immunization activities during covid-19 pandemic · •disruption in routine immunization...
TRANSCRIPT

Immunization Activities during COVID-19 Pandemic
- by Indian Academy of Pediatrics

Current situation: Circulation of virus causing COVID-19 with increasing number of cases being reported in India
Impact on immunization:
• Disruption in routine immunization
activities due to increased burden on
health infrastructure and resources
• Decreased demand for vaccination
because of physical distancing
requirements and community
reluctance

Potential impact of COVID-19 on health scenario: Current and Future
One of the most important measures: Lockdown and
Restricting community spread
Impact on patients and health related activities
Chronic Patients: Disease management (e.g. Dialysis, cancer care)
Public and Private Immunization: Drop in vaccination both mandatory and recommended
Post COVID possible VPD (Vaccine Preventable Disease) outbreaks
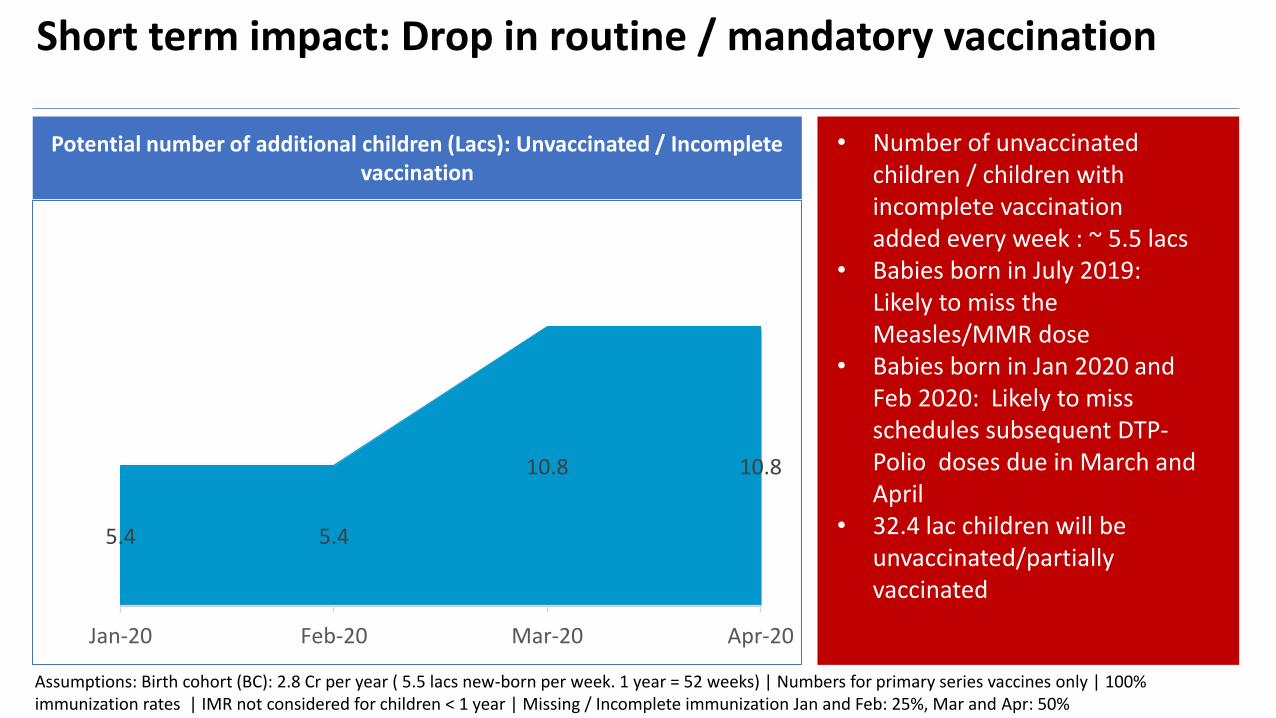
Short term impact: Drop in routine / mandatory vaccination
5.4 5.4
10.8 10.8
Jan-20 Feb-20 Mar-20 Apr-20
Assumptions: Birth cohort (BC): 2.8 Cr per year ( 5.5 lacs new-born per week. 1 year = 52 weeks) | Numbers for primary series vaccines only | 100% immunization rates | IMR not considered for children < 1 year | Missing / Incomplete immunization Jan and Feb: 25%, Mar and Apr: 50%
• Number of unvaccinated children / children with incomplete vaccination added every week : ~ 5.5 lacs
• Babies born in July 2019: Likely to miss the Measles/MMR dose
• Babies born in Jan 2020 and Feb 2020: Likely to miss schedules subsequent DTP-Polio doses due in March and April
• 32.4 lac children will be unvaccinated/partially vaccinated
Potential number of additional children (Lacs): Unvaccinated / Incomplete vaccination

Longer term impact on health scenario: Due to disruption in routine immunization
Icons made by Freepik from Flaticon
Any disruption of immunization services, even for
short periods, will result in an accumulation of
susceptible individuals: Higher likelihood of VPD
outbreak (Especially Measles & Polio)
Such outbreaks may result in:
• VPD-related deaths
• Increased burden on health systems already
strained by the response to COVID-19 outbreak
• Decline in immunization related health indicators
Plan to secure future: Maintain routine immunization as long as COVID-19 response measures permit
Immediate Action Required: Plan for detailed assessment of VPD epidemiology, transmission scenarios of COVID-19, impact in these scenarios and corresponding mitigation measures

Icons made by Srip from Flaticon
Review current immunization levels and potential future (impact of Covid-19)
Prioritize efforts and resources: Initial focus on epidemic prone VPDs
• VPD surveillance data (measles, polio, H1N1)• Incorporate regional & ICMR knowledge
• Sustain measles elimination and polio eradication• Focus on At-risk population and HCWs
Critical to maintain Polio-free status of India: Increased efforts for checking any sewerage isolation/AFP. Continued use of IPV and bOPV is an absolute must with additional efforts to be deployed on catch-up immunization
Longer term impact of immunization disruption: Higher probability of VPD occurrence

Icons made by Photo 3 Idea Studio from Flaticon
Vaccinate newborns (as per the national immunization schedule) in maternity hospitals
Follow guidelines on COVID-19 infection prevention during immunization sessions
Prioritize primary series vaccinations for poliomyelitis-containing vaccines, measles-rubella and other combination vaccines
Avoid mass vaccination campaigns until the COVID-19 situation resolves
Prioritize pneumococcal and seasonal influenza vaccines for vulnerable population groups including Healthcare workers
WHO recommendation for Europe: Potential actions for India20th March 2020

Key areas to consider
Epidemiological
situation of COVID-19
and related
mitigation measures
in place
Health system and
immunization
delivery services
characteristics and
constraints
Supply of vaccines:
Timely and in
adequate quantities
Epidemiological risks
of VPDs among the
general population
and specific
vulnerable groups
Icons made by Freepik from Flaticon
Appropriateness of chosen options should be monitored and periodically reassessed (based on impact) as the COVID-19 situation evolves

Potential high level plan: Current and Future
Surveillance , especially for Polio, Measles, etc
01 Issuance of National Guidelines: Separate for Public and Private Sector
Ensure important vaccinations at Birth: Polio-DTP and Measles a PriorityPneumococcal & influenza vaccines
02
Increased surveillance for VPDs: Especially for Polio, Measles, etc
03
Catch up or Intensified Immunization post COVID-19: Similar to Pulse Polio or Mission Indradhanush
04
• Guidelines for ASHA & ANM for Vaccination Dos & DONTs• Media dissemination to reassure parents and HCWs• Private sector may work with OPPI to work on Immunization
• Ensure completion of at Birth vaccines: Maternity homes and Hospitals
• Evaluate alignment with EU guidelines by WHO March 2020• Polio-DTP and Measles vaccination: Absolute Priority
• Intensify VPD surveillance: Especially polio and Measles• Ensure stocking of mandatory vaccines: bOPV, IPV, DTP and
Measles vaccine / MMR
• Catch-up vaccination: Planning for campaigns• Reactivate successful Govt. Programs: e.g. Mission
Indradhanush and Pulse Polio• Vulnerable population: Pneumonia and Influenza vaccination

Parents to be reassured
During this COVID Pandemic:
**vaccination at a later date is manageable
***Message should reach to the public via print media/TV/Radio

In Conclusion
Regular or heightened surveillance to continue for VPDs especially Polio and Measles
Infected or quarantined mothers to be advised to get their children vaccinated, on advise of their treating physician
Ensure continuity of Birth dose BCG, b-OPV & Hep B
COVID-19 govt. recommendation to be followed and social distancing maintained
Advisory to parents to immediately start immunization on receiving Govt. notification / communication
Prioritize primary schedule dosesPrioritize Polio, Influenza, MMR and Pneumococcal vaccination for infantsPrioritize Influenza vaccination for Vulnerable population including HCWs
Missed immunization: Parents to be reassured that subsequent vaccine doses have permissible window to vaccinate
01
07 02
06 03
05 04

Thank You
Await next advisory on Vaccinations after relaxation of “Lockdown”.
Will be released soon

Evaluate WHO recommendations* for Interrupted or Delayed Routine ImmunizationAntigen Age of 1st Dose Doses in Primary Series (min
interval between doses)Interrupted primary series Doses for those who start vaccination late Booster
If ≤ 12 months of age If > 12 months of age
BCG As soon as possible after birth 1 dose NA 1 dose 1 dose Not recommended
Hepatitis B As soon as possible after birth (<24h)
Birth dose <24 hrs plus 2-3 doses with DTPCV (4 weeks)
Resume without repeating previous dose
3 doses 3 doses Not recommended
Polio bOPV + IPV 6 weeks (see footnote for birth dose)
4 doses (IPV dose to be given with bOPV dose from 14 weeks of age) (4 weeks)
Resume without repeating previous dose
4 doses (IPV to be given with 1st dose of bOPV)
4 doses (IPV to be given with 1st dose of bOPV)
Not recommended
IPV / bOPV Sequential8 weeks (IPV 1st)
1-2 doses IPV and 2 doses bOPV(4 weeks)
Resume without repeating previous dose
1-2 doses IPV and 2 doses bOPV1-2 doses
IPV and 2 doses bOPV Not recommended
IPV8 weeks
3 doses (4 weeks) Resume without repeating previous dose
3 doses 3 dosesIf the primary series begins < 2 months of age, booster to be given at least 6 months after the last dose
DTP-containing vaccine (DTPCV)
6 weeks (min) 3 doses (4 weeks)
Resume without repeating previous dose 3 doses
3 doses with interval of at least 4 weeks between 1st & 2nd dose, and at least 6 mosbetween 2nd & 3rd dose. (if > 7 yrs use only aP containing vaccine
3 boosters: 12-23 months (DTP containing vaccine); 4-7 years (Td/DT containing vaccine; and 9-15 yrs (Td containing) (if > 7 yrs use only aP containing vaccine).
Pneumococcal (Conjugate) 6 weeks (min)
3 doses (3p+0) with DTPCV (4 weeks) or 2 doses (2p+1) (8 weeks)
Resume without repeating previous dose 2-3 doses
1-5 yrs at high-risk: 2 dosesBooster at 9-18 months if following 2 dose schedule Another booster if HIV+ or preterm neonate
Rotavirus 6 weeks (min)
2 or 3 depending on product given with DTPCV
Resume without repeating previous dose
2 or 3 depending on product>24 months limited benefit
Not recommended
Measles 9 or 12 months (6 months min, see footnote)
2 doses (4 weeks) Resume without repeating previous dose
2 doses2 doses Not recommended
Rubella 9 or 12 months
1 dose with measles containing vaccine
NA 1 dose 1 dose Not recommended
Mumps 12-18 months
2 doses with measles containing vaccine (4 weeks)
Resume without repeating previous dose
Not recommended2 doses Not recommended
Seasonal influenza (inactivated quadrivalent)
6 months (min)< 9 yrs: 2 doses (4 weeks) ≥ 9 yrs: 1 dose
Resume without repeating previous dose
2 doses < 9 yrs: 2 doses ≥ 9 yrs:1 dose Revaccinate annually 1 dose only
Varicella 12-18 months
1-2 (4 weeks – 3 months, depending on manufacturer)
Resume without repeating previous dose
Not recommended 1-2 doses
*Summary of WHO Position Papers dated April 2019