imaging of pulmonary nodules - healthcare professionals
TRANSCRIPT

Imaging of Pulmonary Nodules
Bradley R. Trotter, MD, DABR, DABNM
Department of Radiology
B R Trotter, MD Scott & White Healthcare

Imaging of Pulmonary Nodules:Overview
• Background: From Nodules to Lung Cancer
• Review of Imaging Modalities: Tools of theTrade
• Review of Imaging Features: “To benign ornot to benign, that is the question.”
• Likelihood of Malignancy: “… damned lies,and statistics”
• Recommendations: Putting it together
B R Trotter, MD Scott & White Healthcare

Background: From Nodules toLung Cancer
B R Trotter, MD Scott & White Healthcare

Background: Pulmonary Nodules
• “A round opacity, at least moderately wellmarginated, and no greater than 3 cm inmaximum diameter”
• “Round” meaning roughly circular or ovalshaped but also “spherical” in its 3-dimensional nature (not flat or plaque-like)
• Completely surrounded by lung parenchymaand not associated with adenopathy,atelectasis, or pneumonia
B R Trotter, MD Scott & White Healthcare

Background: Pulmonary Nodules
• May be solitary (SPN) or multiple, whichaffects likelihood of various differentialdiagnostic considerations
• When multiple, imaging features of eachnodule identified must be considered , inaddition to consideration as a whole
• Although our discussion primarily relates tosolitary (or clearly dominant) pulmonarynodules, also useful in the setting of multiple
B R Trotter, MD Scott & White Healthcare

Background: Pulmonary Nodules
• Very common imaging finding, particularlysince advent of helical and multidetector CT
• Studies report prevalence of one or morenodules from 8% to 69% on CT
• Vast majority are benign (95%-98% in moststudies)
B R Trotter, MD Scott & White Healthcare

Background: Pulmonary Nodules
• Idealistic goals of imaging:
– Definitively identify all malignant nodules, andthereby beneficially affect patient outcomes
– Definitively identify all benign nodules, andthereby avoid the morbidity and cost of invasiveprocedures or further imaging that provide notrue benefit
• Disappointingly, this remains elusive despiteextensive experience and research
B R Trotter, MD Scott & White Healthcare

Background: Pulmonary Nodules
• Realistic goal of imaging of pulmonarynodules:
– Determine which are benign and need no furtherevaluation
– Determine which are suspicious for malignancyand refer for definitive resolution
– For nodules that remain indeterminate:
• Determine which require biopsy
• Determine which require follow-up
B R Trotter, MD Scott & White Healthcare

Background: Lung Cancer
• Our discussion of pulmonary nodulesultimately falls within the context of lungcancer, which directly influences ourmanagement decisions regarding nodules
• A few points are worth noting for ourdiscussion …
B R Trotter, MD Scott & White Healthcare

Background: Lung Cancer
• It is, overall, an aggressive disease:
– “More people in the United States die from lungcancer than from any other type of cancer. This istrue for both men and women.”
– In the United States in 2008:
• 208,493 diagnosed with lung cancer
• 158,592 died from lung cancer
• Although, incidence and death has more recently beendeclining following a trend of decreasing smoking
B R Trotter, MD Scott & White Healthcare
Background: Lung Cancer
• It is a costly disease:
– Estimated impact on U. S. economy is over $300billion annually
– Management decisions should includeconsideration of cost effectiveness that is, asmuch as possible, based on proven clinicaloutcomes research
B R Trotter, MD Scott & White Healthcare

Background: Lung Cancer
• There are known risk factors:
– Smoking:
• Accounts for 90% of lung cancers in the U. S.
• 15x to 30x more likely to develop or die from lungcancer than nonsmokers
• Risk increases with degree and duration (pack years)
• Currently estimated 94 million current or formersmokers in the U. S. at increased risk
B R Trotter, MD Scott & White Healthcare

Background: Lung Cancer
• Other known risk factors include:– Second hand smoke
– Asbestos, radon, or uranium exposure
– Radiation therapy to the thorax, such as withlymphoma or breast cancer
– Family history of lung cancer in 1st degree relative
– Age: risk increases with age; rare under age 35
– Chronic lung diseases
– Personal history of prior lung cancer
B R Trotter, MD Scott & White Healthcare
Background: Lung Cancer
• It is a heterogeneous disease:
– Non-small cell lung cancer (NSCLC)
• 80%-85% of lung cancer
• Squamous cell, Adenocarcinoma, Large-cell, other
• 5 year survival 50%-70% stage IA to 2% stage IV
• Can be detected at earlier stages with CT (NLST: 30%-75% stage 1A depending on type of NSCLC)
• Role of screening with CT to detect at earlier stage?
• The primary focus when discussing imaging ofpulmonary nodules
B R Trotter, MD Scott & White Healthcare

Background: Lung Cancer
• It is a heterogeneous disease:
– SCLC
• 15%-20% of lung cancers
• 5 year survival 20% limited-stage to <1% extensive-stage
• Unlikely detection when limited-stage due to itsaggressive nature
• Screening with CT less likely to impact outcome (NLST:86% stage III-IV)
B R Trotter, MD Scott & White Healthcare

Review of Imaging Modalities:Tools of the Trade
B R Trotter, MD Scott & White Healthcare

Review of Imaging Modalities:Pulmonary Nodules
• Chest radiograph (CXR)
• Computed Tomography (CT)
• Positron Emission Tomography (PET)
• PET-CT (no, it’s not the same thing)
• (Flouroscopy, MRI, US)
B R Trotter, MD Scott & White Healthcare

Review of Imaging Modalities:Chest Radiograph
• Low cost
• Low radiation exposure
• Low utility as primary imaging modality ofpulmonary nodules
• No utility for lung cancer screening
B R Trotter, MD Scott & White Healthcare
Review of Imaging Modalities:Chest Radiograph
• However, CXR is a common entry point intothe evaluation of pulmonary nodules whendetected incidentally
• Prevalence of nodules on CXR is about 0.2% to9% depending on population
B R Trotter, MD Scott & White Healthcare

Review of Imaging Modalities:Computed Tomography
• Tomographs (slices) eliminate the problem ofsuperimposed structures on radiographs
• Volumetric data acquisition on modern scannersallows slice reconstruction in any plane
• Highly sensitive for detection of pulmonarynodules as small as 1-2 mm
• Unfortunately limited specificity
• Can be performed with or without IV contrastenhancement
B R Trotter, MD Scott & White Healthcare

Review of Imaging Modalities:Computed Tomography
• High spatial and contrast resolution allowdetermination of important morphologicfeatures of nodules
• Thin-sections (1-3 mm slice thickness) shouldbe utilized for evaluation of nodulemorphology (IV contrast unnecessary)
B R Trotter, MD Scott & White Healthcare

Review of Imaging Modalities:Computed Tomography
• IV contrast-enhanced densitometry can beperformed to assess nodule enhancementcharacteristics
• More accurate determination of importantancillary findings: adenopathy, bronchialinvolvement, pleural involvement, etc.
• Low-dose (radiation) imaging may be used forany needed follow-up exams (or screening)
B R Trotter, MD Scott & White Healthcare

Review of Imaging Modalities:Positron Emission Tomography
• IV administration of 18F-fluorodeoxyglucose(FDG)
• Degree of tissue uptake reflects its relativemetabolic activity (glucose)
• Many malignancies demonstrate significantlygreater uptake of FDG compared with normaltissues and appear “hot” on PET images
• >90% sensitivity for nodules 1-3 cm; lowerspecificity is about 80%
B R Trotter, MD Scott & White Healthcare

Review of Imaging Modalities:PET-CT
• It’s like Reese’s Peanut Butter Cups
• It’s a PET scan with an anatomic contrastagent
• It’s a CT scan with a metabolic contrast agent
• Either way, combines benefits of bothmodalities with higher sensitivity andspecificity than for either PET or CT alone
• Reimbursement? (CMS <4 cm; confirm local)
B R Trotter, MD Scott & White Healthcare

Review of Imaging Modalities:Other
• Flouroscopy:
– Biopsy guidance
– Can be used as an inexpensive problem solving tool
• MRI has little role in imaging of pulmonarynodules but has utility in the evaluation ofthoracic malignancies
• Ultrasound has little role in imaging of pulmonarynodules although may occasionally be used forbiopsy localization
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:“To benign or not to benign,
that is the question.”
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:“To benign or not to benign …”
While there are a few imaging features thatallow for a confidant diagnosis of a benignpulmonary nodule, there are none that arediagnostic of malignancy
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Benign
• Benign pattern of calcification
• Stability of size
• Presence of fat
• (Keep in mind the definition of a pulmonarynodule)
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Benign
• Benign patterns of calcification in a smoothlymarginated nodule (or smoothly lobulated ifhamartoma):
– Diffuse (granuloma)
– Central (granuloma)
– Laminated or concentric (granuloma)
– Popcorn (hamartoma)
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Benign
• Any other pattern of calcification isindeterminate
• “Caveat”: patients with history of bonemalignancy may have calcified nodules thatresemble benign granulomas
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Benign
• Stability of size:– Comparison with older exams is essential in
evaluation of pulmonary nodules (retrospect?)
– 2 years of stability widely accepted as consistentwith benign etiology and standard of care
– 2 years based on studies of volume doubling-timeof benign and malignant lesions:
• 30-480 days typical of malignant nodules
• Median about 160-180 days for malignant nodules
• However, reported range is actually quite broad
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Benign
• CT 2004 • CT 2012
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Benign
• Stability of size:
– Caveat: non-solid (ground-glass opacity) nodulesthat are malignant are more likely to havesignificantly longer doubling times and should befollowed longer (3+ years)
– Measurement accuracy is critical
– For “spherical” structures, diameter increase ofonly 26% is a doubling of volume: Equates tomere 1 mm diameter increase for a 4mm nodule!
B R Trotter, MD Scott & White Healthcare
Review of Imaging Features:Benign
• Stability of size:
– Especially for smaller nodules, visual comparisonhas been shown inaccurate, and physicalmeasurement should be performed
– Measurement most accurate on soft-copy imageswith electronic calipers
– Any enlargement compared with baselinemeasurement considered suspicious and shouldprompt further evaluation
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Benign
• Stability of size:
– Automated volumetric analysis software haspromise to allow for more precise determinationof nodule growth
– Caution: cancers may occasionally demonstratetemporary decrease of overall size—a single studydemonstrating decrease of size may not beadequate to confirm a benign etiology
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Benign
• Presence of fat:– Within a smooth or smoothly lobulated SPN
essentially diagnostic of hamartoma
– Present in approximately 60%
• Caution: be certain the lesion contains fat asartifact from volume averaging may mimic
• “Caveat”: metastases from liposarcoma andrenal cell carcinoma may occasionally containfat
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Benign
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Probably Benign
• Other probably benign imaging findings:
– FDG PET standardized uptake value (SUV)<2.5
– Clustered nodules
– Very small size (<4 mm <<1%)
– Concave margins
• Follow-up CT imaging
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Mimics
• Additional benign pulmonary imaging findingsmay mimic a nodule (experience…or cojones):– Arteriovenous malformation—feeding and
draining vessels
– Mucocele—tubular branching mucus filled dilatedbronchi
– Rounded atelectasis—comet tail appearance andassociated with pleural thickening
– Flat lesions—scarring that may be appreciatedwith multiplanar imaging
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Mimics
• Rounded atelectasis • Flat lesion/scar
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Mimics
• Mucocele • Mucocele
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Suspicious for Malignancy
• Larger size: as size approaches 3 cm,likelihood of malignancy approaches 90%
• Spiculated margin: approximately 90%predictive value for cancer
• Lobulated margin more suspicious thansmooth
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Suspicious for Malignancy
• Non-solid attenuation or ground-glass opacity(GGO) in part or entirety:
– 34%-43% of GGO nodules cancer
– 40%-50% of partial-solid nodules <1.5 cm cancerand increases further with increasing size
• Cavitation with thick walls:
– 84%-95% cancer if wall thickness >16 mm
– 95% benign when wall thickness <4 mm
B R Trotter, MD Scott & White Healthcare
Review of Imaging Features:Suspicious for Malignancy
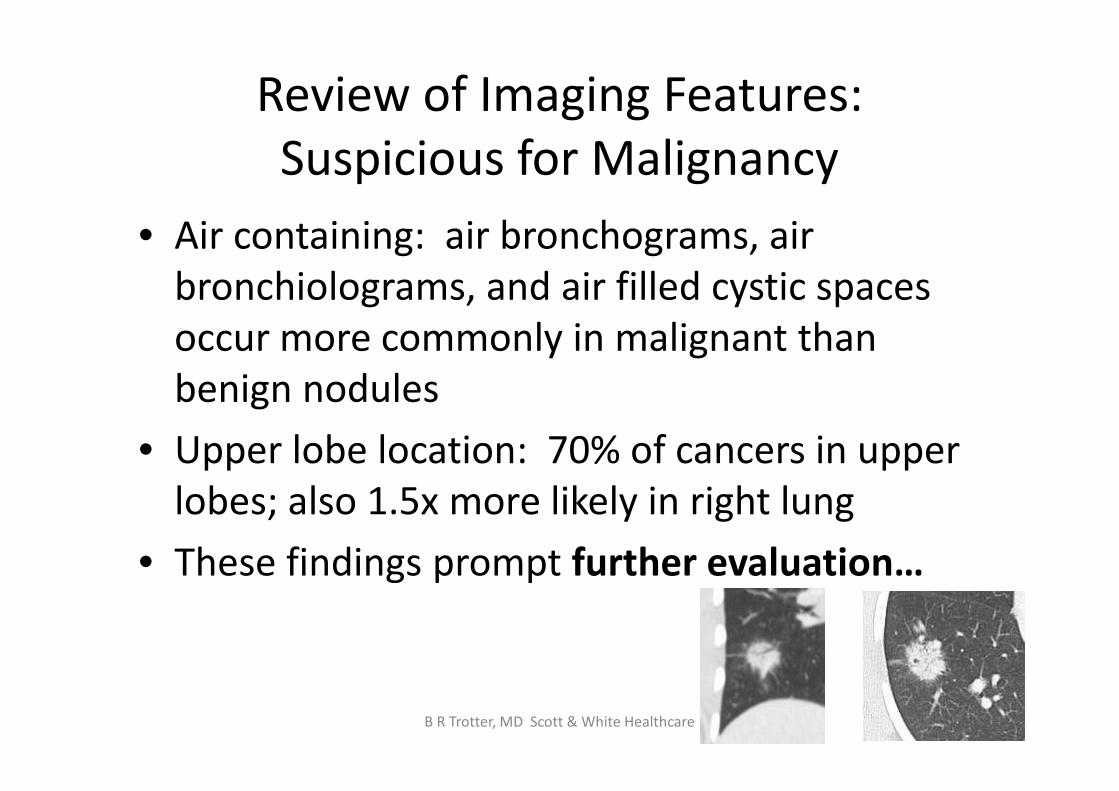
• Air containing: air bronchograms, airbronchiolograms, and air filled cystic spacesoccur more commonly in malignant thanbenign nodules
• Upper lobe location: 70% of cancers in upperlobes; also 1.5x more likely in right lung
• These findings prompt further evaluation…
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Further Evaluation
• FDG PET-CT
– Usable for nodules >8-10 mm diameter
– Because volume averaging from motion canartificially decrease apparent FDG activity, may beless useful for nodules located near diaphragm orheart, especially if small
B R Trotter, MD Scott & White Healthcare
Review of Imaging Features:Further Evaluation
• FDG PET-CT
– Much more reliable for solid than GGO nodules:
• >90% sensitivity for cancer in solid nodules (withexception of carcinoid tumor—probably 50%)
• Probably <50% sensitive for purely GGO cancers such asadenocarcinoma in situ (formerly BAC)
– Result determined by degree of activity in nodulerelative to other body structures:
• Subjective visual evaluation
• Quantitative evaluation (SUV 2.5)
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Further Evaluation
• Solid nodule • GGO nodule
B R Trotter, MD Scott & White Healthcare
Review of Imaging Features:Further Evaluation
• FDG PET-CT
– Excellent test when used appropriately butprobably a tendency for overutilization
– Questions to consider:
• Is it uncertain whether to simply watch and wait or toproceed with biopsy/resection? If yes then…
• Will the PET result determine whether or not toproceed with biopsy/resection? If yes then…
• Proceed with PET imaging
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Further Evaluation
• FDG PET-CT
– Most useful and cost effective when:
• Low to moderate (5%-60%) pre-test probability ofmalignancy
• Clinical risk assessment and nodule morphologiccharacteristics are discordant
• Indeterminate nodule in a high risk patient
– May be useful in other situations but can be anunnecessary and added expense—be judicious
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Further Evaluation
• FDG PET-CT
– If very low (<5%) likelihood of malignancy, PET isnot needed to justify observation (watch and wait)with follow-up CTs
– If high (>60%) likelihood of malignancy, PET is notneeded to justify biopsy/resection
– Important: All PET negative nodules should beobserved with follow-up CTs to confirm stabilityfor at least 2 years: If grow, biopsy
B R Trotter, MD Scott & White Healthcare

Review of Imaging Features:Further Evaluation
• Contrast Enhanced CT Densitometry:
– Usable for nodules at least 10 mm diameterwithout cavitation or central necrosis
– Compare baseline unenhanced attenuation withpeak contrast-enhanced attenuation
– <15 Hounsfield units (HU) enhancement isessentially diagnostic of benign etiology (99%)
– >15 HU is nonspecific
– “Ask your doctor if this test is right for you…”
B R Trotter, MD Scott & White Healthcare

Likelihood of Malignancy:“…damned lies, and statistics”
B R Trotter, MD Scott & White Healthcare

Likelihood of Malignancy
• Determining the statistical probability ofmalignancy for a given nodule is essential toproper management, including decisionsregarding imaging studies
– Qualitatively by an experienced clinician—there isprobably a tendency to overestimate theprobability of malignancy in low risk patients
– Quantitatively with mathematical model
B R Trotter, MD Scott & White Healthcare

Likelihood of Malignancy:Logistic Regression Model
• Mayo clinic study using multiple logisticregression analysis identified 6 independentpredictors, 3 clinical and 3 imaging related:
– Age, smoking, and history of prior extrathoraciccancer more than 5 years earlier
– Nodule diameter, spiculated margin, and upperlobe location
B R Trotter, MD Scott & White Healthcare

Likelihood of Malignancy:Logistic Regression Model
• Probability of Malignancy = eˣ/(1+eˣ)
– Where x = -6.872 + (0.0391 x Years of age)
+ (0.1274 x Diameter in mm)
+ 0.7917 if smoker
+ 1.3388 if prior extrathoracic cancer >5 years ago
+ 1.0407 if spiculated margin
+ 0.7838 if upper lobe
B R Trotter, MD Scott & White Healthcare

Likelihood of Malignancy:Logistic Regression Model
• 40 year old, nonsmoker, no prior malignancy,with a 5 mm smoothly marginated nodule in alower lobe: Probability of malignancy = 0.9%
• 65 year old, smoker, no prior malignancy, witha 15 mm spiculated nodule in an upper lobe:Probability of malignancy = 55%
• 70 year old, smoker, no prior malignancy, witha 25 mm spiculated nodule in an upper lobe:Probability of malignancy = 87%
B R Trotter, MD Scott & White Healthcare
Likelihood of Malignancy:Bayesian Analysis
• Uses validated likelihood ratios for variousindependent clinical and imaging variables toestimate the probability of malignancy
• Based on Bayes Theorem:
New odds = Prior odds x Likelihood Ratio
• Likelihood ratios >1 increase the probability ofmalignancy while ratios <1 lower it
B R Trotter, MD Scott & White Healthcare

Likelihood of Malignancy:Bayesian Analysis
• Clinical variables increasing probability:
– Age >50 years
– Smoking history ≥30 pack years
– Hemoptysis
– History of prior malignancy
B R Trotter, MD Scott & White Healthcare

Likelihood of Malignancy:Bayesian Analysis
• Imaging variables increasing probability:
– Diameter >2.0 cm
– Upper or middle lobe location
– Spiculated margin
– Thick walled cavitation
– Absence of calcification
– FDG PET SUV >2.5
– CT densitometry enhancement >15 HU
B R Trotter, MD Scott & White Healthcare

Likelihood of Malignancy:“SPN Calculator”
• An easily accessible and useable “SPNCalculator” with both the Bayesian analysisand logistic regression models can be foundon the web at
www.chestx-ray.com/SPN/SPNProb.html
• Extremely cool so check it out
B R Trotter, MD Scott & White Healthcare


Recommendations:Putting It Together
B R Trotter, MD Scott & White Healthcare

Recommendations:
• Clinical management of an imaging finding
• Distill the clinical and imaging variables andformulate a plan of action that is broadlyapplicable and adheres to the standard of care
B R Trotter, MD Scott & White Healthcare

Recommendations:
• First things first:– Comparison with old imaging studies cannot be
overemphasized! (Turn on the retrospectoscope)• May obviate need for any further expensive and
potentially harmful evaluation. Team effort of clinician,radiologist, and patient.
• In general, clearly growing nodules should move totissue diagnosis if not contraindicated
– If suspected infectious etiology, further diagnosticintervention, therapy, and short-term follow-upimaging best initial management
B R Trotter, MD Scott & White Healthcare

Recommendations:
• Breaks down into two categories:
– Management of small nodules ≤8-10 mm
– Management of larger nodules >8-10 mm
B R Trotter, MD Scott & White Healthcare

Small Nodules ≤8-10 mm
B R Trotter, MD Scott & White Healthcare

Recommendations:Small Nodules ≤8-10 mm
• Fleischner Society guidelines for managementof small nodules have been widely adopted
• Apply to:
– Incidentally detected nodules on CT
– Patients 35 years of age and older
• Do not apply to:
– Patient with known or suspected malignancy
– Patient with unexplained fever
B R Trotter, MD Scott & White Healthcare

Recommendations:Small Nodules ≤8-10 mm
MacMahon H, et al. Guidelines for management of small pulmonary nodules detected on CT scans: a statement from the FleischnerSociety. Radiology 2005; 237: 395-400

Recommendations:Small Nodules ≤8-10 mm
• A few key rationales for FSG:
– Differing follow-up times for low and high riskcategories because malignant nodules generallygrow faster in smokers
– Even in smokers, <1% of nodules <4 mm willbecome lethal cancers, but this increases to 10%-20% for size about 8 mm
B R Trotter, MD Scott & White Healthcare

Recommendations:Small Nodules ≤8-10 mm
• A few points regarding Fleischner SocietyGuidelines (FSG):
– Are about managing nodules ≤8 mm and not meant to define management of larger nodules—FSG clearly indicate flexibility in this category
– Note that FSG do not distinguish between singleand multiple nodules
– Diameter is average of length and width
– Remember longer follow-up of GGO nodules
B R Trotter, MD Scott & White Healthcare

Recommendations:Small Nodules ≤8-10 mm
• Other groups:
– Patients <35 years:
• In general, follow-up CT imaging should be avoided
• Consider a 6-12 month follow-up CT if have knownmalignancy
– Patients with known or suspected malignancy falloutside of the FSG (not part of the “high risk”group) and should be managed according to thespecific clinical situation and/or protocol
B R Trotter, MD Scott & White Healthcare

Recommendations:Small Nodules ≤8-10 mm
• Additional considerations:
– For nodules detected incidentally on non-thoraxCT and lungs not completely evaluated, considerobtaining dedicated CT thorax to assess for anyother nodules (no consensus)
– CT image reconstruction should be contiguousslices with thickness ≤3 mm, or potentially losing important morphologic information
– Consider limited coverage on follow-up CTs
B R Trotter, MD Scott & White Healthcare

Larger Nodules >8-10 mm
B R Trotter, MD Scott & White Healthcare

Recommendations:Larger Nodules >8-10 mm
• Morphologic characterization with thin-section CT is the key imaging step:
– Diagnostic benign features?
– If not, detailed accounting of morphology
• Determining probability of malignancy is thekey clinical step
– Accounting of relevant clinical history
– Estimate or calculate probability
B R Trotter, MD Scott & White Healthcare
Recommendations:Larger Nodules >8-10 mm
• More diagnostic options become feasible withlarger nodules:
– Advanced imaging with FDG PET or contrastenhanced CT densitometry
– Percutaneous needle biopsy or bronchoscopy
• Many management algorithms in theliterature—most are very similar
• Best integrate clinical and imaging variables
B R Trotter, MD Scott & White Healthcare

A management algorithm for patients with SPNs >8 mm and <30 mm in diameter.
Adapted from: Evaluation of patients with pulmonary nodules: when is it lung cancer?, ACCP evidence-based clinical practice guidelines (2nd ed.). Chest 2007; 132: 108S-130S

Recommendations:Larger Nodules >8-10 mm
• “Ask your doctor if this test is right for you…”
• Details of application depend on availablelocal resources, expertise, and the wishes ofthe fully informed patient
B R Trotter, MD Scott & White Healthcare

Thank you for your attention
B R Trotter, MD Scott & White Healthcare

Resources
• cdc.gov• Chestx-ray.com• Gould MK, et al. Evaluation of patients with pulmonary nodules: when is it
lung cancer?, ACCP evidence-based clinical practice guidelines (2nd ed.). Chest2007; 132: 108S-130S
• MacMahon H, et al. Guidelines for management of small pulmonary nodulesdetected on CT scans: a statement from the Fleischner Society. Radiology2005; 237: 395-400
• NLST Research Team. Reduced lung cancer mortality with low-dose computedtomographic screening. N Engl J Med 2011; 365: 395-409
• Winer-Muram HT. The solitary pulmonary nodule. Radiology 2006; 239: 34-49
• Nicholas E, et al. Evaluation of the solitary pulmonary nodule: A practicalapproach. Applied Radiology 2010. Vol 40, No 12: 6-15
• Swenson SJ, et al. The probability of malignancy in solitary pulmonarynodules: application to small radiologically indeterminate nodules. ArchIntern Med 1997; 157: 849-855
B R Trotter, MD Scott & White Healthcare