immunity & hypersensitivity matt vreugde – [email protected]@warwick.ac.uk...
TRANSCRIPT

Learning Outcomes
List the components of the innate immune system
• List the components of the adaptive immune system
• Describe the normal functioning of the innate immune system
• Describe the normal functioning of the adaptive immune system
• Explain the interaction of key cell types in the recognition of self
& non-self as part of immune function
Relate the process of acute inflammation to the development and presentation of hypersensitivity
Describe how immune mechanisms can cause or worsen disease with reference to hypersensitivity and anaphylaxis
Explain the underlying mechanism of allergy
Outline the mechanism of action and target of the classes of drugs used to treat hypersensitivity reactions
Outline the range of allergic conditions, their investigations and management
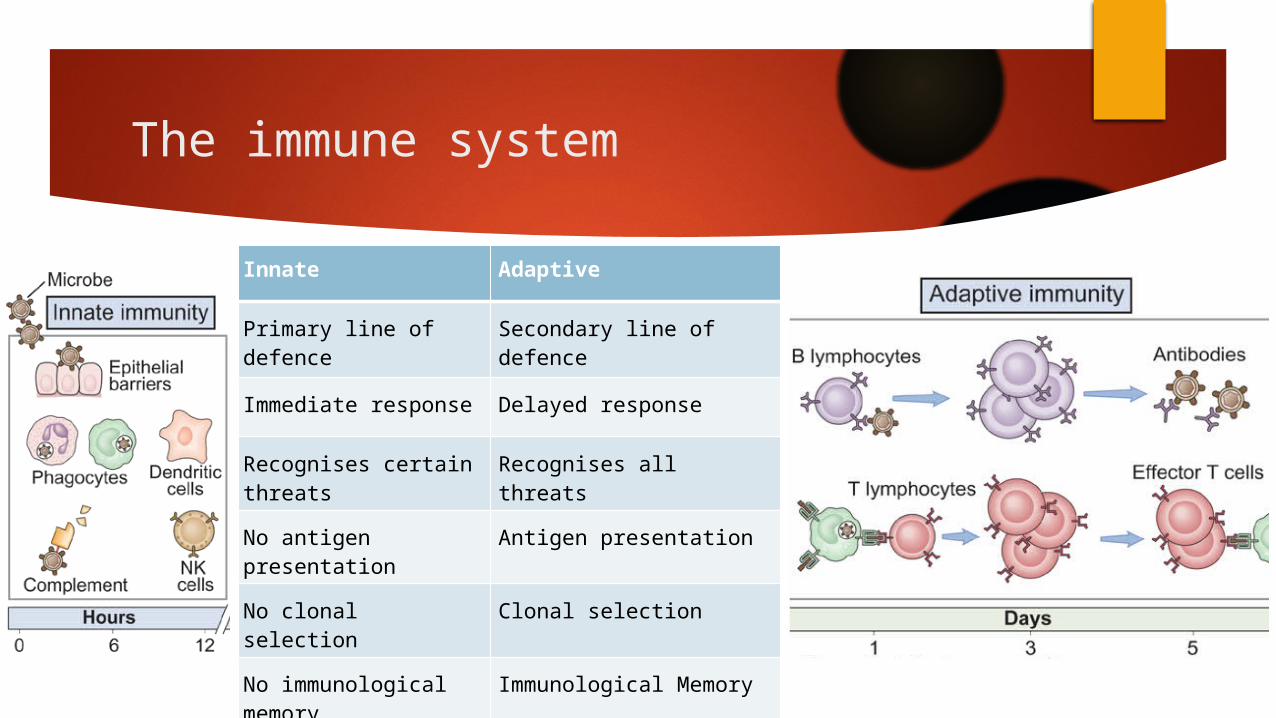
The immune system
Innate Adaptive
Primary line of defence
Secondary line of defence
Immediate response Delayed response
Recognises certain threats
Recognises all threats
No antigen presentation
Antigen presentation
No clonal selection Clonal selection
No immunological memory
Immunological Memory

Cells

Lymphocytes

Antibodies and the complement cascade

MHC Complexes & Antigen Presentation

Cell mediated vs humoral mediated immunity
B Cells & Antibodies
T Cells and antigen presenting cells

Cell Mediated Immunity
Tc+
Cell+Ag
Tc Th1
Ts
Tcm
Ag = antigen
Tc = undifferentiated T cytotoxic cell
Ts = T suppressor cell
Th1 = T helper cell
Tc+ = activated T cytotoxic cell
Tcm = T cytotoxic memory cell
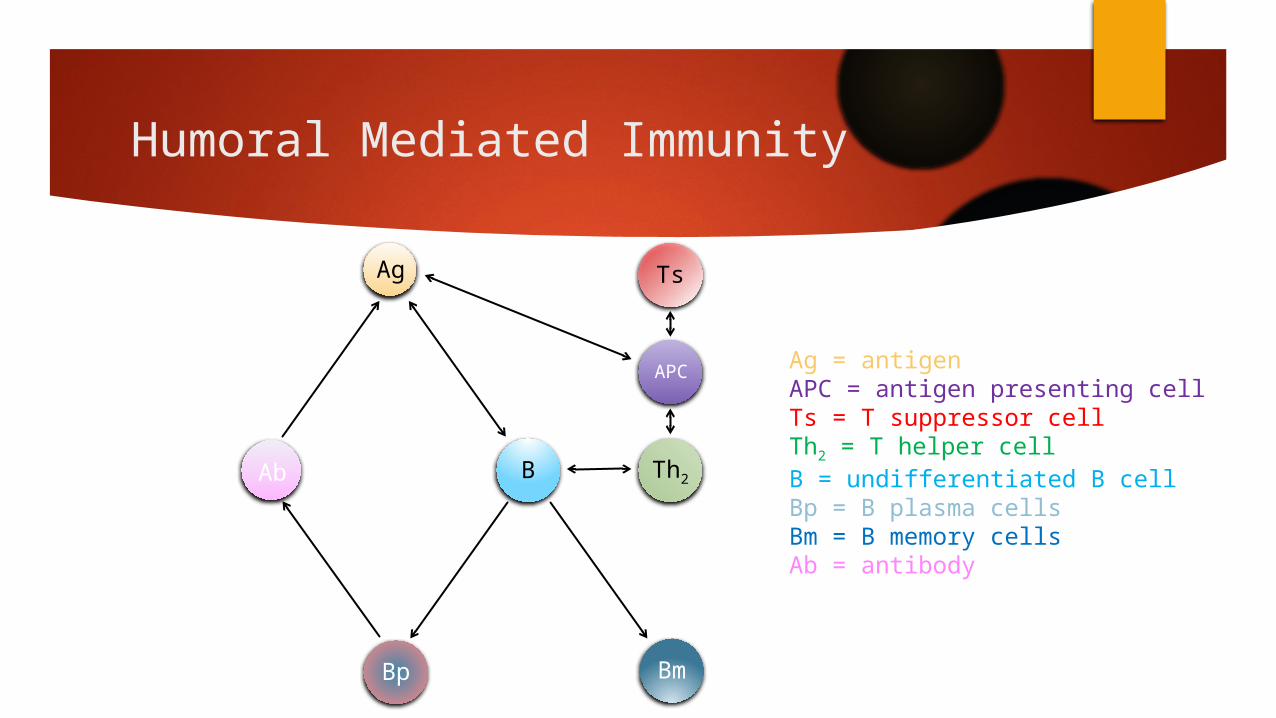
Humoral Mediated Immunity
Ag Ts
B
Bp
Ab Th2
APC
Bm
Ag = antigen APC = antigen presenting cell Ts = T suppressor cellTh2 = T helper cellB = undifferentiated B cellBp = B plasma cellsBm = B memory cellsAb = antibody

Immunological Memory

Hypersensitivity
Hypersensitivity = an inappropriate & excessive immunological reaction to an (external) antigen
• Allergy = local reaction (eg. mucous membranes, skin, lungs)
• Anaphylaxis = systemic reaction (including shock & death)
Allergen = antigen that induces a hypersensitivity reaction
(Autoimmunity = an inappropriate & excessive immunological reaction to a self-antigen / auto-antigen)
Due to dysfunctional control of the immune system (& tolerance)

Classes of hypersensitivity (LEARN!)
Type Name Mediators Examples
I Immediate or IgE-Mediated IgE + mast cells
Allergies (most)Anaphylaxis
AsthmaAtopy
II Antibody-Dependent IgM / IgG
Autoimmune haemolytic anaemia Goodpasture’s syndrome
Myasthenia gravisGraves’ disease
III Immune Complex IC
Serum SicknessExtrinsic allergic alveolitis (EAA)
Rheumatoid arthritis (RA)Systemic lupus erythematosus (SLE)
IV Delayed or Cell-Mediated T lymphocytes
Allergic contact dermatitisChronic transplant rejection
Multiple sclerosis (MS)Tuberculin skin test (TST)

Clinical Features & Symptoms
Type IAirway & eye mucous membranes → pruritus & sneezing, rhinorrhoea & lacrimationSkin → pruritus & urticariaOral & intestinal mucous membranes → pruritus & angioedemaSystemic exposure → anaphylaxis = local swelling, flushed, faint, dyspnoea, peri-oral paraesthesia, throat/chest tightness, wheeze, pale, sweaty, hypotensive, collapse, unconscious, death
Type IVSlowly developing, localised immune reactions e.g. contact dermatitisCan be fulminant and life-threatening e.g. organ rejection
Investigations
To prove Type 1 (immediate/IgE-mediated) hypersensitivity → measure blood markers such as tryptase, IgE, eosinophil count
To identify exact allergen (whether causing Type 1 or IV reaction) → skin patch testing (works for full range of allergens) :
Apply solutions of appropriate test allergens, plus negative & positive controls (saline & histamine) to the skin & review at 7 days
Positive result = lesion >3mm larger than negative control

Treatment
Avoidance : pollen, house dust mites & animals,insects, food & drugsmetals (eg. nickel) & chemicals (eg. latex)
Anti-histamines : topical (eg. eye drops) or systemic (eg. tablets)
Steroids : topical (eg. nasal spray) or systemic (eg. tablets)
De-sensitisation : also called “allergen immunotherapy”relies on creating tolerance to allergensby exposure to gradually increasing dosesdelivered sublingually or subcutaneouslysmall risk of anaphylaxis during therapyrequires weekly/monthly treatment for ~3 years

Emergency Treatment
Airway – Breathing – Circulation
Lie patient down
High-flow oxygen
IV fluids
Adrenaline (epinephrine) 500 mcg IM (0.5 ml of 1mg/ml)
IV chlorphenamine (anti-histamine)
IV hydrocortisone (steroid)
Nebulised salbutamol (bronchodilator)
Repeat adrenaline IM if no improvement after 5 minutes