impact of perioperative blood pressure variability on health resource utilization after cardiac...
TRANSCRIPT

After Cardiac Surgery: An A
Impact of Perioperative Blood Pressure Variability on Health Resource Utilizationnalysis of the ECLIPSE Trials
Solomon Aronson, MD, MBA, FACC, FAHA, FCCM, FASE,* Jerrold H. Levy, MD, FAHA, FCCM,*
Philip D. Lumb, MD, BS, MCCM,† Manuel Fontes, MD,* Yamei Wang, MS,‡ Tracy A. Crothers, PharmD, BCPS,‡
Katherine A. Sulham, MPH,‡ and Marco S. Navetta, MD‡
Objective: To examine the impact of blood pressure con-
trol on hospital health resource utilization using data from
the ECLIPSE trials.
Design: Post-hoc analysis of data from 3 prospective,
open-label, randomized clinical trials (ECLIPSE trials).
Setting: Sixty-one medical centers in the United States.
Participants: Patients 18 years or older undergoing car-
diac surgery.
Interventions: Clevidipine was compared with nitrogly-
cerin, sodium nitroprusside, and nicardipine.
Measurements and Main Results: The ECLIPSE trials
included 3 individual randomized open-label studies com-
paring clevidipine to nitroglycerin, sodium nitroprusside,
and nicardipine. Blood pressure control was assessed as
the integral of the cumulative area under the curve (AUC)
outside specified systolic blood pressure ranges, such that
lower AUC represents less variability. This analysis examined
surgery duration, time to extubation, as well as intensive care
unit (ICU) and hospital length of stay (LOS) in patients with
AUC r10 mmHg � min/h compared to patients with
Journal of Cardiothoracic and Vascular Anesthesia, Vol ], No ] (Month), 2
AUC 410 mmHg � min/h. One thousand four hundred ten
patients were included for analysis; 736 patients (52%) had
an AUC r10 mmHg � min/h, and 674 (48%) had an
AUC 410 mmHg � min/h. The duration of surgery and
ICU LOS were similar between groups. Time to extubation
and postoperative LOS were both significantly shorter (p ¼0.05 and p o 0.0001, respectively) in patients with
AUC r10. Multivariate analysis demonstrates AUC r10
was significantly and independently associated
with decreased time to extubation (hazard ratio 1.132,
p ¼ 0.0261) and postoperative LOS (hazard ratio 1.221,
p ¼ 0.0006).
Conclusions: Based on data derived from the ECLIPSE
studies, increased perioperative BP variability is associated
with delayed time to extubation and increased postoper-
ative LOS.
& 2014 Elsevier Inc. All rights reserved.
KEY WORDS: health resources, thoracic surgery, hemostasis,antihypertensive agents, perioperative hypertension
From the *Department of Anesthesiology, Duke University MedicalCenter, Durham, NC, †Department of Anesthesiology, Keck School ofMedicine of the University of Southern California, Los Angeles, CA;and ‡The Medicines Company, Parsippany, NJ.
Address reprint requests to Solomon Aronson, MD, MBA, DukeUniversity Medical Center, Department of Anesthesiology 3094, 101Baker House, Duke South, Durham, NC 27710. E-mail: [email protected]© 2014 Elsevier Inc. All rights reserved.1053-0770/2601-0001$36.00/0http://dx.doi.org/10.1053/j.jvca.2014.01.004
DESPITE LARGE INVESTMENTS of resources in theform of skilled providers, hemodynamic monitoring, and
drugs to ensure cardiovascular stability, perioperative bloodpressure (BP) control remains a significant clinical focus.1–3
Perioperative BP, when highly variable or poorly controlled,has been reported to increase the risk of myocardial ischemia,stroke, neurocognitive dysfunction, acute kidney injury, andbleeding.4–6 Among several indices of BP variability, the meanduration of systolic BP excursion as well as the cumulativeproduct of the duration and magnitude of excursions eitherabove or below a clinical target range were shown to bepredictive of 30-day mortality in patients undergoing cardiacsurgery.7
Given the risk of these costly complications during cardiacsurgery, a better understanding of the association betweenclinical BP targets, including variability around these targets,and related health resource utilization in the United States isneeded. This analysis examines the impact of BP variability onhealth resource utilization using data from the ECLIPSE(Evaluation of Clevidipine in the Perioperative Treatment ofHypertension Assessing Safety Events) trials. The ECLIPSEtrials compared the safety and efficacy of perioperative BPcontrol in patients undergoing coronary artery bypass graft(CABG), valve surgery, or a combination between clevidipineand nitroglycerin, sodium nitroprusside, and nicardipine.3 Inthose trials, BP control was quantified by an area under thecurve (AUC) analysis that captured the magnitude and durationof excursions outside a specified range for systolic BP; lowerAUC values represented better BP control.
The study was designed to examine the association betweenBP variability as measured by AUC in patients undergoingcardiac surgery with surgery duration, time to extubation,intensive care unit (ICU) length of stay (LOS), and
postoperative LOS. It was hypothesized that reducing BPvariability and improving BP control would be associated withdecreased healthcare resource utilization.
METHODS
The methodology of the ECLIPSE trials has been publishedpreviously.3 It included 3 individual randomized open-label studiescomparing the safety of clevidipine with nitroglycerin, sodium nitro-prusside, and nicardipine in patients undergoing cardiac surgery.Written informed consent was obtained from all patients beforeenrollment, and the study was approved by the IRB at each participat-ing institution. The primary endpoint was safety, as assessed by theincidence of death, stroke, myocardial infarction, and renal dysfunctionthrough postoperative day 30.
The ECLIPSE trials enrolled adults (ages Z18 years; n ¼ 1,964)scheduled for cardiac surgery, including on- or off-pump CABG and/orvalve replacement or repair surgery at 61 medical centers in the UnitedStates between April 2004 and October 2006.3 Eligible patients wererandomized on a 1:1 basis to receive clevidipine, nitroglycerin, sodiumnitroprusside, or nicardipine in each of the 3 parallel studies. The needfor antihypertensive therapy and the appropriate level of BP controlwere determined by the study physician and continued until discharge
014: pp ]]]–]]] 1
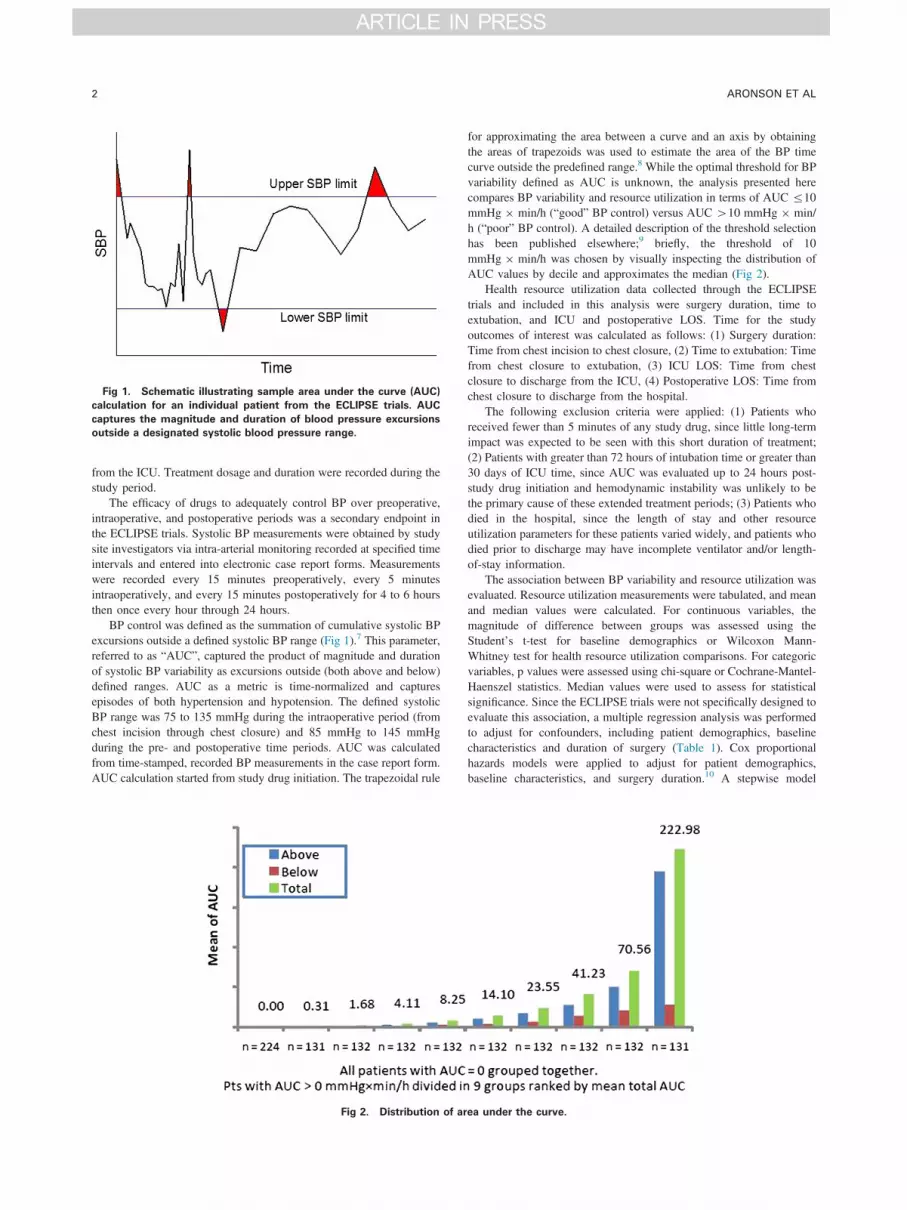
Fig 1. Schematic illustrating sample area under the curve (AUC)
calculation for an individual patient from the ECLIPSE trials. AUC
captures the magnitude and duration of blood pressure excursions
outside a designated systolic blood pressure range.
ARONSON ET AL2
from the ICU. Treatment dosage and duration were recorded during thestudy period.
The efficacy of drugs to adequately control BP over preoperative,intraoperative, and postoperative periods was a secondary endpoint inthe ECLIPSE trials. Systolic BP measurements were obtained by studysite investigators via intra-arterial monitoring recorded at specified timeintervals and entered into electronic case report forms. Measurementswere recorded every 15 minutes preoperatively, every 5 minutesintraoperatively, and every 15 minutes postoperatively for 4 to 6 hoursthen once every hour through 24 hours.
BP control was defined as the summation of cumulative systolic BPexcursions outside a defined systolic BP range (Fig 1).7 This parameter,referred to as “AUC”, captured the product of magnitude and durationof systolic BP variability as excursions outside (both above and below)defined ranges. AUC as a metric is time-normalized and capturesepisodes of both hypertension and hypotension. The defined systolicBP range was 75 to 135 mmHg during the intraoperative period (fromchest incision through chest closure) and 85 mmHg to 145 mmHgduring the pre- and postoperative time periods. AUC was calculatedfrom time-stamped, recorded BP measurements in the case report form.AUC calculation started from study drug initiation. The trapezoidal rule
Fig 2. Distribution of ar
for approximating the area between a curve and an axis by obtainingthe areas of trapezoids was used to estimate the area of the BP timecurve outside the predefined range.8 While the optimal threshold for BPvariability defined as AUC is unknown, the analysis presented herecompares BP variability and resource utilization in terms of AUC r10mmHg � min/h (“good” BP control) versus AUC 410 mmHg � min/h (“poor” BP control). A detailed description of the threshold selectionhas been published elsewhere;9 briefly, the threshold of 10mmHg � min/h was chosen by visually inspecting the distribution ofAUC values by decile and approximates the median (Fig 2).
Health resource utilization data collected through the ECLIPSEtrials and included in this analysis were surgery duration, time toextubation, and ICU and postoperative LOS. Time for the studyoutcomes of interest was calculated as follows: (1) Surgery duration:Time from chest incision to chest closure, (2) Time to extubation: Timefrom chest closure to extubation, (3) ICU LOS: Time from chestclosure to discharge from the ICU, (4) Postoperative LOS: Time fromchest closure to discharge from the hospital.
The following exclusion criteria were applied: (1) Patients whoreceived fewer than 5 minutes of any study drug, since little long-termimpact was expected to be seen with this short duration of treatment;(2) Patients with greater than 72 hours of intubation time or greater than30 days of ICU time, since AUC was evaluated up to 24 hours post-study drug initiation and hemodynamic instability was unlikely to bethe primary cause of these extended treatment periods; (3) Patients whodied in the hospital, since the length of stay and other resourceutilization parameters for these patients varied widely, and patients whodied prior to discharge may have incomplete ventilator and/or length-of-stay information.
The association between BP variability and resource utilization wasevaluated. Resource utilization measurements were tabulated, and meanand median values were calculated. For continuous variables, themagnitude of difference between groups was assessed using theStudent’s t-test for baseline demographics or Wilcoxon Mann-Whitney test for health resource utilization comparisons. For categoricvariables, p values were assessed using chi-square or Cochrane-Mantel-Haenszel statistics. Median values were used to assess for statisticalsignificance. Since the ECLIPSE trials were not specifically designed toevaluate this association, a multiple regression analysis was performedto adjust for confounders, including patient demographics, baselinecharacteristics and duration of surgery (Table 1). Cox proportionalhazards models were applied to adjust for patient demographics,baseline characteristics, and surgery duration.10 A stepwise model
ea under the curve.
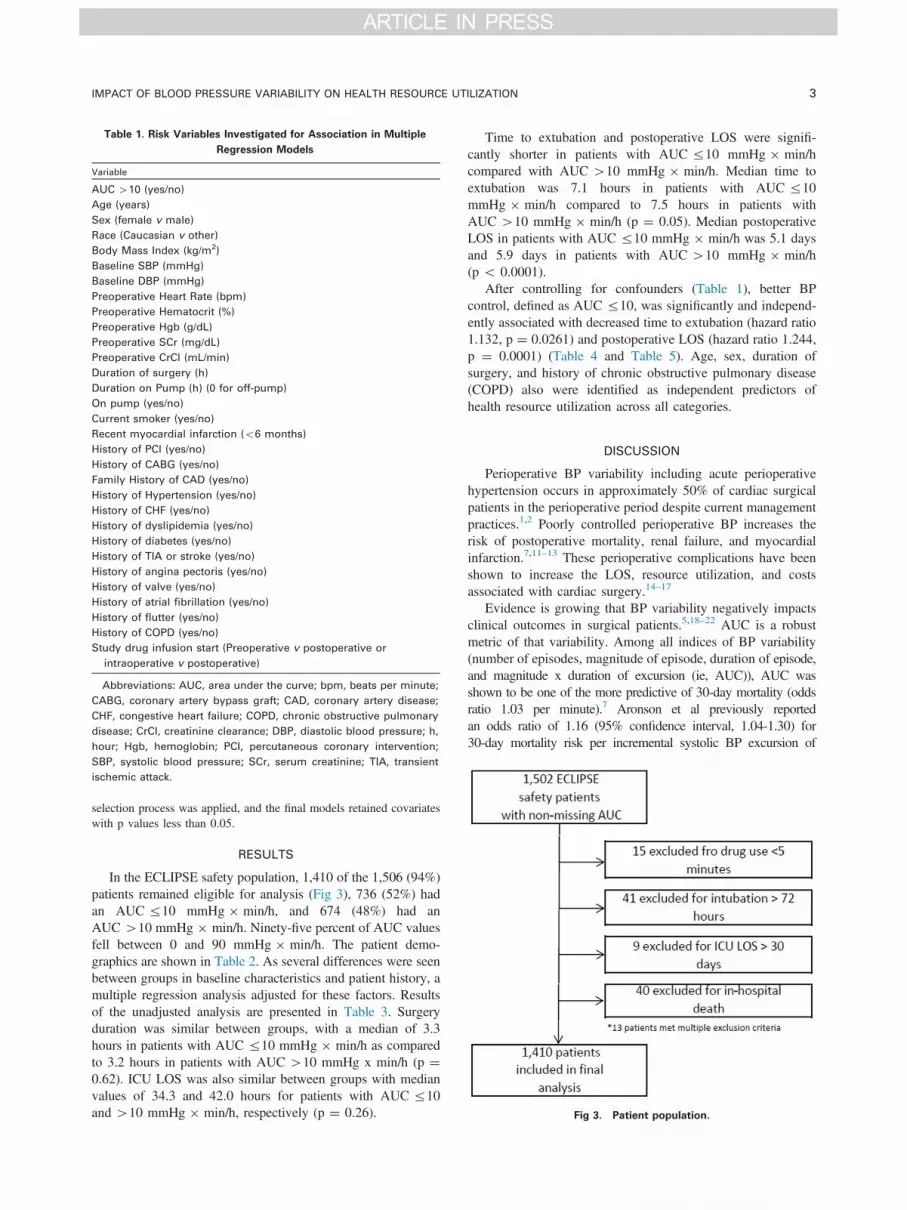
Fig 3. Patient population.
Table 1. Risk Variables Investigated for Association in Multiple
Regression Models
Variable
AUC 410 (yes/no)
Age (years)
Sex (female v male)
Race (Caucasian v other)
Body Mass Index (kg/m2)
Baseline SBP (mmHg)
Baseline DBP (mmHg)
Preoperative Heart Rate (bpm)
Preoperative Hematocrit (%)
Preoperative Hgb (g/dL)
Preoperative SCr (mg/dL)
Preoperative CrCl (mL/min)
Duration of surgery (h)
Duration on Pump (h) (0 for off-pump)
On pump (yes/no)
Current smoker (yes/no)
Recent myocardial infarction (o6 months)
History of PCI (yes/no)
History of CABG (yes/no)
Family History of CAD (yes/no)
History of Hypertension (yes/no)
History of CHF (yes/no)
History of dyslipidemia (yes/no)
History of diabetes (yes/no)
History of TIA or stroke (yes/no)
History of angina pectoris (yes/no)
History of valve (yes/no)
History of atrial fibrillation (yes/no)
History of flutter (yes/no)
History of COPD (yes/no)
Study drug infusion start (Preoperative v postoperative or
intraoperative v postoperative)
Abbreviations: AUC, area under the curve; bpm, beats per minute;
CABG, coronary artery bypass graft; CAD, coronary artery disease;
CHF, congestive heart failure; COPD, chronic obstructive pulmonary
disease; CrCl, creatinine clearance; DBP, diastolic blood pressure; h,
hour; Hgb, hemoglobin; PCI, percutaneous coronary intervention;
SBP, systolic blood pressure; SCr, serum creatinine; TIA, transient
ischemic attack.
IMPACT OF BLOOD PRESSURE VARIABILITY ON HEALTH RESOURCE UTILIZATION 3
selection process was applied, and the final models retained covariateswith p values less than 0.05.
RESULTS
In the ECLIPSE safety population, 1,410 of the 1,506 (94%)patients remained eligible for analysis (Fig 3), 736 (52%) hadan AUC r10 mmHg � min/h, and 674 (48%) had anAUC 410 mmHg � min/h. Ninety-five percent of AUC valuesfell between 0 and 90 mmHg � min/h. The patient demo-graphics are shown in Table 2. As several differences were seenbetween groups in baseline characteristics and patient history, amultiple regression analysis adjusted for these factors. Resultsof the unadjusted analysis are presented in Table 3. Surgeryduration was similar between groups, with a median of 3.3hours in patients with AUC r10 mmHg � min/h as comparedto 3.2 hours in patients with AUC 410 mmHg x min/h (p ¼0.62). ICU LOS was also similar between groups with medianvalues of 34.3 and 42.0 hours for patients with AUC r10and 410 mmHg � min/h, respectively (p ¼ 0.26).
Time to extubation and postoperative LOS were signifi-cantly shorter in patients with AUC r10 mmHg � min/hcompared with AUC 410 mmHg � min/h. Median time toextubation was 7.1 hours in patients with AUC r10mmHg � min/h compared to 7.5 hours in patients withAUC 410 mmHg � min/h (p ¼ 0.05). Median postoperativeLOS in patients with AUC r10 mmHg � min/h was 5.1 daysand 5.9 days in patients with AUC 410 mmHg � min/h(p o 0.0001).
After controlling for confounders (Table 1), better BPcontrol, defined as AUC r10, was significantly and independ-ently associated with decreased time to extubation (hazard ratio1.132, p ¼ 0.0261) and postoperative LOS (hazard ratio 1.244,p ¼ 0.0001) (Table 4 and Table 5). Age, sex, duration ofsurgery, and history of chronic obstructive pulmonary disease(COPD) also were identified as independent predictors ofhealth resource utilization across all categories.
DISCUSSION
Perioperative BP variability including acute perioperativehypertension occurs in approximately 50% of cardiac surgicalpatients in the perioperative period despite current managementpractices.1,2 Poorly controlled perioperative BP increases therisk of postoperative mortality, renal failure, and myocardialinfarction.7,11–13 These perioperative complications have beenshown to increase the LOS, resource utilization, and costsassociated with cardiac surgery.14–17
Evidence is growing that BP variability negatively impactsclinical outcomes in surgical patients.5,18–22 AUC is a robustmetric of that variability. Among all indices of BP variability(number of episodes, magnitude of episode, duration of episode,and magnitude x duration of excursion (ie, AUC)), AUC wasshown to be one of the more predictive of 30-day mortality (oddsratio 1.03 per minute).7 Aronson et al previously reportedan odds ratio of 1.16 (95% confidence interval, 1.04-1.30) for30-day mortality risk per incremental systolic BP excursion of
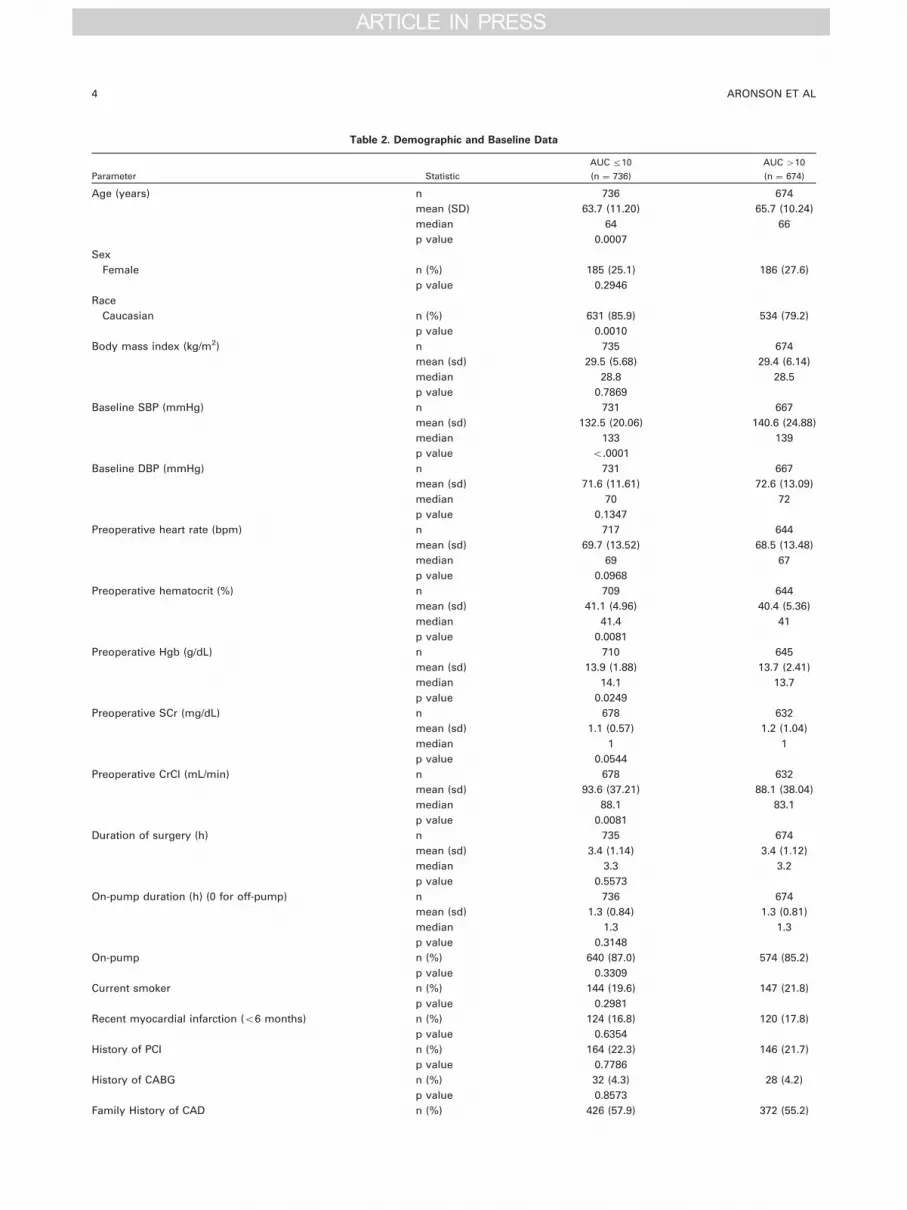
Table 2. Demographic and Baseline Data
Parameter Statistic
AUC r10
(n ¼ 736)
AUC 410
(n ¼ 674)
Age (years) n 736 674
mean (SD) 63.7 (11.20) 65.7 (10.24)
median 64 66
p value 0.0007
Sex
Female n (%) 185 (25.1) 186 (27.6)
p value 0.2946
Race
Caucasian n (%) 631 (85.9) 534 (79.2)
p value 0.0010
Body mass index (kg/m2) n 735 674
mean (sd) 29.5 (5.68) 29.4 (6.14)
median 28.8 28.5
p value 0.7869
Baseline SBP (mmHg) n 731 667
mean (sd) 132.5 (20.06) 140.6 (24.88)
median 133 139
p value o.0001
Baseline DBP (mmHg) n 731 667
mean (sd) 71.6 (11.61) 72.6 (13.09)
median 70 72
p value 0.1347
Preoperative heart rate (bpm) n 717 644
mean (sd) 69.7 (13.52) 68.5 (13.48)
median 69 67
p value 0.0968
Preoperative hematocrit (%) n 709 644
mean (sd) 41.1 (4.96) 40.4 (5.36)
median 41.4 41
p value 0.0081
Preoperative Hgb (g/dL) n 710 645
mean (sd) 13.9 (1.88) 13.7 (2.41)
median 14.1 13.7
p value 0.0249
Preoperative SCr (mg/dL) n 678 632
mean (sd) 1.1 (0.57) 1.2 (1.04)
median 1 1
p value 0.0544
Preoperative CrCl (mL/min) n 678 632
mean (sd) 93.6 (37.21) 88.1 (38.04)
median 88.1 83.1
p value 0.0081
Duration of surgery (h) n 735 674
mean (sd) 3.4 (1.14) 3.4 (1.12)
median 3.3 3.2
p value 0.5573
On-pump duration (h) (0 for off-pump) n 736 674
mean (sd) 1.3 (0.84) 1.3 (0.81)
median 1.3 1.3
p value 0.3148
On-pump n (%) 640 (87.0) 574 (85.2)
p value 0.3309
Current smoker n (%) 144 (19.6) 147 (21.8)
p value 0.2981
Recent myocardial infarction (o6 months) n (%) 124 (16.8) 120 (17.8)
p value 0.6354
History of PCI n (%) 164 (22.3) 146 (21.7)
p value 0.7786
History of CABG n (%) 32 (4.3) 28 (4.2)
p value 0.8573
Family History of CAD n (%) 426 (57.9) 372 (55.2)
ARONSON ET AL4
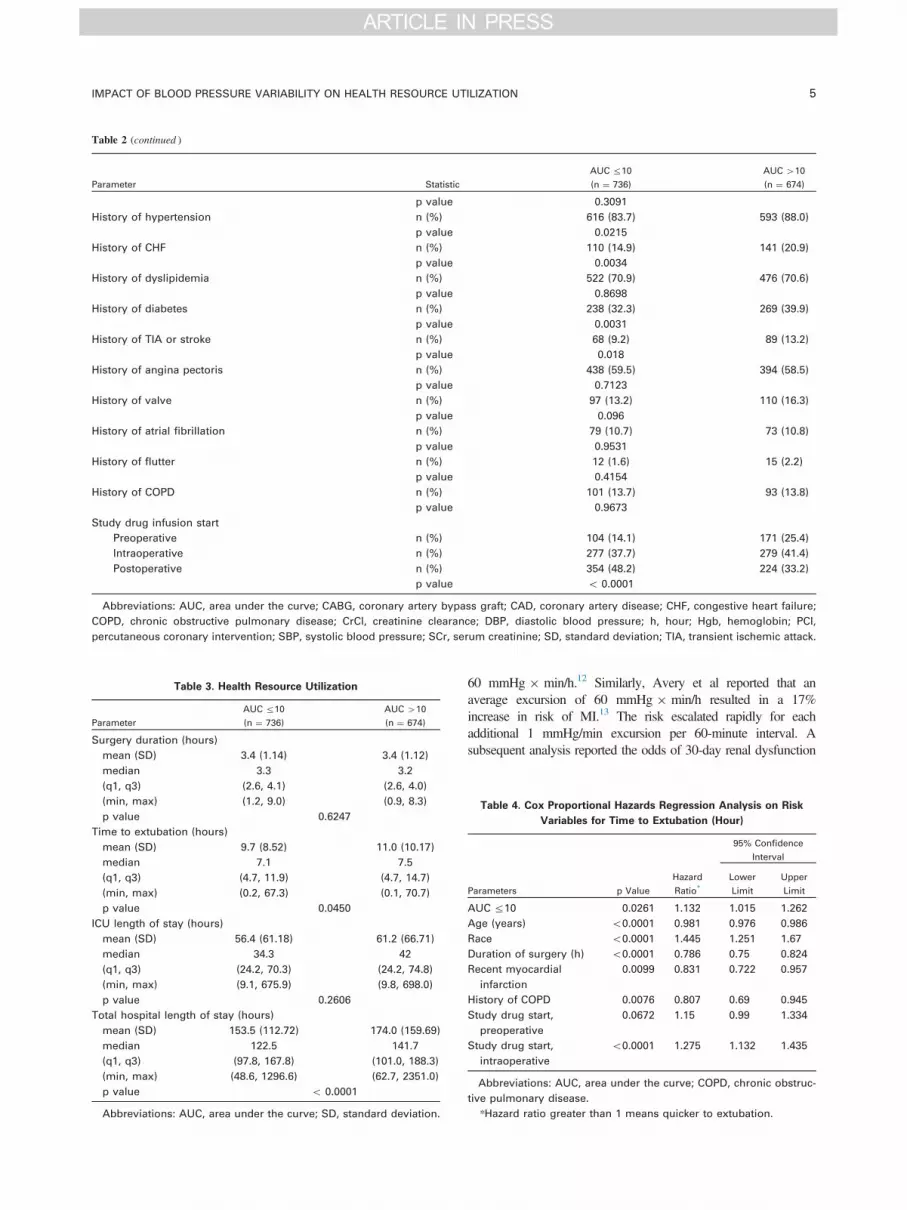
Table 2 (continued )
Parameter Statistic
AUC r10
(n ¼ 736)
AUC 410
(n ¼ 674)
p value 0.3091
History of hypertension n (%) 616 (83.7) 593 (88.0)
p value 0.0215
History of CHF n (%) 110 (14.9) 141 (20.9)
p value 0.0034
History of dyslipidemia n (%) 522 (70.9) 476 (70.6)
p value 0.8698
History of diabetes n (%) 238 (32.3) 269 (39.9)
p value 0.0031
History of TIA or stroke n (%) 68 (9.2) 89 (13.2)
p value 0.018
History of angina pectoris n (%) 438 (59.5) 394 (58.5)
p value 0.7123
History of valve n (%) 97 (13.2) 110 (16.3)
p value 0.096
History of atrial fibrillation n (%) 79 (10.7) 73 (10.8)
p value 0.9531
History of flutter n (%) 12 (1.6) 15 (2.2)
p value 0.4154
History of COPD n (%) 101 (13.7) 93 (13.8)
p value 0.9673
Study drug infusion start
Preoperative n (%) 104 (14.1) 171 (25.4)
Intraoperative n (%) 277 (37.7) 279 (41.4)
Postoperative n (%) 354 (48.2) 224 (33.2)
p value o 0.0001
Abbreviations: AUC, area under the curve; CABG, coronary artery bypass graft; CAD, coronary artery disease; CHF, congestive heart failure;
COPD, chronic obstructive pulmonary disease; CrCl, creatinine clearance; DBP, diastolic blood pressure; h, hour; Hgb, hemoglobin; PCI,
percutaneous coronary intervention; SBP, systolic blood pressure; SCr, serum creatinine; SD, standard deviation; TIA, transient ischemic attack.
Table 3. Health Resource Utilization
Parameter
AUC r10
(n ¼ 736)
AUC 410
(n ¼ 674)
Surgery duration (hours)
mean (SD) 3.4 (1.14) 3.4 (1.12)
median 3.3 3.2
(q1, q3) (2.6, 4.1) (2.6, 4.0)
(min, max) (1.2, 9.0) (0.9, 8.3)
p value 0.6247
Time to extubation (hours)
mean (SD) 9.7 (8.52) 11.0 (10.17)
median 7.1 7.5
(q1, q3) (4.7, 11.9) (4.7, 14.7)
(min, max) (0.2, 67.3) (0.1, 70.7)
p value 0.0450
ICU length of stay (hours)
mean (SD) 56.4 (61.18) 61.2 (66.71)
median 34.3 42
(q1, q3) (24.2, 70.3) (24.2, 74.8)
(min, max) (9.1, 675.9) (9.8, 698.0)
p value 0.2606
Total hospital length of stay (hours)
mean (SD) 153.5 (112.72) 174.0 (159.69)
median 122.5 141.7
(q1, q3) (97.8, 167.8) (101.0, 188.3)
(min, max) (48.6, 1296.6) (62.7, 2351.0)
p value o 0.0001
Abbreviations: AUC, area under the curve; SD, standard deviation.
IMPACT OF BLOOD PRESSURE VARIABILITY ON HEALTH RESOURCE UTILIZATION 5
60 mmHg � min/h.12 Similarly, Avery et al reported that anaverage excursion of 60 mmHg � min/h resulted in a 17%increase in risk of MI.13 The risk escalated rapidly for eachadditional 1 mmHg/min excursion per 60-minute interval. Asubsequent analysis reported the odds of 30-day renal dysfunction
Table 4. Cox Proportional Hazards Regression Analysis on Risk
Variables for Time to Extubation (Hour)
Parameters p Value
Hazard
Ratio*
95% Confidence
Interval
Lower
Limit
Upper
Limit
AUC r10 0.0261 1.132 1.015 1.262
Age (years) o0.0001 0.981 0.976 0.986
Race o0.0001 1.445 1.251 1.67
Duration of surgery (h) o0.0001 0.786 0.75 0.824
Recent myocardial
infarction
0.0099 0.831 0.722 0.957
History of COPD 0.0076 0.807 0.69 0.945
Study drug start,
preoperative
0.0672 1.15 0.99 1.334
Study drug start,
intraoperative
o0.0001 1.275 1.132 1.435
Abbreviations: AUC, area under the curve; COPD, chronic obstruc-
tive pulmonary disease.
*Hazard ratio greater than 1 means quicker to extubation.

Table 5. Cox Proportional Hazards Regression Analysis on Risk
Variables for Time From Chest Closure to Hospital Discharge (Hour)
Parameter p Value
Hazard
Ratio*
95% CI
Lower
Limit
Upper
Limit
AUC r10 0.0006 1.221 1.09 1.367
Age (years) 0.0002 0.988 0.982 0.994
Sex 0.0029 0.817 0.716 0.933
Race 0.0103 1.231 1.05 1.443
Body mass index 0.0116 0.985 0.973 0.997
Preoperative heart rate 0.0002 0.992 0.988 0.996
Preoperative CrCl o0.0001 1.005 1.003 1.007
Duration of surgery (h) o0.0001 0.839 0.785 0.896
Duration on Pump (h) 0.0043 0.874 0.797 0.959
History of CHF 0.0102 0.814 0.696 0.952
History of TIA or stroke 0.0291 0.814 0.676 0.979
History of COPD 0.0015 0.763 0.646 0.901
Abbreviations: AUC, area under the curve; CrCl, creatinine clear-
ance; h, hour; CHF, congestive heart failure; CI, confidence interval;
COPD, chronic obstructive pulmonary disease; TIA, transient ischemic
attack.
*Hazard ratio greater than 1 means shorter hospital length of stay.
ARONSON ET AL6
were 1.725 higher in patients with poorer BP control.12 In patientsundergoing non-cardiac and non-neurological surgical procedures,mean BP decreases of more than 30% from baseline wereassociated with a significant increase in risk of postoperativestroke.21 These data demonstrate that BP variability is commonand negatively impacts clinical outcomes in the surgical setting.
Despite this evidence, an optimal standard clinical thresholdfor adequate BP control using indices of variability has yet to beestablished. Establishing a threshold of variability that repre-sents adequate BP control will permit analysis of the clinicaland economic consequences of perioperative BP control andfacilitate specific recommendations regarding appropriate treat-ment strategies. The threshold of AUC r10 mmHg � min/hrhas been used in previous analyses.9 This analysis of theECLIPSE data demonstrated that BP control, specificallydefined as AUC r10 mmHg � min/h, was associated withimproved health resource utilization evidenced by decreasedtime to extubation and hospital discharge in patients undergoingcardiac surgery. Both mean and median values were similar andshowed directionally similar results regarding reduced resourceutilization with improved BP control, providing greater con-fidence in the results of the analysis.
This is the first analysis describing the association betweenBP control and resource utilization in the perioperative setting.In cardiac surgery, hemodynamic stability is often a thera-peutic threshold that, when met, allows patients to move from
higher-acuity care (eg, ICU setting) to lower-acuity care or totake the next step in a care pathway such as discontinuation ofmechanical ventilation.23,24 There is a need for better BPcontrol in order to reduce healthcare resource utilization inthe cardiac surgical care setting, and the relationship amongtreatment selection, BP control, and clinical and economicoutcomes may aid in improving cardiac care management andreducing costs.
Health care decisions are increasingly driven by a need toimprove clinical efficacy as well as reduce complications andhospital resource utilization. These needs dictate a requirementfor comparisons in efficacy, safety, and resource utilizationamong treatment options. Clinical issues such as BP instability,mechanical ventilation, bleeding, and other complications areassociated with increased ICU LOS, thereby increasingresource utilization and, ultimately, the cost of care.15,25 Thisanalysis demonstrated that adequately controlled BP, defined asAUC r10 mmHg � min/h, is associated with a reduction intime cardiac surgery patients spend on mechanical ventilationand in the hospital, avoiding both the clinical consequences andeconomic costs associated with each.
These data quantify (the trapezoidal assumptions) thedeviation from a clinically predetermined systolic BP set point.BP variability around this set point does not assume a normaltarget systolic BP but a variation around the set point. Studieshave shown that in hypertensive patients, increased variabilityis associated with more target organ damage.26 Additionally,there is no standard metric of measurement of BP variability.The ECLIPSE trials were not designed or powered for analysisof BP variability or health resource utilization across treatmentcomparisons; nevertheless, the authors’ findings demonstratethat BP variability is a key factor impacting total resourceutilization. Other limitations of the analysis include lack ofprotocol for weaning and extubation from mechanical ventila-tion and for discharge from the ICU and hospital; though thismay also result in the findings being considered to be morereflective of real-world practice. Resource utilization dataderived from randomized, controlled trials are often criticizedas being heavily protocol-driven and therefore not reflective ofreal-world practice. As these particular endpoints were notprotocol-driven, it is likely that extubation and dischargedecisions were made on the basis of clinical stability.These and other factors that may impact resource utilizationoutside of those described in Table 1 were not included inthe regression analysis. Finally, it is worth noting that thesedata were collected in 2004, and many changes in cardiacsurgical practice have since occurred, although theauthors maintain the principal importance of this associationremains.
REFERENCES
1. Vuylsteke A, Feneck RO, Jolin-Mellgård A, et al: Perioperativeblood pressure control: A prospective survey of patient management incardiac surgery. J Cardiothorac Vasc Anesth 14:269-273, 20002. Varon J, Marik PE: Perioperative hypertension management. Vasc
Health Risk Manag 4:615-627, 20083. Aronson S, Dyke CM, Stierer KA, et al: The ECLIPSE trials:
Comparative studies of clevidipine to nitroglycerin, sodium
nitroprusside, and nicardipine for acute hypertension treatment incardiac surgery patients. Anesth Analg 1071110-1071121, 20084. Aronson S, Boisvert D, Lapp W: Isolated systolic hypertension is
associated with adverse outcomes from coronary artery bypass graftingsurgery. Anesth Analg 94:1079-1084, 20025. Reich DL, Bennett-Guerrero E, Bodian CA, et al: Intraoperative
tachycardia and hypertension are independently associated with adverse
IMPACT OF BLOOD PRESSURE VARIABILITY ON HEALTH RESOURCE UTILIZATION 7
outcome in noncardiac surgery of long duration. Anesth Analg 95:273-277, 20026. Ono M, Arnaoutakis GJ, Fine DM, et al: Blood pressure
excursions below the cerebral autoregulation threshold during cardiacsurgery are associated with acute kidney injury. Crit Care Med 41:464-471, 20137. Aronson S, Stafford-Smith M, Phillips-Bute B, et al: Intraoperative
systolic blood pressure variability predicts 30-day mortality in aorto-coronary bypass surgery patients. Anesthesiology 113:305-312, 20108. Epperson JF: An Introduction to Numerical Methods and Anal-
ysis. Rev. ed. Hoboken, NJ: John Wiley & Sons, 20079. Getsios D, Wang Y, Stolar M, et al: Improved perioperative blood
pressure control leads to reduced hospital costs. Expert Opin Pharmac-other 14:1285-1293, 201310. Basu A, Manning WG, Mullahy J: Comparing alternative models:
Log vs Cox proportional hazard. Health Economics 13:749-765, 200411. Aronson S, Cheung A, Stierer K, et al: Perioperative blood
pressure control predicts renal dysfunction in cardiac surgery patients.Anesthesiology 107:A1253, 200712. Aronson S, Dyke CM, Levy JH, et al: Does perioperative systolic
blood pressure variability predict mortality after cardiac surgery? Anexploratory analysis of the ECLIPSE trials. Anesth Analg 113:19-30, 201113. Avery E, Richardson J Jr, Dyke C, et al: Blood pressure control
predicts 30-day myocardial infarction in cardiac surgery patients:Analysis from the ECLIPSE trials. Anesth Analg 106(SCA Suppl):1-128; SCA69, 200814. Ghali WA, Hall RE, Ash AS, et al: Identifying pre- and
postoperative predictors of cost and length of stay for coronary arterybypass surgery. Am J Med Qual 14:248-254, 199915. Brown PP, Kugelmass AD, Cohen DJ, et al: The frequency and
cost of complications associated with coronary artery bypass graftingsurgery: Results from the United States Medicare program. Ann ThoracSurg 85:1980-1986, 2008
16. Hall RE, Ash AS, Ghali WA, et al: Hospital cost of complica-tions associated with coronary artery bypass graft surgery. Am JCardiol 79:1680-1682, 199717. Dasta JF, Kane-Gill S, Durtschi AJ, et al: Costs and outcomes of
acute kidney injury (AKI) following cardiac surgery. Nephrol DialTransplan 23:1970-1974, 200818. Aronson S, Boisvert D, Lapp W: Isolated systolic hypertension is
associated with adverse outcomes from coronary artery bypass graftingsurgery. Anesth Analg 94:1079-1084, 200219. Charlson ME, MacKenzie CR, Gold JP, et al: Intraoperative
blood pressure. What patterns identify patients at risk for postoperativecomplications? Ann Surg 212:567-580, 199020. Charlson ME, MacKenzie CR, Gold JP, et al: The preoperative
and intraoperative hemodynamic predictors of postoperative myocar-dial infarction or ischemia in patients undergoing noncardiac surgery.Ann Surg 210:637-648, 198921. Bjilker JB, Persoon S, Peelen LM, et al: Intraoperative
hypotension and perioperative ischemic stroke after general surgery:A nested case-control study. Anesthesiology 116:658-664, 201222. Sessler DI, Sigl JC, Kelley SD, et al: Hospital stay and mortality
are increased in patients having a “triple low” of low blood pressure,low bispectral index, and low minimum alveolar concentration ofvolatile anesthesia. Anesthesiology 116:1195-1203, 201223. Higgins TL, Yared JP, Ryan T: Immediate postoperative care of
cardiac surgical patients. JCVA 10:643-658, 199624. Hajjar LA, Vincent JL, Gales FRBG, et al: Transfusion require-
ments after cardiac surgery: The TRACS randomized controlled trial.JAMA 304:1559-1567, 201025. Dasta JF, McLaughlin TP, Mody SH, et al: Daily cost of an
intensive care unit day: The contribution of mechanical ventilation. CritCare Med 33:1266-1271, 200526. Rothwell PM, Howard SC, Dolan E, et al: Prognostic signifi-
cance of visit-to-visit variability, maximum systolic blood pressure, andepisodic hypertension. Lancet 375:895-905, 2010