imaging of the patient with obstructive jaundice arye blachar md department of radiology tel aviv...
TRANSCRIPT

Imaging of the patient with Imaging of the patient with obstructive jaundiceobstructive jaundice
Arye Blachar MDArye Blachar MD
Department of RadiologyDepartment of Radiology
Tel Aviv Sourasky Medical CenterTel Aviv Sourasky Medical Center

IntroductionIntroduction
• Cholestasis: Clinical and biochemical syndrome, results when bile flow is impaired.
• Impairment of bile flow- hepatic cell bile canaliculus ampula of vater
• Intra hepatic: hepatitis, drug toxicity, alcoholic liver disease, PBC, PSC, metastatic carcinoma, CholangioCA, etc
• Extra hepatic: Pancreatic tumor, ampulary tumor, CholangioCA, biliary stone disease, pancreatitis, pancreatic pseudocyst, PD stricture

Extra-hepatic cholestasis: Extra-hepatic cholestasis: Pancreatic tumorPancreatic tumor
• Malignant tumor arising from epithelium of exocrine pancreas
• 5th leading cause of death
• Risk: smoking, diabetes, chr. Pancreatitis, high fat diet
• Mean age: 55 yrs, peak 7th decade, m:f-2:1
• Presentation: head: jaundice, pain, weight loss; body tail: weight loss. Mets to liver

Extra-hepatic cholestasis: Extra-hepatic cholestasis: Pancreatic tumorPancreatic tumor - location - location
• Head* – 60-70%- causes jaundice
• Body** – 20%
• Tail** –10%
• Diffuse involvement – 5-10%
* Average diameter 2.5-3.0 cm
** Average diameter 5.0-7.0 cm

Extra-hepatic cholestasis: Extra-hepatic cholestasis: Pancreatic tumor Pancreatic tumor imagingimaging
Helping the General Surgeon:
• Is there a pancreatic tumor?
• What is the tumor type?
• Is the tumor resectable?
• Are there any significant anatomical variants?

Extra-hepatic cholestasis: Extra-hepatic cholestasis: Pancreatic tumorPancreatic tumor Imaging - TechniqueImaging - Technique
• Pure water or milk 4%
• Non-ionic contrast 120- 150cc at 4-5cc/sec
• Thin slices
• Arterial phase: 25sec after the start of inj.
• “Pancreatic phase”: 40-50sec after start of inj.
• “Liver phase”: 70sec after the start of inj.

Extra-hepatic cholestasis: Extra-hepatic cholestasis: Pancreatic tumorPancreatic tumor Imaging - TechniqueImaging - Technique
Multi plannar reformats, 3D imaging and review on a workstation are very helpful:
• Improved tumor conspicuity
• Improved depiction of PD and CBD
• Better delineation of vascular anatomy
Raptopoulos et al, Radiology 1998; 207:317-324
Nino Murcia et al, AJR 2001; 176:689-693
Prokesch et al, Radiology 2002; 225:759-765
Extra-hepatic cholestasis: Extra-hepatic cholestasis: Pancreatic tumorPancreatic tumor - - Tumor DetectionTumor Detection
• Focal enlargement of the gland
• Hypodense mass on enhanced CT
Secondary signs:
• Mass effect or convex contour abnormality
• Atrophic distal pancreatic parenchyma
• Dilatation of CBD and MPD in the absence of obstructive calculus (interupted duct sign)

Extra-hepatic cholestasis: Extra-hepatic cholestasis: Pancreatic tumorPancreatic tumor - Unresectability - Unresectability
• Vascular invasion
• Invasion of adjacent organs:
– Stomach, spleen, left adrenal, mesentery
• Distal metastasis:
– Liver (30%), regional LN, omentum, ascites (10%), lungs, pleura, bone

Extra-hepatic cholestasis: Extra-hepatic cholestasis: Pancreatic tumorPancreatic tumor - - Unresectability vascular invasionUnresectability vascular invasion
Involvement of SMA, Celiac, SMV, PV or SV (isolated focal SV or PV?)
• Axial images: CT grading of circumferential tumor-vessel contiguity (>50%) [sen-84%, spec-98%] Lu et al AJR 1997; 168:1439-1443
• MPR/3D/CTA images: Evaluate change in vessel caliber or occlusion
Raptopoulos et al AJR 1997; 168:971-977
Prokesch et al, Radiology 2002; 225:759-765

Extra-hepatic cholestasis: Extra-hepatic cholestasis: Pancreatic tumorPancreatic tumor – – Unresectability- Unresectability- Mets
Hepatic Metastases
• Hypovascular best seen on PVP
• Sensitivity for detection of mets >1cm ~90%
• Overall sensitivity for mets- 75%
• Even small <5mm mets may be detected
LN mets- CT not accurate
• >10mm sensitivity 14%, specificity 85% PPV 17% Roche ET AL, AJR 2003;180:475-480

Extra-hepatic cholestasis: Extra-hepatic cholestasis: Pancreatic tumorPancreatic tumor - Imaging - How good are we? - Imaging - How good are we?
• Accuracy of tumor detection 80-91% using older dynamic scanners. Accuracy with MDCT 95-96%. Overall CT staging accuracy 90%
• PPV for surgical unresectability 89%-100% but PPV for resectability up to 80%
• Poor performance in detecting: small hepatic metastases, small peritoneal implants, LN mets in normal size LN

Pancreatic cancer staging – Pancreatic cancer staging – PET CTPET CT
• PET – not yet widely used for pancreatic cancer staging, though promising results are being reported.
• FDG-PET is a very useful tool in diagnosing pancreatic cancer. FDG-PET may be also used as an adjunct for determining the treatment modality of pancreatic cancer and evaluating tumor response to therapy .J Clin Gastroenterol. 2006 Nov-Dec;40(10):923-9

Pancreatic cancer staging – PET CTPancreatic cancer staging – PET CT
• PET – not yet widely used for pancreatic cancer staging, though promising results are being reported.
• FDG-PET is a very useful tool in diagnosing pancreatic cancer. FDG-PET may be also used as an adjunct for determining the treatment modality of
pancreatic cancer and evaluating tumor response to therapy .J Clin Gastroenterol. 2006 Nov-Dec;40(10):923-9

Extra-hepatic cholestasis: Extra-hepatic cholestasis: Ampulary tumorAmpulary tumor
• Malignant epithelial tumor , ampula of vater
• Presents with jaundice, weight loss. Abd or back pain
• Age: mean 65 yrs, no sex predeliction
• Prognosis: depends on nodeal status and differentiation of tu, better than panc ca
5 yrs- 38% if resected
Treatment: Whipple if pos.

Extra-hepatic cholestasis: Extra-hepatic cholestasis: Ampulary tumorAmpulary tumor
• Imaging:
– Lobulated soft tissue mass at ampula
– “Double duct” sign
– CT: Hypodense mass , distention of du helpful

Extra-hepatic cholestasis: Extra-hepatic cholestasis: CholangiocarcinomaCholangiocarcinoma
• Cholangio-cellular carcinoma, arises from the IHBD or EHBD epithelium
• 2ND most common primary hep tumor
• Types:
– Intra-hepatic- peripheral (exophytic, polypoid, infiltrative)
– Intra-hepatic central or hilar
– Extra hepatic originates from CBD as stricture or mass

Extra-hepatic cholestasis: Extra-hepatic cholestasis: CholangiocarcinomaCholangiocarcinoma
• Age: 6-7th decade, M:F-3:2
• Risk: biliary lithiasis, clonorchiasis, rec. pyogenic infections, PSC, IBD, caroli disease, choledochal cyst, thorotrast exposure, BD papilomatosis,alfa-1 anti-tripsin
• Presentation: by location,jaundice, weight loss, abd pain, palpable mass
• Treat: surgical resection (<20%), radiation, chemo, stenting
• Prognosis: poor extra(1.6% 5yrs), intra (30%)
Extra-hepatic cholestasis: Extra-hepatic cholestasis: CholangiocarcinomaCholangiocarcinoma
• US: dilated BD, mass hyperechogenic(75%)
• CT: hypodense mass, IHBD dilatation, rim enhancement with prog central patchy enhancement, persistent enhancement on delayed scan
Extra-hepatic cholestasis: Extra-hepatic cholestasis: Gallstone disease
• 15%-20% of the population
• Passage of gallstones through biliary system causes ----->
– Biliary colic
– Acute cholecystitis
– Choledocholithiasis
– Cholecystoenteric fistula

Biliary tree imaging modalities: Biliary tree imaging modalities: ERCP, MRCP,PTCERCP, MRCP,PTC
• CT and US are excellent for dilated ducts but not for assessing the entire tree.
• ERCP –contrast media is placed endoscopically through the biliary tree.

Biliary tree imaging modalities: Biliary tree imaging modalities: ERCP, MRCP, PTCERCP, MRCP, PTC
• MRCP –specific MR sequence is employed to demonstrate the biliary tree.
• No IV contrast and definitely no biliary cannulation involved.

Biliary tree imaging modalities: Biliary tree imaging modalities: ERCP, MRCP, PTCERCP, MRCP, PTC
• PTC – direct cannulation of the biliary tree, and iodinated contrast injection.
• Advantageous over MRCP for showing distal, small duct pathology and walls irregularity.

PTCPTC
Percutaneous access to
the biliary tree, through the
CBD, if possible, and into
the duodenum.
Downsides:
• External drainage
• Procedural risks:
– Coagulopathy
– ascites
Biliary stone disease - summaryBiliary stone disease - summary
• US is the modality of choice for demonstrating gallstones.
• US is the very good for demonstrating biliary ducts.
• CT will show biliary ducts, less reliable for filling defects. Good for neoplastic disease.
• MRCP is the non invasive study
• ERCP is invasive but potentially therapeutic.
• PTC even more invasive, when ERCP is limited.
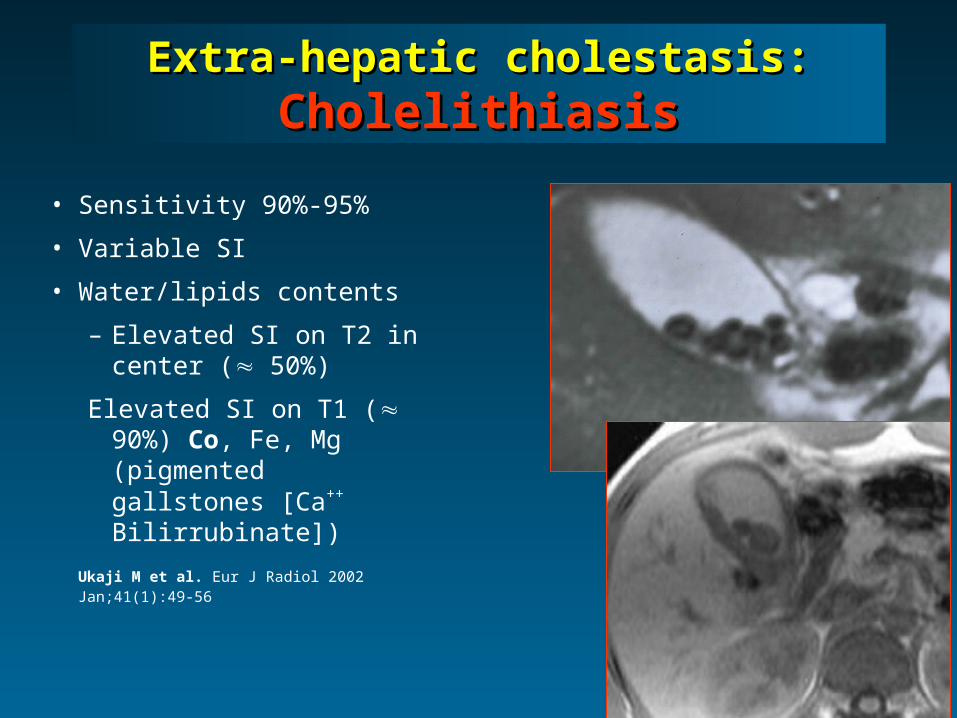
Extra-hepatic cholestasis: Extra-hepatic cholestasis: CholelithiasisCholelithiasis
• Sensitivity 90%-95%
• Variable SI
• Water/lipids contents
– Elevated SI on T2 in center ( 50%)
Elevated SI on T1 ( 90%) Co, Fe, Mg (pigmented gallstones [Ca++ Bilirrubinate])
Ukaji M et al. Eur J Radiol 2002 Jan;41(1):49-56

CholedocholithiasisCholedocholithiasis• Asymptomatic
• Symptoms: calculi in distal CBD (90%)• CBD stones
• 15% pts. with gallstones
• 15% pts. with acute cholecystitis• Diagnosis pre laparoscopic cholecystectomy
• ERCP
– Stones in only 27-50% of pts with clinical suspicion

Choledocholithiasis MRCholedocholithiasis MR
• Normal CBD
– 98% of the pts
– Foci of low SI surrounded by bright bile (T2-WI)
• Stones 2 mm
• CBD stones
– Sensitivity 85-100%
– Specificity 90-99%
– Accuracy 89-97%
– PPV 77-93%
– NPV 94-100%