. DeBakey himself, who developed aortic dissection at age 97, and at age 98 became the oldest patient to survive the surgical procedure he pioneered.
Signs and symptoms
Sudden onset of severe chest pain that often has a tearing or ripping quality (classic symptom)Chest pain may be mildAnterior chest pain: Usually associated with anterior arch or aortic root dissectionNeck or jaw pain: With aortic arch involvement and extension into the great vesselsTearing or ripping intrascapular pain: May indicate dissection involving the descending aortaNo pain in about 10% of patientsSyncopeCerebrovascular accident (CVA) symptoms (eg, hemianesthesia, and hemiparesis, hemiplegia) [1]
Altered mental statusNumbness and tingling, pain, or weakness in the extremitiesHorner syndrome (ie, ptosis, miosis, anhidrosis)DyspneaHemoptysisDysphagiaFlank pain (with renal artery involvementAbdominal pain (with abdominal aorta involvement)FeverAnxiety and premonitions of death

Risk factors for aortic dissection -Long-standing hypertension -Male -Advanced age -Prior cardiac surgery -Known aortic aneurysm or prior dissection-Cardiac catheterization/surgery-Connective tissue disorders- Marfan’s syndrome -Ehlers−Danlos syndrome -Bicuspid aortic valve, Coarctation of the aorta, Hereditary thoracic aortic disease, Vascular inflammation ,Deceleration injury ,Cocaine, Peripartum
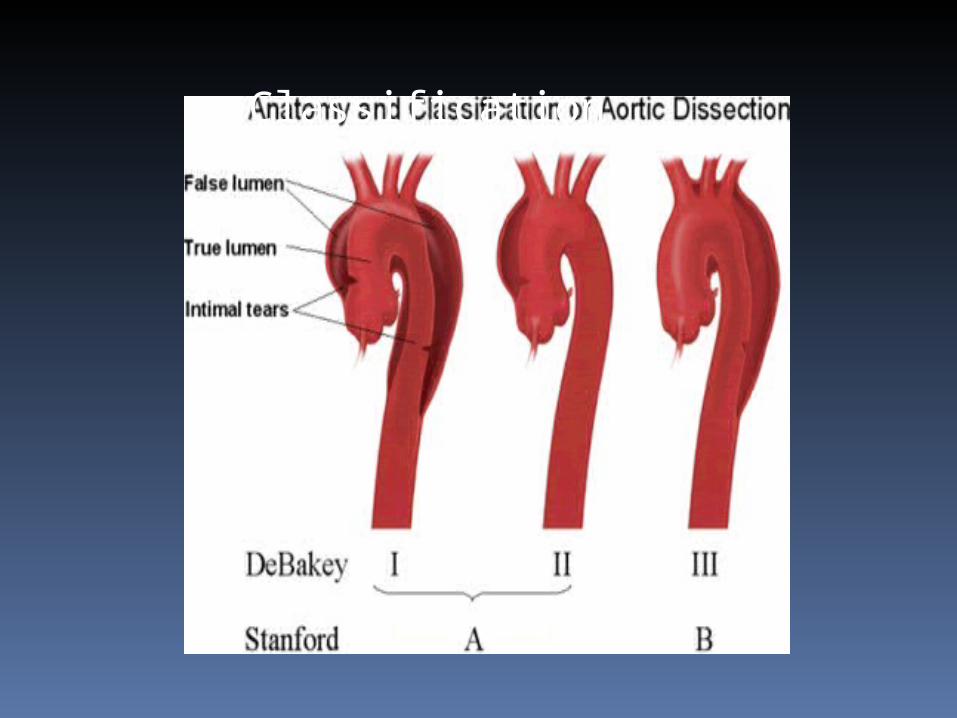
Classification

Classic Aortic Dissection is the most common entity causing an acute aortic syndrome (70%).Incidence: 1-10 : 100.000mostly menhypertension > 70%Type A mortality 1-2% per hour after onset of symptoms, total up to 90% non-treated, 40% when treated.1 year survival Type B up to 85% if medically treated (5 year > 70%)
Aortic Dissection (AD)
Management decisions are based on the following information:Type A or Type BPlace of entry & re-entrySide branches involved, originating from true / false lumenOrgans at risk (1/3 of mortality is caused by organ failure)Complications (rupture, coronary occlusion, aortic insufficiency, neurological )Diameters of true and false lumina at: proximal and distal landing zones, at entry and at minimumIliac vessel turtuosity.
Aortic Dissection (AD)

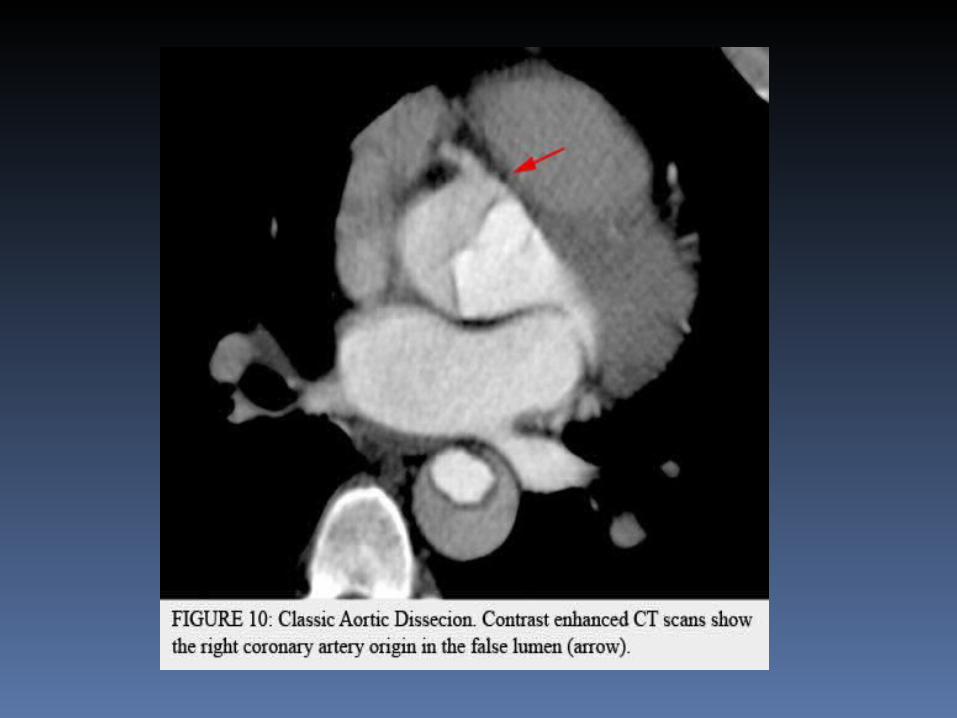
-Most classic aortic dissections begin at 3 distinct anatomic locations: the aortic root; 2 cm above the aortic root; and just distal to the left subclavian artery. Ascending aortic involvement may result in death from wall rupture, hemopericardium and tamponade, occlusion of the coronary ostia with myocardial infarction, or severe aortic insufficiency.
Aortic Dissection (AD)
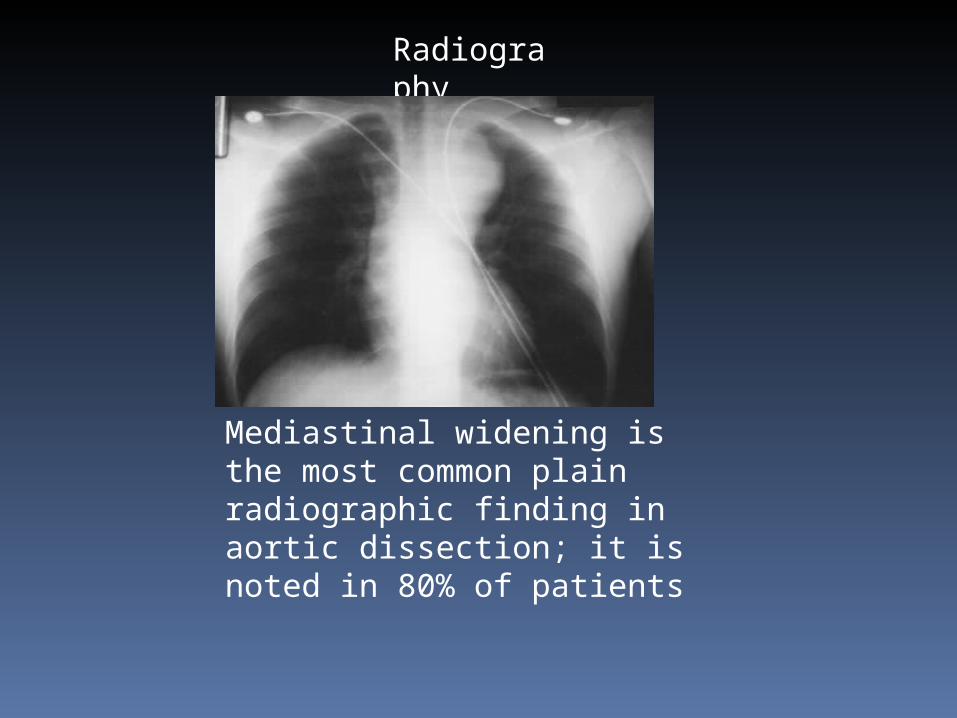
Radiography
Mediastinal widening is the most common plain radiographic finding in aortic dissection; it is noted in 80% of patients

Radiography
Irregular aortic contour
Other radiographic findings include the following:Double aortic knob sign (present in 40% of patients)Diffuse enlargement of the aorta with poor definition or irregularity of the aortic contourInward displacement of aortic wall calcification by more than 10 mmTracheal displacement to the rightPleural effusion (more common on the left side; suggests leakage)Pericardial effusionCardiac enlargementDisplacement of a nasogastric tubeLeft apical opacity
Radiography

Inward displacement of aortic wall calcification by more than 10 mm
Radiography
Radiography
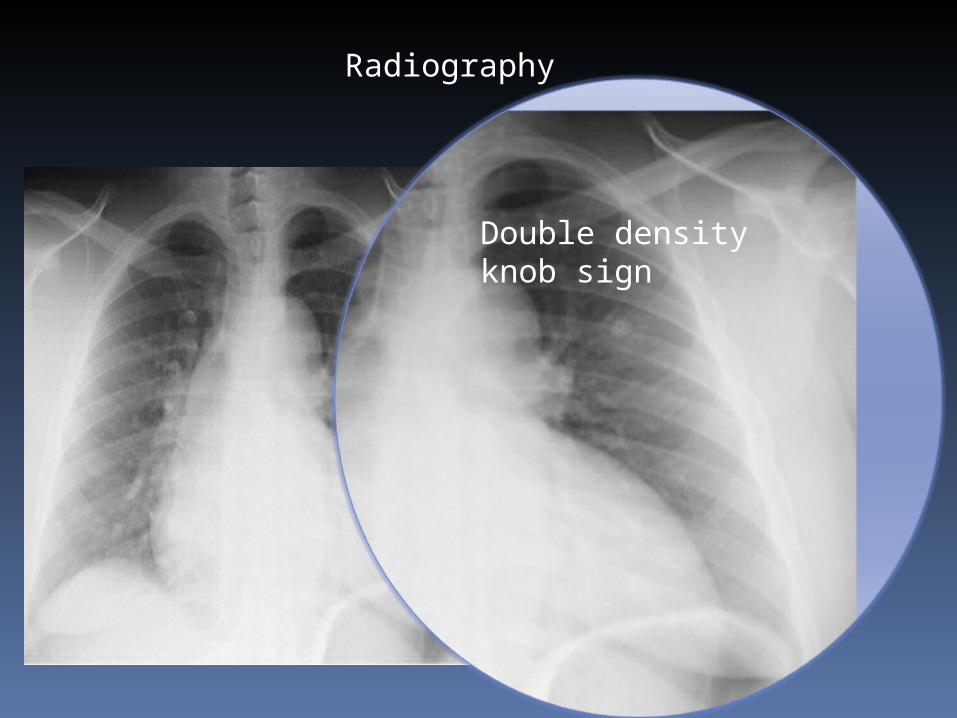
Double density knob sign

Computed TomographyThe sensitivity of CT for aortic dissection is 87-94%, and the specificity is 92-100%.
Multidetector CT may be performed with 1-2.5 mm collimation. Initial nonenhanced CT is used for the diagnosis of acute hemorrhage and aortic rupture. This is followed by helical CT performed approximately 25-30 seconds after the injection of contrast material. Nonionic contrast material (120-135 mL) is power injected via a peripheral intravenous site at a rate of 3-4 mL/s.
Usually, scanning is performed from the thoracic inlet to the common femoral arteries. When a dissection is identified, repeat scanning may be performed to obtain delayed images of the false lumen and aortic branches. Multiplanar reformation images are obtained in sagittal, coronal, oblique sagittal,

Computed Tomography
Typical CT findings in acute dissection include the following:-Detection of intimal flap which separates two lumina in the involved part .
True lumen:Surrounded by calcifications (if present)Smaller than false lumenUsually origin of celiac trunk, SMA and right renal artery

False lumen:Flow or occluded by thrombus (chronic).Delayed enhancementWedges around true lumen (beak-sign)Collageneous media-remnants (cobwebs)Larger than true lumenCircular configuration (persistent systolic pressure)Outer curve of the archUsually origin of left renal arterySurrounds true lumen in Type A dissection


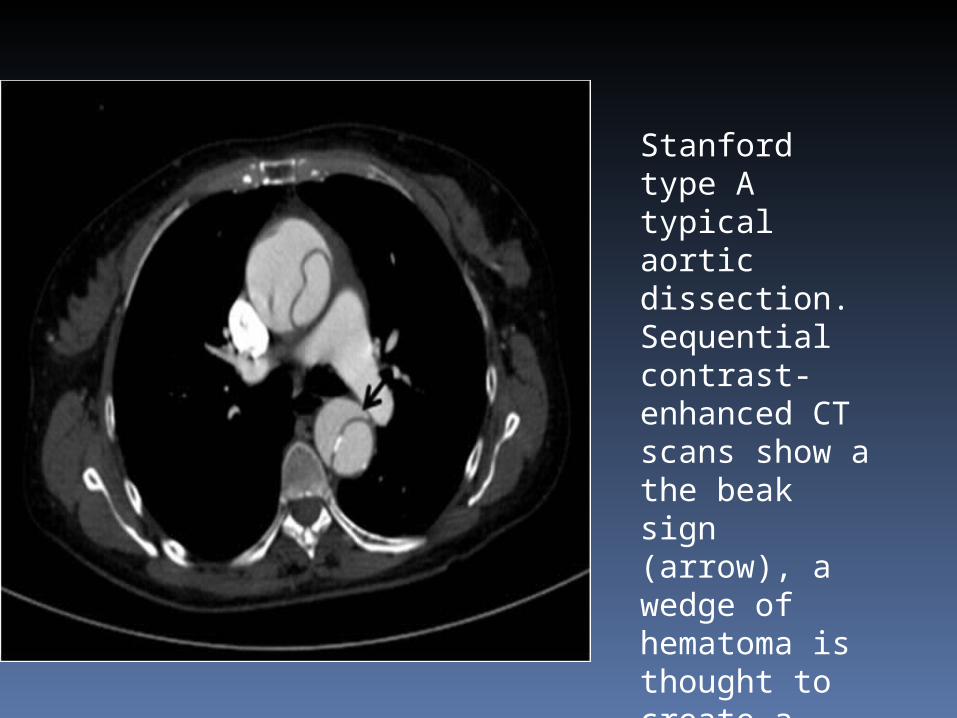
Stanford type A typical aortic dissection. Sequential contrast-enhanced CT scans show a the beak sign (arrow), a wedge of hematoma is thought to create a space for the development of the false lumen
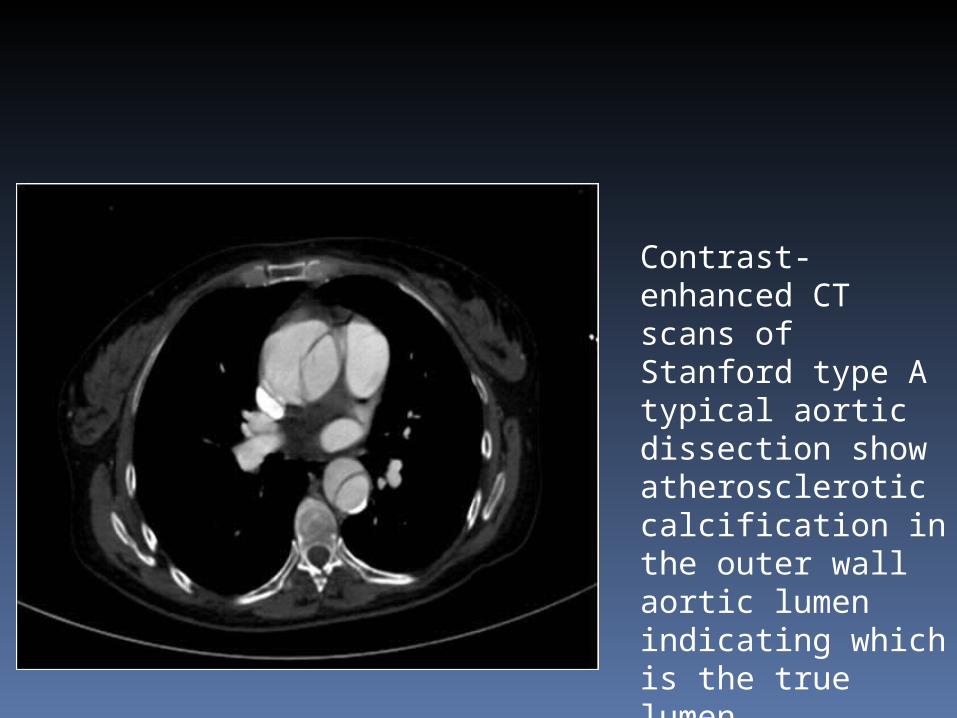
Contrast-enhanced CT scans of Stanford type A typical aortic dissection show atherosclerotic calcification in the outer wall aortic lumen indicating which is the true lumen



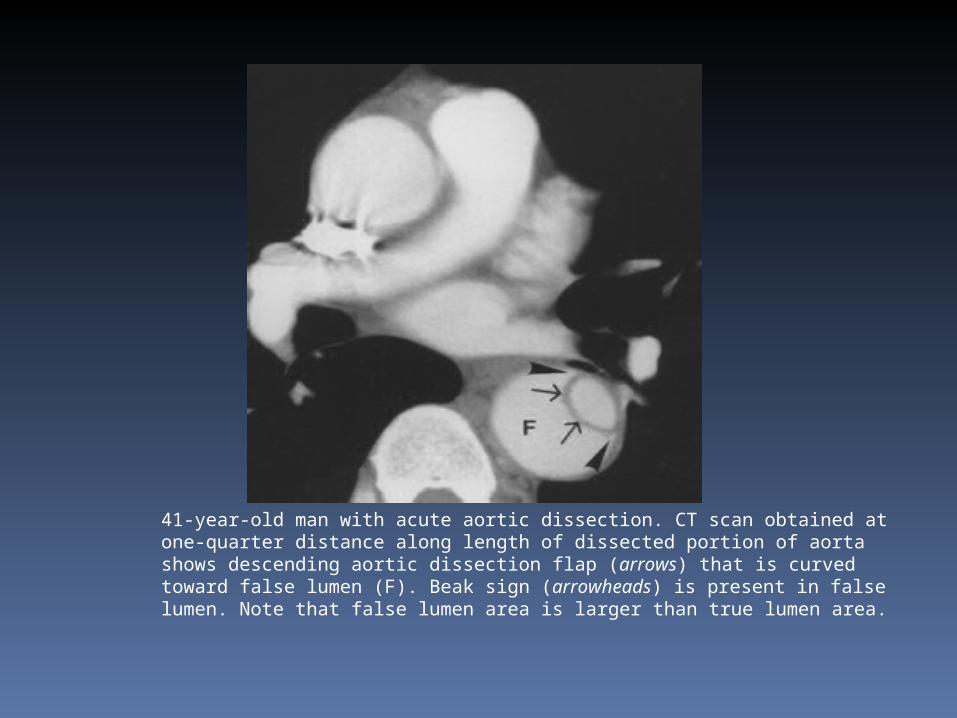
41-year-old man with acute aortic dissection. CT scan obtained at one-quarter distance along length of dissected portion of aorta shows descending aortic dissection flap (arrows) that is curved toward false lumen (F). Beak sign (arrowheads) is present in false lumen. Note that false lumen area is larger than true lumen area.

51-year-old woman with chronic aortic dissection. CT scan obtained at one-half distance along length of dissected portion of aorta shows flat dissection flap. False lumen beaks are filled with lowattenuation thrombus (arrowheads). Faintly visualized cobweb (arrows) is present in false lumen (F).
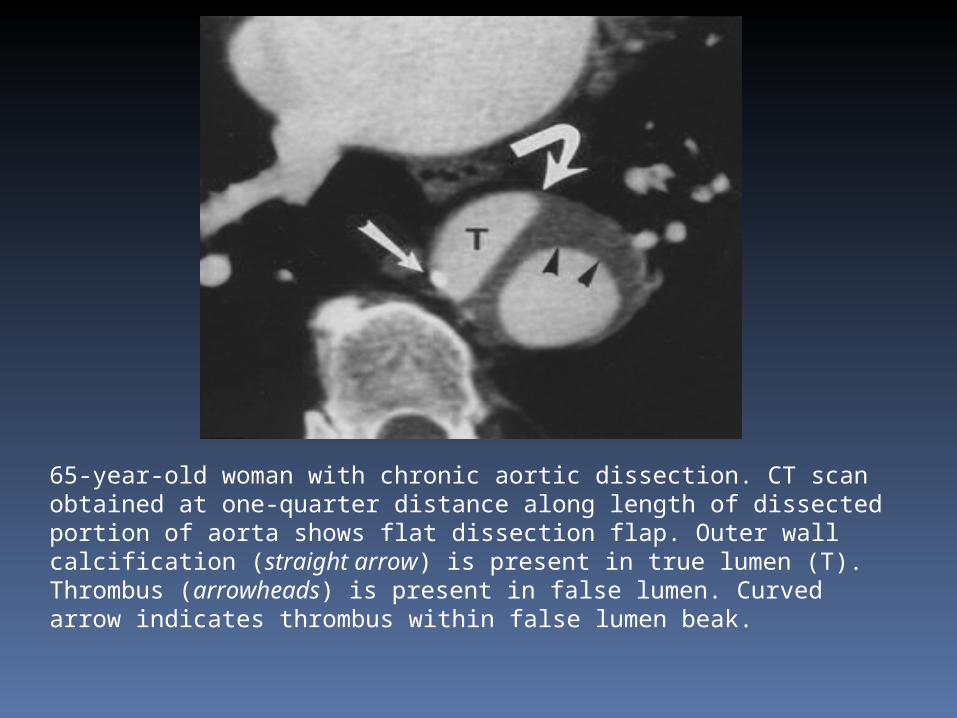
65-year-old woman with chronic aortic dissection. CT scan obtained at one-quarter distance along length of dissected portion of aorta shows flat dissection flap. Outer wall calcification (straight arrow) is present in true lumen (T). Thrombus (arrowheads) is present in false lumen. Curved arrow indicates thrombus within false lumen beak.
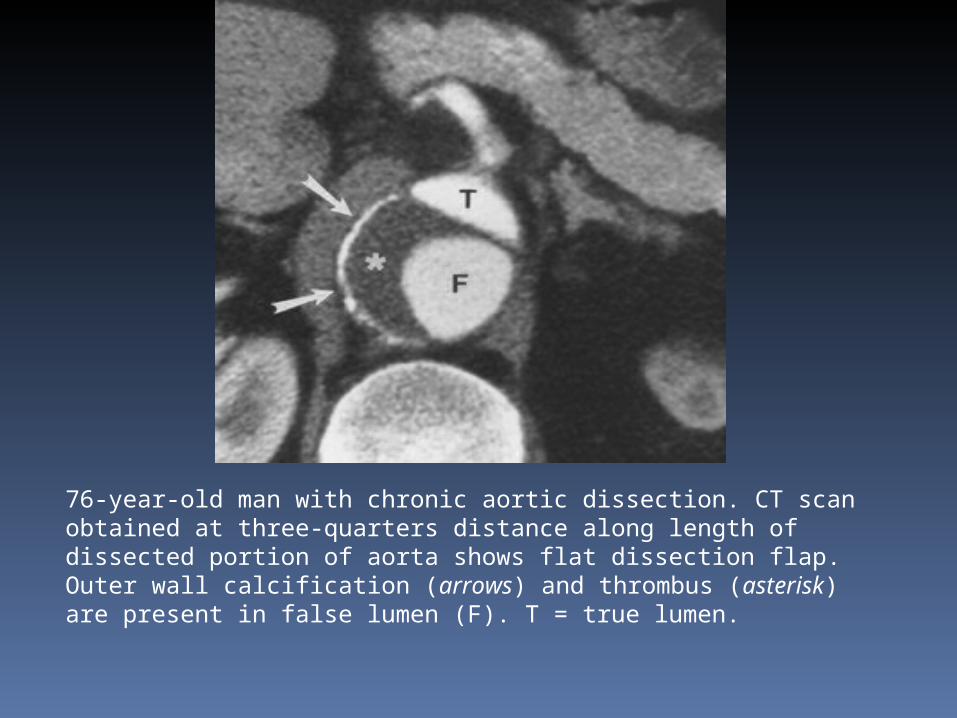
76-year-old man with chronic aortic dissection. CT scan obtained at three-quarters distance along length of dissected portion of aorta shows flat dissection flap. Outer wall calcification (arrows) and thrombus (asterisk) are present in false lumen (F). T = true lumen.
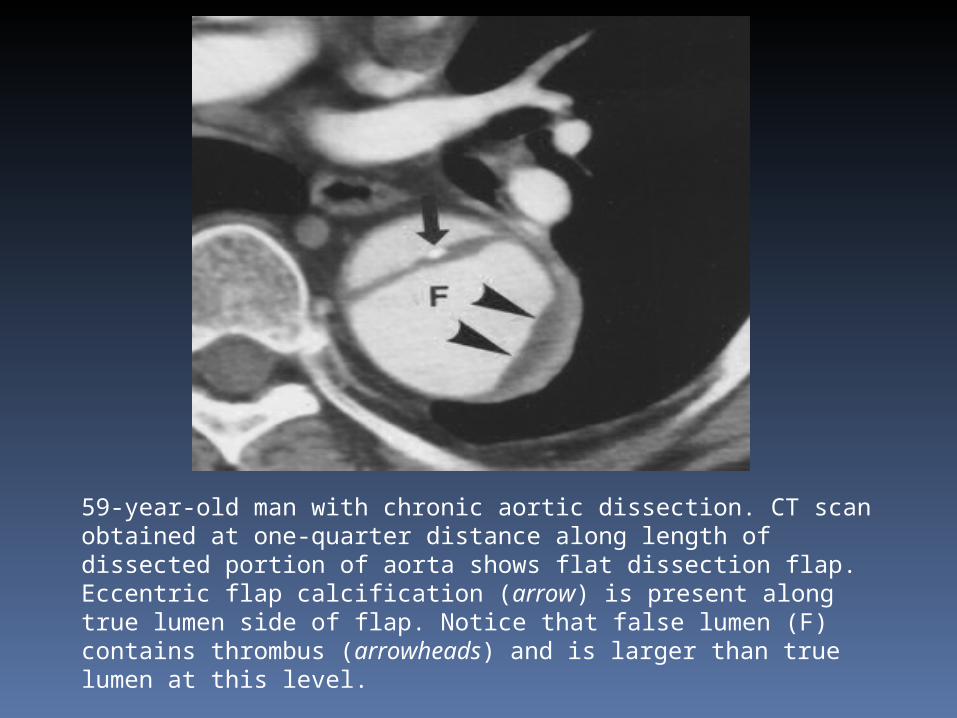
59-year-old man with chronic aortic dissection. CT scan obtained at one-quarter distance along length of dissected portion of aorta shows flat dissection flap. Eccentric flap calcification (arrow) is present along true lumen side of flap. Notice that false lumen (F) contains thrombus (arrowheads) and is larger than true lumen at this level.

69-year-old woman with acute aortic dissection. CT scan obtained at level of transverse aortic arch shows that outer false lumen (F) wraps around inner true lumen (T). Dissection flap extends into innominate artery. Note cobweb in false lumen (arrow) and bilateral pleural effusions (P).

Axial double-inversion-recovery MR images (TR/TE, 1875/18; inversion time, 150 msec) of 37-year-old man with Marfan syndrome. Image shows classic aortic dissection with double-channel aorta. True lumen (straight arrow) is smaller than false lumen (curved arrow). High-velocity flow in true lumen causes signal void. Slower flow with higher signal can be seen in false lumen.
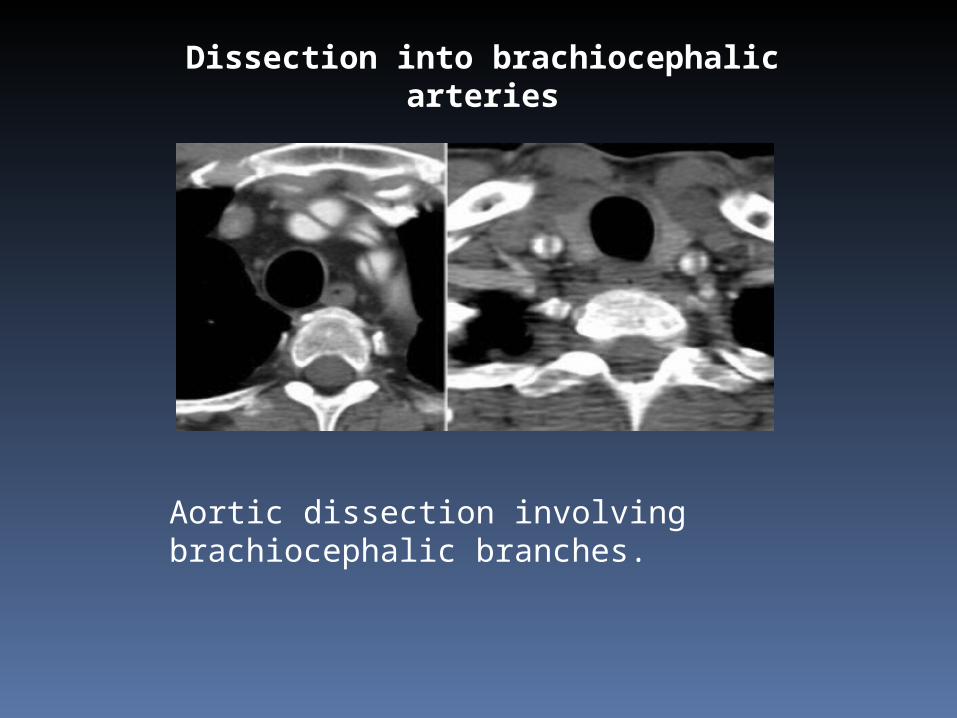
Dissection into brachiocephalic arteries
Aortic dissection involving brachiocephalic branches.

Dissection into abdominal arteries

61-year-old man with symptoms of right hemispheric stroke who was found to have marked blood pressure discrepancy between arms and hypertension. Urgent CT scan (not shown) revealed type A aortic dissection. Patient went into asystole and died 15 hr after imaging. Axial CT scan shows dissection continuing along right wall of abdominal aorta (arrow). No enhancement of right kidney parenchyma was present.
Dissection into abdominal arteries
The celiac trunk, SMA and right renal artery flow usually originates from the true lumen.
Dissection into abdominal arteries
Left renal artery flow mostly originates from the false lumen.Impaired perfusion of end-organs can be due to 2 mechanisms: 1) static = continuing dissection in the feeding artery (usually treated by stenting)
2) dynamic = dissection flap hanging in front of ostium like a curtain (usually treated with fenestration).
When no end-organs are compromised and there is sufficient perfusion, dissection can be left alone.
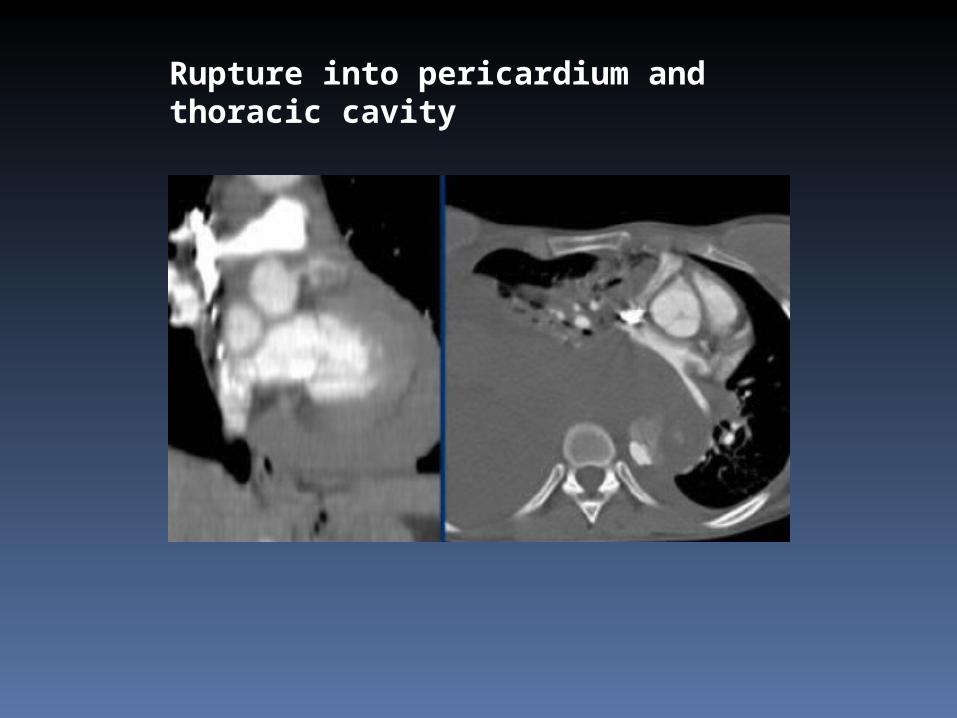
Rupture into pericardium and thoracic cavity

Aneurysm with thrombus versus thrombosed dissection
LEFT: Dissection with a thrombosed false lumen. RIGHT: Aneurysm with thrombus on the inner side of the intimal calcifications.

Intramural Hematoma
Brief facts:Spontaneous hemorrhage caused by rupture of vasa vasorum in media13% of dissections, usually no pulse deficitDifficult to distinguish from thrombosed ADCan proceed to classic dissection (16-47%)Long time to diagnosis: usually overlooked due to lack of non-enhanced scanMortality at 1 year after dismission ~ 25%
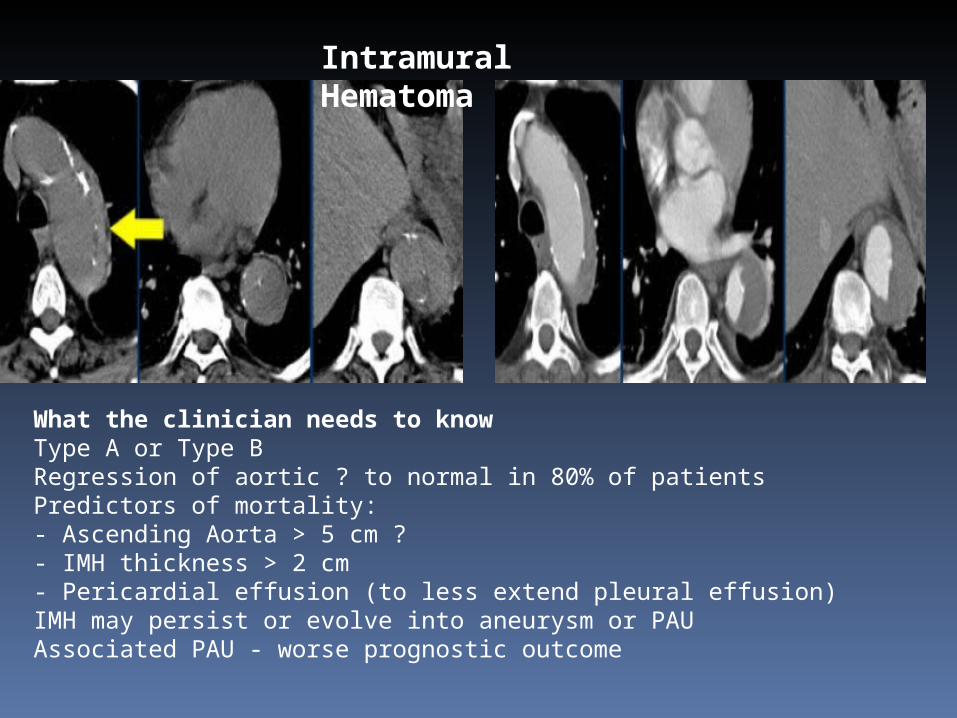
Intramural Hematoma
What the clinician needs to knowType A or Type BRegression of aortic ? to normal in 80% of patientsPredictors of mortality: - Ascending Aorta > 5 cm ?- IMH thickness > 2 cm- Pericardial effusion (to less extend pleural effusion)IMH may persist or evolve into aneurysm or PAUAssociated PAU - worse prognostic outcome

6-year-old man with concurrent intramural hematoma involving ascending aorta and communicating dissection involving descending aorta. Axial unenhanced CT scan shows hyperdense crescentic hematoma in wall of ascending aorta (white arrow) with eccentric narrowing of lumen, type A intramural hematoma. Small intramural hematoma (arrowhead) is also noted at left lateral aspect of proximal descending aorta. High-attenuation dissection flap (black arrow) is seen in descending aorta.
Axial contrast-enhanced CT scan obtained at same level as A shows wall thickening in ascending and descending aorta, but high-attenuation intramural hematoma is less obvious. Classic intimomedial flap (arrow) dividing true and false lumens in descending aorta is more conspicuous after contrast administration. Note irregular margin of flap on false lumen side. Intramural hematoma (arrowhead) is seen along lateral wall of false lumen.

Intramural hematoma revealed by displaced intimal calcifications on noncontrast helical CT (window = 440, level = 40). High attenuation material in the wall of the descending aorta .

Penetrating Atherosclerotic Ulcer
PAU is defined as an ulceration of an atheromatous plaque that has eroded the inner elastic layer of the aortic wall.It has reached the media and produced a hematoma within the media.
Brief facts:Patients with severe systemic atherosclerosisRarely rupture, yet worse prognosis due to extensive atherosclerosis which causes organfailure (e.g. acute myocardial infarction)Cause of most saccular aneurysmsLocated in arch and descending aortaOften multiple (therefore surgical treatment difficult, mostly treated medically)
Penetrating Atherosclerotic Ulcer
What the clinician needs to knowType A or Type BSingle or multipleAssociated IMH (if not present, be cautious to mention PAU, clinical symptoms might not be caused by PAU, which is probably stable)Possibility of endovascular treatment
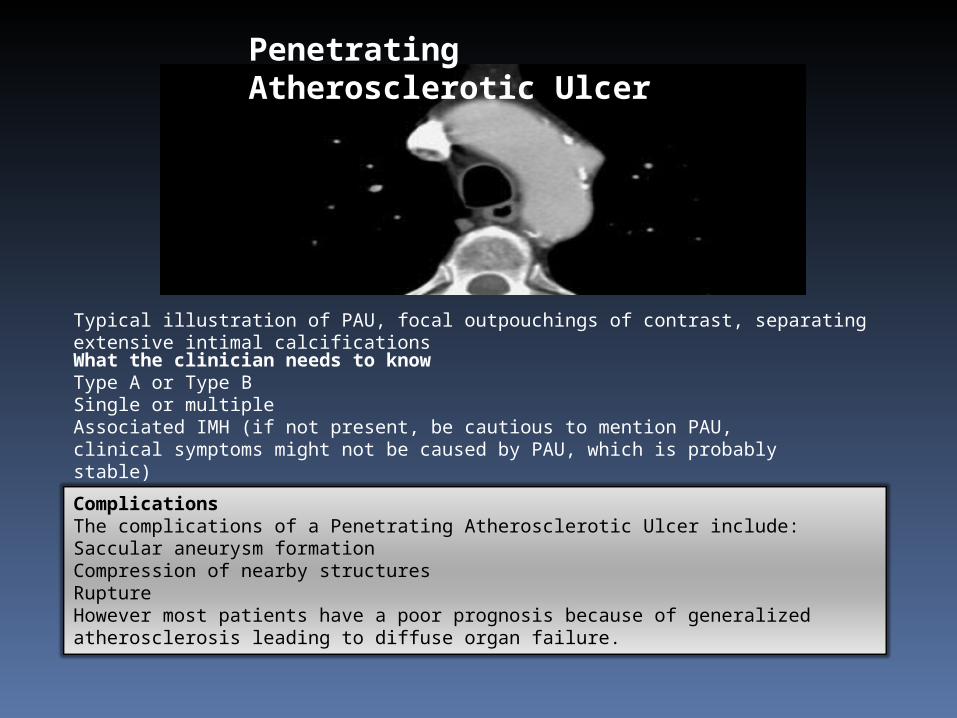
Typical illustration of PAU, focal outpouchings of contrast, separating extensive intimal calcifications
ComplicationsThe complications of a Penetrating Atherosclerotic Ulcer include:Saccular aneurysm formationCompression of nearby structuresRuptureHowever most patients have a poor prognosis because of generalized atherosclerosis leading to diffuse organ failure.
Penetrating Atherosclerotic Ulcer
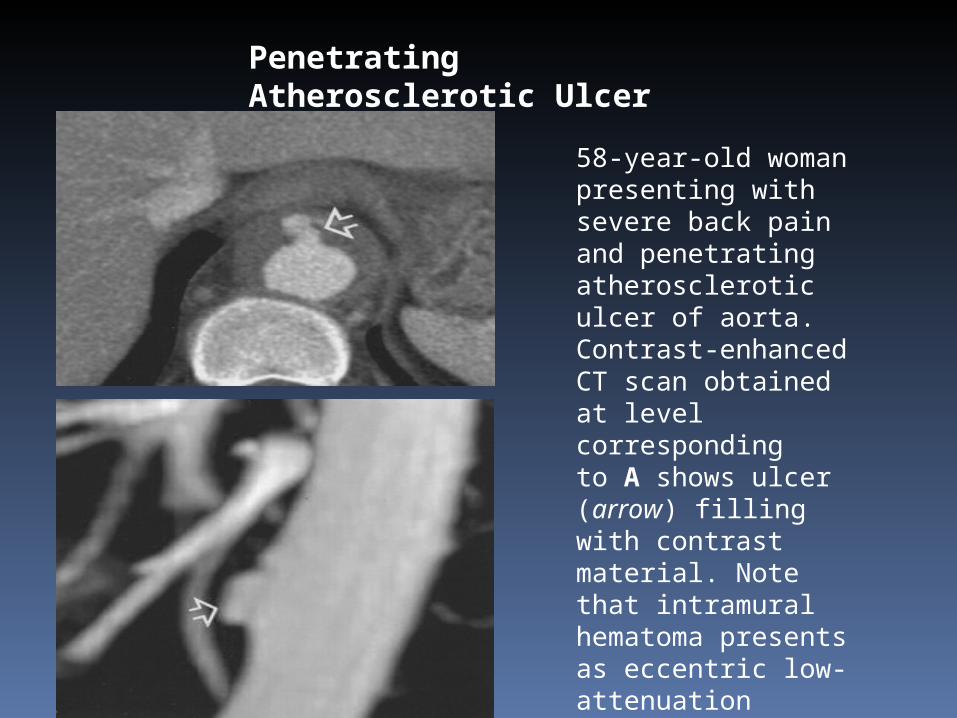
58-year-old woman presenting with severe back pain and penetrating atherosclerotic ulcer of aorta. Contrast-enhanced CT scan obtained at level corresponding to A shows ulcer (arrow) filling with contrast material. Note that intramural hematoma presents as eccentric low-attenuation thickening of aortic wall.
THE END