impact of antenatal selective serotonin reuptake inhibitor exposure on pregnancy outcomes in mice
TRANSCRIPT

IeS
Oo
Sdtdcl
Rd
CO
Cdndtpfca
FMGtP(PU
PMM
Ra
RMOUY
Ta
0©d
SMFM Papers www.AJOG.org
mpact of antenatal selective serotonin reuptake inhibitorxposure on pregnancy outcomes in mice
amuel Bauer, MD; Catherine Monk, PhD; Mark Ansorge, PhD; Cynthia Gyamfi, MD; Michael Myers, PhD
h(HH
Ctw
K
BJECTIVE: This study investigates fluoxetine (FLX) exposure as an eti-logy for altered gestational length and adverse pregnancy outcomes.
TUDY DESIGN: Two experiments were performed exposing mice torinking water (H2O) or H2O�FLX. Primary outcomes included gesta-ional length, litter size, and live birth rate. In experiment 1, time-matedams were monitored for spontaneous birth, and gestational length wasalculated. In experiment 2, dams were dissected on day 14 to verifyitter size and qualities of embryo implantation.
ESULTS: There was no difference in gestational length between H2O
bstet Gynecol 2010;203:375.e1-4.
cls(osd
crphuTSbttf
tsnapolsScaehad higher rates of s
oi: 10.1016/j.ajog.2010.05.008
ours), P � .70. Mean litter size was decreased in H2O�FLX dams4.1 � 1.3/litter) compared to H2O dams (5.5 � 1.9/litter), P � .04.
2O�FLX dams were less likely to have live births (25.4%) compared to
2O dams (49.3%), P � .01.
ONCLUSION: Antenatal FLX exposure did not statistically alter gesta-ional length, but did affect litter size and spontaneous loss in mice. Thisarrants further investigation.
ey words: birth outcomes, mouse model, pregnancy, preterm birth,
ams (480.7 � 13.2 hours) and H2O�FLX dams (483.5 � 10.1 selective serotonin reuptake inhibitorite this article as: Bauer S, Monk C, Ansorge M, et al. Impact of antenatal selective serotonin reuptake inhibitor exposure on pregnancy outcomes in mice. Am J
tw
daacsnbteoatcspiimot
MTemmNapE
linical depression is a commoncondition among women of repro-
uctive age. Between 14-23% of preg-ant women will experience a depressiveisorder during pregnancy.1 Althoughhere is no standard screening protocol,renatal depression is one of the most
requently encountered medical compli-ations during pregnancy. The trend ofntidepressant use during pregnancy has
rom the Division of Maternal-Fetaledicine, Department of Obstetrics andynecology (Drs Bauer and Gyamfi), and
he Division of Developmentalsychobiology, Department of PsychiatryDrs Monk, Ansorge, and Myers), College ofhysicians and Surgeons, Columbianiversity, New York, NY.
resented as a poster at the 30th Annualeeting of the Society for Maternal-Fetaledicine, Chicago, IL, Feb. 1-6, 2010.
eceived March 1, 2010; revised April 8, 2010;ccepted May 6, 2010.
eprints: Samuel Bauer, MD, Division ofaternal-Fetal Medicine, Department ofbstetrics and Gynecology, Columbianiversity, 622 W.168 St., PH 16–66, Nework, NY 10032. [email protected].
he study was supported by the Wharton Fundt Columbia University.
002-9378/$36.002010 Mosby, Inc. All rights reserved.
ontinued to rise over the last decadeargely as a result of the increased use ofelective serotonin reuptake inhibitorsSSRIs).2,3 In 2003, approximately 13%f women took an antidepressant atome point in pregnancy, a rate that hasoubled since 1999.4
While several research studies have fo-used on the potential maternal and fetalisks of SSRI use in pregnancy, includingossible teratogenic effects, other studiesave suggested that the increase in SSRIse may also affect prematurity rates.5-7
he rate of preterm birth in the Unitedtates is approximately 12.7% of liveirths, which is an increase of �15% inhe last decade.8 This study will focus onhe effect of SSRI exposure as an etiologyor preterm birth in a mouse model.
Conflicting data exist linking SSRI useo an increased risk for preterm birth,hortened gestational length, or sponta-eous fetal loss.9-15 While Chambers etl15 showed that third-trimester SSRI ex-osure was associated with higher ratesf premature delivery, Malm et al16 pub-
ished a conflicting population-basedtudy of pregnant women exposed toSRIs vs matched controls finding no in-reased risk of preterm birth. Two meta-nalyses have demonstrated that womenxposed to SSRIs in the first trimester
pontaneous abor- e
OCTOBER 2010 Americ
ions when compared to a group ofomen who were not exposed.17,18
Deficiencies within the literature existemonstrating an association betweenntenatal fluoxetine (FLX) exposure anddverse pregnancy outcomes. Histori-ally, studies have not accounted for ob-tetric factors relating to preterm birth,amely, history of a previous pretermirth or prior preterm premature rup-ure of membranes; nor have they differ-ntiated among a spontaneous, indicted,r elective preterm birth. While thesend many other factors are difficulto control in human studies, causal asso-iations between FLX exposure andhortened gestational length can be ap-roached using animal models. Accord-
ngly, this study was initiated to study thempact of antenatal FLX exposure in a
ouse model and to begin investigationsf mechanistic pathways if an associa-ion was confirmed.
ATERIALS AND METHODSwo prospective, blinded observationalxperiments were performed. In experi-ent 1, 52 virgin female 129/SvEvTacice (Taconic Farms, Germantown,ew York) were time-mated (2 females
nd 1 male per cage) over 4 hours justrior to the end of the daily light cycle.ach female was examined for the pres-
nce of an ejaculatory plug in the vagina.an Journal of Obstetrics & Gynecology 375.e1
Ttdotc(atbrctduds
SmjcrGtcsdniHfiptawia
bsadttmbboFFlebcuaialm1o
laUiwswmwoC
watnmtsrnpmeiFnc
RTpiganmlfHa1phe�
com
SMFM Papers www.AJOG.org
3
he plug, composed of coagulated secre-ions from male accessory sex glands, in-icated that coitus and ejaculation hadccurred. Dams were randomly assignedo 1 of 2 cohorts. Group 1 (n � 29) hadontinuous access to drinking waterH2O) only, while group 2 (n � 23) hadccess to H2O�FLX. Dams were moni-ored every 12 hours for spontaneousirth and length of gestation, which wereecorded and analyzed. The individualages were monitored for the date andime of birth every 4 hours starting onay 18. The mouse dams and pups weretilized in subsequent experiments, in-ependent of this study, and ultimatelyacrificed.
In experiment 2, 76 virgin female 129/vEvTac mice (Taconic Farms) wereated (2 females and 1 male per cage)
ust prior to the end of the daily light cy-le. After plug confirmation, dams wereandomly assigned to 1 of 2 cohorts.roup 1 (n � 40) had continuous access
o H2O, while group 2 (n � 36) had ac-ess to H2O�FLX. Plugged dams wereacrificed, dissected, and analyzed onay 14 following mating to verify preg-ancy and assess for litter sizes and qual-
ties of embryo implantation. H2O or
2O�FLX was initiated after plug con-rmation and continued until the end ofregnancy. FLX was dissolved in H2O athe dose of 4 mg/50 mL to achieve anpproximate 10 mg/kg/d dosing. FLXas freely available in the animal’s H2O
n opaque bottles to protect from light
TABLEPregnancy outcomes
Outcome
Experiment 1 (n � 52)
Drinking wateronly (n � 29)
Drinkplus(n �
Length of gestation, h 480.7 � 13.2 483....................................................................................................................
Mean weight gain atgestational day 14, g
6.1 � 2.7 4.
...................................................................................................................
Live birth rate (confirmedpregnancy/plugged)
44.8% (13/29) 17.
...................................................................................................................
Mean litter size (pups/litter)
5.8 � 1.7 4.
...................................................................................................................
Missed abortion rate NA NA...................................................................................................................
NA, not applicable.
Bauer. Antenatal SSRI exposure impact on pregnancy out
nd changed weekly. FLX was chosen C
75.e2 American Journal of Obstetrics & Gynecolo
ecause it is the most commonly pre-cribed antidepressant during pregnancynd because of its extended half-life. Theosing regimen utilized by our labora-ory and others has repetitively producedherapeutically relevant blood levels in
ice. FLX and the metabolite levels haveeen measured in serum and wholerain and serum, and it has been previ-usly shown that steady state for bothLX is achieved by 5 days of receivingLX in the H2O (10 mg/kg/d), as serum
evels after 5 or 90 days of treatment arequivalent. FLX levels were determinedy liquid chromatography with fluores-ence detection.19,20 Detection of a cop-latory plug designated gestational daynd time 0. The mated mice were housedndividually and were weighed weeklynd at the time of delivery. The averageength of gestation of a 129/SvEvTac
ouse is 480 hours, and the average29/SvEvTac dam produces a litter sizef 6.4 � 0.88 pups (Taconic Farms).Animals were maintained in a 12-hour
ight and dark cycle in a temperature-nd humidity-controlled environment.nlike the animal care technicians, the
ndividuals observing the pup deliveriesere blinded and unaware of the compo-
ition of the subjects’ H2O. The animalsere fed with standard food pellets. Ani-al testing was conducted in accordanceith the National Institutes of Health lab-ratory animal care guidelines and witholumbia University Institutional Animal
Experiment 2 (n � 76)
waterxetine
PDrinking wateronly (n � 40)
Drinking waterplus fluoxetine(n � 36)
10.1 .70 NA NA.........................................................................................................................
1.3 .44 6.1 � 2.4 4.9 � 1.0
.........................................................................................................................
4/23) .04 52.5% (21/40) 30.6% (11/36)
.........................................................................................................................
1.7 .22 5.5 � 1.9 4.1 � 1.3
.........................................................................................................................
NA 0.0% (0/21) 18.2% (2/11).........................................................................................................................
es in mice. Am J Obstet Gynecol 2010.
are and Use Committee approval. b
gy OCTOBER 2010
Based on pilot data, a power analysisas performed, with an alpha of 0.05,
nd a beta of 0.80, and it was determinedhat a minimum of 21 dams would beeeded in each group for each experi-ent to demonstrate a decrease in gesta-
ional age by 1.1 days or 5%, for a totalample size of 42 dams. The live birthate was calculated as the ratio of preg-ant dams to the total number oflugged dams. The data are expressed asean � SD. The significance of differ-
nces among the groups was assessed us-ng 1-way analysis of variance test andisher’s exact test. The criterion for sig-ificance for all analyses was P � .05. Theriterion for a trend was .05 � P � .1.
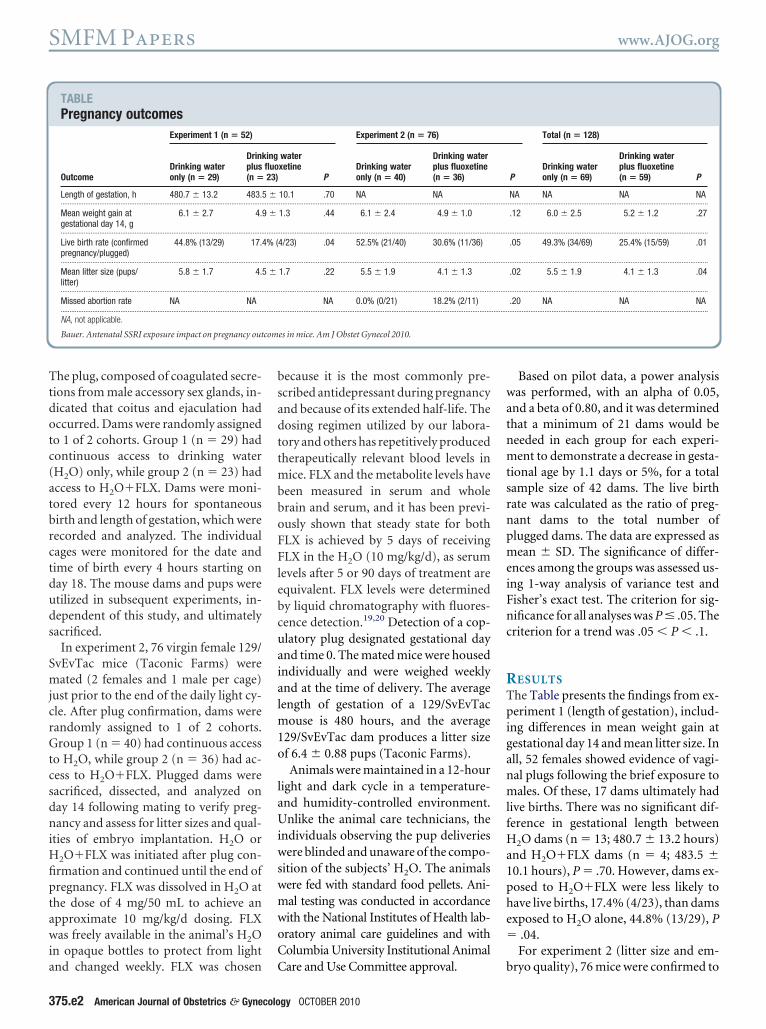
ESULTShe Table presents the findings from ex-eriment 1 (length of gestation), includ-
ng differences in mean weight gain atestational day 14 and mean litter size. Inll, 52 females showed evidence of vagi-al plugs following the brief exposure toales. Of these, 17 dams ultimately had
ive births. There was no significant dif-erence in gestational length between
2O dams (n � 13; 480.7 � 13.2 hours)nd H2O�FLX dams (n � 4; 483.5 �0.1 hours), P � .70. However, dams ex-osed to H2O�FLX were less likely toave live births, 17.4% (4/23), than damsxposed to H2O alone, 44.8% (13/29), P
.04.For experiment 2 (litter size and em-
Total (n � 128)
PDrinking wateronly (n � 69)
Drinking waterplus fluoxetine(n � 59) P
NA NA NA NA..................................................................................................................
.12 6.0 � 2.5 5.2 � 1.2 .27
..................................................................................................................
.05 49.3% (34/69) 25.4% (15/59) .01
..................................................................................................................
.02 5.5 � 1.9 4.1 � 1.3 .04
..................................................................................................................
.20 NA NA NA..................................................................................................................
ingfluo23)
5 �......... .........
9 �
......... .........
4% (
......... .........
5 �
......... .........
......... .........
ryo quality), 76 mice were confirmed to

buclld3tWhpvdHacn
swpbpcatddmdchs
CLcwmlnctHHalfdlctaha
cmeacal
1tortbuaicscu
nsifmtlmpnstsddwtpm
tatwtwtwspca
tFritflltrdFpty
dmttsacpbvaohFmestmiSmmmcetumbntvp
pltF
www.AJOG.org SMFM Papers
e pregnant by presence of a vaginal cop-latory plug. Mean litter size was de-reased in H2O�FLX dams (4.1 � 1.3/itter) compared to H2O dams (5.5 � 1.9/itter), P � .02. Live birth rates wereecreased in dams exposed to H2O�FLX,0.6%(11/36), comparedtodamsexposedo H2O alone, 52.5% (21/40), P � .05.
hile not statistically significant, uterineorn dissection to assess for nonviableregnancy tissue or missed abortion re-ealed an 18.2% (2/11) rate in H2O�FLXams compared to a 0.0% (0/21) rate in
2O dams, P � .20. The mean weight gaint day 14 in H2O�FLX dams (4.9 � 1.0 g)ompared to H2O dams (6.1 � 2.4 g) didot reach statistical significance, P � .12.Given the identical experimental de-
ign, data between experiments 1 and 2ere combined to increase statisticalower. For the combined dataset, liveirth rates were decreased in dams ex-osed to H2O�FLX, 25.4% (15/59),ompared to dams exposed to H2Olone, 49.3% (34/69), P � .01. Mean lit-er size was decreased in H2O�FLXams (4.1 � 1.3/litter) compared to H2Oams (5.5 � 1.9/litter), P � .04. Theean weight gain at day 14 in H2O�FLX
ams (5.2 � 1.2 g) was decreased whenompared to H2O dams (6.0 � 2.5 g);owever, this finding was not statisticallyignificant.
OMMENTength of gestation, the primary out-ome, was not affected by FLX exposurehen compared to H2O alone in a mouseodel; however, FLX exposure did affect
itter size and spontaneous fetal loss. Sig-ificant findings within this study in-lude the decrease in live birth rate and inhe mean litter size in dams receiving2O�FLX compared to dams receiving2O. These findings potentially suggestphysiological alteration at the placenta
evel during implantation and warranturther investigation. Current availableata on adverse pregnancy outcomes fol-
owing antenatal exposure to SSRIs, in-luding spontaneous abortion and pre-erm birth, in both human beings andnimals, remain contradictory. Severaluman studies support SSRI exposure as
n etiology for adverse pregnancy out- domes. Sparse literature from animalodels is available for comparison. Bairy
t al21 evaluated FLX exposure in ratsnd concluded that there was no signifi-ant alteration in the gestation period,nd reported no significant alterations initter size or birthweight.
The serotonin system includes at least4 receptors, multiple enzymes, andransporter proteins that exert influencen serotonin metabolism, release, andeuptake.22 SSRIs actively pass throughhe placenta and their metabolites haveeen detected in roughly equivalent val-es in both umbilical cord blood andmniotic fluid.23 Three plausible biolog-cal pathways for adverse pregnancy out-ome as a result of antenatal SSRI expo-ure are SSRI-associated increases inortisol, increases in estriol levels, andterine artery vasoconstriction.The first mechanism involves mater-
al cortisol levels, which have beenhown to predict the rise in corticotrop-n-releasing hormone (CRH), providingurther evidence of how stress hormones
ay work in concert to lead to early par-urition. SSRIs influence the hypotha-amic pituitary-adrenal axis feedback
echanisms, which also change duringregnancy. Glucocorticoids during preg-ancy have been shown to cause a progres-ive 20-fold increase in CRH levels acrosshe course of pregnancy. Hobel24 demon-trated that CRH levels increased moreramatically in women at risk for pretermelivery. FLX infusion has been associatedith an additional increase in the magni-
ude of the normal antenatal rise in fetallasma CRH, adrenocorticotropic hor-one, and cortisol concentrations.25
Next, salivary estriol has been showno be a marker for preterm birth. Suri etl26 measured salivary estriol, a hormonehat increases exponentially in the feweeks before the onset of spontaneous
erm and preterm labor, in pregnantomen with and without antidepressant
reatment. Prenatal antidepressant useas associated with significantly higher
alivary estriol levels in the second half ofregnancy. Whether estriol reflects aausal mechanism by which women onntidepressants have shorter pregnancy
uration remains to be further studied.27 pOCTOBER 2010 Americ
A final proposed mechanism relates tohe effect of FLX on plasma serotonin.LX prolongs exposure to endogenouslyeleased serotonin, a known potent uter-ne vasoconstrictor, thus leading to aransient reduction in uterine bloodow. This, in turn, would reduce the de-
ivery of oxygen and nutrients to the fe-us, thereby presenting a mechanism foreducing growth and/or eliciting pretermelivery.28 Following administration ofLX to pregnant ewes, Morrison et al29 re-orted a transient decrease in uterine ar-ery blood flow, fetal partial pressure of ox-gen and oxygen saturation.
One strength of this study includes theegree of precision to which the timedating was performed. Day 0 of gesta-
ion was estimated within 4 hourshereby providing a robust method fortudying the antenatal exposure of FLXs an etiology of adverse pregnancy out-omes. In addition, by calculating a sam-le size, statistical significant results cane confidently reported. This study pro-ides a novel method for studying thentenatal exposure of FLX as an etiologyf adverse pregnancy outcomes. Studiesave shown that placental transfer ofLX is similar between mouse and hu-an.30 Despite the advantage of targeted
xperiments in the mouse model andimilarities in placental cell types be-ween the mouse and human, the animal
odel might be limiting in understand-ng all aspects of the effects of antenatalSRI exposure in the physiology ofouse and human pregnancies.31 Theode of implantation differs betweenouse and human; there is shallow de-
idual invasion in mouse compared toxtensive uterine remodeling by invasiverophoblasts in human. In addition, theterine spiral arterioles in mice are re-odeled by maternal factors rather than
y invasive trophoblasts in human preg-ancies.32 Moreover, the short gesta-
ional period in mice and incomplete de-elopment at birth are unlike humanregnancies.In conclusion, we found that mice ex-
osed to FLX had similar gestationalengths, but FLX exposure did affect lit-er size and spontaneous loss. WhetherLX exposure induces these results on
regnancy outcome independently re-an Journal of Obstetrics & Gynecology 375.e3

maacpaniic
R1PcT2cAwi13WuptB4IA5tis56Rvub7Ssb8p2
9AstP1Aarnh81sn91tpa1cA1PpM1Rw11ah11oua1Kpt21qb22t
pi2Mq22tp2tdnI2O2nn2AaB2ar92dD2Rts43vovtO3c3Tf9
SMFM Papers www.AJOG.org
3
ains unclear. These findings warrantdditional investigation as they point tosignificant impact on pregnancy out-
omes associated with antenatal FLX ex-osure. Studies of the effects of serotonint the placental level at the time of preg-ancy implantation may also provide ev-
dence for some of the clinical outcomesdentified in this study and seen in thelinical literature. f
EFERENCES. Gaynes BN, Gavin N, Meltzer-Brody S, et al.erinatal depression: prevalence, screening ac-uracy, and screening outcomes. Evid Repechnol Assess (Summ) 2005;199:1-8.. American College of Obstetricians and Gyne-ologists Committee on Obstetric Practice.COG committee opinion no. 354: treatmentith selective serotonin reuptake inhibitors dur-
ng pregnancy. Obstet Gynecol 2006;108:601-3.. Bakker MK, Kolling P, van den Berg PB, dealle HE, de Jong van den Berg LT. Increase in
se of selective serotonin reuptake inhibitors inregnancy during the last decade, a popula-ion-based cohort study from the Netherlands.r J Clin Pharmacol 2007;65:600-6.. Cooper WO, Willy ME, Pont SJ, Ray WA.
ncreasing use of antidepressants in pregnancy.m J Obstet Gynecol 2007;196:544.e1-5.. Chambers CD, Hernandez-Diaz S, Van Mar-er LJ, et al. Selective serotonin-reuptake inhib-tors and risk of persistent pulmonary hyperten-ion of the newborn. N Engl J Med 2006;354:79-87.. Alwan S, Reefhuis J, Rasmussen SA, OlneyS, Friedman JM. National birth defects pre-ention study: use of selective serotonin-re-ptake inhibitors in pregnancy and the risk ofirth defects. N Engl J Med 2007;356:2684-92.. Louik C, Lin AE, Werler MM, Hernández-Díaz, Mitchell AA. First-trimester use of selectiveerotonin-reuptake inhibitors and the risk ofirth defects. N Engl J Med 2007;356:2675-83.. Hamilton BE, Martin JA, Ventura SJ. Births:reliminary data for 2005. Natl Vital Stat Rep
006;55:1-18. p75.e4 American Journal of Obstetrics & Gynecolo
. Suri R, Altshuler L, Hellemann G, Burt VK,quino A, Mintz J. Effects of antenatal depres-ion and antidepressant treatment on gesta-ional age at birth and risk of preterm birth. Am Jsychiatry 2007;164:1206-13.0. Oberlander TF, Warburton W, Misri S,ghajanian J, Hertzman C. Neonatal outcomesfter prenatal exposure to selective serotonineuptake inhibitor antidepressants and mater-al depression using population-based linkedealth data. Arch Gen Psychiatry 2006;63:98-906.1. Wen S, Yang Q, Garner P, et al. Selectiveerotonin reuptake inhibitors and adverse preg-ancy outcomes. J Obstet Gynecol 2006;194:61-6.2. Zeskind PS, Stephens LE. Maternal selec-ive serotonin reuptake inhibitor use duringregnancy and newborn neurobehavior. Pedi-trics 2004;113:368-75.3. Simon GE, Cunningham ML, Davis RL. Out-omes of prenatal antidepressant exposure.m J Psychiatry 2002;159:2055-61.4. Costei AM, Kozer E, Ho T, Ito S, Koren G.erinatal outcome following third trimester ex-osure to paroxetine. Arch Pediatr Adolesced 2002;156:1129-32.5. Chambers CD, Johnson KA, Dick LM, FelixJ, Jones KL. Birth outcomes in pregnantomen taking fluoxetine. N Engl J Med996;335:1010-5.6. Malm H, Klaukka T, Neuvonen PJ. Risksssociated with selective serotonin reuptake in-ibitors in pregnancy. Obstet Gynecol 2005;06:1289-96.7. Rahimi R, Nikfar S, Abdollahi M. Pregnancyutcomes following exposure to serotonin re-ptake inhibitors: a meta-analysis of clinical tri-ls. Reprod Toxicol 2006;22:571-5.8. Hemels ME, Einarson A, Koren G, LanctôtL, Einarson TR. Antidepressant use duringregnancy and the rates of spontaneous abor-ions: a meta-analysis. Ann Pharmacother005;39:803-9.9. Santarelli L, Saxe M, Cross C, et al. Re-uirement of hippocampal neurogenesis for theehavioral effects of antidepressants. Science003;301:305-9.0. Ansorge MS, Morelli E, Gingrich JA. Inhibi-ion of serotonin but not norepinephrine trans-
ort during development produces delayed,gy OCTOBER 2010
ersistent perturbations of emotional behaviorsn mice. J Neurosci 2008;28:199-207.1. Bairy KL, Madhyastha S, Ashok KP, Bairy I,alini S. Developmental and behavioral conse-uences of prenatal fluoxetine. Pharmacology007;79:1-11.2. Heils A, Teufel A, Petri S, et al. Allelic varia-ion of human serotonin transporter gene ex-ression. J Neurochem 1996;66:2621-4.3. Rampono J, Proud S, Hackett LP, Kris-ensen JH, Ilett KF. A pilot study of newer anti-epressant concentrations in cord and mater-al serum and possible effects in the neonate.
nt J Neuropsychopharmacol 2004;7:329-34.4. Hobel CJ. Stress and preterm birth. Clinbstet Gynecol 2004;47:856-80.5. Belik J. Fetal and neonatal effects of mater-al drug treatment for depression. Semin Peri-atol 2008;32:350-4.6. Suri R, Hellemann G, Cohen L, Aquino A,ltshuler L. Saliva estriol levels in women withnd without prenatal antidepressant treatment.iol Psychiatry 2008;64:533-7.7. Heine RP, McGregor JA, Goodwin TM, etl. Serial salivary estriol to detect an increasedisk of preterm birth. Obstet Gynecol 2000;6:490-7.8. Lundy B, Jones NA, Field T, et al. Prenatalepression effects on neonates. Infant Behavev 1999;22:119-29.9. Morrison JL, Chien C, Riggs KW, Gruber N,urak D. Effect of maternal fluoxetine adminis-
ration on uterine blood flow, fetal blood gastatus, and growth. Pediatr Res 2002;51:33-42.0. Noorlander CW, Ververs FF, Nikkels PG,an Echteld C, Visser G, Smidt MP. Modulationf serotonin transporter function during fetal de-elopment causes dilated heart cardiomyopa-hy and lifeline behavioral abnormalities. PLoSne 2008;3:e2782.1. Carter AM. Animal models of human pla-entation–a review. Placenta 2007;28:S41-7.2. Pijnenborg R, Vercruysse L, Hanssens M.he uterine spiral arteries in human pregnancy:
acts and controversies. Placenta 2006;27:39-58.