immumed, inc.© 2009 - 2015 1 passive immunity for hiv ** adjuvant therapy for slowing worldwide...
TRANSCRIPT

ImmuMed, Inc.© 2009 - 2015 1
PASSIVE IMMUNITY FOR HIV **
Adjuvant Therapy for Slowing Worldwide AIDS Epidemic
No Treatment Due to Drug Availability / Expense
Supplements Antiretroviral Drugs To Reduce Viral Load in:
Antiretroviral Treatment Failures
Patient Non-compliance in Taking Medication
Viron mutation or development of drug resistance
** See Definitions

ImmuMed, Inc.© 2009 - 2015 2
GLOBAL HIV ESTIMATES
Adults and Children Living with AidsDecember 2011
34.0 million [ 31.4 – 35.9 million ]
2.5 million [2.2 – 2.8 million]
1.7 million [1.5 – 1.9 million]
People living with HIV
New HIV infections in 2011
Deaths due to AIDS in 2012
UN AIDS.ORG 2011 Annual Report
ImmuMed, Inc.© 2009 - 2015 3
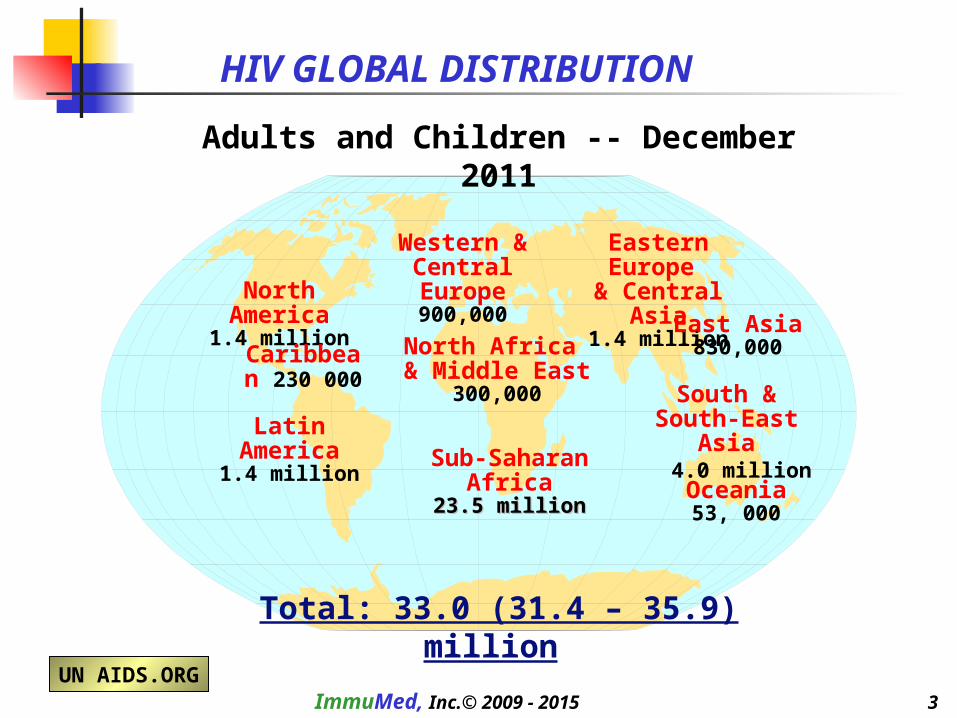
HIV GLOBAL DISTRIBUTION
North America1.4 million
Western & Central Europe
900,000
North Africa & Middle East
300,000
Sub-Saharan Africa23.5 million23.5 million
Eastern Europe & Central Asia
1.4 million
South & South-East Asia
4.0 million
Caribbean 230 000
Oceania53, 000
Latin America1.4 million
East Asia830,000
Adults and Children -- December 2011
Total: 33.0 (31.4 – 35.9) million
UN AIDS.ORG
ImmuMed, Inc.© 2009 - 2015 4
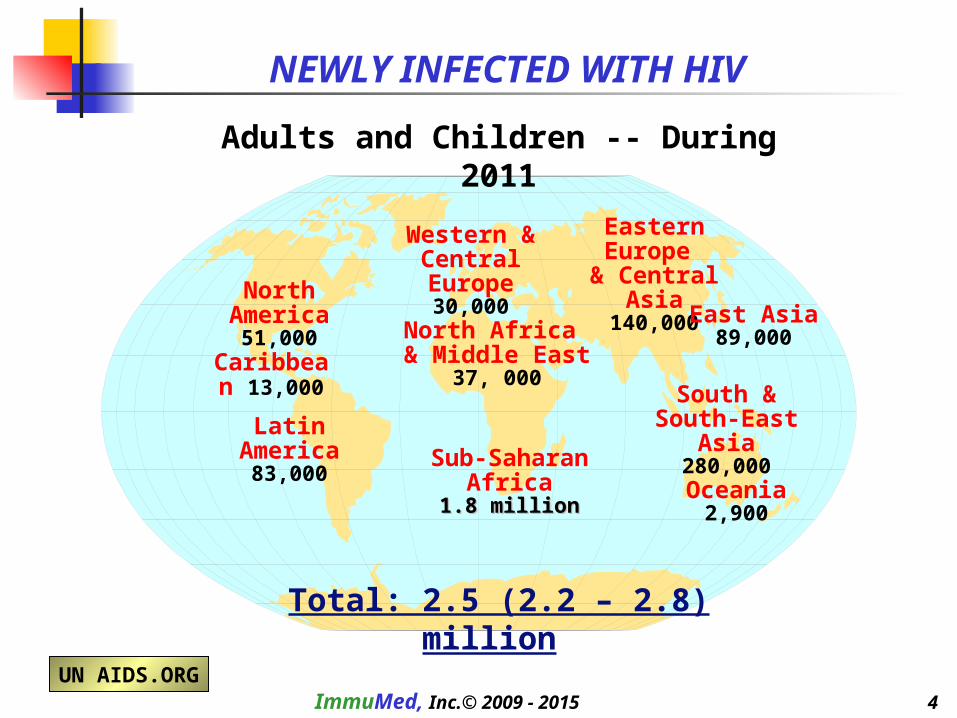
North America51,000
Western & Central Europe
30,000
North Africa & Middle East
37, 000
Sub-Saharan Africa1.8 million1.8 million
Eastern Europe & Central Asia
140,000
South & South-East Asia
280,000
Caribbean 13,000
Oceania2,900
Latin America83,000
East Asia89,000
UN AIDS.ORG
Adults and Children -- During 2011
NEWLY INFECTED WITH HIV
Total: 2.5 (2.2 – 2.8) million

ImmuMed, Inc.© 2009 - 2015 5
ESTIMATED DEATHS FROM AIDS
Adults and Children -- 2011
North America21,000
Western & Central Europe
7,000
North Africa & Middle East
23,000
Sub-Saharan Africa1.2 million1.2 million
Eastern Europe & Central Asia
92,000
South & South-East Asia
250,000
Caribbean 10,000
Oceania1,300
Latin America54000
East Asia59,000
UN AIDS.ORG Total: 1.7 (1.5 – 1.9) million

ImmuMed, Inc.© 2009 - 2015 6
North America11,000
Western & Central Europe
6,200
North Africa & Middle East
24, 000
Sub-Saharan Africa1.9 million1.9 million
Eastern Europe & Central Asia
8,800
South & South-East Asia
170,000
Caribbean 23,000
Oceania700
Latin America26,000
East Asia9,400
UN AIDS.ORG
CHILDREN LIVING WITH HIV (<15 YEARS)
Estimated as of -- December 2011
Total: 2.2 (2.0 – 2.6) million

ImmuMed, Inc.© 2009 - 2015 7
Adults and Children – 2010Incidence HIV per 100,000 population**
U.S. - DEMOGRAPHICS
**AidVu
ImmuMed, Inc.© 2009 - 2015 8
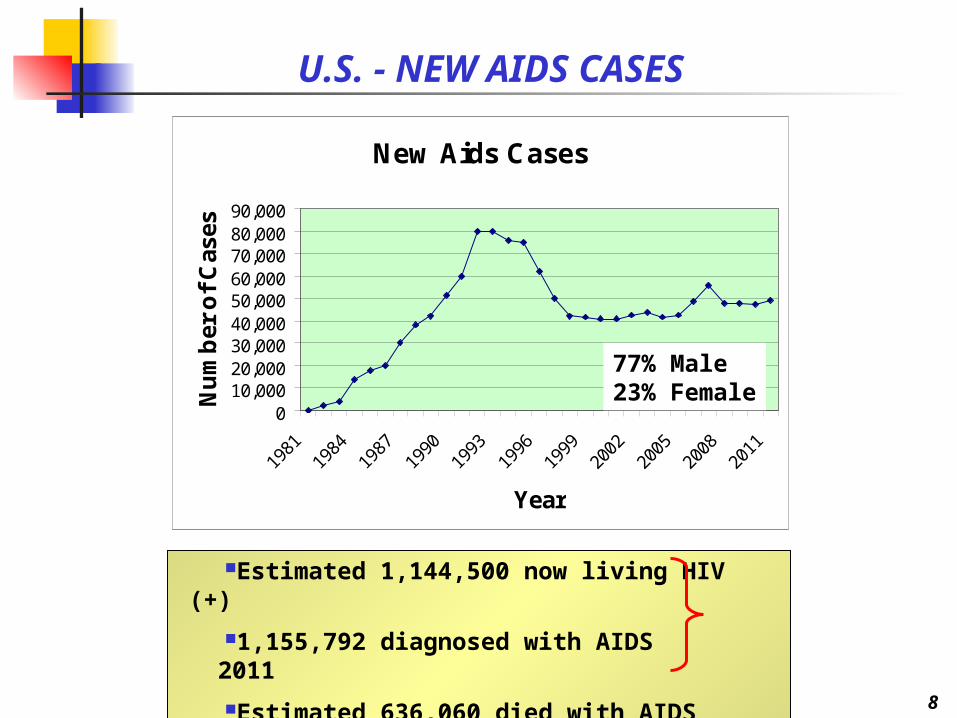
New Aids Cases
010,00020,00030,00040,00050,00060,00070,00080,00090,000
1981
1984
1987
1990
1993
1996
1999
2002
2005
2008
2011
Year
Nu
mb
er o
f C
ases
U.S. - NEW AIDS CASES
77% Male23% Female
Estimated 1,144,500 now living HIV (+)
1,155,792 diagnosed with AIDS 2011
Estimated 636,060 died with AIDS
ImmuMed, Inc.© 2009 - 2015 10
BUSINESS MODEL
As an established antibody company, intent is to apply for grants, donations and government programs to fund:
Validation of the clinical benefit of an antibody for controlling viral load when used as supplemental
passive immunity.To established the economic value of this clinical approachin the U.S. markets:
Extend this clinical therapy to under-served countries when economic support is available.
Extend ImmuMed’s protein (antibody) purification technology to the HIV market, manufacturing a supplemental antibody
product for economically controlling viral load in defined clinical circumstances.
Enhances revenue return from this technology.
ImmuMed, Inc.© 2009 - 2015 11
THERAPEUTIC RATIONAL **
Maintaining low viral loads is critical to the development of AIDS.
New agents evolve rapidly. AIDS patients less responsive to new agents after first being treated with older therapy.
Scientific literature documents antibody can reduce viral load toundetectable levels, delay onset of first AIDS event and reduce the cumulative number of such events. Monthly IM gamma globulin may be effective in supplementing control of viral load given patient nonadherence (approximately 47%).
Sustained antibody use and resistance has not been well documented.
Antibody use may forestall the need to administer antiretroviral
agents earlier. This effect needs further documentation.
** Bibliography on Request
Rapidly decreasing viral load may be important as rescue therapy in very ill patients
ImmuMed, Inc.© 2009 - 2015 12
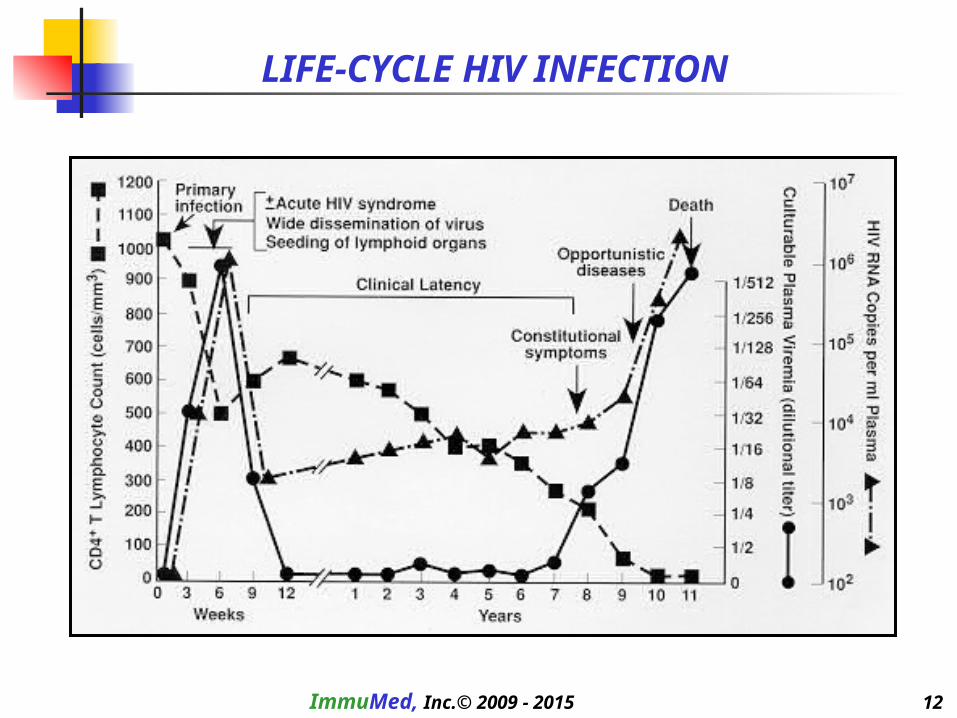
LIFE-CYCLE HIV INFECTION

ImmuMed, Inc.© 2009 - 2015 13
CD4 Count(cells/ml)
Three-year Probability of AIDS (%)
Viral Load
(RNA-1concentration [X 102 copies/ml])
PROGNOSIS FOR DEVELOPING AIDS
Importance of Controlling Viral Load
Decreasing Immunity
IncreasingInfection

ImmuMed, Inc.© 2009 - 2015 14
MARKET ASSUMPTIONS
Incidence of antiretroviral therapy in Africa and other epidemic areas:
15% treated, 85% untreated
Cumulative AIDS cases 1,919,970 less 27.30% deaths (524,060) equals U.S. AIDS treatment population: 435,925 plus HIV(+) carriers
Estimated U.S. HIV carrier population, 1.1 million; 959,985 in plasma pool.
New U.S. AIDS cases: Adults - 44,000 per year Children (<13 years) less than 100 per
yearAIDS deaths (U.S.) 16,000 = Pre-mortality rescue therapy opportunity
Treatment failures @ 15% of treated population
Antiretroviral therapy cost $900 per month (triple therapy) in U.S..
HIVIG antibody $200 per treatment (22% of antiretroviral therapy)Dosage of 1 gram HIVIG maintains therapeutic levels for at least 60 days

ImmuMed, Inc.© 2009 - 2015 15
POTENTIAL Rx OPPORTUNITIES
Treatment failures: optimally twelve treatments per year in a population of 65,000 patients
Pre-mortality rescue therapy: anticipating six treatments in 16,000 patients
U.S. Market First
Prevention: onset of AID symptoms, maintain CD4+ levels and delay
use of antiretroviral therapy. Occupational accidents:
Under-Served Countries
Same markets as above magnified by at least 10 X
Vertical transmission: infected mother to fetus or newborn700,000 live births annually in infected mothers
Hepatitis C patients not responding to therapy:

ImmuMed, Inc.© 2009 - 2015 16
U.S. ANNUAL REVENUE POTENTIAL
Population Assumptions:
Treated PopulationDeathsNewly Infected
Adults
431,998 15,944 44,100
Children
3,927 56 100
Total
435,92516,00044,200
TherapeuticIndication
Hepatitis C FailureOccupational AccidentTreatment FailuresPre-Morbid RescueDelay Antiretroviral
Total Revenue
Number of Treatments
------12 6 6
Cost Per Treatment
--- ---
$350$350
$350
% Population Treated
--- --- 65%95%50%
Potential Revenue
------
$178,511,288$31,920,000$46,410,000
$256,841,288
Under-Served Countries -- Market Potential 10 X U.S. Market

ImmuMed, Inc.© 2009 - 2015 17
COMPETITION
Processing disease-state plasma not widespread among validated manufacturers
Review of current FDA clinical trials does not reveal any ongoing passive immunity studies from among the 35 reported studies on the FDA web site.
Normal human immunglobulin is occasionally used for passive immunity in children. The Company is not aware of a specific HIV hyperimmune globulin product, although plasma collection companies, such as NABI have collected high-titer HIV plasma previously.

ImmuMed, Inc.© 2009 - 2015 18
REGULATORY
The FDA regulatory burden has not been established currently.
No licensed HIVIG product exists today
Clinical trials in foreign venues are becoming more prevalent.[1] A foreign clinical trial deemed to be shorter and more cost-effective.
[1] Fortune July 21, 2005
ImmuMed, Inc.© 2009 - 2015 19
MANUFACTURING
Validation of viral removal and clearance of HIV and Hepatitis agents is establish as an integral part to manufacturing MALG.
With minor modifications, technology is essentially established because equine plasma for MALG is considered and treated asa disease-state plasma.
First steps in MALG processing is sanitizing the plasma with respect to viral and bacterial contamination.
Purification of human plasma to gamma globulin will employ essentially the same processes used for MALG from equine plasma

ImmuMed, Inc.© 2009 - 2015 20
INTELLECTUAL PROPERTY
The Company believes that patented products may be derived from differential formulations specific to the composition direct
against the variety of HIV subtypes. This formulation is possible because
of chromatography techniques used in plasma purification. Thus, it isanticipated new patents can issue both from a composition (formulation) and manufacturing (methods) perspective.
There are two main subtypes of HIV virus, HIV-1 and HIV-2. At least six subtypes of HIV-1 have been described, designated HIV-1a through HIV-1f. Subtypes of HIV-2 also exist.
Data suggest that the majority of HIV-1 subtypes may be derived from independent recombinational events.
None established for HIVIG presently

ImmuMed, Inc.© 2009 - 2015 21
EXECUTION STRATEGY
A clinical trial design will be created during the period of plasma processing, and when approved (both manufacturing and trial design) by the FDA, the Company will execute its clinical trial.
Based on historic precedent and easily measured primary endpoints
(viral load and CD4 counts), the Company believes a late-stage trial can be initiated early.
Execution depends of financing.
Current plasmaphersis centers have established protocols for collecting disease-state plasma. They will be contracted to collect the requisite plasma volume.
The Company will establish plasma collection centers in world regions where HIV is prevalent, if and when HIVIG is marketed in under-served regions of the world.

ImmuMed, Inc.© 2009 - 2015 22
LOGISTICS
Assuming that 50% of the current carriers have sufficient titer to donate, each qualified carrier will need to donate 500 ml of plasma once per year. Thus, it may reasonably be concluded that a
sufficient carrier pool exists in the U.S..
Purification will be contracted to a dedicated center. At 100% capacity to meet the supply demand, processing one 10,000-liter lot per month
is required.
At the indicated dose of 1 gram IM per treatment, 489,000 grams of purified gamma globulin per year will be required for the predicted revenue projections.
Assuming a 50% purification yield of gamma globulin, one 500 ml plasma donation will yield 1 gram purified gamma globulin;
489,000 plasma donations will be needed this product volume.

ImmuMed, Inc.© 2009 - 2015 23
DEFINITIONS
Passive Immunity: high-dose intravenous immunoglobulin (antibodies) administered for the prevention and treatment of infectious disease. Antibodies neutralize toxins, and with complement, promote bacteriolysis; in viral disease, antibodies block viral entry into uninfected cells, promote antibody-directed cell-mediated cytotoxicity by natural killer cells, and neutralize virus alone or with complement.
Most commonly used for the prevention of measles, hepatitis A, hepatitis B, tetanus, varicella, rabies, vaccinia and certain viral infections in immunocompromised patients (e.g., cytomegalovirus, parvovirus B19, enterovirus, Ebola virus) and refractory staphylococcal infections and toxic shock syndrome. High-titer plasma is pooled, sterilized, purified and administered to symptomatic HIV-positive patients as a monthly intravenous infusion in an effort to provide passive immunotherapyHIV: classified as a retrovirus, is an RNA virus that codes for the enzyme reverse transcriptase;
transcribes viral genomic RNA into a DNA copy that integrates into the host cell genome.HIV (+): a state of primary HIV infection associated with HIV viremia and decline of CD4+ T cells in
peripheral blood. The median period between infection with HIV and onset of clinically apparent disease (AIDS) is approximately 10 years ( in western countries).
AIDS: a pathologic state characterized by the progressive loss of CD4+ helper/inducer subset of T lymphocytes, leading to immunosuppression, constitutional diseases, neurological complications, opportunistic infections and neoplasms rarely occurring with intact immune function.

ImmuMed, Inc.© 2009 - 2015 24
Antiretroviral Therapy: drugs administered to suppress viral replication in human immunodeficiency virus (HIV) infection. Three classes: (1) nucleoside analog reverse transcriptase inhibitors, (2) nonnucleoside reverse transcriptase inhibitors and (3) protease inhibitors. Today most commonly give as combination therapy using two or more antiretroviral agents when with a viral load higher than 5,000 to 20,000 copies per ml, regardless of the CD4+ count.
Viral Load: the measurement of HIV RNA concentration expressed as number of copies per ml plasma.
CD4 Count: the measurement o CD4+ circulating in peripheral blood expressed as number of cells per mm3
Treatment failure: the failure of antiretroviral drugs to suppress viral load. Virologic failure is defined as a viral load > 1000 copies/mL for at least 4 months after starting treatment.
HIVIG: is a hyperimmune anti HIV human immune globulin purified from high-titer HIV(+) plasma. Asymptomatic persons infected with HIV (HIV+) produce antibodies against viral RNA (when measurable = seropositive conversion). Such antibodies in conjunction with the CD4 T cells
are responsible for the period of clinical latency observed. When these antibodies reach a high
concentration, persons are deemed to have high-titers of antibody. Plasmapheresis of these antibodies is performed when there is a high-titer p24 antibodies, no detectable p24 antigen, and a helper-induced T-cell count greater than 400.
DEFINITIONS