immunologia e cancro: differenze di...
TRANSCRIPT

Anna Maria Di GiacomoMedical Oncology and Immunotherapy
Center for Immuno-Oncology
SIENA, ITALY
Immunologia e Cancro: Differenze di Genere

Cancer immunotherapy, a very long standing concept
Venuti A. J Exp Clin Cancer Res. 2009.
The concept that a vaccine could be useful in the treatment of cancer is a long-held
hope coming from the observation that patients with cancer who developed bacterial
infections experienced remission of their malignancies.
The earliest mention of cancer-fighting infections dates to a
citation from Ebers papyrus (1550 B.C.) attributed to the Egyptian
physician Imhotep (2600 B.C.), who recommended to treat
tumors (swellings) with a poultice followed by an incision which
would result in infection of the tumor and therefore its regression.
In 1896, the surgeon William Coley locally injected streptococcal
broth cultures to induce erysipelas in an Italian patient (Mr. Zola)
with an inoperable neck sarcoma, obtaining a tumour regression.
Although therapy was toxic, the patient's tumour ultimately
regressed, and he lived disease-free for 8 years before
succumbing to his cancer.

Hallmarks of cancer2000: immune mechanisms not recognized
Hanahan D, Weinberg RA, Cell 2000; 100: 57-70

The cancer immunoediting concept
R D Schreiber et al. Science 2011

Hallmarks of cancer2011: immune mechanisms recognized
Hanahan D, Weinberg RA, Cell 2011; 144: 646-674

Surgery
Radiotherapy
Chemotherapy
Evolving Therapeutic Options for
Cancer Treatment

Surgery
Radiotherapy
Chemotherapy
Immunotherapy
Evolving Therapeutic Options for
Cancer Treatment

8
Adapted from Pardoll DM 2012.
APC/
TumorT cell
CD40 CD40L
CD137
OX40
CD137L
OX40L
Activation
Activation
Activation
PD-1
B7-1 (CD80)
PD-L1
PD-L2
LAG-3
MHC
CD28 ActivationB7-2 (CD86)
B7-1 (CD80) CTLA-4 Inhibition
TCR
Inhibition
Inhibition
Inhibition
These pathways can be
blocked via I-O agents to
counteract tumor-
mediated inhibition
These pathways can be
activated via I-O agents to
counteract tumor-mediated
inhibition
APC=antigen-presenting cell; CTLA-4=cytotoxic T-lymphocyte antigen-4; LAG-3=lymphocyte activation gene-3; MHC=major
histocompatibility complex;
PD-1=programmed death-1; PD-L1=PD ligand-1; PD-L2=PD ligand-2; TCR=T-cell receptor.
Pardoll DM. Nat Rev Cancer. 2012;12:252-264.
T-cell Checkpoint and Co-stimulatory Pathways

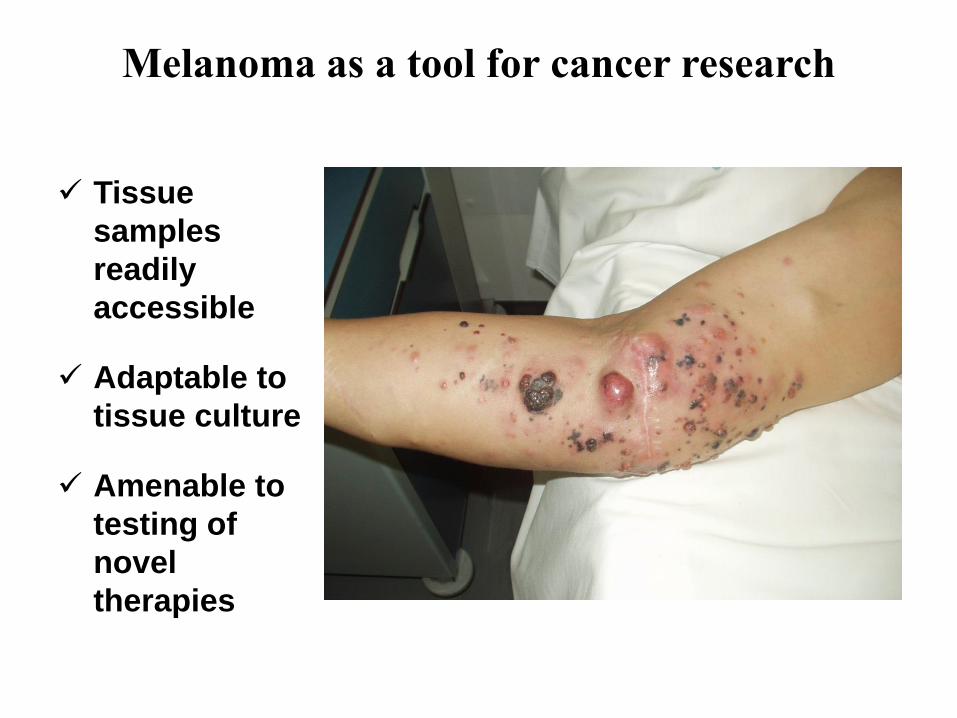
Tissue
samples
readily
accessible
Adaptable to
tissue culture
Amenable to
testing of
novel
therapies
Melanoma as a tool for cancer research

0 1 2 3 4 5 6 7 8 9 10
100
90
80
70
60
0
50
40
30
20
10
Overa
ll S
urv
ival (%
)
Years
IPI (Pooled analysis)1
NIVO Monotherapy (Phase 3 Checkmate 066)3
N=210
NIVO Monotherapy (Phase 1 CA209-003)2
N=107
N=1,861
11
Immune Checkpoint Inhibitors Provide Durable Long-
term Survival for Patients with Advanced Melanoma
1. Schadendorf et al. J Clin Oncol 2015;33:1889-1894; 2. Current analysis; 3. Poster presentation by Dr. Victoria Atkinson at SMR 2015 International Congress.

Immune Checkpoint Pathways
CTLA-4 = cytotoxic T-lymphocyte-associated antigen 4 ; MHC = major histocompatibility complex; PD-1 = programmed death-1;
PD-L1 = programmed death ligand 1; TCR = T-cell receptor.
CTLA-4 Blockade (ipilimumab) PD-1 Blockade (nivolumab)
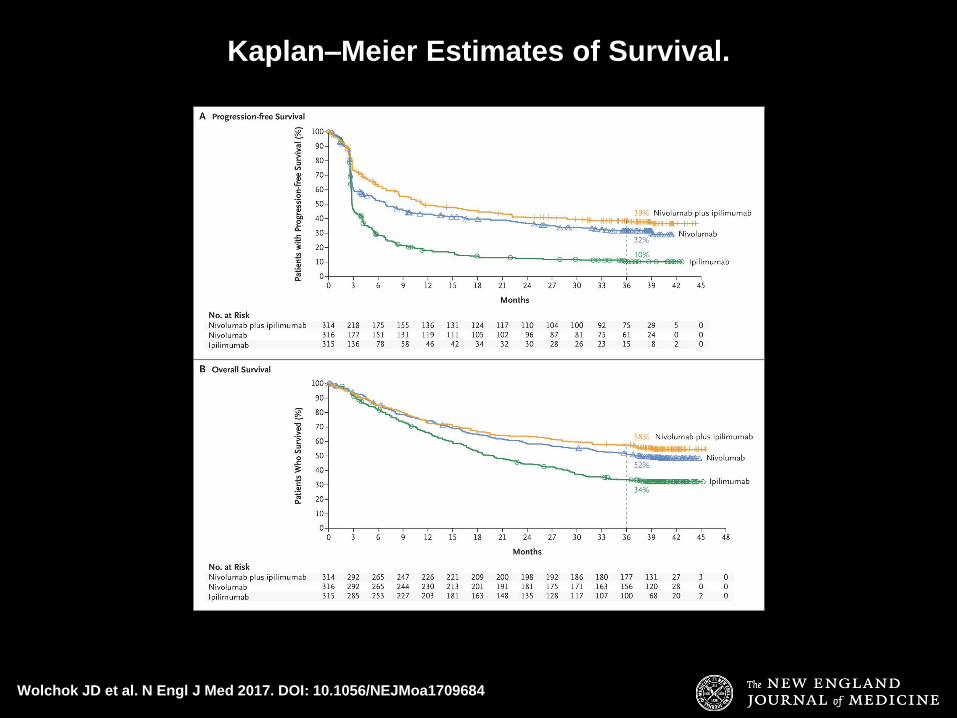
Wolchok JD et al. N Engl J Med 2017. DOI: 10.1056/NEJMoa1709684
Kaplan–Meier Estimates of Survival.

A
B
C
D
**
F
* * *
*
C E
Baseline 3 weeks after the first dose 20 weeks after the first dose
Baseline 9 weeks after the first dose 20 weeks after the first dose
Danielli R et al, unpublished

Immunotherapy in solid tumors with
immunomodulating antibodies
www.ImmunOncologia.org


ASCO 2016
CheckMate 017 and CheckMate 057 Study Designs
17
LCSS = Lung Cancer Symptom Scale; ORR = objective response rate; OS = overall survival; PD = progressive disease; PFS = progression-free survival; TKI = tyrosine kinase inhibitor
CheckMate 017 (NCT01642004; N = 272)
CheckMate 057 (NCT01673867; N = 582)
Docetaxel 75 mg/m2 IV Q3W
until PD or
unacceptable toxicity
(n = 290)
Key eligibility criteria
•Stage IIIB/IV SQ NSCLC
•ECOG PS 0–1
•One prior platinum-based chemotherapy
•Pretreatment (archival or fresh) tumor
samples required for PD-L1 analysis
Key eligibility criteria
•Stage IIIB/IV non-SQ NSCLC
•ECOG PS 0–1
•One prior platinum-based chemotherapy
•Pretreatment (archival or fresh) tumor
samples required for PD-L1 analysis
•Prior maintenance therapy allowed
•Prior TKI therapy allowed for known ALK
translocation or EGFR mutation Ran
do
miz
e 1
:1R
an
do
miz
e 1
:1
Endpoints
• Primary‒ OS
• Additional‒ ORR‒ PFS‒ Efficacy by tumor PD-L1 expression‒ Safety‒ Quality of life (LCSS)
Endpoints
• Primary‒ OS
• Additional‒ ORR‒ PFS‒ Efficacy by tumor PD-L1 expression‒ Safety‒ Quality of life (LCSS)
Nivolumab 3 mg/kg IV Q2W
until PD or
unacceptable toxicity
(n = 292)
Docetaxel 75 mg/m2 IV Q3W
until PD or
unacceptable toxicity
(n = 137)
Nivolumab 3 mg/kg IV Q2W
until PD or
unacceptable toxicity
(n = 135)

ASCO 201618
CI = confidence interval; HR = hazard ratio
Kaplan–Meier Estimates of OS(3 Years Minimum Follow-up)
29
2
19
4
14
8
11
2
82 58 49 39 7 0
29
0
19
5
11
2
67 46 35 26 16 1 0
13
5
86 57 38 31 26 21 16 8 0
13
7
69 33 17 11 10 8 7 3 0
CheckMate 057 (non-SQ NSCLC)CheckMate 017 (SQ NSCLC)
No. of patients at risk
Nivolumab
Docetaxel
No. of patients at risk
Nivolumab
Docetaxel
0 6 12 18 24 30 36 42 48 54
Δ10%
Nivolumab (n = 135)
Docetaxel (n = 137)
1-y OS = 42%
2-y OS = 23%
3-y OS = 16%1-y OS = 24%
2-y OS = 8%3-y OS = 6%
HR (95% CI): 0.62 (0.48, 0.80)
100
80
60
40
20
0
OS
(%
)
Months
Δ18%
Δ15%
0 6 12 18 24 30 36 42 48 54
Months
1-y OS = 51%
2-y OS = 29%
3-y OS = 18%
1-y OS = 39%
2-y OS = 16%
3-y OS = 9%
Nivolumab (n = 292)
Docetaxel (n = 290)
HR (95% CI): 0.73 (0.62, 0.88)
100
80
60
40
20
0O
S (
%)
Δ12%
Δ13%
Δ9%
Felip E, ESMO 2017

ASCO 2016

5-Year Estimates of OS
Median OS (95% CI), mo
Overall (N = 129) 9.9 (7.8, 12.4)
100
80
60
40
20
0
0 1 2 3 4 5 6 7 8
129 49 27 20 17 16 3 1 0
YearsNo. at Risk
OS
(%
)
1 y OS, 42%
2 y OS, 24%3 y OS, 18% 5 y OS, 16%
aThere were 3 deaths between 3 and 5 years, all due to disease progression; 1 surviving patient was censored for OS prior to 5 years (OS: 58.2+ months)
AACR 2017
BMS CA209-003: phase 1 dose finding study in NSCLC

BMS HIGHLY CONFIDENTIAL. For internal use only.
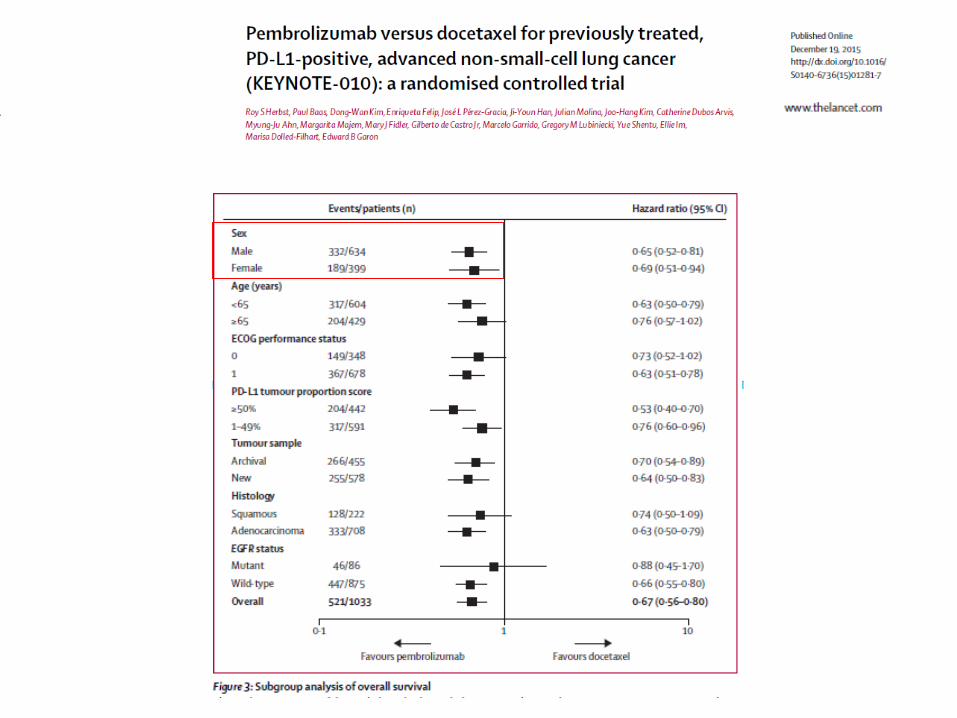
Herbst, Lancet, 2016
Garon, ASCO 2016
Keynote 010
All PD-L1 PD-L1 ≥ 50%
PD-L1 = 1-49%

KEYNOTE-024 Study Design (NCT02142738)
Presented By Julie Brahmer at 2017 ASCO Annual Meeting

Kaplan-Meier Estimate of PFS2
Presented By Julie Brahmer at 2017 ASCO Annual Meeting

Kaplan-Meier Estimate of OS: <br />Updated Analysis
Presented By Julie Brahmer at 2017 ASCO Annual Meeting

Jun 16, 2016


Ph. III Anti-PD1/PD-L1 combination trials in first line advanced NSCLC

Immunotherapy in solid tumors with immunomodulating antibodies
www.ImmunOncologia.org

Design of phase III CheckMate 025 study
Motzer RJ, et al. N Engl J Med 2015;373:1803–13.
Patient
eligibility
• aRCC with
clear-cell
component
• KPS ≥70%
• One or two
prior anti-
angiogenic
therapies
• Progression
within 6
months prior
to enrollment
Nivolumab
3 mg/kg
intravenously
every 2 weeks
Everolimus
10 mg orally
once daily
Ra
nd
om
ize
1:1
Study
endpoints
• Primary
– OS
• Secondary
– ORR
– PFS
– Safety
– HRQoL
10
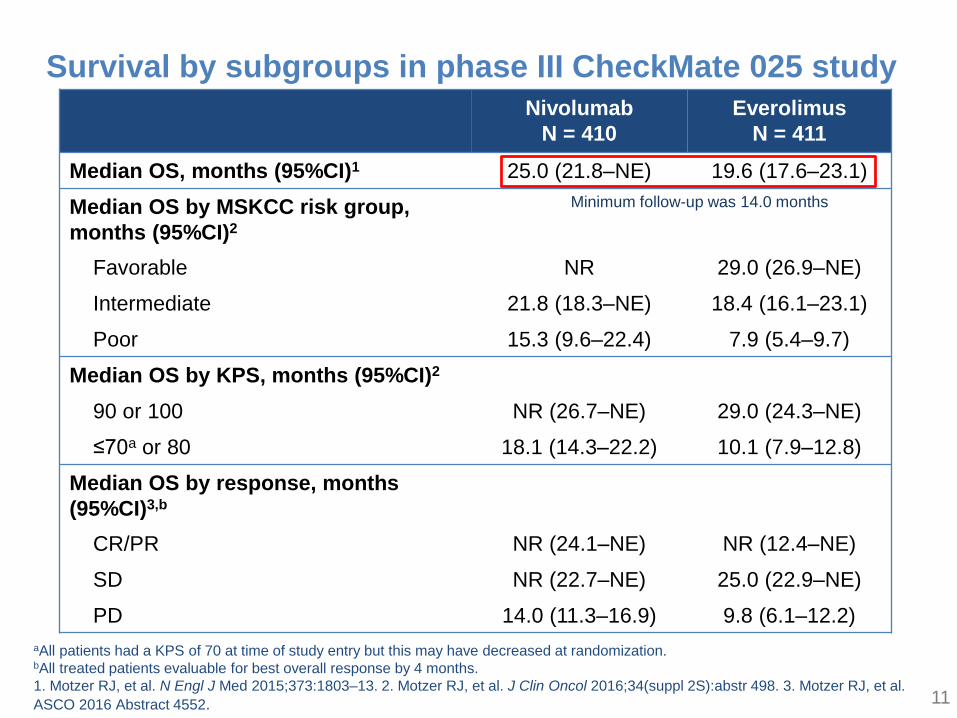
Survival by subgroups in phase III CheckMate 025 study
Nivolumab
N = 410
Everolimus
N = 411
Median OS, months (95%CI)1 25.0 (21.8–NE) 19.6 (17.6–23.1)
Median OS by MSKCC risk group,
months (95%CI)2
Favorable NR 29.0 (26.9–NE)
Intermediate 21.8 (18.3–NE) 18.4 (16.1–23.1)
Poor 15.3 (9.6–22.4) 7.9 (5.4–9.7)
Median OS by KPS, months (95%CI)2
90 or 100 NR (26.7–NE) 29.0 (24.3–NE)
≤70a or 80 18.1 (14.3–22.2) 10.1 (7.9–12.8)
Median OS by response, months
(95%CI)3,b
CR/PR NR (24.1–NE) NR (12.4–NE)
SD NR (22.7–NE) 25.0 (22.9–NE)
PD 14.0 (11.3–16.9) 9.8 (6.1–12.2)
aAll patients had a KPS of 70 at time of study entry but this may have decreased at randomization.bAll treated patients evaluable for best overall response by 4 months.
1. Motzer RJ, et al. N Engl J Med 2015;373:1803–13. 2. Motzer RJ, et al. J Clin Oncol 2016;34(suppl 2S):abstr 498. 3. Motzer RJ, et al.
ASCO 2016 Abstract 4552.
Minimum follow-up was 14.0 months
11

Summary of safety in phase III CheckMate 025 study
Nivolumab
N = 406
Everolimus
N = 397
Any
grade
Grade
3–4
Any
grade
Grade
3–4
Treatment-related
AEs, %78.6 18.7 87.9 36.5
Treatment-related
AEs leading to
discontinuation, %
7.6 4.7 13.1 7.1
12Motzer RJ, et al. N Engl J Med 2015;373:1803–13.

CheckMate 214: Study design
IMDC, International Metastatic RCC Database Consortium; KPS, Karnofsky performance status; Q2W, every 2 weeks; Q3W, every 3 weeks
Treatment until
progression or
unacceptable
toxicity
• Treatment-naïve
advanced or
metastatic clear-cell
RCC
• Measurable disease
• KPS ≥70%
• Tumor tissue
available for PD-L1
testing
TreatmentPatients
Randomize 1:1
Arm A
3 mg/kg nivolumab IV +
1 mg/kg ipilimumab IV Q3W
for four doses, then
3 mg/kg nivolumab IV Q2W
Arm B
50 mg sunitinib orally once
daily for 4 weeks
(6-week cycles)
Stratified by
•IMDC prognostic score
(0 vs 1–2 vs 3–6)
•Region (US vs
Canada/Europe vs Rest
of World)

ORR and DOR: IMDC intermediate/poor risk
N = 847
Outcome
NIVO +
IPI
N = 425
SUN
N = 422
Confirmed ORR,a % (95%
CI)
42 (37–
47)
27 (22–
31)
P < 0.0001
Confirmed BOR,a %
Complete response
Partial response
Stable disease
Progressive disease
Unable to determine/not
reported
9b
32
31
20
8
1b
25
45
17
12
aIRRC-assessed ORR and BOR by RECIST v1.1; bP < 0.0001
SUN
NIVO + IPI
No. at Risk
177 146 120 55 3
112 75 52 17 0
0.0
0.1
0.2
0.3
0.4
0.5
0.6
0.7
0.8
0.9
1.0
0 6 12 18 24Months
Du
rati
on
of
Resp
on
se (
Pro
bab
ilit
y)
Co-primary endpoint: ORR
Median duration of
response, months
(95% CI)
Patients with
ongoing
response, %
NIVO +
IPI
NR (21.8–
NE)72
SUN18.2 (14.8–
NE)63
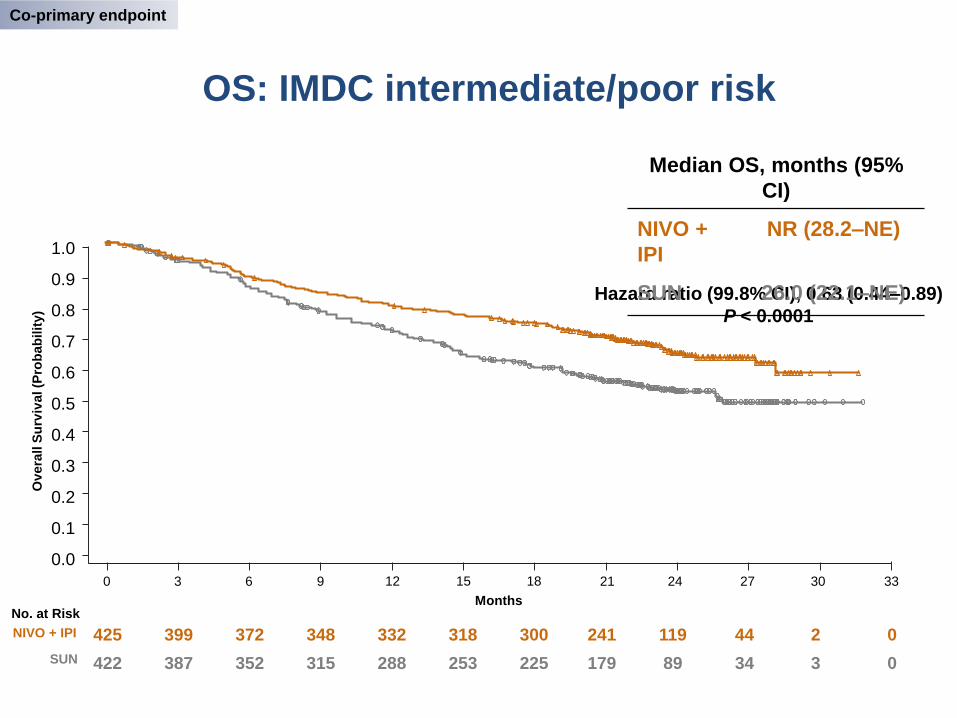
OS: IMDC intermediate/poor risk
Hazard ratio (99.8% CI), 0.63 (0.44–0.89)
P < 0.0001
Median OS, months (95%
CI)
NIVO +
IPI
NR (28.2–NE)
SUN 26.0 (22.1–NE)
Ov
era
ll S
urv
ival (P
rob
ab
ilit
y)
425 399 372 348 332 318 300 241 119 44 2 0
422 387 352 315 288 253 225 179 89 34 3 0
No. at Risk
NIVO + IPI
SUN
Months
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0.0
18 21 24 27 30 3315129630
Co-primary endpoint
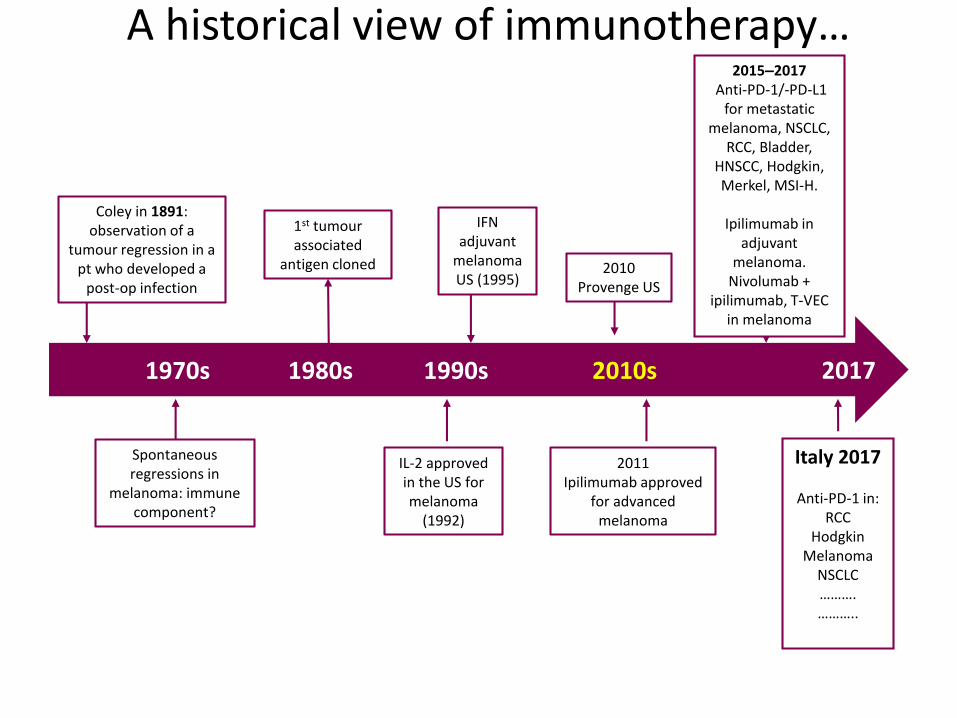
1970s 1980s 1990s 2010s
Spontaneous regressions in
melanoma: immune component?
1st tumour associated
antigen cloned
IL-2 approved in the US for melanoma
(1992)
IFN adjuvant
melanoma US (1995)
2011Ipilimumab approved
for advanced melanoma
2015–2017Anti-PD-1/-PD-L1
for metastatic melanoma, NSCLC,
RCC, Bladder, HNSCC, Hodgkin, Merkel, MSI-H.
Ipilimumab in adjuvant
melanoma. Nivolumab +
ipilimumab, T-VEC in melanoma
2010 Provenge US
Coley in 1891: observation of a
tumour regression in a pt who developed a
post-op infection
A historical view of immunotherapy…
Italy 2017
Anti-PD-1 in: RCC
HodgkinMelanoma
NSCLC……….………..
2017
The theoretical right patient for immunotherapy?
• Low tumor burden ?
• Slow progressive disease ?
• Untreated ?
• Younger ?
• Gender ?
• Normal biohumoral parameters (e.g. LDH) ?
• Molecularly addicted ?

Individuality and Variation of Personal Regulomes
in Primary Human T Cells
Qu et al., 2015, Cell Systems

KEYNOTE-006

Overall 19/3558/86
0.35 (0.19–0.64)0.62 (0.39–0.98)
Age Category<65
≥65
8/1734/4911/1824/37
0.26 (0.11–0.64)0.72 (0.40–1.29)0.50 (0.21–1.19)0.54 (0.26–1.12)
GenderMale
Female
7/1626/4212/1932/44
0.45 (0.18–1.12)0.47 (0.24–0.94)0.27 (0.12–0.61)0.80 (0.44–1.48)
Baseline ECOG Performance Status0
1
12/2437/587/10
21/28
0.33 (0.16–0.69)0.52 (0.30–0.91)0.41 (0.13–1.25)0.83 (0.37–1.86)
M Stage at Study EntryM1c 12/22
36/530.37 (0.17–0.84)0.54 (0.29–1.00)
Baseline LDH≤ULN
>ULN
9/1827/4310/1729/41
0.22 (0.09–0.54)0.43 (0.23–0.82)0.45 (0.19–1.07)0.71 (0.36–1.40)
Checkmate 067- PFS by Subgroups
39
Hazard Ratio (95% CI)Events/patients NIVO+IPI NIVO
0.0 0.2 0.4 0.6 0.8 1.0 1.2 1.4
NIVO or NIVO+IPI better IPI better
BMS HIGHLY CONFIDENTIAL. For internal use only.
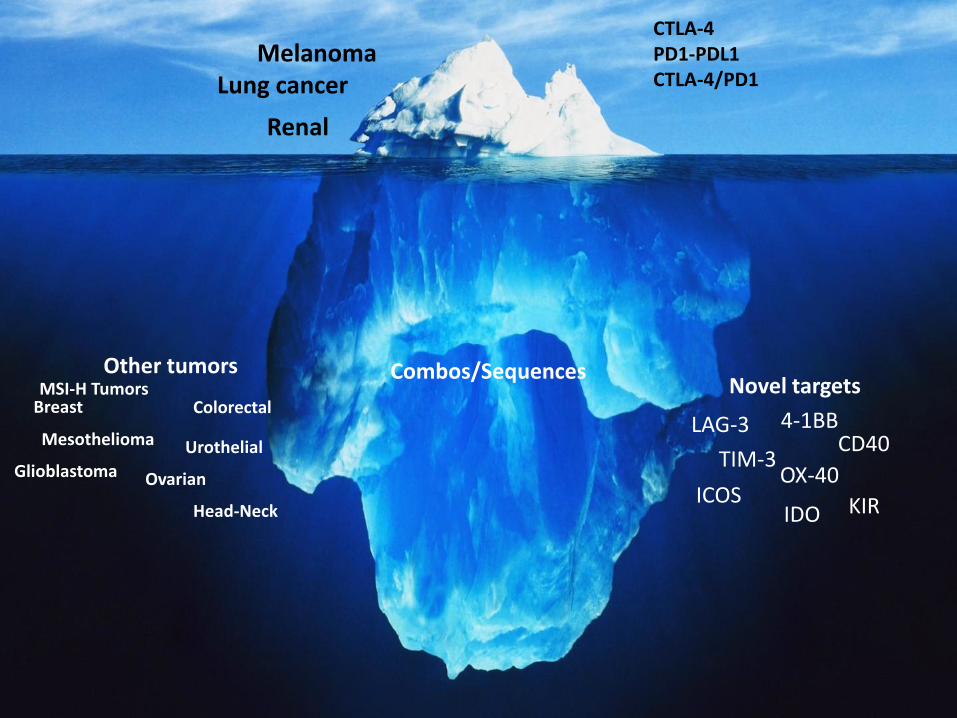
CTLA-4PD1-PDL1CTLA-4/PD1
Combos/Sequences
MelanomaLung cancer
Novel targets
4-1BB
OX-40ICOS KIR
TIM-3
LAG-3CD40
IDO
Renal
Other tumors
Mesothelioma Urothelial
Colorectal
Glioblastoma
Head-Neck
Ovarian
BreastMSI-H Tumors

• Maresa Altomonte• Erika Bertocci• Luana Calabrò• Ornella Cutaia• Riccardo Danielli• Anna Maria Di Giacomo• Carolina Fazio• Ester Fonsatti• Carla Chiarucci• Gianluca Giacobini• Andrea Lazzeri
Medical Oncology and ImmunotherapyCenter for Immuno-Oncology
University Hospital of Siena - Italy
• Francesca Colizzi• Sandra Coral• Alessia Covre• Elisabetta Fratta• Hugues Nicolay• Luca Sigalotti• Maria Lofiego• Patrizia Tunici• Antonello Lamboglia• Monica Valente• Armida D’Incecco