immunotherapy for type 1 diabetes-an update · immunotherapy for type 1 diabetes-an update mark s....
TRANSCRIPT

Immunotherapy for Type 1 Immunotherapy for Type 1 DiabetesDiabetes--an updatean update
Mark S. Anderson, MD, PhDAssistant Professor
UCSF Diabetes Center
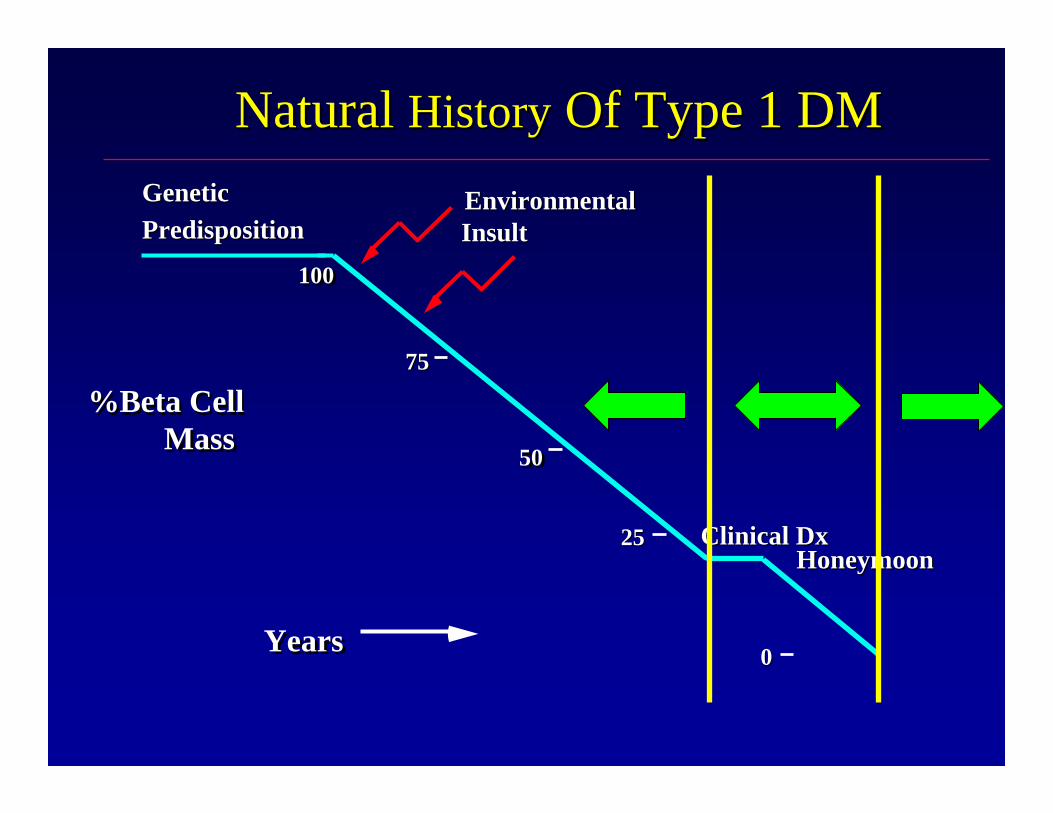
Natural Natural HistoryHistory Of Type 1 DMOf Type 1 DM
%Beta CellMass
%Beta CellMass
GeneticGeneticPredispositionPredisposition
EnvironmentalEnvironmentalInsultInsult
Clinical Clinical DxDx
7575
5050
2525
00
100100
YearsYears
HoneymoonHoneymoon

Processes of Autoimmunity in T1D
MHC-peptideTCR
Plasma Cell
TH2 Cell
TH1 Cell
TNFαIL-1 IL-6 GM-CSFIFNα
AutoreactiveB Cell
Dendritic Cell
IFNγIL-2
TLR
IL-12IL-15IL-18
NOPGE
TLR
IL-10
CD8+ CTL
Macrophage
IL-4IL-5IL-10IL-13
Pancreatic Lymph node
Pancreas
Treg Cell
IL-35TGFβIL-10

Progression in Type 1 DiabetesProgression in Type 1 Diabetes
Human T1D (Mark Atkinson – nPOD)
Mouse T1D - NODNon-diabetic Mouse
β cells in the islets at the time of diagnosisare marginally insulin+
76 y.o. M with T1D (>50 yrs)

•• 7 of 7 insulin 7 of 7 insulin independent at 1 independent at 1 yr!yr!
•• High quality isletsHigh quality islets–– Usually need 2 Usually need 2
donorsdonors
•• New New immunoimmuno--suppressant suppressant cocktailcocktail–– No steroidsNo steroids

•• 21 out of 36 21 out of 36 reached insulin reached insulin independenceindependence
•• 16 of these 21 16 of these 21 needed to start needed to start insulin again at 2 insulin again at 2 yearsyears

Islets...where do we stand?Islets...where do we stand?•• What are the short and long term risks?What are the short and long term risks?
–– Bleeding, clots from procedureBleeding, clots from procedure–– LongLong--standing standing immunosuppressionimmunosuppression
•• How robust are the islets?How robust are the islets?–– Only 10% remain off exogenous insulin by 5 yrsOnly 10% remain off exogenous insulin by 5 yrs
•• Can the procedure be exported to other centers?Can the procedure be exported to other centers?•• Can we optimize the procedure? Can we optimize the procedure?
–– islet preparation and infusionislet preparation and infusion–– Currently need 2 or more donorsCurrently need 2 or more donors–– alloallo-- and autoand auto--immunityimmunity
•• Do we have enough islets? Do we have enough islets? –– 3,000 cadaveric pancreases / yr3,000 cadaveric pancreases / yr–– 35, 000 new onset Type 1 / yr, 1.8 million with established 35, 000 new onset Type 1 / yr, 1.8 million with established
T1DM T1DM •• What about stem cells?What about stem cells?
–– Can we make beta cells?Can we make beta cells?–– Concern with onConcern with on--going immunity issuesgoing immunity issues

Natural Natural HistoryHistory Of Type 1 DMOf Type 1 DM
%Beta CellMass
%Beta CellMass
GeneticGeneticPredispositionPredisposition
EnvironmentalEnvironmentalInsultInsult
Clinical Clinical DxDx
7575
5050
2525
00
100100
YearsYears
HoneymoonHoneymoon
Type 1 DM PreventionType 1 DM Prevention
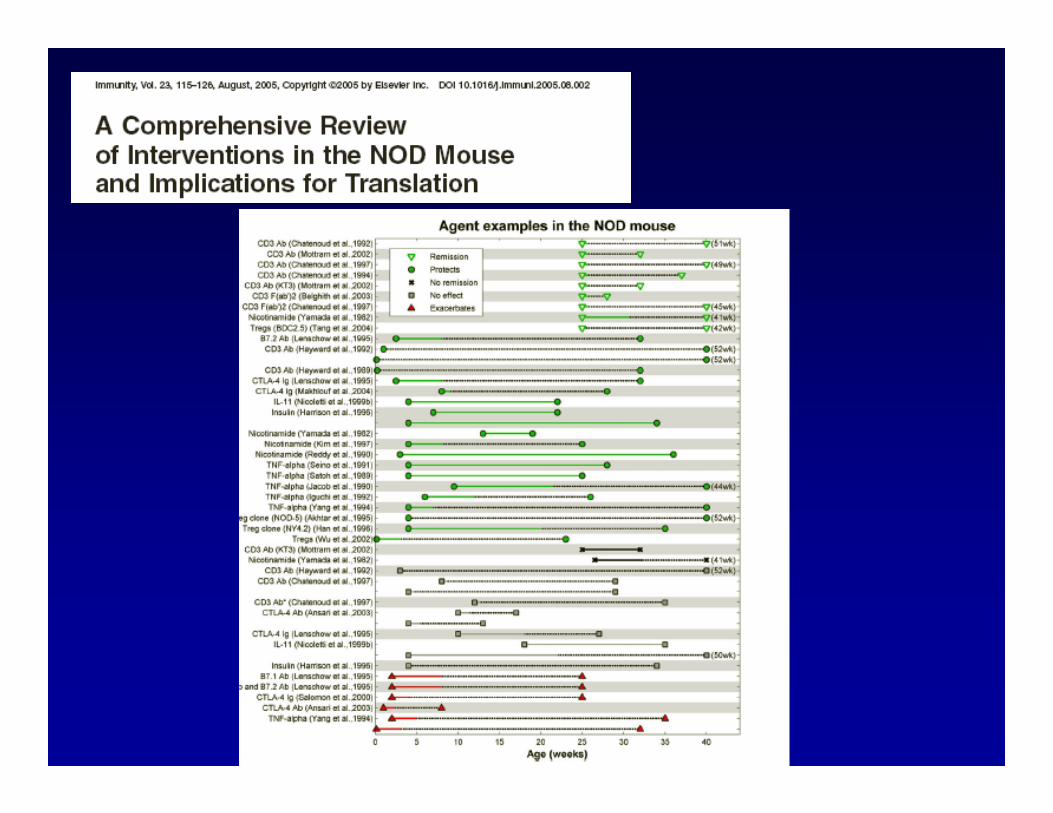
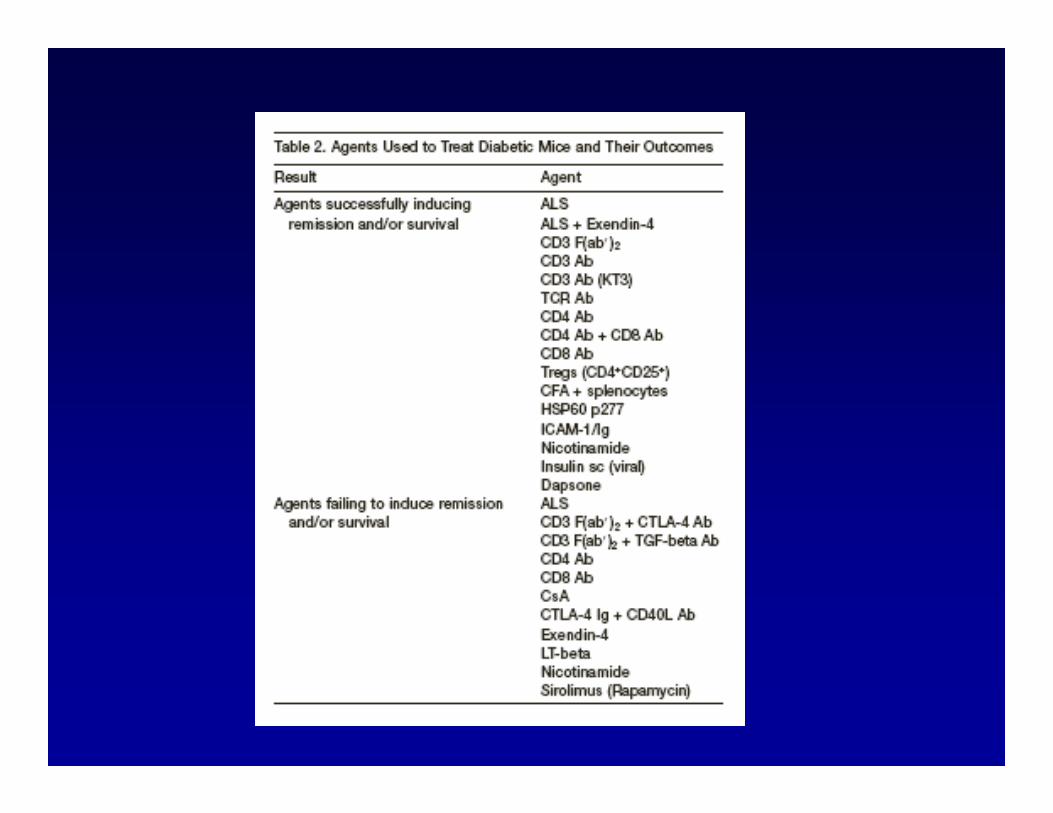
•• Over 25 years of experience with various Over 25 years of experience with various animal modelsanimal models–– StreptozotocinStreptozotocin inductioninduction–– BB ratBB rat–– NOD mouseNOD mouse
•• Limitations from inLimitations from in--bred strains, nonbred strains, non--primate primate modelsmodels
•• How does this translate to man?How does this translate to man?–– DosingDosing–– TimingTiming

NOD mouse mechanismsNOD mouse mechanisms
•• T cells are drivers and T cellT cells are drivers and T cell--deficient deficient mice do not get diseasemice do not get disease
•• Prevention vs. InterventionPrevention vs. Intervention
•• AntigenAntigen--specific tolerance? Insulin?specific tolerance? Insulin?
•• B cells as B cells as APCAPC’’ss??
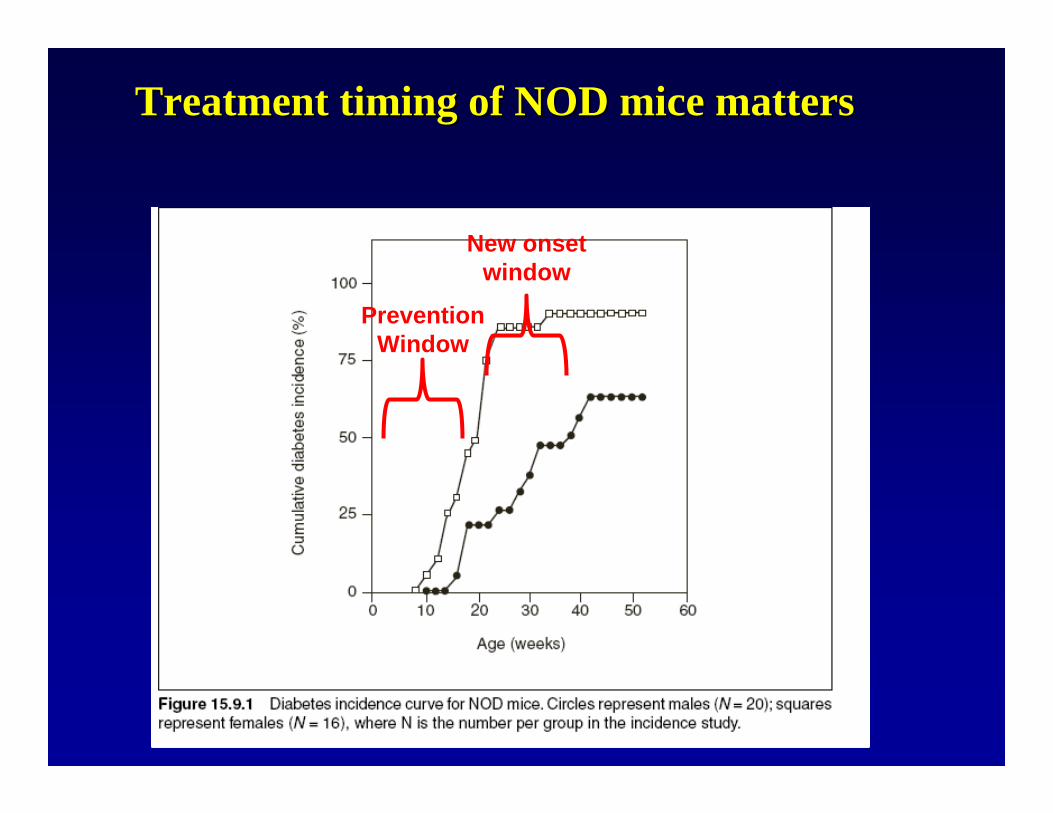
Treatment timing of NOD mice mattersTreatment timing of NOD mice matters
Prevention Window
New onset window
NOD mouse mechanismsNOD mouse mechanisms
•• Remember! Generally the cleaner your Remember! Generally the cleaner your NOD colony the higher the diabetes NOD colony the higher the diabetes incidenceincidence
•• Likewise: General inflammation can Likewise: General inflammation can lower incidence of diabetes. CFA lower incidence of diabetes. CFA prevents diabetes. Does your treatment prevents diabetes. Does your treatment prep have LPS????prep have LPS????

Interventions For Type 1 DMInterventions For Type 1 DM
%Beta CellMass
%Beta CellMass
Clinical Clinical DxDx
7575
5050
2525
00
100100
Abnormal IVGTTAbnormal IVGTT
YearsYears
AutoAbsAutoAbs
11oo
22oo
33oo
22oo
Dilemma For DM InterventionsDilemma For DM Interventions•• Attempts at early preventionAttempts at early prevention
–– Less likely to predict who will ultimately get DMLess likely to predict who will ultimately get DM–– Less aggressive intervention, such as dietary Less aggressive intervention, such as dietary
manipulation or antigenmanipulation or antigen--based therapy, more likely based therapy, more likely to be efficaciousto be efficacious
–– Clinical trials involve large number of patients are Clinical trials involve large number of patients are LONG LONG
•• Later stages of interventionLater stages of intervention–– Greater likelihood of predicting who will get DMGreater likelihood of predicting who will get DM–– Later intervention may require more aggressive and Later intervention may require more aggressive and
potentially toxic agents to have efficacypotentially toxic agents to have efficacy

Limitations For Clinical Trials In T1DMLimitations For Clinical Trials In T1DM
•• Existing therapy is available, and improvingExisting therapy is available, and improving–– Not a life threatening conditionNot a life threatening condition
•• Limited by lack of surrogate markers available to assess treatmeLimited by lack of surrogate markers available to assess treatment nt efficacyefficacy–– AutoAbsAutoAbs help with prediction of disease, but do not predict response tohelp with prediction of disease, but do not predict response to
therapytherapy–– Changes in circulating T cells or other parameters may not be reChanges in circulating T cells or other parameters may not be relevant levant
to local milieu in pancreasto local milieu in pancreas–– No direct visualization, via biopsy or imaging at presentNo direct visualization, via biopsy or imaging at present–– Have to wait for change in beta cell function over time, which tHave to wait for change in beta cell function over time, which takes at akes at
least 1least 1--2 yrs, but is e2 yrs, but is especially an issue in prevention studiesspecially an issue in prevention studies
•• For prevention, will need to find means to apply to general For prevention, will need to find means to apply to general population, not just first degree relativespopulation, not just first degree relatives–– 90% of new onset T1DM occurs in families without 90% of new onset T1DM occurs in families without probandproband
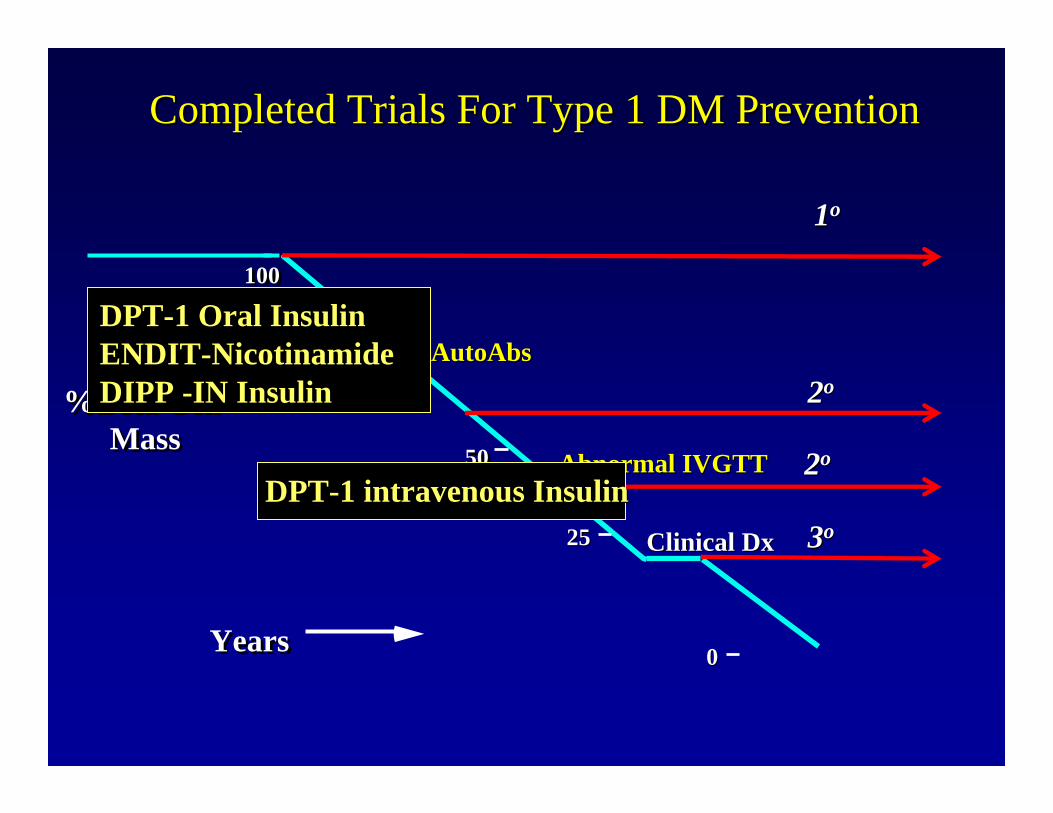
Completed Trials For Type 1 DM PreventionCompleted Trials For Type 1 DM Prevention
%Beta CellMass
%Beta CellMass
Clinical Clinical DxDx
7575
5050
2525
00
100100
Abnormal IVGTTAbnormal IVGTT
YearsYears
AutoAbsAutoAbs
11oo
22oo
33oo
22oo
DPTDPT--1 Oral Insulin1 Oral InsulinENDITENDIT--NicotinamideNicotinamideDIPP DIPP --IN InsulinIN Insulin
DPTDPT--1 intravenous Insulin1 intravenous Insulin

Rationale For InsulinRationale For Insulin•• Documented as possible antigen Documented as possible antigen
in T1DMin T1DM•• Effective for T1DM prevention Effective for T1DM prevention
in animal models, clinical pilot in animal models, clinical pilot studiesstudies
•• In newly diagnosed patients and In newly diagnosed patients and those in DCCT, intensive insulin those in DCCT, intensive insulin therapy prolonged honeymoontherapy prolonged honeymoon
•• Well studied, safe, and available Well studied, safe, and available in large quantitiesin large quantities
Can insulin prevent or delay onset of T1DM?

Effect of Insulin Injections on Effect of Insulin Injections on Diabetes & InsulitisDiabetes & Insulitis
0102030405060708090
100
Placebo Insulin
% D
iabe
tes
Female NOD MiceFemale NOD Mice
AtkinsonAtkinson
0
0.5
1
1.5
2
2.5
3
Placebo Insulin
Insu
litis
Sco
re
DPTDPT--1 Strategy1 Strategy
•• Screen 1Screen 1stst degree relatives for degree relatives for AutoAbsAutoAbs•• Stage by immunological, genetic, and metabolic criteriaStage by immunological, genetic, and metabolic criteria•• Stratify intervention according to riskStratify intervention according to risk
–– High risk, > 50% chance of DM in next 5 yrsHigh risk, > 50% chance of DM in next 5 yrs•• ICA+, low FPIRICA+, low FPIR•• Randomized to trial with Randomized to trial with parenteralparenteral insulininsulin
–– Intermediate risk, 25Intermediate risk, 25--50% chance of DM in next 5 50% chance of DM in next 5 yrsyrs
•• AutoAbsAutoAbs ++•• Randomized to trial with oral insulinRandomized to trial with oral insulin

DPTDPT--1 Parenteral Study 1 Parenteral Study –– Time to DiabetesTime to DiabetesBy TreatmentBy Treatment
1.01.0
0.90.9
0.80.8
0.70.7
0.60.6
0.50.5
0.40.4
0.30.3
0.20.2
0.10.1
0.00.0169169170170
144144131131
9696101101
69696969
39394040
13131414 11
Number at RiskNumber at Risk
Surv
ival
Dis
trib
utio
n Fu
nctio
nSu
rviv
al D
istr
ibut
ion
Func
tion
PP-- Value= 0.796Value= 0.796(Log Rank Test)(Log Rank Test)
InterventionInterventionObservationObservation
00 11 22 33 44 55 66
Years FollowedYears Followed
STRATA:STRATA: InterventionIntervention ObservationObservation
ControlControl
TreatedTreated
New Engl J Med 2002; 346:1685-91

Implications Of DPTImplications Of DPT--1 1 ParenteralParenteral TrialTrial
•• Can conduct large clinical trials for type 1 DM prevention in USCan conduct large clinical trials for type 1 DM prevention in USAA
•• Predictive strategies workedPredictive strategies worked–– able to identify a high risk cohort and keep them enrolledable to identify a high risk cohort and keep them enrolled
•• Status of insulin:Status of insulin:–– parenteralparenteral protocol is safe but not efficaciousprotocol is safe but not efficacious–– would different dosing regimen or alternate route have been effewould different dosing regimen or alternate route have been effective?ctive?
•• dose limitations from metabolic effects if given dose limitations from metabolic effects if given subQsubQ–– variants of insulin therapy still to be consideredvariants of insulin therapy still to be considered
•• B chain, peptides B chain, peptides •• Insulin analog B25 Insulin analog B25 PhePhe AspAsp
–– Does not bind to insulin receptorDoes not bind to insulin receptor–– Efficacious in NOD mouse at 20X dose used in DPTEfficacious in NOD mouse at 20X dose used in DPT--11
KarounosKarounos et al, JCI 1997et al, JCI 1997

What about oral insulin?What about oral insulin?
•• Subjects are earlier in the course of beta Subjects are earlier in the course of beta cell destructioncell destruction
•• Oral insulin has no metabolic effectsOral insulin has no metabolic effects•• May induce tolerance by presentation of May induce tolerance by presentation of
peptides to immune system via gutpeptides to immune system via gut•• Effective in animal modelsEffective in animal models

OOralral ToleranceTolerance: Mode of Action: Mode of ActionProtective Cytokines
Insulin Producingβ-cells
Oral Antigen
Inhibition of β-CellAutoimmunity andPrevention of DM
Autoimmune Lymphocytes
Regulatory (Th2 / Th3) Lymphocytes Producing
Protective Cytokines

Skyler et al, Diabetes Care 2005, 28: 1068
Effect Of Oral Insulin On Progression To T1DMEffect Of Oral Insulin On Progression To T1DM

Skyler et al, Diabetes Care 2005, 28: 1068
Effect Of Oral Insulin On Progression To T1DMEffect Of Oral Insulin On Progression To T1DMOnly subjects with IAA Only subjects with IAA >> 8080
Oral insulin may delay DM onset ~ 4.5 yrs

Ongoing Or PlannedOngoing Or PlannedPrimary Prevention Trials For Type 1 DMPrimary Prevention Trials For Type 1 DM
%Beta CellMass
%Beta CellMass
GeneticGeneticPredispositionPredisposition
Clinical Clinical DxDx
7575
5050
2525
00
100100
Abnormal IVGTTAbnormal IVGTT
YearsYears
AutoAbsAutoAbs
11ooTRIGRTRIGRNIPNIPPOINTPOINTBabyDietBabyDietVitamin DVitamin D

Natural Natural HistoryHistory Of Type 1 DMOf Type 1 DM
%Beta CellMass
%Beta CellMass
GeneticGeneticPredispositionPredisposition
EnvironmentalEnvironmentalInsultInsult
Clinical Clinical DxDx
7575
5050
2525
00
100100
YearsYears
HoneymoonHoneymoon

‘‘New OnsetNew Onset’’ Vs Vs ‘‘At RiskAt Risk’’ TrialsTrials
•• Easier to find subjects, may be more motivated for recruitmentEasier to find subjects, may be more motivated for recruitment
•• By the time of diagnosis, there may be By the time of diagnosis, there may be >> 1515--40% of beta cell function 40% of beta cell function remainingremaining
•• Maintenance of beta cell function over time, even if on supplemeMaintenance of beta cell function over time, even if on supplemental insulin, ntal insulin, is valuableis valuable–– Decrease risk of hypoglycemia, lower HbA1C, lower risk for Decrease risk of hypoglycemia, lower HbA1C, lower risk for
complicationscomplications–– Metabolic memory: early control can have long term effectsMetabolic memory: early control can have long term effects
•• May be valuable lessons learned regarding safety and efficacyMay be valuable lessons learned regarding safety and efficacy–– Past experience with cyclosporinePast experience with cyclosporine–– Can prolong honeymoonCan prolong honeymoon
•• Not all respond; toxicities; effect wanes over time or when off Not all respond; toxicities; effect wanes over time or when off drugdrug–– Some Some RxsRxs may accelerate disease processmay accelerate disease process
•• Interventions at this stage may guide us for prevention studiesInterventions at this stage may guide us for prevention studies
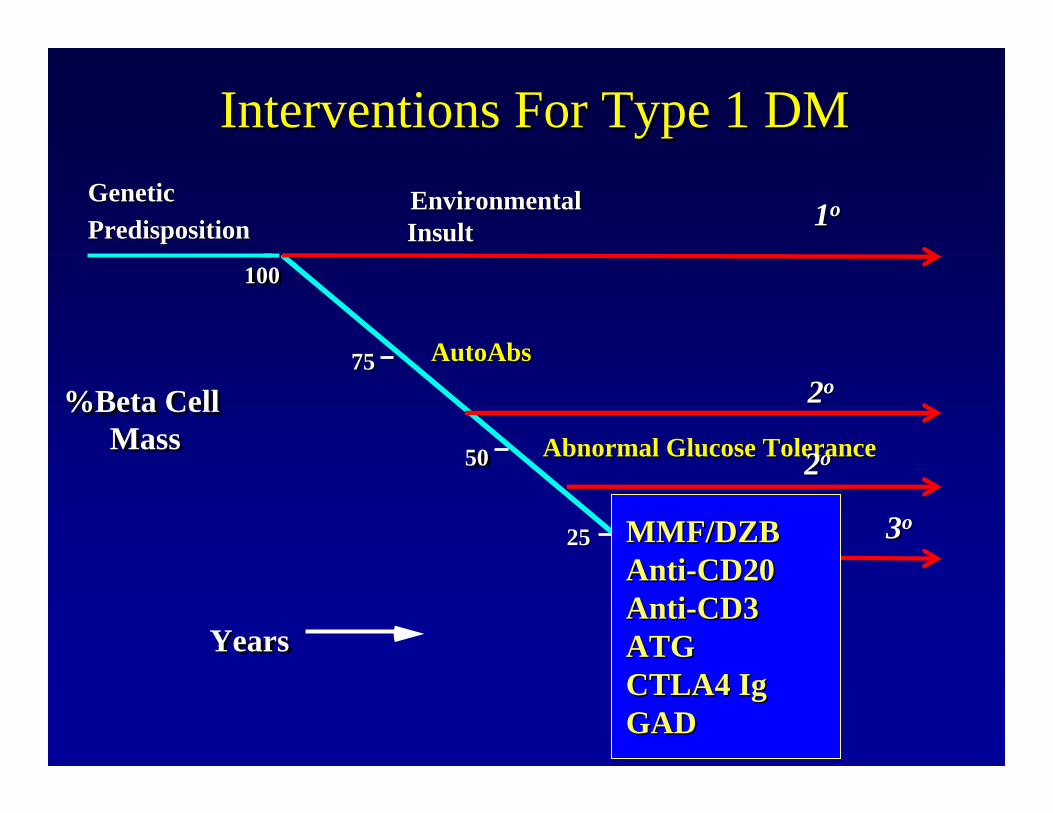
Interventions For Type 1 DMInterventions For Type 1 DM
%Beta CellMass
%Beta CellMass
GeneticGeneticPredispositionPredisposition
EnvironmentalEnvironmentalInsultInsult
Clinical Clinical DxDx
7575
5050
2525
00
100100
Abnormal Glucose ToleranceAbnormal Glucose Tolerance
YearsYears
AutoAbsAutoAbs
11oo
22oo
33oo
22oo
MMF/DZBMMF/DZBAntiAnti--CD20CD20AntiAnti--CD3CD3ATG ATG CTLA4 CTLA4 IgIgGADGAD
33oo

Antigen Presenting Cell
T Cell
*
*
*
*
*
Activation Of Auto-reactive T Cells
hOKT3hOKT3γγ1(ala1(ala--ala)ala)•• Monoclonal Monoclonal AbAb directed against CD3directed against CD3--εε epitopeepitope of the of the
T cell receptor (from OKT3)T cell receptor (from OKT3)•• Humanized by engrafting amino acids of the combining Humanized by engrafting amino acids of the combining
site onto human IgG1 backbonesite onto human IgG1 backbone•• Two amino acids in Two amino acids in FcFc portion of portion of IgIg changed to Ala to changed to Ala to
render render MabMab FcRFcR nonnon--bindingbinding–– reduces cytokine release syndromereduces cytokine release syndrome
•• Mechanism of action not fully understoodMechanism of action not fully understood
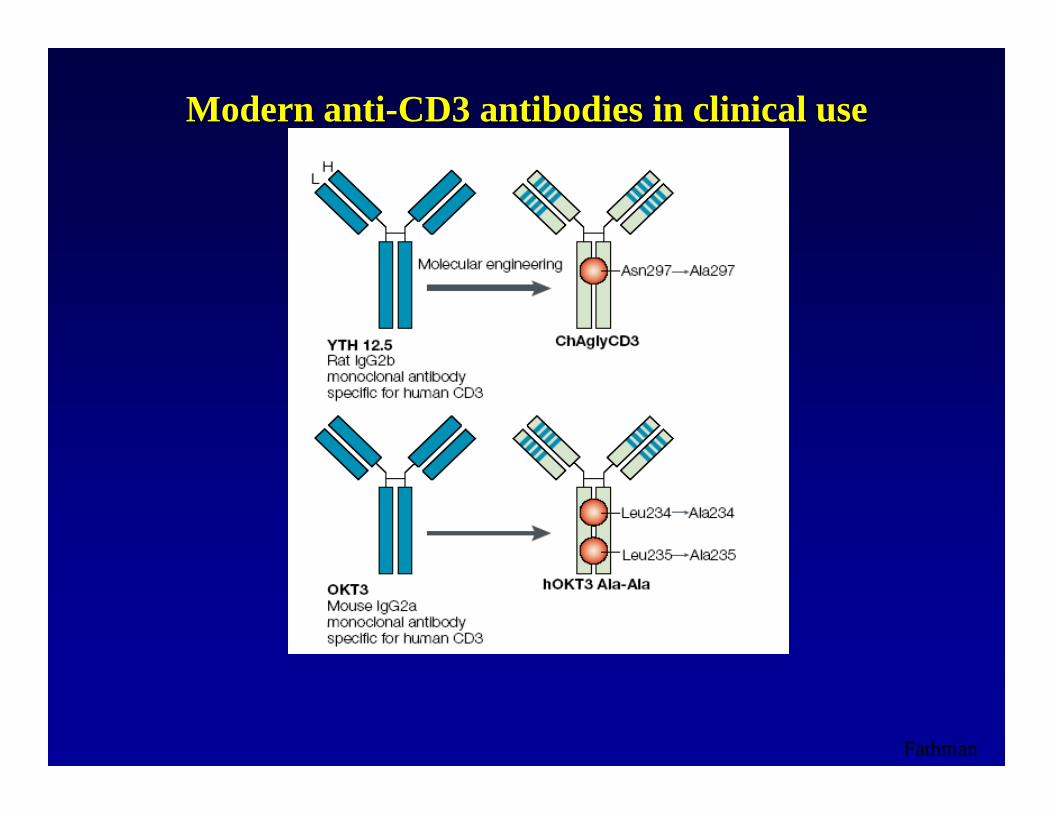
Modern antiModern anti--CD3 antibodies in clinical useCD3 antibodies in clinical use
Fathman
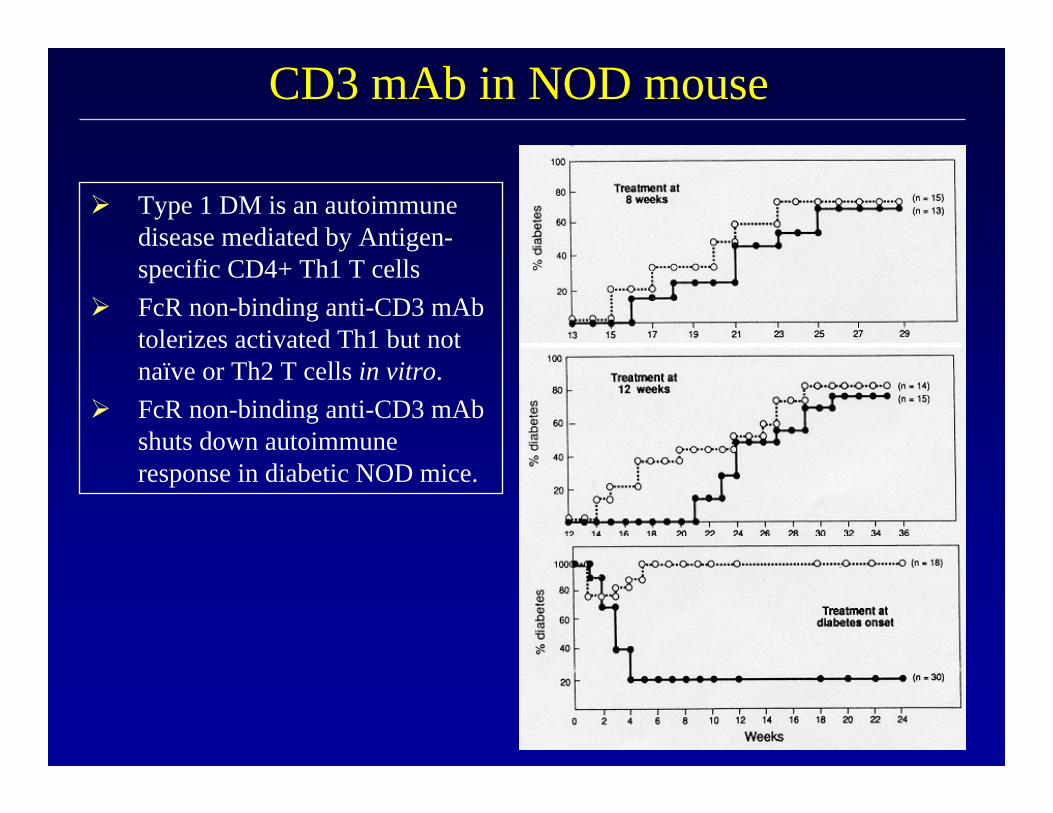
CD3 CD3 mAbmAb in NOD mousein NOD mouse
Type 1 DM is an autoimmune disease mediated by Antigen-specific CD4+ Th1 T cellsFcR non-binding anti-CD3 mAbtolerizes activated Th1 but not naïve or Th2 T cells in vitro.FcR non-binding anti-CD3 mAbshuts down autoimmune response in diabetic NOD mice.

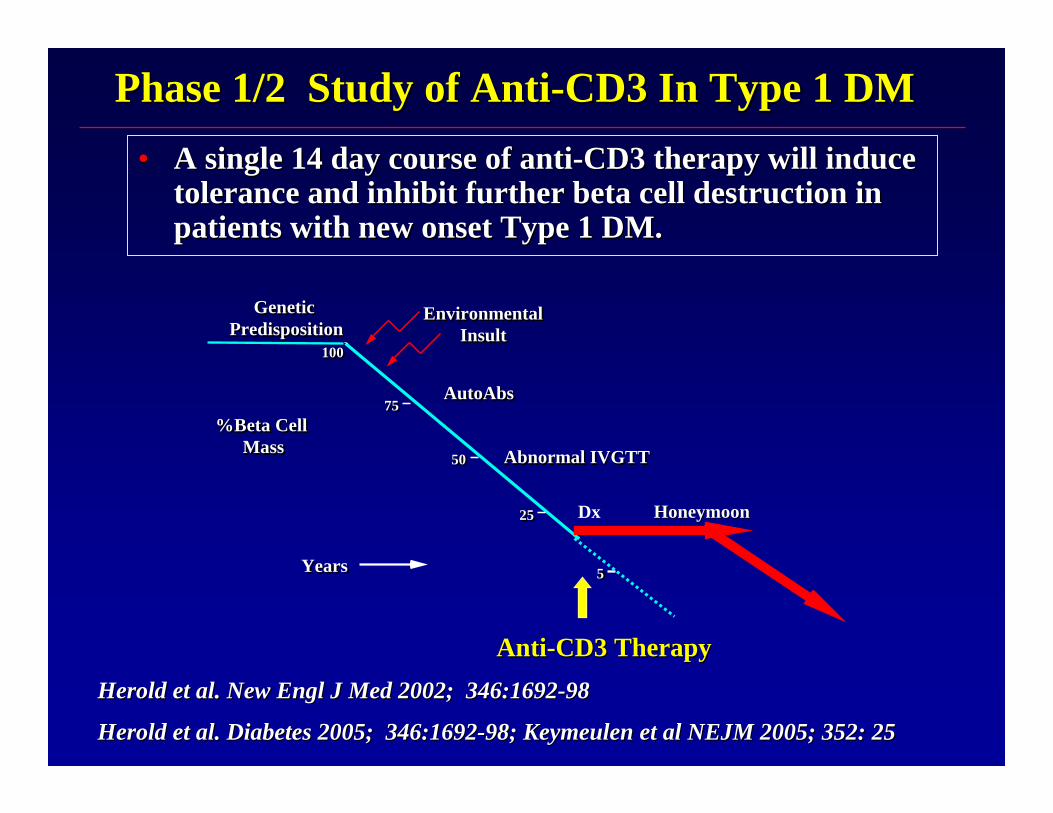
Phase 1/2 Study of AntiPhase 1/2 Study of Anti--CD3 In Type 1 DMCD3 In Type 1 DM•• A single 14 day course of antiA single 14 day course of anti--CD3 therapy will induce CD3 therapy will induce
tolerance and inhibit further beta cell destruction in tolerance and inhibit further beta cell destruction in patients with new onset Type 1 DM. patients with new onset Type 1 DM.
%Beta CellMass
%Beta CellMass
GeneticPredisposition
GeneticPredisposition
EnvironmentalInsult
EnvironmentalInsult
Dx
7575
5050
2525
05
100100
Abnormal IVGTTAbnormal IVGTT
YearsYears
HoneymoonHoneymoon
AutoAbsAutoAbs
AntiAnti--CD3 TherapyCD3 Therapy
?

Changes In Incremental AUC CChanges In Incremental AUC C--peptide insulin From Phase I/II Trial peptide insulin From Phase I/II Trial
In New Onset T1DMIn New Onset T1DM
0
20
40
60
80
100
120
140
160
Cel
l Mea
n
AUC@0 AUC@6 AUC@12Cell
controldrug
AU
C in
MM
TT (p
mol
/ml/2
40m
in)
000 6 mos 12 mos

Changes In CChanges In C--peptide insulin peptide insulin AUC to MMTT Over TimeAUC to MMTT Over Time
0
50
100
150
0 6 12 18 24
Months
AU
C (p
mol
/ml/2
40m
in)
drug
control
Phase 1/2 Study of AntiPhase 1/2 Study of Anti--CD3 In Type 1 DMCD3 In Type 1 DM•• A single 14 day course of antiA single 14 day course of anti--CD3 therapy will induce CD3 therapy will induce
tolerance and inhibit further beta cell destruction in tolerance and inhibit further beta cell destruction in patients with new onset Type 1 DM. patients with new onset Type 1 DM.
%Beta CellMass
%Beta CellMass
GeneticPredisposition
GeneticPredisposition
EnvironmentalInsult
EnvironmentalInsult
Dx
7575
5050
2525
05
100100
Abnormal IVGTTAbnormal IVGTT
YearsYears
HoneymoonHoneymoon
AutoAbsAutoAbs
AntiAnti--CD3 TherapyCD3 TherapyHerold et al. New Herold et al. New EnglEngl J Med 2002; 346:1692J Med 2002; 346:1692--9898
Herold et al. Diabetes 2005; 346:1692Herold et al. Diabetes 2005; 346:1692--98; 98; KeymeulenKeymeulen et al NEJM 2005; 352: 25et al NEJM 2005; 352: 25

What is antiWhat is anti--CD3 doing?CD3 doing?

Changes in ALC with treatment
Day
0 10 20 30 40 50 60 70
ALC
% b
asal
20
40
60
80
100
120
140
Change In Lymphocyte Count With Drug TreatmentChange In Lymphocyte Count With Drug Treatment
% C
hang
e in
B
asal
ALC
Days

TH1Cells
IFN-γ, IL-2DestructiveCytokines
Cell mediated immunity
TH2Cells
IL-4, IL-5, IL-10 TGF-β
TH3Cells
ProtectiveCytokines
Humoral immunity
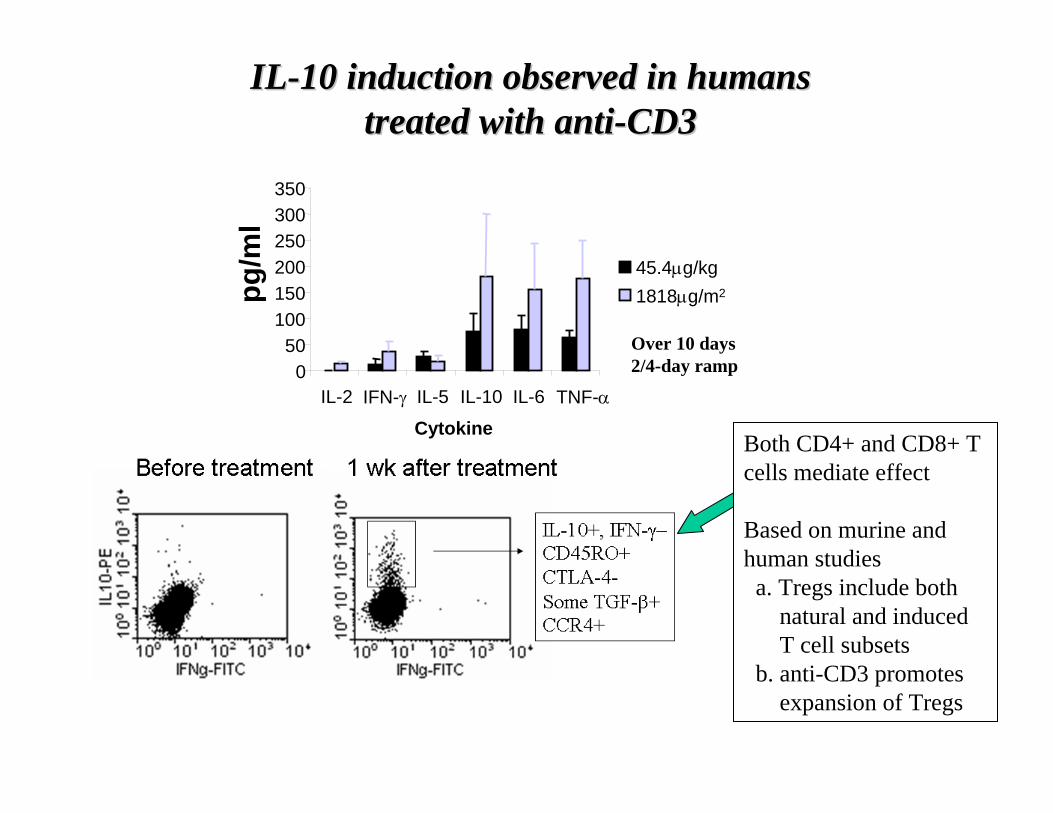
ILIL--10 induction observed in humans10 induction observed in humanstreated with antitreated with anti--CD3CD3
pg/m
l
050
100150200250300350
IL-2 IFN-γ IL-5 IL-10 IL-6 TNF-α
Cytokine
45.4μg/kg1818μg/m2
Over 10 days2/4-day ramp
Both CD4+ and CD8+ T cells mediate effect
Based on murine and human studies a. Tregs include both
natural and inducedT cell subsets
b. anti-CD3 promotes expansion of Tregs
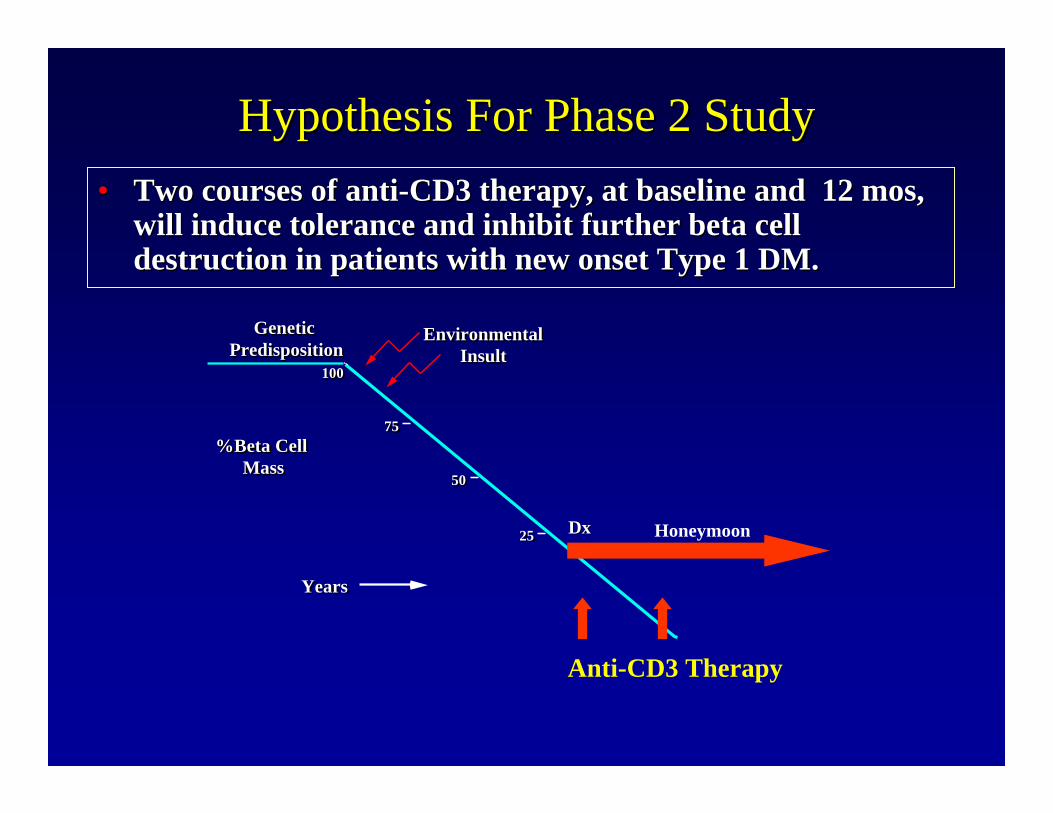
Hypothesis For Phase 2 StudyHypothesis For Phase 2 Study•• Two courses of antiTwo courses of anti--CD3 therapy, at baseline and 12 CD3 therapy, at baseline and 12 mosmos, ,
will induce tolerance and inhibit further beta cell will induce tolerance and inhibit further beta cell destruction in patients with new onset Type 1 DM. destruction in patients with new onset Type 1 DM.
%Beta CellMass
%Beta CellMass
GeneticPredisposition
GeneticPredisposition
EnvironmentalInsult
EnvironmentalInsult
7575
5050
2525
100100
YearsYears
Honeymoon
Anti-CD3 Therapy
DxDx

Where Do We Go From Here With Where Do We Go From Here With AntiAnti--CD3?CD3?
•• Does therapy have to be used so early in the courseDoes therapy have to be used so early in the course……what is the what is the window of opportunity?window of opportunity?–– Clinical trial with first dose given Clinical trial with first dose given 4 to 12 4 to 12 mosmos from diagnosisfrom diagnosis
•• Can we simplify the dosing regimen?Can we simplify the dosing regimen?•• Can we improve efficacy if it is combined with an agent that worCan we improve efficacy if it is combined with an agent that works ks
via another mechanism?via another mechanism?–– AntiAnti--CD3 + CD3 + ExenatideExenatide–– AntiAnti--CD3 + Antigen (insulin or GAD)CD3 + Antigen (insulin or GAD)
•• Can it prevent type 1 diabetes?Can it prevent type 1 diabetes?–– Trial for those with + Trial for those with + Ab(sAb(s) and IGT) and IGT
•• Will it be helpful for pancreas or islet transplantation?Will it be helpful for pancreas or islet transplantation?•• How does this work?How does this work?
–– 25% are non25% are non--respondersresponders——is there a surrogate marker to identify is there a surrogate marker to identify these pts, and offer other therapies these pts, and offer other therapies

Halloran N Engl J Med 2004, 351: 2715-29
Potential TherapiesPotential TherapiesAnti-CD20
T Cell
*
*
*
*
*
Anti-Thymocyte Globulin(S. Gitelman UCSF)

AntiAnti--ThymocyteThymocyte Globulin (ATG) For New Onset T1DMGlobulin (ATG) For New Onset T1DMRationaleRationale
•• ATG induces tolerance in NOD mouse, BB rat with new onset DMATG induces tolerance in NOD mouse, BB rat with new onset DM
•• Promising clinical studies with ATG in autoimmunity, transplantPromising clinical studies with ATG in autoimmunity, transplant–– ““partialpartial”” tolerance in transplantationtolerance in transplantation–– AplasticAplastic anemiaanemia–– Type 1 DMType 1 DM
•• Pilot studies from Eisenbarth 1985, Saudek 2004, Pilot studies from Eisenbarth 1985, Saudek 2004, VolaterelliVolaterelli 20200707
•• Multiple Potential MechanismsMultiple Potential Mechanisms–– TT--cell depletion, eliminates cell depletion, eliminates autoreactiveautoreactive, pathogenic T, pathogenic T--cellscells–– Modulation, Modulation, anergyanergy of remaining Tof remaining T--cellscells–– Homeostatic proliferation, possible induction of T regulatory ceHomeostatic proliferation, possible induction of T regulatory cellslls–– May affect TMay affect T--cell migrationcell migration–– May affect antigenMay affect antigen--presenting cell functionpresenting cell function

Antigen Presenting Cell
T Cell
*
*
*
*
*
Activation Of The Immune System
B Cells ?


T Cell
*
*
*
*
*
T Regulatory Cell

Reversal of diabetes in NOD mice with Reversal of diabetes in NOD mice with TregsTregs
SummarySummary
•• Series of prevention and new onset trials Series of prevention and new onset trials launched to alter the natural course of launched to alter the natural course of T1DMT1DM
•• AntiAnti--CD3 studies are encouragingCD3 studies are encouraging•• Many other agents to evaluate, either Many other agents to evaluate, either
alone or in combinationalone or in combination•• Current strategy is to use new onset Current strategy is to use new onset
studies as the mainstay for trials (faster, studies as the mainstay for trials (faster, lower subject numbers)lower subject numbers)

Summary (cont)Summary (cont)
•• Current new onset studies completed Current new onset studies completed enrollment:enrollment:–– AntiAnti--CD20 (CD20 (RituximabRituximab))–– MMFMMF--DZBDZB–– CTLA4CTLA4--Ig (Ig (BelateceptBelatecept))
•• New onset studies recruitingNew onset studies recruiting–– Phase II antiPhase II anti--CD3 (doses one year apart)CD3 (doses one year apart)–– ThymoglobulinThymoglobulin
•• Coming soon in new onset diabetesComing soon in new onset diabetes–– GAD antigen administrationGAD antigen administration

Summary (cont)Summary (cont)
•• Current prevention studies recruitingCurrent prevention studies recruiting–– Oral insulin administrationOral insulin administration
•• Prevention studies recruiting completedPrevention studies recruiting completed–– NIP (nutritional intervention study)NIP (nutritional intervention study)
•• The future??The future??–– Regulatory T cell treatment of type 1 Regulatory T cell treatment of type 1
diabetesdiabetes
ResourcesResources
Immune Tolerance Network
http://www.diabetestrialnet.org
http://www.immunetolerance.org
http://www.diabetes.ucsf.edu/